Embed Size (px)
Citation preview

The Path of Least Resistance:
A Primer on Outpatient
Antimicrobial StewardshipJason Alegro, Pharm.D., BCPS, Infectious Diseases Clinical Specialist, Mount Sinai Hospital
Tanya Abi-Mansour, Pharm.D., Infectious Diseases/Stewardship Clinical Specialist, IU Health

▶Dr. Alegro and Dr. Abi-Mansour declare no conflicts of
interest, real or apparent, and no financial interests in
any company, product, or service mentioned in this
program, including grants, employment, gifts, stock
holdings and honoraria.
Disclosures and Conflict of Interest
At the conclusion of the program, the pharmacists will be
able to:
1. Describe current issues in antibiotic resistance and the
consequences of inappropriate outpatient antibiotic
prescribing.
2. Discuss the 2017 Joint Commission Standard of Antibiotic
Stewardship as well as the Centers for Disease Control
(CDC) Core Elements of Outpatient Antibiotic
Stewardship.
3. Identify evidence-based interventions that can be
implemented in the outpatient setting in order to promote
appropriate antibiotic prescribing.
Pharmacist Objectives

At the conclusion of this program, the pharmacy technicians
will be able to:
1. Define outpatient antibiotic stewardship.
2. List consequences of inappropriate antibiotic prescribing.
3. Describe the role of the pharmacist in antibiotic
stewardship.
Technician Objectives
1. Which of the following best describes antimicrobial
stewardship?
a. Choosing the least expensive antibiotic for a patient
b. Choosing the most appropriate antibiotic for a patient
c. Choosing the most broad-spectrum antibiotic for a patient
d. Choosing the antibiotic which a patient most prefers
Pre-Test Questions

2. Which of the following is a benefit of antimicrobial
stewardship?
a. Decrease in superinfections due to Clostridium difficile
b. Development of antimicrobial resistance
c. Increased antimicrobial costs
d. Increased use of intravenous antibiotics
Pre-Test Questions

3. Which of the following is NOT a CDC core element of
antibiotic stewardship?
a. Action for policy and practice
b. Tracking and reporting
c. Education and expertise
d. Prescriber disciplinary action
Pre-Test Questions

4. Which of the following is an intervention that can improve
utilization of antibiotics in the outpatient setting?
a. Utilize watch and wait practices when appropriate
b. Reprimand patients when they ask for antibiotics
c. Always advocate for empiric antibiotic use
d. Provide education to prescribers only, not patients
Pre-Test Questions

A Day in the Life of an Antibiotic
Steward

A few questions for you!
https://i.ytimg.com/vi/-XLPptxdlic/maxresdefault.jpg

Antimicrobial Resistance:
What’s the Big Deal?
Antibiotics: A Patient Safety Issue
▶ More than 2,000,000 Americans develop infection resistant to one or
more antibiotics
▶ At least 23,000 people die each year as a direct result
▶ Clostridium difficile has become the most common cause of health
care-associated infection
▶ Causes 500,000 infections annually
▶ Excess health care costs ~$4.8 billion for acute care facilities alone
Antibiotic Resistance Threats in the United States, 2013. CDC. Published online September 16, 2013.
13

How well do we use antibiotics?
Of the estimated 154 million outpatient
prescriptions for antibiotics, 30% are unnecessary
Antibiotic Use in the United States, 2017: Progress and Opportunities, 2017. CDC
14
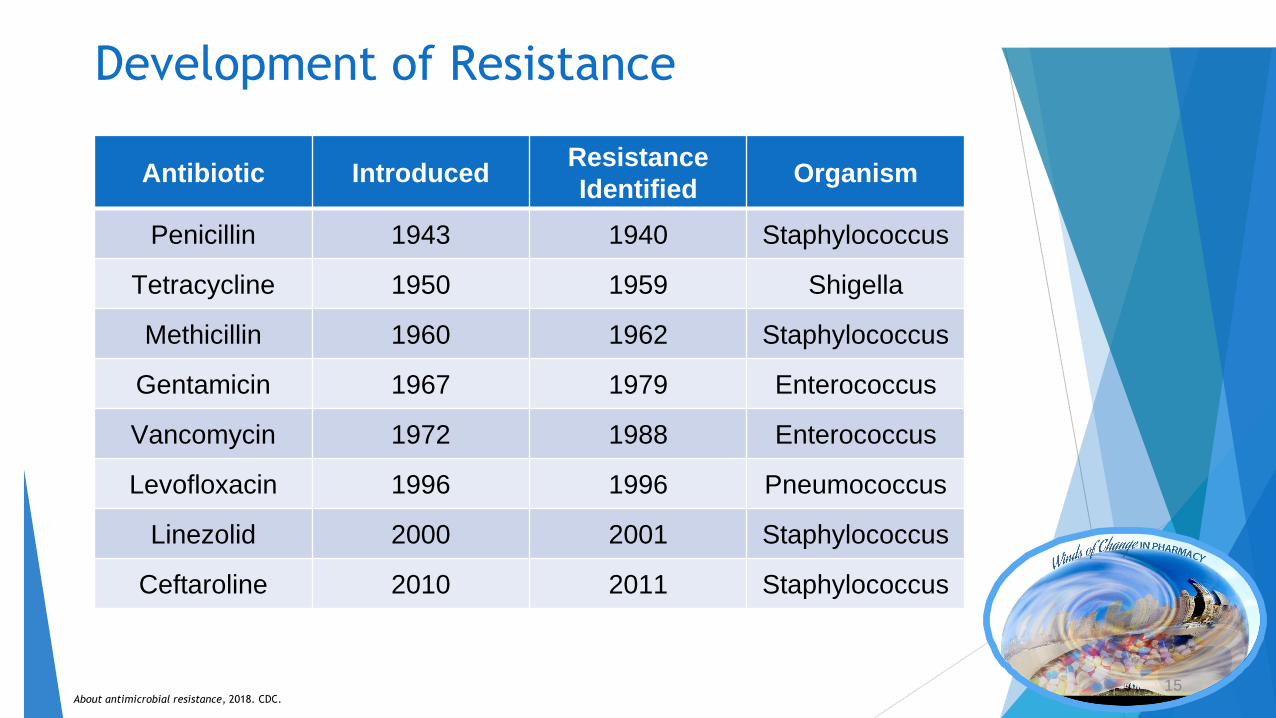
Development of Resistance
Antibiotic IntroducedResistance
IdentifiedOrganism
Penicillin 1943 1940 Staphylococcus
Tetracycline 1950 1959 Shigella
Methicillin 1960 1962 Staphylococcus
Gentamicin 1967 1979 Enterococcus
Vancomycin 1972 1988 Enterococcus
Levofloxacin 1996 1996 Pneumococcus
Linezolid 2000 2001 Staphylococcus
Ceftaroline 2010 2011 Staphylococcus
About antimicrobial resistance, 2018. CDC. 15

National Resistance ThreatsUrgent Threats
• Clostridium difficile • Carbapenem-resistant Enterobacteriaceae (CRE) • Drug-resistant N. gonorrhoeae
Serious Threats • MDR Acinetobacter • MDR Pseudomonas aeruginosa • Extended-spectrum β-lactamases in
Enterobacteriaceae (ESBLs) • Vancomycin-resistant Enterococcus (VRE) • Methicillin-resistant S. aureus (MRSA)
Concerning Threats • Vancomycin-resistant S. aureus (VRSA)
Antibiotic Resistance Threats in the United States, 2013. CDC. Published online September 16, 2013.
16

Oneill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. Review on Antimicrobial Resistance. 2014.
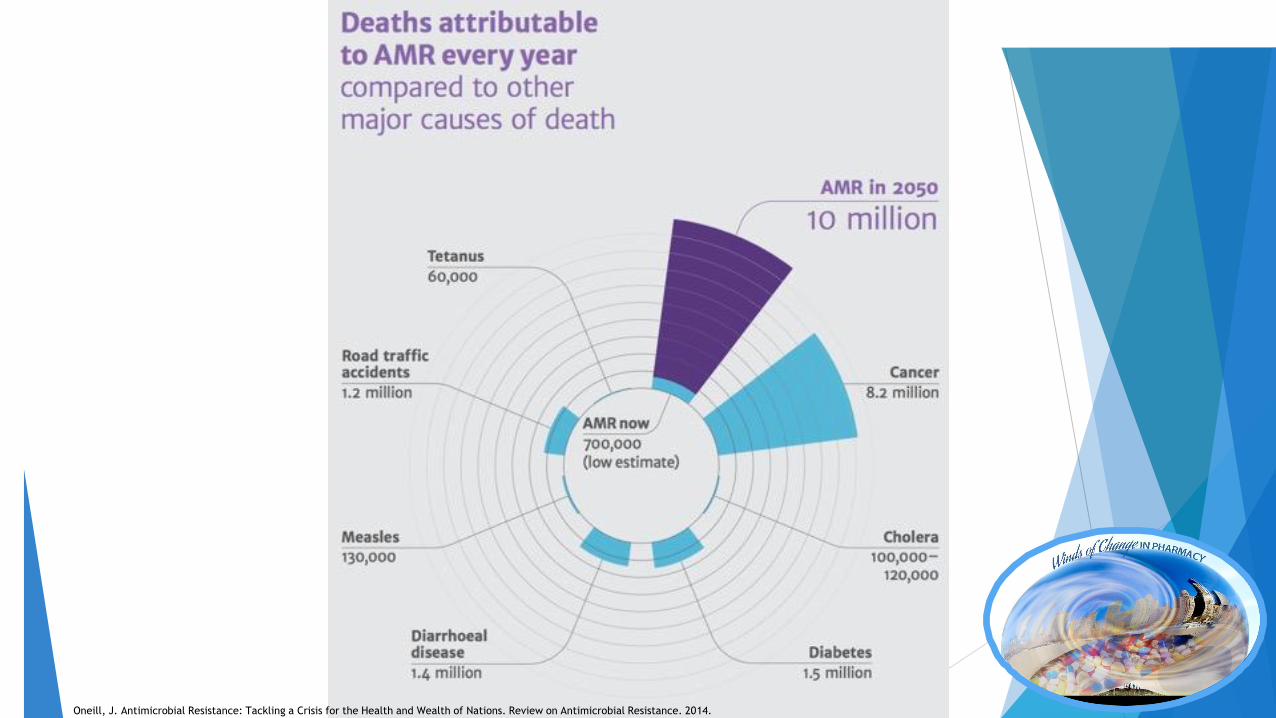
Oneill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. Review on Antimicrobial Resistance. 2014.

What is Antibiotic Stewardship?
http://2.bp.blogspot.com/-skCPGjig6Nw/UrRT5z4B8mI/AAAAAAAAApk/zHuX1yMUiGM/s1600/education--Quotes-Albert-Einstein.jpg

What is Antimicrobial Stewardship?
Antimicrobial Stewardship
Right Diagnosis
Right Drug
Right Dose
Right Duration
De-esclation
Clin Infect Dis. 2016 May 15; 62(10) e51-77.
The selection of the optimal antimicrobial drug regimen, including dose, route,
and duration of therapy
20
The Right Diagnosis
Does this patient have bacterial pneumonia, the flu, or an acute viral illness?
Does the patient meet the appropriate criteria for antibiotic treatment for a COPD exacerbation?
Does the child meet appropriate criteria for receiving antibiotics for acute otitis media?
Clin Infect Dis. 2016 May 15; 62(10) e51-77.
The Right Drug
Is a fluoroquinolone appropriate for a patient based on their indication?
Does the patient require coverage for drug-resistant organisms (i.e. Methicillin-resistant Staphylococcus aureus or Pseudomonas aeruginosa
Does the patient have a true penicillin allergy where a beta-lactam would be inappropriate?
Clin Infect Dis. 2016 May 15; 62(10) e51-77.
The Right Dose
Is the antibiotic dose appropriate for the patient’s renal function?
Is the dose appropriate for the patient’s weight?
Is the antibiotic dose appropriate if the patient is on interacting medications?
Clin Infect Dis. 2016 May 15; 62(10) e51-77.

▶Guideline-recommended duration of therapies for
commonly treated outpatient infections▶ Community-acquired pneumonia: 5 days
▶ Skin and soft tissue Infections: 5-7 days
▶ Urinary Tract Infections:▶ Uncomplicated Cystitis: 1-7 days
▶ Pyelonephritis: 7-14 days
▶ Acute Otitis Media: 10 days
▶ Sinusitis: 5-7 days
The Right Duration
Clin Infect Dis. 2016 May 15; 62(10) e51-77.
Clin Infect Dis. 2007; 44: S27-72.
Clin Infect Dis. 2014; 59(2):e10-52.
Clin Infect Dis. 2011; 52(5):e103–e120
Clin Infect Dis. 2012; 54(8):e72–112
Pediatrics. 2013; 131(3): e964-999.
Clin Infect Dis. 2012; 55(10):e86–102

▶ De-escalation is the process of simplifying an antibiotic regimen to
ensure the spectrum activity only covers for organisms infecting the
patient, with minimal additional coverage
▶ This intervention can be comfortably performed when more data of
the patient’s infectious process is revealed (i.e organism
identification, organism susceptibility, symptomatic improvement,
etc)
The Right De-escalation
Clin Infect Dis. 2016 May 15; 62(10) e51-77.
▶ In 2015, 269.4 million antibiotics were prescribed in the U.S.
▶ Per 1,000 people▶ 838 prescriptions
▶ Women > men
▶ Above 20 years old > below 20 years old
▶ Most antibiotics per provider▶ Mid-level providers
▶ Dermatologists
▶ Primary care physicians
▶ Emergency medicine physicians
Why is Outpatient Antibiotic
Stewardship So Important?
Clin Infect Dis, 2015. 60(9): p.1308-16.

Why is Outpatient Antibiotic
Stewardship So Important?
Outpatient Antibiotic Prescriptions – United States, 2015. Atlanta (GA). Centers for Disease Control and Prevention; 2015. https://www.cdc.gov/antibiotic-
use/community/programs-measurement/state-local-activities/outpatient-antibiotic-prescriptions-US-2015.html. Accessed April 14, 2018.

Outpatient antibiotics prescribed based on drug class
Outpatient Antibiotic Prescriptions – United States, 2015. Atlanta (GA). Centers for Disease Control and Prevention; 2015. https://www.cdc.gov/antibiotic-
use/community/programs-measurement/state-local-activities/outpatient-antibiotic-prescriptions-US-2015.html. Accessed April 14, 2018.

Interactive Antibiotic Prescriptions
Dispensed Map in the United States
Antibiotic Prescriptions Dispensed in U.S. Community Pharmacies Per 1000 Population. Atlanta (GA). Centers for Disease Control and Prevention; 2015.
https://gis.cdc.gov/grasp/PSA/AUMapView.html
▶ A 2016 JAMA study sampled 184,032 U.S. ambulatory clinic visits in
2010-2011 to describe inappropriate outpatient antibiotic prescribing
▶ 12.6% were associated with antibiotic prescriptions
▶ Children 0-2 years old demonstrated highest prescription rates at
1,287 per 1,000 children
▶ Top 3 diagnoses included sinusitis, suppurative otitis media, and
pharyngitis
▶ Authors adjudicated appropriateness of antibiotic prescribing based
on national guidelines
Why is Outpatient Antibiotic Stewardship
So Important?
JAMA. 2016;315(17):1864-1873.

Why is Outpatient Antibiotic Stewardship
So Important?
JAMA. 2016;315(17):1864-1873.
Diagnosis/Group Weighted Mean
Annual of Antibiotic
Rx (95% CI)
Estimated Appropriate
Annual Rate of Abx Rx
Potential Reduction in
Annual Abx Rx Rates,
%
Pharyngitis (0-19 y) 91 (76, 105) 60 -34
Sinusitis (20-64 y) 55 (45, 64) 27 -51
All acute respiratory
conditions (all ages)
211 (198, 245) 111 -50
All conditions/age
groups
506 (458, 554) 353 -30

National Initiatives:
The Joint Commission Stewardship Standard &
The CDC Core Elements of Outpatient Antibiotic
Stewardship

The Joint Commission Standard on
Antimicrobial Stewardship (2017)
▶ Mandated in 2017 for all hospitals, critical access hospitals, and nursing care centers
▶ Requires all institutions to establish an antimicrobial stewardship program with the
following elements of performance in order to comply with accreditation standards:
1. Leaders establish antimicrobial stewardship as an organizational priority
2. Educate staff and practitioners involved in antimicrobial ordering, dispensing,
administration, monitoring
3. Educate patients and their families regarding the appropriate use of
antimicrobial medications
4. Team members consist of ID physician, infection preventionists,
pharmacist(s), other practitioners
5. The program includes CDC Core elements of hospital antibiotic stewardship
programs
6. The program uses organization-approved multidisciplinary protocols in order
to improve antibiotic prescribing and use
a. Ex: formulary restriction, system-wide empiric guidelines, parenteral
to oral antibiotic conversion, etc.
The Joint Commission. New Antimicrobial Stewardship Standard. Oakbrook, IL. Joint Commission Perspectives, 2016.

The CDC Core Elements of Outpatient
Antibiotic Stewardship
▶ Published in 2016 by the Centers for Disease Control and Prevention (CDC)
▶ Outlines the appropriate audiences for outpatient stewardship, initial
steps for implementation of stewardship activities, and potential
collaborative opportunities when starting an outpatient stewardship
program
▶ Defines the four core elements to ensure a successful outpatient
stewardship program: ▶ Commitment
▶ Action for Policy and Practice
▶ Tracking and Reporting
▶ Education and Expertise
MMWR Recomm Rep 2016;65(No. RR-6):1–12.

From Policies to Pragmatism:
Implementation Strategies for
Outpatient Stewardship

Is Outpatient Stewardship Right for My
Institution?
▶ The following groups are identified by the CDC as the
intended audience for Outpatient Stewardship ▶ Primary care clinics and clinicians
▶ Emergency departments and emergency medicine clinicians
▶ Dental clinics and dentists
▶ Retail health clinics and clinicians
▶ Outpatient specialty and subspecialty clinics and clinicians
▶ Urgent care clinics and clinicians
▶ Nurse practitioners and physician assistants
▶ Health care systems
MMWR Recomm Rep 2016;65(No. RR-6):1–12.

How to start the process of antimicrobial
stewardship at my area of practice
MMWR Recomm Rep 2016;65(No. RR-6):1–12.
1
2
3

The CDC Core Elements of
Outpatient Antibiotic
Stewardship
MMWR Recomm Rep. 2016;65(No. RR-6):1–12.
▶ Write and display public commitments in support of antibiotic
stewardship
▶ Identify a single leader to direct antibiotic stewardship activities
within a facility
▶ Include antibiotic stewardship-related duties in position descriptions
or job evaluation criteria
▶ Communicate with all clinic staff members to set patient
expectations
Commitment
MMWR Recomm Rep. 2016;65(No. RR-6):1–12.
“Demonstrate dedication to and accountability for optimizing
antibiotic prescribing and patient safety.”

▶ Implement at least one policy or practice to improve antibiotic
prescribing, assess whether it is working, and modify as needed
▶ Use delayed prescribing practices or watchful waiting, when
appropriate
▶ Require explicit written justification in the medical record for non-
recommended antibiotic prescribing
▶ Provide support for clinical decisions
▶ Use call centers, nurse hotlines, or pharmacist consultations as triage
systems to prevent unnecessary visits
Action for Policy and Practice
MMWR Recomm Rep. 2016;65(No. RR-6):1–12.
Implement at least one policy or practice to improve antibiotic
prescribing, assess whether it is working, and modify as needed.
▶ Self-evaluate antibiotic prescribing practice
▶ Participate in continuing medical education and quality improvement
activities to track and improve antibiotic prescribing
▶ Implement at least one antibiotic prescribing tracking and reporting
system
▶ Assess and share performance on quality measures and established
reduction goals addressing appropriate antibiotic prescribing from
health care plans and payers
Tracking and Reporting
MMWR Recomm Rep. 2016;65(No. RR-6):1–12.
Monitor antibiotic prescribing practices and offer regular feedback to
clinicians, or have clinicians assess their own antibiotic prescribing
practices themselves

▶ Use effective communications strategies to educate patients about
when antibiotics are and are not needed
▶ Educate patients about the potential harms of antibiotic treatment
▶ Provide patient education materials
▶ Provide continuing education activities for clinicians
▶ Ensure timely access to persons with expertise
Education and Expertise
MMWR Recomm Rep. 2016;65(No. RR-6):1–12.
Provide educational resources to clinicians and patients on antibiotic
prescribing, and ensure access to needed expertise on optimizing
antibiotic prescribing

Illinois Department of Public Health:
Precious Drugs and Scary Bugs Campaign
Precious Drugs & Scary Bugs. Illinois Department of Public Health. <http://www.dph.illinois.gov/topics-services/prevention-wellness/patient-safety-quality/precious-drugs-scary-bugs>

▶ Targets healthcare providers in outpatient settings to promote appropriate
use of antibiotics, increase healthcare provider and patient knowledge
regarding appropriate antibiotic use, and provide resources to support
clinicians in improving antibiotic prescribing
▶ Focus on acute respiratory infections
▶ Current participating providers (as of 2015) include:▶ A to Z Pediatrics
▶ Amita Health Medical Group
▶ Community Health Improvement Center
▶ Heartland Health Outreach
▶ OSF Medical Group
▶ Southern Illinois University School of Medicine
▶ Can get involved by completing a Facility Interest Form and a Provider
Commitment Form
Illinois Department of Public Health:
Precious Drugs and Scary Bugs Campaign
Precious Drugs & Scary Bugs. Illinois Department of Public Health. <http://www.dph.illinois.gov/topics-services/prevention-wellness/patient-safety-quality/precious-drugs-scary-bugs>\
▶ Targets healthcare providers in outpatient settings to promote
appropriate use of antibiotics
▶ Increase healthcare provider and patient knowledge regarding
appropriate antibiotic use
▶ Provide resources to support clinicians in improving antibiotic
prescribing
▶ Focus on acute respiratory infections
IDPH Precious Drugs and Scary Bugs
Campaign Initiatives
Precious Drugs & Scary Bugs. Illinois Department of Public Health. <http://www.dph.illinois.gov/topics-services/prevention-wellness/patient-safety-quality/precious-drugs-scary-bugs>\

▶ Current participating providers (as of 2015) include:▶ A to Z Pediatrics
▶ Amita Health Medical Group
▶ Community Health Improvement Center
▶ Heartland Health Outreach
▶ OSF Medical Group
▶ Southern Illinois University School of Medicine
▶ Can get involved by completing a Facility Interest Form and a
Provider Commitment Form
IDPH Precious Drugs and Scary Bugs
Campaign Participants
Precious Drugs & Scary Bugs. Illinois Department of Public Health. <http://www.dph.illinois.gov/topics-services/prevention-wellness/patient-safety-quality/precious-drugs-scary-bugs>\

Vaccine
Percent of children aged
19-35 months receiving
vaccinations in 2016
Diphtheria, Tetanus, Pertussis 84.6%
Polio 93.7%
Measles, Mumps, Rubella (MMR) 91.9%
Haemophilus influenzae tybe b 82.7%
Chickenpox (Varicella) 91.8%
Pneumococcal conjugate vaccine (PCV) 84.1%
Combined 7-vaccine series 72.2%
Improving Immunization Rates
Immunizations. CDC. Retrieved from: https://www.cdc.gov/nchs/fastats/immunize.htm

Apply your knowledge!

1. Which of the following best describes antimicrobial
stewardship?
a. Choosing the least expensive antibiotic for a patient
b. Choosing the most appropriate antibiotic for a patient
c. Choosing the most broad-spectrum antibiotic for a patient
d. Choosing the antibiotic which a patient most prefers
Post-Test Questions

1. Which of the following best describes antimicrobial
stewardship?
a. Choosing the least expensive antibiotic for a patient
b. Choosing the most appropriate antibiotic for a patient
c. Choosing the most broad-spectrum antibiotic for a patient
d. Choosing the antibiotic which a patient most prefers
Think as simple as possible, but not simpler! Must take into
account efficacy, safety, costs, and the most narrow agent
that will get the job done.
Post-Test Questions

2. Which of the following is a benefit of antimicrobial
stewardship?
a. Decrease in superinfections due to Clostridium difficile
b. Development of antimicrobial resistance
c. Increased antimicrobial costs
d. Increased use of intravenous antibiotics
Post-Test Questions

2. Which of the following is a benefit of antimicrobial
stewardship?
a. Decrease in superinfections due to Clostridium difficile
b. Development of antimicrobial resistance
c. Increased antimicrobial costs
d. Increased use of intravenous antibiotics
The primary risk factor for Clostridium difficile infection is
antibiotic use. If unnecessary antibiotic use is minimized,
normal GI flora will not be disturbed and allow the
C. difficile organism to overgrow in the intestines and
cause infection.
Post-Test Questions

3. Which of the following is NOT a CDC core element of
antibiotic stewardship?
a. Action for policy and practice
b. Tracking and reporting
c. Education and expertise
d. Prescriber disciplinary action
Post-Test Questions
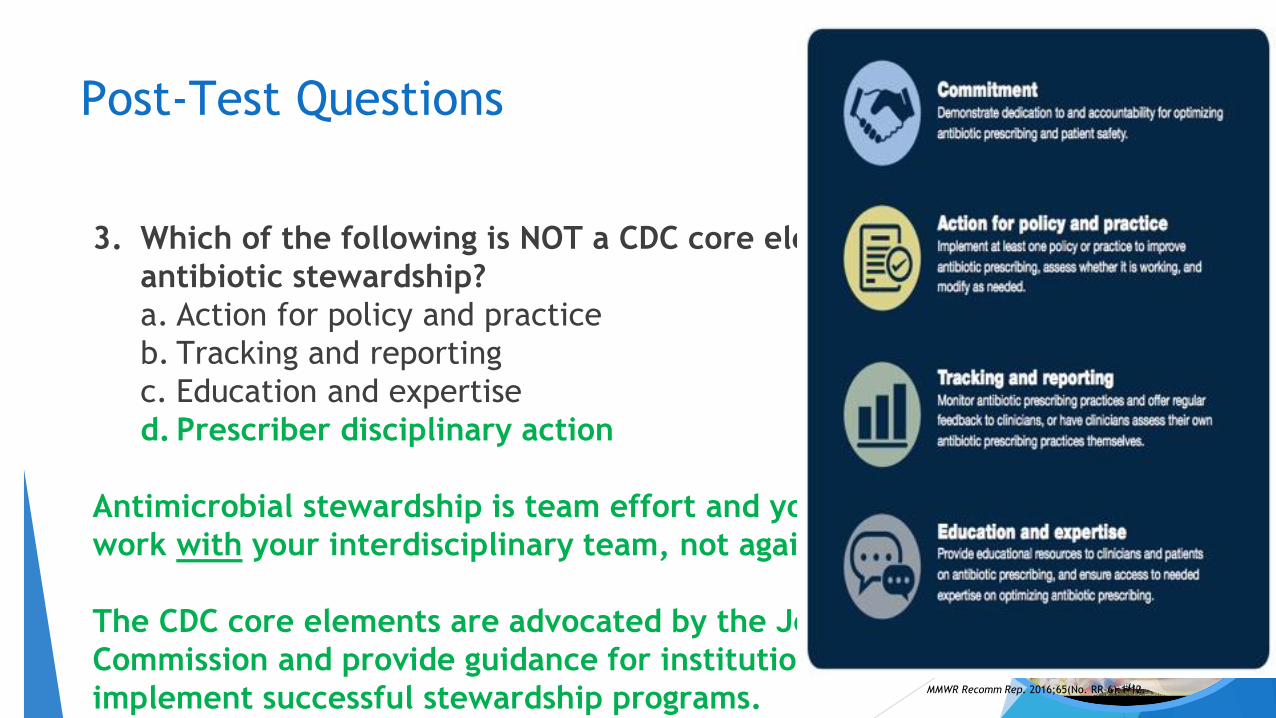
3. Which of the following is NOT a CDC core element of
antibiotic stewardship?
a. Action for policy and practice
b. Tracking and reporting
c. Education and expertise
d. Prescriber disciplinary action
Antimicrobial stewardship is team effort and you want to
work with your interdisciplinary team, not against them!
The CDC core elements are advocated by the Joint
Commission and provide guidance for institutions to
implement successful stewardship programs.
Post-Test Questions
MMWR Recomm Rep. 2016;65(No. RR-6):1–12.

4. Which of the following is an intervention that can improve
utilization of antibiotics in the outpatient setting?
a. Utilize watch and wait practices when appropriate
b. Reprimand patients when they ask for antibiotics
c. Always advocate for empiric antibiotic use
d. Provide education to prescribers only, not patients
Post-Test Questions
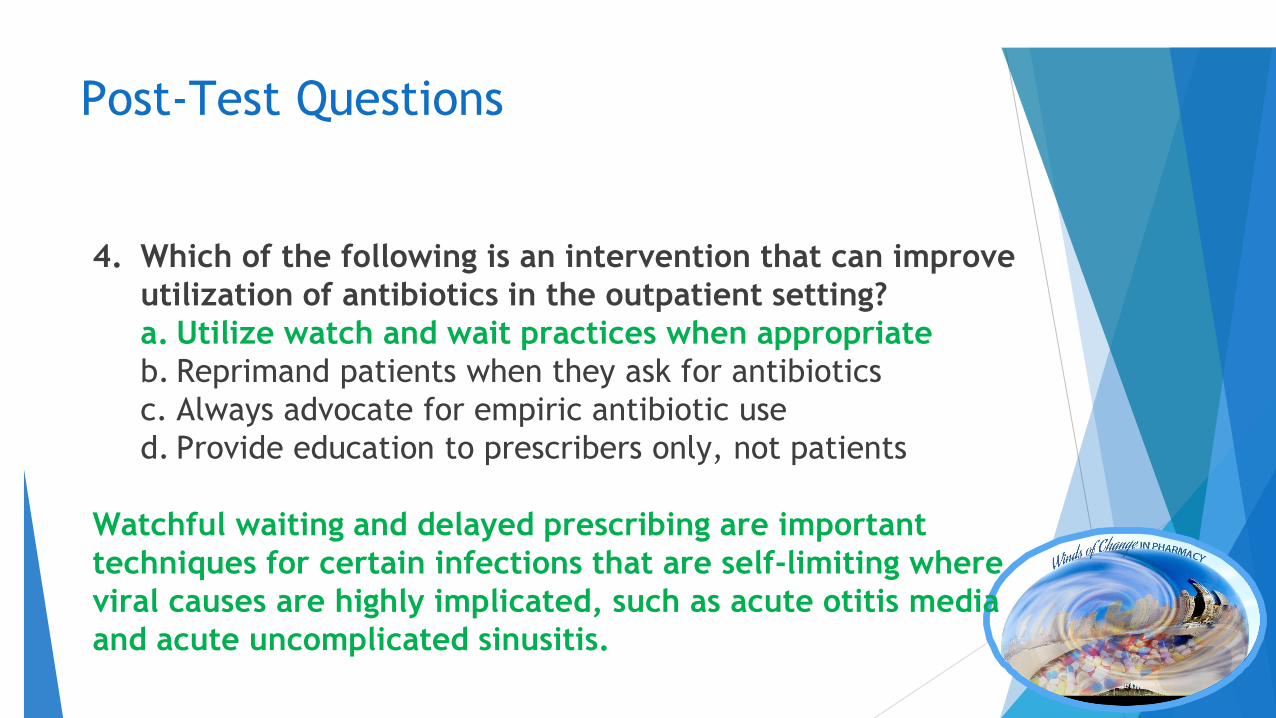
4. Which of the following is an intervention that can improve
utilization of antibiotics in the outpatient setting?
a. Utilize watch and wait practices when appropriate
b. Reprimand patients when they ask for antibiotics
c. Always advocate for empiric antibiotic use
d. Provide education to prescribers only, not patients
Watchful waiting and delayed prescribing are important
techniques for certain infections that are self-limiting where
viral causes are highly implicated, such as acute otitis media
and acute uncomplicated sinusitis.
Post-Test Questions

▶Select a disease state
▶ Example: urinary tract infections
▶ Identify barriers
▶ Example: physicians like to prescribe fluoroquinolones due to
comfortability and familiarity
▶Educate and establish standard
▶ FDA warning on prescribing/adverse drug effects
▶ C. difficile superinfection
▶ Resistance
Application
U.S. Food and Drug Administration. 26 July 2016. Retrieved from https://www.fda.gov/Drugs/DrugSafety/ucm500143.htm
▶ Side effects: tendon, joint and muscle pain, a “pins and needles” tingling or
pricking sensation, confusion, and hallucinations
▶ “Collateral damage”
Application
FDA Warning: “We have determined that fluoroquinolones should
be reserved for use in patients who have no other treatment
options for acute bacterial sinusitis (ABS), acute bacterial
exacerbation of chronic bronchitis (ABECB), and uncomplicated
urinary tract infections (UTI) because the risk of these serious side
effects generally outweighs the benefits in these patients. For
some serious bacterial infections the benefits of fluoroquinolones
outweigh the risks, and it is appropriate for them to remain
available as a therapeutic option.”
U.S. Food and Drug Administration. 26 July 2016. Retrieved from https://www.fda.gov/Drugs/DrugSafety/ucm500143.htm

C.difficile Superinfection
Antibiotic CDI Adjusted Hazard Ratio
(95% CI)
Fluoroquinolones 4.0 (2.7, 5.9)
Aminoglycosides 0.9 (0.3, 3.0)
Clindamycin 1.9 (0.8, 4.4)
3rd/4th Generation Cephalosporins 3.1 (1.9, 5.2)
Fluoroquinolones
Stevens V et al. Clin Infect Dis. 2011;53(1):42-48.
59

Collateral Damage: Resistance
0
0.5
1
1.5
2
2.5
3
0 4 8 12 14
Co
ncen
trati
on
(µ
/mL
)
Hours
Ciprofloxacin 750mg PO MIC Breakpoint
“The Sanford Guide to Antimicrobial Therapy.” 2018: p 95. Print.
Peak: 3.6 µ/mL
PB: 20-40%
T ½: 4 h
David HW, et al. Journal of Antimicrobial Chemotherapy. 2000 (46) (5): 669-683

1. Antimicrobial stewardship is EVERYONE’s responsibility, not just
those with special training, knowledge, or job titles focused on
infectious disease
2. The 5 D’s of antimicrobial stewardship include making the right
diagnosis, choosing the right drug initially at the right dose, for the
right duration, and performing appropriate de-escalation once you
have additional clinical data
3. Core elements of outpatient antibiotic stewardship include
commitment, action for policy and practice, tracking and reporting,
and education and expertise
TAKE HOME POINTS
1. https://www.cdc.gov/antibiotic-use/community/index.html
2. https://www.cdc.gov/antibiotic-use/community/pdfs/16_268900-
A_CoreElementsOutpatient_508.pdf
3. https://www.jcrinc.com/antimicrobial-stewardship-toolkit/
4. http://www.dph.illinois.gov/sites/default/files/publications/opps-
antibiotic-stewardship-toolkit-dentists-final-121217.pdf
Resources & References

Questions??
Fleming A. Penicillin's finder assays its future. New York Times. 1945 June 26;:21.
The Path of Least Resistance:
A Primer on Outpatient
Antimicrobial StewardshipJason Alegro, Pharm.D., BCPS, Infectious Diseases Clinical Specialist, Mount Sinai Hospital
Email: [email protected]
Tanya Abi-Mansour, Pharm.D., Infectious Diseases/Stewardship Clinical Specialist, IU Health
Email: [email protected]





























