Embed Size (px)
Citation preview

Laboratory for cell and tissue engineering
Institute for Complex Molecular Systems (ICMS)
Department of Biomedical Engineering
The role of shear forces and shear strains in the development of pressure ulcers.
Cees Oomens, Dan Bader
“Shear and tissue integrity – the state of the science” London, October 2014

definition of a pressure ulcer
A pressure ulcer is a localized injury to the skin and/or underlying tissue, usually over a bony prominence, resulting from sustained pressure (including pressure associated with shear). A number of contributing or confounding factors are also associated with pressure ulcers; the primary of which are impaired mobility and impaired sensory perception.
EPUAP/NPUAP/PPPIA, 2014

definition of a pressure ulcer
A pressure ulcer is a localized injury to the skin and/or underlying tissue, usually over a bony prominence, resulting from sustained pressure (including pressure associated with shear).
EPUAP/NPUAP/PPPIA, 2014

Problem with definition
• The definition suggests that we have to focus on pressures and shear forces when we study pressure ulcers
• It even suggests that it is primarily the interface pressure and shear force that are relevant
Normal force (pressure)
Shear force
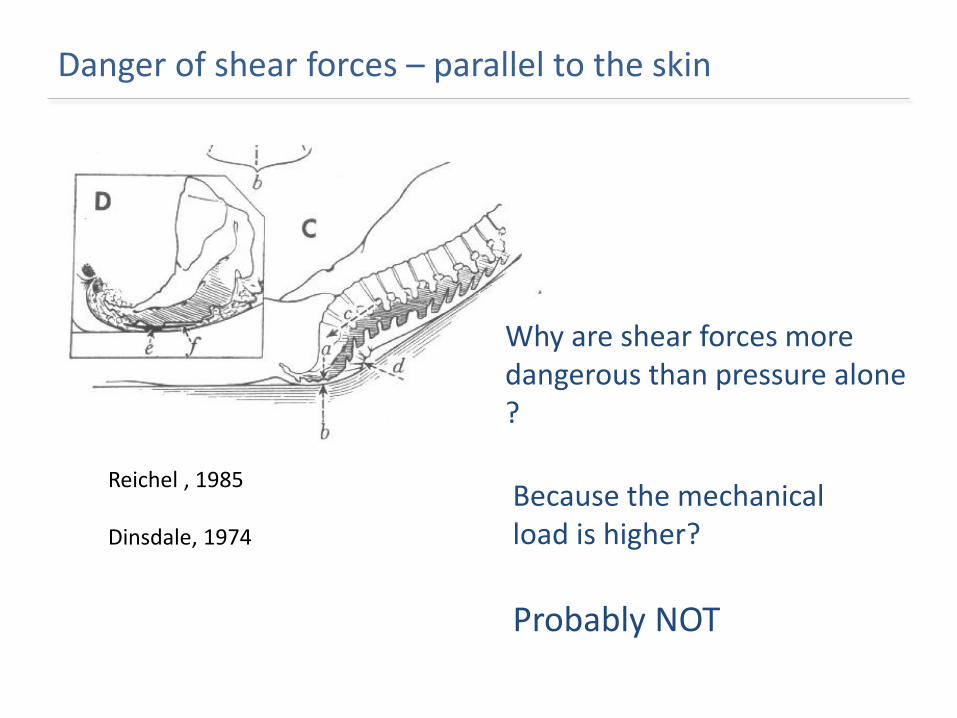
Danger of shear forces – parallel to the skin
Reichel , 1985 Dinsdale, 1974
Why are shear forces more dangerous than pressure alone ? Because the mechanical load is higher?
Probably NOT

Hypothesis of damage mechanisms due to shear forces
Skin wrinkles: This leads to very high deformations in the skin

Hypothesis of damage mechanisms due to shear forces
Delamination of skin layers
Hagisawa, 2005

shear modulus [kPa]
Indentation modulus [kPa]
Young’smodulus [kPa]
humidity
Stratum corneum 25% 30 600 0.04-10∙106
98%
10 ? 6-10∙104
Viable epidermis 25% 30 600 ?
98%
10 ? ?
Dermis 8 1-10 1-20∙103
Hypodermis 24 20-30 ?
Red: Geerligs et al. 2011,2012, Black: literature values
Hypothesis of damage mechanisms due to shear forces
Shear modulus much lower than Young’s modulus – Anisotropic Behaviour

Hypothesis of damage mechanisms due to shear forces
Easier to block blood vessel by shearing

Hypothesis of damage mechanisms due to shear forces
Effect of frictional sliding on skin
Heat generation Abrasion of tiny particles from Stratum Corneum at each sliding Up-regulation of cytokines in skin

Effect of shear forces seems important near surface
• All mechanisms described so far are important near the surface layers of the skin
• But what is the effect of pressure and shear in deeper layers?

How about strain/deformation?

How about strain/deformation?

Shear deformation is everywhere

Inhomogeneous shear strains – highest near bones
Chow,Odell, 1978
Todd, Thacker, 1994
Dabnichki et al., 1994
Oomens et al., 2003

Inhomogeneous shear strains – highest near bones
Chow,Odell, 1978
Todd, Thacker, 1994
Dabnichki et al., 1994
Oomens et al., 2003
muscle
skin
fat

Internal strains in a sitting person
Linder-Ganz et al.. J Biomech, 2007.

18
High strain often found near bony prominence
MR image during sitting
Linder-Ganz et al.. J Biomech, 2007.
Strain distribution

Internal strain and stress are very nonuniform
The initiation of damage is a very local phenomenon – at cellular level – and we need to know the effects of mechanical loading at a very local level.

Model systems to study etiology of pressure ulcers
Model system
single cell studies
Tissue engineered muscle
Rat model human volunteers

Cells and tissues
PAGE 21
Bouten et al. Ann. Biomed. Eng. (2001)
Breuls et al. Ann. Biomed. Eng. (2003)
Peeters et al. Med. Biol. Engng. Comp. (2003)
10 µm
Cells die as a result of moderate, but sustained
deformation even if oxygen and nutrient
supply are normal

Tissue engineered muscle
Damagemarkers
fluorescent markers
Gawlitta et al. J. Appl. Physiol. (2007) Gawlitta et al. Ann. Biomed. Eng (2007)
Deformation damage starts
fast
Hypoxia leads to change in metabolism
Low pH and lack of nutrients cause cell death at a longer time scale
Gefen et al. J.Biomech. 2008

23
The concept of animal studies
A. Stekelenburg et al. Med. Eng. Phys. (2006)
T2 – weighted MRI Perfusion measurements Animal specific theoretical models
In vivo studies confirm in-vitro studies
deformation damage fast and strong
correlation with level of deformation
Ischaemic damage slower process
Time scale is different from in-vitro scale

Two mechanisms for damage development
PAGE 24 17-11-2014
strain

Two mechanisms for damage development
PAGE 25 17-11-2014
strain

Two mechanisms for damage development
PAGE 26 17-11-2014
strain
Occlusion of blood vessel
Change in metabolism
Accumulation of waste products
pH decrease
CELL DEATH

Two mechanisms for damage development
PAGE 27 17-11-2014
strain
Occlusion of blood vessel
Change in metabolism
Accumulation of waste products
pH decrease
CELL DEATH
Direct deformation related damage
Membrane failure
Disruption of cytoskeleton
?

time
Exte
rnal
Pre
ssu
re
Reswick and Rogers, 1976
Recent research suggests a new risk curve
High Risk
Low Risk
INTE
RN
AL
LOC
AL
STR
AIN
/DEF
OR
MAT
ION

Clinical relevance
If mechanical loads causing ischaemia (threshold 1) cannot be avoided relieve the load at regular times (within 4 hours) to reset metabolic equilibrium.
Indeed try to avoid shear forces as much as possible
Avoid high loads above threshold 2.
17-11-2014

Clinical relevance
PAGE 30 17-11-2014
Do not pull or push the soft tissue around the wound at the time of body transfer, repositioning, diaper changing and bed operation.
(T.Ohura, 2012)

Acknowledgments
Dan Bader
Frank Baaijens
Klaas Nicolay
Gustav Strijkers
Jo Habets
Carlijn Bouten
Amit Gefen
31
Marielle Bosboom Roel Breuls Emiel Peeters Debby Gawlitta Debbie Bronneberg Lisette Cornelissen Karlien Ceelen Anke Stekelenburg Sandra Loerakker Willeke Traa Jules Nelissen Kevin Moerman Jibbe Soetens





























