Embed Size (px)
Citation preview

THE SANDWICH THEORYA bioactivity based explanation for posterior capsule opacification after cataract surgery with intraocular lens implantation
REIJOLINNOLA
Department of Ophthalmology,Department of Medical Biochemistry,
Collagen Research Unit,University of Oulu
OULU 2001

REIJO LINNOLA
THE SANDWICH THEORYA bioactivity based explanation for posterior capsule opacification after cataract surgery with intraocular lens implantation
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in the Auditorium 5 of the University Hospitalof Oulu, on June 18th, 2001, at 12 noon.
OULUN YLIOPISTO, OULU 2001

Copyright © 2001University of Oulu, 2001
Manuscript received 26 April 2001Manuscript accepted 3 May 2001
Communicated byDocent Hannu UusitaloDocent Risto Uusitalo
ISBN 951-42-5979-3 (URL: http://herkules.oulu.fi/isbn9514259793/)
ALSO AVAILABLE IN PRINTED FORMATISBN 951-42-5978-5ISSN 0355-3221 (URL: http://herkules.oulu.fi/issn03553221/)
OULU UNIVERSITY PRESSOULU 2001

Linnola, Reijo, The sandwich theory. A bioactivity based explanation for posteriorcapsule opacification after cataract surgery with intraocular lens implantationDepartment of Ophthalmology, Department of Medical Biochemistry, University of Oulu, P.O.Box5000, FIN-90014 University of Oulu, Finland, Collagen Research Unit, University of Oulu,Kajaanintie 52 A, FIN-90220 Oulu, Finland 2001Oulu, Finland(Manuscript received 26 April 2001)
Abstract
This study was undertaken to identify mechanisms of adhesion of intraocular lenses (IOLs) to thecapsular bag after cataract surgery and IOL implantation. It was also done to challenge the sandwichtheory presented for posterior capsular opacification (PCO): If the IOL is made of a bioactive materialit would allow a single lens epithelial cell layer to bond both to the IOL and the posterior capsule atthe same time. This would produce a sandwich pattern including the IOL, the cell monolayer and theposterior capsule. The sealed sandwich structure would prevent further epithelial ingrowth. Thedegree of bioactivity of the IOL could explain the basic difference in the incidence of PCO andcapsulotomy rates with different IOL materials.
The sandwich theory was put forward on the basis of a search for a keratoprosthesis material,which would allow maximal adhesion of the prosthesis to corneal tissue. Titanium and glass-ceramiccoated titanium were found to develop better adhesion than poly (methyl methacrylate) (PMMA).The adhesion of PMMA to the corneal stromal tissue was loose, and down growth of cornealepithelial cells was seen around the prosthesis.
The differences between various IOL materials were first tested with rabbit corneal tissuecultures. There was better adhesion of corneal tissue to soft, hydrophobic acrylate than to PMMA,heparin surface modified (HSM)-PMMA, silicone or hydrogel IOLs.
To assess differences in protein adhesion to IOL surfaces, different IOLs were incubated for 24hours with radioactive iodine labeled fibronectin. Soft hydrophobic acrylate (AcrySof®) showed thehighest binding of fibronectin, and the differences relative to all the other materials were significant(p<0.01-0.001), except to PMMA (p=0.31).
The sandwich theory and the results with rabbit corneal tissue cultures and the protein adhesionstudy in vitro were evaluated against the results found in pseudophakic autopsy eyes. Altogether, 70autopsy eyes were analyzed. From 38 autopsy eyes containing PMMA, silicone, soft hydrophobicacrylate or hydrogel IOLs histological sections were prepared from the capsular bag andimmunohistochemical analyses were performed for fibronectin, vitronectin, laminin and collagentype IV. A total of 152 specimens were analyzed. From 32 autopsy eyes containing IOLs made ofPMMA, silicone, acrylate or hydrogel, IOLs were explanted from the capsular bag andimmunohistochemical analysis was done on both sides of the IOLs for fibronectin, vitronectin,laminin or collagen type IV. Soft hydrophobic acrylate IOLs had significantly more adhesion offibronectin to their surfaces than PMMA or silicone IOLs. Also, more vitronectin was attached toacrylate IOLs than to the other IOL materials. Silicone IOLs had more collagen type IV adhesion incomparison to the other IOL materials studied. In histologic sections a sandwich-like structure(anterior or posterior capsule-fibronectin-one cell layer-fibronectin-IOL surface) was seensignificantly more often in eyes with acrylate IOLs than in PMMA, silicone or hydrogel IOL eyes.
These studies support the sandwich theory for posterior capsule opacification after cataractsurgery with IOLs. The results suggest that fibronectin may be the major extracellular proteinresponsible for the attachment of acrylate IOLs to the capsular bag. This may represent a truebioactive bond between the IOL and the lens epithelial cells, and between the IOL and the capsularbag. This may explain the reason for clinical observations of less posterior capsular opacification andlower capsulotomy rates with the soft hydrophobic acrylate material of AcrySof® IOLs compared tothe other IOL materials studied.
Keywords: intraocular lenses, cataract surgery, posterior capsule opacification, fibronectin,vitronectin, laminin, collagen type IV

To Antti, Mikko, Lassi and Saku
The Linnola Boys go to New York


Acknowledgements
The research for this thesis was carried out at the Departments of Ophthalmology andMedical Biochemistry, University of Oulu, the Departments of Prosthetics andMaxillofacial Surgery, Institute of Dentistry, University of Turku, and at the Center forResearch on Ocular Therapeutics and Biodevices, Storm Eye Institute, MedicalUniversity of South Carolina, Charleston, USA, during the years 1991-2000.
I wish to express my gratitude to emeritus Professor Ulf Krause, the Department ofOphthalmology, University of Oulu, for first introducing me to scientific research. Withhis personal experience in operating keratoprosthesis into patient eyes, we started ourstudy with different materials in keratoprostheses. Again, by his initiative, we tookcontact with the Departments of Prosthetics and Maxillofacial Surgery, Institute ofDentistry, University of Turku, because of their invention and experience of bioactiveglass- ceramic in dental prostheses. In Turku, I want to thank all our co-workers,Professor Antti Yli-Urpo and Professor Risto-Pekka Happonen, Erik Vedel, M.Sc. andÖrjan Andersson, Ph.D. Especially Professor Risto-Pekka Happonen used his time andexperience in pathology in analyzing the histologic specimen together with me. Themanufacturing of the prostheses and analyzing of the histologic results were done inTurku. The operations of the rabbits were done in the University of Oulu, where I want tothank Mr. Veikko Lähteenmäki and Mr. Rauno Pudas for their help in the operations, andMr. Heikki Nieminen for his help in photography.
Still, this thesis would not have been done without Mr. Tero Sandberg, at that timebeing working with Pharmacia & Upjohn, Finland. He asked me to participate in a studyfor intraocular lenses (IOL). This study thought me the real methods and hard workneeded to produce the information for American FDA approval for a new silicone IOL.At the same time I learned a critical attitude for observation the postoperative IOLperformance in the eye. At this place I also want to thank Tom Henricson, MD, formerchief of the Department of Ophthalmology, Central Hospital of Vaasa, for teaching mehow to operate cataract patients.
I express my gratitude to Richard Lambert, PhD, D.V.M, Surgical Products Research,Alcon Laboratories, Fort Worth, USA. After the Sandwich theory was published, he wasinterested enough to visit me in Vaasa, for discuss further ways to study the IOL, lensepithelial cell, and capsular bag interaction after cataract surgery. In later studies he has
helped us together the many people in their research department. For his help he will begranted a reindeer skin, when I will next time meet him. He has also helped in revisingthe English language in this thesis together with Professor Leila Laatikainen, theDepartment of Ophthalmology, and University of Helsinki. I greatly thank both of them.
I want to thank Professor Taina Pihlajaniemi, Malin Sund, MD and Riikka Ylönen,Med Cand, for their excellent co-working in our protein adhesion studies at the CollagenResearch Unit, Biocenter and the Department of Medical Biochemistry, University ofOulu. It was their knowledge of extracellular proteins and the methods for studying them,which helped us further. Our next study was also greatly helped by Malin Sund, MD,because she helped me to plan the methods to evaluate the extracellular matrix proteins inthe pseudophakic autopsy eyes.Finally, the results of our keratoprosthesis study, the sandwich theory, and the resultsobtained in rabbit tissue cultures and in protein adhesion studies to the IOLs, could beevaluated against the results obtained with human pseudophakic autopsy eyes at theCenter for Research on Ocular Therapeutics and Biodevices, Storm Eye Institute,Medical University of South Carolina, Charleston, USA. I wish to express my gratitudeto Professor David Apple, for taking interest in our project, being with it, and helping itwith all the means the Storm Eye Institute offers. I warmly want to thank all the people,who worked in our project there: Liliana Werner, MD, PhD, Marcela Escobar-Gomez,MD, Suresh K. Pandey, MD, and Sergey L. Znoiko, MD, PhD. Without their hard workthis thesis would not have been possible to finish. And not to forget the invaluable help ofJoyce Edmonds, HTL, for providing us the numerous sections we needed all the time, andnearly always in a hurry. These studies in Charleston generated huge amount of data, andI want to thank Dr. David J. Schaeffer, Ecohealth Research, Inc., Champaign, Illinois,USA, for running the statistical analyses for us.
I owe my heartfelt gratitude to my mother Liisa, my father Veikko, and to my sistersMarja-Leena and Satu. My parents have taught me how to work to obtain the coals I haveset for me and I have always got the most wonderful support for my studies there. Iremember the atmosphere in my childhood home to have been a very optimistic one, andI am happy to be able to say, that I carry the same optimism still. I thank my wife Tarja,for taking care of our children Antti, Mikko, Lassi, and Saku, while I have been away forthe studies for this thesis. She has been patient for doing this, and she has never lost anopportunity to encourage me during this time.
This research has been supported by grants provided by the University of Oulu,Sokeain Ystävät r.y, the Finnish Eye and Tissue bank, Technology Development Center inFinland (TEKES), the Medical Research Council of the Academy of Finland, the FinnishAssociation for Eye Research, the Eye Foundation, the Medical Association of Vaasa, andAlcon, USA. Kabi Pharmacia, Uppsala, Sweden, kindly provided the PMMA optics forthe keratoprostheses. The numerous IOLs needed in rabbit corneal culture studies and invitro protein adhesion studies were kindly provided by Alcon, Helsinki, Finland, AllerganMedical Optics, Helsinki, Finland, Bausch & Lomb, Helsinki, Finland, and Pharmacia,Helsinki, Finland.

Abbreviations
AEC aminoethylcarbazoleACO anterior capsule opacificationα-SM α-smooth muscle actinBAB blood-aqueous barrierBGC bioactive glass-ceramicCAM cell adhesion moleculesCBS corneal basement membrane CCC continuous curvilinear capsulorhexisCCT computer-compatible tape stepsCNC computer numeric controlledCME cystoid macular edemaDMDPS dimethyldiphenylsiloxaneECCE extracapsular cataract extractionECM extracellular matrixEDXA energy dispersive x-ray analysesIOL intraocular lensIOP intraocular pressureLEC lens epithelial cellNd: YAG neodymium: yttrium-aluminium-garnetPBS phosphate-buffered salinePCCC posterior continuous curvilinear capsulorhexisPCO posterior capsule opacificationPMMA poly (methyl methacrylate)SD standard deviationSEM scanning electron microscopyTGF- β transforming growth factor - β


List of original publications
This thesis is based on the following articles, which are referred to in the text by theirRoman numerals:
I Linnola RJ, Happonen R-P, Andersson ÖH, Vedel E, Yli-Urpo AU, Krause U &Laatikainen L (1996) Titanium and bioactive glass-ceramic coated titanium as mate-rials for keratoprosthesis. Exp Eye Res 63:471-478.
II Linnola RJ (1997) The sandwich theory: a bioactivity based explanation for poste-rior capsule opacification after cataract surgery. J Cataract Refract Surg 23:1539-1542.
III Linnola RJ, Salonen JI & Happonen R-P (1999) Intraocular lens bioactivity testedusing rabbit corneal tissue cultures. J Cataract Refract Surg 25:1480-1485.
IV Linnola RJ, Sund M, Ylönen R & Pihlajaniemi T (1999) Adhesion of solublefibronectin, laminin, and collagen type IV to intraocular lens materials. J CataractRefract Surg 25:1486-1491.
V Linnola RJ, Werner L, Pandey SK, Escobar-Gomez M, Znoiko S & Apple DJ (2000)Adhesion of fibronectin, vitronectin, laminin and collagen type IV to intraocularlens materials in pseudophakic human autopsy eyes; Part 1: Histological sections. JCataract Refract Surg 26:1792-1806.
VI Linnola RJ, Werner L, Pandey SK, Escobar-Gomez M, Znoiko S & Apple DJ (2000)Adhesion of fibronectin, vitronectin, laminin and collagen type IV to intraocularlens materials in pseudophakic human autopsy eyes; Part 2: Explanted IOLs. J Cata-ract Refract Surg 26:1807-1818.


Contents
Abstract Acknowledgements Abbreviations List of original publications1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 172 Review of literature . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
2.1 Posterior capsule opacification after cataract surgery with intraocular lens implantation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.1.1 Embryology and anatomy of the lens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 192.1.2 Cataract surgery with intraocular lens implantation . . . . . . . . . . . . . . . . . . 20
2.1.2.1 History of intraocular lens implantation surgery . . . . . . . . . . . . . . 202.1.2.2 Effects of cataract surgery on the blood aqueous barrier . . . . . . . . 202.1.2.3 Cell reactions on the anterior surface of intraocular lenses . . . . . . 23
2.1.3 Definition and origin of posterior capsule opacification . . . . . . . . . . . . . . 242.1.4 Methods to evaluate posterior capsule opacification . . . . . . . . . . . . . . . . . 252.1.5 Amount of posterior capsule opacification with different intraocular
lens materials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 262.1.6 Extracellular matrix proteins associated with posterior
capsule opacification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292.2 Anterior capsule opacification and movement over
the intraocular lens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322.3 Methods for preventing posterior capsule opacification . . . . . . . . . . . . . . . . . . . 33
2.3.1 Design of the intraocular lens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 332.3.2 Surface modification and coating of the intraocular lens . . . . . . . . . . . . . . 342.3.3 Capsular bag tension ring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 352.3.4 Posterior continuous curvilinear capsulorhexis . . . . . . . . . . . . . . . . . . . . . 362.3.5 Agents for inhibiting lens epithelial cell growth . . . . . . . . . . . . . . . . . . . . 36
2.3.5.1 Antimetabolites . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 372.3.5.2 Immunotoxins and lens epithelial cell adhesion molecules as
blocking agents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 372.3.5.3 Anti-inflammatory and immunomodulating drugs . . . . . . . . . . . . 38
2.4 Methods to treat posterior capsule opacification . . . . . . . . . . . . . . . . . . . . . . . . . 382.4.1 Surgical discission and polishing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38

2.4.2 Neodymium: YAG-laser capsulotomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 392.4.2.1 Complications after neodymium: YAG-laser capsulotomy . . . . . . 39
3 Purpose of the present study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 414 Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
4.1 Study of the corneal tissue response and formation of a bioactive bond between rabbit corneal tissue and different keratoprosthesis materials . . . . . . . 434.1.1 Model and fabrication of keratoprosthesis . . . . . . . . . . . . . . . . . . . . . . . . . 434.1.2 Implantation of the prosthesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 444.1.3 Analysis of corneal tissues with the keratoprosthesis . . . . . . . . . . . . . . . . 45
4.2 Rabbit corneal tissue cultures on different IOL materials . . . . . . . . . . . . . . . . . . 454.2.1 IOLs used in tissue culture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 454.2.2 Preparation of histologic sections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
4.3 Adhesion of soluble fibronectin, laminin and collagen type IV to differentIOL materials in vitro . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 474.3.1 Incubation method and IOLs used with radioactive labeled proteins . . . . 47
4.4 Adhesion of fibronectin, vitronectin, laminin and collagen type IV to IOL materials in pseudophakic human autopsy eyes; The histologic sections 484.4.1 Immunohistochemical method and IOLs used . . . . . . . . . . . . . . . . . . . . . . 484.4.2 Statistical analyses used for histologic sections . . . . . . . . . . . . . . . . . . . . . 50
4.5 Adhesion of fibronectin, vitronectin, laminin and collagen type IV to IOL materials in pseudophakic human autopsy eyes; explanted IOLs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 504.5.1 Histologic methods and IOLs used . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 504.5.2 Statistical analyses used for explanted IOLs . . . . . . . . . . . . . . . . . . . . . . . 51
5 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 525.1 Outcome of keratoprosthesis made of titanium, bioactive glass-coated
titanium and PMMA in rabbit cornea (I) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 525.1.1 Clinical findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 525.1.2 Histologic findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 535.1.3 Scanning electron microscopy (SEM) and energy dispersive X-ray
analysis (EDXA) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.2 Outcome of rabbit corneal tissue cultures on different
IOL materials (III) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 555.3 Adhesion of soluble fibronectin, laminin and collagen type IV to different IOL
materials in vitro (IV) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 565.4 Adhesion of fibronectin, vitronectin, laminin and collagen
type IV to IOL materials in pseudophakic human autopsy eyes;the histologic sections (V) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
5.5 Adhesion of fibronectin, vitronectin, laminin and collagentype IV to IOL materials in pseudophakic human autopsy eyes;Explanted IOLs (VI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
6 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 606.1 Bioactive bonding of different keratoprosthesis materials to tissues . . . . . . . . . 606.2 Sandwich theory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 616.3 Cell and tissue reactions and adhesion to different IOL materials . . . . . . . . . . . 63

6.4 Extracellular matrix proteins with different IOL materials in vitro and in vivo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 646.4.1 Fibronectin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 646.4.2 Vitronectin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 656.4.3 Laminin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 666.4.4 Collagen type IV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
7 Summary and conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68Color plate 1-5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78


1 Introduction
Posterior capsule opacification (PCO) is a major complication of successful cataractsurgery. Secondary cataract caused by PCO is one of the leading causes of blindness inunderdeveloped countries. It can be treated with Nd: YAG laser capsulotomy, but theprocedure is not without complications: marks on the IOL (12%), transient elevation ofIOP (8.5%), cystoid macular edema (0.68%), retinal detachment (0.17%), hyphema(0.15%), iritis (0.10%), and IOL entrapment (0.10%) have been reported (Shah et al.1986). To treat PCO requires resources in medical personnel and it is not free of costs.Also, patients need to know that the complication will likely occur, so that they can seekmedical help if the visual acuity declines after initial successful cataract surgery.Particularly in underdeveloped countries, both the lack of this knowledge and theresources for performing Nd: YAG capsulotomy can prevent the treatment.
The number of cataract operations in Finland in 1998 was 36574. This is 7,1operations per 1000 inhabitants; the method for operation was phacoemulsification in94.7% (Krootila 2000). The number of capsulotomies performed per year is not known.The same numbers in the USA in 1998 were: 1.6 million cataract operations and 573000Nd:YAG capsulotomies (the Health Care Financing Administration 2000).
Capsulotomy frequencies in various series using different IOL types are shown inTable 1. In studies with the longest follow-up times (36-144 months), the capsulotomyrates range from 50-55% for PMMA or heparin surface-modified PMMA (Khan et al.1999, Winther-Nielsen et al. 1998), and 40.6% for silicone (Milazzo et al. 1996) to 0.75%for soft, hydrophobic acrylate IOLs (Akahoshi 1999). The square edge of an IOL optichas been shown to be an advantage in hindering PCO (Nishi et al. 1998a, Oshika et al.1998, Kruger et al. 2000, Peng et al. 2000a), and the surgical prevention of PCO is helpedby thorough cortical material removal by hydrodissection (Peng et al. 2000b). It seems,however, that the choice of the IOL material makes a significant difference in theincidence of PCO and the amount of work needed after cataract surgery.
This study was undertaken to identify mechanisms of adhesion of intraocular lenses(IOLs) to the capsular bag after cataract surgery and IOL implantation. It was also done tochallenge the sandwich theory presented for posterior capsular opacification (PCO). Inthe following text, IOLs made of PMMA, HSM-PMMA, silicone or hydrogel are referred

18
to according to their material, and hydrophobic soft acrylate IOLs (AcrySof®, Alcon,Fort Worth, TX) are referred to hereafter as acrylate IOLs. In the case of other softacrylate IOLs being studied, their names are mentioned.

2 Review of literature
2.1 Posterior capsule opacification after cataract surgery with intraocular lens implantation
2.1.1 Embryology and anatomy of the lens
The lens is derived from surface ectoderm. According to Olson (1989), the lens vesicleseparates from the ectoderm after the approaching optic vesicle has influenced a changein cuboidal cells to a single layer of columnar cells. In this phase, the apices of the cellsare turned inward, and the basement membrane, which originally supported the surface ofectoderm, now lies on the exterior surface of the structure and becomes the lens capsule.Cells under the anterior capsule remain as a single layer of cells, which divide and movehorizontally. Primary lens fibers are formed by elongation of the cells in the posteriorregion until they reach the apices of the anterior cells, and secondary fibers are formed bythe proliferation of equatorial cells. The equatorial diameter of the lens is 6.5 mm at birth,reaches 9.0 mm by the age 15 years, and remains constant thereafter. The anteroposteriordiameter of the lens is 3.5 mm in a newborn and reaches 5.0 mm in the adult (Olson1989).
The lens capsule is a transparent, PAS-positive, anteriorly 14-21 µm, posteriorly in themiddle 4 µm thick, elastic basement membrane. It is first a thin structure increasing inthickness until approximately 35 years of age when the equator and the posterior surfacethin slightly while the anterior surface remains stable (Olson 1989). The components ofthe capsule can be studied with immunohistochemical methods. The posterior capsuleshows immunoreactivity for laminin and collagen type IV (Saika et al. 1998a). The outerportion of anterior capsule stains for collagen type IV and V, and the inner portion forcollagen type IV (Saika et al. 1998a).
The normal adult lens is 65% water. In this relatively dehydrated state, the lens has arefractive index different from either aqueous or the vitreous. A concentration gradient ofions between the inside of the lens and the aqueous has been demonstrated. It ismaintained with active potassium-pump mechanisms located primarily in the membraneof the lens epithelial cells. This mechanism actively pumps potassium into the cells and

20
sodium outward. Glucose from aqueous is the primary substrate providing energy to thepump mechanism and for cell growth inside the lens (Olson 1989). A cataract is anyopacity of the lens.
2.1.2 Cataract surgery with intraocular lens implantation
2.1.2.1 History of intraocular lens implantation surgery
Sir Harold Ridley implanted the first IOL on November 29, 1949, in a 42-year-oldwoman, after removing the cataract by extracapsular cataract extraction (ECCE) threemonths earlier. The IOL was made of Plexiglass (PMMA) and it was biconvex (Rosen1997). The Plexiglass material was chosen because Ridley noted that pilots whose eyeswere injured by fragments of shattered Plexiglas had an insignificant tissue reaction to thematerial. ECCE requires a sclerocorneal wound of 110-180 degrees and sutures. CharlesKelman introduced phacoemulsification to cataract surgery (Kelman 1967). Thistechnique made it possible to remove lens material and to implant a foldable IOL througha 3.0 mm incision. This, in turn, opened the field to new IOL materials that could befolded and inserted through a smaller incision, and started the search for a materialassociated with less PCO than PMMA.
2.1.2.2 Effects of cataract surgery on the blood aqueous barrier
Cataract surgery and IOL implantation causes breakdown of the blood-aqueous barrier(BAB). Clinically this disruption can be detected by aqueous flare, which indicates theextent of protein leakage into the anterior chamber. The degree of BAB breakdown andchanges over time can be quantitatively measured in the anterior chamber by laser flare-cell photometry (Sawa et al. 1988, Ohara et al. 1989, Yoshitomi et al. 1990, Shah et al.1991, El-Maghraby et al. 1993). The relationship of events causing BAB breakdown afterIOL implantation, according to Nishi�s hypothesis, is shown in Figure 1, modified byMiyake (Miyake 1996a, Nishi 1996a). Surgical trauma, the IOL as a foreign body andinflammatory mediators synthesized by lens epithelial cells (LECs) are the components ofNishi�s hypothesis.

21
Fig.
1. N
ishi
�s h
ypot
hesis
, mod
ified
by
Miy
ake:
The
rel
atio
nshi
p be
twee
n L
EC
s and
pse
udop
haki
c in
flam
mat
ion
(Miy
ake
1996
a).

22
The size of the wound affects the degree of the BAB breakdown. Oshika et al. (1992)found significant differences in the laser flare-cell counts between ECCE with a PMMAIOL (11 mm incision group), phacoemulsification with a PMMA IOL (7 mm incisiongroup), and phacoemulsification with foldable silicone single-piece IOL implantation (4mm incision group). A significant difference in flare and cell counts was seen at days 1and 2 between 11 mm and 7 mm groups, and at days 1, 2 and one week between 11 and 4mm incision groups (Oshika et al. 1992). Pande et al. (1996a) confirmed these results.They had an ECCE group with a 7.0 mm optic diameter PMMA IOL, and aphacoemulsification group with continuous curvilinear capsulorhexis and 5.0x6.0 mmoptic diameter PMMA IOL. A significant difference in the mean flare measurement wasseen at day 1, one week and one month postoperatively between these groups (Pande etal. 1996a). Chee et al. (1999) saw significantly higher flare values in eyes operated withECCE using 9.0 to 10 mm limbal incisions than in eyes operated withphacoemulsification and a 6.0 mm sclerocorneal tunnel incision. Significant differenceswere seen at days 4, 15, 30 and 60. Flare levels in the ECCE group returned topreoperative values by the second month; the phacoemulsification group achievedpreoperative levels by 1 month. The IOL in both groups was a 6.0 mm PMMA IOL (Cheeet al. 1999).
Wound location also affects the degree of the BAB breakdown. Dick et al. (2000)found significantly lower postoperative flare values in eyes operated with a clear cornealincision compared with a sclerocorneal tunnel incision. Both incisions were 3.2 mm wide,and the implanted silicone IOL was of the same type. This significant difference wasfound at 6 hours, and at days 1, 2 and 3 after the operation. After 5 months, nostatistically significant difference was found (Dick et al. 2000). Vascular (limbal)incisions in cataract operations were shown to heal faster than clear corneal incisions infeline eyes (Ernest et al. 1998). Histological analyses confirmed that starting incisions inthe vascular region (limbus) resulted in a fibroblastic response that enhanced incisionstability and allowed rapid incision healing within 7 days postoperatively compared withthe 60 days healing time required for incisions started in the avascular region of thecornea (Ernest et al. 1998).
The location of the IOL in the eye also matters. Schalnus et al. (1995) studied thedifference in BAB breakdown after Nd: YAG capsulotomy when the IOL was situated insulcus or in the capsular bag. Aqueous laser flare was increased by 140 % in eyes withsulcus fixation and 95 % in eyes with capsular fixation of the IOL. Alio et al. (1997)evaluated the difference in laser flare-cell counts with ECCE and PMMA IOLimplantation when the IOL haptics were placed in sulcus, sulcus-bag or both haptics inthe bag. One day postoperatively, the cell count was significantly higher with sulcusimplantation, the difference in flare was not statistically significant. There were nosignificant between-group differences on day 2 and thereafter (Alio et al. 1997).
The intact capsulorhexis margin with continuous curvilinear capsulorhexis isassociated with less BAB breakdown than a capsulorhexis with a tear (Pande et al.1996b). In cataract operations with ECCE and PMMA IOL implantation, the tear grouphad significantly higher anterior chamber flare measurements, but only at day onepostoperatively. Anterior chamber cell measurements were higher in the tear group at 1day, 1 week, and 1 month, but not at 3 months (Pande et al. 1996b).

23
IOL material may have an effect on the breakdown of the BAB. Miyake et al. (1996b)concluded that lenses with hydrophobic surfaces induced greater postoperativeinflammation than lenses with more hydrophilic surfaces at 3 months postoperatively.This difference was seen between HSM-PMMA and PMMA IOLs but not between soft,hydrophobic acrylate IOLs and MemoryLens® IOLs. This is in contrast to theirconclusion of higher inflammation with hydrophobic IOLs. At 1 and 3 monthspostoperatively, laser flare-cell values were significantly higher in eyes with siliconeIOLs than in acrylate IOLs (Miyake et al. 1996b). Alio et al. (1996) did not findsignificant differences in laser flare-cell meter values in ECCE operated eyes betweenPMMA, HSM-PMMA, Ioptex surface passivated PMMA, silicone, polyHEMA Iogel®IOLs or with eyes left without an IOL. Mester et al. (1998) confirmed the significantlyhigher laser flare-cell values at 6 weeks and 3 months postoperatively with PMMA IOLswhen compared to HSM-PMMA IOLs in high-risk patients (e.g., diabetes mellitus,glaucoma, pseudoexfoliation and uveitis). Schauersberger et al. (1999) compared thelaser flare-cell values between 4 different foldable IOLs, and could not find any clinicallyrelevant differences in the course of postoperative inflammation. Two of the IOLs werehydrophobic (silicone and acrylate) and two hydrophilic (hydrogel and polyHEMA). Theonly difference was that acrylate IOLs on the first postoperative day had significantlyhigher flare values than silicone and polyHEMA IOLs (Schauersberger et al. 1999).
The disruption of the BAB after cataract surgery with IOL implantation may bemediated by prostaglandin E2 and various cytokines, such as interleukin-1 andinterleukin-6 (Nishi et al. 1996a and 1996b) (Fig. 1). Nishi et al. (1996a and 1996b) haveshown with cell culture that LECs are capable of producing these mediators.Prostaglandin E2 synthesis by LECs was lower when LECs were cultured on HSM-PMMA IOLs than on PMMA IOLs (Nishi et al. 1996a and 1996b). Still, PCO was notdecreased in a rabbit study, although prostaglandin E2 synthesis was inhibited with anindomethacin containing polylactic acid carrier disk implanted during the operation(Nishi 1996c). Aqueous flare values were significantly lower in the indomethacin groupthan control group at days 2, 3 and 4, and at weeks 1, 2, and 3 (Nishi 1996c).
2.1.2.3 Cell reactions on the anterior surface of intraocular lenses
Cells from the blood after breakdown of the BAB, lens epithelial cells from the lenscapsule, and melanocytes from the iris can be found on the IOL surface after cataractsurgery. In vivo these cells can be studied by specular microscopy (Wenzel et al. 1988,Okada et al. 1991 and Spalton et al. 1993). Wolter has described the cytopathology of thecells on explanted IOLs. First monocytes leave the blood vessels and become larger,develop short cytoplasmic processes, and are so transformed to macrophages. Thesemacrophages on the IOL surfaces can become fibroblast like cells and produce opticallyclear membranes composed of fibroblasts and a film of proteinaceous material.Macrophages can also form multinucleated giant cells on the IOL surface (Wolter 1982,1983a, 1983b, 1983c, 1983d, 1985). Mouse macrophages were shown to produce thiskind of membrane in 96 hours in tissue culture (Wolter 1883c and 1983d). Ishibashi et al.(1989) used a transmission electron microscope to study PMMA IOLs implanted in

24
monkey eyes and found similar, thin membrane-like structure covering the IOL surfacetogether with polymorphonuclear leukocytes, macrophages and multinucleated giantcells. Macrophages and giant cells on IOL surfaces have been shown to be capable ofproducing fibronectin (Kanagawa et al. 1990 and Saika et al. 1993). LECs also grow ontothe anterior surface of IOLs from the capsulorhexis margin (Ibaraki et al. 1995). Theyfound LEC membrane growth on PMMA IOLs most prominent on day 7 postoperatively;no membranes were observed after 4 weeks. The growth of LECs from the capsulorhexismargin onto the IOL surface varies with different IOL materials (Ibaraki et al. 1995).Hollick et al. (1999a) found most prominent LEC growth with hydrogel IOLs, with noregression of growth when compared to PMMA and silicone IOLs. Immunohistochemicalevaluation of cells on the IOL surface can be used to differentiate the origin of the cells.Saika et al. (1998a) showed that some of the cells on the IOL surface were LECs,because they stained positive for αB crystalline (a lens protein produced by LECs), andsome of the cells were macrophages because they stained positive to CD68 antigen, amacrophage marker.
The IOL material has an effect to the amount of cells attached to the IOL surface.Fewer cells were attached to HSM-PMMA than to PMMA IOLs (Larsson et al. 1989,Ygge et al. 1990, Miyake & Maekubo 1991a). When one-half of a PMMA IOL wascoated with poly dimethyl siloxane, fewer cells were attached on the silicone surface thanto the PMMA surface (Okada et al. 1993). In contrast, more small cells were seenattached to silicone IOLs than to PMMA and acrylate IOLs, and significantly fewer giantcells were seen on acrylate IOLs than on PMMA and silicone IOLs (Hollick et al. 1998).LECs cultured on human anterior capsules reacted differently when put in contact withacrylate, silicone or PMMA IOLs (Majima 1998). LECs were seen to attach to the opticand proliferate when in contact with acrylate IOLs. LECs did not show anymorphological changes when in contact with PMMA and silicone IOLs (Majima 1998).
2.1.3 Definition and origin of posterior capsule opacification
In extracapsular cataract surgery the lens capsule is opened and the lens epithelial cellsand lens fibers are evacuated. The intraocular lens is implanted in the capsular bag. Themost common cause of posterior capsule opacification (PCO) is proliferation andmigration of retained lens epithelial cells and their derivatives into the visual axis.According to Apple & Rabb (1998) the cells causing PCO are: (1) epithelium present onthe anterior capsule and in the equatorial lens bow, and epithelial cells that migrateposteriorly, (2) retained cortical fibers (elongated lens epithelial cells), (3) bladder cells(Wedl cells, the histopathologic correlate of clinical Hirschberg-Elshnig pearls), (4)fibrocyte-like cells derived from metaplasia of lens epithelial cells (pseudofibrousmetaplasia), and (5) myoepithelial cells (contractile smooth muscle-containing cellsderived from transformed lens epithelial cells). The LECs proliferating between the IOLand the posterior capsule cannot survive indefinitely; destroyed intracellular organellesand debris from degenerated LECs were seen in human and rabbit eyes (Saika et al.1998b).

25
Clinically, posterior capsule opacification is associated with declining visual acuityand other visual disturbances such as halos, after successful cataract surgery. Often thenear vision is affected first.
2.1.4 Methods to evaluate posterior capsule opacification
Clinically, PCO can be evaluated by a decrease of visual acuity compared to the firstpost-operative best-corrected visual acuity. Often Nd: YAG-laser capsulotomy isperformed if the visual acuity declines significantly, or if reading becomes difficult aftercataract surgery.
For other objective evaluations of the amount of PCO, different methods have beendeveloped. High-resolution digital retroillumination imaging is a system that uses coaxialillumination and imaging based on Zeiss® components with a digital camera directlylinked to a computer for online image verification and image analysis. The systemproduces high-resolution digital images with even background illumination of sufficientquality to demonstrate progressive lens epithelial cell changes that are amenable tocomputer image analysis. These images are objective documentation of PCO and allowquantitative measurements (Pande et al. 1997). The EPCO (Evaluation of PosteriorCapsule Opacification) image analysis system developed in Heidelberg usesretroillumination color photographs taken with a Zeiss® photoslit-lamp (model 40 SL/P)to score PCO. The individual PCO score is calculated by multiplying the density of theopacification, graded from 0 to 4 (0= none, 1 = minimal, 2 = mild, 3 = moderate, 4 =severe), by the area of the posterior optic involved, calculated between 0 and 1 (Tetz et al.1996a and 1997). Both systems evaluate a larger area of the posterior capsule than doesvisual acuity testing, and therefore are better tests for PCO formation with various IOLtypes and materials.
Hayashi K et al. (1998a) and Hayashi H et al. (1998) introduced a method for in vivoquantitative measurement of PCO using the Scheimpflug photography system called theAnterior Eye Segment Analysis System (EAS-1000; Nidek, Gamagori, Japan). Thecentral 3-mm portion of the posterior capsule is quantitated by means of areadensitometry. Scheimpflug slit images of the implanted IOL are taken at 0º, 45º, 90º, 135ºmeridians after full dilatation. The highest quality image of each meridian is selected andthen transferred to an online computer. The axial densitometry of the computer is used tocalculate the scatter light density of the central 3-mm area of the posterior capsule and theIOL of the same-size area. The density value is expressed in computer-compatible tapesteps (CCT). The density value of one section is determined by subtracting the scatterlight density in the IOL from the measured value of the posterior capsule. The averageddensity values of the 4 meridians are considered to be the PCO value. (Hayashi K et al.1998a, Hayashi H et al. 1998).

26
2.1.5 Amount of posterior capsule opacification with different intraocular lens materials
First of all, implantation of an IOL following cataract surgery decreases the incidence ofPCO (Nishi 1986). In highly myopic eyes, the incidences of PCO and retinal detachmentwere higher if the eye was left without an IOL (Badr et al. 1995). The best place for theIOL and its haptics is in the capsular bag after continuous curvilinear capsulorhexis(CCC) and phacoemulsification (Gimbel & Neuhann 1990). Significantly more IOLdecentration was found with asymmetrical bag-sulcus fixation or if the capsulorhexis wastorn (Legler et al. 1992 and Assia et al. 1993). Asymmetrical fixation also provides apathway for LEC proliferation behind the IOL optic. A CCC opening smaller than theIOL optic has resulted in less PCO with PMMA and polyHEMA IOLs (Ravalico et al.1996) and with soft, hydrophobic acrylate IOLs (Akahoshi 1999).
The amount of PCO increases with time after the cataract operation. Studies should beevaluated and compared against this time frame, and every study should also have an endpoint, when all the patients are examined. Sundelin et al. (1999) could find a hiddenpopulation of 9% of the operated population who were in need for Nd: YAG capsulotomybecause of PCO. Clinically significant PCO was seen in 14 % of patients who had not yethad capsulotomy. Table 1 collects Nd: YAG capsulotomy data from different studies withdifferent IOLs, with a follow-up of at least one year and in most cases a study group of atleast 50 operated eyes. The frequency of capsulotomies for PMMA IOLs has beenbetween 9-50 % (Condon et al. 1995, Winther-Nielsen et al. 1998, Pötzsch & Pötzsch1996, Khan & Percival 1999, Hayashi et al. 1998, Olson & Crandall 1998, Hollick et al.1999b, Erie et al. 1998, Oner et al. 2000), for HSM-PMMA 4-67 % (Amon & Menapace1993, Condon et al. 1995, Winther-Nielsen et al. 1998), for silicone plate haptic IOLs2.3-30.2% (Cumming 1993, Zehetmayer et al. 1994, Mamalis et al. 1996), for 3-piecesilicone IOLs 5.7-40.6% (Cumming 1993, Mamalis et al. 1996, Milazzo et al. 1996,Hayashi et al. 1998, Linnola & Holst 1998, Olson & Crandall 1998, Hollick et al. 1999b),for 2-hydroxyethyl methacrylate (HEMA) or poly (hydroxyethyl methacrylate (P-HEMA)) containing IOLs 9.5-22.2 % (Pötzsch & Pötzsch 1996, Khan & Percival 1999,Piovella et al. 2000), for hydrogel IOLs (combination of HEMA and HOHEXMA)(Bausch & Lomb Hydroview�) 17-17.3 % (Johnson 2000, Morris 2000), for soft,hydrophobic acrylate IOLs (Alcon AcrySof®) 0-14.3 % (Oshika et al. 1996, Hayashi etal. 1998, Hollick et al. 1999b, Akahoshi 1999, Auffarth 2000, Oner et al. 2000, Perez2000), and for soft hydrophobic acrylate (AMO Sensar®) 8-8.5 % (Perez 2000, Tjia2000). The follow-up time for a HEMA-based co-polymer with porcine collagen (StaarCollamer®) IOL was only 6 months with 4.7 % of eyes having an Nd: YAG capsulotomy(Brown et al. 1998). The number of operated eyes in many of the above-mentionedstudies has been low with the exception of the study presented by Akahoshi in 1999.

Table 1. Com
parison of Nd: YAG
capsulotomies w
ith different IOL m
aterials. Data of N
d: YAG capsulotom
ies in different studies with
different IOL m
aterials with a follow-up of at least one year.
InvestigatorIO
LM
aterialLoop M
aterialH
ydrophobicH
ydrophilicN
o: of operated
ECC
E or Phaco
follow-up
Months
Nd: YA
G %
Condon et al. (1995)
Pharmacia 720A
PMM
APM
MA
hydrophobic121
ECC
E12
9W
inther-Nielsen et al. (1998)
Pharmacia 725b
PMM
APM
MA
hydrophobic60
ECC
E36
43W
inther-Nielsen et al (1998)
Pharmacia 700b
PMM
APM
MA
hydrophobic62
ECC
E36
43.5Pötzsch et al. (1996)
OR
C U
V381K
2PM
MA
polypropylenehydrophobic
36phaco
4838.9
Hayashi et al. (1998)
Alcon M
Z60BD
PMM
APM
MA
hydrophobic69
phaco24
30.4O
lson et al. (1998)*
PMM
APM
MA
hydrophobic59
phaco36
33K
han et al. (1999)C
ilco JF1LRU
PMM
APM
MA
hydrophobic40
ECC
E144
50H
ollick et al. (1999)A
lcon MC
60BM
PMM
APM
MA
hydrophobic23
ECC
E36
26Erie et al. (1998)
Pharmacia 720/Storz
650 CU
VPM
MA
PMM
Ahydrophobic
198phaco
4126.5
Erie et al. (1998)Pharm
acia 805/Storz 359PM
MA
PMM
Ahydrophobic
171phaco
4123.5
Oner et al. (2000)
Opsia-A
gena 550PM
MA
PMM
Ahydrophobic
77phaco
17.8+1.726.3
Am
on et al. (1993)Pharm
acia 725CH
SM-PM
MA
PMM
Ahydrophilic
50phaco
16+410
Condon et al. (1995)
Pharmacia 720C
HSM
-PMM
APM
MA
hydrophilic118
ECC
E12
4W
inther-Nielsen et al. (1998)
Pharmacia H
SM-725b
HSM
-PMM
APM
MA
hydrophilic70
ECC
E36
44W
inther-Nielsen et al.(1998)
Pharmacia H
SM-700b
HSM
-PMM
APM
MA
hydrophilic58
ECC
E36
67
Cum
ming (1993)
*silicone
plate haptichydrophobic
503phaco
302.3
Cum
ming (1993)
*silicone
polypropylenehydrophobic
253phaco
127.1
Zehetmayer et al. (1994)
Staar AA
-4203silicone
plate haptichydrophobic
54phaco
56+ 8.913
Mam
alis et al. (1996)Staar A
A-4203
siliconeplate haptic
hydrophobic139
phaco21
30.2M
amalis et al. (1996)
AM
O SI18N
B/SI30N
Bsilicone
polypropylenehydrophobic
349phaco
23.339.1
Milazzo et al. (1996)
AM
O SI18/19/20N
Bsilicone
polypropylenehydrophobic
86phaco
5740.6
Hayashi et al. (1998)
AM
O SI30N
Bsilicone
polypropelenehydrophobic
70phaco
245.7
Linnola et al. (1998)Pharm
acia CeeO
n 920silicone
PMM
Ahydrophobic
45phaco
1211
Olson et al. (1998)
AM
O SI30N
Bsilicone
polypropelenehydrophobic
60phaco
3624
27

Hollick et al. (1999)
Iolab LI41Usilicone
PMM
Ahydrophobic
22EC
CE
3614
Pötzsch et al. (1996)O
RC
Mem
oryLens**
polypropylenehydrophilic
36phaco
4822.2
Piovella et al. (2000)M
emoryLens
**polypropylene
hydrophilic673
phaco7 years³
9.5K
han et al. (1999)Iogel PC
12P-H
EMA
¹single piece
hydrophilic35
ECC
E144
20Johnson (2000)
Storz Hydroview
hydrogelhydrogel
hydrophilic75
phaco>12
17.3M
orris (2000)Storz H
ydroviewhydrogel
hydrogelhydrophilic
963phaco
>1217
Oshika et al. (1996)
Alcon A
crySof MA
60BM
acrylatePM
MA
hydrophobic64
ECC
E24
11.1H
ayashi et al. (1998)A
lconAcrySof M
A60B
Macrylate
PMM
Ahydrophobic
73phaco
242.7
Hollick et al. (1999)
Alcon A
crySof MA
60BM
acrylatePM
MA
hydrophobic19
ECC
E36
0A
kahoshi (1999)A
lcon AcrySof M
A30B
A/
MA
60BM
acrylatePM
MA
hydrophobic10000
phaco51
0.75
Oner et al. (2000)
Alcon A
crySof MA
30BA
acrylatePM
MA
hydrophobic80
phaco17.8+1.7
14.3 4
Perez (2000)A
lcon AcrySof M
A30B
Aacrylate
PMM
Ahydrophobic
100phaco
180
Auffart (2000)
Alcon A
crySofacrylate
PMM
Ahydrophobic
53phaco
360
Perez (2000)A
mo Sensar A
R40
acrylatePM
MA
hydrophobic100
phaco18
8Tjia (2000)
Am
o Sensar AR
40acrylate
PMM
Ahydrophobic
100phaco
158.5
Brow
n et al. (1998)Staar C
ollamer
HEM
A-porcine
Collagen 2
plate-haptichydrophilic
125phaco
6 54.7
AM
O= A
llergan Medical O
ptics. OR
C = O
ptical Radiation C
orp. * = data not available. ** = co-polymer of m
ethyl methacrylate, 2-hydroxyethyl m
ethacrylate (HEM
A),
and 4-methacryloxy 2-hydroxy-benzo-phenone. 1 = P-H
EMA
= poly (hydroxylethyl methacrylate). 2 = H
EMA
-based co-polymer in w
hich porcine collagen and ultravio-let-absorbing chrom
ophore is bonded. 3 = longest follow-up 7 years, m
ean follow-up tim
e not known. 4 = The only eye w
ith severe PCO
in this group was also unusual in
that it had a central firm fibrotic plaque on the posterior capsule w
hich was observed prior to im
plantation; Nd: YA
G capsulotom
y was perform
ed 4 months postopera-
tively (Oner et al. 2000). 5 = follow
-up only 6 months, because this is the only available data for this IO
L material.
InvestigatorIO
LM
aterialLoop M
aterialH
ydrophobicH
ydrophilicN
o: of operated
ECC
E or Phaco
follow-up
Months
Nd: YA
G %
28

29
More information on the amount of PCO with different IOLs can be found when PCOis assessed objectively by digital retroillumination imaging using dedicated software andwhere PCO is calculated as the percentage area of opacified capsule. With this methodHollick et al. (1999b) found significant differences (P=0.0001) in percentage of PCOafter 3 years between acrylate (PCO 10%), silicone (PCO 40%), and PMMA IOLs (PCO56%). EPCO analysis also resulted in a significant difference (P<0.001) between PMMAand acrylate IOLs (Auffarth 2000). In his study, with 53 patients in each group, theaverage total PCO index for acrylic IOLs was 0.15+ 0.27 and for PMMA 1.03+0.62. Nocapsulotomies were performed for acrylic IOL implanted eyes during the follow-up of 3years (Auffarth 2000).
2.1.6 Extracellular matrix proteins associated with posterior capsule opacification
Extracellular matrix (ECM) contains three major classes of biomolecules (Murray &Keeley 1996): (1) the structural proteins, collagen, elastin, and fibrillin; (2) certainspecialized proteins, such as fibronectin, vitronectin and laminin, which have specificfunctions in the extracellular matrix; and (3) proteoglycans, which consist of long chainsof repeating disaccarides (glycosaminoglycans)(GAGs), attached to specific coreproteins.
The following extracellular matrix proteins have been found attached to the IOL or inthe fibrocellular tissue responsible for the posterior capsule opacification after cataractsurgery: fibronectin (Kappelhof et al. 1986, Kanagawa et al. 1990, Boyd et al. 1992,Kochounian et al. 1994), cellular fibronectin (Saika et al. 1993, Saika et al. 1995, Saika etal. 1997a, Saika et al. 1997b, Saika et al. 1998c), vitronectin (Saika et al. 1995), laminin(Saika et al. 1998c), hyaluronan (Saika et al. 1998d), collagen (Ishibashi et al. 1995),collagen type I (Saika et al. 1992, Ishibashi et al. 1994, Saika et al. 1995, Saika et al.1997a, Saika et al. 1997b, Saika et al. 1998c), collagen type III (Ishibashi et al. 1994,Saika et al. 1995, Saika et al. 1997a, Saika et al. 1997b, Saika et al. 1998c), collagen typeIV (Ishibashi et al. 1994, Saika et al. 1998c), and collagen type V and VI (Saika et al.1998c).
Fibronectin is a major glycoprotein of the extracellular matrix, and it is also found insoluble form in plasma. In general, of all the non-collagenous extracellular matrixproteins, fibronectin is found in places where firm binding is needed, for examplebetween the collagen fibers of a tendon and bone and at myotendinous junctions (Kannuset al. 1998). Normal values for plasma fibronectin are 250-400 µg / ml (Diacor ClinicalLaboratory Examinations 1991). The concentration of soluble fibronectin in aqueoushumor in human eyes with a cataract was 0.136+ 0.192 µg / ml (Kim et al. 1992), and0.064 µg / ml (range 0.000-0.202) (Vesaluoma et al. 1998). The measurements were madeprior the cataract operation. Soluble fibronectin is produced in liver parenchymal cells;cellular fibronectin is produced and secreted by many other types of cells locally, forexample macrophages (Alitalo et al. 1980). It is also produced by lens epithelial cells,which are transformed into fibroblasts (Saika et al. 1995). The difference between solubleand cellular fibronectin is in their structures. Soluble fibronectin has region V that cellular

30
fibronectin does not have, and only cellular fibronectin has region EIII (Paul et al. 1986).Murray and Keeley (1996) have described the structure and functions of fibronectin asfollows: �Fibronectin consists of two identical subunits, each of about 230 kDa, joined bytwo disulfide bridges near their carboxyl terminals. Fibronectin contains three types ofrepeating motifs (I, II, and III), which are organized into functional domains (at leastseven): functions of these domains include binding heparin and fibrin, collagen, DNA,and cell surfaces. The amino acid sequence of the fibronectin receptor in fibroblasts hasbeen derived, and the protein is a member of the transmembrane integrin glass ofproteins.
The integrins are heterodimers, containing various types of α and β polypeptidechains. Fibronectin contains an Arg-Gly-Asp (RGD) sequence that binds to the receptor.The RGD sequence is shared by a number of other proteins present in the extracellularmatrix that bind to integrins present in the cell surface. By binding to the cell membraneintegrin receptor, fibronectin interacts indirectly with actin microfilaments present in thecell cytosol. These proteins inside the cell are known as attachment proteins and includetalin, vinculin, an actin-filament capping protein, and α - actinin. With this mechanismfibronectin can affect cell behavior in cell adhesion and cell migration�.
The growth and migration of LECs can be rapid. A confluent monolayer of LECs overthe posterior capsule was seen after 5.8 + 0.6 days vs. 7.2 + 0.7 days for capsules aged<40 years and >60 years, respectively (Liu et al. 1996). This was an in vitro study withhuman autopsy eyes after a sham cataract operation. Olivero & Furcht (1993) found thatfibronectin, laminin and collagen type IV promoted LEC adhesion and migration in arabbit LEC culture. Collagen type IV promoted maximal in vitro adhesion of rabbit LECsat lower concentrations in comparison to fibronectin and laminin. Fibronectin promotedmaximal in vitro migration of rabbit LECs at lower concentrations in comparison tocollagen type IV and laminin (Olivero & Furcht 1993). Nishi et al. (1997a) studied celladhesion molecules (CAMs) in human LECs. β1 integrin, intercellular adhesionmolecule-1 (ICAM-1), and hyaluronan receptor CD44 were found directly after surgeryin LECs obtained with a piece of the anterior capsule. These CAMs could also be foundafter two-weeks of culture time. When monoclonal antibodies were added to the cultureto block these CAMs, LEC proliferation was inhibited (Nishi et al. 1997a). Theexpression of CD44 in human LECs was confirmed in another study (Saika et al. 1998d).Versura et al. (1999) studied the adhesion mechanisms of LECs cultured on PMMA,HSM-PMMA, polyHEMA and silicone IOLs. When they measured the intracellularadhesion molecules actin, vinculin, and talin by immunocytochemical analysis, thesemolecules were found only on LECs cultured over PMMA IOLs (Versura et al. 1999).
Vitronectin is another major glycoprotein involved in cell adhesion. It has the ability toattach to collagen I, II, III, IV and V. There is vitronectin in blood, and probably mostvitronectin is produced in the liver (Seiffert 1997a, Seiffert & Smith 1997b, Yoneda et al.1998). The circulating form of vitronectin is inactive, but in an area of tissue injury it istransformed into an active adhesive glycoprotein (Seiffert & Smith 1997b). Vitronectin isalso produced by human monocytes and macrophages (Hetland et al. 1989).
Laminin (about 850kDa) consists of three distinct elongated polypeptide chains (A,B1, and B2). The laminin molecule has an asymmetric crosslike structure with three shortarms and one long arm. It has binding sites for type IV collagen, heparin, and integrins onthe cell surface (Murray & Keeley 1996). Burgeson et al. (1994) presented a new,

31
systematic nomenclature for laminins. They are named from laminin-1 to laminin-11according to their α-, β-, and γ-chain compositions. There are α-chains from α1 to α5, β-chains β-1 and β-2, and γ-chains γ-1 and γ-2. Laminin promotes cell attachment,spreading, motility, neurite outgrowth, as well as cell proliferation and differentiation(Engvall et al. 1990). Laminin and collagen type IV seem to reappear later thanfibronectin, during the biological healing processes. When laminin with corneal basementmembrane (CBS) was removed by superficial keratectomy in a rabbit study, it wasrestored in the CBS 2-4 weeks afterwards, together with focal bands of collagen type IV(Fujikawa et al. 1984). Fibronectin was found much earlier, after only 8 hours (Fujikawaet al. 1984).
Hyaluronan (hyaluronic acid: sodium hyaluronate) is a glycosaminoglycan composedof glucuronic acid and N-acetylglucosamine (Saika et al. 1998c). It binds to cell surfacemolecules, and cell adhesion molecule CD44 (Saika et al. 1998c). Cell adhesion moleculeCD44 has been found in LECs removed with a piece of anterior capsule (Nishi et al.1997a), and its presence has been shown in posterior capsules removed together with theIOL (Saika et al. 1998c). The presence of CD 44 molecules does not mean that the tissuecontains hyaluronan; CD44 binds also to several collagens and fibronectin (Nishi et al.1997a).
Collagen is the major component of connective tissue and it provides an extracellularframework for tissues. According to Murray & Keeler (1996), the synthesis of collagen isas follows: �Preprocollagen is synthesized on ribosomes in the cell. As it enters theendoplasmic reticulum, its leader sequence is enzymatically removed and procollagen isformed. Now follows hydroxylation of proline and lysine residues, and glycosylation ofhydroxylysines. Three of these collagen molecules bond with interchain disulfide bondsand the triple helix is formed. Following secretion from the cell, extracellular enzymesremove the extension peptides at the amino and carboxyl terminal ends. Once thepropeptides are removed, the triple helical collagen molecules, containing approximately1000 amino acids per chain, spontaneously assemble into collagen fibers�. Of the 19collagen types collagen type I, III, IV, V and VI have been found associated with theextracellular matrix in fibrotic tissue of PCO. Collagen types I, II and V belong to fibrilforming, IV to network-like, and VI to beaded filaments class of collagens (Murray &Keeley 1996). Lens capsule is made mainly of collagen type IV (Saika et al. 1998c).After LECs are transformed into a myofibroblastic phenotype, they have been shown toexpress prolyl 4-hydroxylase and α -smooth muscle actin (Saika et al. 1998d and 1998e).Prolyl 4-hydroxylase is needed when collagen molecules are formed (Pihlajaniemi et al.1991).
Transforming growth factor-β (TGF-β) is a family of multifunctional cytokines, whichare in part responsible for regulation of collagen and other ECM component biosynthesis.The human TGF-β family consists of three isoforms: TGF-β1, TGF-β2, and TGF-β3.These isoforms showed quantitatively similar biological activity when tested in vitro(Graycar et al. 1989).
Fibronectin is shown to be available in aqueous humor before surgery (Kim et al.1992, Vesaluoma et al. 1998). Because plasma contains fibronectin and vitronectin, theyare available directly after cataract surgery, after the breakdown of BAB. After surgery,rapid protein adsorption begins on the IOL surface. Shigematsu (1991) found an ultrathinmembrane-like structure composed of fine, granular material, 0.01 to 0.08 µm thick,

32
which covered the entire explanted IOL surface regardless of the implant period (3 daysto 88 months) and kind of the IOL (PMMA, silicone, P-HEMA, coated PMMA) in humaneyes. The structure was determined to be a layer of adsorbed protein (Shigematsu 1991).In a rabbit study with implanted PMMA IOLs removed after 48 hours, the IOLs wereshown to have absorbed fibrinogen/fibrin, fibronectin, albumin, immunoglobulin G (IgG)and minor amounts of transferrin and complement C3 (Kochounian et al. 1994). In thesame study, incubation of PMMA IOLs in rabbit plasma for 3 hours was associated withmore albumin, transferrin and IgG attachment in relation to fibrin and fibronectinattached in vivo (Kochounian et al. 1994). Johnston et al. (1999) showed better surfaceadsorption of fibronectin to a hydrophobic soft acrylate IOL than to a PMMA IOL invitro, and they found this difference to be significant when measured after one day andone week. Saika et al. (2000) found cell deposits on 12 IOLs and proteinaceous depositson 16 of 32 PMMA IOLs explanted from Japanese patients.
2.2 Anterior capsule opacification and movement over the intraocular lens
Anterior capsule opacification (ACO) after cataract surgery and IOL implantation issimilar to posterior capsule opacification, including LEC proliferation and extracellularmatrix formation with collagen (Hara et al. 1992). In monkey eyes with IOLimplantation, proliferating LECs and extracellular matrix stained positively withcuprolinic acid (stains proteoglycans) (Ishibashi et al. 1993). LEC proliferation under andover the anterior capsule, together with extracellular matrix formation with PMMA IOLs,was seen in a rabbit study (Saika et al. 1997c). Tissue sections from human anteriorcapsule fibrosis contained dense fibrous tissue and numerous activated fibroblasts withcontractile capacity, because α-smooth muscle (α-SM) actin was found in the cellcytoplasm (Caporossi et al. 1998). The origin of fibroblasts (myofibroblasts) was thoughtto be transformed LECs. No inflammatory cells or TGF-β were found in the fibrocellulartissue (Caporossi et al. 1998). Significantly less ACO was found with soft, hydrophobicacrylate IOLs in human pseudophakic autopsy eyes when compared with PMMA anddifferent silicone plate haptic and 3-piece silicone IOLs (Werner et al. 2000). The highestACO rate was found with plate haptic silicone IOLs; ACO scores were calculated as thethickness of cell and fibrocellular tissue proliferation between the anterior capsule andIOL (Werner et al. 2000).
The contraction of CCC openings over the IOL anterior face is different with differentIOL materials. Significantly less movement was seen with soft, hydrophobic acrylateIOLs than with PMMA and silicone IOLs; PMMA IOLs had less movement than siliconeIOLs (Ursell et al. 1997, Cochener et al. 1999). Hayashi et al. (1997) found similarchanges but no significant difference between the same IOL materials. The hapticmaterial [polypropylene versus poly (methyl methacrylate)] with two otherwise similarsilicone IOLs did not have an effect on the amount of anterior capsule contraction(Gallagher & Pavilack 1999). Anterior capsule contraction requiring Nd: YAG anteriorcapsulotomy has been reported in normal eyes with silicone IOLs, and the risk for

33
contraction was greater in eyes with pseudoexfoliation syndrome (Toldos et al. 1996 andDahlhauser et al. 1998). Retinitis pigmentosa was a risk factor for anterior capsulecontraction with PMMA IOLs (Hayashi et al. 1998b).
2.3 Methods for preventing posterior capsule opacification
2.3.1 Design of the intraocular lens
During the time when only PMMA IOLs were available, studies were done to assess theeffect of different optic designs on PCO. The optic had a convex or plano side against theposterior capsule, or the IOL had a bi-convex design. Less PCO was found when the IOLwas placed convex side against the posterior capsule (Sterling & Wood 1986, Snellman &Lindstrom 1988, Born & Ryan 1990). The type of PCO also was different; Elschnig pearlproliferation was seen more with IOLs placed plano side against the posterior capsule,and fibrosis when the convex side was posterior (Sterling & Wood 1986, Snellman &Lindstrom 1988). Laser ridge IOLs had a ridge on the optic, which was against theposterior capsule. It was a lens that purposely held the posterior capsule away from thelens optic. Maltzman et al. (1989) found a beneficial effect in reducing PCO with laserridge IOLs, but a longer follow-up study with a larger number of patients found plano-convex /biconvex IOLs to have been associated with fewer capsulotomies than laser ridgeIOLs (capsulotomy rate 6.5% versus 40% at five years) (Born & Ryan 1990).
The position of the IOL haptics can also have an effect on PCO. PMMA IOLs with theconvex surface posterior, together with angled haptics, produced less PCO than uniplanarPMMA IOLs (Downing 1986). Mamalis et al. (1995) found less PCO requiring Nd: YAGcapsulotomies in a PMMA IOL group with an overall lens diameter less than 13.5 mm,than in a PMMA IOL group with an overall diameter of 13.5 mm or larger.
During the period of modern continuous curvilinear capsulorhexis withphacoemulsification, the plano-convex PMMA IOLs succeeded better than bi-convexPMMA IOLs. The Nd: YAG rates were 5.9% versus 32.5%, respectively (Yamada et al.1995).
With foldable lenses the model of the IOL can also be a one-piece, plate haptic modelor a disc model. Cumming (1993) and Zehetmayer et al. (1994) found less PCO with aplate haptic silicone IOL than with 3-piece silicone IOLs. Mamalis et al. (1996) could notshow as beneficial an effect of plate haptic IOLs. A silicone disc model was implanted in35 eyes and associated with a PCO rate of 33% after 38 months (Duncker et al. 1995). Inan analysis of 100 explanted plate-haptic and 3-piece silicone lenses, decentration was themost common reason for explantation for both lens types (Auffarth et al. 1995). Still,when comparing the results to explanted PMMA IOLs, there was no difference (Auffarthet al. 1995). Plate haptic silicone, as well as plate haptic polymacon (polyHEMA) IOLshas been reported to luxate into the vitreous cavity after Nd: YAG laser capsulotomy(Levy et al. 1990, Lowe & Easty 1992, Schneiderman et. al. 1997, Dahlhauser et al.1998, Dick et al. 1998). To minimize this risk, silicone IOLs have been produced withlarger holes, or mini-haptics at the haptic end of the IOL. Larger holes or mini-haptics

34
were associated with better fixation within the capsular bag by allowing LECproliferation through the holes (Kent et al. 1997, Kent et al. 1998, Whiteside et al. 1998).
Nishi et al. (1998a) have shown the significant advantage of the square edge of soft,hydrophobic acrylate (AcrySof®) IOLs in reducing PCO. The acrylate IOL was the onlyone to show a sharp, square edge in scanning electron microscope evaluation; other 5IOLs made of PMMA and silicone had round and smooth edges. The histopathologicstudy of rabbit lens capsules 2, 3, and 4 weeks after implantation revealed, that PCO wassignificantly reduced in the eyes with the square edged acrylate IOL compared to theother, rounded edge IOLs (Nishi et al. 1998a). Oshika et al. (1998) found similarinhibition of LEC migration by the square edged acrylate IOL (AcrySof®) in a rabbitstudy. They also analyzed the adhesion force of the posterior capsule to the acrylate IOLoptic and found more adhesion with the acrylate IOL than with PMMA and siliconeIOLs. In another part of the study the adhesion force of these IOLs to a type I collagensheet was measured in vitro. The mean adhesive force was significantly higher withacrylate than with PMMA and silicone IOLs (Oshika et al. 1998). Nagata et al. (1998)reported similar results in their in vitro adhesion study. Nishi and Nishi (1999) alsoshowed that LEC migration was prevented with the square edge acrylate IOL and asquare edge model of a PMMA IOL. This was a study with four rabbits, with an acrylateIOL in one eye and PMMA IOL in the contralateral eye; the follow-up time was 3 weeks(Nishi & Nishi 1999).
Clinical evidence of the barrier effect with square edge IOLs has been found in a studywith human, pseudophakic autopsy eyes (Peng et al. 2000a). This study included 150eyes: three types (50 each) of posterior chamber IOLs, based on different optic materials:PMMA designs made by all major manufacturers; silicone IOLs made by Allergan, Staar,and Bausch & Lomb; a soft, hydrophobic acrylate IOL (Alcon AcrySof®). Acrylate IOLshad total fusion of the anterior and posterior capsules with no Soemmerring�s ring in 52%of cases. PMMA and silicone IOLs both had no Soemmerring�s ring in 10% of cases. Thesquare optic edge of acrylate IOLs blocked LEC growth in 25% of the cases; the roundedoptic edge could not hinder LEC growth for any of the silicone IOLs and blocked it inonly for 9% of PMMA IOLs (Peng et al. 2000a). Kruger et al. (2000) found a differencebetween round and square edge silicone IOLs (Pharmacia CeeOnTM 920 versusPharmacia CeeOnTM 911F). After two years there were no Nd: YAG capsulotomies in thesquare edge IOL group (0 of 22); and 8 % (2 of 23 patients) in the rounded edge group(Kruger et al. 2000). A better blocking effect was seen with soft, hydrophobic acrylateIOLs (Alcon AcrySof® MA60BM) than with a 3-piece silicone IOL with a square edge(Pharmacia CeeOnTM 911), but there were no apparent differences between them in PCOdevelopment in a rabbit study (Nishi et al. 2000).
2.3.2 Surface modification and coating of the intraocular lens
In general, the idea behind coating the IOL surface is to render it less attractive to cellattachment and cell growth. Tamada & Ikada (1994) found that fibroblasts couldproliferate at the highest rate, and showed normal in situ morphology, when cultured on asubstrate with a contact angle around 70°, which was also most favorable for cell

35
adhesion. They also found that collagen synthesis per cell was more active on surfacespoor for cell growth than on the good ones (Tamada & Ikada 1994). Contact angle isdependent on the IOL material and coating of the IOL surface. It is a measure of surfacetension, which in turn, defines the relative hydrophobicity of the IOL material. Surfacepassivation alters the PMMA IOL surface energy and makes it more hydrophobic, with acontact angle of 90° (Umezawa & Shimizu 1993 and Boulton et al. 1994). Heparin can becovalently bound to a PMMA IOL surface producing a heparin-surface-modified IOLwith a hydrophilic surface and a contact angle of 33° (Larsson et al. 1989, Ygge et al.1990, Miyake & Maekubo 1991a, Umezawa & Shimizu 1993, Boulton et al. 1994). Thecontact angles mentioned above have been measured with a sessile drop method. Anglesmeasured with the same method for three different silicone IOLs were 109.8°-116.7°, forPMMA 68.1°, for a hydrophobic, soft acrylate 87.6° (Allergan Medical Optics Sensar®AR40), and for hydrophobic, soft acrylate 72.7° (Alcon AcrySof® MA60BM) (Cunananet al. 1998). Different contact angles were found when lenses were measured in water(Cunanan et al. 1998). PMMA can also be coated with fluorine. Boulton et al. (1994) didnot find any difference in cell adhesion between surface passivated and normal PMMAIOLs, but significantly fewer cells attached to HSM-IOL surfaces. This differencebetween HSM-PMMA and PMMA IOLs has been shown in other studies (Larsson et al.1989, Ygge et al. 1990, Miyake & Maekubo 1991a). Although heparin on the IOLsurface decreases the amount of cell attachment, it has not been shown to make anydifference in the PCO these IOL materials induce in the eye (Winther-Nielsen et al.1998). Miyake (1990) suggested collagen as a coating material for IOLs, and tested IOLsmade of collagen type IV in rabbits (Miyake et al. 1991b). In order to make the surface ofa PMMA IOL less attractive for adhesion, it has been coated with annexin V (Chollet etal. 1996) and fluorocarbon (Werner et al. 1997). In rabbit studies both these materialswere associated with less adhesion to cells than PMMA (Chollet et al. 1996, Werner et al.1997). Latz et al. (2000) studied the effect of LEC growth on normal PMMA IOLs andsubstituted PMMA IOL surfaces. They found less cell growth and migration onsubstituted PMMA IOL surfaces. The modified polymer surface was thought to effectLEC growth by producing conformational changes in fibronectin molecules inhibitingtheir interaction with LECs (Latz et al. 2000).
2.3.3 Capsular bag tension ring
The use of a capsular bag tension ring to prevent PCO has been studied (Hara et al. 1995,Hashizoe et al. 1998, Nishi et al. 1998b). Hara et al. (1995) used a flexible silicone ring(outer diameter 11.0 mm; width 1.5 mm; and thickness 1.5 mm) in a rabbit study. Thering had square edges against the capsule and it was implanted after phacoemulsification.A 6.0 mm PMMA IOL was implanted after the ring. The follow-up time before histologicevaluation was 3.5 + 1.4 months. Two eyes that received only the IOL had severe PCO.In nine (90%) of the 10 eyes that were implanted with the rings, the circular contour ofthe equator was preserved, and seven (70%) of these eyes had transparent posteriorcapsules (Hara et al. 1995). The same ring was used in monkey eyes with a significantreduction of PCO (P=0.017) (Hashizoe et al. 1998). Nishi et al. (1998b) concluded that a

36
discontinuous bend in the capsule significantly inhibited LEC migration in rabbit eyes.The bend was created with a capsular tension ring with square edges or with an IOL withthe ring being continuous with it. The IOL and the ring were made of PMMA, and theshape of the ring was an open-circular loop 1.0 mm wide and 0.2 mm thick, with adiameter of 14 mm (Nishi et al. 1998b).
2.3.4 Posterior continuous curvilinear capsulorhexis
One way to hinder PCO is to do a posterior continuous capsulorhexis (PCCC) during theprimary cataract operation. Before PCCC was introduced, Kraff et al. (1984) studied theeffect of an intact posterior capsule. There were 136 patients who had ECCE orphacoemulsification, PMMA IOL implantation and wound suturing, and 152 patientswho had the same procedure but after suturing, a primary capsulotomy of 3-4 mm wasdone with a bent needle. Angiographically it was confirmed (183 of 288 patients) thatcystoid macular edema (CME) occurred significantly more often in the primarycapsulotomy group (20 of 93 patients) than in the intact capsule group (4 of 71 patients),for an incidence 21.5% vs. 5.6% (P=0.003) (Kraff et al. 1984). Zaczek et al. (1998) couldnot find a significant difference in CME between eyes with and without PCCC. They hadtwo groups of 25 patients with phacoemulsification and implantation of a silicone IOL.PCCC was performed in one group. There was also no significant difference in BABbreakdown as measured by laser flare meter, and the incidence of clinical CME was 4 %in the PCCC group compared to 8 % in the control group (Zaczek et al. 1998).
The situation is different with children. Gimbel (1996 and 1997), BenEzra & Cohen(1997) and Vasavada & Desai (1997) have all confirmed the advantage of primary PCCCand primary anterior vitrectomy in reducing postoperative PCO. The method of choicepresented by Gimbel (1997) is PCCC together with anterior vitrectomy and IOL opticcapture (IOL optic is placed through PCCC behind the posterior capsule).
2.3.5 Agents for inhibiting lens epithelial cell growth
Efforts to prevent posterior capsule opacification after cataract surgery have includedeliminating lens epithelial cells during the operation, or affecting the growth of these cellsafter the operation. Drugs used for these purposes can be applied during the operation. Along acting delivery system for these substances has also been tried by using poly-DL-lactid, a polymer of the monomeric lactid acid as a carrier substance, which slowlydelivered specific drugs (Tetz et al. 1996b). Three different groups of drugs have beentried. Antimetabolites are designed to kill the remaining LECs, immunotoxins are mostlyused for inhibiting the proliferation and migration, and anti-inflammatory drugs are usedto hinder inflammatory reactions after cataract surgery.

37
2.3.5.1 Antimetabolites
Many antimetabolites have been tried in an effort to hinder the proliferation of lensepithelial cells. Actinomycin D (Chan & Emery 1984), methotrexate (Chan & Emery1984, Hansen et al. 1987), daunomycin (Weller et al. 1988, McDonnell et al. 1988,Hartmann et al. 1989, Sourdille & Ducournau 1990, Power et al. 1994, Ruiz et al. 1990,Tetz et al. 1996b), 5-fluorouracil (McDonnell et al. 1988, Ruiz et al. 1990, Ismail et al.1996), colchicine (Chan & Emery 1984, McDonnell et al. 1988, Legler et al. 1993),doxorubicin (McDonnell et al. 1988), cytosine arabinoside (McDonnell et al. 1988), andmitomycin C (Ismail et al. 1996, Chung et al. 2000) have all been tested. Colchicine is analkaloid used to treat gout; it destroys proliferating cells by arresting mitosis. The otherpharmacological agents mentioned above are used in cancer therapy; they also inhibitrapidly dividing, mitotic cells. Methotrexate-anticollagen conjugate was seen to hinderLEC growth in cell culture. In in vivo rabbit eyes some of it was also found later incorneal tissue, suggesting the possibility of corneal damage (Hansen et al. 1987). In adose dependent manner, 5-fluorouracil, daunomycin, colchicine, doxorubicin andcytosine arabinoside all hindered LEC growth in cell culture (McDonnell et al. 1988).Colchicine was also effective in a rabbit study, but with dose related side effects such asretinal necrosis, corneal clouding and anterior chamber reaction (Legler et al. 1993). PCOwas reduced by 5-fluorouracil in a rabbit study, but a long application time of 10 minutesduring the operation was a disadvantage (Ruiz et al. 1990). 5-fluorouracil wassignificantly more effective than mitomycin C in a rabbit study (Ismail et al. 1996).Significant PCO reduction was found with sustained release of daunomycin in a rabbitstudy (Tetz et al. 1996b), together with mild inflammation at the limbus area and someendothelial cell loss. Daunomycin is the only one of all the antimetabolites, to reachclinical human studies for this purpose (Hartmann et al. 1989, Sourdille & Ducournau1990), but no further results of its use have been published.
2.3.5.2 Immunotoxins and lens epithelial cell adhesion molecules as blocking agents
Lens epithelial necrosis factor (LENF) (Hunold et al. 1991), antitransferrin receptorimmunotoxin (Goins et al. 1994), ethylenediaminetetra-acetic acid (Humphry et al. 1988,Nishi et al. 1996d), 4187X-ricin A immunoconjugate (Tarsio et al. 1997), lens epithelialcell adhesion molecule blocking agent (Nishi et al. 1997b), and immunotoxin MDX-RA(Clark et al. 1998) have been tried as inhibitors of PCO after cataract surgery and IOLimplantation.
LENF, antitransferrin receptor immunotoxin and 4187X-ricin A immunoconjugatecould all inhibit LEC growth in cell cultures (Hunold et al. 1991, Goins et al. 1994,Tarsio et al. 1997). Antitransferrin receptor immunotoxin consists of a monoclonalantibody of the IgG type directed against transferrin receptors, and it is chemically linkedto protein synthesis inhibiting ricin-A (Goins et al. 1994). The idea is to destroy rapidlydividing LECs, which have a higher density of transferrin receptors as do all rapidlydividing cells (Goins et al. 1994). 4187X-ricin A immunoconjugate reacts specifically

38
with an antigen on the human LEC membrane, and the ricin component inhibits proteinsynthesis (Tarsio et al. 1997). In cell culture, protein synthesis and LEC proliferation wasalmost completely inhibited (Tarsio et al. 1997).
In a rabbit study, ethylenediaminetetra-acetic acid significantly reduced PCO, and lensepithelial cell adhesion molecule blocking agent slightly inhibited LEC migration to theposterior capsule. Ethylenediaminetetra-acetic acid also disrupts the binding of LECintegrins to their ligands by chelating Ca2+ cations, and therefore it can inhibit LECmigration and proliferation (Nishi et al. 1996d). Lens epithelial cell adhesion moleculeblocking agent had a synthetic RGD peptide, which was used to inhibit LEC integrins bycompetitive binding to the integrin beta chain (Nishi et al. 1997b). The onlyimmunotoxin, which has been tried in human cataract operations, is immunotoxin MDX-RA (Clark et al. 1998). It could significantly reduce PCO and was well tolerated (Clark etal. 1998). Thapsigargin and caffeine inhibited LEC growth in cell culture (Duncan et al.1996). Thapsigargin-coated IOLs inhibited LEC growth in a human capsular bag culturesystem and total cell death of the residual anterior epithelial cells was achieved withhigher concentrations (Duncan et al. 1997). Thapsigargin and caffeine both inactivateCa2+ cations, thapsigargin by blocking the Ca2+�ATPase reuptake mechanism, andcaffeine by blocking the release channel of Ca2+ from the cell (Duncan et al. 1997).
2.3.5.3 Anti-inflammatory and immunomodulating drugs
Indomethacin (Nishi et al. 1995a, Nishi et al. 1995b, Nishi et al. 1996e, Tetz et al.1996b), diclofenac sodium (Nishi et al. 1995a, Cortina et al. 1997,) and cyclosporin A(Cortina et al. 1997) inhibited LEC proliferation in cell culture. They all were shown todecrease the amount of prostaglandin E2 produced by the LECs. Indomethacin-coatedIOLs significantly reduced postoperative inflammation and PCO in rabbit eyes (Nishi etal. 1995b). Sustained release of indomethacin also significantly decreased inflammation,but it did not reduce PCO in rabbit eyes (Nishi et al. 1996e, Tetz et al. 1996b).
2.4 Methods to treat posterior capsule opacification
2.4.1 Surgical discission and polishing
The opacified posterior capsule can be opened surgically or polished. In discission aneedle is inserted into the eye via pars plana, and an opening is made into the fibroticposterior capsule. Shah et al. (1986) found more complications related to surgicaldiscission (retinal detachments 3% and cystoid macular edema 2%) than to Nd: YAGlaser capsulotomy (retinal detachments 0.17% and cystoid macular edema 0.68%). At thesame study, polishing the posterior capsule was as safe method as Nd: YAG lasercapsulotomy.

39
2.4.2 Neodymium: YAG-laser capsulotomy
The principle of Nd: YAG laser capsulotomy in treating PCO is to cause photodisruptionat extremely high energy levels, thereby disintegrating tissues (Bell & Landt 1967,Barnes & Rieckhoff 1968, Fradin et al. 1973, Aron-Rosa et al. 1981, Ficker & Steele1985). The target tissue at the laser focus absorbs energy and is ionized to a gaseous state.There is an instantaneous temperature rise of about 10.000 degrees C°, which results inrapid expansion, explosive in nature and generates a powerful shock wave. This acoustictransient is a function of the power and duration of the laser pulse.
Nd: YAG laser capsulotomy has been shown to significantly improve visual acuity,contrast sensitivity, and glare disability (Magno et al. 1997), but the procedure is notwithout risks.
2.4.2.1 Complications after neodymium: YAG-laser capsulotomy
After an analysis of 3000 Nd: YAG laser capsulotomies, Shah et al. (1986) detailed thefollowing complications: marks on IOL 12%, transient elevation of IOP 8.5%, cystoidmacular edema 0.68%, retinal detachment 0.17%, hyphema 0.15%, iritis 0.10% and IOLentrapment 0.10%.
All IOL materials can be marked during Nd: YAG laser capsulotomy, but there aredifferences in damage thresholds and pit size. Dick et al. (1997) found silicone,polyHEMA, and acrylic IOLs containing HEMA to have the highest YAG laserresistance, with the smallest amount of posterior surface damage in comparison toPMMA IOLs. This large study compared 17 different IOL types. Newland et al. (1999)compared PMMA, silicone and soft, hydrophobic acrylate IOLs and found that siliconehad the lowest threshold for laser-induced damage, and greater linear extension ofdamage than PMMA and acrylic polymers. The discrepancy of results is explained bydifferent study patterns; Dick et al. (1997) measured the area of damage and Newland etal. (1999) the depth of the damage in the IOLs. Worst case, marks in the IOL can lead toIOL explantation because of increased glare (Bath et al. 1987).
The intraocular pressure (IOP) rise after Nd: YAG laser capsulotomy can be transient(Shah et al. 1986) or long-term (Fourman & Apisson 1991, Steinert et al. 1991, Jahn &Emke 1996). After a mean follow-up of 3 years, a late-onset elevation of IOP was seen in1.4% of uncomplicated ECCE patients, and in 5.9% of uncomplicated ECCE and Nd:YAG laser capsulotomy cases (Fourman & Apisson 1991). The risk for worsening ofpreexisting glaucoma was 0.56% (Steinert et al. 1991).
Cystoid macular edema has occurred in 0.68-1.23% of patients after Nd: YAG lasercapsulotomy (Shah et al. 1986, Steinert et al. 1991). Development of bilateral macularholes has been reported after an uncomplicated ECCE and Nd: YAG laser capsulotomy(Blacharski & Newsome 1988).
The incidence of lifetime retinal detachment in emmetropes is 0.06% and between 0.7-6.6% in myopes (Curtin 1985). ECCE and IOL implantation increased the risk inemmetropes to 1.4%, and in high myopia (axial length over 25-26mm) from 3.5 to 9.9 %(Clayman et al. 1981, Percival et al. 1983, Coonan et al. 1985, Lindstrom et al. 1988,
40
Javitt et al. 1991). The incidence of retinal detachment after phacoemulsification and IOLimplantation alone was 0.4 - 0.75% (Powell & Olson 1995 and Olsen & Olson 2000) andin high myopia 1.9% (Colin & Robinet 1997). After ECCE, IOL implantation and Nd:YAG laser capsulotomy, the incidence of retinal detachment was from 0.89% to 1.64%(Ambler & Constable 1988, Dardenne et al. 1989, Steinert et al. 1991), but a lowerincidence of 0.17% has also been shown (Shah et al. 1986), and in high myopic eyes 6%(Nissen et al. 1998). The incidence of retinal detachment after phacoemulsification, IOL,and Nd: YAG laser capsulotomy was from 0.85% to 1.59% (Dardenne et al. 1989, Powell& Olson 1995). Olsen & Olson (2000) found no detachments after phacoemulsification,IOL implantation and Nd: YAG capsulotomy. The risk factors for retinal detachment wereatrophic holes, particularly in the superior quadrants of the retina (Ranta & Kivelä 1998).The risk factors were the same for patients after ECCE and IOL implantation with anintact posterior capsule, and after Nd: YAG laser capsulotomy (Ranta & Kivelä 1998).Laser parameters, such as the energy and amount of exposure, did not correlate with theincidence of retinal detachment (Dardenne et al. 1989, Steinert et al. 1991).
IOL luxation into the vitreous cavity after Nd: YAG laser capsulotomy has beenreported with hydrogel and silicone plate haptic IOLs (Levy et al. 1990, Lowe & Easty1992, Schneiderman et. al 1997, Dahlhauser et al. 1998, Dick et al. 1998). IOL luxationcan occur due to IOL backward movement after Nd: YAG capsulotomy (Findl et al.1999). The backward movement was more pronounced with plate haptic silicone IOLsthan with PMMA, 3-piece silicone, polyHEMA (MemoryLens®), or soft, hydrophobicacrylate IOLs (AcrySof®) (Findl et al. 1999). Exacerbation of an intraocular infection hasbeen reported after Nd: YAG laser capsulotomy in a previously inflammation-free eye(Tetz et al. 1987). The IOL had to be explanted and Propione acnes bacteria were foundto be the reason for inflammation, after bacteria had been released from a closed capsularbag after laser capsulotomy (Tetz et al. 1987).

3 Purpose of the present study
The primary aim of the first part of the study was:
1. To study bioactive bonding of different keratoprosthesis materials to cornealstromal tissue in a rabbit model.
Our study with titanium and glass ceramic-coated titanium keratoprosthesis was doneat the time when most IOLs used in cataract surgery were made of PMMA. After havingnoticed that a keratoprosthesis made of PMMA did not attach to the corneal stromaltissue, and after my own good clinical experience and successful clinical reports withsoft, hydrophobic acrylate IOLs, the later part of the study was started to find the possiblereasons for less PCO with IOLs made of acrylate material. Specifically, the detailed aimsof these studies were:
2. To relate the findings of corneal tissue attachment to a bioactive glass-ceramiccoated keratoprosthesis and the bioactive IOL bonding to the capsular bag: thesandwich theory.
For an IOL with a suitable amount of bioactivity, the sandwich theory related to PCOformation is presented in Fig. 2 (color plate): A continuous curvilinear capsulorhexis isperformed during cataract surgery. The anterior capsule over the IOL�s bioactive surfacebonds directly, or as a result of the remaining LECs to the IOL surface, preventing furtherLEC proliferation. Thus, the anterior capsule over the IOL remains clear. When thisbonding is complete, the IOL and the capsular bag are a closed system. Inside the bag, theremaining LECs proliferate and start to migrate behind the IOL. The 90 degree edge ofthe IOL optic against the posterior capsule partly hinders and directs the proliferatingLECs to form a monolayer between the IOL and the posterior capsule. Another bioactivebond is formed when a single lens epithelial cell has the posterior capsule on one side andthe bioactive IOL surface on the other side. The sandwich is formed and the cell-posteriorcapsule and the cell-bioactive IOL surface junctions prevent more cells from migratingbehind the IOL. The posterior capsule remains clear. After some time, some of themonolayer cells will die because of aging, poor nutrition or the IOL-induced pressure onthe posterior capsule. After presenting the sandwich theory, the detailed aims of thesubsequent studies were:

42
3. To study the possible bonding of rabbit corneal stromal tissue to different IOLmaterials in a tissue culture.
4. To study the possible mechanisms behind bioactive bonding of different IOLmaterials by comparing differences in protein adhesion to IOL surfaces betweendifferent IOL materials.
5. To evaluate the theory and the results of the above mentioned studies against thefindings in human pseudophakic autopsy eyes.

4 Methods
4.1 Study of the corneal tissue response and formation of a bioactive bond between rabbit corneal tissue and different keratoprosthesis
materials
4.1.1 Model and fabrication of keratoprosthesis
The keratoprostheses were made of commercial pure titanium or PMMA using acomputer numeric controlled (CNC) lathe. The design of the intracorneal implant is seenin paper I, Fig. 1. The prosthesis model was the same as previously used by Kirkham &Dangel (1991). It has a 9.0 mm diameter flange with 8 holes, and a supporting part for theoptic in the center. The optic part was made of poly (methyl methacrylate) (PMMA),provided by Kabi Pharmacia AB (Uppsala, Sweden). Eleven of the 22 titanium implantswere coated with a SiO2-CaO-MgO-P2O5 based apatite (Ca l0 (PO4) 6 0) and wollastonite(SiCaO3) containing glass-ceramic (I: Fig. 2) (Pajamäki et al. 1995). The starting frit forthe bioactive glass-ceramic (BGC) coating of the titanium implants was prepared bymixing the glass powder (diameter < 45 µm), ethanol and acetone. The titanium implant,which was cleaned in 30% HCl solution and then in acetone, was dipped once in the frit.The frit was leveled out by microvibrations and dried for 1-2 minutes in a stream of warmair. The coated prosthesis was then preheated for one hour at 400°C. Firing was carriedout for 20 minutes in a protective Argon atmosphere at 900°C. The implant was cooled(5°C/min) under Argon gas to 500°C, after which the cooling proceeded to roomtemperature with the cooling of the furnace without the protective gas. A clear PMMA-optic was mounted in the titanium frame. The titanium implant was first treated with aprimer (Scotch Bond, 3M, St. Paul, MN, USA) on the surface of the hole for the opticpart. The primer was allowed to dry for some minutes in air after which a multipurposelight curing bonding agent (Scotch Bond, 3M, St Paul, MN, USA) was applied and theoptic part was mounted in place under a stereomicroscope. The bonding agent was thenlight cured for 30 seconds using blue light curing equipment for dental fillings (Visilux,3M, St. Paul, MN, USA). After the mounting of the lens, the keratoprosthesis wascleaned in ethanol, dried, and sterilized with ethylene oxide gas.
44
4.1.2 Implantation of the prosthesis
In the study 25 New Zealand White rabbits were operated on. 11 titanium-, 11 glass-ceramic coated- and 3 PMMA-prostheses were used. The rabbits were anesthetized with a50%/50% mixture of medetomidine hydrochlorid 10 mg/ml, 300 µg/kg (Domitor forte®,Orion, Turku, Finland) and ketamine hydrochloride 50 mg/ml, 20mg/kg (Ketalar®,Parke-Davis Scandinavia, Espoo, Finland) given intramuscularly. When the rabbits wereanesthetized, an intravenous cannula was inserted in a vein of the rabbits� ear and theanesthesia was maintained with the same drugs. The cornea was anesthetized withoxybuprocain hydrochloride (Oftan Obucain®, Leiras, Tampere, Finland). Both eyeswere examined with an operating microscope and only rabbits with two healthy eyeswere included in the study. Only one eye was operated on.
The eye was covered with a plastic dressing (Tegaderm 1626 Transparent Dressing,3M, St.Paul, MN, USA), which was opened with scissors, and the eyelid retractor was putin place. The eye was rinsed with neomycin and chloramphenicol drops (MinimsChloramphenicol and Neomycin®, Smith & Nephew Pharmaceuticals LTD, Romford,England). Sterile aqua was dropped over the cornea to haze the epithelium and the epithe-lium was removed with a knife (Alcon Ophthalmic Crescent Knife, angled bevel up,Alcon Surgical, Inc., Fort Worth, TX, USA). A 3.0 mm diameter trephine was used tomake a round incision for the optic part of the prosthesis. The trephination in the corneawas made as deep as possible without perforating it. The trephinated cornea was cut witha knife (Alcon Ophthalmic Crescent knife, angled bevel up). A second corneal limbal150°-170° incision was made superiorly with a 45° knife (Moria #45000, Moria, Paris,France), also close to Descemet´s membrane. From this incision, a lamellar dissection ofthe cornea was made with a knife. In the last three operations the lamellar dissection wasstarted from the trephination towards the limbus. By doing so, it was easier to get adeeper lamellar dissection without perforating the cornea. The supra-Descemet´s mem-brane prosthesis was put in place and the limbal incision was sutured with 9.0 polypropy-lene (Prolene®, Ethicon, Inc., Somerville, New Jersey, USA) and 10.0 monofilamentnylon knots (Ethilon®, Ethicon LTD, Edinburgh, U.K.). The conjunctiva was opened360° from the limbus, released and sutured with 8.0 silk knots and a running suture overthe prosthesis (Virgin silk®, Ethicon LTD, Edinburgh, U.K.). Dexamethasone-chloram-phenicol-ointment (Oftan-Dexa-Chlora®, Leiras, Tampere, Finland) was put over thesutured conjunctiva and a temporary tarsorrhaphy was made with three 5.0 monofilamentnylon knots (Dermalon®, Davis & Geck, Cyanamid Medical Device Co., Inc., Anyang,Korea). Postoperatively, chloramphenicol (Oftan-kloramfenikol®, Leiras, Tampere, Fin-land) was applied twice a day in the operated eye for two weeks. After two weeks the tar-sorrhaphy was opened. At this time the optic part had already shown itself through theconjunctiva in every eye. The sutures in the cornea were not removed.
Two rabbits in each group were randomly selected for follow-up at 1, 2, 4, or 8months. The observation period of the remaining 3 rabbits was 12 months. A thoroughclinical examination and photography of the eyes of each rabbit were performed at thetime periods given above. The animals were sacrificed with an overdose of pentobarbitalgiven intravenously (60 mg/kg; Mebumat®, Orion, Espoo, Finland). Two rabbits with atitanium prosthesis died 6.5 and 10.5 months after the operation, respectively. These twoeyes were included in the follow-up groups of 8 and 12 months, respectively.

45
4.1.3 Analysis of corneal tissues with the keratoprosthesis
The enucleated eyes were fixed in 4% phosphate-buffered neutral formalin and embeddedin plastic (Technovit, Kulzer GmbH, Wehrheim, Germany). Histologic sections wereprepared through the central part of the cornea and the prosthesis using a cutting-grindingmethod and stained with toluidine blue (Donath & Breuner 1982). The histologicalanalysis was made on both halves of the implant separately to provide two analysis areasin each eye. The inflammatory reaction around the implant was graded as none, mild,moderate or severe. The extent of epithelial ingrowth was graded from 0 to 4. In grade 0,the epithelium remained beside the optic part. Epithelial ingrowth not extending furtherthan half way to the external side of the flange was graded as 1. In grade 2, growth ofepithelium up to the whole length of the external aspect of the flange was seen. Grades 3and 4 were used if the epithelium grew under the flange or under the optic part,respectively. Grades 0 and 1 were considered a non-significant ingrowth of epithelium. Ingrade 0 there was no ingrowth at all, and in grade 1 the amount of the ingrowth would notendanger the stability of the keratoprosthesis or its optical performance in the eye.
The blocks remaining from the cutting-grinding process were coated with carbon andscanning electron microscopy (SEM) and energy dispersive x-ray analyses (EDXA)(Stereoscan 360, Cambridge Instrument Ltd, Cambridge, UK) were used to study thereactions of the glass-ceramic.
4.2 Rabbit corneal tissue cultures on different IOL materials
4.2.1 IOLs used in tissue culture
Rabbit corneal tissue cultures were set up on different types of IOLs: PMMA (Pharmacia& Upjohn 809P), heparin-surface-modified PMMA (Pharmacia & Upjohn 808C),silicone (Allergan Medical Optics SI-30), and acrylate (Alcon AcrySof®). In the secondcultures series another kind of silicone (Pharmacia & Upjohn CeeOn 920�) andhydrogel (Storz Hydroview�) IOLs were also studied. The material in both siliconeIOLs tested was dimethyldiphenylsiloxane (DMDPS)
4.2.2 Preparation of histologic sections
The goal was to evaluate tissue attachment to the IOL. Corneal tissue was obtained fromrabbits that had been killed no longer than 20 minutes before explantation. A surgicalknife (Alcon Ophthalmic Knife, 15 degrees) was used to cut the corneal tissue. The eyewas kept moist with culture medium at the time of the explant preparation. The culturemedium was also applied to the IOL surface before the explant was put on it. Culturedtissue consisted of intact epithelium and half the thickness of the corneal stroma, whichwas placed against the IOL (Fig. 3). Two square 1.0 to 2.0 mm × 1.0 to 2.0 mm explantswere cultured for 1 week on each IOL in Dulbecco minimum essential medium (MEM)

46
(Sigma) with bovine fetal calf serum 5% (BFCS) (Sigma) and antibiotics (streptomycinsulfate 100 µg/mL and sodium G-penicillin 100 IU/mL).
Fig. 3. Cultured tissue consists of intact epithelium and half the thickness of the corneal stroma,which was placed against the IOL. The 1.0 to 2.0 mm × 1.0 to 2.0 mm explants were culturedfor 1 week in cell culture medium.
The Petri dishes were kept at 37°C in humidified chambers. The gas atmospherecontained carbon dioxide 5%. During the one-week culture period, the medium waschanged once. For light microscopy, the cultured explants were fixed in formalin andembedded in plastic. Sections from the explants were made by using the cutting andgrinding method and stained with toluidine blue. The growth of the epithelium wasexamined to evaluate the attachment of the explant to the IOL and, as a consequence, theability of this attachment to prevent epithelial ingrowth between the stroma and the IOL.The findings were classified as no attachment, epithelial attachment, or stromalattachment (Fig. 4).
Fig. 4. The growth of the epithelium was examined to evaluate attachment of the explant to theIOL, and thus the ability of the attachment to prevent epithelial ingrowth between the stromaand the IOL. The findings were classified as no attachment, epithelial attachment, or stromalattachment.
IOL
IOL IOL IOL
No attachment Epithelial attachment Stromal attachment

47
4.3 Adhesion of soluble fibronectin, laminin and collagen type IV to different IOL materials in vitro
4.3.1 Incubation method and IOLs used with radioactive labeled proteins
Intraocular lenses composed of poly (methyl methacrylate) (PMMA) (Alcon CrystalSeries type 02), heparin-surface-modified PMMA (809C, Pharmacia and Upjohn),silicone (CeeOn� 920, Pharmacia & Upjohn), acrylate (AcrySof®, Alcon), and hydrogel(Hydroview�, Storz) were incubated with 3 radioactively labeled extracellular matrixproteins: type IV collagen and laminin extracted from Engelbreht-Holm-Swarm-mousetumor and human fibronectin. Labeling with type IV collagen, laminin, and fibronectinwas repeated 5 times for each IOL material. Thus, 75 IOLs were used.
Proteins were radioactively labeled with iodinating tyrosine residues according to thefollowing protocol: laminin and fibronectin were diluted in sterile water and type IVcollagen in 0.05 M hydrochloride. Then, 2 µg of protein in 30 µL of dilution buffer wasincubated with 10 µL of chloramine T (0.5 mg/mL) and 1 µL of I-125 for 60 seconds.The reaction was terminated by 10 µL of sodium metabisulfite (1 mg/mL). Thechloramine T and sodium metabisulfite were diluted in 0.25 M sodium phosphate (pH7.3). A balanced salt solution (Endosol®, Allergan Medical Optics) was added to a finalvolume of 100 µL. The radioactively labeled proteins were separated fromunincorporated I-125 residues by gel filtration using 1% bovine-serum albumin-coatednick columns and Endosol® as a buffer. Fractions of approximately 100 µL werecollected, and the one containing the purified labeled protein was used for the adhesionstudies.
The labeled probe was diluted with Endosol® buffer to a suitable radioactivity. Then,500 µL of the reaction buffer was measured into radioimmunoassay bottles and the initialradioactivity was measured with a wavelength counter (LBK-Wallac 1260 MultiGamma)before the IOLs were added. Each IOL was incubated with the labeled protein for 24hours at 37°C in a water bath. The IOLs were then washed repeatedly in Endosol buffer,and the amounts of radioactively labeled protein that had adhered to them were measuredwith the wavelength counter and expressed as counts per minute (cpm).The binding of protein (cpm) was measured for each IOL type, and the means andstandard deviations were calculated. Differences between the IOL types were tested withthe Student t test or the Mann�Whitney U test when variances between the samples wereunequal.
48
4.4 Adhesion of fibronectin, vitronectin, laminin and collagen type IV to IOL materials in pseudophakic
human autopsy eyes; The histologic sections
4.4.1 Immunohistochemical method and IOLs used
Thirty-eight human autopsy eyes containing IOLs made of poly (methyl methacrylate)(PMMA; n = 10), silicone (n = 10), hydrophobic soft acrylate (n = 14) or hydrogel (n = 4)were analyzed. The PMMA IOLs were single-piece designs from various manufacturers.The silicone IOLs were 3-piece model with silicone optic and a polypropylene(Prolene®) haptics (8 Allergan Medical Optics SI-30 and 2 IOLAB). The acrylate IOLswere all AcrySof® IOLs (Alcon). The hydrogel IOLs were single-piece plate-hapticdesign (Iogel PC-12, Alcon). The time from cataract surgery to death of the eye-bankdonors is unknown.
Gross photographs of the IOLs in the capsular bag were taken from a posterior viewusing the Miyake-Apple technique, and from an anterior (surgeon�s) view after the corneaand iris were removed. All eyes were fixed in formalin 10 % and cut in the pupil-opticnerve plane, with the cuts oriented parallel to the IOL haptics so the entire IOL in theentire capsular bag could be seen.
After the samples were dehydrated and embedded in paraffin, 12-15 serial, 3 µm-thicksections were made from each eye. Two sections from each eye were stained withMasson�s trichrome for normal histological evaluation, and the others were used forimmunohistochemical detection of fibronectin, vitronectin, laminin and collagen type IV.One hundred fifty-two immunohistochemical specimens were evaluated from 38 eyes.
For the immunohistochemical reactions, the sections were put in xylene to remove theparaffin and rehydrated in a series of alcohols. The sections were rinsed in phosphate-buffered saline (PBS) at pH 7.4, and then rinsing the sections with hydrogen peroxide-methanol 3 % for 20 minutes eliminated endogenous peroxidase activity. The sectionswere then again rinsed with PBS. To eliminate non-specific background staining, thesections were incubated with non-immune serum from the Histostain®-Plus kit (ZymedLaboratories Inc, San Francisco, CA, USA). The primary antibodies were allowed to reactwith the sections for 60 min at room temperature. Antibodies used were mouseantifibronectin monoclonal (reacts with the cellular- as well as plasma-derived form offibronectin), mouse antihuman vitronectin monoclonal (reacts with vitronectin in itsnative and denatured forms), mouse anti-human collagen type IV monoclonal (reacts withα2 chains of collagen type IV, Chemicon International Inc., Temecula, CA, USA) andrabbit anti-laminin polyclonal (Sigma, St. Louis, MO, USA). The dilution for theseantibodies was 1:100, with the exception of 1:25 for the anti-laminin antibody. Theincubating time used for the biotinylated secondary antibody was 30 minutes.
The bound primary antibodies were visualized using the avidin-biotin-horseradishperoxidase method with aminoethylcarbazole (AEC) as chromogen (Histostain®-Plus kit,Zymed Laboratories Inc., San Francisco, CA, USA)(Fig. 5). The sections werecounterstained with hematoxylin. Negative control sections, (i.e. sections processed

49
without the primary antibody) were included in every staining patch. Purified humanfibronectin, vitronectin (Chemicon International Inc., Temecula, CA, USA), and laminin(Sigma, St. Louis, Mo, USA) were used as positive controls. Sections from the capsularbag and the liver of a rat were used as positive controls for collagen IV.
The histologic sections were examined and photographed using a light microscope(Olympus Optical Co. Ltd., Japan). The presence of extracellular proteins was recorded inthe following anatomical location: in the lining over the anterior capsule, within theanterior capsule, in the LECs, in the fibrotic tissue on the inner surface of the anteriorcapsule, in Soemmerring�s ring, in the lining of the haptic, in the fibrotic tissue betweenthe IOL and the posterior capsule, in the lining of the posterior capsule, and within theposterior capsule. The sections were also evaluated for the presence of a sandwich-likestructure containing fibronectin, vitronectin, or laminin (e.g., anterior or posteriorcapsule/fibronectin/LEC layer/fibronectin/IOL surface) (color plate: Fig. 6, V: Fig. 1).Staining was noted as positive, negative, tissue not present in the eye or tissue notavailable for evaluation in the specimen. As the chromogen used for color reaction wasAEC, positive staining was red or purple red in the sections and photomicrographs.
Fig. 5. Immunohistochemical method used in papers V and VI. Extracellular matrix proteinsin the histologic section or on the IOL surface are recognized with primary antibody.Biotinylated secondary antibody is added, and the bound primary antibodies are visualizedusing the avidin-biotin-horseradish peroxidase method with aminoethylcarbazole (AEC) as thechromogen.
AEC -kromogen colored sediment (red, purple)
+
horseradishperoksidase enzyme connected to avidin
secondary antibody connected to biotin
primary antibodies against fibronectin, vitronectin, laminin, and collagen type IV
extracellular matrix, cells, or IOL surface with antigen on the surface

50
4.4.2 Statistical analyses used for histologic sections
An exact test of the difference between binomial proportions was used to determine pair-wise differences between IOLs for fibronectin, vitronectin and laminin in the sandwich-like structure and laminin on the inner surface of the anterior capsule. To adjust for thenumber of comparisons, significance was declared at a Bonferroni adjusted level (α=0.05/6 ≈ 0.01). Comparisons between tissues, or between proteins, were made using exactKruskal Wallace tests. The exact tests for differences between binomial proportions andthe exact Kruskal Wallace tests were performed using StatXact 4 (Cytel, Cambridge,MA). After the Kruskal Wallace tests, logistic regression was used to determine thesignificance of differences of the other IOL materials relative to acrylate. Significance inthe Kruskal Wallace tests, and logistic regression analysis, was declared at P=0.05.Logistic regression was done using LogXact 2 (Cytel, Cambridge, MA).
4.5 Adhesion of fibronectin, vitronectin, laminin and collagen type IV to IOL materials in pseudophakic
human autopsy eyes; explanted IOLs
4.5.1 Histologic methods and IOLs used
Thirty-two autopsy eyes containing IOLs made of poly (methyl methacrylate)(PMMA;n = 8), silicone (n = 9), hydrophobic soft acrylate (n = 13) (referred hereafter as acrylate)or hydrogel (n = 2) were analyzed. The PMMA IOLs were one-piece designs fromvarious manufacturers. The silicone IOLs were 3-piece model with silicone optic and apolypropylene (Prolene®) haptics (SI-30NB, Allergan Medical Optics). The acrylateIOLs were AcrySof® IOLs (12 MA30 and one MA60, Alcon). The hydrogel IOLs were asingle-piece plate-haptic design (Iogel PC-12, Alcon). The time from cataract surgery todeath of the eye-bank donors is unknown.
Gross photographs of the IOLs in the capsular bag were taken from a posterior viewusing the Miyake-Apple technique and from an anterior (surgeon�s) view after the corneaand iris were removed. All eyes were then fixed in formalin 10%. The IOLs wereexplanted from the capsular bag under an operating microscope.
Immunohistochemical analysis of the extracellular matrix proteins on the IOLs wasperformed for fibronectin, vitronectin, laminin and collagen type IV. One hydrogel IOLwas analyzed for fibronectin and the other, for laminin. Five PMMA IOLs were analyzedfor fibronectin and one each for laminin, vitronectin and collagen type IV. Five siliconeIOLs were analyzed for fibronectin, 2 for collagen type IV, and 1 each for laminin andvitronectin. Five acrylate IOLs were analyzed for fibronectin, 6 for vitronectin and oneeach for laminin and collagen type IV. The immunohistochemical method for detectingthese proteins was the same as in 4.5.1.
Of the acrylate IOLs analyzed for vitronectin, 2 were processed according to themethod described above, and 2 were incubated with the primary antibody for 40 minutesat 37°C instead of room temperature. For the other acrylate IOLs, purified human

51
vitronectin (Chemicon International Inc., Temecula, CA, USA) was allowed first to reactwith vitronectin antibody at a dilution of 5:1 for 30 minutes. The IOLs were thenprocessed according to the normal immunostaining method described in 4.5.1. Thisblocked the antibody to ensure that staining observed on the IOL surfaces was from thepositive staining of the protein, not the color reagents used. One capsular bag from oneeye containing an acrylate IOL was examined for fibronectin and vitronectin.
The IOLs and the capsular bag were examined for the presence of the extracellularmatrix proteins and cells and photographed using a light microscope (Olympus OpticalCo. Ltd., Japan). The anterior and posterior surfaces of the IOLs were analyzed bychanging the microscope�s focus. The chromogen used for color reaction wasaminoethylcarbazole, which produced red staining on the IOL surfaces. The grading forthe extracellular proteins was as follows: no adhesion (0), low adhesion (1 to 3), moderateadhesion (4 to 6), high adhesion (7 to 9), and fully covered (10) with protein. The numberof cells on the IOLs was counted and scored as: 0 = no cells, 1 = 1 to 5 cells, 2 = 6 to 10cells, 3 = 11 to 15 cells and 4 = over 16 to 20 cells. Cells were counted separately in the3.0 mm central optic zone of the IOL, at the periphery of the IOL, and in the area of theIOL optic-haptic junction.
4.5.2 Statistical analyses used for explanted IOLs
Cell count data was expressed as the midpoints of the classes, (e.g., classes 0, 1, 2, 3, 4were replaced by numbers 0, 3, 8, 13, and 18, respectively). Protein adhesion data hadbeen recorded as no adhesion (0), low adhesion (1 to 3), moderate adhesion (4 to 6), highadhesion (7 to 9), and fully covered (10). The midpoints of these classes were also usedfor analysis. Defining R as a matrix of the number of cells, or protein quantities, in thehaptic area and on the anterior and posterior surfaces of each lens, the repeated measuresmodel used for both cell data and adhesion data was:
R = µ + protein + IOL + protein × IOL.
The quantity, µ, is estimated by the mean of all of the sample data (µ is comprised ofµhaptic, µanterior and µposterior). R is a set of responses that occur in a specified sequencedetermined by physiology of the eye, that is: the haptic area, anterior surface, andposterior surface occur in a fixed sequence, which can not be randomized under thecontrol of the researcher. The right side of the equation says that the changes in R arerelated to protein and IOL through additive and multiplicative combinations. Theequation says, that changes in the response, R, are due to changes in protein and IOL, thatare additive to each other, and additionally, that changes in protein and IOL also affect theresponse in a nonlinear way. The equation also says, that the causes of the changes (thatis, the right side of the equation) affect the responses (that is, the haptic area, posteriorand anterior) in quantitatively similar ways. Differences with a P value less than 0.05were considered significant, and differences with P value less than 0.1 were consideredmarginal. An overall test for IOL was performed over all levels of R and protein, and anoverall test for protein was performed over all levels of R and IOL. Post hoc tests ofcombinations of IOLs and/or protein and R were done.

5 Results
5.1 Outcome of keratoprosthesis made of titanium, bioactive glass-coated titanium and PMMA in rabbit cornea (I)
5.1.1 Clinical findings
All the 11 titanium prostheses and 9 of the 11 BGC-coated titanium prostheses (colorplate: Fig. 7) were retained for the time periods planned. Neovascularization over thesupporting part of the prosthesis was noticed in all eyes one month postoperatively andwas considered a desired result for the healing process and nutrition for the cornea. Theglass-ceramic coating of the two prostheses lost prematurely (rabbits No. 19 and 15) wasconsiderably thicker than that of the other coated implants making the prostheses thickerthan the cornea proper. In rabbit No. 19 three extra holes appeared in the external corneallamellae over the thick prosthesis during the insertion and two of them could not besutured. This prosthesis extruded two weeks postoperatively and the animal wassacrificed two weeks later. The cornea was healed without perforation. In rabbit No. 15,the corneal lamellae over the prosthesis broke in two areas and two extra sutures wereneeded. The prosthesis was noticed to be mobile at sacrifice one month after theoperation. For the obvious difficulties related to the surgery these two rabbits were notincluded in the analysis of the results. Two micro perforations in the anterior chamberoccurred during the surgery of two other rabbits but they did not cause any harm. Nopostoperative infections occurred. One month postoperatively the optic part had comethrough the conjunctiva in all eyes. At the end of the follow-up periods the red reflex andthe iris could be seen through the optic in all but three glass-ceramic coated prostheses inwhich the epithelium grew partly over the prosthesis, and in one titanium prosthesis,which had epithelial ingrowth under the prosthesis. The fundus of the eye could be seenwith an ophthalmoscope but we were unable to get fundus photographs from livingrabbits.

53
All three keratoprostheses made of PMMA (color plate: Fig. 8) were removed with theglobe for evaluation after one month. The optic area was visible with no cornealepithelium growing over it. All three prostheses were noticed to be mobile at the time ofsacrifice.
5.1.2 Histologic findings
Altogether, 11 titanium prostheses (22 analysis areas), 9 glass-ceramic coated prostheses(18 analysis areas), and 3 PMMA prostheses were available for histological examination.Inflammatory reaction was almost nonexistent in 19/22 of the analyzed areas in thetitanium group. In the remaining 3 analysis areas a mild to moderate inflammationconsisting of a mixture of mononuclear and polymorphonuclear inflammatory cells wasseen around the implant. None of the 3 implants with inflammation had been followed formore than 4 months. The clinically observed neovascularization over the flange could notbe seen in histological specimens and there was no neovascularization under the opticpart of the prostheses. The epithelial ingrowth according to the follow-up time ispresented in Table 2. The epithelium was found to grow through the hole of thesupporting flange in 5 analysis areas. This phenomenon was accompanied with a mildinflammatory reaction in one of the 5 areas. Nine out of 18 analysis areas in the BGC-coated group were virtually free of inflammation. A mild, moderate and severe mixedinflammatory reaction was seen in 6, 1, and 2 analysis areas, respectively. Theinflammatory infiltrate was band-like and confined to the close vicinity of the implant.The 3 analysis areas graded as moderate to severe were connected with two differentprostheses followed for 4 and 12 months, respectively. No epithelial ingrowth was seen inconnection with the 12-month implant. The epithelial ingrowth along the BGC-coatedprostheses is presented in Table 2. The epithelium grew through the hole of one flangeand over the optic part of two implants.
The histological analysis revealed considerable variation in the thickness of the BGC-coating. A reaction layer seen as a dark zone in the histological sections was noticed onthe surface of the BGC-coating at 2 months. This layer became thicker with time and wasfound to have grown through the whole coating at 8 months. Signs of the resorption of thecoating were detected in 10 analyzed areas. The resorption was more frequent in theimplants with the follow-up of 12 months and often accompanied with an inflammatorycell infiltrate. The detachment of the coating indicated by the growth of connective tissuebetween the titanium flange and the BGC-coating was noted in 3 analysis areas.
All three PMMA prostheses had epithelial ingrowth around the whole implant (Table2). The epithelial cell layer was several cells thick, and had quite intense inflammatoryreaction around the prosthesis (color plate: Fig. 8). A mixture of mononuclear andpolymorphonuclear inflammatory cells was seen around the implant.
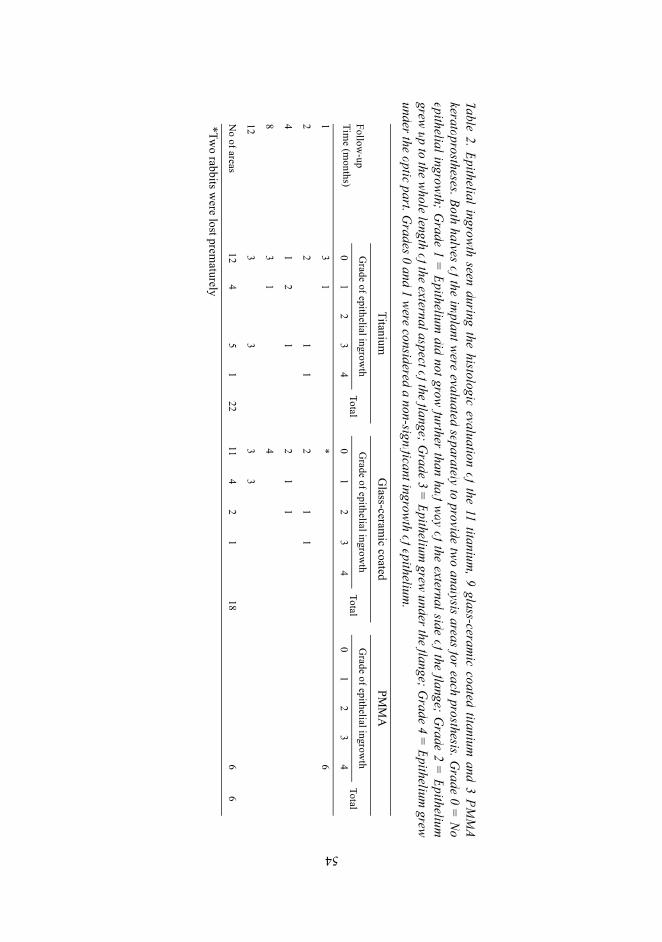
Table 2. Epithelial ingrowth seen during the histologic evaluation of the 11 titanium, 9 glass-ceram
ic coated titanium and 3 PM
MA
keratoprostheses. Both halves of the implant were evaluated separately to provide tw
o analysis areas for each prosthesis. Grade 0 =
Noepithelial ingrow
th; Grade 1 =
Epithelium did not grow
further than half way of the external side of the flange; Grade 2 =
Epitheliumgrew
up to the whole length of the external aspect of the flange; Grade 3 =
Epithelium grew
under the flange; Grade 4 =
Epithelium grew
under the optic part. Grades 0 and 1 were considered a non-significant ingrowth of epithelium
.
TitaniumG
lass-ceramic coated
PMM
A
Follow-up
Time (m
onths)G
rade of epithelial ingrowth
TotalG
rade of epithelial ingrowth
TotalG
rade of epithelial ingrowth
Total0
12
34
01
23
40
12
34
13
1*
6
22
11
21
1
41
21
21
1
83
14
123
33
3
No of areas
124
51
2211
42
118
66
*Two rabbits w
ere lost prematurely
54

55
5.1.3 Scanning electron microscopy (SEM) and energy dispersive X-ray analysis (EDXA)
The reaction layer of the coating seemed less dense than the unreacted glass-ceramiclayer examined with SEM. An EDX analysis showed that the content of Si and Mg haddecreased and that of P increased in the reaction layer. The findings on the thickness ofthe reaction layer were consistent with that seen in the histological analysis.
In conclusion (5.1), a good attachment to the corneal tissue was seen for the prosthesismade of titanium. Considering the histological findings, the glass-ceramic coatedprostheses performed better than the titanium prostheses. PMMA prostheses did not showany attachment to the corneal stromal tissue, indicating that PMMA as a material did notshow bioactive properties.
5.2 Outcome of rabbit corneal tissue cultures on different IOL materials (III)
The results are shown in paper III: Table 1. The corneal tissue samples grew well underthe culture conditions used, and the results were similar in two culture series. There wasno attachment of corneal tissue on any silicone IOL. Also, there was no tissue attachmentto any hydrogel IOL, but in most cases (3 of 4), 1 monolayer of cells grew on the IOL�ssurface. The cells were elongated, exhibiting epithelial cell characteristics. The PMMAand HSM-PMMA IOLs gave equivalent results. Six of the 8 specimens showed noattachment; in 2, the tissue was attached with epithelial cells. The acrylate IOLs reacteddifferently. There was a stromal attachment in 3 of the 8 specimens. Three otherspecimens were also attached, but in these cases epithelial cells mediated the attachment.
In conclusion, only acrylate IOLs did show direct, stromal attachment of culturedcorneal tissue to the IOL surface. This finding suggests that acrylate IOLs may havebioactive properties. Silicone IOLs had a bioinert interaction with the tissue, with noadhesion of cultured tissue to their surfaces. Hydrogel IOLs showed no tissue attachmentat all, but epithelial cells were seen to form a monolayer of cells on the IOL surfaces as asign of good material biocompatibility. This indicates that IOL bioactivity andbiocompatibility are two different qualities of the IOLs. The reactions of PMMA andHSM-PMMA IOLs were more bioinert than bioactive with the cultured tissues.

56
5.3 Adhesion of soluble fibronectin, laminin and collagen type IV to different IOL materials in vitro (IV)
Fibronectin adhered best to the acrylate IOLs; the differences between acrylate andsilicone (p<0.01), hydrogel (p<0.01), and HSM PMMA (p<0.001) were significant.Acrylate bound fibronectin better than PMMA, but the difference was not significant(p=0.31) (IV: Fig. 1). Fibronectin bound better to PMMA than to HSM PMMA(p<0.001), silicone (p<0.01), and hydrogel (p<0.05).
Although significantly more laminin bound to acrylate than HSM PMMA (p<0.05),PMMA (p<0.01), and silicone (p<0.001), hydrogel showed the highest binding to thisprotein, with significant differences between it and acrylate, PMMA, silicone (p<0.0001),and HSM PMMA (p<0.001) (IV: Fig. 2).
Hydrogel also had significantly higher binding of type IV collagen than any othermaterial (p<0.01 to 0.0001) (IV: Fig. 3). Both acrylate and silicone bound significantlymore type IV collagen than PMMA or HSM PMMA (p<0.01). Table 1 in paper IV showsthe means and standard deviations for protein adhesion to the IOLs.
In conclusion, all IOL materials studied had different extracellular matrix proteinadhesion to their surfaces in vitro. The stronger binding of fibronectin and laminin toacrylate may be the biological mechanism behind the better adhesion of acrylate IOLs tothe capsular bag. Collagen type IV adhesion was greatest to hydrogel IOLs.
5.4 Adhesion of fibronectin, vitronectin, laminin and collagentype IV to IOL materials in pseudophakic human autopsy eyes;
the histologic sections (V)
The anatomic structure of the posterior capsule and the cells behind the IOL weredifferent in the acrylate group than in the PMMA, silicone or hydrogel groups. Thepresence and location of fibronectin, vitronectin, laminin and collagen type IV are shownin paper V: Tables 1 to 4, respectively. The relationships between protein, tissue, and IOLare shown in paper V, Fig. 2.
Acrylate was the only group in which there was no fibrocellular tissue between theposterior IOL surface and the capsule in 12 of the 14 eyes. A sandwich-like structure(anterior or posterior capsule/ 1 cell layer/IOL surface) was observed in 12 of 14 eyes (in6-8 sections) in the acrylate group, in 3 of the 10 eyes in the PMMA group (P=0.0094), in1 of the 10 in the silicone group (P=0.0022) and in 0 of 4 in the hydrogel group(P=0.0041) (V: Fig. 3). The incidence of this structure was significantly higher in theacrylate group than in the other groups. There were no statistically significant differencesin incidence of the structure among PMMA, silicone and hydrogel IOL groups. Themediating extracellular protein in the pattern was fibronectin, which could be seenbetween the capsule and the LECs, and then between the LECs and the IOL surface in 12eyes with acrylate IOL (color plate: Fig. 6, 9, 10, 11 and V: Table 1, Fig. 1, 4-6).

57
Fibronectin was also found between the thick fibrocellular tissue on the inner surfacesof the anterior and posterior capsules and the PMMA IOL surface in the PMMA group(color plate: Fig. 12 and V: Table 1, Fig. 7). On silicone IOLs, collagen type IV was foundat the interface between a thick fibrotic tissue and the IOL surface (color plate: Fig. 13and V: Table 4, Fig. 8D, 9), the fibrocellular tissue contained fibronectin (V: Fig. 8A).Eyes with hydrogel IOLs also had thick fibrocellular tissue at the junction between theanterior capsule and the IOL (V: Fig. 10). The IOL-capsule interface in hydrogel IOL No4 was mediated by collagen IV (V: Fig. 10C).
In general, vitronectin (V: Fig. 8B, 10B, 11, 12) and laminin (V: Fig. 8C, 10D, 13, 14)could be seen in areas where fibrotic tissue accumulated (i.e., in the fibrocellular tissue atthe inner surface of the anterior capsule and beside the IOL optic) However, theseproteins were not in the layer next to the IOL surfaces, nor were they present in thesandwich-like structure of IOL/ LECs/capsule (V: Tables 2 and 3).
There was no difference among the IOL groups in the presence of vitronectin in theinner surface of the anterior capsule. However, there was less laminin on the inner surfaceof the anterior capsule in the acrylate group than in the other groups (acrylate versusPMMA, P=0.044, acrylate versus silicone, P=0.0024; acrylate versus hydrogel, P=0.011)(V: Table 3). The presence of collagen type IV in specimens is shown in paper V, Table 4and in Fig. 8D, 9, 10C, 15 and 16. In general, it was possible to assess for the presence ofcollagen type IV in sections. However, because of excessive and therefore unspecificstaining (e.g., on both sides of the anterior and posterior capsules), it could not bedetermined whether collagen type IV was found in the sandwich-like structures (V: Table4, Fig. 2).
In conclusion, acrylate IOLs were associated with less fibrocellular tissue between thelens capsule and the IOL than with PMMA, silicone, and hydrogel IOLs. Significantlymore often fibronectin was seen lining one LEC layer between the acrylate IOLs and theanterior or posterior capsules. This suggests that fibronectin may be responsible for thebioactive bond between acrylate IOLs and the LECs or the capsule. PMMA, silicone, orhydrogel IOLs were not seen to produce this kind of sandwich structure with LECs.Vitronectin and laminin were not found at the fibrocellular tissue-IOL interface in anyspecimen. Therefore they seem not to be responsible for the adhesion of the IOLs to thecapsular bag. The thicker fibrocellular tissue on the inner surface of the anterior orposterior capsule that was contact in silicone IOLs was lined with collagen type IV. Thismay suggest that collagen type IV does not mediate as strong adhesion as fibronectinbetween the capsules and the IOLs, and is here more as a result of insufficient adhesionand product of free proliferating LECs.
5.5 Adhesion of fibronectin, vitronectin, laminin and collagentype IV to IOL materials in pseudophakic human autopsy eyes;
Explanted IOLs (VI)
The assessments of cell and fibronectin, vitronectin, laminin, and collagen type IVadhesion to the IOL surfaces are shown in paper VI, Tables 1, 2, 3, and 4, respectively.

58
In the PMMA, acrylate and silicone groups, both the anterior and posterior surfacescould be evaluated. The hydrogel IOLs became opaque during the processing, and only 1side could be analyzed. The hydrogel IOL data were not used in the statistical analysesbecause the IOL x protein term in the model could not be solved because data forvitronectin and collagen type IV were missing.
There were more cells attached to acrylate IOLs than to PMMA or silicone IOLs.When all surfaces were counted (overall), the differences between acrylate and PMMA(P<0.05) or silicone (P<0.01) IOLs were significant. The overall difference betweenPMMA and silicone was also significant (P<0.05), with the silicone IOLs having fewercells attached to the surface. Table 5 in paper VI shows the P values for cell adhesion onthe IOLs� anterior and posterior surfaces and haptic area.
Overall protein adhesion differed significantly between acrylate IOLs and PMMA orsilicone IOLs, but not between PMMA and silicone IOLs. Protein in the haptic area, butnot in the anterior or posterior regions, differed significantly between acrylate IOLs (leastsquares mean 6.3±0.8[SE]) and PMMA (least squares mean 1.7±1.0[SE]) or silicone(least squares mean 1.5±0.9[SE]) IOLs.
The relationships between proteins and IOL materials are shown in color plate in Fig.14, and in paper VI in Fig. 1 and 2, and Tables 6-7. Significantly more fibronectin(overall surfaces) was attached to acrylate IOL surfaces than to PMMA (P<0.01) orsilicone (P<0.01) IOLs. The significant difference was seen relative to silicone for allsurfaces, and for PMMA at the posterior surface and haptic area. There were nosignificant difference in fibronectin adhesion between PMMA and silicone IOLs.
More vitronectin was attached to acrylate IOLs than to the single PMMA IOL assessed(P<0.06). Marginally more vitronectin was attached to the PMMA IOL than to siliconeIOL (P<0.1). There was more vitronectin on the posterior surfaces and haptic areas of theacrylate IOLs than on those areas of 1 silicone IOL; however, the difference was notsignificant overall.
There were no significant differences in laminin adhesion among acrylate, PMMA andsilicone IOLs. Significantly more collagen type IV was attached to silicone than toacrylate IOLs (P<0.05). More collagen type IV was attached to acrylate than to PMMAIOLs; the difference was marginally significant (P<0.06). No difference was foundbetween PMMA and silicone IOLs.
Minimal amounts of fibronectin and laminin adhered to the anterior surface of thehydrogel IOLs. The IOL stained for laminin had some cells on its surface. The cytoplasmof these cells, which resembled lens epithelial cells (LECs), also stained positively forlaminin and suggests that they were capable of producing this protein.
Fibronectin adhered to the anterior (color plate: Fig. 15, VI: Fig. 3A1, A2, B1, B2) andposterior (VI: Fig. 3C1, C2) surfaces of acrylic IOLs. Silicone IOLs had very little proteinor cell adhesion in all 3 areas (color plate: Fig 16, VI: Fig. 4A1, 4A2). On PMMA IOLs,minimal to moderate amounts of fibronectin adhered both to the anterior (color plate: Fig.17, VI: Fig. 4B1, 4B2) and posterior surfaces. Figures 3 and 4 in paper VI show thedifferent fibronectin adhesion patterns; for example, more fibronectin was attached to theanterior surface of the acrylate IOLs than to silicone IOLs.
Silicone IOLs had fewer cells on the surface than PMMA or acrylate IOLs (VI: Tables1-5). The acrylate IOL optic-haptic junction design allowed cells to grow inside the opticalong the haptic insertion, and the cell count was 4 in this area for acrylate IOLs. Most

59
cells on all the lenses had the appearance of LECs. There was fibronectin activity withinthe cells of 1 of the 5 PMMA IOLs, but none with the silicone IOLs. There wasfibronectin activity within the cells of 4 of the 5 acrylate IOLs (VI: Table 1).
Because of the large amounts of vitronectin observed on the first acrylate IOL, anadditional acrylate IOL was assessed. It also had large amounts of vitronectin (color plate:Fig. 18, VI: Fig. 5A-5D). To verify this adhesion pattern, 2 additional acrylate IOLs wereincubated with the primary antibody at 37°C. Similar results were obtained at this higherincubation temperature. Staining for vitronectin on the surfaces of acrylate IOLs washindered in 2 lenses when they were incubated in a mixture of purified human vitronectinand vitronectin antibody at a dilution of 5:1.
Minimal amounts of laminin were attached to PMMA and acrylate IOLs. The siliconeIOL had no laminin on its surface (VI: Table 3).
There was little adhesion of collagen IV to PMMA (VI: Fig. 6A) and acrylate IOLs(VI: Fig. 6B), and moderate adhesion to the silicone IOL (color plate: Fig. 19, VI: Fig.6C-6D). Therefore, one additional silicone IOL was analyzed for collagen type IV; moresurface collagen adhesion was found than on the first IOL. Collagen type IV activity wasalso seen within the cells on the silicone and acrylate IOLs (VI: Table 4). The differentcollagen adhesion pattern can be seen in paper VI, Fig. 6 and the relationships of theseproteins and different IOL materials, in paper VI, Fig. 2.
In one eye with an acrylate IOL, the capsulorhexis edges extended over and coveredpart of the IOL optic surface (color plate: Fig. 20, VI: Fig. 7A). The anterior capsule wasexplanted and cut in half, with one analyzed for fibronectin and the other for vitronectin.Large amounts of vitronectin were seen only in the area where the capsule covered theIOL optic surface (color plate: Fig 20, VI: Fig. 7B-7D). In contrast, large amounts offibronectin were seen in the area of the IOL optic and more peripherally, outside of theoptic, in the area of anterior and posterior capsule fusion (color plate: Fig. 20, VI: Fig.7E-7F).
In conclusion, hydrophobic soft acrylate IOLs had significantly more fibronectinadhering to their surfaces than PMMA and silicone IOLs, as well as more vitronectin.Silicone IOLs had more collagen type IV adhesion to their surfaces than the other IOLs.Collective protein adhesion differed significantly between soft acrylate and PMMA orsilicone, but not between PMMA and silicone. The greater amount of protein on thehydrophobic soft acrylate IOLs seems to support an adhesive mechanism for theirattachment to the capsular bag. Fibronectin and vitronectin have functional domains thatbind them to the lens epithelial cells and the collagenous capsule. The role of theseproteins is covered further in the Discussion.

6 Discussion
6.1 Bioactive bonding of different keratoprosthesis materials to tissues
One of the current problems with keratoprostheses is the ingrowth of epithelium betweenthe corneal stroma and the prosthesis material into the anterior chamber. Epitheliumopens a canal for infections, causes the extrusion of the prosthesis, produces a retroprosthetic membrane and induces secondary glaucoma by growing into the chamberangle. These complications are caused mostly by insufficient attachment of the prosthesisto the corneal tissue. It is not enough to have a material with good biocompatibility;bioactive behavior in the tissue is also needed. The attachment needs to be a true tissuegrowth together with the prosthesis, which could be called a bioactive type of attachment.Problems related to various keratoprostheses have led to the search for more suitablematerials.
The keratoprosthesis consists of an optic part and an anchoring flange, which holds theprosthesis in the corneal tissue. Several materials for the keratoprosthesis flange havebeen tried: acrylate (Cardona 1962), poly (methylmetacrylate) (PMMA) (Cardona 1962,Dohlman et al. 1974, Choyce 1977, Girard et al.1977, Gullapalli et al. 1979, Aquavella1983, Cardona 1983, Girard 1983, Sletteberg et al. 1990a and 1990b), Dacron, Teflon,siliconized Teflon, Silastic, fiberglass, nylon, cellulose (Cardona 1967), Dacron tissuecolonisable keratoprosthesis (Pintucci et al. 1995), aluminium oxide ceramic (Al2O3)(Heimke & Polack 1980, Polack 1983), a vitreous carbon-Teflon, fluorocarbon polymer(Proplast) (Barber et al. 1980, Barber 1988, White & Gona 1988), carbon fibers fixedwith silicone optic (Kain 1990), poly (2-hydroxyethyl methacrylate)=PHEMA (Mester etal. 1978), platinum (Cuperus et al. 1989), collagen-coated PMMA (Kirkham & Dangel,1991), fluorocarbon polymers (Impra and Gore-tex)(Legeais et al. 1992), biocolonizablemicroporous fluorocarbon (Legeais et al. 1995) and glass-ceramic (Bioverit)(Krause,1992). Blenke was the first to suggest glass-ceramic for the keratoprosthesis material(Blenke et al. 1978). Yakimenko (1993) has used a PMMA-optic with a tantalum-titanium alloy haptic. Strampelli and Marchi (1970), and after them some others, seem tohave been successful in achieving long-term attachment to the corneal tissue by using anosteo-odonto-keratoprosthesis. However, this three-stage-operation is difficult andrequires the use of the patient's own tooth.

61
Our study demonstrated the possibility of obtaining a bioactive kind of attachmentwith both titanium and glass-ceramic coated titanium keratoprostheses to the cornealtissue (I). All 11 titanium prostheses were retained for the time period planned. Twoglass-ceramic coated prostheses were lost at 2 and 4 weeks, respectively. This was causedby difficulties at surgery due to the glass-ceramic coating being too thick. These eyeswere excluded from the histologic analysis. No significant ingrowth of epithelium wasseen in 15/18 (83 %) and in 16/22 (73 %) of the analyzed areas of the glass-ceramiccoated and titanium prostheses, respectively. Our results agree with Yakimenko�s results(1993) for the titanium prosthesis. In our study the results were even better when thetitanium prosthesis had a glass-ceramic coating. In a clinical study with a PMMAkeratoprostheses, extrusion, leakage, retro-prosthetic membrane or endophthalmitisoccurred in 34 % of the eyes of 124 patients (Girard 1983). Furthermore, retinaldetachment was observed in 20 % and conjunctival retraction or scleral erosion in 48 %of the eyes. In our study (I), all three PMMA prostheses were found to be mobile at thetime of sacrifice, and in histologic analyses they were found to have epithelial ingrowtharound the whole implant. The epithelial cell layer was seen to be several cells thick, andthere was quite an intense inflammatory reaction around the prosthesis. No type ofbioactive attachment was seen with the PMMA prostheses. By increasing the bioactivityof the prosthesis by coating the prosthesis with glass-ceramic, a better attachment tocorneal tissue was achieved.
6.2 Sandwich theory
The sandwich theory related to PCO formation is based on the following assumptions: 1)Epithelial ingrowth can be hindered by bioactive bonding between the implant and thecorneal cells, as shown in the keratoprosthesis study. 2) The IOL can be biocompatible ina bioinert or bioactive way. 3) A clinically clear posterior capsule can have a monolayerof epithelial cells on it. According to the theory, an IOL made of bioactive material wouldallow a single lens epithelial cell to bond both to the IOL and the posterior capsule at thesame time. This would produce a sandwich pattern including the IOL, the cell monolayerand the posterior capsule. The sealed sandwich structure would prevent further epithelialingrowth. The degree of bioactivity of the IOL could explain the basic difference in PCOand Nd: YAG rates with different IOL materials.
Thus, the sandwich theory (II) takes into account two characteristics the IOL shouldhave to hinder posterior capsule opacification. Firstly, the square edge is needed to hinderlens epithelial cell ingrowth or direct the LECs to grow as a monolayer between thecapsule and the IOL surface. Secondly, the material has to be bioactive, i.e. it has to havethe ability to attach the growing LEC layer to the capsule and the surface of the IOL at thesame time. This kind of bioactive bonding then hinders further cell growth because everycell has a biological attachment on both sides.
The basic idea for the theory was obtained during a study with silicone IOLs (Linnola& Holst 1998) in which the patients were examined with dilated pupils one day, oneweek, 1, 6, and 12 months postoperatively. After only one month, cell growth could beseen between the posterior surface of the silicone IOL and the posterior capsule. At the

62
same time, eyes implanted with AcrySof (Alcon) IOLs had no cell growth on theposterior capsule and clear posterior capsules. This brought about the idea of a bioactiveattachment of the capsule and the LECs to the IOLs, as had been the case withkeratoprostheses with a glass-ceramic coating (I). The beneficial effect of the square edgecan be seen in the histologic pictures of the present study (color plate: Fig. 21-23, IV: Fig.4-6) and in other studies (Oshika et al. 1998, Nishi et al. 1998a, Nishi & Nishi 1999, Penget al. 2000, Kruger et al. 2000, Nishi et al. 2000).
The square edge of the optic cannot alone explain the adhesion of the anterior capsuleto the AcrySof (Alcon) IOLs� anterior surface as seen in studies IV and V. A tightadhesion of the anterior and posterior capsules to the IOL was seen with no cells (IV).Other studies have found less movement of the anterior capsule with AcrySof (Alcon)IOLs than with silicone and PMMA IOLs (Ursell et al. 1997, Cochener 1999). With nomovement, there has to be adhesion between the capsule and the IOL. We could see theanterior capsule attached to the AcrySof IOLs with only a layer of fibronectin or with asingle layer of LECs (IV&V) as is proposed in the sandwich theory. Direct attachment oran attachment with a one layer of LECs also produces less anterior capsule opacification,as was seen in a study by Werner et al. (2000). Indirect evidence for the meaning of noanterior capsule attachment and more movement comes from silicone IOLs. Anteriorcapsule contraction requiring Nd: YAG anterior capsulotomy with silicone IOLs has beenreported in normal eyes, and the risk for contraction was greater in eyes withpseudoexfoliation syndrome (Toldos et al. 1996, Dahlhauser et al. 1998). We did not seedirect attachment of silicone IOLs to the anterior or posterior capsules, but there wasmore fibrocellular tissue between the capsule and the IOL (V). Werner et al. (2000)reported this same growth pattern with silicone IOLs.
Together, the square edge and IOL material behavior could explain the significantdifferences in Nd: YAG rates with acrylate, PMMA and silicone IOLs (Table 1). Recentstudies with more accurate methods to evaluate PCO with the retroillumination (Hollicket al. 1999b) or EPCO methods (Auffarth 2000) have confirmed this difference. Theseresults indicate that PCO can be hindered with an IOL with a biological adhesion to LECsand the capsule. Previously researchers have coated the IOL with different materials toproduce a surface that would have minimal adherence to cells or the capsule (Larsson etal. 1989, Ygge et al. 1990, Miyake & Maekubo 1991a, Umezawa & Shimizu 1993,Boulton et al. 1994, Chollet et al. 1996, Werner et al. 1997) or the adhesion has beenhindered by blocking LEC adhesion molecules, inhibiting their attachment to the capsule(Humphry et al. 1988, Nishi et al. 1996d, Nishi et al. 1997b). Of these, only heparincoated PMMA IOLs have been in broad clinical use. Although heparin on an IOL surfacedecreases the amount of cell attachment to its surface, difference in PCO between PMMAand HSM-PMMA IOL materials have not been found (Winther-Nielsen et al. 1998). Withno adhesion of the IOL material to the capsule or the LECs, there is a free growth of thesecells and production of extracellular matrix proteins resulting in PCO.
Further studies on the importance of IOL material versus the square edge model areunderway. Also, further studies have revealed, that there are significant differencesbetween soft acrylate IOLs in fibronectin adhesion, according to if the acrylate material ishydrophilic or hydrophobic in character (Linnola et. al, unpublished data).

63
6.3 Cell and tissue reactions and adhesion to different IOL materials
We could see a bioactive kind of bonding of rabbit corneal tissue to soft, hydrophobicacrylate AcrySof (Alcon) IOLs (III). When grown on PMMA, HSM-PMMA, silicone,and hydrogel, the corneal tissue did not attach to the IOL or the epithelium grew aroundthe explant, suggesting that the attachment of the corneal stroma to the IOL was poor ornonexistent. The culture time was one week. This was enough for corneal epithelium togrow around the tissue block, if the IOL-tissue attachment was not tight enough to hinderepithelial growth. Some in vitro studies suggest that this kind of attachment does not haveto be biologically mediated, but caused by the IOL surface properties only (Nagata et al.1998). Oshika et al. (1998) showed in their in vitro study, that AcrySof IOLs adheredbetter to a collagen sheet than PMMA IOLs, and silicone IOLs showed no adhesiveness.In their study, the adhesive force to collagen type I sheet was 1697 mg for acrylatefoldable, 583 mg for PMMA, and 0 mg for silicone IOLs. Adhesion force of the IOL torabbit posterior capsule 3 weeks after implantation, as measured by scores (0-5), was 4.5for acrylic, 3.0 for PMMA and 0.40 for silicone. These studies show that the difference inadhesive force between acrylate and PMMA was 2.9x in vitro, and only 1.5x in vivo.However, because collagen type I belongs to a fibril-forming class of collagen�s, and thelens capsular bag is mostly made of collagen type IV, which belongs to a network-likeclass of collagens (Prockop & Kivirikko 1995), these in vitro results need to be confirmedwith collagen type IV. With all specimens in our study (V), there was no adhesion of thesoft acrylic IOL to the capsule without extracellular matrix proteins, which speaks againstthe direct adhesion of the material itself to the capsule.
Significantly more cells were attached to the surfaces of soft, hydrophobic AcrySof(Alcon) IOLs than to PMMA and silicone IOLs (VI). Silicone IOLs had fewer cells onthe surface than PMMA or acrylate IOLs. The acrylate IOL optic-haptic junction designallowed cells to grow inside the optic along the haptic insertion, and the cell count washigher in this area for acrylate IOLs. Most cells on all the lenses had the appearance ofLECs. There was fibronectin activity within the cells on 1 of the 5 PMMA IOLs, but nonewith the silicone IOLs. Again, there was fibronectin activity within the cells on 4 of the 5acrylate IOLs (VI). This suggests that they had already changed into fibroblasts, becausein this form they are able to produce fibronectin as Saika et al. (1995) have shown.Tamada & Ikada (1994) found that fibroblasts could proliferate at the highest rate, andshowed the highest-order morphology, when cultured on a substrate with a contact anglearound 70°, which was also most favorable for cell adhesion. Therefore, different contactangles between IOL materials can partly explain our results (III, V & VI). Contact anglesmeasured with a sessile drop method for three different silicone IOLs were 109.8°-116.7°;for PMMA 68.1°, for hydrophobic, soft acrylate 87.6° (Allergan Medical Optics Sensar®AR40), and for hydrophobic, soft acrylate 72.7° (Alcon AcrySof® MA60BM) (Cunananet al. 1998). Soft hydrophobic acrylate (AcrySof) IOLs seem to be a material with asuitable contact angle for cell adhesion, and to have a good adsorption capacity forfibronectin, which in turn promotes LEC adhesion.

64
6.4 Extracellular matrix proteins with different IOL materials in vitro and in vivo
6.4.1 Fibronectin
Fibronectin is a major glycoprotein of the extracellular matrix that is also found insoluble form in plasma (Saika et al. 1997b). It is also produced by LECs that havetransformed into fibroblasts, and by macrophages during inflammation. Fibronectin hasseveral functional domains, two of which are for binding it to collagen and to the cellsurface (Murray & Keeley 1996). As the lens capsule is made of collagen, fibronectincould be a mediator for adhesion between the IOL and the capsule.
The presence of fibronectin attached to the IOLs, or in the fibrocellular tissueresponsible for the posterior capsule opacification after cataract surgery, has beenpreviously shown (Kappelhof et al. 1986, Kanagawa et al. 1990, Boyd et al. 1992,Kochounian et al. 1994, Saika et al. 1993, Saika et al. 1995, Saika et al. 1997a, Saika etal. 1997b, Saika et al. 1998c). Our studies (V & VI) confirm these previous findings withPMMA and silicone IOLs, and we were the first to report an association of fibronectinwith hydrogel and soft hydrophobic acrylate IOLs. Fibronectin was found in the layerimmediately against the IOL surface, both with PMMA and acrylate IOLs, suggestingthat the protein plays a more important role than other extracellular proteins in the IOL�capsular bag attachment. However, the PMMA IOLs had more fibrotic tissue and celllayers than the acrylate IOLs. Many sections of the acrylate IOLs were directly attachedto the capsular bag by a layer of fibronectin, or with one layer of LECs and fibronectin.Our results also suggest that the adhesion of fibronectin might be stronger and faster toacrylate than to PMMA. If the capsule was attached by fibronectin without cells, thisindicates that the attachment occurred before LEC proliferation. Therefore our study alsosuggests a time frame for fibronectin-mediated adhesion. Lens epithelial cells in capsularbags from cadaver eyes produced a confluent monolayer over the posterior capsule after5.8-7.2 days in culture (Liu et al. 1996). With no cells, fibronectin adhesion should haveoccurred earlier. In areas with no cells, the origin of fibronectin between the capsule andthe IOL must be from the aqueous humor directly (Kim et al. 1992, Vesaluoma et al.1998) or from the blood after breakdown of the blood-aqueous barrier. The highest valuesmeasured by laser flare- cell photometry were 6 hours after the operation (Dick et al.2000). This means that fibronectin, together with other proteins, are available soon afterthe operation. Because fibronectin activity was seen inside LECs in our studies, thissuggests that these cells might be able to produce fibronectin themselves (V & VI). Themonoclonal anti-fibronectin antibody used (V & VI) reacts both with the cellular- as wellas plasma-derived form of fibronectin, and therefore we were not able to differentiate theorigin of fibronectin directly. Johnston et al. (1999) found better surface adsorption offibronectin to a hydrophobic soft acrylate IOL than to a PMMA IOL in vitro, and theyfound this difference to be significant when measured after one day, and after one week.We confirmed better adsorption of fibronectin to hydrophobic soft acrylate IOLs than toPMMA IOLs in vitro, although the difference was not significant (IV). Significantly morefibronectin was attached to acrylate than to silicone, HSM-PMMA or hydrogel IOLs (IV).After fibronectin adhesion to the IOL surface, fibronectin can promote LEC migration

65
(Olivero & Furcht 1993). The two main adhesion domains of fibronectin are for collagenand the cell surface (Murray & Keeley 1996). The lens capsule is made of collagen; thus,fibronectin could be a mediator for adhesion between an IOL and the capsule. Our studysupports this hypothesis; we found that fibronectin was a mediator between LECs and theIOL surface. A sandwich-like structure (anterior or posterior capsule/fibronectin/one celllayer/fibronectin/IOL surface) was seen significantly more often with soft acrylate IOLsthan with PMMA, silicone or hydrogel IOLs (V). These findings support the sandwichtheory and suggest a bioactive kind of attachment of soft hydrophobic acrylate(AcrySof) IOLs to the LECs and the capsular bag.
6.4.2 Vitronectin
Vitronectin is another major glycoprotein involved in cell adhesion. It was studiedbecause of its ability to attach to collagen IV; the material of the capsular bag, and ittherefore could be a mediator in adhesion between the IOL and the LECs or the capsularbag. Most vitronectin is produced in the liver (Seiffert 1997a, Seiffert & Smith 1997b,Yoneda et al. 1998), and therefore is available to contribute to IOL adhesion after BABbreakdown associated with cataract surgery.
Saika et al. (1995) reported finding vitronectin in granular and membranous depositson explanted PMMA IOLs. There are no other reports of vitronectin associated withIOLs. Our study is the first to report an association of vitronectin with silicone, hydrogel,and soft hydrophobic acrylate (AcrySof) IOLs (V & VI). We found more vitronectin onthe surface of soft hydrophobic acrylate IOL surfaces than on silicone and PMMA IOLs.There was vitronectin activity in the cells on the acrylate IOL anterior surface (VI). Thesecells looked like LECs, but without immunohistochemical confirmation we were not ableto say if these vitronectin producing cells were LECs or macrophages. We foundvitronectin in the capsular bag in the fibrocellular tissue under the anterior capsule, theoptic edge area, and over the posterior capsule, but not directly next to the IOLs (V). Thissuggests that vitronectin is probably not responsible for the adhesion of IOLs to thecapsular bag. There was a large accumulation of vitronectin near the Nd: YAG opening ofone IOL (V), confirming its association with tissue injury (Seiffert & Smith 1997b).Immunohistochemical assessment of the capsular bag from one acrylate IOL sectionshowed that vitronectin was associated with the area where the IOL optic was in contactwith the capsular bag (VI). In this case, the entire capsule was stained; making itimpossible to determine the specific tissue level at which vitronectin staining occurred.No vitronectin was observed outside the optic area. In contrast, fibronectin was found inthe area of the optic contact with the capsular bag, and the area of fusion between theanterior and posterior capsules, peripheral to the optic. This suggests the 2 proteins playdifferent roles. Fibronectin was present in all areas of the specimens, indicating that it ispart of the normal healing process.

66
6.4.3 Laminin
Laminin is another extracellular glycoprotein, and it promotes cell attachment, spreading,motility, neurite outgrowth, as well as cell proliferation and differentiation (Engvall et al.1990). It has binding sites for collagen type IV and cell surfaces (Murray & Keeler 1996).In the present study we tried to elucidate its role in IOL adhesion to the capsular bag.
Only one study has previously reported the presence of laminin together with IOLs(Saika et al. 1998c). They found laminin activity in the LECs attached to the anteriorcapsule obtained from cataract surgery. Postoperatively, laminin activity was seen in theposterior capsule and around the cells in fibrocellular tissue. In contrast, we did not findany laminin in the anterior or posterior capsules (V). We evaluated first the adhesion ofsoluble laminin to poly (methyl methacrylate) [PMMA], heparin-surface-modifiedPMMA (HSM-PMMA), silicone, acrylate and hydrogel IOLs in vitro (IV). HydrogelIOLs (Hydroview) showed the highest binding of laminin, with significant differencesrelative to acrylate, PMMA, silicone, and HSM-PMMA. In histological sections lamininwas seen mostly in the fibrotic tissues on the inner surface of the anterior capsule and theoptic edge of the IOL (V). Laminin was not present between the fibrotic tissue and theIOL, and therefore did not seem to be related to the direct attachment of the IOL materialto the capsular bag. It seemed primarily to be involved in the healing process after IOLimplantation. Laminin adhesion was minimal on explanted IOLs (VI), with no differencesamong IOL materials. However, only one IOL of each material was evaluated forlaminin. This protein was also found in the LEC cytoplasm, suggesting that cells on thePMMA, acrylate and hydrogel IOL surfaces might produce laminin. There were no cellson the silicone IOL; thus, no conclusions were reached regarding laminin activity onthese IOLs.
Laminin has been shown to promote LEC adhesion and migration in cell culture(Olivero & Furcht 1993). As we saw more laminin adhesion to hydrogel IOLs (VI),laminin may have a role in the more aggressive LEC growth over the hydrogel IOLanterior surface after cataract surgery as reported by Hollick et al. (1999a). Laminin wasshown to reappear later (2-4 weeks) than fibronectin (8 hours) after keratectomy(Fujikawa et al. 1984). Therefore the action of laminin is too slow in hindering PCO byattaching the LECs or the IOL to the capsular bag. During that time LEC proliferationbetween the posterior capsule and the IOL would produce PCO. No free soluble lamininavailable has been reported in the anterior chamber after surgery.
6.4.4 Collagen type IV
Of the 19 collagen types, collagen types I, III, IV, V and VI have been found associatedwith the extracellular matrix in fibrotic tissue of PCO: collagen (Ishibashi et al. 1995),collagen type I (Saika et al. 1992, Ishibashi et al. 1994, Saika et al. 1995, Saika et al.1997a, Saika et al. 1997b, Saika et al. 1998c), collagen type III (Ishibashi et al. 1994,Saika et al. 1995, Saika et al. 1997a, Saika et al. 1997b, Saika et al. 1998c), collagen typeIV (Ishibashi et al. 1994, Saika et al. 1998c), collagen type V and VI (Saika et al. 1998c).Collagen types I, II and V belong to fibril forming, IV to network-like, and VI to the

67
beaded filaments class of collagens. We found collagen type IV to be present in largeamounts in fibrocellular tissues of ACO and PCO, and in the capsular bag (V & VI). Thisagrees with findings of previous studies (Ishibashi et al. 1994, Saika et al. 1998c). LECsare capable of producing collagen (Laurent et al. 1981). We could confirm that LECs onthe silicone and acrylate IOL surfaces contained collagen type IV (VI), and in histologicsections collagen activity was seen in LECs on PMMA, acrylate, silicone, and hydrogelIOLs (V). This may indicate production of this collagen in LEC.
In vitro, hydrogel IOLs had significantly higher binding of type IV collagen thanPMMA, HSM-PMMA, acrylate and silicone (IV). In vivo we saw significantly morecollagen type IV attached to silicone than to PMMA or acrylate IOLs. The small numberof hydrogel IOLs available did not allow statistical comparison between them andPMMA, acrylate and silicone IOLs. We saw thicker fibrocellular tissue with LECs andextracellular matrix proteins between the anterior and posterior capsules and silicone IOLsurfaces (V). This tissue was lined with collagen type IV against the silicone IOL surface,just as the IOL had been encapsulated with this tissue. Tamada & Ikada (1994) found, thatcollagen synthesis per cell was more active on the surfaces less favorable for cell growththan on the good ones. This agrees with our study (V & VI), where silicone IOL surfacewith a contact angle far from optimal for cell attachment were seen to produce morefibrocellular tissue with collagen type IV. Our study suggests that fibronectin mediatesbetter attachment than collagen type IV for the following reasons: (1) the anterior capsulemoves more over silicone IOLs than over acrylate IOLs (Ursell et al. 1997, Hayashi et al.1997 and Cochener et al. 1999); (2) we found collagen type IV lining the fibrocellulartissue that was against the silicone surface, and the fibronectin that was against theacrylate IOL surface (V & VI). Although collagen and fibronectin are both extracellularmatrix components, they are classified in different groups. Collagen is more stable, and isin the structural proteins group. Fibronectin is among the specialized proteins involved incell adhesion and migration (Murray & Keeley 1996).

7 Summary and conclusions
This report consists of series of studies with animal experiments, in vitro intraocular lensstudies, and studies with pseudophakic human autopsy eyes. Assessment of titanium andbioactive glass-ceramic coated titanium as materials for keratoprosthesis was a co-operative study with the Department of Ophthalmology, University of Oulu and theDepartment of Prosthetics, Institute of Dentistry, University of Turku. This study wasdone at a time when most IOLs were made of PMMA. We could see that akeratoprosthesis made of PMMA did not attach to the corneal stromal tissue. After ourown clinical experience, and successful clinical reports with soft hydrophobic acrylateIOLs, the latter studies were started to discover the possible reasons for less PCO beingassociated with IOLs made of this material. The sandwich theory as an explanation forvariable PCO formation with different IOLs was presented in 1996. It connects the resultsfrom the keratoprosthesis study and the clinical behavior of soft hydrophobic acrylateIOLs. The intraocular lens bioactivity of different IOL materials was tested with rabbitcorneal tissue cultures in the Department of Oral and Maxillofacial Surgery, Institute ofDentistry, University of Turku. Better adhesion of tissue was associated with softhydrophobic acrylate IOLs. Extracellular matrix protein adhesion to IOLs was studiedwith a radioactive iodine labeling method performed at the Collagen Research Unit,Biocenter and the Department of Medical Biochemistry, University of Oulu. The role offibronectin, vitronectin, laminin and collagen type IV was finally analyzed inpseudophakic human autopsy eyes. This part of the study was done at the Center forResearch on Ocular Therapeutics and Biodevices, Storm Eye Institute, MedicalUniversity of South Carolina, Charleston, USA. The main results and conclusions of allof the studies are as follows:1. A bioactive type of bonding of keratoprosthesis material to corneal stromal tissue was
obtained with bioactive glass-ceramic coated titanium. Bioinert titanium alsomanaged well, but when histologic findings were considered, bioactive glass-coatedprostheses were shown to have a better bioactive attachment with less epithelialingrowth. Prostheses made of PMMA did not show any attachment at all to thecorneal stromal tissue. After only one month, they were totally surrounded byepithelial ingrowth.

69
2. For an IOL with a suitable amount of bioactivity, the sandwich theory of PCOformation was created: A continuous curvilinear capsulorhexis is performed duringcataract surgery. The anterior capsule over the IOL bonds directly, or as a result of theremaining LECs, to the IOL�s bioactive surface, preventing further LEC proliferation.Thus, the anterior capsule over the IOL remains clear. When this bonding is complete,the IOL and the capsular bag are a closed system. Inside the bag, remaining LECsproliferate and migrate behind the IOL. The 90° edge of the IOL optic against theposterior capsule hinders or directs the proliferating LECs to form a monolayerbetween the IOL and the posterior capsule. Another bioactive bond is formed when asingle lens epithelial cell has the posterior capsule on one side and the bioactive IOLsurface on the other side. The sandwich is formed, and the cell-posterior capsule andthe cell-bioactive IOL surface junctions prevent more cells from migrating behind theIOL. The posterior capsule remains clear. After some time, some of the monolayercells will die because of aging, poor nutrition or the IOL-induced pressure on theposterior capsule.
3. Rabbit corneal tissue cultures were set up on poly (methyl methacrylate) (PMMA),heparin-surface-modified-PMMA (HSM-PMMA), silicone, acrylate and hydrogelIOLs for one week. The tissue consisted of intact epithelium and half of the thicknessof the corneal stroma, which was placed against the IOL. The growth of theepithelium was examined by light microscopy in order to evaluate the attachment ofthe explant to the IOL surface. When grown on PMMA, HSM-PMMA, silicone andhydrogel, the tissue did not attach to the IOL or the epithelium grew around theexplant suggesting that the attachment of the stroma to the IOL was poor, or did notexist. By contrast, some of the explants grown on acrylate IOLs (AcrySof) hadattached directly to the IOL surface with no epithelial ingrowth between the stromaand the IOL. The results suggested that acrylate IOLs might have bioactiveproperties.
4. In order to discover, if there are differences in extracellular matrix protein adhesion todifferent IOL materials, 75 intraocular lenses were incubated with radioactive iodine-labeled soluble fibronectin, laminin or collagen type IV. Twenty-five IOLs wereanalyzed for each protein; 5 each were made of PMMA, HSM-PMMA, silicone,acrylate and hydrogel. The amount of absorbed protein was measured with a gammacounter. Soft hydrophobic acrylate (AcrySof®) showed the highest binding offibronectin, the difference being significant relative to all the other materials exceptPMMA. Hydrogel (Hydroview) had the highest overall binding of laminin.Acrylate bound significantly more laminin than PMMA, HSM-PMMA or silicone.Hydrogel also showed significantly more binding of type IV collagen than any of theother IOLs.
5. Tight adhesion of anterior and posterior capsule to soft hydrophobic acrylate(AcrySof®) IOLs was seen in plastic embedded sections of a human pseudophakicautopsy eye. A structure as proposed in the sandwich theory was seen with amonolayer of lens epithelial cells. In the immunohistochemical part of the study,thirty-eight autopsy eyes containing PMMA, silicone, hydrophobic acrylate, orhydrogel IOLs were assessed. Histologic sections were prepared from each eye, andimmunohistochemical analyses were performed for fibronectin, vitronectin, lamininand collagen type IV. One hundred fifty-two specimens were analyzed. A sandwich-

70
like structure (anterior or posterior capsule/fibronectin/one cell layer/fibronectin/IOLsurface) was seen significantly more often with soft acrylate IOLs, than with PMMA,silicone, or hydrogel IOLs. The thicker fibrocellular tissue on the inner surface of theanterior or posterior capsule that was in contact with silicone IOLs was lined withcollagen type IV. Vitronectin and laminin were not found at the fibrocellular tissue-IOL interface of any specimen. When explanted IOLs from thirty-two human autopsyeyes were examined, a significant difference in protein adsorption was seen.Hydrophobic soft acrylate (AcrySof®) IOLs had significantly more fibronectinadhering to their surfaces than PMMA and silicone IOLs, as well as more vitronectin.Silicone IOLs had more collagen type IV adhesion than the other IOLs. Collectiveprotein adhesion differed significantly between soft acrylate and PMMA or silicone,but not between PMMA and silicone.
In conclusion, this study supports the sandwich theory of PCO formation and suggeststhat fibronectin plays a major role in adhesion of the IOL and the lens capsule. Ourfindings also show that fibronectin is the major extracellular protein between thehydrophobic soft acrylate (AcrySof®) IOL and the capsular bag. Because of the acceptedbiological role of fibronectin, it is likely to act as a true bioactive bond between the IOLand the LECs or capsular bag, which suggests a reason for the lower PCO and Nd: YAG-rates with an AcrySof® lens. The good results obtained with this IOL seem to be relatedto its optimal design with a square edge, its optimal material structure with a contactangle suitable for cell attachment, and good adhesion properties for maximal fibronectinadhesion to its surface.

71
Color plate 1-5
Fig. 2
Fig. 6.

72
Fig. 9. Fig. 10.
Fig. 11. Fig. 12.
Fig. 7. Fig. 8.

73
Ant. SurfacePost. SurfaceHaptic Area
Fig. 13.
Fig. 14.
Fig. 15.
Fig. 19.
Fig. 16.
Fig. 17.
Fig. 18.

74
Fig. 20.
F
DC
E
BA

75
Fig. 21.
Fig. 22.
Fig. 23.

76
Fig. 2. The sandwich theory: Phase 1. Schematic picture of an IOL with optic made of bioac-tive material in the capsular bag. The anterior capsule over the bioactive surface of the IOLbonds directly or through the remaining lens epithelial cells to the IOL. The IOL and the cap-sular bag have formed a closed system. Inside the bag the remaining lens epithelial cells prolif-erate and migrate behind the IOL. A 90° degree edge of the IOL optic against the posteriorcapsule can now direct the lens epithelial cells to proliferate as a monolayer of cells betweenthe IOL and the posterior capsule. Phase 2. The bioactive bond is formed when a single lensepithelial cell has the posterior capsule on one side and the bioactive IOL surface on the otherside. The sandwich is formed and the cell-posterior capsule junction and the cell-bioactiveIOL surface junction prevent more cells from migrating behind the IOL. The posterior cap-sule remains clear. Phase 3. After some time, a part of these monolayer cells die. The reasonmay be aging, lack of nutrition or the pressure of the IOL against the posterior capsule. A truecontact with the IOL and the posterior capsule is formed in these places.
Fig. 6. (Color plate: Fig. 6, V: Fig. 1) Immunohistochemical staining for fibronectin (redcolor). The Sandwich structure of the anterior capsule (*), fibronectin-LECs-fibronectin isseen with acrylate IOL No 7 (V). The last thin layer of extracellular matrix protein against theIOL is fibronectin (arrows) [original magnification x 400].
Fig. 7. (Color plate: Fig. 7) Histologic photograph of a rabbit cornea, two months after im-plantation with a keratoprosthesis supported by a bioactive glass-ceramic coated flange. Thetitanium flange (TF), the bioactive glass-ceramic coating (BCG), the corneal stroma (C) andthe epithelium (E) can be seen. The corneal epithelium has attached to the bioactive glass-ce-ramic coating and there is no ingrowth (original magnification x 32).
Fig. 8. (Color plate: Fig. 8, II: Fig. 1) Histologic photograph of a rabbit cornea with a PMMAkeratoprosthesis 1 month postoperatively. The empty space inside the cornea shows where theoptic part (O) and left side of the flange (F) have been. The prosthesis was removed during tis-sue processing. Arrows show epithelial ingrowth along the PMMA prosthesis. The bioinertPMMA did not hinder epithelial ingrowth (original magnification x 4).
Fig. 9. (Color plate: Fig. 9, V: Fig. 4) Immunohistochemical staining for fibronectin (redcolor). Photomicrograph showing the anterior capsule (*) of hydrophobic soft acrylate IOLNo 12 (V). Some LECs can be seen as a monolayer against the IOL anterior surface, but theIOL has been attached to the capsule primarily directly with fibronectin (arrows)[originalmagnification x 400].
Fig. 10. (Color plate: Fig. 10, V: Fig. 5) Immunohistochemical staining for fibronectin (redcolor). Photomicrograph showing the posterior capsule (**) of hydrophobic soft acrylate IOLNo 6 (V). The attachment has been mediated with fibronectin (arrows). Some LECs can beseen as a monolayer, and they are attached with fibronectin to the posterior IOL surface. TheIOL was dissolved during the preparation of the specimen (original magnification x 400).
Fig. 11. (Color plate: Fig. 11, V: Fig. 6) Immunohistochemical staining for fibronectin (redcolor). Photomicrograph showing hydrophobic soft acrylate IOL No 10 at the top, the posteri-or capsule (**), and fibronectin (arrows) on the posterior capsule (V). The fibronectin mem-brane over the posterior capsule was broken in some places by processing of the section (origi-nal magnification x 400).
Fig. 12. (Color plate: Fig. 12, V: Fig. 7) Immunohistochemical staining for fibronectin (redcolor). A thick layer of fibrocellular tissue can be seen lining the anterior (*) and posteriorcapsule (**). Multiple layers of LECs are attached to the posterior capsule and the posteriorsurface of poly(methyl methacrylate) [PMMA] IOL No 5 (V) with fibronectin (arrows)[origi-nal magnification x 200].
Fig. 13. (Color plate: Fig. 13, V: Fig. 9) Immunohistochemical staining of silicone IOL No 9(V) for collagen type IV (red color) shows intense reactivity for collagen type IV (arrows). The

77
fibrocellular tissue is lined with collagen type IV next to the IOL surface (original magnifica-tion x 200).
Fig. 14. (Color plate: Fig. 14, VI: Fig. 2) The relationships between protein adhesion and IOLmaterials. The anatomic locations examined were as follows: IOL anterior surface (red), IOLposterior surface (blue), and the haptic area (green). PMMA = poly (methyl methacrylate),and acrylate = hydrophobic soft acrylate.
Fig. 15. (Color plate: Fig. 15, VI: Fig. 3A1) Immunohistochemical staining for fibronectin (redcolor, arrows). Large amounts of fibronectin were attached to the anterior surface of acrylateIOL No. 1 (VI) at the area where the anterior capsule was in contact with the anterior IOLsurface (double-headed arrows) [original magnification x 40].
Fig. 16. (Color plate: Fig. 16, VI: Fig. 4A1) Immunohistochemical staining for fibronectin (redcolor, arrows). The posterior surface of silicone IOL No. 1 (VI) has only traces of fibronectinattached to the IOL surface (original magnification x 20).
Fig. 17. (Color plate: Fig. 17, VI: Fig. 4B1) Immunohistochemical staining for fibronectin (redcolor, arrows). The anterior surface of PMMA IOL No. 4 (VI) has minimal amounts of fi-bronectin attached to the IOL surface (original magnification x 20).
Fig. 18. (Color plate: Fig. 18, VI: Fig. 5D) Immunohistochemical staining for vitronectin (redcolor, arrows) on soft acrylate IOL No. 7 (V) (original magnification x 100). Large amounts ofvitronectin can be seen on the anterior IOL surface and the anterior surface of the IOL is par-tially coated with vitronectin. Note the square edge of the AcrySof® IOL.
Fig. 19. (Color plate: Fig. 19, VI: Fig. 6D) Immunohistochemical staining for collagen type IV(red color, arrows). Silicone IOL No. 8 (VI) has moderate amounts of collagen type IV at-tached to its surface, mostly at the lateral side of the IOL (original magnification x 100).
Fig. 20. (Color plate: Fig. 20, VI: Fig. 7) Gross photograph (anterior view) of soft acrylate IOLNo. 11 (V) in the capsular bag (A) [the IOL itself was quantitated for vitronectin, see paper VI,Table 2]. The right side of the capsular bag was assessed. Immunohistochemical staining of thecapsular bag for vitronectin (red color in figures B, C and D, arrows) shows that vitronectinreactivity is strictly related to the area covering the IOL optic (double-headed arrow in B).The rectangular area in B can be seen at higher magnification in C. The area where the hapticresided has a lens epithelial cell lining which can be seen in picture D (double headed arrow).Immunohistochemical staining of the capsular bag for fibronectin (red color in Fig. E and F,arrows) shows that fibronectin reactivity can be seen both in the area covering the IOL optic(double-headed arrow in E) and in the area of anterior and posterior capsule fusion. The rec-tangular area in E can be seen at higher magnification in F [B and E, original magnification x100; C and F, original magnification x 400; D, original magnification x 200].
Fig. 21. (Color plate: Fig. 21, IV: Fig. 4) AcrySof® IOL in the eye of a patient who died oneyear after implantation. The IOL is tightly attached to the anterior and posterior capsules.The iris is seen above (original magnification x 50).
Fig. 22. (Color plate: Fig. 22, IV: Fig. 5) A higher magnification of the IOL in Fig. 21. One lay-er of lens epithelial cells is interposed between the lens capsule and the IOL, and also at theside of the IOL. There are no cells beyond the square edge, between the posterior capsule andthe IOL (original magnification x 400).
Fig. 23. (Color plate: Fig. 23, IV: Fig. 6) A higher magnification of the IOL in Fig. 21. The IOL(above) and posterior capsule are tightly attached, with no lens epithelial cells (original magni-fication x 400).

References
Akahoshi T (1999) 10000 AcrySof implantation. Proc. ASCRS Symposium on Cataract, IOL and Re-fractive Surgery, Seattle, USA, Abstr. p 176.
Alio JL, Sayans JA & Chipont E (1996) Laser flare-cell measurement of inflammation after unevent-ful extracapsular cataract extraction and implantation of intraocular lens implantation. J CataractRefract Surg 22 (suppl 1): 775-779.
Alio JL, Sayans JA & Chipont E (1997) Flare-cell meter measurement of inflammation after unevent-ful cataract surgery with intraocular lens implantation. J Cataract Refract Surg 23: 935-939.
Alitalo K, Hovi T & Vaheri A (1980) Fibronectin is produced by human macrophages. J Exp Med151: 602-613.
Amon M & Menapace R (1993) Long-term results and biocompatibility of heparin-surface-modifiedintraocular lenses. J Cataract Refract Surg 19: 258-262.
Ambler JS & Constable IJ (1988) Retinal detachment following Nd: YAG capsulotomy. Aust NZ JOphthalmol 16: 337-341.
Apple DJ & Rabb MF (1998) Lens and pathology of intraocular lenses. In: Apple DJ & Rabb MF(eds) Ocular Pathology. Mosby, St. Louis, Missouri, p 175.
Aquavella JV (1983) Clinical experience with the Cardona keratoprosthesis. Cornea 2: 177-178.Aron-Rosa D, Griesmann J-C & Aron J-J (1981) Use of a pulse ND: YAG laser (picosecond) to open
the posterior lens capsule in traumatic cataract: a preliminary report. Ophthalmic Surg 12: 496-499.
Assia EI, Legler UFC, Merril C, Hicklin JC, Castaneda VE, Hoggatt JP, Wasserman D & Apple DJ(1993) Clinicopathologic study of the effect of radial tears and loop fixation on intraocular lensdecentration. Ophthalmology 100: 153-158
Auffarth GU, Wilcox BS, Sims JCR, McCabe C, Wesendahl TA & Apple DJ (1995) Analysis of 100explanted one-piece and three-piece silicone intraocular lenses. Ophthalmology 102: 1122-1150.
Auffarth GU (2000) Quantification of posterior capsule opacification in acrylic foldable lenses(AcrySof). Proc. XVIII Congress of the ESCRS, Brussels, Belgium, Abstr. p 90.
Badr IA, Hussain HM, Jabak M & Wagoner MD (1995) Extracapsular cataract extraction with orwithout posterior chamber intraocular lenses in eyes with cataract and high myopia. Ophthalmol-ogy 102: 1139-1143.
Barber JC, Feaster F & Priour D (1980) The acceptance of a vitreous carbon alloplastic material, Pro-plast, in the rabbit eye. Invest Ophthalmol Vis Sci 19: 182-191.
Barber JC (1988) Keratoprostheses: Past and present. Int Ophthalmol Clin 28: 103-109.Barnes PA & Rieckhoff KE (1968) Laser-induced underwater sparks. Appl Phys Letters 13: 282-284.Bath PE, Hoffer KJ, Aron-Rosa D & Dang Y (1987) Glare disability secondary to intraocular lens
damage. J Cataract Refract Surg 13: 309-313.Bell CE & Landt JA (1967) Laser-induced high-pressure shock waves in water. Appl Phys Letters
10: 46-48.

79
BenEzra D & Cohen E (1997) Posterior capsulotomy in pediatric cataract surgery. The necessity ofa choice. Ophthalmology 104: 2168-2174.
Blacharski PA & Newsome DA (1988) Bilateral macular holes after Nd: YAG laser posterior cap-sulotomy. Am J Ophthalmolol 105: 417-418.
Blencke B-A, Hagen P, Brömer H & Deutscher K (1978) Untersuchungen über die Verwendbarkeitvon Glaskeramiken zur Osteo-Odonto-Keratoplastik. Ophthalmologica 176: 105-112.
Born CP & Ryan DK (1990) Effect of intraocular lens optic design on posterior capsular opacifica-tion. J Cataract Refract Surg 16: 188-192.
Boulton M, Kelly SP, Moriarty P, Jarvis-Evans J & Rosen ES (1994) Cell attachment to standard andsurface-modified intraocular lenses. Eur J Implant Ref Surg 6: 190-194.
Boyd W, Peiffer RL, Siegal G, Eifrig DE (1992) Fibronectin as a component of pseudophakic acel-lular membranes. J Cataract Refract Surg 18: 180-183.
Brown DC, Grabow HB, Martin RG, Rowen SL, Shephard JR, Williamsson CH & Ziémba SL (1998)Staar Collamer intraocular lens: Clinical results from the Phase I FDA core study. J Cataract Re-fract Surg 24: 1032-1038.
Burgeson RE, Chiquet M, Deutzmann R, Ekblom P, Engel J, Kleinman H, Martin GR, Meneguzzi G,Paulsson M, Sanes J, Timpl R, Tryggvason K, Yamada Y & Yurchenco PD (1994) A new nomen-clature for the laminins. Matrix Bio; 14: 209-211.
Caporossi A, Casprini F, Tosi GT, Balestazzi A, Stumpo M & Toti P (1998) Histology of anteriorcapsule fibrosis following phacoemulsification. J Cataract Refract Surg 24: 1343-1346.
Cardona H (1962) Keratoprosthesis. Acrylic optical cylinder with supporting intralamellar plate. AmJ Ophthalmol 54: 284-294.
Cardona H (1967) Keratoprosthesis with a plastic fiber meshwork supporting plate. Am J Ophthalmol64: 228-233.
Cardona H (1983) Prostokeratoplasty. Cornea 2: 179-183.Chan RY & Emery JM (1984) Mitotic inhibitors in preventing posterior lens capsule opacification:
2.5 year follow-up. In: Emery JM & Jacobson AC (eds) Current Concepts in Cataract Surgery:Selected Proceedings of the Eight Biennial Cataract Surgical Congress. Mosby, St. Louis, Mis-souri, pp 303-312.
Chee S-P, Seng-Ei T, Sivakumar M & Tan DTH (1999) Postoperative inflammation: Extracapsularcataract extraction versus phacoemulsification. J Cataract Refract Surg 25: 1280-1285.
Chollet P, Malecaze F, Toan PLL, Lamche H & Arne JL (1996) Annexin V-coated intraocular lenses.J Cataract Refract Surg 22: 818-824.
Choyce DP (1977) The Choyce 2-piece perforating kerato-prosthesis: 107 cases 1967-1976. Ophthal-mic Surg 8: 117-216.
Chung HS, Lim SJ & Kim HB (2000) Effect of mitomycin-C on posterior capsule opacification inrabbit eyes. J Cataract Refract Surg 26: 1537-1542.
Clark DS, Emery JM, Munsell MF (1998) Inhibition of posterior capsule opacification with an im-munotoxin specific for lens epithelial cells: 24 months clinical results. J Cataract Refract Surg 24:1614-1620.
Clayman HM, Jaffe NS, Light DS, Jaffe MS & Cassady JC (1981) Intraocular lenses, axial length,and retinal detachment. Am J Ophthalmol 92: 778-780.
Curtin BJ (1985) Myopias: Basic Science and clinical management. Harper & Row, Philadelphia, PA,p 337.
Cochener B, Jacg P-L & Colin J (1999) Capsule contraction after continuous curvilinear capsulorhex-is: Poly (methyl methacrylate) versus silicone intraocular lenses. J Cataract Refract Surg 25: 1362-1369.
Colin J & Robinet A (1997) Clear lensectomy and implantation of a low-power posterior chamberintraocular lens for correction of high myopia. A four-year follow-up. Ophthalmology 104: 73-78.
Condon PI, Brancato R, Hayes P, Pouliquen Y, Saari KM & Wenzel M (1995) Heparin- surface-mod-ified IOLs compared with regular PMMA IOLs in patients with diabetes and/or glaucoma � 1 yearresults of a double-blind randomized multi-independent trial. Eur J Implant Ref Surg 7: 194-201.
Cortina P, Gomez-Lechon MJ, Navea A, Menezo JL, Terencio MC & Diaz-Llopis M (1997) Di-clofenac sodium and syklosporin A inhibit human lens epithelial cell proliferation in culture.Graefes Arch Clin Exp Ophthalmol 235: 180-185.

80
Coonan P, Fung WE, Webster RG Jr, Allen AW Jr., Abbott RL (1985) The incidence of retinal de-tachment following extracapsular cataract extraction; a ten-year study. Ophthalmology 92: 1096-1101.
Cumming JS (1993) Postoperative complications and uncorrected acuities after implantation of platehaptic silicone and three-piece silicone intraocular lenses. J Cataract Refract Surg 19: 263-273.
Cunanan CM, Ghazizadeh M, Buchen SY & Knight PM (1998) Contact-angle analysis of intraocularlenses. J Cataract Refract Surg 24: 341-351.
Cuperus PL, Jongebloed WL, van Andel P & Worst JGF (1989) Glass-metal keratoprosthesis: Lightand electron microscopical evaluation of experimental surgery on rabbit eyes. Docum Ophthalmol71: 29-47.
Dahlhauser KF, Wroblewski & Mader TH (1998) Anterior capsule contraction with foldable siliconeintraocular lenses. J Cataract Refract Surg 24: 1216-1219.
Dardenne M-U, Gerten G-J, Kokkas K & Kermani O (1989) Retrospective study of retinal detach-ment following neodymium: YAG laser posterior capsulotomy. J Cataract Refract Surg 15: 676-680.
Diacor (1990) Clinical Laboratory Examinations 1991. Otava, Helsinki, p 248.Dick B, Schwenn O & Pfeiffer N (1997) Schadensausmaß bei vershiedenen Intraokularlinsen durch
die Neodymium: YAG-Laser Behandlung-Eine experimentelle Studie. Klin Monatsbl Augen-heilkd 211: 263-271.
Dick B, Schwenn O, Stoffelns B & Pfeiffer N (1998) Späte Luxation einer Schiffenförnigen Silikon-linse in den Glaskörper nach Nd: YAG-Kapsulotomie. Ein Fallbericht. Ophthalmologe 95: 181-185.
Dick HB, Schwenn O, Krummenauer F, Krist R & Pfeiffer N (2000) Inflammation after sclerocornealversus clear corneal tunnel phacoemulsification. Ophthalmology 107: 241-247.
Dohlman CH, Sneider HA & Doane MG (1974) Prosthokeratoplasty. Am J Ophthalmol. 77: 694-700.Donath K & Breuner G (1982) A method for the study of undecalcified bones and teeth with attached
soft tissues. J Oral Pathol 11: 318-326.Downing JE (1986) Long-term discission rate after placing posterior chamber lenses with the convex
surface posterior. J Cataract Refract Surg 12: 651-654.Duncan G, Riach RA, Williams MR, Webb SF, Dawson AP & Reddan JR (1996) Calcium mobiliza-
tion modulates growth of lens cells. Cell Calcium 19: 83-89.Duncan G, Wormstone IM, Liu CSC, Marcantonio JM & Davies PD (1997) Thapsigargin-coated in-
traocular lenses inhibit human lens cell growth. Nature 3: 1026-1028.Duncker GIW, Westphalen S & Behrendt S (1995) Complications of silicone disc intraocular lenses.
J Cataract Refract Surg 21: 562-566.El-Maghraby AE, Marzouki A, Matleen TM, Souchek J & Karr MVD (1993) Reproducibility and va-
lidity of laser flare/cell meter measurements of intraocular inflammation. J Cataract Refract Surg19: 52-55.
Engvall E, Earwicker D, Haaparanta T, Ruoslahti E & Sanes JR (1990) Distribution and isolation offour laminin variants: tissue restricted distribution of heterotrimers assembled from five differentsubunits. Cell Regulation 1: 731-740.
Erie JC, Hardwig PW & Hodge DO (1998) Effect of intraocular lens design on neodymium: YAGlaser capsulotomy rates. J Cataract Refract Surg 24: 1239-1242.
Ernest P, Tipperman R, Eagle R, Kardasis C, Lavery K, Sensoli A & Rhem M (1998) Is there differ-ence in incision healing based on location? J Cataract Refract Surg 24: 482-486.
Ficker LA & Steele AD (1985) Complications of Nd: YAG laser posterior capsulotomy. Trans Oph-thalmolol Soc U.K. 104: 529-532.
Findl O, Drexler W, Menapace R, Georgopoulos M, Rainer G, Hitzenberger CK & Fercher AF (1999)Changes in intraocular lens position after neodymium: YAG capsulotomy. J Cataract Refract Surg25: 659-662.
Fourman S & Apisson J (1991) Late-onset elevation in intraocular pressure after Neodymium-YAGlaser posterior capsulotomy. Arch Ophthalmol 109: 511-513.
Fradin DW, Bloembergen N & Letellier JP (1973) Dependence of laser-induced breakdown fieldstrength on pulse duration. Appl Phys Letters 22: 635-637.

81
Fujikawa LS, Foster CS, Gipson IK & Colvin RB (1984) Basement membrane components in healingrabbit corneal epithelial wounds: Immunofluorescence and ultrastructural studies. J Cell Biol 98:128-138.
Gallagher SP & Pavilack MA (1999) Risk factors for anterior capsule contraction syndrome withpolypropylene or poly (methyl methacrylate) haptics. J Cataract Refract Surg 25: 1356-1361.
Gimbel HV & Neuhann T (1990) Development, advantages, and methods of continuous circular cap-sulorhexis technique. J Cataract Refract Surg 16: 31-37.
Gimbel HV (1996) Posterior capsulorhexis with optic capture in pediatric cataract and intraocularlens surgery. Ophthalmology 103: 1871-1875.
Gimbel HV (1997) Posterior continuous curvilinear capsulorhexis and optic capture of the intraocularlens to prevent secondary opacification in pediatric cataract surgery. J Cataract Refract Surg 199723 (suppl 1) 652-656.
Girard W, Hawkins RS, Nieves R, Borodofsky T & Grant G (1977) Keratoprosthesis: A 12 year fol-low-up. Trans Am Acad Ophthalmol Otolaryngol 83: 252-267.
Girard LJ (1983) Keratoprosthesis. Cornea 2: 207-224.Goins KM, Ortiz JR, Fulcher SFA, Handa JT, Jaffe GJ, Foulks GN & Cobo LM (1994) Inhibition of
proliferating lens epithelium with antitransferrin receptor immunotoxin. J Cataract Refract Surg20: 513-516.
Graycar JL, Miller DA, Arrick BA, Lyons RM, Moses HL & Derynck R (1989) Human transforminggrowth factor-β3: Recombinant expression, purification, and biological activities in comparisonwith transforming growth factor-β1and -β2. Mol Endocrinol 3: 1977-1986.
Gullapalli NR, Blatt HL & Aquavella JV (1979) Results of keratoprosthesis. Am J Ophthalmol 88:190-196.
Hansen TJ, Tyndall R & Soll DB (1987) Methotrexate-anticollagen conjugate inhibits in vitro lenscell outgrowth. Invest Ophthalmolol Vis Sci 28: 1206-1209.
Hara T, Azuma N, Chiba K, Ueda Y & Hara T (1992) Anterior capsule opacification after endocap-sular cataract surgery. Ophthalmic Surg 23: 94-98.
Hara T, Hara T, Sakanishi K & Yamada Y (1995) Efficacy of equator rings in an experimental rabbitstudy. Arch Ophthalmol 113: 1060-1065.
Hartmann C, Wiedemann P, Weller M, Pharmakakis N & Heimann K (1989) In vitro Veränderungendes Linsenepithels und Hornhautendothels durch das Zytostaticum Daunomycin. Fortschr Oph-thalmol 86: 167-171.
Hashizoe M, Hara T, Ogura Y, Sakanishi K, Honda T & Hara T (1998) Equator ring efficacy in main-taining capsular bag integrity and transparency after cataract removal in monkey eyes. GraefesArch Clin Exp Ophthalmol 236: 375-379.
Hayashi K, Hayashi H, Nakao F & Hayashi F (1997) Reduction in the area of the anterior capsuleopening after polymethylmethacrylate, silicone and soft acrylic intraocular lens implantation. AmJ Ophthalmol 123: 441-447.
Hayashi K, Hayashi H, Nakao F & Hayashi F (1998a) In vivo quantitative measurement of posteriorcapsule opacification after extracapsular cataract surgery. Am J Ophthalmol 125: 837-843.
Hayashi K, Hayashi H, Matsuo K, Nakao F & Hayashi F (1998b) Anterior capsule contraction andintraocular lens dislocation after implant surgery in eyes with retinitis pigmentosa. Ophthalmolo-gy 105: 1239-1243.
Hayashi H, Hayashi K, Nakao F & Hayashi F (1998) Quantitative comparison of posterior capsuleopacification after polymethylmethacrylate, silicone, and soft acrylic intraocular lens implanta-tion. Arch Ophthalmol 116: 1579-1582.
Health Care Financing Administration (2000) The 1998 Medicare Frequency Data tables. Washing-ton: U.S. department of health & human services.
Heimke G & Polack FM (1983) Ceramic keratoprosthesis: Biomechanics of extrusion in through-the-lid implantation. Cornea 2: 197-201.
Hetland G, Pettersen HB, Mollnes TE & Johnson E (1989) S-protein is synthesized by human mono-cytes and macrophages in vitro. Scand J Immunol 29: 15-21.
Hollick EJ, Spalton DJ, Ursell PG & Pande MV (1998) Biocompatibility of poly (methyl methacr-ylate, silicone, and AcrySof intraocular lenses: Randomized comparison of the cellular reactionon the anterior lens surface. J Cataract Refract Surg 24: 361-366.

82
Hollick EJ, Spalton DJ & Ursell PG (1999a) Surface cytologic features on intraocular lenses. Can in-creased biocompatibility have disadvantages? Arch Ophthalmol 117: 872-878.
Hollick EJ, Spalton DJ, Ursell PG, Pande MV, Barman SA, Boyce JF & Tilling K (1999b) The effectof polymethylmethacrylate, silicone, and polyacrylic intraocular lenses on posterior capsularopacification 3 years after cataract surgery. Ophthalmology 106: 49-55.
Humphry RC, Davies EG, Jacob TJC & Thompson GM (1988) The human anterior lens capsule � anattempted chemical debridement of epithelial cells by ethylenediaminetetracetic acid (EDTA) andtrypsin. Br J Ophthalmol 72: 406-408.
Hunold W, Wirtz M, Kreiner C, Greite JH & Kaden P (1991) Linsen-Epithel-Nekrose-Faktor (LENF)zur Nachstarverhütung. Fortschr Ophthalmol 88: 386-389.
Ibaraki N, Ohara K & Miyamoto T (1995) Membranous outgrowth suggesting lens epithelial cell pro-liferation in pseudophakic eyes. Am J Ophthalmol 119: 706-711.
Ishibashi T, Sugai S, Kubota T, Ohnishi Y & Inomata H (1989) Cytopathology of early cellular reac-tion on implant lenses in monkeys. A transmission electron microscopic study. Graefes Arch ClinExp Ophthalmol 227: 470-475.
Ishibashi T, Araki H, Sugai S, Tawara A, Ohnishi Y & Inomata H (1993) Anterior capsule opacifica-tion in monkey eyes with posterior chamber intraocular lenses. Arch Ophthalmol 111: 1685-1690.
Ishibashi T, Hatae T & Inomata H (1994) Collagen types in human posterior capsule opacification. JCataract Refract Surg 20: 643-646.
Ishibashi T, Araki H, Sugai S, Tawara A & Inomata H (1995) Detection of proteoglycans in humanposterior capsule opacification. Ophthalmic Res 27: 208-213.
Ismail MM, Alio JL & Moreno JMR (1996) Prevention of secondary cataract by antimitotic drugs:Experimental study. Ophthalmic Res 28: 64-49.
Jahn CE & Emke M (1996) Long-term elevation of intraocular pressure after Neodymium: Yag laserposterior capsulotomy. Ophthalmologica 210: 85-89.
Javitt JC, Vitale S, Canner JK, Krakauer H, McBean AM & Sommer A (1991) National outcomes ofcataract extraction I, Retinal detachment after inpatient surgery. Ophthalmology 98: 895-902.
Johnson N (2000) Hydroview® H60M intraocular lens European clinical trial. Proc. XVIII Congressof the ESCRS, Brussels, Belgium, Abstr. p 132.
Johnston RL, Spalton DJ, Hussain A & Marshall J (1999) In vitro protein adsorption to 2 intraocularlens materials. J Cataract Refract Surg 25: 1109-1115.
Kain HL (1990) Experimentelle und theoretische Studien. Ein neues Konzept zur Keratoprothese.Klin Mbl Augenheilkd 197: 386-392.
Kannus P, Jozsa L, Järvinen TAH, Järvinen TLN, Kvist M, Natri A & Järvinen M (1998) Locationand distribution of non-collagenous matrix proteins in musculoskeletal tissues of rat. HistochemJ 39: 799-810.
Kappelhof JP, Pameyer JH, De Jong PTVM, Jongkind JF & Vrensen GFJM (1986) The proteinaceouscoating and cytology of implant lenses in rabbits. Am J Ophthalmol 102: 750-758.
Kanagawa R, Saika S, Ohmi S, Tamura M & Nakao T (1990) Presence and distribution of fibronectinon the surface of implanted intraocular lenses in rabbits. Graefes Arch Clin Exp Ophthalmol 228:398-400.
Kelman CD (1967) Phaco-emulsification and aspiration: a new technique of cataract removal. Am JOphthalmol 64: 23-25.
Kent DG, Peng Q, Isaacs RT, Whiteside SB, Barker DL & Apple DJ (1997) Security of capsular fix-ation: Small-versus large-hole plate-haptic lenses. J Cataract Refract Surg 23: 1371-1375.
Kent DG, Peng Q, Isaacs RT, Whiteside SB, Barker DL & Apple DJ (1998) Mini-haptics to improvecapsular fixation of plate-haptic silicone intraocular lenses. J Cataract Refract Surg 24: 666-671.
Khan AJ & Percival PB (1999) 12 years results of a prospective trial comparing poly (methyl meth-acrylate) and poly (hydroxyethyl methacrylate) intraocular lenses. J Cataract Refract Surg 25:1404-1407.
Kim K, Lee B-H & Kim I-S (1992) The measurement of fibronectin concentration in human aqueoushumor. Korean J Ophthalmol 6: 1-5.
Kirkham SM & Dangel ME (1991) The keratoprosthesis: Improved biocompatibility through designand surface modification. Ophthalmic Surg 22: 455-461.

83
Kochounian HH, Kovacs SA, Sy J, Grubbs DE & Maxwell WA (1994) Identification of intraocularlens adsorbed proteins in mammalian in vitro and in vivo systems. Arch Ophthalmol 112: 395-401.
Kraff MC, Sanders DR, Jampol LM & Lieberman HL (1984) Effect of primary capsulotomy with ex-tracapsular surgery on the incidence of pseudophakic cystoid macular edema. Am J Ophthalmol98: 166-170.
Krause A (1992) Intracorneal biocompatibility of glass ceramics. Contactologia 14 E: 28-31.Krootila K (2000) Practice styles and preferences of Finnish cataract surgeons � 1999 survey. Proc.
XVIII Congress of the ESCRS, Brussels, Belgium, no abstr.Kruger AJ, Schauersberger J, Abela C, Schild G & Amon M (2000) Two years results: Sharp versus
rounded optic edges on silicone lenses. J Cataract RefractSurg 26: 566-570.Larsson R, Selen G, Björklund h & Fagerholm P (1989) Intraocular PMMA lenses modified with sur-
face-immobilized heparin: evaluation of biocompatibility in vitro and in vivo. Biomaterials 10:511-516.
Latz C, Migonney V, Pavon-Djavid G, Rieck P, Hartmann C, Renard G & Legeais J-M (2000) Inhi-bition of lens epithelial cell proliferation by substituted PMMA intraocular lenses. Graefes ArchClin Exp Ophthalmol 238: 697-700.
Laurent M, Kern P, Courtois Y & Regnault F (1981) Synthesis of types I, III and IV collagen by bo-vine lens epithelial cells in long-term culture. Exp Cell Res 134: 23-31.
Legeais J-M, Rossi C, Renard G, Salvoldelli M, D Hermies F & Pouliquen YJ (1992) A new fluoro-carbon for keratoprosthesis. Cornea 11: 538-545.
Legeais J-M, Renard G, Parel J-M, Savoldelli M & Pouliquen Y (1995) Keratoprosthesis with bio-colonizable microporous fluorocarbon haptic. Arch Ophtalmol 113: 757-763.
Legler UFC, Assia EI, Castaneda VE, Hoggatt JP & Apple DJ (1992) Prospective experimental studyof factors related to posterior chamber intraocular lens decentration. J Cataract Refract Surg 1992;18: 449-455.
Legler UFC, Apple DJ, Assia EI, Bluestein EC, Castaneda VE & Mowbray SL (1993) Inhibition ofposterior capsule opacification: The effect of colchicine in a sustained drug delivery system. J Cat-aract Refract Surg 19: 462-470.
Levy JH, Pisacano AM & Anello RD (1990) Displacement of bag-placed hydrogel lenses into vitre-ous following neodymium: YAG laser capsulotomy. J Cataract Refract Surg 16: 563-566.
Lindstrom RL, Lindquist TD, Huldin J & Rubenstein JB (1988) Retinal detachment in axial myopiafollowing extracapsular cataract surgery. In: Caldwell DR (eds) Cataracts: Transactions of theNew Orleans Academy of Ophthalmology, pp 253-268.
Linnola RJ & Holst A (1998) Evaluation of a 3-piece silicone intraocular lens with poly (methylmethacrylate) haptics. J Cataract Refract Surg 24: 1509-1514.
Liu CSC, Wormstone IM, Duncan G, Marcantonio JM, Webb SF & Davies PD (1996) A study ofhuman lens cell growth in vitro. A model for posterior capsule opacification. Invest OphthalmolVis Sci 37: 906-914.
Lowe KJ & Easty DL (1992) a comparison of 141 polymacon (Iogel) and 140 poly (methyl methacr-ylate) intraocular lens implants. Br J Ophthalmol 76: 88-90.
Magno BV, Datiles MB, Lasa MSM, Fajardo MOQ, Caruso RC & Kaiser-Kupfer MI (1997) Evalu-ation of visual function following neodymium: YAG laser posterior capsulotomy. Ophthalmology104: 1287-1293.
Majima K (1998) The relationship between morphological changes of lens epithelial cells and in-traocular lens optic material. Jpn J Ophthalmol 42: 46-50.
Maltzman BA, Haupt E & Cucci P (1989) Effect of the laser ridge on posterior capsule opacification.J Cataract Refract Surg 15: 644-646.
Mamalis N, Crandall AS, Linebarger E, Sheffield WK & Leidenix MJ (1995) Effect of intraocularlens size on posterior capsule opacification after phacoemulsification. J Cataract Refract Surg 21:99-102.
Mamalis N, Phillips B, Kopp CH, Crandall AS & Randall JO (1996) Neodymium: Yag capsulotomyrates after phacoemulsification with silicone posterior chamber intraocular lenses. J Cataract Re-fract Surg 22 (suppl 2): 1296-1302.

84
McDonnel PJ, Krause W& Glaser BM (1988) In vitro inhibition of lens epithelial cell proliferationand migration. Ophthalmic Surg 19: 25-30.
Mester U, Bours J & Stuthe W (1978) Eiweissbestimmungen im Kammerwasser nach Einpflanzungvon Hornhautprothesen aus hydrophilem weichen Kunststoff. Ber dtsch Ophthalmol Ges 75: 215-219.
Mester U, Strauß M & Grewing R (1998) Biocompatibility and blood-aqueous barrier impairment inat-risk eyes with heparin-surface-modified or unmodified lenses. J Cataract Refract Surg 24: 380-384.
Milazzo S, Turut P, Bassam A & Charlin J-F (1996) Long-term follow-up of three-piece, looped, sil-icone intraocular lenses. J Cataract Refract Surg 22 (suppl 2): 1259-1262.
Miyake K (1990) Proposal for an ideal surface modification of IOLs. Eur J Implant Ref Surg 2: 209-212.
Miyake K & Maekubo K (1991a) Comparison of heparin surface modified and ordinary PCLs: A Jap-anese study. Eur J Implant Ref Surg 3: 95-97.
Miyake K, Maekubo K, Gravagna P & Tayot JL (1991b) Collagen IOLs: A suggestion for IOL bio-compatibility. Eur J Implant Ref Surg 3: 99-102.
Miyake K (1996a) The significance of inflammatory reactions following cataract extraction and in-traocular lens implantation. J Cataract Refract Surg 22 (suppl 1): 759-763.
Miyake K, Ota I, Miyake S & Maekubo K (1996b) Correlation between intraocular lens hydrophilic-ity and anterior capsule opacification and aqueous flare. J Cataract Refract Surg 22 (suppl 1): 764-769.
Morris RJ (2000) Hydroview® H60M intraocular lens- anterior and posterior capsule opacificationrates. Proc. XVIII Congress of the ESCRS, Brussels, Belgium, Abstr, p 155.
Murray RK & Keeley FW (1996) The extracellular matrix. In: Murray RK, Granner DK, Mayes PA& Rodwell VW (eds) Harpers� Biochemistry. Appleton & Lange, Stamford, Connecticut, pp 667-673.
Nagata T, Minakata A & Watanabe I (1998) Adhesiveness of AcrySof to a collagen film. J CataractRefract Surg 24: 367-370.
Newland TJ, McDermott ML, Eliott D, Hazlett LD, Apple DJ, Lambert RJ & Barret PR (1999) Ex-perimental neodymium: YAG laser damage to acrylic, poly (methyl methacrylate), and siliconeintraocular lens materials. J Cataract Refract Surg 25: 72-76.
Nishi O (1986) Incidence of posterior capsule opacification in eyes with and without posterior cham-ber intraocular lenses. J Cataract Refract Surg 12: 519-522.
Nishi O, Nishi K, Fujiwara T & Shirasawa E (1995a) Effects of diclofenac sodium and indomethacinon proliferation and collagen synthesis of lens epithelial cells in vitro. J Cataract Refract Surg 21:461-465.
Nishi O, Nishi K, Yamada Y & Mizumoto Y (1995b) Effect of indomethacin-coated posterior cham-ber intraocular lenses on postoperative inflammation and posterior capsule opacification. J Cata-ract Refract Surg 21: 574-578.
Nishi O, Nishi K, Imanishi M, Mano C, Yamada Y, Tada Y, Shirasawa E & Härfstrand A (1996a)Decreased prostaglandin E2 synthesis by lens epithelial cells cultured on heparin-surface-modi-fied poly (methyl methacrylate). J Cataract Refract Surg 22 (suppl 1): 859-862.
Nishi O, Nishi K & Ohmoto Y (1996b) Synthesis of interleukin-1, interleukin-6, and basic fibroblastgrowth factor by human cataract lens epithelial cells. J Cataract Refract Surg 22 (suppl 1): 852-853.
Nishi O, Nishi K, Takakazu M, Tada Y, Shirasawa E & Sakanishi K (1996c) Effect of intraocularsustained release of indomethacin on postoperative inflammation and posterior capsule opacifica-tion. J Cataract Refract Surg 22 (suppl 1): 806-810.
Nishi O, Nishi K, Saitoh I & Sakanishi K (1996d) Inhibition of migrating lens epithelial cells by sus-tained release of ethylenediaminetetracetic acid. J Cataract Refract Surg 22: 863-868.
Nishi O, Nishi K, Morita T, Tada Y, Shirasawa E & Sakanishi K (1996e) Effect of intraocular sus-tained release of indomethacin on postoperative inflammation and posterior capsule opacification.J Cataract Refract Surg 22: 806-810.
Nishi O, Nishi K, Akaishi T & Shirasawa E (1997a) Detection of cell adhesion molecules in lens ep-ithelial cells of human cataracts. Invest Ophthalmol Vis Sci 38: 579-585.

85
Nishi O, Nishi K, Mano C, Ichihara M, Honda T & Saitoh I (1997b) Inhibition of migrating lens ep-ithelial cells by blocking the adhesion molecule integrin: A preliminary report. J Cataract RefractSurg 23: 860-865.
Nishi O, Nishi K & Sakanishi K (1998a) Inhibition of migrating lens epithelial cells at the capsularbend created by the rectangular optic edge of a posterior chamber intraocular lens. OphthalmicSurg Lasers 29: 587-594.
Nishi O, Nishi K, Mano C, Ichihara M & Honda T (1998b) The inhibition of lens epithelial cell mi-gration by a discontinuous capsular bend created by a band-shaped circular loop or a capsule-bending ring. Ophthalmic Surg Lasers 29: 119-125.
Nishi O & Nishi K (1999) Preventing posterior capsule opacification by creating a discontinuoussharp bend in the capsule. J Cataract Refract Surg 25: 521-526.
Nishi O, Nishi K & Wicksrtöm K (2000) Preventing lens epithelial cell migration using intraocularlenses with sharp rectangular edges. J Cataract Refract Surg 26: 1543-1549.
Nissen KR, Fuchs J, Goldschmidt E, Andersen CU, Bjerrum K, Corydon L, Degn T, Eisgart F, Hen-ning V, Jensen JE, Krogh E, Lowes M, Mortensen K, Nielsen CH, Olsen T, Storr-Paulsen A, Sø-rensen TB & Winther-Nielsen A (1998) Retinal detachment after cataract extraction in myopiceyes. J Cataract Refract Surg 24: 772-776.
Ohara K, Okubo A, Miyazawa A, Miyamoto T, Sasaki H & Oshima F (1989) Aqueous flare and cellmeasurements using laser in endogenous uveitis patients. Jpn J Ophthalmol 33: 265-270.
Okada K, Takahashi K, Sagawa H & Abe K (1991) Evaluation of the images of specular microscopyof the cells on implanted intraocular lenses in vivo. Cells & Materials 1: 119-128.
Okada K, Funahashi M, Iseki K & Ishii Y (1993) Comparing the cell population on different intraoc-ular lens materials in one eye. J Cataract Refract Surg 19: 431-434.
Olsen G & Olson RJ (2000) Update on a long-term, prospective study of capsulotomy and retinal de-tachment rates after cataract surgery. J Cataract Refract Surg 26: 1017-1021.
Olson RJ & Crandall AS (1998) Silicone versus polymethylmethacrylate intraocular lenses with re-gard to capsular opacification. Ophthalmic Surg Lasers 29: 55-58.
Olson L (1989) Anatomy and Embryology of the lens. In: Tasman W & Jaeger EA (eds) Duane�sClinical Ophthalmology. Lippincott Company, Philadelphia, Pennsylvania, p 1- 3.
Olivero DK & Furcht LT (1993) Type IV collagen, laminin, and fibronectin promote the adhesionand migration of rabbit lens epithelial cells in vitro. Invest Ophthalmol Vis Sci 34: 2825-2834.
Oner FH, Gunenc Ü & Ferliel ST (2000) Posterior capsule opacification after phacoemulsification:Foldable acrylic versus poly (methyl methacrylate) intraocular lenses. J Cataract Refract Surg 26:722-726.
Oshika T, Yoshimura K & Miyata N (1992) Postsurgical inflammation after phacoemulsification andextracapsular extraction with soft or conventional intraocular lens implantation. J Cataract RefractSurg 18: 356-361.
Oshika T, Suzuki Y, Kizaki H & Yaguchi S (1996) Two year clinical study of a soft acrylic intraoc-ular lens. J Cataract Refract Surg 22: 104-109.
Oshika T, Nagata T & Ishii Y (1998) Adhesion of lens capsule to intraocular lenses of polymethyl-methacrylate, silicone, and acrylic foldable materials: an experimental study. Br J Ophthalmol 82:549-553.
Pajamäki KJJ, Andersson ÖH, Vedel E, Lindholm TS, Karlsson KH, Yli-Urpo A & Happonen R-P(1995) Bioactive glass and glass ceramic coated hip endoprosthesis: experimental study in rabbit.J Mater Sci Mater Med 5: 4-18.
Pande MV, Spalton DJ, Kerr-Muir M & Marshall J (1996a) Postoperative inflammatory response tophacoemulsification and extracapsular cataract surgery: Aqueous flare and cells. J Cataract Re-fract Surg 22 (suppl 1): 770-774.
Pande MV, Spalton DJ & Marshall J (1996b) Continuous curvilinear capsulorhexis and intraocularlens biocompatibility. J Cataract Refract Surg 22: 89-97.
Pande MV, Ursell PG, Spalton DJ, Heath G & Kundaiker S (1997) High-resolution digital retroillu-mination imaging of the posterior lens capsule after cataract surgery. J Cataract Refract Surg 23:1521-1527.
Paul JI, Schwarzbauer JE, Tamkun JW & Hynes RO (1986) Cell type specific fibronectin subunitsgenerated by alternative splicing. J Biol Chem 261: 12258-12265.

86
Peng Q, Visessook N, Apple DJ, Pandey SK, Werner L, Escobar-Gomez M, Schoderbek R, SolomonK & Guindi A (2000a) Surgical prevention of posterior capsule opacification Part 3: Intraocularlens optic barrier effect as a second line of defense. J Cataract Refract Surg 26: 198-213.
Peng Q, Apple DJ, Visessook N, Werner L, Pandey SK, Escobar-Gomez M, Schoderbek R & GuindiA (2000b) Surgical prevention of posterior capsule opacification Part 2: Enhancement of corticalcleanup by focusing on hydrodissection. J Cataract Refract Surg 26: 188-197.
Percival SPB, Anand V & Das SK (1983) Prevalence of aphakic retinal detachment. Br J Ophthalmol67: 43-45.
Perez M (2000) Posterior capsule opacification after 18 months in two different hydrophobic acrylicIOL implantation. Proc. XVIII Congress of the ESCRS, Brussels, Belgium, Abstr, p 165.
Pihlajaniemi T, Myllylä R & Kivirikko KI (1991) Prolyl 4-hydroxylase and its role in collagen syn-thesis. J Hepatol 13 (Suppl): S2-S7.
Pintucci S, Pintucci F, Cecconi M & Caiazza S (1995) New dacron tissue colonisable keratoprosthe-sis: clinical experience. Br J Ophthalmol 79: 825-829.
Piovella M, Camesasca FI & Gratton I (2000) MemoryLens® 1993-2000: Seven years experienceand new perspectives. Proc. XVIII Congress of the ESCRS, Brussels, Belgium, Abstr, p 168.
Polack FM & Heimke G (1980) Ceramic keratoprostheses. Ophthalmology 87: 693-698.Polack FM (1983) Clinical results with a ceramic keratoprosthesis. Cornea 2: 185-196.Powell SK & Olson RJ (1995) Incidence of retinal detachment after cataract surgery and neodymium:
Yag laser capsulotomy. J Cataract Refract Surg 21: 132-135.Power WJ, Neylan D & Collum LM (1994) Daunomycin as an inhibitor of human lens epithelial cell
proliferation in culture. J Cataract Refract Surg 20: 287-290.Prockop DJ & Kivirikko KI (1995) Collagens: Molecular biology, diseases, and potentials for thera-
py. Annu Rev Biochem 64: 403.Pötzsch DF & Pötzsch CM (1996) Four year follow-up of the MemoryLens. J Cataract Refract Surg
22 (suppl 2): 1336-1341.Ranta P, Kivelä T (1998) Retinal detachment in pseudophakic eyes with and without Nd:YAG laser
posterior capsulotomy. Ophthalmology 105: 2127-2133Ravalico G, Tognetto D, Palomba M, Busatto P & Baccara F (1996) Capsulorhexis size and posterior
capsule opacification. J Cataract Refract Surg 22: 98-103.Rosen E (1997) History in the making. J Cataract Refract Surg 23: 4-5.Ruiz JM, Medrano M, Alio JL (1990) Inhibition of posterior capsule opacification by 5-fluorouracil
in rabbits. Ophthalmic Res 22: 201-208.Saika S, Tamura M, Uenoyama K, Yamanaka A, Ohkubo K, Fukuda K & Iwane H (1992) Collagen-
ous deposits on explanted intraocular lenses. J Cataract Refract Surg 18: 195-199.Saika S, Kobata S, Yamanaka O, Yamanaka A, Okubo K, Oka T, Hosomi M, Kano Y, Ohmi S, Ue-
noyama S, Tamura M, Kanagawa R & Uenoyama K (1993) Cellular fibronectin on intraocularlenses explanted from patients. Graefes Arch Clin Exp Ophthalmol 231: 718-721.
Saika S, Yamanaka A, Tanaka S, Ohmi S, Ohnishi Y & Ooshima A (1995) Extracellular matrix onintraocular lenses. Exp Eye Res 61: 713-721.
Saika S, Tanaka S, Ohmi S, Minamide A, Ohnishi Y, Yamanaka A, Ooshima A & Kimura M (1997a)Deposition of extracellular matrix on intraocular lenses in rabbits: an immunohistochemical andtransmission electron microscopic study. Graefes Arch Clin Exp Ophthalmol 235: 241-247.
Saika S, Ohmi S, Ooshima A, Kimura M, Tanaka S, Okada Y, Ohnishi Y & Yamanaka A (1997b)Deposition of extracellular matrix on silicone intraocular lens implants in rabbits. Graefes ArchClin Exp Ophthalmol 235: 517-522.
Saika S, Ohmi S, Tanaka S, Miyamoto T, Kawashima Y, Ohnishi Y, Kanagawa R, Yamanaka A &Ooshima A (1997c) Cell proliferation on the outer anterior capsule surface after extracapsular lensextraction in rabbits. J Cataract Refract Surg 23: 1528-1531.
Saika S, Miyamoto T, Yamanaka A, Kawashima Y, Okada Y, Tanaka S-I, Yamanaka O, Ohmi S,Ohnishi Y & Ooshima A (1998a) Immunohistochemical evaluation of cellular deposits on poste-rior chamber intraocular lenses. Graefes Arch Clin Exp Ophthalmol 236: 758-765.
Saika S, Miyamoto T, Kimura M, Ohmi S, Ohkawa K, Kawashima Y, Ohnishi Y, Ooshima A & Ya-manaka A (1998b) Degenerated lens epithelial cells in rabbit and human eyes after intraocular lensimplantation. J Cataract Refract Surg 24: 1396-1398.

87
Saika S, Kawashima Y, Miyamoto T, Okada Y, Tanaka S, Yamanaka O, Ohnishi Y, Ooshima A &Yamanaka A (1998c) Immunolocalisation of hyaluronan and CD44 in quiescent and proliferatinghuman lens epithelial cells. J Cataract Refract Surg 24: 1266-1270.
Saika S, Kawashima Y, Miyamoto T, Okada Y, Tanaka SI, Ohmi S, Minamide A, Yamanaka O,Ohnishi Y, Ooshima A & Yamanaka A (1998d) Immunolocalisation of prolyl 4-hydroxylase sub-units, alfa-smooth muscle actin, and extracellular matrix components in human lens capsules withlens implants. Exp Eye Res 66: 283-294.
Saika S, Kawashima Y, Miyamoto T, Tanaka S, Okada Y, Yamanaka O, Katoh T, Ohnishi Y, OhmiS, Ooshima A & Yamanaka A (1998e) Immunolocalization of prolyl 4-hydroxylase in rabbit lensepithelial cells. J Cataract Refract Surg 24: 1261-1265.
Saika S, Miyamoto T, Okada Y, Yamanaka O, Ohnishi Y & Ooshima A (2000) Transforming growthfactor- β isoform proteins in cell and matrix deposits on intraocular lenses. J Cataract Refract Surg26: 709-715.
Sawa M, Tsurimaki Y, Tsuru T & Shimizu H (1988) New quantitative method to determine proteinconcentration and cell number in aqueous in vivo. Jpn J Ophthalmol 32: 132-142.
Schneiderman TE, Johnson MW, Smiddy WE, Flynn HW, Bennett SR & Cantrill HL (1997) Surgicalmanagement of posteriorly dislocated silicone plate haptic intraocular lenses. Am J Ophthalmolol123: 629-635.
Schalnus RW, Ohrloff C & Magone T (1995) Die Kammerwasser-Glaskörper-Barriere und die Blut-Kammerwasser-Schranke nach YAG-Laser-Kapsulotomie bei Kapselback- vs. Sulcus-ciliaris-Fixierung der IOL. Ophthalmologe 92: 289-292.
Schauersberger J, Kruger A, Abela C, Müllner-Eidenböck A, Petternel V, Svolba G & Amon M(1999) Course of postoperative inflammation after implantation of 4 types of foldable intraocularlenses. J Cataract Refract Surg 25: 1116-1120.
Seiffert D (1997a) Constitutive and regulated expression of vitronectin. Histol Histopathol 12: 787-797.
Seiffert D & Smith JW (1997b) The cell adhesion domain in plasma vitronectin is cryptic. J BiolChem 272: 13705-13710.
Sellman TR & Lindstrom RL (1988) Effect of a plano-convex posterior chamber lens on capsularopacification from Elschnig pearl formation. J Cataract Refract Surg 14: 68-72.
Shah GR, Gills JP, Durham DG & Ausmus WH (1986) Three thousand YAG lasers in posterior cap-sulotomies: An analysis of complications and comparison to polishing and surgical discission.Ophthalmic Surg 17: 473-477.
Shah SM, Spalton DJ & Smith SE (1991) Measurement of aqueous cells and flare in normal eyes. BrJ Ophthalmol 75: 348-352.
Shigemitsu T (1991) Ultrastructural study of adsorbed protein on extracted intraocular lenses. Jpn JOphthalmol 35: 354-358.
Sletteberg O, Hovding G & Bertelsen T (1990a) Keratoprosthesis I. Results obtained after implanta-tion of 12 one-piece prostheses. Acta Ophthalmol 68: 369-374.
Sletteberg O, Hovding G & Bertelsen T (1990b) Keratoprosthesis II. Results obtained after implan-tation of 27 dismountable two-piece prostheses. Acta Ophthalmol 68: 375-383.
Sourdille P & Ducournau Y (1990) Action de la daunomycine sur les cellules epitheliales du cristal-lin. Etude experimentale et clinique. Ophtalmologie 4: 107-108.
Spalton DJ, Shah SM & Kerr Muir MG (1993) Specular microscope of the anterior intraocular lenssurface. Eye 7: 707-710.
Steinert RF, Puliafito CA, Kumar SR, Dudak SD & Patel Samir (1991) Cystoid macular edema, ret-inal detachment, and glaucoma after Nd: YAG laser posterior capsulotomy. Am J Ophthalmol112: 373-380.
Sterling S & Wood TO (1986) Effect on intraocular lens convexity on posterior capsule opacification.J Cataract Refract Surg 12: 655-657.
Strampelli B & Marchi V (1970) Osteo - odonto - keratoprosthesis. Ann Ottalmol Clin Ocul 96: 1-57.Sundelin K & Sjöstrand J (1999) Posterior capsule opacification 5 years after extracapsular cataract
extraction. J Cataract Refract Surg 25: 246-250.Tamada Y & Ikada Y (1994) Fibroblast growth on polymer surfaces and biosynthesis of collagen. J
Biomed Mat Res 28: 783-789.

88
Tarsio JF, Kelleher PJ, Tarsio M, Emery JM & Lam DM-K (1997) Inhibition of cell proliferation onlens capsules by 4197X-ricin A immunoconjucate. J Cataract Refract Surg 23: 260-266.
Tezt MR, Apple DJ, Price FW, Piest KL, Kicaid MC & Bath PE (1987) Case reports. A newly de-scribed complication of neodymium: YAG laser capsulotomy: Exacerbation of an intraocular in-fection. Arch Ophthalmol 105: 1324-1325.
Tetz M, Sperker M, Blum M, Auffart GU & Völcker HE (1996a) Klinische Nachstarbewertung inpseudophaken Augen. Ophthalmologe 93: 33-37.
Tezt MR, Ries MW, Lucas C, Stricker H & Völcker HE (1996b) Inhibition of posterior capsule opaci-fication by an intraocular-lens-bound sustained drug delivery system: An experimental animalstudy and literature review. J Cataract Refract Surg 22: 1070-1078.
Tetz MR, Auffart GU, Sperker M, Blum M & Völcker HE (1997) Photographic image analysis sys-tem of posterior capsule opacification. J Cataract Refract Surg 23: 1515-1520.
Tjia KF (2000) AMO acrylic IOL Sensar AR40, clinical results. Proc. XVIII Congress of the ESCRS,Brussels, Belgium, Abstr, p 189.
Toldos JJM, Roig AA & Benabent EC (1996) Total anterior capsule closure after silicone intraocularlens implantation. J Cataract Refract Surg 22: 269-271.
Umezawa S & Shimizu K (1993) Biocompatibility of surface-modified intraocular lenses. J CataractRefract Surg 19: 371-374.
Ursell PG, Spalton DJ & Pande MV (1997) Anterior capsule stability in eyes with intraocular lensesmade of poly (methyl methacrylate), silicone, and AcrySof. J Cataract Refract Surg 23:1532-1538.
Vasavada A & Desai J (1997) Primary posterior capsulorhexis with or without anterior in congenitalcataracts. J Cataract Refract Surg 23 (suppl 1) 23: 645-651.
Weller M, Wiedemann P, Fischbach R, Hartmann C & Heimann K (1988) Evaluation of daunomycintoxicity on lens epithelium in vitro. Int Ophthalmol 12: 127-130.
Wenzel M, Reim M, Heinze M & Böcking A (1988) Cellular invasion on the surface of intraocularlenses. In vivo cytological observations following lens implantation. Graefes Arch Clin Exp Oph-thalmol 226: 449-454.
Werner LP, Legeais J-M, Durand J, Savondelli M, Legeay G & Renard G (1997) Endothelial damagecaused by uncoated and fluorocarbon-coated poly (methyl methacrylate) intraocular lenses. J Cat-aract Refract Surg 23: 1013-1019.
Werner L, Pandey SK, Escobar-Gomez M, Visessook N, Peng Q & Apple DJ (2000) Anterior capsuleopacification. A histopathological study comparing different IOL styles. Ophthalmology 107:463-471.
Vesaluoma M, Mertaniemi P, Mannonen S, Lehto I, Uusitalo R, Sarna S, Tarkkanen A & Tervo T(1998) Cellular and plasma fibronectin in aqueous humour of primary open-angle glaucoma, ex-foliative glaucoma and cataract patients. Eye 12: 886-890.
White JH and Gona O (1988) �Proplast� for keratoprosthesis. Ophthalmic Surg 19: 331-333.Whiteside SB, Apple DJ, Peng Q, Isaacs RT, Guindi A & Draughn RA (1998) Fixation elements on
plate intraocular lens. Large positioning holes to improve security of capsular fixation. Ophthal-mology 105: 837-843.
Winther-Nielsen A, Johansen J, Pedersen GK & Corydon L (1998) Posterior capsule opacificationand neodymium: YAG capsulotomy with heparin-surface-modified intraocular lenses. J CataractRefract Surg 24: 940-944.
Versura P, Torreggiani, Cellini M & Caramazza R (1999) Adhesion mechanisms of human lens epi-thelial cells on 4 intraocular lens materials. J Cataract Refract Surg 25: 527-533.
Wolter RJ (1982) Cell life on the surface of lens implants. Graefes Arch Clin Exp Ophthalmol 218:244-249.
Wolter RJ (1983a) Reactive membrane on a lens implant: three moths after implantation. GraefesArch Clin Exp Ophthalmol 220: 53-57.
Wolter RJ (1983b) Fusion of macrophages on lens implants resulting in the formation of giant cells.Graefes Arch Clin Exp Ophthalmol 221: 1-7.
Wolter RJ (1983c) Formation of proteinaceous capsules on plastic lens implants-by mouse macro-phages under tissue culture conditions. Ophthalmic Surg 14: 828-833.

89
Wolter RJ (1983d) Cellular membranes on glass lens implants-formed in tissue culture by mousemacrophages. Ophthalmic Surg 14: 834-838.
Wolter RJ (1985) Cytopathology of intraocular lens implantation. Ophthalmology 92: 135-145.Zaczek A, Petrelius A & Zetterström C (1998) Posterior continuous curvilinear capsulorhexis and
postoperative inflammation. J Cataract Refract Surg 24: 1339-1342.Zehetmayer M, Skorpik C, Weghaupt H & Scholz U (1994) Langzeitergebnisse nach Implantation
einer Plattenhaptik-Silikonlinse in den Kapselsack. Klin Monatsbl Augenheilkd 204: 220-225.Yakimenko S (1993) Results of a PMMA / titanium keratoprosthesis in 502 eyes. Refract Corneal
Surg 9: 197-198.Yamada K, Nagamoto T, Yozawa H, Kato K, Kurosaka D, Miyajima HB & Kimura C (1995) Effect
of intraocular lens design on posterior capsule opacification after continuous curvilinear capsulor-hexis. J Cataract Refract Surg 21: 697-700.
Ygge J, Wenzel M, Philipson B & Fagerholm P (1990) Cellular reactions on heparin-surface-modi-fied versus regular PMMA lenses during the first postoperative month. Ophthalmology 97: 1216-1224.
Yoneda A, Ogavwa H, Kojima K & Matsumoto I (1998) Characterization of the ligand binding ac-tivities of vitronectin: Interaction of vitronectin with lipids and identification the binding domainsfor various ligands using recombinant domains. Biochemistry 37: 6351-6360.
Yoshitomi T, Wong AS, Daher E & Sears SE (1990) Aqueous flare measurement with laser flare-cellmeter. Jpn J Ophthalmol 32: 132-142.


Original publications






























