Embed Size (px)
Citation preview

1
The role of Prasugrel in the management of the ACS-PCI patient
Professor Gilles Montalescot
This symposium has been sponsored by the Alliance of Daiichi Sankyo and Eli Lilly and Company. The speaker has been selected, briefed and paid an honorarium by the Alliance. Prescribing Information can be found on the last slide.
UKEFF01023a Date of Preparation Jan 2014

2
Disclosures of Interest
• Pr G. Montalescot reports receiving research grants to the institution or consulting/lecture fees
from Abbott Vascular, AstraZeneca, Biotronik, Daiichi-Sankyo, Eli Lilly, Fédération Française de
Cardiologie, Fondation de France, INSERM, Institut de France, Medtronic, Nanospheres, Pfizer,
Roche, Sanofi-Aventis, Stentys, Société Française de Cardiologie, The Medicines Company,
BMS, Menarini, Accumetrics, Bayer, Boehringer-Ingelheim, Duke Institute, Europa, GSK, Iroko,
Lead-Up, Novartis, Springer, TIMI group, WebMD, Wolters.

3
Licensed indication
1. Efient SPC (EF9M). eMC. http://www.medicines.org.uk/emc/ (document last updated on the eMC: 02/01/2014; date of first authorisation: 25 February 2009).
Efient® (prasugrel) therapeutic indications1
Efient, co-administered with acetylsalicylic acid (ASA), is indicated
for the prevention of atherothrombotic events in adult patients with
acute coronary syndrome (i.e. unstable angina, non-ST segment
elevation myocardial infarction [UA/NSTEMI] or ST segment
elevation myocardial infarction [STEMI]) undergoing primary or
delayed percutaneous coronary intervention (PCI)
A treatment of up to 12 months is recommended, unless the
discontinuation of prasugrel is clinically indicated.1

4
All patients (n=13,608)
• UA/NSTEMI (n=10,074)
• STEMI (n=3534)
Clopidogrel 300 mg LD
+ ASA
n=6795
Prasugrel 60 mg LD
+ ASA
n=6813
PCI
A loading dose of
study drug was
administered any time
between
randomisation and
1 hour after leaving
the cardiac
catheterisation
laboratory
PCI
Coronary angiography
Clopidogrel 75 mg MD
+ASA
Prasugrel 10 mg MD
+ASA
A treatment of up to 12 months is
recommended unless the
discontinuation of prasugrel is clinically
indicated 2
Duration of follow-up: 6-15 months
TRITON-TIMI 38: Study design1
Primary efficacy endpoint: Death from cardiovascular causes, nonfatal myocardial infarction or nonfatal stroke1
Primary safety endpoint: Non-CABG-related TIMI major bleeding 1
1. Wiviott S et al. Prasugrel versus clopidogrel in patients with acute coronary syndrome. N Engl J M 2007; 357(20): 2001-2015.
2. Efient SPC (EF9M). eMC. http://www.medicines.org.uk/emc/ (document last updated on the eMC: 02/01/2014; date of first authorisation: 25 February 2009).
LD: loading dose MD: maintenance dose

5
TRITON-TIMI 38: all ACS-PCI (n=13,608)
Please note
The “overall cohort” of TRITON-TIMI 38 is referred to as “all ACS-PCI “ in this presentation1.
1. Wiviott S et al. Prasugrel versus clopidogrel in patients with acute coronary syndrome. N Engl J M 2007; 357(20): 2001-2015.

6
Prasugrel + ASA
(n=6,813)
Adapted from reference 1 and 2
1. Wiviott S et al. Prasugrel versus clopidogrel in patients with acute coronary syndrome. N Engl J M 2007; 357(20): 2001-2015.
2. DoF0007TT38PrasEffic365dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries.
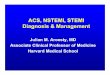
TRITON-TIMI 38 All ACS-PCI: primary efficacy endpoint (12 months)
Primary efficacy endpoint: death from cardiovascular causes,
nonfatal myocardial infarction or nonfatal stroke1,2
ARR: 2% RRR: 19% NNT: 50 HR: 0.81 ( 0.73 - 0.90) p=0.0001
365 180 90 60 30 0
Days from randomisation
Prim
ary
Eff
icacy E
nd
po
int (%
)
14
12
10
8
6
4
2
0
Clopidogrel + ASA
(n=6,795)
11.4%
9.4%

7 1. Wiviott S et al. Prasugrel versus clopidogrel in patients with acute coronary syndrome. N Engl J M 2007; 357(20): 2001-2015.
TRITON-TIMI 38 All ACS-PCI: primary efficacy endpoint (3 days)
0 1 2 3
5.6
4.7
Days after randomisation
0
2
4
6
8
Prasugrel
Clopidogrel
ARR: 0.9%
HR: 0.82
(0.71-0.96)
p=0.01
1
3
5
7
Prim
ary
Eff
icacy E
nd
po
int (%
)
Timing of benefit at 3 days: primary end point of death from
cardiovascular causes, nonfatal myocardial infarction or nonfatal stroke1-2

8
0 5 10 15 20 25 30
7.4
5.7
Days
0
2
4
6
8
Prasugrel
Clopidogrel
TRITON-TIMI 38 All ACS-PCI: primary efficacy endpoint (30 days)
Timing of benefit at 30 days: primary end point of death from
cardiovascular causes, nonfatal myocardial infarction or nonfatal stroke1,2
Adapted from reference 1.and 2
NB: Trial not powered for the 30-day landmark analyses
ARR: 2.3%
HR: 0.77
(0.67–0.88)
p=0.0001
1. Antman E. 40th Annual NY Symposium December 2007. New York
2. Wiviott S et al. Prasugrel versus clopidogrel in patients with acute coronary syndrome. N Engl J M 2007; 357(20): 2001-2015.
Prim
ary
Eff
icacy E
nd
po
int (%
)

9
All ACS-PCI, N=13,457
Event
Through 12 months Through study end (15 months)
Prasugrel
+ASA
Clopidogrel
+ASA
Prasugrel
+ASA
Clopidogrel
+ASA
(n=6741) (n=6716) HR (95% CI) p value (n=6741) (n=6716) HR (95% CI) p value
TIMI major
bleeding (primary) 2 1.6
1.24
(0.96, 1.59) 0.098 2.2 1.7
1.32
(1.03, 1.68) 0.029
Life-threatening 1.1 0.8 1.38
(0.97, 1.95) 0.068 1.3 0.8
1.52
(1.08, 2.13) 0.015
– Fatal 0.3 0.1 4.48
(1.52, 13.2) 0.003 0.3 0.1
4.19
(1.58, 11.1) 0.002
–- Symptomatic
ICH 0.2 0.2
0.94
(0.46, 1.89) 0.853 0.3 0.3
1.12
(0.58, 2.15) 0.737
TIMI minor
bleeding 2.3 1.8
1.29
(1.02, 1.64) 0.035 2.4 1.9
1.31
(1.04, 1.66) 0.022
1. Efient SPC (EF9M). eMC. http://www.medicines.org.uk/emc/ (document last updated on the eMC: 02/01/2014; date of first authorisation: 25 February 2009).
2. EMEA Assessment Report for Efient 117561/2009.
3. DOF009TT38PrasSftBl365-450dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries..
TRITON-TIMI 38 All ACS-PCI: safety endpoints (12 and 15 months)
Observed Event Rates of Non-CABG-related bleeding at 12 and 15 months (% patients)1-3
A treatment of up to 12 months is recommended unless the discontinuation of prasugrel is clinically indicated 1

10
TRITON-TIMI 38: STEMI-PCI (n=3,534)
Please note: TRITON-TIMI 38 was not prospectively designed or powered to show superiority of prasugrel over clopidogrel in the STEMI cohort alone.1
1. Montalescot G et al. Prasugrel compared with clopidogrel in patients undergoing percutaneous coronary intervention for ST-elevation myocardial
infarction (TRITON-TIMI 38): double-blind, randomised controlled trial. Lancet 2009; 373(9665): 723-731.

11
Prasugrel + ASA
(n=1,769)
Adapted from reference 1 and 2
TRITON-TIMI 38 STEMI-PCI: primary efficacy endpoint (12 months)
Death from cardiovascular causes, nonfatal myocardial infarction
or nonfatal stroke1,2
ARR: 2.5% RRR: 23% NNT: 40 HR: 0.77 (0.63 - 0.95) p=0.013
365 180 90 60 30 0
Days from randomisation
14
12
10
8
6
4
2
0
Clopidogrel + ASA
(n=1,765)
12.1
9.6
1. DoF0007TT38PrasEffic365dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries. .
2. Montalescot G et al. Prasugrel compared with clopidogrel in patients undergoing percutaneous coronary intervention for ST-elevation myocardial
infarction (TRITON-TIMI 38): double-blind, randomised controlled trial. Lancet 2009; 373(9665): 723-731.
Prim
ary
Eff
icacy E
nd
po
int (%
)

12
1. DoF0007TT38PrasEffic365dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries.
2. DoF0012TT38PrasEffic30dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries.
TRITON-TIMI 38 STEMI-PCI and All ACS-PCI: CV mortality (30 and 365 days)
STEMI-PCI: CV mortality at 30 and 365 days1,2
2.4
3.2
1.4
2.3
0
1
2
3
4
5
30 days 365 days
Pa
tie
nts
(%
)
ARR: 1% RRR: 39% HR: 0.61 (0.37 -1.00) p=0.047
p=0.097
STEMI-PCI
Prasugrel +
ASA (n=1,769)
Clopidogrel +
ASA (n=1,765)
1.2
2.2
0.9
1.9
0
1
2
3
4
5
30 days 365 days
Pa
tie
nts
(%
)
p=0.169
p=0.210
All ACS-PCI
Prasugrel + ASA
(n=6,813)
Clopidogrel +
ASA (n=6,795)
All ACS-PCI: CV mortality at 30 and 365 days1,2

13
1. Efient SPC (EF9M). eMC. http://www.medicines.org.uk/emc/ (document last updated on the eMC: 02/01/2014; date of first authorisation: 25 February 2009).
2. EfientDOF009TT38PrasSftBl365-450dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries. .
Observed Event Rates of Non-CABG-related bleeding at 12 and 15 months (% patients)1,2
STEMI-PCI, N=3476
Event
Through 12 months Through study end (15 months)
Prasugrel
+ASA
Clopidogrel
+ASA
Prasugrel
+ASA
Clopidogrel
+ASA
(n=1740) (n=1736) HR (95% CI) p value (n=1740) (n=1736) HR (95% CI) p value
TIMI major
bleeding (primary) 2.1 2.0
1.06
(0.66, 1.69) 0.82 2.2 2.0 1.11
(0.70, 1.77) 0.645
Life-threatening 1.0 1.0 0.94
(0.49, 1.83) 0.861 1.2 1.0 1.11
(0.59, 2.10) 0.75
– Fatal 0.3 0.1 NE NE 0.4 0.1 NE NE
–- Symptomatic
ICH 0.1 0.2 NE NE 0.2 0.2 NE NE
TIMI minor
bleeding 2.6 2.5
1.07
(0.70, 1.62) 0.764 2.7 2.6 1.04
(0.69, 1.57) 0.849
NE = not evaluated due to insufficient sample size
TRITON-TIMI 38 STEMI-PCI: safety endpoints (12 and 15 months)
A treatment of up to 12 months is recommended unless the discontinuation of prasugrel is clinically indicated 1

14
TRITON-TIMI 38: Diabetic ACS-PCI (n=3,146)
1. Wiviott S et al. Greater clinical benefit of more intensive oral antiplatelet therapy with prasugrel in patients with diabetes mellitus in the trial to assess improvement
in therapeutic outcomes by optimizing platelet inhibition with prasugrel thrombolysis in mycocardial infarction 38 Circulation 2008;118(16): 1626-1636.

15
1. DoF0008TT38PrasEfficDiabet365dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries.
2. Wiviott S et al. Greater clinical benefit of more intensive oral antiplatelet therapy with prasugrel in patients with diabetes mellitus in the trial to assess improvement
in therapeutic outcomes by optimizing platelet inhibition with prasugrel thrombolysis in mycocardial infarction 38 Circulation 2008;118(16): 1626-1636.
TRITON-TIMI 38 Diabetic ACS-PCI: primary efficacy endpoint (12 months)
Death from cardiovascular causes, non-fatal myocardial infarction or
non fatal stroke in diabetic ACS-PCI cohort1,2
ARR: 4.1% RRR: 29% NNT: 24 HR: 0.71 (0.58 - 0.86) p=0.0006
365 180 90 60 30 0
Days from randomisation
Pa
tie
nts
(%
)
18
16
14
10
8
6
2
0
15.5
11.4
Prasugrel + ASA
(n=1,576)
Clopidogrel + ASA
(n=1,570)
Adapted from reference 2
12
4

16
TRITON-TIMI 38 Diabetic ACS-PCI: primary efficacy endpoint (30 and 365 days)
Death from cardiovascular causes, non-fatal myocardial infarction or
non fatal stroke at 30 and 365 days1,2
1. DoF0011TT38PrasEfficDiabet30dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries.
2. DoF0008TT38PrasEfficDiabet365dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries
8.2
15.5
5.0
11.4
0
2
4
6
8
10
12
14
16
18
30 days 365 days
Pa
tie
nts
(%
) ARR: 3.2%
RRR: 40%
NNT: 31
HR: 0.60
(0.45 – 0.79)
p=0.0003
ARR: 4.1%
RRR: 29%
NNT: 24
HR: 0.71
(0.58 – 0.86)
p=0.0006 Prasugrel + ASA
(n=1,576)
Clopidogrel + ASA
(n=1,570)

17 1. DOF0010TT38PrasSftBlDiabet365-450dy Data on file, Daiichi Sankyo, Inc. and Eli Lilly and Company and/or one of its subsidiaries..
TRITON-TIMI 38 Diabetic ACS-PCI: safety endpoints (12 and 15 months)
Observed event rates of Non-CABG-related bleeding at 12 and 15 months (% patients)1
Diabetic ACS-PCI, N=3,108
Event
Through 12 months Through study end (15 months)
Prasugrel
+ASA
Clopidogrel
+ASA
Prasugrel
+ASA
Clopidogrel
+ASA
(n=1555) (n=1553) HR (95% CI) p value (n=1555) (n=1553) HR (95% CI) p value
TIMI major
bleeding (primary) 2.2 2.1
1.03 (0.64, 1.66)
0.9 2.3 2.2 1.06 (0.66,
1.69) 0.807
Life-threatening 1.5 1.2 1.21 (0.66,
2.23) 0.533 1.6 1.3
1.25 (0.70, 2.26)
0.450
– Fatal 0.5 0.1 NE NE 0.5 0.2 2.36 (0.61,
9.11) 0.2
– Symptomatic
ICH 0.3 0.5
0.57 (0.17, 1.94)
0.360 0.3 0.5 0.62 (0.20,
1.90) 0.401
TIMI minor
bleeding 2.7 1.9
1.46 (0.91, 2.34)
0.116 2.8 1.9 1.53 (0.96,
2.45) 0.073
NE = not evaluated due to insufficient sample size
A treatment of up to 12 months is recommended unless the discontinuation of prasugrel is clinically indicated 1

18
DOSING
• A treatment of up to 12 months is recommended, unless the discontinuation of prasugrel is clinically indicated.
• In UA/NSTEMI patients, where coronary angiography is performed within 48 hours after admission, the loading
dose should only be given at the time of PCI.1
1. Efient SPC (EF9M). eMC. http://www.medicines.org.uk/emc/ (document last updated on the eMC: 02/01/2014; date of first authorisation: 25 February 2009).
Appropriate use of prasugrel1
< 60kg 60mg 5mg
≥ 60kg and < 75 years 60mg 10mg
Loading dose Maintenance
dose
After careful risk-benefit evaluation
≥ 75 years Generally not recommended 60mg 5mg
Hypersensitivity to the active substance, or to any of the excipients
History of stroke or TIA
Severe hepatic impairment (Child-Pugh class C)
Active pathological bleeding CONTRAINDICATED
Please see the full Summary of Product Characteristics before prescribing