Embed Size (px)
Citation preview

The Role of Assertiveness and DecisionMaking in Early Adolescent Substance
Initiation: Mediating Processes
Linda Trudeau, Catherine Lillehoj, Richard Spoth,and Cleve Redmond
Iowa State University
This study examined the mediating processes linking assertiveness anddecision making to early adolescent substance initiation, along with themoderating effect of gender on those processes. Models specifying negativeexpectancies and refusal intentions as mediators of individual rightsassertiveness and decision-making effects on substance initiation wereevaluated across 18 months on a nontreatment cohort of young adolescentsparticipating in a prevention trial (average age 12.3 years at baseline;N5 357). Results indicated that individual rights assertiveness and decisionmaking had indirect effects on substance initiation through effects onnegative outcome expectancies and refusal intentions. Gender differenceswere found in both the average level and the pattern of relationships amongthe variables. For girls, refusal intentions were negatively associated withlater substance initiation. For boys, early levels of substance initiation werenegatively associated with later levels of negative expectancies and refusalintentions. Implications for prevention programming are discussed.
A recent report suggests that substance use among young adolescents inthe United States remains high (Johnston, O’Malley, & Bachman, 2002).Because substance use during early adolescence has been associated withmultiple negative outcomes (Dryfoos, 1990; Riggs &Whitmore, 1999), thepast two decades have seen an increase in approaches to delay and
JOURNAL OF RESEARCH ON ADOLESCENCE, 13(3), 301–328Copyright r 2003, Society for Research on Adolescence
Requests for reprints should be sent to Linda Trudeau, Institute for Social and BehavioralResearch, ISU Research Park, Building 2, Suite 500, 2625 North Loop Drive, Iowa StateUniversity, Ames, IA 50010. E-mail: [email protected]

prevent the initiation of substance use (see Institute of Medicine, 1994;Peters & McMahon, 1996; Spoth, Kavanaugh, & Dishion, 2002). In thiscontext, prevention experts and federal agencies have emphasized theimportance of designing preventive interventions based on sound theoryand empirical science (Mrazek & Haggerty, 1994; National Institute onDrug Abuse, 1997).
Knowledge about adolescent psychosocial development contributes tothe determination of appropriate timing and content of interventions toproduce the greatest impact on early adolescent substance initiation(Langer, 1996). Regarding timing of interventions, for example, retro-spective reports from the Monitoring the Future Study 1974–1994(Johnston, O’Malley, & Bachman, 1996) indicate that cigarette initiationpeaks during sixth and seventh grades, and alcohol initiation peaksduring seventh through ninth grades. This pattern of initiation suggeststhe importance of early intervention. Regarding intervention programcontent, research indicates that adolescence is a time of considerablepsychosocial development, including: cognitive growth (Keating, 1990);changes in peer group importance, composition, and acceptance (Brown,1990; Dishion, Capaldi, & Yoerger, 1999); increasing influence of peerfriendship and dating relationships (Brown, Dolcini, & Leventhal, 1997;Buhrmester, 1996) and struggles with identity issues (Erikson, 1968;Harter, 1990). In addition, the transition from elementary school to middleschool is accompanied by increased autonomy and the necessity for moreindependent decision making (Entwistle, 1990). Appropriate interven-tions for early adolescence should consider developmental timing totarget influences on cultural, interpersonal, and intrapersonal variablesthat can delay substance initiation.
Theories of adolescent development (Ausubel, Montemeyor, & Svajian,1977; Feldman & Elliott, 1990), social cognition (Ajzen, 1985; Bandura,1986), problem behavior (Jessor & Jessor, 1977), and personal and socialdevelopment (Erikson, 1993; Rosenberg, 1989) have contributed toclarifying the etiology of substance use and mechanisms of behaviorchange that have guided the development of numerous preventionprograms. Recently, researchers have drawn on this work to articulateintegrated models related both to etiology of substance use and tomechanisms of intervention effects (Botvin, 1999; Petraitis, Flay, & Miller,1995; Spoth & Redmond, 2002).
The current research contributes to the knowledge base by exploringmediational processes associated with models of intrapersonal influenceson substance initiation during early adolescence and by examining gendermoderation of those processes. Although constructs were selected thatrepresent frequently targeted school- and family-based prevention
302 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

program content (see Botvin & Botvin, 1992; Kumpfer & Turner, 1990;Tobler et al., 2000), the current study assessed only noninterventionadolescents from a large-scale preventive intervention trial to evaluatenaturally occurring changes and relevant influences on substanceinitiation. Subsequently, when additional waves of data are available,further analyses will evaluate intervention and control differences inchange over time for proposedmediator variables and proposed processesof influence. These analyses will supplement intervention outcomeanalyses conducted earlier that demonstrated support for the efficacy ofthe interventions for substance use outcomes (Spoth, Redmond, Trudeau,& Shin, 2002).
For the current study, constructs were chosen that represent both moredistal intrapersonal influences on substance initiation and more proximalattitudinal influences. The more distal intrapersonal influences weexamined were individual rights assertiveness and decision-makingskills. Individual rights assertiveness is defined as learned, goal-oriented,primarily verbal behavior that increases the likelihood that personal needswill be met in the context of interpersonal relationships (Lazarus, 1973;Wolpe, 1973). Decision-making skills are active strategies to gatherinformation, weigh pros and cons, solve problems, and choose appro-priate actions (Byrnes, 1998). The more proximal attitudinal influences weexamined were negative expectancies and refusal intention. Negativeexpectancies are the perceived negative social and personal consequencesof substance use (Bandura, 1997). Refusal intention is defined as the self-assessed likelihood of refusing or resisting substance offers. Substanceinitiation represents the initiation of one, two, or three substances:cigarettes, alcohol, and marijuana.
Petraitis and colleagues (1995; Petraitis, Flay, Miller, Torpy, & Greiner,1998) described a matrix of substance use etiology integrating severaldevelopmental theories and etiological models. Petraitis and colleagues’matrix identified three types and three levels of influence on substanceuse. Types of influence are cultural and attitudinal (e.g., public policy,conventional values), social and interpersonal (e.g., parental warmth,normative beliefs), and intrapersonal (e.g., temperament, coping skills).Levels of influence are proximal, distal, and ultimate. Intervention effortshave primarily targeted distal and proximal influences, presumablybecause they are more amenable to change than ultimate influences (e.g.,parental divorce, neighborhood climate, biological dispositions).
Petraitis et al. (1995) also suggested that mediational processes relatedto more distal intrapersonal influences have not been explored andthat the role of moderator variables has received little attention. AlthoughPetraitis et al. (1998) acknowledged disagreements regarding the
EARLYADOLESCENT SUBSTANCE INITIATION 303

placement or the ordering of variableswithin their matrix formulation, theorganization of the variables assessed in the current study followed thePetraitis et al. (1995) model.
Petraitis et al. (1995) theorized that intrapersonal constructs such as‘‘inadequate social skills’’ and ‘‘weak academic skills’’ (p. 82) are moredistal influences on substance use. Those constructs correspond to theintrapersonal constructswe evaluated: individual rights assertiveness anddecision-making skills. The Petraitis et al. model’s cultural and attitudinalconstructs posited as more proximal predictors of substance use are‘‘expected costs and benefits of substance use, evaluation of costs andbenefits of substance use, and attitudes toward substance use’’ (p. 82).Negative expectancies and refusal intentions correspond to these moreproximal attitudinal predictors.
Intrapersonal Influences
Assertiveness and decisionmaking have often been explored as protectivefactors in research on substance use (Hawkins, Catalano, & Miller, 1992;Paglia & Room, 1999).1 Although higher levels of assertiveness have beenfound to be negatively associated with adolescent substance use (Epstein,Griffin, & Botvin, 2000; Pentz, 1985), results finding no relationship or apositive relationship with substance use also have been reported (Scheier,Botvin, Diaz, & Griffin, 1999; Wills, Baker, & Botvin, 1989).
Recent findings related to adolescent assertiveness and alcohol useshed some light on these conflicting findings. A study investigatingassertiveness and its relationship to alcohol use and intentions found fivefactors in a commonly used measure of assertiveness (Lillehoj, Spoth, &Trudeau, 2002). One of those factors—individual rights assertiveness—was negatively associated with alcohol use intentions, whereas anotherfactor—social approach assertiveness—was positively associated withboth intentions and current use. These results and related findings(Epstein, Botvin, & Diaz, 1999; Scheier, Botvin, & Baker, 1997; Wills et al.,1989) suggest that the various measures of assertiveness in the literaturemay not have consistently measured the same construct and, furthermore,that various dimensions of assertive behavior differentially affectsubstance use. The current study examined individual rights assertive-ness, which relates to assertive behavior in relatively close relationships.This dimension of assertiveness is relevant to adolescent substance use,which generally takes place within the peer group (Paglia & Room, 1999).
1Assertiveness has been defined as a social or interpersonal competency, rather than anintrapersonal competency, by some authors (e.g., Scheier et al., 1997; Scheier et al., 1999).
304 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

In contrast to assertiveness, decision-making skills have been foundconsistently to protect against substance use. For example, weak decision-making skills have been associated with adolescent cigarette and alcoholuse (Epstein et al., 1999; Scheier & Botvin, 1998). Because of this significantassociation, decision-making skills are frequently included in adolescentsubstance use prevention programs (Tobler et al., 2000), and preventionprograms have been shown to strengthen and improve decision-makingskills (Gersick, Grady, & Snow, 1988). In addition, research has suggestedthat there may be gender differences in decision-making processes andproblem-solving skills, with girls demonstrating higher levels of skill(Radecki & Jaccard, 1996).
Attitudinal Influences
The two relatively more proximal attitudinal influences on substanceinitiation, expectancies and intentions, have also frequently beenexamined in prevention research. Expectancies are considered by social-cognitive and learning theory to be a powerful motivator either to performor to avoid a behavior (Bandura, 1997). Research findings havedemonstrated that expectancies about the affective, behavioral, and socialconsequences of substance use are strong predictors of substance use(Petraitis et al., 1995; Scheier & Botvin, 1997). Intentions have beenclassified as the most immediate proximal predictor of substance use(Petraitis et al., 1995; Petraitis et al., 1998). Cognitive-affective theories ofhealth behavior (Ajzen, 1985) have also posited behavioral intention as themost immediate cause of behavior and the mediator of more distalcognitive influences, such as expectancies and perceived norms.
Mediational Relationships
Research has suggested that individual rights assertiveness and decisionmaking may influence expectancies and refusal intentions, which in turninfluence substance initiation. Regarding individual rights assertivenessand expectancies, research suggests that individuals who lack assertive-ness aremore likely to expect substances to aid in coping, allowing them torelieve stress, increase positive affect, and increase social support (Wills &Shiffman, 1985). Also, earlier research found that individual rightsassertiveness was negatively associated with future intentions to use(Lillehoj et al., 2002), suggesting that individual rights assertiveness alsowould be associated with future refusal intentions. For example, studentswho assessed themselves as highly assertive in interpersonal situations
EARLYADOLESCENT SUBSTANCE INITIATION 305

also would be likely to assess their refusal self-efficacy as high, and refusalself-efficacy would likely be incorporated into a self-assessment of refusalintentions. In addition, students with higher levels of individual rightsassertiveness would likely feel they had the capacity to meet theirinterpersonal needs; therefore, they would not be as likely to feel the needto relieve stress or increase positive affect through the use of substances.Extrapolating from these studies, we hypothesized that individual rightsassertiveness would influence both negative expectancies and refusalintentions.
It also seemed likely that individual rights assertiveness may interactwith both negative expectancies and refusal intentions, such thatindividual rights assertiveness would influence substance initiationdifferently depending on the levels of negative expectancies and refusalintentions. In other words, a higher level of individual rights assertivenesswould be associatedwith a lower level of substance initiation only if levelsof negative expectancies or refusal intentions were relatively high. Weevaluated these potential interactions.
Regarding decision making, findings in previous studies suggest thatdecision-making skills (e.g., weighing alternatives and consideringconsequences) contribute to the decision to use or to refuse substanceoffers (Epstein et al., 1999; Epstein et al., 2000). Also, decision-makingskills related to information processing (gathering relevant information)are used in forming expectancies (Langer, 1996). Based on this research,we hypothesized that decision-making skills would influence bothnegative expectancies and refusal intentions.
Although expectancies influence intentions (Webb, Getz, Baer, &McKelvey, 1999), it is likely that expectancies also exert an independentinfluence on early adolescent substance initiation. In support of thathypothesis, research has shown that early adolescent substance initiationis not entirely planned behavior. In the context of offers by peers,adolescent substance initiation may be independently influenced byexpectancies regarding the immediate social consequences of use orrefusal, in addition to intentions (Gibbons, Gerrard, Ouellette, & Burzette,1998). Therefore, the current study specified negative expectancies asdirectly influencing substance initiation, as well as indirectly througheffects on intentions.
Support for the mediational model is provided by research using thetheory of reasoned action, where intention is specified as the mostimmediate cause of behavior (Sheppard, Hartwick, & Warshaw, 1988).However, research examining expectancies as a mediator of variablesrelated to substance use has been mixed (Ennett & Bauman, 1991;Greenbaum, Brown, & Friedman, 1995;Webb, Baer, Francis, & Caid, 1993).
306 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

Such mixed results suggest that exploration of mediational relationshipsamong the variables that influence substance use should continue withgreater specificity. For example, it is possible that the variables andprocesses that influence substance use may differ depending on theoutcome analyzed, (e.g., initiation, progression, or frequency; varyingsubstance types), or by participants’ age, gender, or other moderators(MacKinnon et al., 1991; Spoth, Redmond, & Shin, 1998).
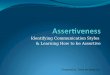
The mediational model to be tested is diagrammed in Figure 1. Wehypothesized that individual rights assertiveness and decision makingwould demonstrate a positive relationship with later negative expectan-cies and refusal intentions, which would in turn show a negativerelationship with substance initiation. Negative expectancies werespecified as contributing to substance initiation directly, as well asindirectly, by influencing refusal intentions. In addition, we hypothesizedthat Time 1 substance initiation would negatively influence Time 2negative expectancies and refusal intentions. A reciprocal relationship ispredicted by social-cognitive learning theory (Bandura, 1997), wherebehavior at an initial assessment affects cognitions at a later assessment,and cognitions, in turn, affect later behavior. This reciprocity has beenempirically demonstrated for substance use behavior and expectancies(Scheier & Botvin, 1997).
Moderating Influences
Research has found gender differences in substance initiation, with boysdisplaying both higher rates and earlier initiation than girls (Johnston
T1 T2 T3
Decision-makingSkills
+
+
+
_
_
_
_
+
_
+
+ Substance Initiation
+
Substance Initiation
Individual RightsAssertiveness
Negative Expectancies
Refusal Intentions
_
FIGURE1 Hypothesized mediational model.
EARLYADOLESCENT SUBSTANCE INITIATION 307

et al., 1996, 2002). Gender differences also have been found in the strengthand pattern of relationships among some predictors of substance use (e.g.,stress was more associated with substance use among early adolescentgirls than boys and early conduct problemsweremore strongly associatedwith later marijuana use among girls; Pedersen, Mastekaasa, & Wich-strom, 2001). Because evidence of differing influences on substanceinitiation for boys and girls could be important to prevention programdevelopers and implementers, the current study evaluated genderdifferences in descriptive statistics and the pattern of relationships amongthe variables.
METHOD
Participants
Participants in the study were seventh graders at the time of pretestingenrolled in 36 rural schools in 22 counties in a Midwestern state. Arandomized block design guided the assignment of the schools withineach block into one of the three experimental conditions: (a) thosereceiving the 15-session in-school classroom-based Life Skills TrainingProgram (LST; Botvin, 1996, 2000); (b) those receiving the LST plus theseven-session family-focused Strengthening Families Program: ForParents and Youth 10–14 (SFP 10–14; Molgaard, Kumpfer, & Fleming,1997); or (c) those receiving minimal contact in a control condition. At thetime they were recruited into the study, schools did not know theexperimental condition to which they would be assigned. Only the controlcondition students were selected for this analysis.
All seventh-grade students in participating schools were recruited forparticipation. A total of 494 students (93% of eligible students) in the 12schools assigned to the control condition completed the baseline (T1)assessment conducted when the students were in the first semester ofseventh grade. Posttest (T2) assessments approximately 6 months after T1were conductedwith 463 (94%) of the students. Of these, 416 (90% of thoseposttested) students completed a 1 1/2-year follow-up (T3) assessment.The retention rate from T1 to T3 was 84%. On average, 41 students in eachschool completed the T1 assessment. Their average age was 12.3 years.Slightly more than half of the students were male (51%), and the majoritywere Caucasian (97%). Approximately 77% lived with both biologicalparents, and approximately 23% qualified for free or reduced-cost schoollunches. Only students with complete information on the study measureswere included in the analyses.
308 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

Procedure
The data collectionwas conducted in classrooms by a two- or three-personresearch team during regular school periods. A consent procedureallowed parents to decline participation for their adolescent, andadolescents could also decline on their own behalf. Participation ratesdid not differ by intervention condition. Students were assured, bothverbally and in writing, that their responses to the questionnaires wouldbe kept confidential. In addition, each student exhaled into a balloon thatwas connected to a carbon monoxide (CO) meter to provide a CO readingand to serve as a ‘‘bogus pipeline’’ to enhance validity in answering thesmoking-related questions. This procedure provides an independent andobjective physiological measure to compare with the adolescent’s self-report and is frequently used to increase the truthfulness of self-reportedsmoking behavior (Jones & Sigall, 1971; Murray, O’Connell, Schmid, &Perry, 1987). Studentswere told that CO readings could be used to validateself-reports. The same procedures were employed in each data-collectionwave. For the current study, CO readings were not evaluated or correlatedwith smoking self-reports, primarily because the readings wouldonly validate recent smoking, and our measure was a lifetime-usemeasure.
Measures
To assess individual rights assertiveness, six items were derived from theGambrill and Richey Assertion Inventory (1975) and were modified to besuitable for adolescents (Wills et al., 1989). Previous research hasdemonstrated the validity of the factor structure of the original inventoryand provided support for the scale integrity of a reduced set of items (Willset al., 1989). A principal components exploratory factor analysisconducted on the modified 15-item inventory revealed four factors,including the dimension of individual rights assertiveness representing anadolescent’s willingness to express assertiveness skills in relatively closeinterpersonal relationships. The individual rights assertiveness scale hasbeen used in previous research to predict adolescent substance intentionand use (Lillehoj et al., 2002; Scheier & Botvin, 1998). The scale included sixitems, such as: ‘‘Say ‘no’ when someone asks you to do something youdon’t want to do,’’ and ‘‘Say ‘no’ when someone wants to copy yourhomework.’’ Responses were on a 5-point scale ranging from 1 (definitelywould) to 5 (definitely would not). Responses were rescaled so that higherscores represented a greater level of individual rights assertiveness.
EARLYADOLESCENT SUBSTANCE INITIATION 309

Reliability at T1 was a5 .78. The six items were combined into threeparcels and specified as indicators of the individual rights assertivenessconstruct for the structural equation modeling (SEM) analyses.2
Decision making was measured with a 7-item scale derived from amodified 35-item version of the Coping Assessment Battery (Bugen &Hawkins, 1981). A factor analysis of the measure with a sample ofadolescents revealed a 7-item decision-making dimension that assessedskills related to decision making through active strategies to gatherinformation, make decisions, and solve problems. The 7-item decisionmaking scale has been used extensively in previous research to predictadolescent substance use (Botvin, Griffin, Diaz, & Ifill-Williams, 2001;Epstein et al., 1999; Wills, 1986). The stem for all 7 items was ‘‘When I havea problem, I y’’ Items included: ‘‘y think about what information isnecessary for dealing with the problem’’ and ‘‘y. think about choices thatexist before I take any action.’’ Responses were scored on a 5-point scaleranging from 1 (never) to 5 (always). Reverse-scored items were rescaled sothat higher scores represented more effective decision-making skills.Reliability at T1 was a5 .92. Items were combined into three parcels forthe SEM analyses.
Negative expectancies included negative outcome expectancies relatedto three substances: cigarettes, alcohol, and marijuana. Items wereadapted from a questionnaire to assess beliefs regarding the social andpersonal consequences of substance use (Epstein et al., 1999; U.S. PublicHealth Service, 1974) and are similar to expectancy items frequentlyassessed in adolescent substance use research (MacKinnon et al., 1991;Scheier & Botvin, 1997). Five items relating to cigarettes and marijuanaand eight items relating to alcoholwere included. All itemswere scored ona 5-point scale ranging from 1 (strongly disagree) to 5 (strongly agree).Examples include: ‘‘Kids who [smoke, drink, use marijuana] have morefriends,’’ ‘‘[Smoking cigarettes, drinking alcohol, using marijuana] is agood way of dealing with your problems,’’ and ‘‘Kids who drink alcoholact crazy or stupid.’’ Items were rescaled and averaged so that a higherscore represented a more negative expectancy regarding substance use.Alpha reliabilities at T2 were .91 for the Cigarette subscale, .78 for the
2Combining individual items from a longer scale into parcels reduces the number ofestimated parameters, which is advantageous for smaller samples. In addition, the parcels maybe more strongly related to the latent factors, as they are less influenced by wording and othermethod effects. Except in very small samples, parceling does not have negative effects onmodelconvergence or proper solution (Marsh & Hau, 1999). Item parcels were created using factorloadings from unidimensional constructs. Items with similar communalities were combined toform the parcels; parcels produced similar factor loadingswithin constructs (Bandalos & Finney,2001).
310 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

Alcohol subscale, and .80 for the Marijuana subscale. Scores on the threemeasures were used as indicators of the expectancy construct for the SEManalyses.
Refusal intention was assessed with two scales. The first scale, adaptedfrom a modified version of the Gambrill and Richey Assertion Inventory,assessed refusal intention for offers of specific substances. The item stemwas ‘‘How likely are you to handle these situations in this way?’’Responses identified whether the respondent would say no when askedby someone to try cigarettes, alcohol, or marijuana. Items were scored on a5-point scale ranging from 1 (definitely would say no) to 5 (definitely wouldnot say no). Reliability at T2 was a5 .82. The second scale assessedintentions regarding substance resistance strategies and included fiveitems measured on a 5-point scale assessing responses to offers ofsubstances ranging from 1 (definitely would) to 5 (definitely would not).Responses included: ‘‘Tell them ‘not now,’’’ ‘‘Change the subject,’’ and‘‘Make up an excuse and leave.’’ Reliability at T2 was a5 .85. The twoscales were used as indicators for the refusal intentions construct in theSEM analyses.
The substance initiation index was constructed by combining threedichotomous items regarding the lifetime use of cigarettes, alcohol, andmarijuana. Participants were asked if they had ever ‘‘had a drink ofalcohol,’’ ‘‘smoked a cigarette,’’ or ‘‘smoked marijuana.’’ Responses werecoded 0 for ‘‘no’’ and 1 for ‘‘yes’’ and summed to compute the scale. Foreach wave of data, responses were corrected for consistency, so that if anindividual answered ‘‘yes’’ at any time, the subsequent response to thesame question was also coded ‘‘yes.’’ Scores ranged from 0 (no substanceuse) to 3 (initiation of all three substances). Test–retest reliability between T1and T2was r5 .76. Because the scale was composed of dichotomous items,reliability was also assessedwith the Kuder-Richardson (KR20) formula at.44 at T1 and .55 at T3. Reliability and validity of self-reported substanceuse for purposes of similar types of studies have been previouslyevaluated and considered acceptable (Murray et al., 1987; Oetting &Beauvais, 1990). Prior studies have reported the use and validity of similarsubstance use indexes (Han, McGue, & Iacono, 1999; Spoth, Redmond, &Shin, 2001; Spoth et al., 2002). This index was used as a single indicator ofsubstance initiation in the SEM analyses.
Distributional characteristics of the variables were nonnormal. Thesubstance initiation indexwas positively skewed at T1. That is, most of thestudents identified no or low levels of substance initiation; however,the distribution was less skewed at T3. The other variables all showednegative skew; that is, most of the students identified high levelsof individual rights assertiveness, decision-making skills, negative
EARLYADOLESCENT SUBSTANCE INITIATION 311

expectancies, and refusal intentions. Because of these distributionalcharacteristics, supplemental analyses were conducted to address theseviolations of normality.
Data Analyses
Because students were nested within schools, analyses were conducted toassess the need for multilevel analyses. Attrition analyses were alsoconducted to determine whether study dropouts from T1 to T2 and fromT2 to T3 differed on substance initiation status. Analyses were conductedto evaluate interactions between individual rights assertiveness and bothnegative expectancies and refusal intentions before SEM analyses. Next,SEM was used to assess the relationships among the variables. Aconfirmatory factor analysis (CFA) evaluated the factor loadings for themeasured indicators and the overall fit of the model. The next step was totest the proposed mediational model to determine whether the modeladequately described the sample data. Then, gender differences wereevaluated for themodel constructs andmultigroup SEM evaluated genderdifferences in the pattern of relationships among the variables. Finally,because the data were not normally distributed, supplemental analyseswere conducted to address nonnormality.
RESULTS
School-Level Effects
The intraclass correlations, evaluating the relationship between theschool-level error term as a random variable and the individual-levelerror term, ranged from r5 .02 to r5 .10 across variables. Additionally, amultivariate analysis of variance (MANOVA) determined that the overallschool-level effect on the model variables at the initial assessment wassignificant, F(132, 4653)5 1.65, po.001. Although the intraclass correla-tions were not large, we concluded that analyses controlling for themultilevel effects were the most appropriate choice (Bryk & Raudenbush,1992; Snijders & Bosker, 1999).
Attrition Effects
Attrition analyses were conducted using analysis of variance (ANOVA)and chi-square analyses for dropouts on the substance initiation index anddemographic measures at both T2 and T3. Students who dropped out
312 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

between T1 and T2 (n5 29) had significantly higher scores on thesubstance initiation index, F(1, 469)5 18.85, po.001 (2 students moved,changing conditions between T1 and T2 andwere also eliminated from theanalyses). In addition, students who dropped out between T2 and T3(n5 47) also had significantly higher scores on the substance initiationindex at T2, F(1, 450)5 6.50, po.05. Further analyses revealed thatstudents who dropped out following T1 were more likely to live in single-parent households, w2(1, N5 486)5 7.04, po.01, and to receive free orreduced price school lunches, w2(1, N5 452)5 8.34, po.01. These resultssuggest that the students who dropped out of the study assessmentstended to be at greater risk for substance use and other problem behaviorsthan those remaining in the study.
Continuous Variable Interactions
Analyses were conducted evaluating the interactions between individualrights assertiveness and both negative expectancies and refusal intentionsusing regressionwith SAS PROCMIXED to control for the clustered natureof the sample (Singer, 1998). We determined that a regression model withinteractions using manifest variables should be tested before examininginteractions using SEM. There are many complexities involved whenmodeling continuous variable interactions using SEM (Jaccard & Wan,1996), and our sample sizewas not large; therefore,wewanted to determinewhether interactions were likely to be significant before addressing suchcomplexities.We standardized the variables andmodeled regression effectson the T3 substance initiation index, using the T1 substance initiation indexas a control variable. Models were estimated separately to test theinteraction of individual rights assertiveness with negative expectanciesand the interaction of individual rights assertiveness with refusalintentions. A model that included all variables and both interactions wasalso tested. None of the interactions was significant; therefore, continuousvariable interactions were not modeled in the SEM.
Mediational Model
SEM was conducted with LISREL 8.30 (Joreskog & Sorbom, 1996) usingmaximum likelihood (ML) estimation to evaluate the relationships amongthe variables. The analyses controlled for the effects of the clustered natureof the sample by using the pooled within-variance/covariance matricesfrom the MANOVA as input matrices for SEM analyses (Muthen &Satorra, 1995; SPSS Incorporated, 1988).
EARLYADOLESCENT SUBSTANCE INITIATION 313

Individual rights assertiveness, decision making, negative expectancies,and refusal intentions were all specified as latent variables with multipleindicators (see descriptions in the Measures section). The substanceinitiation index was a single indicator scale with the error term constrainedto zero. The mediating latent variables, negative expectancies and refusalintentions, were assessed at T2. The T1 substance initiation index was usedas a control variable so that effects of the predictor variables on T3 substanceinitiation could be interpreted as effects on changes in substance initiationfrom the T1 assessment (i.e., students who began using one or moresubstances or who used additional substances between T1 and T3). Pathsfrom T1 substance initiation to negative expectancies and refusal intentionsalso were specified. A CFA was conducted for the six-factor model. Thecorrelation matrix, means, and standard deviations of the variables used intesting the model are presented in Table 1. The indicators for each constructare more strongly intercorrelated than they are correlated with otherconstructs, suggesting both convergent and discriminant validity for thestudy constructs. Factor loadings and interfactor correlations are presentedin Table 2. As can be seen by the interfactor correlations, all four predictorvariables had significant negative zero-order correlations with thesubstance initiation index; all the predictor variables were significantlypositively correlated with each other. The measurementmodel provided anacceptable fit to the data, w2(52, N5 357)5 76.99, po.01, goodness-of-fitindex (GFI)5 .97, comparative fit index (CFI)5 .99, root mean square errorof approximation (RMSEA)5 .04, Hoelter’s critical N (CN)5 364.51.
Next, the structural model was tested. Individual rights assertivenessand decision making were specified as correlated exogenous variableswith pathways to negative expectancies and refusal intentions. Negativeexpectancies were specified as influencing the T3 substance initiationindex directly and indirectly through refusal intentions. A pathway fromrefusal intentions to the substance initiation index was specified. Thestructural model proved a good fit, w2(54, N5 357)5 77.71, po.02,GFI5 .97, CFI5 .99, RMSEA5 .04, CN5 372.41. An alternative modelthat added direct effects from individual rights assertiveness and decisionmaking to T3 substance initiation was not a significant improvementover the fully mediated model, Dw2(2)5 0.72, po.70. (See Figure 2 forstandardized coefficients and t values.)
Individual rights assertiveness and decision making were significantpredictors of negative expectancies, but neither was directly related torefusal intentions. However, the indirect effects through negativeexpectancies of both individual rights assertiveness (b5 .17, po.001) anddecision making (b5 .10, po.05) on refusal intentions were significant. Ashypothesized, T1 substance initiation had a significant effect on negative
314 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

TABLE
1
Means,StandardDev
iations,an
dCorrelationsfortheModel
Variables
Measure
12
34
56
78
910
1112
13
Individual
rights
assertiven
ess
1.Parcel1
1.00
2.Parcel2
0.59
1.00
3.Parcel3
0.48
0.47
1.00
Decisionmak
ing
4.Parcel1
0.16
0.25
0.19
1.00
5.Parcel2
0.18
0.26
0.16
0.81
1.00
6.Parcel3
0.17
0.24
0.20
0.82
0.75
1.00
7.Substan
ceinitiationT1
�0.10
�0.11
�0.18
�0.23
�0.22
�0.22
1.00
8.Smokingexpectancy
0.11
0.15
0.21
0.22
0.19
0.17
�0.23
1.00
9.Drinkingexpectancy
0.25
0.23
0.28
0.22
0.20
0.18
�0.26
0.48
1.00
10.Marijuan
aexpectancy
0.14
0.12
0.12
0.20
0.16
0.18
�0.22
0.41
0.51
1.00
11.Refusal
0.14
0.20
0.23
0.20
0.20
0.15
�0.39
0.44
0.48
0.32
1.00
12.Resistance
0.06
0.12
0.13
0.20
0.19
0.16
�0.27
0.31
0.25
0.18
0.53
1.00
13.Substan
ceinitiationT3
�0.12
�0.07
�0.28
�0.24
�0.20
�0.23
0.63
�0.27
�0.34
�0.32
�0.41
�0.24
1.00
Mean
4.32
4.41
4.29
3.56
3.43
3.53
0.60
4.76
4.32
4.59
4.59
4.20
1.18
Standarddev
iation
0.72
0.67
0.86
0.97
1.00
0.98
0.72
0.50
0.64
0.61
0.78
0.75
0.90
Note.
N5
357.
CorrelationsX.07o.13|po
.05|
X.13o
.17|po
.01|
X.17|po
.001
|.
Significan
celevelspo
.05in
bold.
EARLYADOLESCENT SUBSTANCE INITIATION 315

TABLE 2
Factor Loadings and Interfactor Correlations for the Model
Factor Factor Loadings 1 2 3 4 5 6
1. Individual rights assertiveness 1.00
Parcel 1 0.75
Parcel 2 0.76
Parcel 3 0.61
2. Decision making 0.34 1.00
Parcel 1 0.94
Parcel 2 0.85
Parcel 3 0.86
3. T1 Substance initiation 1.00 � 0.13 � 0.25 1.00
4. Negative expectancies 0.36 0.30 � 0.31 1.00
Smoking 0.64
Drinking 0.79
Marijuana 0.64
5. Refusal intentions 0.23 0.25 � 0.43 0.68 1.00
Refusal 0.88
Resistance 0.51
6. T3 Substance initiation 1.00 � 0.14 � 0.23 0.60 � 0.42 � 0.34 1.00
Note. N5 357. Correlationso.15 |po.05|X.15o.25 |po.01|X.25 |po.001|.
Significance levels po.05 in bold.
T1 T2 T3
FIGURE 2 Latent variable model predicting substance initiation.
316 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

expectancies and refusal intentions, in addition to a highly significantstability coefficient for the substance initiation index from T1 to T3.3
Negative expectancies exerted a significant direct effect on the T3substance initiation index, whereas refusal intentions did not. The modelexplained 43% of the variance in the T3 substance initiation index. Theindirect effects of individual rights assertiveness and decision making onT3 substance initiation index were significant (bs5 –.08 and –.04, pso.05,respectively).4
Gender Differences
Gender differences on the variable means were first evaluated with t tests(see Table 3). Girls were lower on T1 substance initiation index than boys;girls were higher on T1 decision making than boys. None of the othervariable means was significantly different across gender. Second, genderdifference in the pattern of relationships among the variables wasevaluated with multigroup SEM. Factor loadings were constrained toequality between the two groups.5 Structural pathways for boys and girls
3 Because both negative expectancies and refusal intentions are theoretically proximal orimmediate precursors to substance initiation, measuring substance initiation at the same timepointmay demonstratemore immediacy. Therefore, an alternativemodelwas estimatedwith T2substance initiation index, rather than T3 substance initiation index, as the outcome variable.This model demonstrated the same pattern of path coefficients, with a significant directpathway from T2 negative expectancies to T2 substance initiation index and a nonsignificantpathway from T2 refusal intentions to T2 substance initiation index.
4 To test alternate causal ordering, we simplified our models by specifying single indicatorsmeasured with error ((1� a) n variance) for all of the variables, with the exception of substanceinitiation index. Substance initiation index was again specified as measured without errorbecause an accurate estimate of error could not be assessed easily for a count variable. We thentested an alternate causal ordering for the T1 to T2 variables, with stabilities for all of thevariables included. In other words, we first specified a model with our original causal order—paths from T1 assertiveness and decision making to T2 negative expectancies and refusalintentions—and an alternative model—paths from T1 negative expectancies and refusalintentions to T2 assertiveness and decision making. Although the models cannot be statisticallycompared because they are not nested, the model specifying the alternative causal orderingshowed a relatively poorer fit to the data, w(14)
2 5 40.59, po.001, CFI5 .97, RMSEA5 .07,CN5 267.40, compared with the originally ordered model, w(14)
2 5 22.83, po.06, CFI5 .99,RMSEA5 .04, CN5 474.52. The difficulty of clearly determining causal ordering has often beendiscussed, and cross-lagged models are not necessarily determinant. It is crucial to considertheory, rather than statistics alone, in determining causal ordering (Rogosa, 1995).
5 Testing tau equivalence for the factor loadings between boys and girls demonstrated thatfive of the seven parameters were equivalent, whereas two were not. Nevertheless, we assumedmeasurement invariance to test a more restrictive model. Assuming measurement equivalenceis theoretically sound because it defines the latent variables as identical between groups.Constraining the factor loadings to equality for five rather than seven parameters resulted inessentially the same results as in the fully constrained model. For the structural model genderequivalence tests, w2 values were generally larger in the less constrained model.
EARLYADOLESCENT SUBSTANCE INITIATION 317

were constrained to equality in one model and allowed to vary in another,and the difference in chi-square results between models was compared.Differences were significant, Dw2(10)5 30.28, po.001 (see Figure 3). Inaddition to the overall difference in the structural parameters, differencesin individual parameters were evaluated. Significant gender moderationwas found in the paths from T1 substance initiation to T2 negativeexpectancies, Dw2(1)5 4.03, po.05; T1 substance initiation to T2 refusalintentions, Dw2(1)5 4.98, po.05; and T2 refusal intentions to T3 substanceinitiation, Dw2(1)5 13.68, po.001. Gender moderation of the path from T2negative expectancies to T3 substance initiation failed to reach significance,Dw2(1)5 1.85, p5 .18. These results suggest that the pattern of influences onsubstance initiation is different for girls and boys. Levels of T1 substanceinitiation are more strongly negatively related to levels of T2 negativeexpectancies and refusal intentions for boys than for girls; levels of T2refusal intentions are significantly and negatively related to T3 substanceinitiation for girls but not for boys.6
TABLE 3
Means, Standard Deviations, and Mean Differences of the Variables by Gender
Measure Mean SD t-value
T1 Individual rights assertiveness
Boys 4.34 0.64
Girls 4.35 0.59 0.13
T1 Decision-making skills
Boys 3.41 0.94
Girls 3.61 0.87 2.00
T1 Substance initiation
Boys 0.68 0.71
Girls 0.51 0.73 2.21
T2 Negative expectancies
Boys 4.52 0.48
Girls 4.60 0.46 1.60
T2 Refusal intentions
Boys 4.35 0.68
Girls 4.44 0.56 1.37
T3 Substance initiation
Boys 1.26 0.83
Girls 1.09 0.97 1.81
Note. N5 187 boys; N5 170 girls. Significance levels po.05 in bold.
6Variance–covariance matrices for the models are available from the first author.
318 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

Violations of the Normality Assumption
Nonnormal distribution of variables in SEM can lead to w2 goodness-of-fittests that reject toomany truemodels and tests of parameter estimates thatare biased, leading to too many significant results (Russell, 2002; West,Finch, & Curran, 1995). Because of the skew in the model variables,various transformations were conducted and evaluated to addressthis issue. The greatest improvement in multivariate normality wasobtained by reversing the scores on the variables (highest value of thescale plus one minus the individual score) and using log base 10transformations (Kline, 1998). Because the substance initiation indexscores were less skewed than the other variables, multivariate skewnesswas closer to normal when the substance initiation index was nottransformed. With the transformed variables, multivariate skewness wasdecreased from a z score of 43.17 to a z score of 20.30—still a highlysignificant departure from normality. The z scores for individualtransformed variables ranged from 2.12 to 4.25. Results found that modelsevaluated with transformed data varied only slightly from the modelswith nontransformed data. Significant gender differences in modelpathways also were found in the model with transformed data. Althoughthe ML estimator is relatively robust to violations of normality with largersample sizes (Bollen, 1989), we also tested our models using the scaled w2
FIGURE 3 Latent variable model predicting substance initiation by gender.
EARLYADOLESCENT SUBSTANCE INITIATION 319

statistic with robust standard errors (Satorra & Bentler, 1994). Resultsreplicated the pattern of relationships among the variables and thesignificance of model parameters; in addition, the fit of the modelsimproved.7
DISCUSSION
The purpose of the current study was to evaluate mediational relation-ships between more distal intrapersonal influences and relatively moreproximal influences on substance initiation, as well as to evaluatepotential differences in influence processes between boys and girls(Petraitis et al., 1995; Petraitis et al., 1998). To elucidate the psychologicalprocesses linking assertiveness and decision making to substanceinitiation, structural models with mediational pathways were tested,and gender differences in mean levels of the variables, as well as theprocesses of influence, were evaluated.
Because previous research has demonstrated that influences onsubstance use may vary across developmental stages, the current studyevaluated mediational processes in a group of young adolescents. Earlyadolescence is the time when substance use typically begins (Johnstonet al., 1996) and is a period of rapid change, including cognitive advances(Keating, 1990), changes in peer relationships (Brown, 1990), and exposureto peer offers of substances (Johnston et al., 1996). Therefore, it isimportant to study influences on substance initiation during this time. Thenegative effects of early substance initiation, including concomitant andsubsequent increases in other problem behaviors (Hawkins et al., 1992;Riggs & Whitmore, 1999) and an increased likelihood of developingsubstance abuse problems in adulthood (Grant & Dawson, 1997) suggestthat delaying substance initiation is an important goal. Empirical supportfor the gateway theory (Kandel, Yamaguchi, & Chen, 1992) has found thatinitiation typically progresses in stages, with earlier initiation of tobacco oralcohol, or both, and later progression to marijuana and other drugs.
For young adolescents, our findings suggested that individual rightsassertiveness and decision-making skills were positively associated withnegative expectancies and refusal intentions, directly or indirectly. In turn,negative expectancies and refusal intentions were negatively associatedwith substance initiation (although findings were mixed with respect to
7Models were estimated using the EQS Program (Bentler & Wu, 1995). This programprovides the scaled w2 statistic and robust standard errors, but has no method to control for theeffects of intraunit dependency (clustering).
320 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

the influence of refusal intentions on subsequent substance initiation).This is consistent with earlier findings in which similar constructs, such asrefusal assertiveness and alcohol expectancies, mediated the effects ofintrapersonal variables on substance use (Epstein et al., 2000; Scheier &Botvin, 1997, 1998). Consistent with Scheier and Botvin (1997) and Webbet al. (1993), negative expectancies were influenced by individual rightsassertiveness, decision-making skills, and earlier levels of substanceinitiation; negative expectancies also contributed to the variance in refusalintentions. These mediational processes were the same for boys and girls,although girls demonstrated significantly higher levels of decision-making skills in the fall semester of seventh grade than boys, as well aslower levels of substance initiation.
We also evaluated potential interactions between individual rightsassertiveness and both negative expectancies and refusal intentions.Clearly, higher levels of individual rights assertiveness were associatedwith higher levels of later negative expectancies and refusal intentions,but there was no evidence that higher levels of individual rightsassertiveness were associated with lower rates of increase in substanceinitiation only among students with higher levels of negative expectanciesor refusal intentions. The lack of interactions can perhaps be explained bythe limited variability in the constructs examined; also, the variablesdemonstrated a high degree of negative skew. In addition, varyingdimensions of assertiveness have not been extensively explored, and it islikely that other assertiveness dimensions would be associated withnegative expectancies, refusal intentions, and substance initiation indiffering ways.
Drawing conclusions regarding the influence of negative expectanciesand refusal intentions on substance initiation is less straightforward thanthe findings discussed earlier. Overall, students with more negativeexpectancies regarding substance use during spring semester of seventhgrade were less likely to report increases in substance initiation betweenfall semester of seventh grade and spring semester of eighth grade,whereas students’ levels of intentions to refuse offers of substance usein that same period did not affect subsequent change in substanceinitiation. Further analysis found results differed by gender. Girls withhigher levels of refusal intentions during the spring semester of seventhgrade were less likely to report increases in substance initiation. However,for boys, levels of refusal intentions were not related to changes insubstance initiation.
Across time, the process of influence was different for boys and girlswith regard to the effects of refusal intentions on change in substanceinitiation; however, it is important to note that the level of refusal
EARLYADOLESCENT SUBSTANCE INITIATION 321

intentions did not differ between genders. One possible explanationfor the difference in influence patterns between boys and girls may berelated to increases in exposure to peer substance use, a likely resultof change in social and interpersonal factors during this time frame(Brown, 1990; Johnston et al., 1996). For example, during fall semester ofseventh grade, 70% of the participants thought that less than half of peopletheir own age drank alcohol; by spring semester of eighth grade, only 43%endorsed that response. As they progress through the middle schoolyears, boys may be influenced more strongly than girls by peer substanceoffers in risk-conducive social situations (see Gibbons et al., 1998). Peerpressure to use substances is more intense for boys because substance useis often perceived as ‘‘macho’’ behavior (Brown, 1982).
In contrast, perhaps the earlier maturation of girls, especially in social-cognitive functioning andmoral development (Silberman& Snarey, 1993),allows girls’ actions to align more closely with their intentions, even aspeer substance offers increase. In addition, results suggest that boysinitiate substances earlier and, furthermore, that early levels of initiationare more likely to lead to later decreases in negative expectancies andrefusal intentions for boys than for girls, placing boys at greater risk forsubsequent initiation of additional substances.
Results suggest that individual rights assertiveness and decision-making skills are important constructs related to substance initiation andshould continue to be promoted as components of prevention programs.Regarding individual rights assertiveness, it is likely that bolstering thisskill, specifically the ability to say no to inappropriate requests, willencourage young adolescents to refuse substance offers. In addition to thecurrent study, earlier research also has found that individual rightsassertiveness, in contrast to social assertiveness, is negatively associatedwith substance use intentions (Lillehoj et al., 2002). This suggests thatprevention program strategies for young adolescents should emphasizecontent related to individual rights assertiveness rather than focusing oncontent related to social approach assertiveness (e.g., overcomingshyness).
Results also suggest that prevention program components related todecision-making skills should be presented to young adolescents. The useof these strategies should be strongly encouraged, especially in risk-conducive social situations. Because decision-making skills appear to beless developed in boys, it may be important to place stronger program-matic emphasis on decision-making skills for boys.
In addition, findings from this study suggest initiation begins earlierfor boys and has a greater degree of negative consequences (i.e., effectson later negative expectancies and refusal intention). These findings
322 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

highlight the importance of appropriate developmental timing ofpreventive interventions, especially for boys.
There are several limitations to be kept in mind regarding the study.First of all, the study was conducted in rural Midwestern communitiesamong primarily Caucasian students. Approximately 77% livedwith bothbiological parents and approximately 23% qualified for free or reducedcost school lunch. Generalizations to populations with different demo-graphic compositions should be made with caution. Also, students whodropped out of the study were significantly more likely to have usedsubstances, to live in single-parent or stepparent households, and to havea lower socioeconomic status (i.e., school lunch program participation).Study loss of these more higher risk students may have biased results.Nevertheless, given the range of substance initiation and demographiccharacteristics that were evaluated with the available data, it is unlikelythat the pattern of results reported was highly biased. In addition, allmeasures were self-reported. Although self-reports are the most appro-priate measures for cognitive variables, such as negative expectancies andrefusal intentions, self-reported measures of behavior would be bolsteredwith the addition of multiple reporters. Nevertheless, self-reportedmeasures of substance use for this age group have been found to bereliable in past research, especially when bogus-pipeline procedures havebeen used with regard to smoking (Murray et al., 1987; Oetting &Beauvais, 1990; Pechacek et al., 1984). In addition, different influencepatterns may be found for different outcome variables (e.g., substancefrequency, varying individual substances).
A further limitation is suggested by the nonnormality of the assessedvariables. As is usually true of young adolescents, rates of substanceinitiation, alongwith scores on the scales of correlates and predictors, werenot normally distributed. Nevertheless, evaluation of models withtransformed variables that attenuated the nonnormality found essentiallysimilar results, demonstrating the same main effects and gendermoderation as models with nontransformed variables. However, werethe scores on the variables more normally distributed, it is likely that thestrengths of the relationships detected in the models could be moreaccurately evaluated (Bollen, 1989).
As data become available, planned analyses will evaluate the effects ofthe LST school-based and SFP 10–14 family-focused interventions onprogram mediators and mechanisms of program effectiveness. Futureanalyses will extend evaluations of intervention-related changes that havebeen demonstrated to date (Spoth et al., 2002).
EARLYADOLESCENT SUBSTANCE INITIATION 323

ACKNOWLEDGMENT
Work on this paper was supported by Grant DA 10815 from the NationalInstitute on Drug Abuse.
REFERENCES
Ajzen, I. (1985). From decisions to actions: A theory of planned behavior. In J. Kuhl, & J.Beckmann (Eds.),Action-control: From cognition to behavior (pp. 11–39). NewYork: Springer.
Ausubel, D. P., Montemeyor, R., & Svajian, P. N. (1977). Theory and problems of adolescentdevelopment. New York: Grune & Stratton.
Bandalos, D. L., & Finney, S. J. (2001). Item parceling issues in structural equation modeling.In G. A. Marcoulides, & R. E. Schumacker (Eds.), New developments and techniques instructural equation modeling (pp. 269–296). Mahwah, NJ: Erlbaum.
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. EnglewoodCliffs, NJ: Prentice-Hall.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: Freeman.Bentler, P. M., & Wu, E. J. C. (1995). EQS for Windows: User’s guide. Encino, CA: Muiltivariate
Software.Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley.Botvin, G. J. (1996). Life skills training: Promoting health and personal development. Princeton, NJ:
Princeton Health Press.Botvin, G. J. (1999). Adolescent drug abuse prevention: Current findings and future
directions. In M. D. Glantz, & C. R. Hartel (Eds.), Drug abuse: Origins & interventions (pp.285–308). Washington, DC: American Psychological Association.
Botvin, G. J. (2000). Life skills training. Princeton, NJ: Princeton Health Press.Botvin, G. J., & Botvin, E. M. (1992). Adolescent tobacco, alcohol, and drug abuse: Prevention
strategies, empirical findings, and assessment issues. Developmental and BehavioralPediatrics, 13, 290–301.
Botvin, G. J., Griffin, K.W., Diaz, T., & Ifill-Williams,W. (2001). Drug abuse prevention amongminority adolescents: Posttest and one-year follow-up of a school-based preventiveintervention. Prevention Science, 2, 1–13.
Brown, B. B. (1982). The extent and effects of peer pressure among high school students: Aretrospective analysis. Journal of Youth and Adolescence, 11, 121–133.
Brown, B. B. (1990). Peer groups and peer cultures. In S. S. Feldman, & G. R. Elliott (Eds.), Atthe threshold: The developing adolescent (pp. 171–196). Cambridge, MA: Harvard UniversityPress.
Brown, B. B., Dolcini, M. M., & Leventhal, A. (1997). Transformations in peer relationships atadolescence: Implications for health-related behavior. In J. Schulenberg, J. Maggs, & K.Hurrelmann (Eds.),Health risks and developmental transitions during adolescence. Cambridge,England: Cambridge University Press.
Bryk, A. S., & Raudenbush, S.W. (1992).Heirarchical linear models: Applications and data analysismethods. Newbury Park, CA: Sage.
Bugen, L. A., & Hawkins, R. C., (1981). Coping Assessment Battery. Unpublished manuscript.Buhrmester, D. (1996). Need fulfillment, interpersonal competence, and the developmental
contexts of early adolescent friendship. In W. Bukoski, A. Newcomb, &W. Hartup (Eds.),The company they keep (pp. 158–185). New York: Cambridge University Press.
324 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

Byrnes, J. P. (1998). The nature and development of decision making: A self-regulation model.Mahwah, NJ: Erlbaum.
Dishion, T. J., Capaldi, D. M., & Yoerger, K. (1999). Middle childhood antecedents toprogressions in make adolescent substance use: An ecological analysis of risk andprotection. Journal of Adolescent Research, 14, 175–205.
Dryfoos, J. (1990). Adolescents at risk: Prevalence and prevention. New York: Oxford UniversityPress.
Ennett, S. T., & Bauman, K. E. (1991). Mediators in the relationship between parental and peercharacteristics and beer drinking by early adolescents. Journal of Applied Social Psychology,21, 1699–1711.
Entwistle, D. (1990). Schools and the adolescent. In S. S. Feldman, & G. R. Elliott (Eds.), At thethreshold: The developing adolescent (pp. 171–196). Cambridge, MA: Harvard UniversityPress.
Epstein, J. A., Botvin, G. J., & Diaz, T. (1999). Social influence and psychological determinantsof smoking among inner-city adolescents. Journal of Child & Adolescent Substance Abuse, 8,1–19.
Epstein, J. A., Griffin, K. W., & Botvin, G. J. (2000). Role of general and specific competenceskills in protecting inner-city adolescents from alcohol use. Journal of Studies on Alcohol, 61,379–386.
Erikson, E. H. (1968). Identity, youth, and crisis. New York: Norton.Erikson, E. H. (1993). The problem of ego identity. In G. H. Pollock (Ed.), Pivotal papers on
identification (pp. 265–303). Madison, CT: International Universities Press.Feldman, S. S., & G. R. Elliott (Eds.). (1990). At the threshold: The developing adolescent.
Cambridge, MA: Harvard University Press.Gambrill, E. D., & Richey, C. A. (1975). An assertion inventory for use in assessment and
research. Behavior Therapy, 6, 550–561.Gersick, K. E., Grady, K., & Snow, D. L. (1988). Social-cognitive skill development with
sixth graders and its initial impact on substance use. Journal of Drug Education, 18,55–70.
Gibbons, F. X., Gerrard, M., Ouellette, J. A., & Burzette, R. (1998). Cognitive antecedents toadolescent health risk: Discriminating between behavioral intention and behavioralwillingness. Psychology and Health, 13, 319–339.
Grant, B. F., &Dawson, D. A. (1997). Age at onset of alcohol use and its associationwithDSM–IV alcohol abuse and dependence: Results from the National Longitudinal AlcoholEpidemiologic Survey. Journal of Substance Abuse, 9, 103–110.
Greenbaum, P. E., Brown, E. C., & Friedman, R. M. (1995). Alcohol expectancies amongadolescents with conduct disorder: prediction and mediation of drinking. AddictiveBehaviors, 20, 321–333.
Han, C.,McGue,M., & Iacono,W. G. (1999). Lifetime tobacco, alcohol and other substance usein adolescent Minnesota twins: Univariate and multivariate behavioral genetic analyses.Addiction, 94, 981–993.
Harter, S. (1990). Self and identity development. In S. S. Feldman, & G. R. Elliott (Eds.), At thethreshold: The developing adolescent (pp. 171–196). Cambridge, MA: Harvard UniversityPress.
Hawkins, J. D., Catalano, R. F., &Miller, J. Y. (1992). Risk and protective factors for alcohol andother drug problems in adolescence and early adulthood: Implications for substanceabuse prevention. Psychological Bulletin, 112, 64–115.
Institute of Medicine. (1994). Reducing risks for mental disorders: Frontiers for preventiveintervention research. Washington, DC: National Academy Press.
EARLYADOLESCENT SUBSTANCE INITIATION 325

Jaccard, J., & Wan, C. K. (1996). LISREL approaches to interaction effects in multipleregression. in M. S. Lewis-Beck (Series Ed.), Series: Quantitative applications in the socialsciences (No. 07-114). Thousand Oaks, CA: Sage.
Jessor, R., & Jessor, S. L. (1977). Problem behavior and psychosocial development: A longitudinalstudy of youth. New York: Academic Press.
Johnston, L. D., O’Malley, P. M., & Bachman, J. G., (1996). National survey results on drug usefrom the Monitoring the Future study, 1975–1994. Volume I: Secondary school students (NIHPub. No. 95-4026).
Johnston, L. D., O’Malley, P. M., & Bachman, J. G. (2002). The Monitoring the Future nationalsurvey results on drug use: Overview of key findings, 2001. (NIH Publication No. 02-5105).Rockville, MD: National Institute on Drug Abuse.
Jones, E. E., & Sigall, H. (1971). The bogus pipeline: A new paradigm formeasuring affect andattitude. Psychological Bulletin, 76, 349–364.
Joreskog, K. G., & Sorbom, D. (1996). LISREL 8: User’s reference guide. Mooresville, IN:Scientific Software.
Kandel, D. B., Yamaguchi, K., & Chen, K. (1992). Stages of progression in drug involvementfrom adolescence to adulthood: Further evidence for the gateway theory. Journal of Studieson Alcohol, 53, 447–457.
Keating, D. P. (1990). Adolescent thinking. In S. S. Feldman, & G. R. Elliott (Eds.), At thethreshold: The developing adolescent (pp. 54–89). Cambridge, MA: Harvard University Press.
Kline, R. B. (1998). Principles and practice of structural equation modeling. New York: Guilford.Kumpfer, K. L., & Turner, C. W. (1990). The social ecology model of adolescent substance
abuse: Implications for prevention. International Journal of the Addictions, 25, 435–463.Langer, L. M. (1996). Modeling adolescent health behavior: The preadult health decision-
makingmodel. In C. B.McCoy, L. R.Metschd, & J. A. Inciardi (Eds.), Intervening with drug-involved youth (pp. 45–78). Thousand Oaks, CA: Sage.
Lazarus, A. A. (1973). On assertive behavior: A brief note. Behavior Therapy, 4, 697–699.Lillehoj, C. J., Spoth, R., & Trudeau, L., (2002). Assertiveness among young rural adolescents:
Relationship to alcohol use. Manuscript submitted for publication.MacKinnon, D. P., Anderson Johnson, C., Pentz, M. A., Dwyer, J. H., Hansen,W. B., & Flay, B.
R., et al. (1991). Mediatingmechanisms in a school-based drug prevention program: First-
year effects of the Midwestern Prevention Project. Health Psychology, 10, 164–172.Marsh, W., & Hau, K. T. (1999). Confirmatory factor analysis: Strategies for small sample
sizes. In R. H. Hoyle (Ed.), Statistical strategies for small sample research (pp. 252–282).Thousand Oaks, CA: Sage.
Molgaard, V., Kumpfer, K., & Fleming, B. (1997). The Strengthening Families Program: ForParents and Youth 10–14. Ames: Iowa State University Extension.
Mrazek, P., & Haggerty, R. (Eds.). (1994). Reducing risks for mental disorders: Frontiers forpreventive intervention research. Washington, DC: National Academy Press.
Murray, D., O’Connell, C., Schmid, L., & Perry, C. (1987). The validity of smoking self-reportsby adolescents: A re-examination of the bogus pipeline procedures.Addictive Behaviors, 12,7–15.
Muthen, B., & Satorra, A. (1995). Complex sample data in structural equation modeling. In P.V. Marsden (Ed.), Sociological methodology (pp. 267–316). Washington, DC: AmericanSociological Association.
National Institute on Drug Abuse. (1997). Preventing drug use among children and adolescents: Aresearched-based guide (NIH Publication No. 97-4212). Rockville, MD: Author.
Oetting, E., & Beauvais, F. (1990). Adolescent drug use: Findings of national and localsurveys. Journal of Consulting and Clinical Psychology, 58, 385–394.
326 TRUDEAU, LILLEHOJ, SPOTH, REDMOND

Paglia, A., & Room, R. (1999). Preventing substance use problems among youth: A literaturereview and recommendations. Journal of Primary Prevention, 20, 3–50.
Pechacek, T., Murray, D., Luepker, R., Mittlemark, M., Johnson, C., & Shutz, J. (1984).Measurement of adolescent smoking behavior: Rationale and methods. Journal ofBehavioral Medicine, 7, 123–140.
Pedersen, W., Mastekaasa, A., &Wichstrom, L. (2001). Conduct problems and early cannabisinitiation: A longitudinal study of gender differences. Addiction, 93, 415–443.
Pentz, M. (1985). Social competence and self-efficacy as determinants of substance use inadolescence. In S. Shiffman, & T. A. Wills (Eds.), Coping and substance use (pp. 117–142).Orlando, FL: Academic Press.
Peters, R. D., &R. J.McMahon (Vol. Eds.). (1996).Preventing childhood disorders, substance abuse,and delinquency. K. D. Craig, K. S. Dobson, R. J.McMahon, &R. D. Peters (Series Eds.),Banffinternational behavioral science series, Vol. 3. Thousand Oaks, CA: Sage.
Petraitis, J., Flay, B., & Miller, T. (1995). Reviewing theories of adolescent substance use:Organizing pieces in the puzzle. Psychological Bulletin, 117, 67–88.
Petraitis, J., Flay, B., Miller, T., Torpy, E., & Greiner, B. (1998). Illicit substance use amongadolescents: A matrix of prospective predictors. Substance Use & Misuse, 33, 2561–2604.
Radecki, C. M., & Jaccard, J. (1996). Gender-role differences in decision-making orientationsand decision-making skills. Journal of Applied Social Psychology, 26, 76–94.
Riggs, P., & Whitmore, E. (1999). Substance use disorders and disruptive behavior disorders.In R. L. Hendren (Ed.), Review of psychiatry. Disruptive behavior disorders in children andadolescents (Vol. 18, pp. 133–164). Washington, DC: American Psychiatric Press.
Rogosa, D. (1995).Myths andmethods:Myths about longitudinal research plus supplementalquestions. In J. Gottman (Ed.), The analysis of change (pp. 3–66). Mahwah, NJ: Erlbaum.
Rosenberg, M. (1989). Self-esteem and adolescent problems. American Sociological Review, 54,1004–1018.
Russell, D. (2002). In search of underlying dimensions: The use (and abuse) of factor analysis.Personality and Social Psychology Bulletin, 28, 1629–1646.
Satorra, A., & Bentler, P. M. (1994). Corrections to test statistics and standard errors oncovariance structure analysis. In A.von Eye, & C. C. Clogg (Eds.), Latent variables analysis(pp. 399–419). Thousand Oaks, CA: Sage.
Scheier, L. M., & Botvin, G. J. (1997). Expectancies as mediators of the effects of socialinfluences and alcohol knowledge on adolescent alcohol use: A prospective analysis.Psychology of Addictive Behaviors, 11, 48–64.
Scheier, L. M., & Botvin, G. J. (1998). Relations of social skills, personal competence, andadolescent alcohol use: A developmental exploratory study. Journal of Early Adolescence,18, 77–114.
Scheier, L. M., Botvin, G. J., & Baker, E. (1997). Risk and protective factors as predictors ofadolescent alcohol involvement and transitions in alcohol use: A prospective analysis.Journal of Studies on Alcohol, 58, 652–667.
Scheier, L. M., Botvin, G. J., Diaz, T., & Griffin, K. W. (1999). Social skills, competence, anddrug refusal efficacy as predictors of adolescent alcohol use. Journal of Drug Education, 29,251–278.
Sheppard, B. H., Hartwick, J., &Warshaw, P. R. (1988). The theory of reasoned action: Ameta-analysis of past research with recommendations for modifications for future research.Journal of Consumer Research, 15, 325–343.
Silberman, M. A., & Snarey, J. (1993). Gender differences in moral development during earlyadolescence: The contribution of sex-related variations in maturation. Current Psychology:Developmental, Learning, Personality, Social, 12, 163–171.
EARLYADOLESCENT SUBSTANCE INITIATION 327

Singer, J. D. (1998). Using SAS PROC MIXED to fit multilevel models, hierarchical models,and individual growth models. Journal of Educational and Behavioral Statistics, 24, 323–355.
Snijders, T., & Bosker, R. (1999). Multilevel analysis: An introduction to basic and advancedmultilevel modeling. London: Sage.
Spoth, R. L., Kavanagh, K., & Dishion, T. (2002). Family-centered preventive interventionscience: Toward benefits to larger populations of children, youth, and families. PreventionScience, 3, 145–152.
Spoth, R., & Redmond, C. (2002). Project Family prevention trials based in community-university partnerships: Toward scaled–up preventive interventions. Prevention Science, 3,203–221.
Spoth, R., Redmond, C., & Shin, C. (1998). Direct and indirect latent-variable parentingoutcomes of two universal family-focused preventive interventions: Extending a publichealth-oriented research base. Journal of Consulting and Clinical Psychology, 66(2), 385–399.
Spoth, R., Redmond, C., & Shin, C. (2001). Randomized trial of brief family interventions forgeneral populations: Adolescent substance use outcomes four years following baseline.Journal of Consulting and Clinical Psychology, 69, 627–642.
Spoth, R., Redmond, C., Trudeau, L., & Shin, C. (2002). Longitudinal substance initiationoutcomes for a universal preventive intervention combining family and school programs.Psychology of Addictive Behaviors, 16, 129–134.
SPSS Incorporated. (1988). SPSS-X User’s Guide (3rd ed.). Chicago: Author.Tobler, N. S., Roona, M. R., Ochshorn, P., Marshall, D. G., Streke, A. V., & Stackpole, K. M.
(2000). School-based adolescent drug prevention programs: 1998 meta-analysis. Journal ofPrimary Prevention, 20, 275–336.
U.S. PublicHealth Service (1974).Teenager’s self-test: Cigarette smoking (DHEWPublicationNo.CDC 74-8723) Washington, DC: Centers for Disease Control, U.S. Public Health Service.
Webb, J. A., Baer, P. E., Francis, D. J., & Caid, C. D. (1993). Relationship among social andintrapersonal risk, alcohol expectancies, and alcohol usage among early adolescents.Addictive Behaviors, 18, 127–134.
Webb, J. A., Getz, J. G., Baer, P. E., & McKelvey, R. S. (1999). Intentions to use alcohol amongfifth and sixth graders: The roles of social and stress/coping motives. American Journal ofOrthopsychiatry, 69, 541–547.
West, S. G., Finch, J. F., & Curran, P. J. (1995). Structural equation models with nonnormalvariables. In R. H. Hoyle, (Ed.), Structural equation modeling: Concepts, issues, andapplications. Thousand Oaks, CA: Sage.
Wills, T. A. (1986). Stress and coping in early adolescence: Relationships to substance use inurban school samples. Health Psychology, 5, 503–529.
Wills, T. A., Baker, E., & Botvin, G. J. (1989). Dimensions of assertiveness: Differentialrelationships to substance use in early adolescence. Journal of Consulting and ClinicalPsychology, 57, 473–478.
Wills, T. A., & Shiffman, S. (1985). Coping and substance use: A conceptual framework. In S.Shiffman, & T. A. Wills (Eds.), Coping and substance use (pp. 1–24). Orlando, FL: AcademicPress.
Wolpe, J. (1973). Supervision transcripts: Mainly about assertive training. Journal of BehaviorTherapy and Experimental Psychiatry, 4, 141–148.
328 TRUDEAU, LILLEHOJ, SPOTH, REDMOND