Embed Size (px)
Citation preview
The role of transplant for CML in the imatinib era
Dr Wendy Ingram
Consultant Haematologist
University Hospital of Wales

What is Haematopoietic Stem Cell Transplantation?
• Deliver high dose chemotherapy +/- radiotherapy– Eradicate tumour cells– Destroys haematopoietic stem cells in bone marrow
• Autologous transplant – Infuse stored stem cells from the patient
• Allogeneic transplant– Replace with alternative donor stem cells
• New blood cells• New immune system – survey the body and aim to prevent
tumour cells from returning
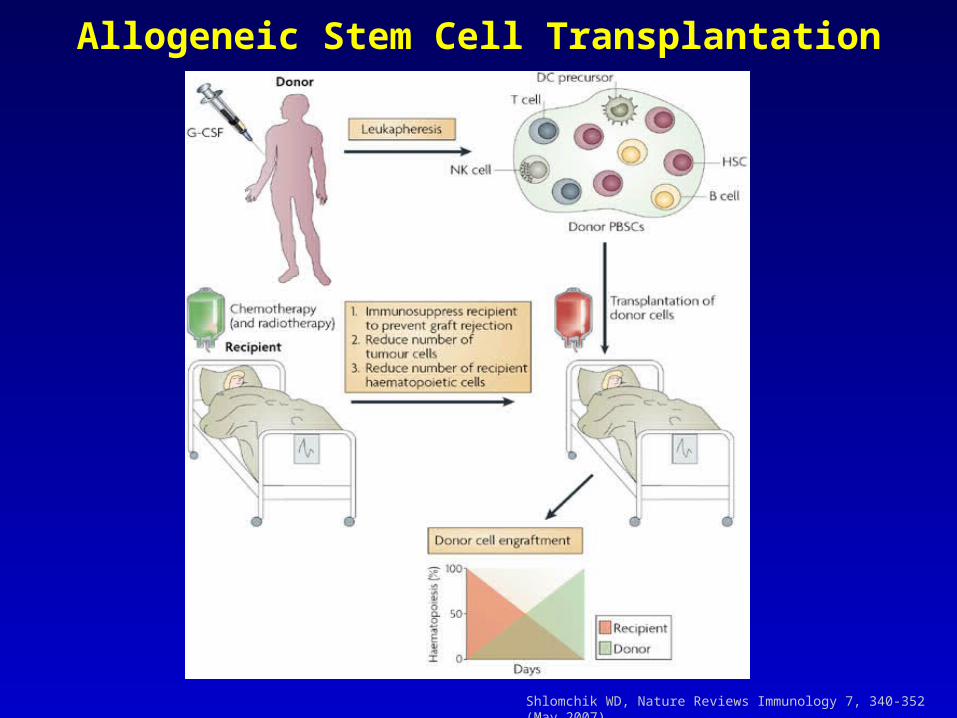
Allogeneic Stem Cell Transplantation
Shlomchik WD, Nature Reviews Immunology 7, 340-352 (May 2007)
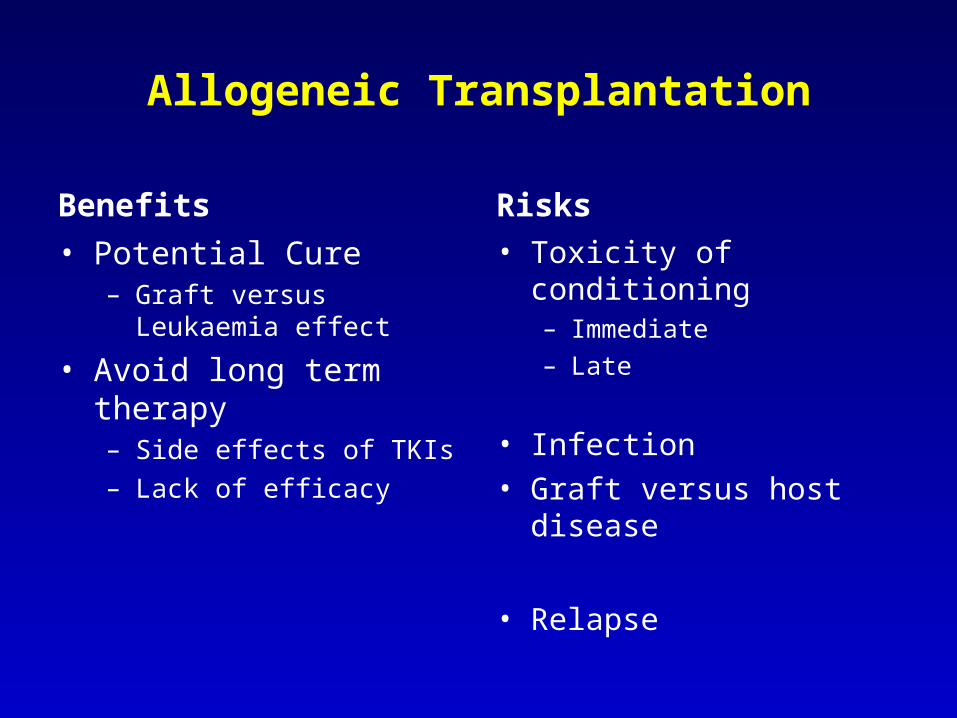
Allogeneic Transplantation
Benefits
• Potential Cure– Graft versus Leukaemia
effect
• Avoid long term therapy– Side effects of TKIs– Lack of efficacy
Risks
• Toxicity of conditioning– Immediate– Late
• Infection• Graft versus host disease
• Relapse
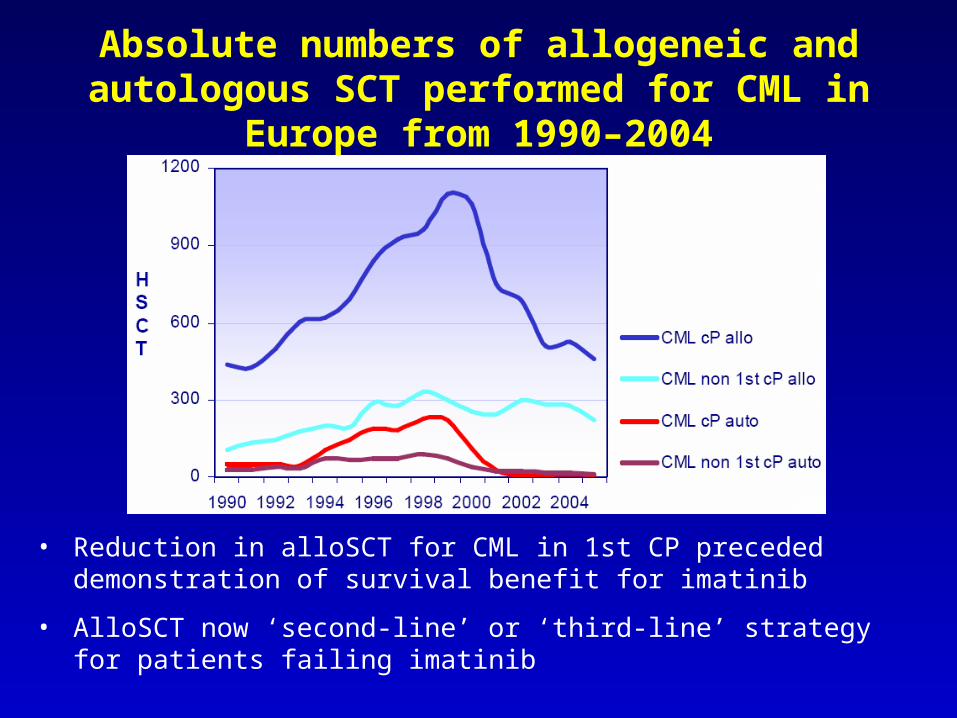
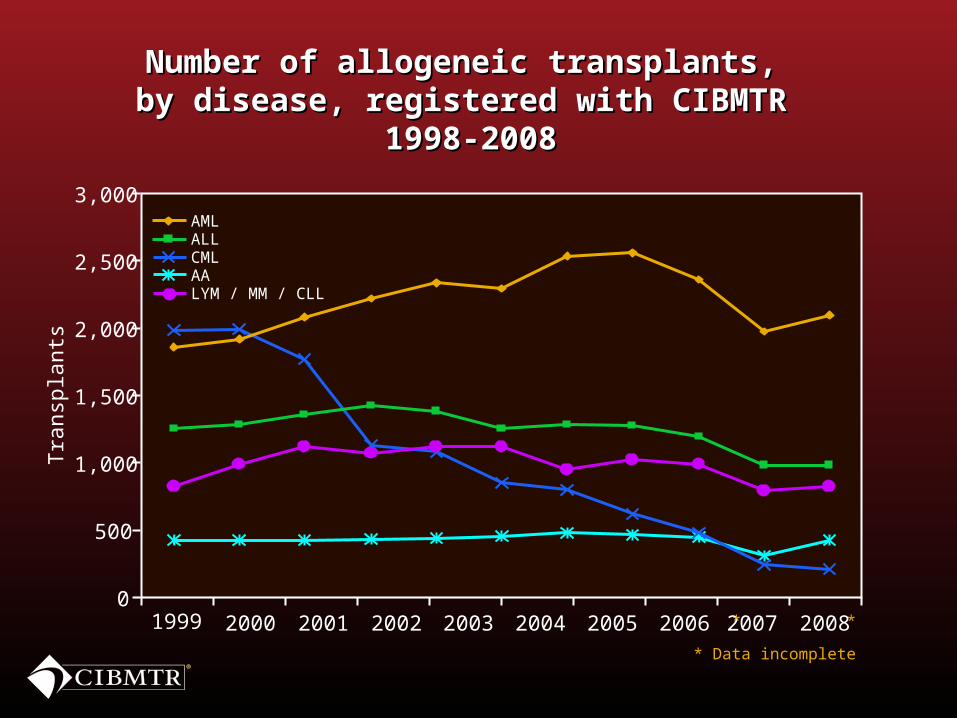
Absolute numbers of allogeneic and autologous SCT performed for CML in Europe
from 1990–2004
• Reduction in alloSCT for CML in 1st CP preceded demonstration of survival benefit for imatinib
• AlloSCT now ‘second-line’ or ‘third-line’ strategy for patients failing imatinib
Tra
nsp
lants
2,000
3,000
1,000
500
0
1,500
2,500
Number of allogeneic transplants, Number of allogeneic transplants, by disease, registered with CIBMTR by disease, registered with CIBMTR
1998-20081998-2008
1999 2000 2001 2002 2003 2004 2005 2007 20082006 * *
* Data incomplete
AMLALLCMLAALYM / MM / CLL
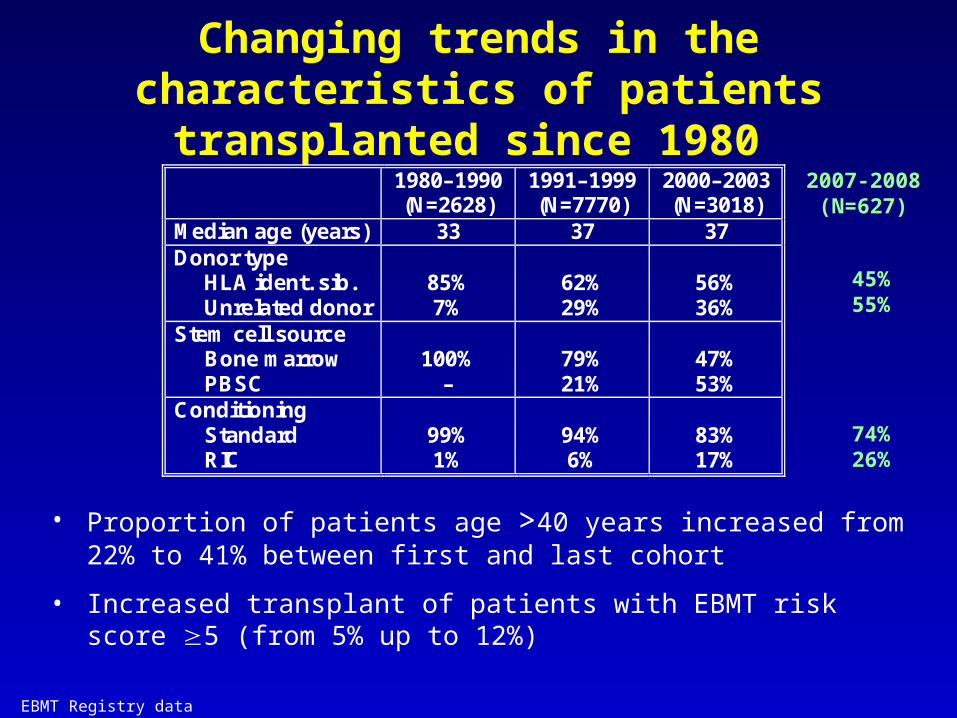
Changing trends in the characteristics of patients transplanted since 1980
1980–1990 (N=2628)
1991–1999 (N=7770)
2000–2003 (N=3018)
Median age (years) 33 37 37 Donor type HLA ident. sib. Unrelated donor
85% 7%
62% 29%
56% 36%
Stem cell source Bone marrow PBSC
100%
–
79% 21%
47% 53%
Conditioning Standard RIC
99% 1%
94% 6%
83% 17%
• Proportion of patients age >40 years increased from 22% to 41% between first and last cohort
• Increased transplant of patients with EBMT risk score 5 (from 5% up to 12%)
2007-2008(N=627)
45%55%
74%26%
EBMT Registry data

Overall Survival of CML by disease stage and type of donor (1997-2008)
HLA-id sib (N=3931)
MUD (N=1806)
p<0.001
HLA-id sib (N=936)
MUD (N=719)
p<0.001
HLA-id sib (N=236)
MUD (N=150)
p=0.55
CP1 CP2/AP
BC
EBMT Registry data
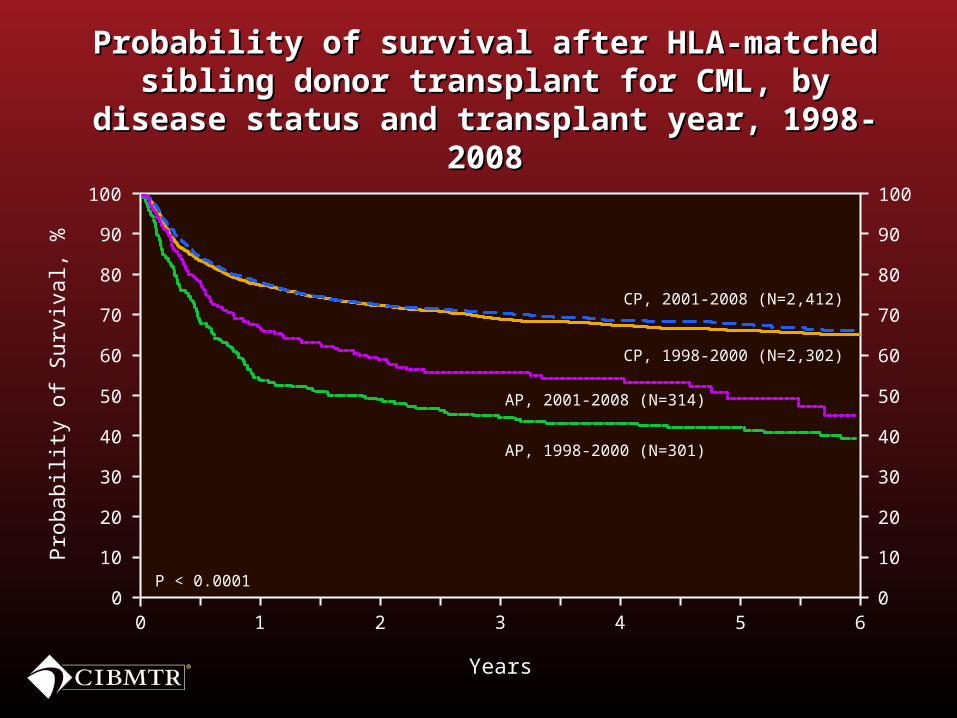
Years
Probability of survival after HLA-matched Probability of survival after HLA-matched sibling donor transplant for CML, by disease sibling donor transplant for CML, by disease
status and transplant year, 1998-2008status and transplant year, 1998-2008
0 2 61 3 4 5
CP, 1998-2000 (N=2,302)
0
20
40
60
80
100
10
30
50
70
90
0
20
40
60
80
100
10
30
50
70
90
Pro
babili
ty o
f Surv
ival, %
CP, 2001-2008 (N=2,412)
AP, 2001-2008 (N=314)
AP, 1998-2000 (N=301)
P < 0.0001
Reduced Intensity SCT in CML
• Percentage of patients undergoing RIC SCT for CML has risen from 1% in 1990 to 31% in 2004
• Highly immunosuppressive• Relies more on graft-versus-leukaemia (GvL) effect than
myeloablation for anti-tumour activity
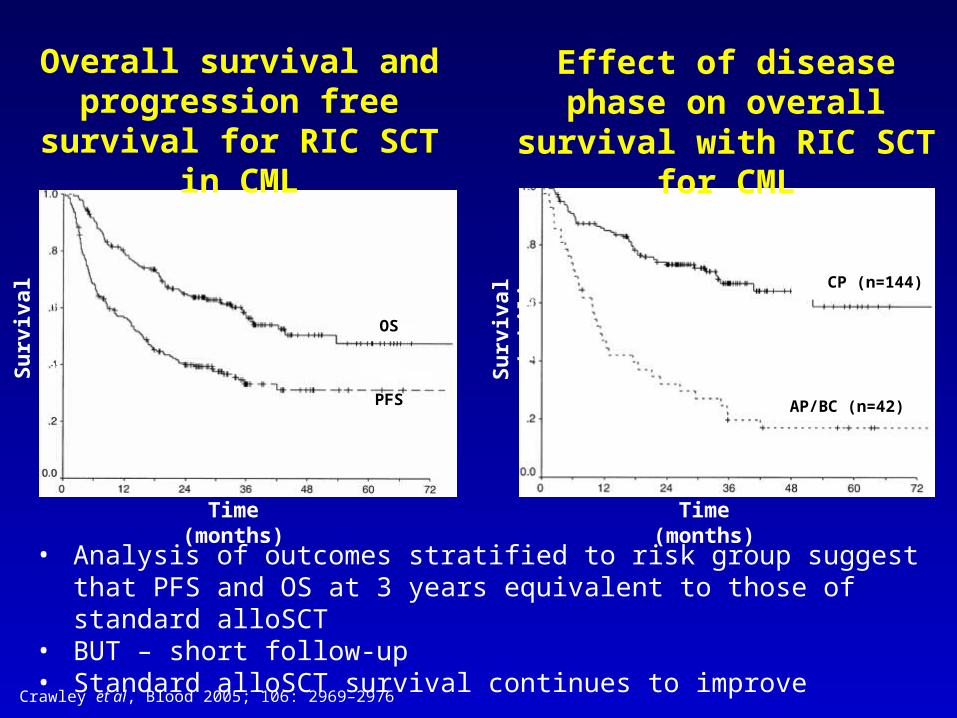
Overall survival and progression free survival
for RIC SCT in CML
Time (months)
Su
rviv
al p
rob
abili
ty
OS
PFS
Su
rviv
al p
rob
abili
tyTime (months)
CP (n=144)
AP/BC (n=42)
Effect of disease phase on overall survival with RIC
SCT for CML
• Analysis of outcomes stratified to risk group suggest that PFS and OS at 3 years equivalent to those of standard alloSCT
• BUT – short follow-up• Standard alloSCT survival continues to improve
Crawley et al, Blood 2005; 106: 2969–2976
UHW experience since 2000
• 9 Chronic Phase 1
• Median age 44 yrs (17-63 yrs)
• Median time from diagnosis to transplant 589 days
• 3 sibling, 6 unrelated• 2 standard, 7 RIC
• 10 Chronic Phase 2• 4 AP, 2 Blast crisis• Median age 50 yrs
(26-65 yrs)• Median time from
diagnosis to transplant 589 days
• 7 sibling, 9 unrelated• 4 standard, 12 RIC
12
CP1
• 10 patients• 2 deaths due to TRM• 2 relapse – 1 rescued
with donor lymphocytes
CP2, AP, BC
• 16 patients• 6 deaths due to TRM• 5 relapse – 1 rescued
with donor lymphocytes
13
UHW experience since 2000
Relapse post Allogeneic SCT
• Occurs in 16–33% of patients post SCT• Decision on how to treat based on risk of GvHD and how
fast BCR-ABL levels are rising– Unrelated donor versus sibling donor– Previous GvHD– Mismatched donor– Age
• Choice lies between either Donor Lymphocyte Infusion (DLI) or imatinib or both– Rarely will consider second alloSCT from different donor
Donor lymphocyte infusions can be used to manage relapse
• Patients relapsing after SCT for CML are very sensitive to DLI
• 60–90% response rate/remission– >90% response in patients transplanted in early CP– Further benefit in subsequent relapse
• Incremental dosing reduces risk of GvHD
Guglielmi et al, Blood 2002; 100: 397–405.

Imatinib for relapse post SCT: What is the evidence for efficacy?
• Imatinib also effective post SCT with benefits in all stages of disease
• Hammersmith study (n=128)1
– CP = 51; AP = 31; BC = 46
– 50 patients failed DLI prior to imatinib
– Overall haematologic response 84%; 98% for patients relapsing in CP
– CCyR: CP, 58%; AP, 48%; BC, 22%
– 25 patients achieved complete molecular remission
• However, response may be less durable than DLI– Higher incidence of relapse and inferior leukaemia-free survival (6/10
patients relapsed on Imatinib)2
• DLI and imatinib may be synergistic3
• However majority of patients now being transplanted are imatinib-resistant or intolerant
1Olavarria et al, Leukaemia 2003; 17(9): 1707–1712; 2Weisser et al, Haematologica 2006; 91: 663–666; 3Savani et al, Lancet Oncology 2005;6:809-812
The impact of newer TKIs on SCT
• Limited data• Likely to have a role in patients relapsing post SCT who
were resistant to / intolerant of imatinib• Often patients have already failed second generation
TKI prior to transplant• For patients who are resistant to or intolerant of imatinib
as first-line therapy, choice lies between alloSCT (if available donor) and second generation TKI

SummaryWho is a candidate for SCT?
• High Sokal score and low EBMT score at presentation– Discuss choice of alloSCT versus imatinib
– Consider trial of Imatinib in these high-risk patients
– Decision to transplant may be based on response
• Intolerance to imatinib and second generation TKI– Consider alloSCT, IFN or experimental therapy
• Choices after failure of or suboptimal response to imatinib 400 mg:– Dose escalation
– Second generation TKI
– For T315I BCR-ABL kinase domain mutation consider SCT or clinical trial
• For patients with blast crisis, consider imatinib or other TKI followed by alloSCT and restart TKI when counts recover post transplant
Acknowledgments
• Dr Mhairi Copland, University of Glasgow• Dr Keith Wilson BMT Programme Director, University
Hospital of Wales• Dr Andy Goringe• Dr Jonathan Kell• Dr Steve Knapper• Referring clinicians





























