Embed Size (px)
Citation preview

The Role of D-Dimer in the Diagnosis of DeepVenous Thrombosis and Pulmonary Embolism
F. J. L. M. Haas1, P. W. Kamphuisen2
1Department of Clinical Chemistry and Haematology, St. Antonius Hospital, Nieuwegein, The Netherlands2Department of Vascular Medicine, Academic Medical Center, Amsterdam, The Netherlands
Correspondence to:Fred J. L. M. HaasDepartment of Clinical Chemistry and Haematology, St. Antonius Hospital, Post Box 2500, 3430, EM Nieuwegein, The NetherlandsTel: +31 30 688 4797; Fax: +31 30 609 2528; E-mail: [email protected]
Key words: D-dimer, deep venous thrombosis, pulmonary embolism.
Summary
The use of the D-dimer concentration for the exclusion
of venous thromboembolism (VTE) has been evaluated
circumstantially in many clinical studies and meta-analy-
ses with different kinds of assays and tests. The sensitivity
and specificity depend upon the prevalence of the VTE in
the patient population and this explains the variety of
results of the different studies. With a combination of
studies in meta-analyses, more reliable results and con-
clusions can be obtained. The quantitative assays have a
higher sensitivity, but a lower specificity than the quali-
tative tests, but no assay or test is sensitive enough for a
safe exclusion of VTE.
Introduction
Over the past decades, there have been many publications
about the diagnostic process of venous thromboembolism
(VTE). The use of the D-dimer assay as a screening test
alone or in combination with clinical risk stratification
models has been evaluated in many clinical studies. The
goal of these studies was the investigation of a safe and
cost-effective diagnostic strategy for exclusion of VTE, with
reduction in additional diagnostic tests and withholding an
unnecessary anticoagulation therapy.
D-dimer methods
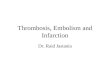
Fibrin is formed by an enzymatic cleavage of fibrinopeptide
A from fibrinogen with thrombin, followed by polymeri-
zation of the resulting fibrin monomers and cross-linking by
factor XIII (Fig. 1). Several enzymes like plasmin, elastase
and cathepsin-G can cleave the cross-linked fibrin com-
pound, forming different fibrin degradation products with
low and high molecular weight. Plasmin proteolysis of
cross-linked fibrin generates fragments D-dimer and E as
terminal products, in contrast to proteolysis of fibrinogen or
non-cross-linked fibrin, where monomeric fragment D is
formed (Fig. 2). Therefore, the dimeric D-domain may
serve as an indicator of in vivo fibrin formation. The
monoclonal antibody used in the D-dimer assay should be
specific for the plasmin formed D-dimer molecule without
any cross-reaction with the other degradation products.
There is a large variety of D-dimer assays commercially
available, evaluated in different studies, and they are as
follows:
1 enzyme-linked immunosorbent assays (ELISA)
2 enzyme-linked fluorescent assays (ELFA)
3 automated latex-enhanced light-scattering immuno-
assays (LIA)
4 membrane-based immunoassays with reflectometric
quantitative detection
5 membrane-based manual immunoassays
6 manual latex agglutination tests (qualitative or semi-
quantitative)
7 whole blood agglutination tests.
The conventional ELISA is performed on microtitre
plates. This type of assay is very time consuming and
therefore not convenient for direct patient care, only for
large series of samples.
An automated ELFA assay has been developed for the
VIDAS analyser, also called ‘rapid ELISA’, with a minimal
response time of 35 min.
The most used method is the automated LIA, with a
response time of 10–15 min, like the D-dimer, IL-Test,
STA-Lia and Tinaquant assays. The Tinaquant assay is
validated for performance in citrate plasma as well as
lithiumheparin plasma (1).
The membrane-based immunoassays are rapid, can be
performed manually with a semi-quantitative or qualitative
test result or a quantitative result by using a reflectometric
optical system. There is no need for a sophisticated
laboratory analyser.
3/2007 n IMAGING DECISIONS

The whole blood agglutination test, a rapid and manual
test, is based on a bivalent antibody directed against the
D-dimer antigen and the red blood cells.
Methods 4, 5 and 7 are suitable for point of care (POC)
use, because they are simple, have a rapid turnaround time
and are inexpensive, but if they are interpreted by visual
inspection, it is advisable that only trained observers
perform and interpret them (2).
D-dimer as diagnostic test
Because the VIDAS assay was one of the first automated
D-dimer assays commercially available, most of the clinical
studies were performed with these assays, followed
by studies with the automated LIAs. The results of the
different clinical studies depend on the patient populations
Action of thrombinFPAFPB
FPAFPB
DD
Fibrinogenmolecule
(a)
(b)
(c)
(d)
Proteolysis
Polymerization Fibrin dimer
Stabilization
Fibrinpolymer
FactorXIII aCa++
Intermediatepolymer
E E ED D D D
D D
D
D
DD E
DD E
E
DE
D
E E ED D D D
E D D E D D
D D DE ED
g
b
b
gThrombin
Fibrin monomer
j Fig. 1. After cleavage of fibrinogenby thrombin and forming of fibrinmonomers, the polymerization startsfollowed by cross-linking.
Formation of D-dimer
D
(a)
(b)
D D
D D D DE
D D
DE
D D D-dimer E D-dimer
X oligomers
P
Plasmin
D D
E
ED
D DE
E
DE E
j Fig. 2. Plasmin cleaves cross-linked fibrin forming D-dimer E andD-dimer molecules.
2 4 n R O L E O F D - D I M E R I N V T E
IMAGING DECISIONS n 3/2007

and the prevalence of deep venous thrombosis (DVT) or
pulmonary embolism (PE) (3–7).
The VIDAS assay and LIAs were compared in different
meta-analyses, in relation to the diagnostic performance of
DVT and PE, with variable results, and so without an
unambiguous conclusion. One of the main causes is the
heterogeneity of the LIA group, different kits measured on
a variety of analysers.
There are many reasons for the heterogeneity of
D-dimer assays, the characteristics of the used monoclonal
antibody, the sensitivity for only the plasmin cleavage
product or cross-reaction with low or high molecular
weight degradation products of fibrin and/or reactivity for
degradation products formed by other enzymes. There is
also a problem in the calibration of the assays, based on the
amount of fibrin fragment D-dimer present in the solution
(D-dimer units), or the amount of fibrinogen used for the
preparation of the degradation products (fibrinogen equiv-
alent units). There is also confusion about the units used:
ng/mL (¼lg/L) or ng/L. Theoretically, based on the
molecular weights of the fibrin D-dimer molecule and that
of fibrinogen, there should be a ratio of 1.8:1 in the test
results, but comparing the numerical values of different or
same assays, the results are not the same.
Because there is no reference method for the D-dimer
assay and thus no international standard, there is a great
need for ‘harmonization’ and the use of accepted calibra-
tion plasma, pooled plasma from different patients with
diseases with high D-dimer values, by all manufacturers of
D-dimer assays (8, 9).
Clinical validation
To validate the D-dimer in a clinical study, it is important to
have a ‘gold standard’, usually an imaging technique. Be-
cause in some strategies patients with a positive D-dimer test
result do not have the same protocol with imaging tech-
niques for further investigation than patients with a negative
test result, there is a great risk for a false negative or false
positive classification, and thus an incorrect calculation of
the sensitivity and specificity of the D-dimer assay.
Every quantitative assay has a certain accepted value as
cut-off value, but to obtain a better sensitivity (and a lower
specificity) sometimes a lower cut-off value is used. In case
of screening of patients suspected of PE, with the STA-Lia
D-dimer assay (standard cut-off value of 500 lg/L), there
is no need for a computed tomography angiography by a
D-dimer value <400 lg/L and there is a high negative
predictive value (NPV) if the value is <1000 lg/L (10).
Not only the sensitivity but also the specificity of the
assay is important. The specificity decreases in inpatients
(11), in older patients (12), in patients with malignancy (13),
during pregnancy (14) and per partum respectively
postpartum (15). Despite a high sensitivity, the number
of false positive diagnosis increases with a decreasing
specificity. This has logistic and financial consequences,
especially in a population of patients with low prevalence
of DVT or PE.
D-dimer concentration in time
The detection of D-dimer is possible within 2 h after the
formation of the clot and during at least 8 h, there is a
progressive increase in concentration (16). In a period of
about 15 days after the VTE, the D-dimer concentration
may be used as a diagnostic tool for exclusion of DVT (17,
18). There is an inverse relation between the duration of
complaints caused by the thrombosis and the D-dimer
concentration (19, 20).
D-dimer concentration and anticoagulation therapy
Some protocols start with administration of heparin to the
patient before the diagnosis is completed. The D-dimer
concentration diminishes after a treatment with unfrac-
tionated or low molecular weight heparin (21). A heparine
treatment for at least 24 h causes a decrease of 25% in the
D-dimer concentration and as a consequence a decrease in
the sensitivity in the range of 95.6–89.4% (22). In addition,
the use of oral vitamin K antagonists may diminish the
D-dimer concentration (23).
D-dimer and DVT
The choice of the reference method of imaging is impor-
tant for determination of the sensitivity, specificity and
NPV of the D-dimer assay. Ultrasonography has a lower
sensitivity for calf DVT than venography, with the risk of
missing the DVT and as a consequence that the result of
the D-dimer assay is classified wrongly as false positive (24).
In a study of outpatients suspected of DVT and a
negative result on proximal vein ultrasonography as first
step, the fast D-dimer test SimlyRED or ultrasonography
was performed after randomization. If the D-dimer test
was negative, there was no further testing and if the
ultrasonography was negative, repeated testing after
1 week and withholding anticoagulation therapy followed
it. There was no significant difference in the incidence of
DVT in the next 6 months’ follow-up, 1.0% and 0.9% (25,
26).
The combination of three meta-analyses, including 97
prospective studies, demonstrated a variation in the
sensitivity and specificity of different commercial available
assays (27–29). This resulted in a mean sensitivity of
90.5% (95% CI 90.0–91.1%) and the mean specificity of
54.7% (95% CI 54.0–55.4%). Besides the substantial
heterogeneity caused by difference in patient populations,
reference method and prevalence for DVT, there was
also a difference in the sensitivity between the different
D-dimer methods: ELISA (94%), quantitative latex agglu-
tination (89%) and the whole blood agglutination (Simply-
RED) (87%). There was no difference in sensitivity
R O L E O F D - D I M E R I N V T E n 2 5
3/2007 n IMAGING DECISIONS

between the two most used methods, VIDAS and
Tinaquant (96%).
In a multi-centre study a new POC D-dimer (CAR-
DIAC D-dimer) was evaluated in comparison with the
VIDAS and Tinaquant assays. It is a membrane-based
immunoassay with reflectometric quantitative detection,
suitable for heparine plasma. The results of the sensitivity
for the three assays, POC D-dimer, Tinaquant and
VIDAS, were 96.9%, 94.9% and 98.2%, specificity
60.8%, 64.8% and 40.7%, area under the curve 0.879,
0.908 and 0.895. These results demonstrate that the POC
D-dimer has a diagnostic performance comparable to the
VIDAS and Tinaquant D-dimer assays (30).
D-dimer concentration and locus
The sensitivity of the D-dimer assay for exclusion of DVT
is affected by the locus and extent of the thrombus.
A meta-analysis of 97 studies, wherein the D-dimer assay
was used for exclusion of DVT, showed a difference in the
sensitivity of the proximal and distal DVT, when reported
separately. The proximal DVT has a higher sensitivity
than the distal DVT, observed with all assays: ELISA 98%
vs. 86%, LIA 94% vs. 79%, and whole blood agglutination
84% vs. 64% (29).
From another meta-analysis of clinical studies in the
period February 1995–October 2003, it was concluded
that the sensitivity for thigh DVT is higher than for isolated
calf DVT. The sensitivity and NPV was often lesser than
90%, thus the D-dimer assay as single test is not safe
enough for exclusion DVT (28).
D-dimer and PE
The clinical studies for exclusion of PE using the D-dimer
concentration were mainly performed with the ELISA,
rapid ELISA and LIA assays and the whole blood agglu-
tination test. In the application of the D-dimer assay for
exclusion of PE, the variation in the sensitivity of the
ELISA and the rapid ELISA, compared with the LIA, was
lower, similar to the results in the DVT studies.
A meta-analysis of studies for exclusion of DVT and PE
with the D-dimer assay, published in the period 1983 to
January 2003, showed that the variability in the sensitivity
of the ELISA and the rapid ELISA is lower than the LIA
assays. Within the group of LIA assays, there was also a
variability in the sensitivity. Both the ELISA and the rapid
ELISA assay were considered as superior for the exclusion
of DVT. The ELISA and the rapid ELISA had a high
sensitivity of 95% (95% CI 88–100%), but a moderate
specificity of 45% (95% CI 38–53%), the sensitivity of the
LIA assay was 90% (95% CI 81–100%) and of whole blood
agglutination test 82% (95% CI 74–91%) (27).
In another meta-analysis of studies in the period 1982 to
November 2002, for exclusion of PE with the D-dimer
assay, it was shown that the LIA assays had a sensitivity of
93% and a specificity of 51%, thus comparable with the
ELISA assays (31).
From an analysis of the results of prospective manage-
ment studies with patients suspected of PE, the negative
likelihood ratios were calculated: ELISA 0.08 (95% CI
0.04–0.18), LIA assay 0.20 (95% CI 0.10–0.39), semi-
quantitative latex test 0.29 (95% CI 0.03–2.46) and whole
blood agglutination test 0.31 (95% CI 0.18–0.56) (32).
The risk of thromboembolic complications during the
3-month follow-up was 0.21% (95% CI 0.0–0.8%) in the
group of quantitative assays (VIDAS, Tinaquant) and
0.42% (95% CI 0.1–1.2%) with the whole blood aggluti-
nation test (SimlyRED) (33).
In three studies with outpatients suspected of PE,
the oral anticoagulation therapy was withheld when the
D-dimer concentration was normal and in the 3-month
follow-up period there were no thromboembolic events, so
the risk was 0% (95% CI 0.0–1.8%) (34–36).
A very recent meta-analysis of studies published before
March 2005, evaluating the diagnostic accuracy of the
D-dimer assay in the diagnosis of VTE, included 217
D-dimer assay evaluations for DVT and 111 for PE. The
results of the comparison of the different assays and tests
are presented in Table 1 (37).
D-dimer concentration and locus
The sensitivity of the D-dimer assay for exclusion of PE,
just like DVT, is affected by the locus and extent of the
thrombus. The sensitivity for exclusion of subsegmental PE
was 50% (95% CI 44–56%) and 93% (95% CI 90–96%)
for segmental PE (17).
From a comparison of the LIA assay (Tinaquant) with
the rapid ELISA (VIDAS) in the exclusion of segmental
and subsegmental PE it was obvious that both assays
j Table 1: Sensitivity and specificity of different D-dimer assays
(37)
Type of D-dimer
study
Deep venous
thrombosis Pulmonary embolism
Median
sensitivity
Median
specificity
Median
sensitivity
Median
specificity
Microplate ELISA
Asserachrome 94 47 96 44
Membrane ELISA
Instantia 86 65 89 62
Nycocard 88 50 91 47
Latex quantitative
Tinaquant 92 53 94 50
STA-Lia test 94 46 96 43
ELFA (rapid ELISA)
VIDAS 96 44 97 41
Whole-blood assay
SimplyRED 82 72 86 70
ELISA: enzyme-linked immunosorbent assay, ELFA: enzyme-linked
fluorescent immunoassay.
2 6 n R O L E O F D - D I M E R I N V T E
IMAGING DECISIONS n 3/2007

behave quite similar and that the sensitivity for the
subsegmental PE (76%) was significantly lower than that
for the segmental PE (98%) (38).
Discussion
The use of the D-dimer assays for exclusion of VTE has
been extensively evaluated in different clinical studies and
meta-analyses. The D-dimer assays are sensitive but non-
specific markers for VTE, so positive D-dimer results are
not useful to ‘rule in’ the diagnosis; rather the potential
value is for a negative test result to ‘rule out’ the diagnosis.
The quantitative assays have higher sensitivity, but lower
specificity than the qualitative tests, but no assay or test has
a sensitivity high enough for a safe exclusion of VTE.
The D-dimer test results should always be combined
with other information obtained by imaging techniques
and/or clinical decision rules for a safe withholding of an
anticoagulation therapy.
References
1. Schutgens RE, Haas FJ, Ruven HJ, Spannagl M, Horn K, Biesma
DH. No influence of heparin plasma and other (pre)analytic variables
on D-dimer determinations. Clin Chem 2002; 48: 1611–1613.
2. Wells PS. Integrated stategies for the diagnosis of venous trom-
boembolism. J Thromb Haemost 2007; 5 (Suppl. 1): 41–50.
3. van der Graaf F, van den Borne H, van der Kolk M, de Wild PJ,
Janssen GW, van Uum SH. Exclusion of deep venous thrombosis with
D-dimer testing comparison of 13 D-dimer methods in 99 outpatients
suspected of deep venous thrombosis using venography as reference
standard. Thromb Haemost 2000; 83: 191–198.
4. Gosselin RC, Owings JT, Kehoe J et al. Comparison of six D-dimer
methods in patients suspected of deep vein thrombosis. Blood Coagul
Fibrinolysis 2003; 14: 545–550.
5. Schutgens RE, Haas FJ, Gerritsen WB, van der Horst F, Nieuwenhuis
HK, Biesma DH. The usefulness of five D-dimer assays in the
exclusion of deep venous thrombosis. J Thromb Haemost 2003; 1:
976–981.
6. Gardiner C, Pennaneac’h C, Walford C, Machin SJ, Mackie IJ. An
evaluation of rapid D-dimer assays for the exclusion of deep vein
thrombosis. Br J Haematol 2005; 128: 842–848.
7. Waser G, Kathriner S, Wuillemin WA. Performance of the auto-
mated and rapid STA Liatest D-dimer on the STA-R analyzer.
Thromb Res 2005; 116: 165–170.
8. Meijer P, Haverkate F, Kluft C, de Moerloose P, Verbruggen B,
Spannagl M. A model for the harmonisation of test results of dif-
ferent quantitative D-dimer methods. Thromb Haemost 2006; 95:
567–572.
9. Dempfle CE. D-dimer assays: the current status and new assay
technologies. Thromb Res 2006; 118: 569–571.
10. Abcarian PW, Sweet JD, Watabe JT, Yoon HC. Role of a quan-
titative D-dimer assay in determining the need for CT angiography
of acute pulmonary embolism. Am J Roentgenol 2004; 182: 1377–
1381.
11. Schrecengost JE, LeGallo RD, Boyd JC et al. Comparison of diag-
nostic accuracies in outpatients and hospitalized patients of D-dimer
testing for the evaluation of suspected pulmonary embolism. Clin
Chem 2003; 49: 1483–1490.
12. Schutgens RE, Haas FJ, Biesma DH. Reduced efficacy of clinical
probability score and D-dimer assay in elderly subjects suspected of
having deep vein thrombosis. Br J Haematol 2005; 129: 653–657.
13. Schutgens RE, Beckers MM, Haas FJ, Biesma DH. The predictive
value of D-dimer measurement for cancer in patients with deep vein
thrombosis. Haematologica 2005; 90: 214–219.
14. Kline JA, Williams GW, Hernandez-Nino J. D-dimer concentrations
in normal pregnancy: new diagnostic thresholds are needed. Clin
Chem 2005; 51: 825–829.
15. Epiney M, Boehlen F, Boulvain M et al. D-dimer levels during
delivery and the postpartum. J Thromb Haemost 2005; 3: 268–271.
16. Mager JJ, Schutgens RE, Haas FJ, Westermann CJ, Biesma DH. The
early course of D-dimer concentration following pulmonary artery
embolisation. Thromb Haemost 2001; 86: 1578–1579.
17. Kelly J, Rudd A, Lewis RR, Hunt BJ. Plasma D-dimers in the
diagnosis of venous thromboembolism. Arch Int Med 2002; 162: 747–
756.
18. de Bastos M, de Bastos MR, Bogutchi T, Carneiro-Proietti AB,
Rezende SM. Duration of symptoms and D-dimer testing in the
ruling-out of venous thromboembolism. J Thromb Haemost 2006; 4:
2079–2080.
19. D’Angelo A, D’Alessandro G, Tomassini L, Pittet JL, Dupuy G,
Crippe L. Evaluation of a new rapid quantitative D-dimer assay in
patients with clinically suspected deep vein thrombosis. Thromb
Haemost 1996; 75: 412–416.
20. Kuruvilla J, Wells PS, Morrow B. Prospective assessment of the nat-
ural history of positive D-dimer results in persons with acute venous
thromboembolism (DVT or PE). Thromb Haemost 2003; 89: 284–
287.
21. Stricker H, Marchetti O, Haeberli A, Mombelli O. Hemostatic acti-
vation under anticoagulant treatment: a comparison of unfractionated
heparin vs. nadroparin in the treatment of proximal deep vein
thrombosis. Thromb Haemost 1999; 82: 1227–1231.
22. Couturaud F, Kearon C, Bates SM, Ginsberg JS. Decrease in sensi-
tivity of D-dimer for acute venous thromboembolism after starting
anticoagulant therapy. Blood Coagul Fibrinolysis 2002; 13: 241–246.
23. Ombandza-Moussa E, Samama MM, Horellou MH, Elalamy I,
Conard J. Potential use of D-dimer measurement in patients treated
with oral anticoagulant for a venous thromboembolic episode. Int
Angiol 2003; 22: 364–369.
24. Philbrick JT, Heim S. The D-dimer test for deep venous thrombosis:
gold standards and bias in negative predictive value. Clin Chem 2003;
49: 570–574.
25. Kearon C, Ginsberg JS, Douketis J et al. A randomized trial of
diagnostic strategies after normal proximal vein ultrasonography for
suspected deep venous thrombosis: D-dimer testing compared with
repeated ultrasonography. Ann Intern Med 2005; 142: 490–496.
26. Hull RD. Revisiting the past strengthens the present: an evidence-
based medicine approach for the diagnosis of deep venous thrombosis.
Ann Intern Med 2005; 142: 583–585.
27. Stein PD, Hull RD, Patel KC et al. D-dimer for the exclusion of acute
venous thrombosis and pulmonary embolism: a systematic review.
Ann Intern Med 2004; 140: 589–602.
28. Heim SW, Schectman JM, Siadaty MS, Philbrick JT. D-dimer testing
for deep venous thrombosis: a metaanalysis. Clin Chem 2004; 50:
1136–1147.
29. Goodacre S, Sampson FC, Sutton AJ, Mason S, Morris F. Variation
in the diagnostic performance of D-dimer for suspected deep vein
thrombosis. QJM 2005; 98: 513–527.
30. Dempfle CE, Korte W, Schwab M, Zerback R, Huisman MV;
CARDIM Study Group. Sensitivity and specificity of a quantitative
point of care D-dimer assay using heparinized whole blood, in pa-
tients with clinically suspected deep vein thrombosis. Thromb
Haemost 2006; 96: 79–83.
31. Brown MD, Lau J, Nelson RD, Kline JA. Turbidimetric D-dimer test
in the diagnosis of pulmonary embolism: a metaanalysis. Clin Chem
2003; 49: 1846–1853.
32. Roy PM, Colombet I, Durieux P, Chatellier G, Sors H, Meyer G.
Systematic review and meta-analysis of strategies for the diagnosis of
suspected pulmonary embolism. BMJ 2005; 331: 259–9.
R O L E O F D - D I M E R I N V T E n 2 7
3/2007 n IMAGING DECISIONS

33. Ten Cate-Hoek AJ, Prins MH. Management studies using a combi-
nation of D-dimer test result and clinical probability to rule out ve-
nous thromboembolism: a systematic review. J Thromb Haemost
2005; 3: 2465–2470.
34. Perrier A, Desmarais S, Miron MJ et al. Non-invasive diagnosis of
venous thromboembolism in outpatients. Lancet 1999; 353: 190–195.
35. Bernier M, Miron MJ, Desmarais S, Berube C. Use of the D-dimer
measurement as the first step in the diagnosis of deep vein thrombosis
(DVT) and pulmonary embolism (PE) in an emergency department.
Thromb Haemost 2001; 7 (Suppl.): P754 (Abstract).
36. Perrier A, Roy PM, Aujesky D et al. Diagnosing pulmonary embolism
in outpatients with clinical assessment, d-dimer measurement, venous
ultrasound, and helical computed tomography: a multicenter man-
agement study. Am J Med 2004; 116: 291–299.
37. Di Nisio M, Squizzato A, Rutjes AW, Buller HR, Zwinderman AH,
Bossuyt PM. Diagnostic accuracy of D-dimer test for exclusion of
venous thromboembolism: a systematic review. J Thromb Haemost
2007; 5: 296–304.
38. Sijens PE, Oudkerk M, Berghout A, van Ingen HE, Kemperman H.
Comparison of a quantitative latex and a quantitative ELISA plasma
D-dimer assay in the exclusion of segmental and subsegmental pul-
monary embolism. Thromb Haemost 2001; 86: 1580–1582.
2 8 n R O L E O F D - D I M E R I N V T E
IMAGING DECISIONS n 3/2007