Embed Size (px)
Citation preview

The pathogenic track to urinary tract
URINARY TRACT INFECTIONS
Ibrahim Al-Orainey,FACP,FRCP(Lond)
Professor of medicine
Faculty of Medicine, King Saud University

Urinary tract infections
• Asymptomatic bacteriuria
• Acute cystitis
• Acute pyelonephritis
Uncomplicated / complicated UTI
Epidemiology of UTI
• UTI is more common in females.(1-2% of young nonpregnant women)
• 40% of females will have a symptomatic UTI in their life time.
• In men: prevalence is 0.04%.• Incidence of UTI increases in old age.
(10% of men & 20% of women)
Risk factors for UTI
• in females:pregnancy, spermicidal contraceptives,
diaphragm, estrogen deficiency, diabetes.
• In males:lack of circumcision, prostatic hypertrophy, use of condom catheter.
• in both :old age , obstruction, vesicoureteric reflux, instrumentation, neurogenic bladder, renal transplantation.

Infecting organisms
E.coli ProteusKlebsiella PseudomonasEnterobacter EnterococciStaphylococci Candida

Pathogenesis of UTI
Host defences:• Urinary bladder is usually resistant to
bacterial colonisation.• Bacteria accessing the bladder are
eliminated by: - flushing mechanism - urine inhibitors (PH, osmolality, urea)
- uroepithelial defences (cytokines,PMNs) - Tamm- Horsfall protien

Pathogenesis of UTI
Organism features:• Most E.coli causing UTI belong to O,K and H
serotypes.• Uropathogenic E.coli virulence factors:
- Have fimbria (for adherence).- Secrete hemolysin & aerobactin.- Resist serum bacterical action.- Have higher K capsular antigen.
• Adherence is important in other bacteria.


Pathogenesis of UTI
• Periutheral area & urethra are colonised by bacteria.
• Bacteria enter bladder in susceptable host.• Adherence properties enable pathogens to
colonise bladder.• Pathogens attach to uroepithelial mucosa
secretion of cytokines recruitment of PMNs inflammation.
• Pathogens may ascend through ureter to kidney pyelonephritis.
Clinical presentation of UTI
Asymptomatic bacteriuria:• Common in females & elderly.• 25% develop symptomatic UTI .• 25% clear spontaneously.• Spontaneous cure & reinfection are common.
Cystitis:• Frequency, dysurea , urgency.• Suprapubic discomfort +/- tenderness.• Fever is often absent.
Clinical presentation of UTI
Acute pyelonephritis:• Fever, abdominal pain, vomiting.• Dysuria ,frequency, flank or loin pain.• Flank or loin tenderness.• In elderly: symptoms are often atypical.• Bacteremia is common.
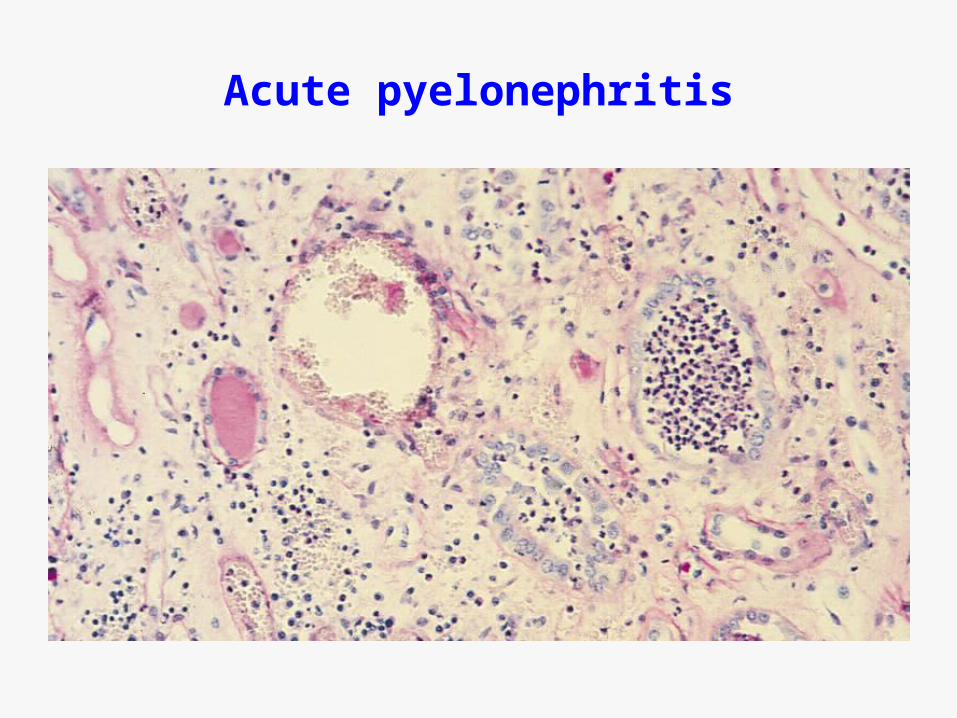
Acute pyelonephritis

Acute pyelonephritis


Special situations

Special situations
UTI in pregnancy:• Asymptomatic bacteriuria occurs in 4-8%.• Of these: 25% develop acute pyelonephritis.• Pyelonephritis in pregnancy predisposes to:
- premature delivery.- low birth weight infant.- increased newborn mortality.

Special situations
Catheter associated UTI :• Bacteriuria occurs in 10-15% of cathed pts. • All chronicly cathed pts. develop bacteriuria.• Organisms: E.coli, Proteus, Klebsiella, Serratia
Pseudomonas, Enterococci, Candida.
• Antibiotic resistance is common.• Symptoms are often absent or minimal.• Intermittent cathing reduces infections.

Diagnosis of UTI
• Urine dipstick:- leukocyte esterase- nitrite
• Urine microscopy:-WBCs, WBC casts, RBCs- Bacteria ( 1 bact/hpf = significant )
Diagnosis of UTI
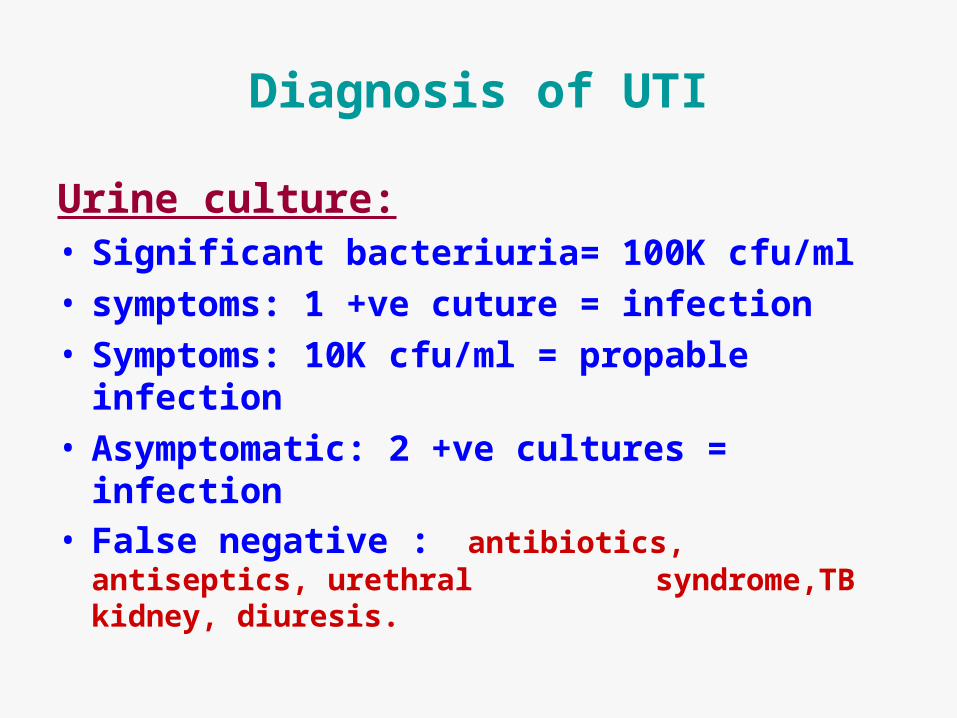
Urine culture:• Significant bacteriuria= 100K cfu/ml• symptoms: 1 +ve cuture = infection• Symptoms: 10K cfu/ml = propable infection• Asymptomatic: 2 +ve cultures = infection• False negative : antibiotics, antiseptics, urethral
syndrome,TB kidney, diuresis.

Natural history of UTI
• Treatment of uncomplicated UTI leads to complete resolution and cure.
• Recurrences occur in some patients usually within 2-3 monthes of initial infection.
• Frequent recurrences usually occur in clusters followed by long remissions.
• Recurrent uncomplicated UTI does not lead to chronic renal impairment or failure.
• Recurrent complicated UTI may lead to renal failure.• UTI may accelerate progression of underlying renal
disease.
Treatment of UTI
Acute pyelonephritis:• Mild infections are treated orally.
(fluoroquinolones,co-trimoxazole,cefuroxime)• Moderate - severe infections – parenteral trt.
(aminoglycosides,ceftriaxone,aztreonam,tazocin)• Therapymarked decline in bact.count after 48hrs.• Persistant fever, +ve blood culture after 3 days of
therapy..R/O obstruction, abscess.• After defervescence..change to oral therapy to
complete 2 weeks.• In males look for a predisposing cause.• FU urine cultures 2 weeks after end of therapy.

Treatment of UTI
• Cystitis:• young females: 3 days of oral therapy
(fluoroquinolone,cotrimoxazole,cefuroxime,augmentin)
• In females: symptoms x 7 days or history of previous infection 7 days
therapy.• In males : oral therapy for 7-10 days.

Treatment of UTI
Asymptomatic bacteriuria• No urgency to treat – confirm by 2 cultures.• Treatment is indicated in :
- Pregnancy- Children with VU reflux- Urinary obstruction
• Treatment is not indicated in :- Young nonpregnant women without
structural abnormalities- Elderly patients

Structural abnormalities should be corrected
Treatment of UTI
• Relapse of infection:• Relapse may be due to :
- renal invovement- structural abnormalities- chronic bacterial prostatitis
• Relapses need to be treated for 2 weeks.• Obstuction should be corrected .• If uncorrectable obstruction: treatment is prolonged
for 4-6 weeks or as required.• The latter group needs FU by monthly cultures and
annual assessment of kidneys.• In males R/O chronic prostatitis.

Treatment of UTI
Recurrent UTI:• Infrequent symptomatic UTI : treat attacks.• In females, reinfections may be related to sexual
activity – attacks may be reduced by: - avioding use of spermicidal contraceptives - voiding after intercourse - post coital single dose therapy
• If no precipitating factors – long term prophylaxis.• Long term prophylaxis is also indicated for frequent
asymptomatic infection in:- Children with VU reflux - Patients with obtructive uropathy

What is the prognosis ?
So I learned something ,how about you ?
وقل رب زدني علما
صدق الله العظيم
Confused..I did not understand any thing,did you?

![7 Catheter-associated Urinary Tract Infection (CAUTI) · UTI Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CAUTI] and Non-Catheter-Associated Urinary Tract](https://img.dokumen.tips/doc/110x75/5c40b88393f3c338af353b7f/7-catheter-associated-urinary-tract-infection-cauti-uti-urinary-tract-infection.jpg)



























