Embed Size (px)
Citation preview
The renaissance of immunotherapy is a revolution for cancer patients
Ira Mellman, Ph.D. Vice President, Cancer Immunology, Genentech
1

2
This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as ‘believes’, ‘expects’, ‘anticipates’, ‘projects’, ‘intends’, ‘should’, ‘seeks’, ‘estimates’, ‘future’ or similar expressions or by discussion of, among other things, strategy, goals, plans or intentions. Various factors may cause actual results to differ materially in the future from those reflected in forward-looking statements contained in this presentation, among others: 1 pricing and product initiatives of competitors; 2 legislative and regulatory developments and economic conditions; 3 delay or inability in obtaining regulatory approvals or bringing products to market; 4 fluctuations in currency exchange rates and general financial market conditions; 5 uncertainties in the discovery, development or marketing of new products or new uses of existing
products, including without limitation negative results of clinical trials or research projects, unexpected side-effects of pipeline or marketed products;
6 increased government pricing pressures; 7 interruptions in production; 8 loss of or inability to obtain adequate protection for intellectual property rights; 9 litigation; 10 loss of key executives or other employees; and 11 adverse publicity and news coverage. Any statements regarding earnings per share growth is not a profit forecast and should not be interpreted to mean that Roche’s earnings or earnings per share for this year or any subsequent period will necessarily match or exceed the historical published earnings or earnings per share of Roche.
For marketed products discussed in this presentation, please see full prescribing information on our website www.roche.com
All mentioned trademarks are legally protected.

The renaissance of immunotherapy is a revolution for cancer patients

Early data suggests that anti-PD-L1/PD-1 is active across a wide range of tumor types
• Melanoma: FDA approval • NSCLC (squamous): FDA approval, 2nd line • Renal cell carcinoma • Breast cancer (e.g. TNBC) • Metastatic bladder cancer • Head & neck cancer • Hodgkin's lymphoma
Response rates are modest, at ~10-30%
Broad activity but most patients do not benefit from single agent therapy
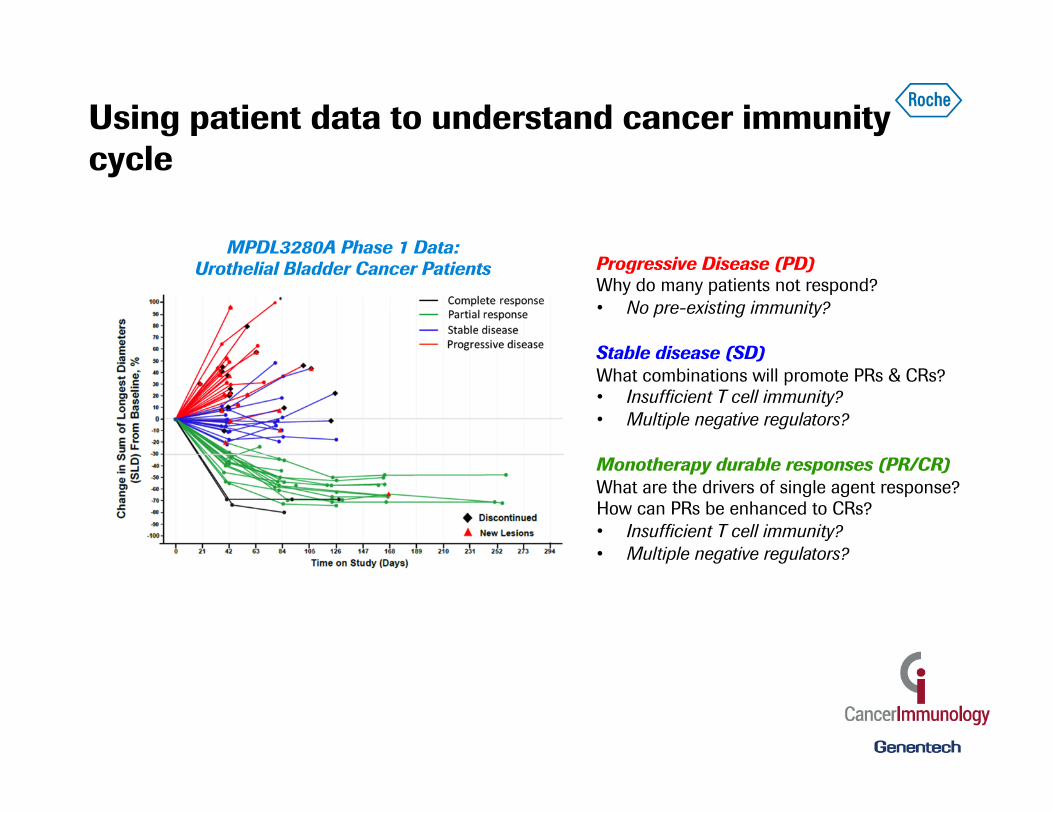
Using patient data to understand cancer immunity cycle
MPDL3280A Phase 1 Data: Urothelial Bladder Cancer Patients Progressive Disease (PD)
Why do many patients not respond? • No pre-existing immunity?
Stable disease (SD) What combinations will promote PRs & CRs? • Insufficient T cell immunity? • Multiple negative regulators?
Monotherapy durable responses (PR/CR) What are the drivers of single agent response? How can PRs be enhanced to CRs? • Insufficient T cell immunity? • Multiple negative regulators?

Chen & Mellman (2013) Immunity
The cancer immunity cycle Immunosuppression as the rate limiting step to effective anti-tumor immunity
α-CTLA4 (ipilumumab)
Immuno- suppression
α-PD-L1/PD-1 (multiple)
Chen & Mellman (2013) Immunity
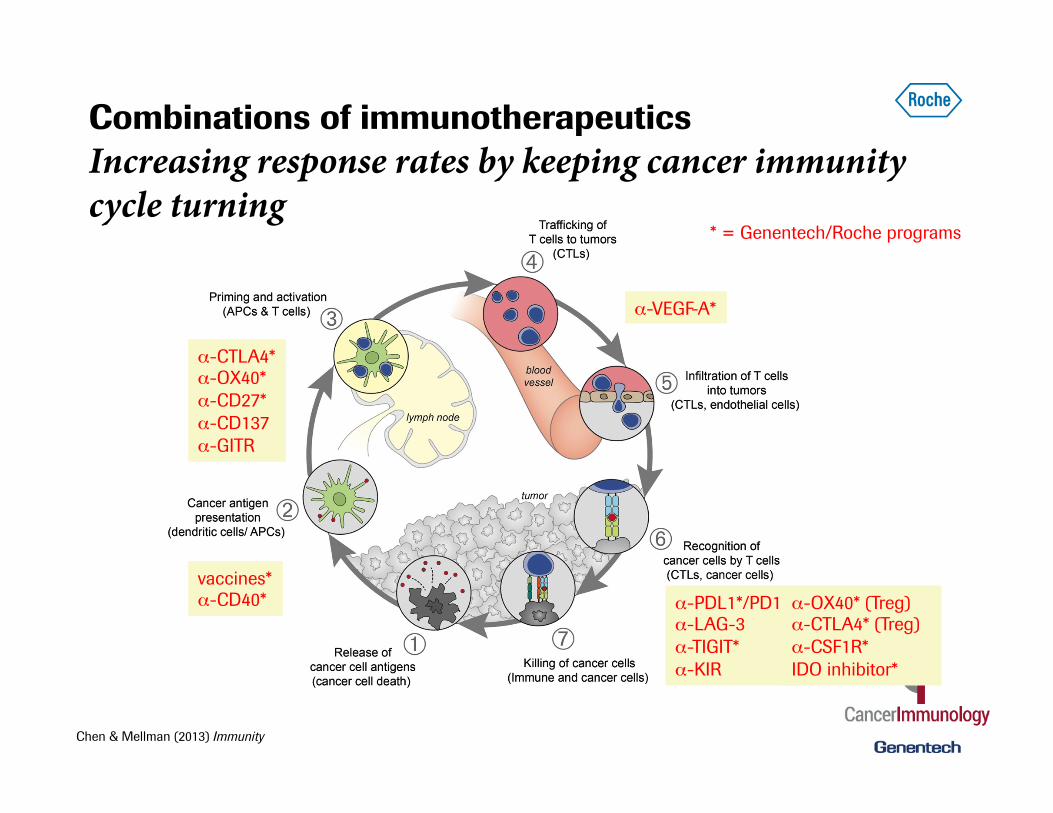
Combinations of immunotherapeutics Increasing response rates by keeping cancer immunity cycle turning
α-PDL1*/PD1 α-LAG-3 α-TIGIT* α-KIR
α-CTLA4* α-OX40* α-CD27* α-CD137 α-GITR
vaccines* α-CD40*
α-VEGF-A*
* = Genentech/Roche programs
α-OX40* (Treg) α-CTLA4* (Treg) α-CSF1R* IDO inhibitor*
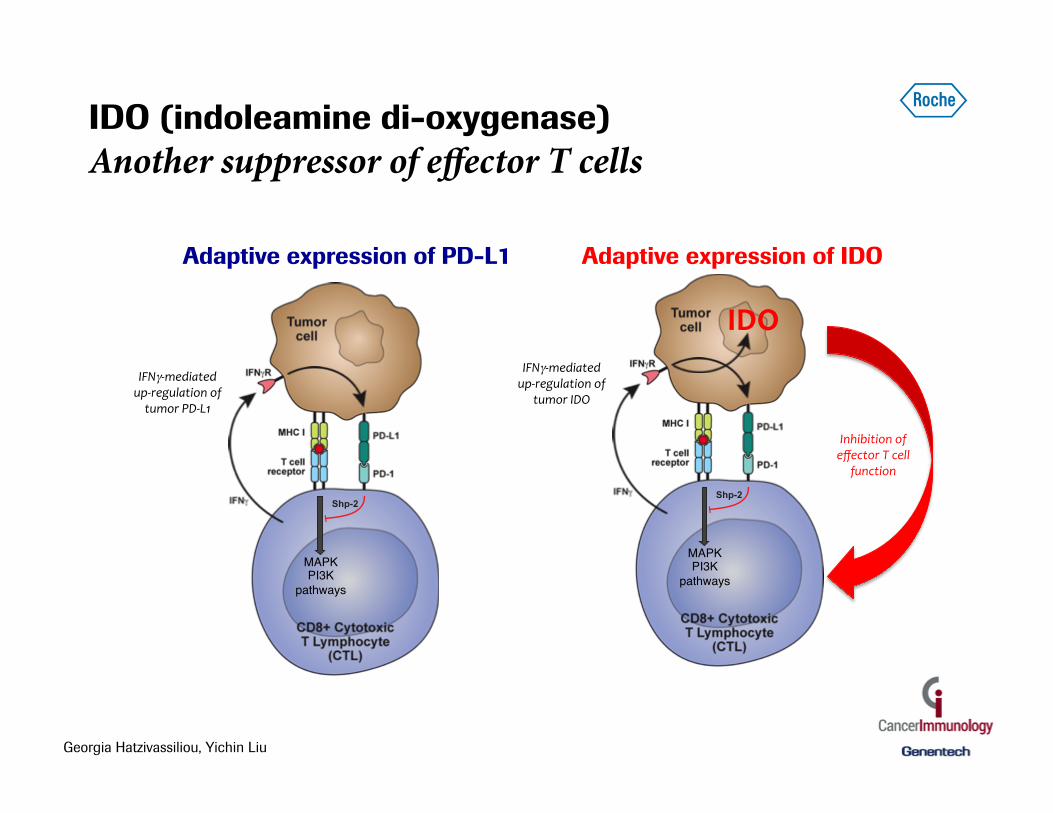
IFNγ-‐mediated up-‐regulation of tumor PD-‐L1
Shp-2
Adaptive expression of PD-L1
MAPK"PI3K
pathways"
IFNγ-‐mediated up-‐regulation of
tumor IDO
Inhibition of effector T cell
function
Shp-2
MAPK"PI3K
pathways"
Adaptive expression of IDO
IDO
Georgia Hatzivassiliou, Yichin Liu
IDO (indoleamine di-oxygenase) Another suppressor of effector T cells

IDO mediates T cell suppression by reducing extracellular tryptophan and increasing kynurenine
mTOR
Promote translation
high
Enhance T reg
arylhydrocarbon receptor
FoxP3
Kynurenine
IDO*
Tumor cells
IFNg activates IDO expression
Suppress T effectors
ñ Uncharged Tryptophanol-tRNA
GCN2 kinase
Stress response
low
suppressive cytokines
Dendritic cells Macrophages
*TDO (tryptophan dioxygenase) is a second related target to IDO
Free tryptophan
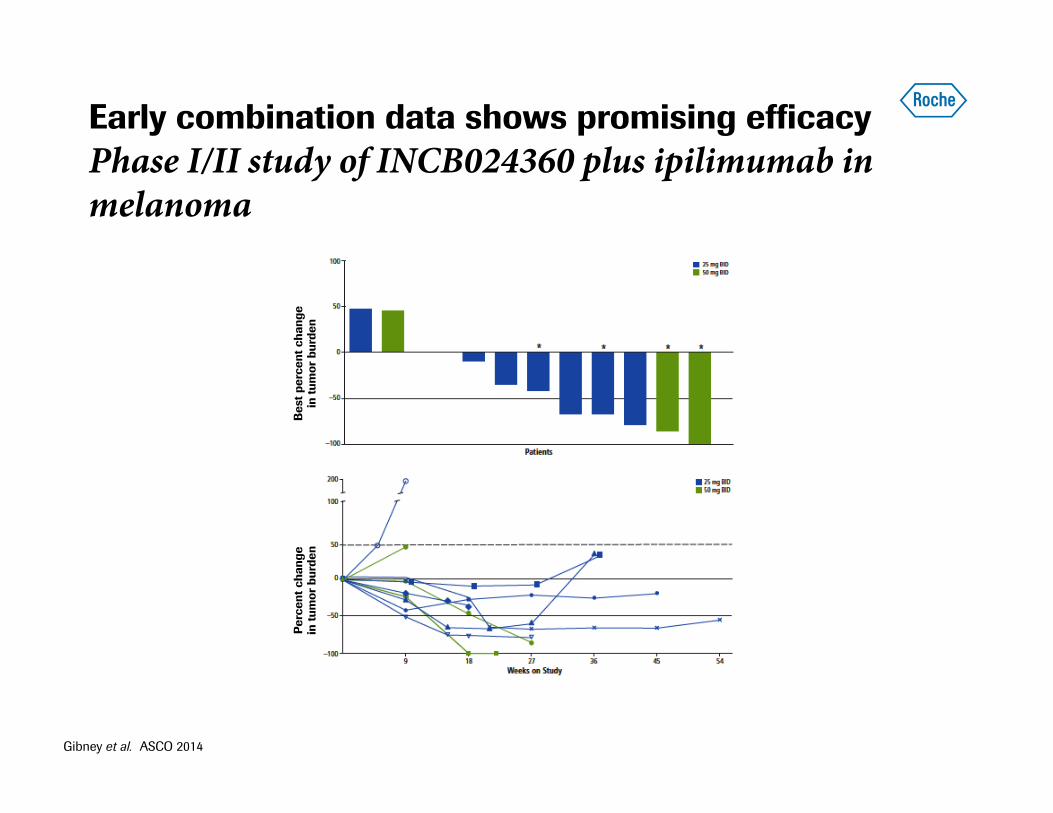
Early combination data shows promising efficacy Phase I/II study of INCB024360 plus ipilimumab in melanoma
Best
per
cent
cha
nge
in
tum
or b
urde
n Pe
rcen
t cha
nge
in
tum
or b
urde
n
Gibney et al. ASCO 2014

TIGIT Model of TIGIT regulation of T cell responses
• Human and murine tumor-infiltrating CD8+ T cells express high levels of TIGIT
• Antibody coblockade of TIGIT and PDL1 elicits tumor rejection in preclinical models
• TIGIT selectively limits the effector function of chronically stimulated CD8+ T cells
• TIGIT interacts with CD226 in cis and disrupts CD226 homodimerization
Tumor cell or DC
PVR
ITIM
Competes with CD226 for PVR
100nm 1nm
TIGIT CD226
ITIM ITAM
Disrupts CD226 ac7va7on Directly inhibits T cell in cis
1
2 3
T cell

TIGIT TIGIT and PD-L1 combination effective in PD-L1 non-responsive model
Tumor cell or DC
PVR
ITIM
Competes with CD226 for PVR
100nm 1nm
TIGIT CD226
ITIM ITAM
Disrupts CD226 ac7va7on Directly inhibits T cell in cis
1
2 3
T cell
0 10 20 30 40 6010
100
1000
10000
Day
Median Tumor Volume (mm3)�
Control �anti-PD-L1 �NME1 �
anti-PD-L1 �+ NME1�
Complete Remission (CR)�
010
2030
4060
10100
1000
10000
Day
Med
ian
Tum
or V
olum
e (m
m3 )�
Cont
rol�
anti-
PD-L
1�NM
E1�
anti-
PD-L
1 �
+ NM
E1�
Com
plet
e Re
miss
ion
(CR)�TIGIT
Anti-PD-L1 + TIGIT
Control Anti-PD-L1

OX40 function and potential in oncology Promote antigen dependent effector T cell activation and T regulatory cell inhibition
Adapted from Nature Rev Immunol. 4:420 (2004).
Effector T cell
TCR
Antigen Presenting Cell
OX40
OX40L
IFN-γ
OX40 engagement on Treg cells
Treg
OX40L
OX40L
OX40
0 10 20 30 40 500
1000
2000
3000
dayTu
mor
Vol
ume
(mm
3 ) ControlAnti-mouse OX40
Treatment
Primary Tumor Challenge (EMT6)
day
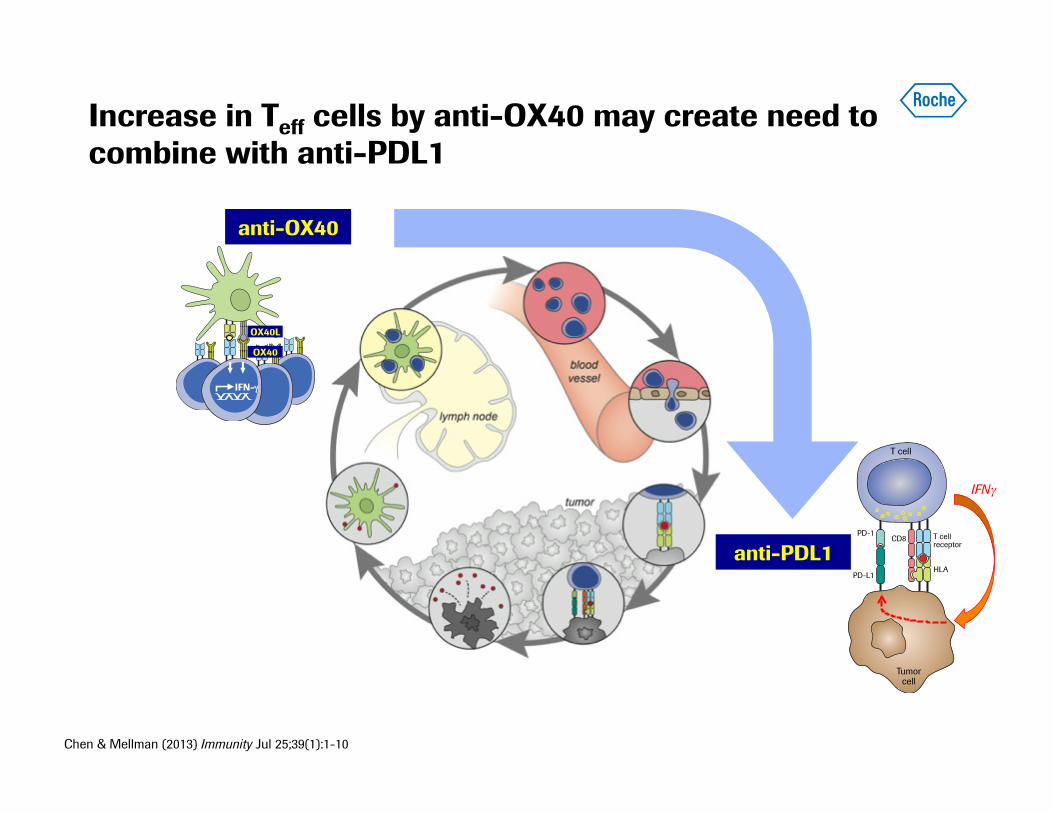
Chen & Mellman (2013) Immunity Jul 25;39(1):1-10
anti-OX40
anti-PDL1 CD8 T cell
receptor
HLA
PD-1
PD-L1
Tumor cell
T cell
IFNγ
PD-L1 increase
Increase in Teff cells by anti-OX40 may create need to combine with anti-PDL1
IFN-γ"
OX40L
OX40
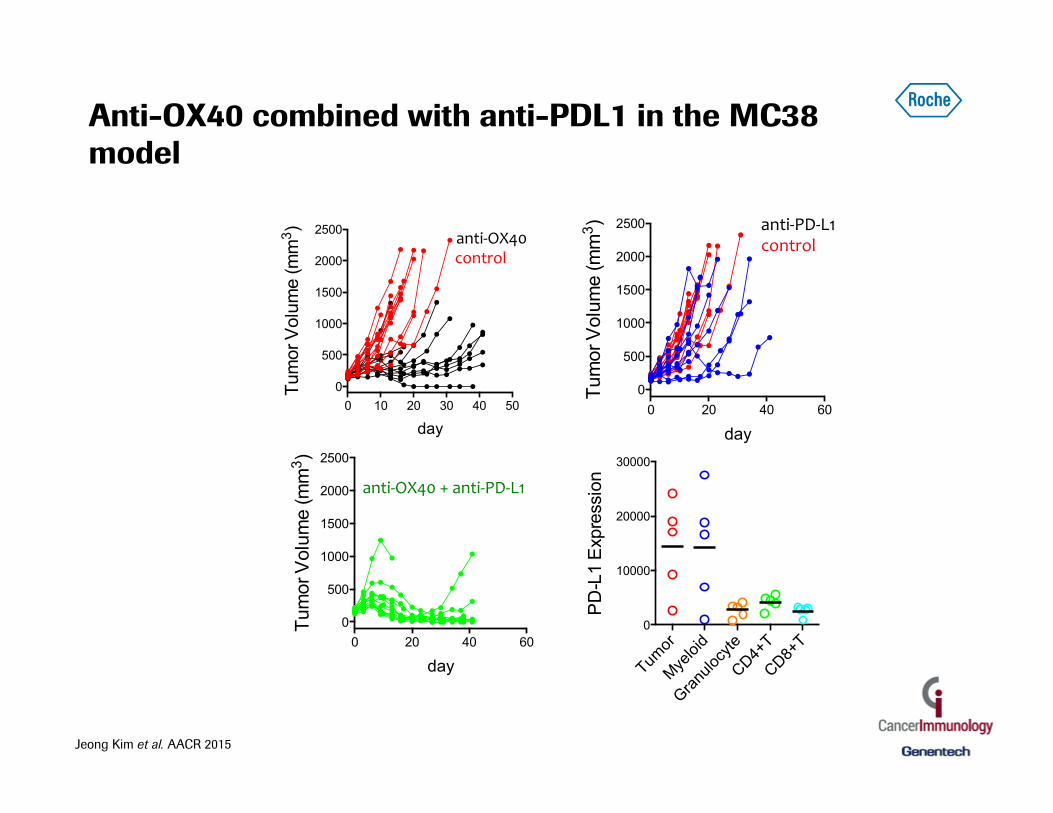
Anti-OX40 combined with anti-PDL1 in the MC38 model
Tumor
Myeloi
d
Granu
locyte
CD4+T
CD8+T
0
10000
20000
30000
PD
-L1
Exp
ress
ion
0 20 40 600
500
1000
1500
2000
2500
day
Tum
or V
olum
e (m
m3 ) anti%PD%L1*
control*
0 20 40 600
500
1000
1500
2000
2500
day
Tum
or V
olum
e (m
m3 )
anti%OX40*+*anti%PD%L1*
0 10 20 30 40 500
500
1000
1500
2000
2500
day
Tum
or V
olum
e (m
m3 ) !!!!!!!!!!!!!!!!!!!!!!!anti&OX40!
!!!!!!!!!!!!!!!!!control!
Jeong Kim et al. AACR 2015

Chen & Mellman (2013) Immunity
Combination with Avastin Increasing response rates by keeping cancer immunity cycle turning
α-VEGF-A
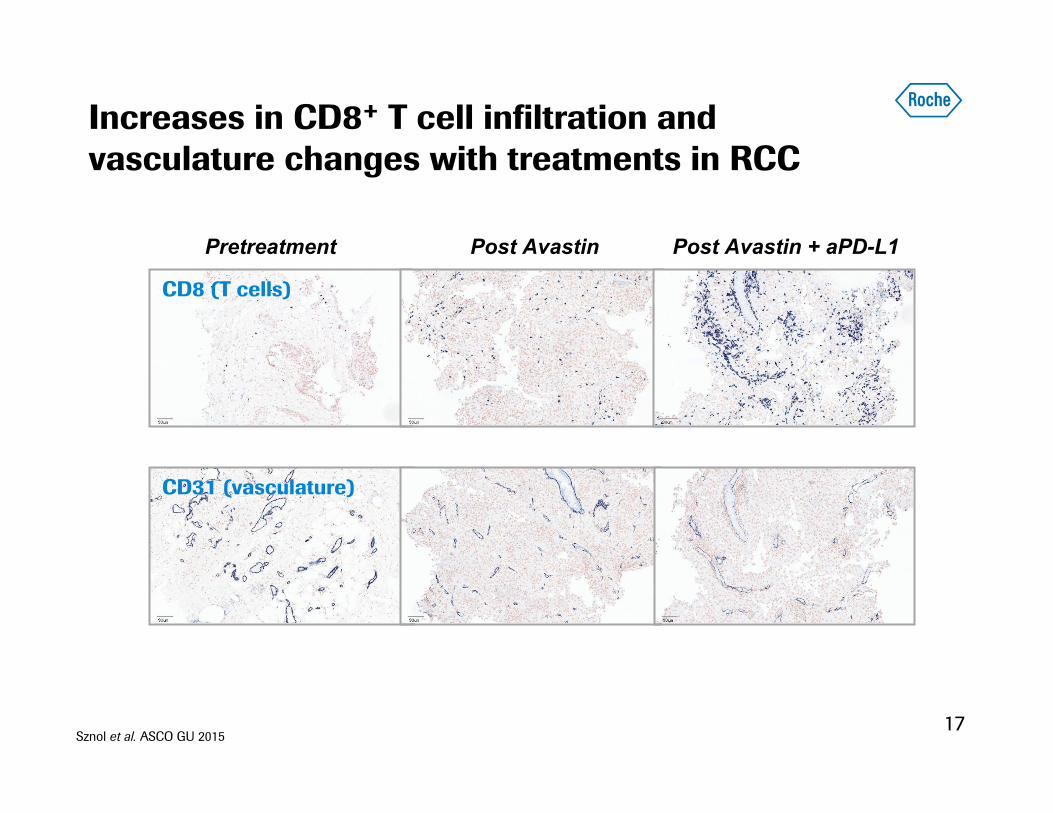
Increases in CD8+ T cell infiltration and vasculature changes with treatments in RCC
17
Pretreatment Post Avastin Post Avastin + aPD-L1
CD8 (T cells)
CD31 (vasculature)
Sznol et al. ASCO GU 2015

Anti-PDL1 in combination with Avastin
18
0
500
1000
1500
2000
0 10 20 30 40 50
Tu
mo
r V
olu
me
, m
m3
Day
Anti-VEGF combination: preclinical data
a-VEGF
a-PD-L1
a-PD-L1 + a-VEGF
Control
Cloudman melanoma
Combination of anti-PDL1 and Avastin (Ph1 data in renal cancer)
Sznol et al. ASCO GU 2015

Chen & Mellman (2013) Immunity
Combinations with chemotherapy Induced inflammation & antigen release may enhance anti-PDL1 efficacy
Chemotherapy

20-30% patients • T cells present in tumor • Chemokines present
(attract leukocytes)
70-80% patients • Lack lymphocytic infiltrates
Non-responsive to single agent immunotherapies
Tumor phenotype by T cell staining
Inflamed Non-inflamed
Responsive to single agent immunotherapies
Can we convert these to responsive?
Can responses be improved?
Inflammation is necessary for response
20
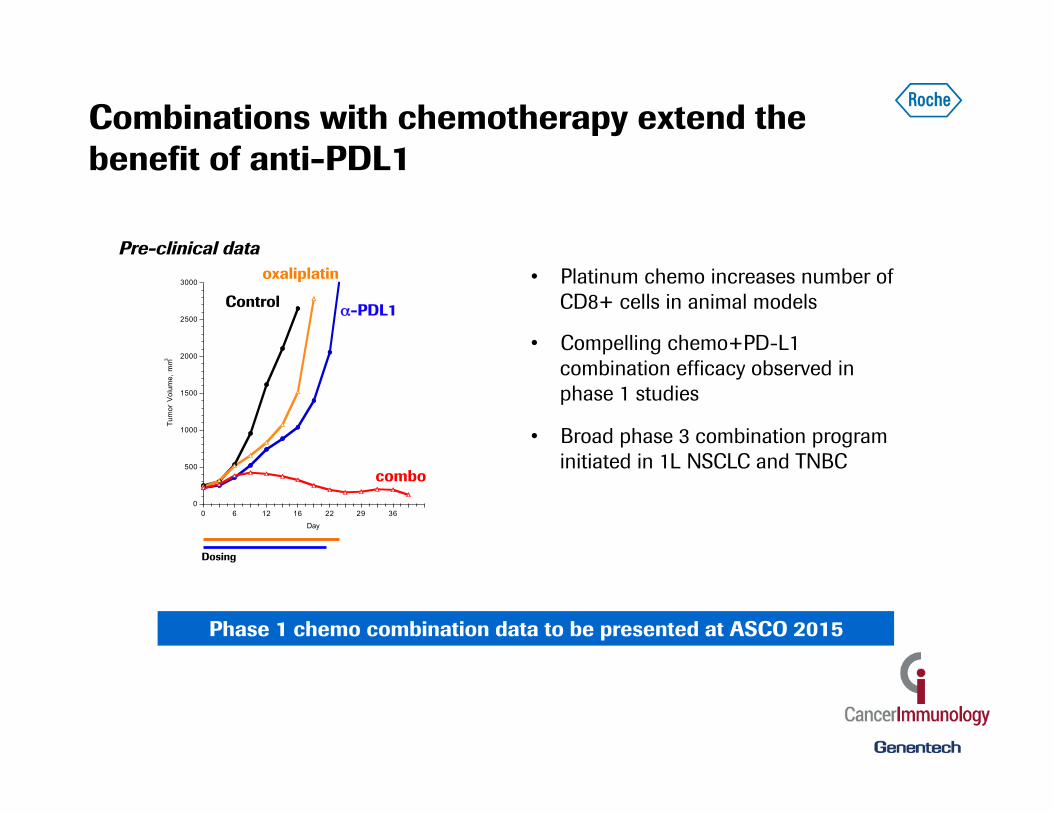
Combinations with chemotherapy extend the benefit of anti-PDL1
• Platinum chemo increases number of CD8+ cells in animal models
• Compelling chemo+PD-L1 combination efficacy observed in phase 1 studies
• Broad phase 3 combination program initiated in 1L NSCLC and TNBC
oxaliplatin
Dosing
0
500
1000
1500
2000
2500
3000
0 6 12 16 22 29 36
Tum
or V
olum
e, m
m3
Day
α-PDL1
combo
Control
Pre-clinical data
Phase 1 chemo combination data to be presented at ASCO 2015

1
2
3
4
5
6
7
Recognition of cancer cells by T cells (CTLs, cancer cells)
ImmTACs Bispecifics
Not all patients may have pre-existing immunity: monitoring & promoting T cell responses ImmTACs and bispecific antibodies

Immune-mobilizing mTCR Against Cancer*
*In colalboaration with Immunocore
T-cell Dependent Bispecific
TCR
Tumor antigen
Cancer cell
T cell Knob into holes full-length IgG
Targeting intracellular tumor markers Targeting extracellular tumor markers
Recruiting T cells to cancer cells ImmTACs and bispecific antibodies

Chen & Mellman (2013) Immunity
1
2
3
4
5
6
7
Cancer antigen presentation
(dendritic cells/APCs) Vaccines: • Endogenous • Exogenous
Not all patients may have pre-existing immunity: monitoring & promoting T cell responses Vaccines

Anti-PDL1 Phase Ia: indication response rates correlate with mutation frequency
Schumacher and Schreiber (2015) Science
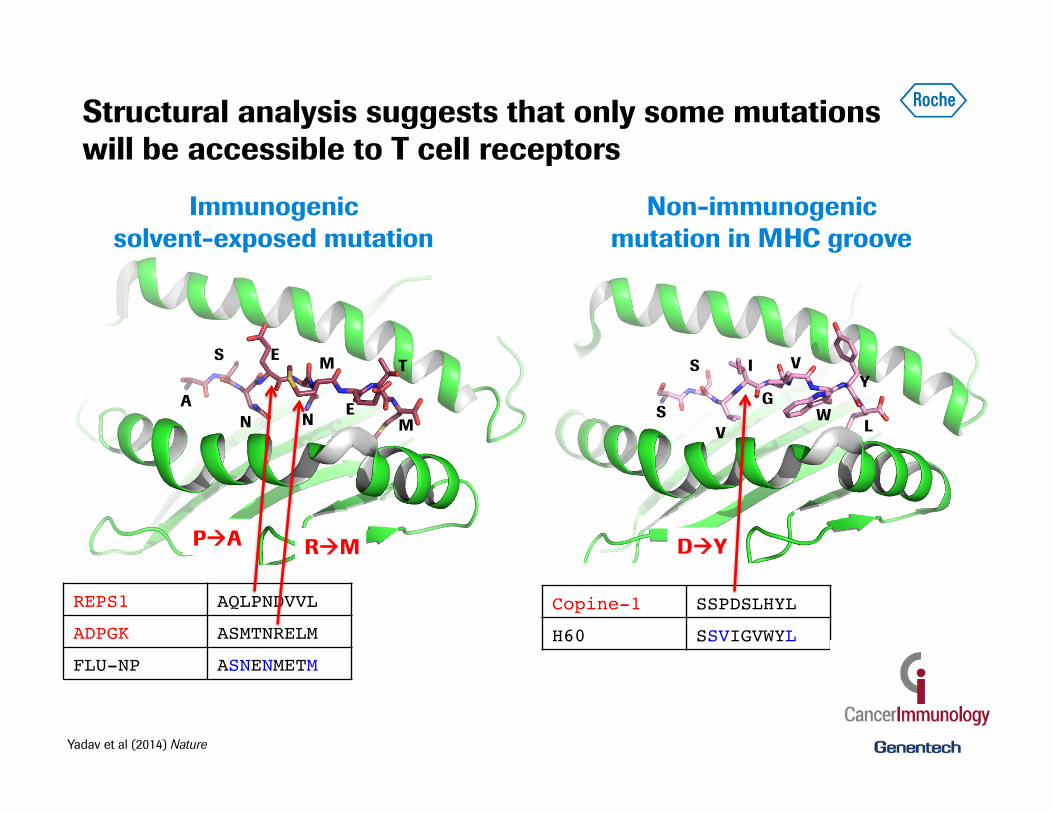
Structural analysis suggests that only some mutations will be accessible to T cell receptors
26
A
S
N
E
N
M
E
T
M S
S
V
I
G
V
W
Y
L
REPS1! AQLPNDVVL!
ADPGK! ASMTNRELM!
FLU-NP! ASNENMETM!
Copine-1! SSPDSLHYL!
H60! SSVIGVWYL!
PàA RàM DàY
Immunogenic solvent-exposed mutation
Non-immunogenic mutation in MHC groove
Yadav et al (2014) Nature

Promise for a PHC vaccine? Immunization with antigenic peptides regresses growth of established MC38 tumors
Dose Groups● 01 − untreated control
02 − d1: anti−CD40 50µg + pIC 100µg, IP injection. d10: anti−CD40 50µg + pIC 100µg, IP injection. (n=10)03 − d1: anti−CD40 50µg + pIC 100µg + 3Xpeptide mix 100µg, IP injection. d10: 3Xpeptide mix anti−CD40 50µg + pIC 100µg, IP injection. (n=10)
Control
Adj
Adj+ Peptides
Immunization
14−0584: mutated MHCI MC38 peptide vaccine; MC−38 Raw and LME Fit Tumor Volume
Day
Tum
or V
olum
e ( m
m3 )
0
100
200
300
400
500
600
700
● ●●●
●
●
●
●
●
●
●
●
●
● ●
●
●
●
●●
●
●
●
●
●
●
●
●
●
●
1
0 2 4 6
●
● ●
●
●●
●●
●
●
●
●
●
●●
●●
●
●
●
●
●
●
●
● ●
●
●
●●
2
0 2 4 60
100
200
300
400
500
600
700
●
●●
● ●●
●
●
●
●
●●
●
● ●
●
●
●
●●
●
● ● ●● ●
●
●
●
●
3
Control Adj
Adj+peptides
14-0584: mutated MHCI MC38 peptide vaccine; MC-38 Overlay Fits Tumor Volume
14-0584: mutated MHCI MC38 peptide vaccine; MC-38 Raw and LME Fit Tumor Volume
Yadav et al (2014) Nature

Strategic vision: lead by developing best in class combination therapies
Combinations with immunotherapies aCD40 ✔ Vaccines, Oncolytic Viruses ✔ ✔ aCTLA-4 ✔ aOX40 ✔ aCD27 ✔ aCEA-IL2v ✔ T Cell Bispecifics ✔ ImmTACs Planned IDOi ✔✔ aCSF1R ✔ aTIGIT Planned Cytokines, anti-cytokines ✔ Combinations with other agents aVEGF ✔ aCD38 ✔ FGFR1 ✔ EGFRi ✔ ✔ ALKi Planned BRAFi ✔ MEKi ✔ BTKi ✔ aCD20 ✔ aHER2 ✔ Chemo ✔ ✔ HDAC ✔ A2V ✔
Internal combo ✔ ✔
Partnered external combo
Chen & Mellman (2013) Immunity
1
2
3
4
5
6
7
Priming & activation anti-CEA-IL2v anti-OX40 anti-CTLA4 anti-CD27* anti cytokine CD38*
Antigen presentation anti-CD40 IMA942 vaccine* oncolytic viruses*
Antigen release EGFRi ALKi BRAFi MEKi Chemo FGFR1* BTKi HDAC
T cell infiltration aVEGF
Cancer T cell recognition anti-HER2-CD3 anti-CD20-CD3 ImmTAC*
T cell killing anti-OX40 anti-CSF-1R anti-CEA-IL2v IDO inhibitor* TIGIT IDO1/TDO inhibitor*
T cell trafficking
Clinical development Preclinical development
* Partnered projects
Immuno- suppression
Doing now what patients need next





























