Embed Size (px)
Citation preview

Clin Exp Immunol 2003;
132
:443–449
© 2003 Blackwell Publishing Ltd
443
&Blackwell Science, Ltd
Oxford, UK
CEIClinical and Experimental Immunology
1365-2249Blackwell Publishing Ltd, 2003
132
3
443449Original Article
Depressed TNF-a in multidrug-resistant tuberculosis patientsJ.-S. Lee et al.
Correspondence: Dr Eun-Kyeong Jo, Department of Microbiology,College of Medicine, Chungnam National University, 6 Munhwa-dong,Jung-ku, Daejeon 301–747, Korea.
E-mail: [email protected]
The production of tumour necrosis factor-alpha is decreased in peripheral blood mononuclear cells from multidrug-resistant tuberculosis patients following
stimulation with the 30-kDa antigen of
Mycobacterium tuberculosis
J.-S. LEE*, C.-H. SONG*, J.-H. LIM*, H.-J. KIM*, J.-K. PARK*, T.-H. PAIK†, C.-H. KIM‡, S.-J. KONG‡, M.-H. SHON‡, S.-S. JUNG§ & E.-K. JO* *
Department of Microbiology and
§
Internal Medicine, College of Medicine, Chungnam National University, Daejeon,
‡
National Mokpo Tuberculosis Hospital, Mokpo, Korea, and
†
Department of Microbiology, College of Medicine, Konyang University, Nonsan, Chungnam, Korea
(Accepted for publication 1 April 2003)
SUMMARY
The clearance of intracellular bacteria requires the appropriate induction of proinflammatory cytokinesand chemokines to recruit macrophages and T cells to the site of infection. In this study, we investigatedthe production of tumour necrosis factor (TNF)-
a
, interleukin (IL)-8 and interferon (IFN)-
g
by theperipheral blood mononuclear cells (PBMC) of patients with multidrug-resistant tuberculosis (MDR-TB) in response to
in vitro
stimulation with the 30-kDa antigen of
Mycobacterium tuberculosis
. Theresults were compared with those from cases of newly diagnosed TB (N-TB) and TB with treatment fail-ure (TF-TB), and healthy tuberculin reactors (HTR). The most significantly depressed TNF-
a
levelswere found in MDR-TB patients. IFN-
g
production was depressed significantly in all groups of TBpatients compared with the HTR group. TNF-
a
secretion in response to the 30-kDa antigen wasunchanged by coculturing with recombinant human interferon (rhIFN)-
g
, and was increased dramati-cally following IL-10 neutralization with an anti-human IL-10 antibody. The IL-8 levels were depressedsignificantly in MDR-TB patients compared with N-TB patients, but were similar to the IL-8 levels inTF-TB patients. Furthermore, rhTNF-
a
directly increased IL-8 secretion, and neutralizing antibody toTNF-
a
inhibited IL-8 production by the PBMC of MDR-TB patients that were stimulated with the 30-kDa antigen. Taken together, these data suggest that the PBMC of MDR-TB patients typically showTNF-
a
depression in response to the 30-kDa antigen, and this effect is modulated by IL-10. In addition,we highlight the role of TNF-
a
in IL-8 secretion in MDR-TB patients.
Keywords
interferon-gamma interleukin-8 multidrug-resistant tuberculosis tumour necosis factor-alpha 30-kDa antigen
INTRODUCTION
Tuberculosis (TB) worldwide has been accompanied by anincrease in the incidence of multidrug-resistant tuberculosis(MDR-TB), which is a significant public health and therapeuticproblem that may rapidly worsen as the human immunodeficiencyvirus epidemic spreads [1]. Research on host defence and theimmunopathogenesis of TB is necessary, because there is anurgent need for a new vaccine and adjunctive immunotherapy,particularly in patients with drug-resistant TB. The cytokine and
chemokine signals in mycobacterial infection play crucial roles inprotective immunity, because this is dependent on the precise co-ordination of T-lymphocyte sensitization and monocyte recruit-ment. Previous studies [2] showed that MDR-TB patients with lowCD4 T cell counts had impaired interferon (IFN)-
g
and interleu-kin (IL)-2 responses. In addition, our previous study [3] showedthat MDR-TB patients had significantly elevated IL-10 and IL-18production, when compared with healthy tuberculin reactors(HTR). However, little is known about tumour necrosis factor(TNF)-
a
or chemokine expression in patients with MDR-TB.The important proinflammatory cytokine TNF-
a
plays a keyrole in the defence against TB [4,5]. Detailed studies of murinemodels have indicated that TNF plays an essential role in protec-tive immunity against TB [6,7]. TNF-
a
contributes to the preven-tion of reactivation of persistent TB, and limits the pathologicalresponse of the host [8]. In humans, the critical role of TNF-
a
was

444
J.-S. Lee
et al.
© 2003 Blackwell Publishing Ltd,
Clinical and Experimental Immunology
,
132
:443–449
emphasized by the reactivation of TB in rheumatoid arthritispatients who were treated with anti-TNF antibodies [4,9,10].However, TNF-
a
may also be responsible for the toxic syndromeand tissue necrosis that accompany TB, since it has importantproinflammatory activities [11]. Thus, successful protective immu-nity to TB may require a balance between antimycobacterialcytokine responses and proinflammatory cytokine responses thatmay result in unwanted tissue damage.
Chemokines belong to a large family of structurally relatedsecreted proteins that are important for leucocyte trafficking dur-ing host defence and inflammation [12,13]. IL-8, which is the bestcharacterized of the CXC subfamily of chemokines, appears to bean important chemokine in the mycobacterial host–pathogeninteraction, and is involved in cellular recruitment to the granu-loma [14]. IL-8 attracts neutrophils and T cells, both directly andindirectly, to sites of infection, and has recently been implicated inmonocyte recruitment [15]. Bronchoalveolar lavage fluid frompatients with active pulmonary TB contains elevated levels of IL-8, compared with healthy controls [16,17], which suggests that IL-8 is involved in protective immune responses to TB through therecruitment of cells for granuloma formation.
Currently, there is great interest in the secreted protein anti-gen (Ag) of
M
.
tuberculosis
in relation to immune responses toinfection. The 30-kDa Ag is a very effective cytokine inducer andhas been reported to strongly induce IFN-
g
[18–20], IL-12, IL-10[20] and TNF-
a
[21] in human monocytes or peripheral bloodmononuclear cells (PBMCs). In addition, the 30-kDa Ag is rec-ognized differently by the immune systems of infected healthyand diseased subjects, and may constitute a potential marker forprotection against TB. Ours [20,22] and other [18] previous stud-ies emphasized the role of the 30-kDa Ag, a major secretory anti-gen from
M
.
tuberculosis
, in eliciting differential IFN-
g
inductionin HTR and active pulmonary TB patients. However, little isknown about the 30-kDa-induced cytokine or chemokineresponses in patients with MDR-TB.
Given this background, this study analysed the TNF-
a
, IFN-
g
and IL-8 secretion profiles of PBMCs from MDR-TB patientsafter
in vitro
stimulation with the 30-kDa Ag. The data were com-pared with those from conventional TB [newly diagnosed TB (N-TB), treatment failure TB (TF-TB)] and HTR. This study showedthat MDR-TB patients produce less TNF-
a
and IFN-
g
in responseto the 30-kDa Ag. However, both the TNF-
a
and IL-8 levels wereelevated significantly in PBMCs from newly diagnosed drug-sensitive TB patients compared with those from MDR-TBpatients. In addition, IL-10 neutralization significantly increasedthe 30-kDa Ag-induced TNF-
a
levels in PBMCs from HTR andMDR-TB patients. Furthermore, TNF-
a
may play a major role inIL-8 expression by the PBMCs of MDR-TB patients following
invitro
stimulation with the 30-kDa Ag of
M
.
tuberculosis
.
MATERIALS AND METHODS
Subjects
Whole blood was obtained by venipuncture from ‘MDR-TB(
n
=
17)’ patients and ‘not MDR-TB (
n
=
40)’ patients at theNational Mokpo Tuberculosis Hospital (Mokpo, Chonnam,Korea), the Catholic University Hospital (Daejeon, Korea) andChungnam National University Hospital (Daejeon, Korea). Thisstudy was approved by the bioethics committee of ChungnamNational University Hospital, and all 1the participants gave theirwritten consent.
The ‘not MDR-TB’ patients were divided into patientswith N-TB (
n
=
19) and TF-TB (
n
=
21). The N-TB patientsparticipated in this study within 1 month of beginning first-lineantituberculosis drug medication. Their diagnoses were bacterio-logically confirmed active TB. The N-TB patients had minimal tomoderate TB, except for two patients who exhibited advanced TBin chest X-rays.
The TF-TB patients were undergoing a second round of treat-ment for TB, because the primary treatment had failed. Thesepatients had histories of incomplete or irregular prior treatmentsand/or inappropriate treatments with the available chemothera-peutic agents. The 17 patients had culture-proven MDR-TB, andall of them had bacteria that were resistant to rifampicin and iso-niazid. All of the patients had parenchymal TB, but none had mil-iary or pleural TB. None of the patients had a previous history ofdiabetes mellitus or steroid therapy, and all were HIV negative.Both the TF-TB and MDR-TB patients had moderate toadvanced radiographic abnormalities upon chest X-ray examina-tion. The mean durations of anti-TB treatment between the TF-TB and MDR-TB groups were 18·0
±
15·2 and 31·8
±
13·3 months,respectively, and the difference between these two groups was sta-tistically significant (
P
<
0·05). A complete history was taken anda physical examination was performed on each patient by one ofthe investigators.
The 20 HTR control subjects exhibited skin reactions of morethan 15 mm after intradermal inoculation of 5 units of PPD-RT23(Statens Seruminstitut, Copenhagen, Denmark) within 1–3 yearsbefore this study. The HTR individuals had no previous history ofclinical TB. All the healthy controls had received
Mycobacteriumbovis
Bacille Calmette–Guérin (BCG) vaccination as children.
Antigen and antibodies
The 30-kDa Ag was purified from
M
.
tuberculosis
strain H37Rvculture filtrate, as described previously [23]. The endotoxin con-tent in the 30-kDa Ag preparations was
<
0·02 ng/mg protein for30-kDa Ag, determined by the
Limulus
amoebocyte assay. Neu-tralizing rat antihuman IL-10 antibodies and the appropriate IgGisotype control antibodies were purchased from Endogen (Bos-ton, MA, USA). The recombinant human IFN-
g
(rhIFN-
g
) andrhTNF-
a
were purchased from R&D Systems (Minneapolis, MN,USA). Phytohaemagglutinin (PHA; Sigma) and lipopolysaccha-ride (LPS; Sigma) were used as positive controls for Ag stimula-tion in this study.
Preparation of PBMC
Whole heparinized venous blood was obtained from each subject.PBMCs were prepared by centrifugation of the blood over Ficoll-Paque gradients, as described previously [20], and were countedand resuspended in complete medium.
Enzyme-linked immunosorbent assays (ELISA)
The TNF-
a
, IFN-
g
, IL-10 and IL-8 content of the supernatantfrom PBMCs stimulated with the 30-kDa Ag was assessed usingcommercially available ELISA kits (PharMingen, San Diego, CA,USA), according to the manufacturer’s instructions. The lowerlimit of detection for all the cytokines is less than 4 pg/ml, exceptfor IL-8, for which it is less than 3 pg/ml.
Statistical methods
The results are presented as the mean
±
s.d. Statistical significancewas calculated using
ANOVA
, Student’s
t
-test or linear regressionanalysis.

Depressed TNF-
a
in multidrug-resistant tuberculosis patients
445
© 2003 Blackwell Publishing Ltd,
Clinical and Experimental Immunology
,
132
:443–449
RESULTS
TNF-
a
and IFN-
g
production by PBMCs from TB patients and HTR controls after
in vitro
stimulation with the 30-kDa Ag
Production of TNF-
a
, IFN-
g
and IL-10 in response to the 30-kDaAg was determined using ELISA in PBMC cultures from eachgroup of patients and HTR. The supernatants were collected 18(TNF-
a
, IL-10) and 96 (IFN-
g
) h after stimulation with the 30-kDa Ag (1·0
m
g/ml), and the cytokine levels peaked at 18 h forTNF-
a
and IL-10, and at 96 h for IFN-
g
(data not shown). As apositive control, supernatants were collected from cells stimu-lated with PHA (10
m
g/ml) at 48 h, or LPS (1
m
g/ml) at 18 h.
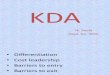
TNF-
a
.
As shown in Fig. 1a, MDR-TB patients had signifi-cantly reduced TNF-
a
production after stimulation with the 30-kDa Ag for 18 h, as compared with the HTR controls or TF-TBpatients (P
<
0·05 in both cases), or the N-TB patients (P
<
0·01).The TNF-
a
levels of PBMCs from MDR-TB patients weredecreased more significantly than those of PBMCs from the othergroups (P
<
0·001) after a 96-h stimulation with the 30-kDa Ag(data not shown). The greatest increase in TNF-
a
production inresponse to the 30-kDa Ag was in the N-TB patients, comparedwith the other groups (HTR, P
<
0·05; TF-TB, P
<
0·05; MDR-TB,P
<
0·01). LPS induced similar TNF-
a
titres in both healthy con-trols and MDR-TB patients (6510
±
2420 versus 5800
±
3190 pg/ml, P
>
0·1; data not shown).
IFN-
g
.
The data for IFN-
g
production by PBMCs were com-pared between groups at 96 h (Fig. 1b). The mean IFN-
g
concen-trations after stimulation with the 30-kDa Ag were significantlylower in each of the TB patient groups than in the HTR controls(N-TB, P
<
0·001; TF-TB, P
<
0·001; MDR-TB, P
<
0·001; Fig. 1b).However, there were no significant differences between thegroups of TB patients in IFN-
g
production after stimulation withthe 30-kDa Ag. PHA induced similar IFN-
g
titres in both healthycontrols and MDR-TB patients (9820
±
4190 versus8160
±
5340 pg/ml, P
>
0·1; data not shown).
IL-10.
As shown in Fig. 1c, IL-10 production was significantlyhigher in the MDR-TB patients than in the HTR controls after an18-h stimulation with the 30-kDa Ag (P
<
0·05). PBMCs from N-TB patients produced significantly more IL-10 after stimulationwith the 30-kDa Ag than did those from HTR controls (P
<
0·01)or TF-TB patients (P
< 0·05). LPS induced similar IL-10 titres inboth healthy controls and MDR-TB patients (1700 ± 555 versus1520 ± 580 pg/ml, P > 0·1; data not shown).
Effect of IFN-g and endogenous IL-10 neutralization on30-kDa Ag-induced TNF-a productionBecause TNF-a secretion in response to the 30-kDa Ag wasdepressed significantly in MDR-TB patients, subsequent experi-ments were carried out to further evaluate the effects of IFN-g orIL-10 on 30-kDa-induced TNF-a production by PBMCs. PBMCs
from five HTR individuals were cultured in complete RPMI withor without the 30-kDa Ag (1 mg/ml) following co-culture withrhIFN-g (10 ng/ml) or neutralizing antibodies to IL-10 (2 mg/ml).Culture supernatants were collected at 18 h and assayed for TNF-a production by ELISA. Endogenous TNF-a production byPBMCs from HTR or MDR-TB patients was unchanged after co-
0
500
1000
1500
0
1000
2000
3000
0
1000
2000
3000
4000 ***
*
**
HTR N-TB TF-TB MDR-TB
TB
Sec
rete
d T
NF
-a (p
g/m
l)
******
***
Sec
rete
d IF
N-g
(pg/
ml)
HTR N-TB TF-TB MDR-TB
TB
Sec
rete
d IL
-10
(pg/
ml)
HTR N-TB TF-TB MDR-TB
TB
****
**
****
(a)
(b)
(c)
Fig. 1. TNF-a and IFN-g production by PBMCs from TB patients andHTR after in vitro stimulation with the 30-kDa Ag of M. tuberculosis. ThePBMCs were stimulated with the 30-kDa Ag, and the supernatant har-vested after 18 and 96 h, respectively. Secreted TNF-a and IFN-g levels inthe culture supernatants were measured by ELISA, as described in Mate-rials and methods. The TNF-a (a), IFN-g (b) and IL-10 (c) levels in PBMCsfrom each group of TB patients and HTR were determined after in vitrostimulation with the 30-kDa Ag. The values are shown as the mean ± s.d.of triplicate supernatant samples. The data are from one representativeexperiment. *P < 0·05; **P < 0·01; ***P < 0·001 (Student’s t-test).

446 J.-S. Lee et al.
© 2003 Blackwell Publishing Ltd, Clinical and Experimental Immunology, 132:443–449
culture with IFN-g (Fig. 2). However, TNF-a secretion as a resultof LPS stimulation was increased significantly in both the HTRand MDR-TB patients (data not shown).
Interestingly, the TNF-a levels were elevated significantly incultures from HTR (P < 0·001) and MDR-TB patients (P < 0·05)that contained the neutralizing antibody to IL-10, whereas anIgG1 isotype control antibody used at the same concentration didnot affect TNF-a secretion (Fig. 2). The increases in TNF-a pro-duction were greater in the HTR group than in the MDR-TBgroup (1·6-fold increase for MDR-TB; 3·4-fold for HTR). There-fore, we found that endogenous IL-10 neutralization, but not theaddition of rhIFN-g, increases the 30-kDa-induced TNF-a secre-tion from the PBMCs of MDR-TB patients.
IL-8 production as a result of in vitro stimulation with the30-kDa Ag of PBMCs from TB patients and HTR controlsWe investigated whether chemokine levels were expressed differ-entially in the various clinical forms of TB. To compare the dif-ferences in IL-8 production between subject groups, the optimalIL-8 production was determined using ELISA in PBMC culturesfrom HTR subjects 6, 18, 48 and 96 h after stimulation with the 30-kDa Ag (1·0 mg/ml), and the peak IL-8 level was observed after 96h of stimulation in different donors (data not shown). Therefore,we compared the individual IL-8 concentrations between thegroups at 96 h poststimulation.
IL-8 production was significantly depressed in MDR-TBpatients in response to the 30-kDa Ag, compared with the N-TBpatients (MDR-TB, 316·2 ± 260·5 ng/ml; N-TB, 686·1 ± 346·8 ng/ml, P < 0·01; Fig. 3a). However, the IL-8 levels in PBMC fromMDR-TB patients did not differ significantly when comparedwith those from either TF-TB patients or HTR (P > 0·1). N-TBpatients showed significantly elevated IL-8 levels, when comparedwith HTR (P < 0·001) or MDR-TB patients. In addition, a signif-icant correlation was observed between IL-8 and TNF-a produc-tion in the culture supernatants of PBMC from TB patients
(n = 57, r = 0·58, P < 0·001; Fig. 3b), but not those from HTR con-trols (n = 20, r = 0·17, P > 0·1; Fig. 3b). LPS induced similar IL-8titres in both healthy controls and MDR-TB patients (790 ± 340versus 620 ± 390 ng/ml, P > 0·1; data not shown).
Effect of IFN-g and TNF-a on 30-kDa Ag-inducedsecretion of IL-8Next, we investigated whether IFN-g or TNF-a interact withchemokine production, thereby contributing to the overall hostdefense and pathogenic responses in TB. Therefore, we assessedthe effects of IFN-g and TNF-a on the levels of IL-8 induced inhuman PBMCs by the 30-kDa Ag. PBMCs from HTR controls(n = 7) were cultured in complete RPMI with or without the 30-kDa Ag (1 mg/ml) following co-culture with rhIFN-g (10 ng/ml),rhTNF-a (10 ng/ml), or both, or rhIFN-g with anti-TNF-a moAb(2 mg/ml). Culture supernatants were collected at 96 h andassayed for IL-8 production by ELISA.
Fig. 2. The effect of rhIFN-g or endogenous IL-10 on TNF-a induction bythe 30-kDa Ag of M. tuberculosis. PBMC from HTR (n = 5) and MDR-TB patients (n = 5) were cultured with or without rhIFN-g, neutralizingantibody to IL-10 (2 mg/ml), or control antibody (2 mg/ml). The 30-kDa Ag(1 mg/ml) was added to each of the cultures. Immunoreactivity for TNF-awas assessed in the culture supernatants at 18 h. The data are the mean ±s.d. of a representative result of three independent experiments. The per-centage increase in TNF-a immunoreactivity relative to the TNF-a levelof a culture that was treated with the 30-kDa Ag alone (100%) is shown.�, 30-kDa only; , 30-kDa + rhIFN-g; �, 30-kDa + a-IL-10; , 30-kDa + control IgG.
0
500
1000
1500
2000
2500
0
500
1000
1500
2000
2500
HTR MDR-TB
% T
NF
-a im
mun
orea
ctiv
ity
*
***
Fig. 3. IL-8 production by PBMC from TB patients and HTR in responseto the 30-kDa Ag of M. tuberculosis. (a) IL-8 production in TB patientsand HTR. The supernatants were prepared after 96 h, and the cytokineconcentrations were measured by ELISA. The values shown are the mean± s.d. of triplicate supernatant samples. The data are from one representa-tive experiment. (b) There was significant correlation between the IL-8and TNF-a levels in 30-kDa Ag-stimulated PBMCs from TB patients(n = 57, r = 0·58, P < 0·001), but not those from HTR controls (n = 20,r = 0·17, P > 0·1). �, HTR; —, HTR reg; r, TB; ···, TB reg.
0 1000 2000 3000 4000
0
500
1000
1500
0
500
1000
1500
2000
Sec
rete
d IL
-8 (
ng/m
l)
*****
HTR N-TB TF-TB MDR-TB
TB
Sec
rete
d IL
-8 (
ng/m
l)
Secreted TNF-a (pg/ml)
(a)
(b)

Depressed TNF-a in multidrug-resistant tuberculosis patients 447
© 2003 Blackwell Publishing Ltd, Clinical and Experimental Immunology, 132:443–449
As shown in Fig. 4a, there was significant up-regulation ofendogenous IL-8 in the Ag-stimulated PBMCs after co-culturewith rhTNF-a (P < 0·01), but not rhIFN-g (P > 0·05). In addition,IL-8 production was activated more significantly by stimulationwith both rhTNF-a and rhIFN-g (P < 0·001) than after co-culturewith rhTNF-a only; however, this effect was abrogated by theaddition of neutralizing anti-TNF-a MoAb (2 mg/ml). Co-culturewith the same concentration of isotype control antibody had noeffect on IL-8 formation (Fig. 4a).
We also assessed the effect of endogenous TNF-a neutraliza-tion on Ag-induced IL-8 secretion. PBMCs from HTR (n = 7)were stimulated with the 30-kDa Ag and cultured in completeRPMI with or without neutralizing antibody to TNF-a (2 mg/ml).The culture supernatants were collected at 96 h and assayed forIL-8 production by ELISA. Neutralization of the endogenousTNF-g with an anti-TNF-a MoAb (2 mg/ml) decreased the IL-8level approximately twofold in Ag-primed PBMCs from HTR,whereas the co-culture with the same concentration of isotypecontrol antibody had no effect on IL-8 formation (Fig. 4b).
Furthermore, PBMCs from MDR-TB patients (n = 7) werecultured in complete RPMI with or without the 30-kDa Ag (1 mg/ml) following co-culture with rhIFN-g (10 ng/ml) for 96 h.Although there was a substantial heterogeneity in the increase inIL-8 production in 30-kDa Ag-induced PBMCs from MDR-TBpatients, PBMCs from MDR-TB patients produced more IL-8after co-culture with rhTNF-a, compared with those by 30-kDaAg alone (Fig. 4c). The mean immunoreactivity of PBMC fromMDR-TB patients for IL-8 at 96 h was increased significantlyafter treatment with rhTNF-a (P < 0·01).
DISCUSSION
In this study, we found that depressed TNF-a levels in response tostimulation with the 30-kDa Ag were characteristic of MDR-TBpatients. MDR-TB patients in this study had clinically advanceddisease; the mean treatment duration was more than 2 years,despite antituberculosis drug therapy. Our data are in partialagreement with previous studies in which patients with fatal M.tuberculosis infection showed reduced secretion of proinflamma-tory cytokines, such as TNF-a, after ex vivo stimulation of wholeblood leucocytes [24]. In addition, monocytes from patients withchronic refractory TB have been found to release significantly
lower amounts of TNF-a than those from patients with N-TB [25].In contrast, a recent study showed that TNF-a production waselevated in cells from pulmonary TB patients in response to the30-kDa Ag, compared with cells from healthy controls [26]. Thisinconsistency may be due to differences in the clinical status of the
0
100
200
300
0
50
100
150
(a)
(b)
(c)
***
% IL
-8 im
mun
orea
ctiv
ity
% IL
-8 im
mun
orea
ctiv
ity
***
**
% IL
-8 im
mun
orea
ctiv
ity
*
0
100
200
300
400
500
++++++++
++++++
MDR-TB
30-kDarh IFN-grh TNF-aa-TNF-aControl IgG
30-kDaa-TNF-aControl IgG +
++++
Fig. 4. Effect of IFN-g and TNF-a on 30-kDa Ag-induced IL-8 productionby PBMC of MDR-TB patients. (a) Effect of rhIFN-g or rhTNF-a (each10 ng/ml) on IL-8 production induced by the 30-kDa Ag. PBMC fromHTR (n = 7) were cultured with or without rhIFN-g, rhTNF-a, rhIFN-g +rhTNF-a, rhIFN-g + anti-TNF-a antibody or rhIFN-g + control antibody.Then 30-kDa Ag (1 mg/ml) was added to each of the cultures. The culturesupernatants were collected at 96 h and assayed for IL-8 production byELISA. The percentage increase in IL-8 immunoreactivity relative to theIL-8 level of a culture that was treated with 30-kDa Ag alone (100%) isshown. (b) Effect of endogenous TNF-a on IL-8 production that wasinduced by the 30-kDa Ag. PBMC from HTR (n = 7) were stimulated withthe 30-kDa Ag and cultured with or without neutralizing antibody to TNF-a (2 mg/ml) or control antibody (2 mg/ml). The percentage increase in IL-8 immunoreactivity relative to the IL-8 level of a culture that was treatedwith 30-kDa Ag alone is shown. (c) Effects of rhTNF-a on 30-kDa Ag-induced IL-8 production by PBMC from MDR-TB patients (n = 7). Thedata are representative of three separate experiments. �, 30-kDa; �, 30-kDa + rhTNF-a.

448 J.-S. Lee et al.
© 2003 Blackwell Publishing Ltd, Clinical and Experimental Immunology, 132:443–449
TB patients studied. It seems that decreased TNF-a levels do notsimply reflect the chronic conditions of these patients, since therewere no significant correlations between treatment duration andTNF-a levels. In addition, there were no significant associationsbetween various parameters (performance status, malnutritionexamined by body mass index, chest X-ray findings or IFN-g lev-els) and TNF-a levels in the patients with MDR-TB and TF-TB.Therefore, our results suggest that TNF-a depression induced bythe 30-kDa antibody is a unique finding associated with the strainsinfecting MDR-TB patients.
The depressed levels of IFN-g in these patients may not beresponsible for the decrease in TNF-a secretion. Our data arepartly in accordance with the previous finding that preincubationof monocytes with IFN-g did not augment BCG-induced TNF-aproduction, whereas LPS induced the production of largeamounts of TNF-a from cultured monocytes [25]. Although IFN-g activates mononuclear phagocytes, which results in enhancedendotoxin-induced TNF-a release [27], both endotoxin and myco-bacterial Ag may stimulate monocytes to produce TNF-a by dif-ferent mechanisms.
The mechanism underlying the decreased TNF-a levels inMDR-TB patients may be associated with the presence of IL-10,based on the finding that IL-10 neutralization significantlyincreased the TNF-a levels in PBMC from HTR and MDR-TBpatients. Our data are partially consistent with previous findingsthat neutralization of IL-10 prolonged TNF-a mRNA expression,and significantly increased net TNF-a production in humanmonocytes after LPS stimulation [28]. The same study demon-strated that potentiation of TNF-a production by IFN-g in mono-cytes was coupled to the inhibition of endogenous IL-10expression [28]. Our previous results [3] and the current data sug-gest that increased IL-10 production by PPD-stimulated PBMCfrom MDR-TB patients is associated with depressed TNF-asecretion in MDR-TB patients. However, the TNF-a increaseswere greater in HTR than in MDR-TB, although the IL-10 levelswere significantly elevated in MDR-TB patients versus HTRpatients. Therefore, our findings show that IL-10 neutralizationplays an important, but not exclusive, role in the TNF-a secretionfrom PBMCs of MDR-TB patients following in vitro stimulationwith the 30-kDa Ag.
We suggest that the rate of apoptosis in monocyte-derivedcells from MDR-TB patients is higher than in HTR after expo-sure to mycobacterial Ags, as seen in a previous study [26]. Thepercentage of apoptotic monocytes tends to be higher in TBpatients than in healthy controls, both in non-stimulated cell cul-tures and in those incubated in the presence of mycobacterialAgs [26]. Although we were not able to examine the rate of apo-ptosis in the Ag-stimulated monocytes from these patients, thenumber of monocytes, which is the main source of TNF-a, wasnot different in MDR-TB patients and HTR (data not shown).In addition, the PBMC of MDR-TB patients showed similarcytokine production patterns in response to LPS when comparedwith HTR.
Previous studies indicate that spontaneous TNF-a and IL-1bsecretion by peripheral blood monocytes is significantly higher inTB patients [29]. Although we did not measure the spontaneoussecretion of TNF-a in all the patients in this study, we suggest thatthe mononuclear cells from these patients are anergic due torepetitive, chronic antigenic stimulation in vivo. Further studiesshould clarify the mechanisms underlying the TNF-a depressionafter stimulation with the 30-kDa Ag.
Several reports have demonstrated that IL-8 is produced bymonocytes and alveolar macrophages that are infected in vitrowith M. tuberculosis or stimulated in vitro with PPD [17,30]. IL-8is a member of the CXC chemokine subfamily, and the mostprominent sources of IL-8 are monocytes and macrophages [31].Although several studies have focused on the central role of IL-8in the normal immune response to TB, i.e. through leucocyterecruitment to areas of granuloma formation [32,33], little isknown about chemokine production in pulmonary TB patients interms of their distinct disease statuses or infecting strains. The cur-rent data show that IL-8 is elevated significantly in the 30-kDaAg-stimulated PBMC from N-TB patients compared with thosefrom MDR-TB patients. However, there were no significant dif-ferences in the levels of IL-8 secretion between MDR-TB and TF-TB patients. However, our data are inconsistent with the previousfinding that IL-8 production by PBMC in response to ex vivo stim-ulation with PPD was similar in normal blood donors and patientswith pulmonary TB [34]. This discrepancy might be due to the dis-ease status of pulmonary TB patients, because the mean durationof anti-TB treatment in the previous studies was approximately6 months [34], and our data are unique in demonstrating differ-ential IL-8 production in various disease states.
We also found that rhTNF-a directly increased IL-8 secretionby PBMC from HTR or MDR-TB patients. TNF-a is a pluripo-tent activator of inflammation and induces a proinflammatorycytokine cascade, which is mediated partly by the inducibleexpression of IL-8 [35]. The previous study also demonstratedthat TNF-a-induced IL-8 expression was dependent on nuclearfactor-kB through a delayed, reactive oxygen species-dependentsignalling pathway [35]. Our data emphasize an additional criticalrole of TNF-a in the regulation of IL-8 expression, and furtherdefinition of this pathway will yield new insights into the mecha-nisms underlying inflammation that is initiated by TNF-a.
In conclusion, our results demonstrate that 30-kDa Ag-stim-ulated PBMCs from MDR-TB patients have significantlydepressed levels of TNF-a, although the levels of IL-8 in PBMCfrom these patients are not significantly different from those ofTF-TB patients. The depression of TNF-a secretion in MDR-TBpatients is partially alleviated by neutralizing antibody to IL-10.In addition, TNF-a may contribute to the innate immuneresponse to TB infection through the regulation of IL-8. There-fore, diminution of TNF-a levels may impair host immunedefences critically in MDR-TB patients.
ACKNOWLEDGEMENTS
This study was supported by a grant of the Korea Health 21 R&D Project,Ministry of Health and Welfare, Republic of Korea (01-PJ10-PG6–01G03-002).
REFERENCES
1 Raviglione MC, Snider DE Jr, Kochi A. Global epidemiology of tuber-culosis. Morbidity and mortality of a worldwide epidemic. JAMA 1995;273:220–6.
2 McDyer JF, Hackley MN, Walsh TE, Cook JL, Seder RA. Patientswith multidrug-resistant tuberculosis with low CD4+ T cell counts haveimpaired Th1 responses. J Immunol 1997; 158:492–500.
3 Lee JS, Song CH, Kim CH et al. Profiles of IFN-g and its regulatorycytokines (IL-12, IL-18, and IL-10) in peripheral blood mononuclearcells from patients with multidrug-resistant tuberculosis. Clin ExpImmunol 2002; 128:516–24.

Depressed TNF-a in multidrug-resistant tuberculosis patients 449
© 2003 Blackwell Publishing Ltd, Clinical and Experimental Immunology, 132:443–449
4 Keane J, Gershon S, Wise RP et al. Tuberculosis associated with inflix-imab, a tumor necrosis factor alpha-neutralizing agent. N Engl J Med2001; 345:1098–104.
5 Flynn JL, Goldstein MM, Chan J et al. Tumor necrosis factor-a isrequired in the protective immune response against Mycobacteriumtuberculosis in mice. Immunity 1995; 2:561–72.
6 Hernandez-Pando R, Orozco H, Arriaga K, Sampieri A, Larriva-SahdJ, Madrid-Marina V. Analysis of the local kinetics and localization ofinterleukin-1, tumour necrosis factor-a and transforming growth fac-tor-b, during the course of experimental pulmonary tuberculosis.Immunology 1997; 90:607–17.
7 Bean AG, Roach DR, Briscoe H et al. Structural deficiencies in gran-uloma formation in TNF gene-targeted mice underlie the heightenedsusceptibility to aerosol Mycobacterium tuberculosis infection, which isnot compensated for by lymphotoxin. J Immunol 1999; 162:3504–11.
8 Mohan VP, Scanga CA, YuK et al. Effects of tumor necrosis factoralpha on host immune response in chronic persistent tuberculosis: pos-sible role for limiting pathology. Infect Immun 2001; 69:1847–55.
9 Maini R, St Clair EW, Breedveld F et al. Infliximab (chimeric anti-tumour necrosis factor monoclonal antibody) versus placebo in rheu-matoid arthritis patients receiving concomitant methotrexate: a ran-domised phase III trial. ATTRACT Study Group. Lancet 1999;354:1932–9.
10 Nunez Martinez O, Ripoll Noiseux C, Carneros Martin JA, GonzalezLara V, Gregorio Maranon HG. Reactivation tuberculosis in a patientwith anti-TNF-a treatment. Am J Gastroenterol 2001; 96:1665–6.
11 Tracey KJ, Cerami A. Tumor necrosis factor: a pleiotropic cytokineand therapeutic target. Annu Rev Med 1994; 45:491–503.
12 Oppenheim JJ, Zachariae CO, Mukaida N, Matsushima K. Propertiesof the novel proinflammatory supergene intercrine cytokine family.Annu Rev Immunol 1991; 9:617–48.
13 Premack BA, Schall TJ. Chemokine receptors: gateways to inflamma-tion and infection. Nature Med 1996; 2:1174–8.
14 Schluger NW, Rom WN. The host immune response to tuberculosis.Am J Respir Crit Care Med 1998; 157:679–91.
15 Gerszten RE, Garcia-Zepeda EA, Lim YC et al. MCP-1 and IL-8 trig-ger firm adhesion of monocytes to vascular endothelium under flowconditions. Nature 1999; 398:718–23.
16 Kurashima K, Mukaida N, Fujimura M et al. Elevated chemokine lev-els in bronchoalveolar lavage fluid of tuberculosis patients. Am JRespir Crit Care Med 1997; 155:1474–7.
17 Sadek IM, Sada E, Toossi Z, Schwander SK, Rich EA. Chemokinesinduced by infection of mononuclear phagocytes with mycobacteriaand present in lung alveoli during active pulmonary tuberculosis. AmJ Respir Cell Mol Biol 1998; 19:513–21.
18 Torres M, Herrera T, Villareal H, Rich EA, Sada E. Cytokine profilesfor peripheral blood lymphocytes from patients with active pulmonarytuberculosis and healthy household contacts in response to the 30-kilo-dalton antigen of Mycobacterium tuberculosis. Infect Immun 1998;66:176–80.
19 Zhang M, Lin Y, Iyer DV, Gong J, Abrams JS, Barnes PF. T-cell cytok-ine responses in human infection with Mycobacterium tuberculosis.Infect Immun 1995; 63:3231–4.
20 Song CH, Kim HJ, Park JK et al. Depressed interleukin-12 (IL-12), butnot IL-18, production in response to a 30- or 32-kilodalton mycobac-
terial antigen in patients with active pulmonary tuberculosis. InfectImmun 2000; 68:4477–84.
21 Aung H, Toossi Z, Wisnieski JJ et al. Induction of monocyte expressionof tumor necrosis factor alpha by the 30-kD alpha antigen of Myco-bacterium tuberculosis and synergism with fibronectin. J Clin Invest1996; 98:1261–8.
22 Jo EK, Kim HJ, Lim JH et al. Dysregulated production of interferon-gamma, interleukin-4 and interleukin-6 in early tuberculosis patients inresponse to antigen 85B of Mycobacterium tuberculosis. Scand JImmunol 2000; 51:209–17.
23 Lim JH, Park JK, Jo EK et al. Purification and immunoreactivity ofthree components from the 30/32-kilodalton antigen 85 complex inMycobacterium tuberculosis. Infect Immun 1999; 67:6187–90.
24 Friedland JS, Hartley JC, Hartley CG, Shattock RJ, Griffin GE. Inhi-bition of ex vivo proinflammatory cytokine secretion in fatal Mycobac-terium tuberculosis infection. Clin Exp Immunol 1995; 100:233–8.
25 Takashima T, Ueta C, Tsuyuguchi I, Kishimoto S. Production of tumornecrosis factor alpha by monocytes from patients with pulmonarytuberculosis. Infect Immun 1990; 58:3286–92.
26 Portales-Perez DP, Baranda L, Layseca E et al. Comparative and pro-spective study of different immune parameters in healthy subjects atrisk for tuberculosis and in tuberculosis patients. Clin Diagn Labora-tory Immunol 2002; 9:299–307.
27 Collart MA, Belin D, Vassalli JD, de Kossodo S, Vassalli P. Gammainterferon enhances macrophage transcription of the tumor necrosisfactor/cachectin, interleukin 1, and urokinase genes, which are con-trolled by short-lived repressors. J Exp Med 1986; 164:2113–8.
28 Donnelly RP, Freeman SL, Hayes MP. Inhibition of IL-10 expressionby IFN-gamma up-regulates transcription of TNF-alpha in humanmonocytes. J Immunol 1995; 155:1420–7.
29 Wang CH, Lin HC, Liu CY, Huang KH, Huang TTYuCT, Kuo HP.Upregulation of inducible nitric oxide synthase and cytokine secretionin peripheral blood monocytes from pulmonary tuberculosis patients.Int J Tuberc Lung Dis 2001; 5:283–91.
30 Zhang Y, Broser M, Cohen H et al. Enhanced interleukin-8 release andgene expression in macrophages after exposure to Mycobacteriumtuberculosis and its components. J Clin Invest 1995; 95:586–92.
31 Yoshimura T, Matsushima K, Tanaka S et al. Purification of humanmonocyte derived neutrophil chemotactic factor that shares sequencehomology with other host defense cytokines. Proc Natl Acad Sci USA1987; 84:9233–7.
32 Kindler V, Sappino AP, Grau GE, Piguet PF, Vassalli P. The inducingrole of tumor necrosis factor in the development of bactericidal gran-ulomas during BCG infection. Cell 1989; 56:731–40.
33 Ameixa C, Friedland JS. Down-regulation of interleukin-8 secretionfrom Mycobacterium tuberculosis-infected monocytes by interleukin-4and -10 but not by interleukin-13. Infect Immun 2001; 69:2470–6.
34 Nakaya M, Yoneda T, Yoshikawa M et al. The evaluation of interleu-kin-8 (IL-8) and tumor necrosis factor-alpha (TNF-alpha) level inperipheral blood of patients with active pulmonary tuberculosis.Kekkaku 1995; 70:461–6.
35 Vlahopoulos S, Boldogh I, Casola A, Brasier AR. Nuclear factor-kap-paB-dependent induction of interleukin-8 gene expression by tumornecrosis factor alpha: evidence for an antioxidant sensitive activatingpathway distinct from nuclear translocation. Blood 1999; 94:1878–89.