Embed Size (px)
Citation preview

British Journal of Plastic Surgery (1982) 35, 80-8 1 0 1982 The Trustees of British Association of Plastic Surgeons
0007-1226/X2/0276-0080 $02.00
The pectoralis major myocutaneous flap for intraoral reconstruction: a word of warning
DARRYL J. HODGKINSON
Newport News, Virginia, USA
Summary-The pectoralis major myocutaneous flap is an extremely versatile flap in head and neck reconstruction. However, failure to drain adequately the neck and chest wounds may lead to serious trouble should a fistula develop. A case report is presented as a cautionary tale.
The use of the pectoralis major myocutaneous flap is an important advance in the reconstructive surgery of the head and neck area particularly after cancer ablation (Ariyan, 1980). Indeed it has been suggested that it can replace the more conventional delto-pectoral flap, over which it has several advantages (Mendelson, 1980).
A recent experience with this flap illustrates a potentially dangerous complication related to the donor defect on the chest wall. If a fistula develops, this closed space may become heavily infected with a mixture of streptococci, gram- negative and anaerobic organisms.
Case report
A man aged 56 presented with a malignant lesion in the posterior tongue and retromolar trigone area with no palpable cervical glands. A classical hemimandibul- ectomy resection of the posterior tongue, floor of mouth, left tonsillar fossa and faucial pillars was performed with a 2cm margin of clearance. A large defect was produced in the posterior oropharynx which was closed with a pectoralis major island flap measur- ing approximately 8 cm x 8 cm. The chest defect was closed and the flap was tunnelled into the neck and turned back on itself to cover the carotid vessels and close the defect in the posterior oropharynx. The cheek flap used for access was replaced. No bone graft was inserted and the contour of the face and neck was restored by the soft tissue bulk only. A tracheostomy was performed and the patient was started immediately on total parenteral feeding. His immediate post-operative course was uneventful and the tracheostomy tube was removed on the fourth day (Fig. 1).
The patient could cough vigorously, suck out his own mouth and was very independent during this period. However, on the sixth day after a bout of rigorous coughing, a haematoma developed in the
chest wall. Repeated coughing forced the haematoma upwards through the neck into the oral cavity to produce a fistula. The haematoma on the chest wall rapidly became infected and within 24 hours a huge abscess cavity had formed, lined by greenish, purulent, necrotic material. On opening the cavity it was noted that the cut borders of the pectoralis muscle were acutely infected. Radical excision of the necrotic material left a defect measuring 30 x 30cm. Cultures from the wound cavity grew enterobacter, streptococci and E. coli. The patient was started on intravenous Keflin (cephalothin) 1 g every four hours and Ticarcillin, 3 g every four hours. The wound was dressed four hourly with fluffed gauze and Betadine. Over the next week the fistula became smaller and granulation tissue appeared (Fig. 2). Split-thickness skin grafts were applied ten days later. The patient was discharged two weeks later. The pectoralis myocut- aneous flap survived.
Discussion
Intraoral reconstruction with a pectoralis major myocutaneous flap may be complicated by in- fection in the chest wall should a fistula develop. Both Ariyan (1980) and Vasconez et al. (1980) have pointed out that the pectoralis major myocutaneous flap can survive in the face of infection but in our case the combination of intraoral organisms in a closed chest-wall hae- matoma produced a fulminating, gangrene in the cut edges of the muscle and the subcutaneous tissues. Prompt drainage of the chest wall and excision of the necrotic tissues were required and the flap survived.
To prevent such infections it is suggested that large suction drains should be placed in the upper and lower sections of the chest-wall defect
80
THE PECTORALIS MAJOR MYOCUTANEOUS FLAP FOR INTRAORAL RECONSTRUCTION 81
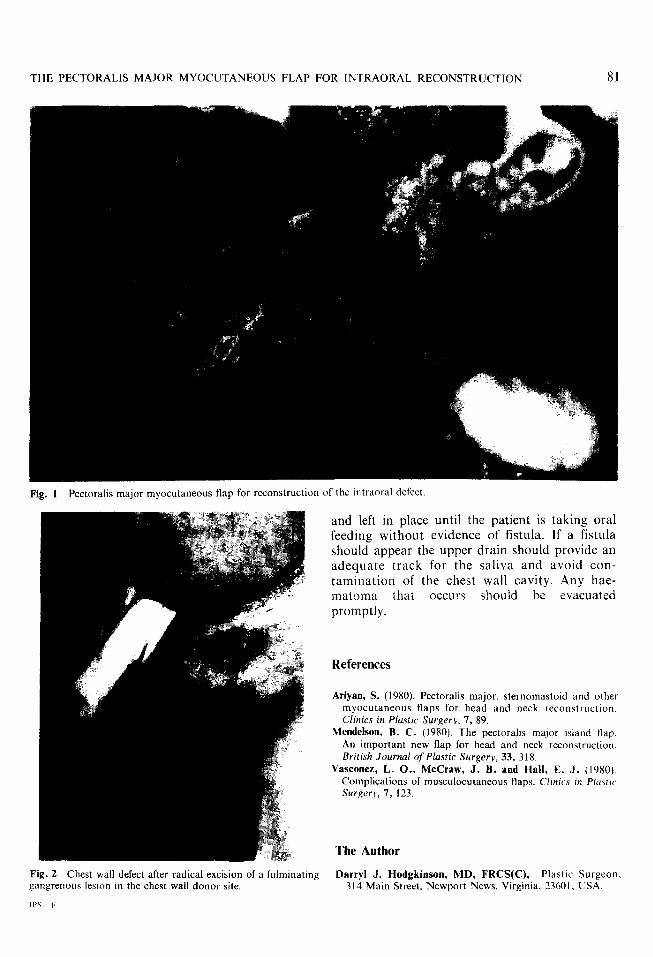
Fig. 1 Pectoralis major myocutaneous flap for reconstruction of the intraoral defect
Fig. 2 Chest wall defect after radical excision of a fulminating gangrenous lesion in the chest wall donor site.
and left in place until the patient is taking oral feeding without evidence of fistula. If a fistula should appear the upper drain should provide an adequate track for the saliva and avoid con- tamination of the chest wall cavity. Any hae- matoma that occurs should be evacuated promptly.
References
Ariyan, S. (1980). Pectoralis major, sternomastoid and other myocutaneous flaps for head and neck reconstructton. Clinics in Plustic Surgery, 7, 89.
Mendelson, B. C. (1980). The pectoralis major island flap. An important new flap for head and neck reconstruction. British Journal of’ Plastic Surgery, 33, 318.
Vasconez, L. O., McGraw, J. B. and Hall, E. J. (1980). Complications of musculocutaneous flaps. Clinics in Plusfit Surger)~, 7, 123.
The Author
Darryl J. Hodgkinson, MD, FRCS(C), Plastic Surgeon. 314 Main Street, Newport News, Virginia. 73601. USA.





























