Embed Size (px)
Citation preview

The Olmstead Decision and Community Integration: Medicaid’s Role
New York State Association of Community and Residential Agencies Annual Leadership Conference
December 5, 2014

Figure 2
• Olmstead was brought by two women with cognitive and mental health disabilities who remained institutionalized in Georgia, despite the fact that their treatment teams had determined that their needs could be met in the community
• The Olmstead plaintiffs argued that their circumstances violated of the Americans with Disabilities Act’s community integration mandate:
– State and local governments are prohibited from disability-based discrimination and must provide services “in the most integrated setting appropriate to the needs of people with disabilities”
– State and local governments must make “reasonable modifications” to policies, practices, and programs to avoid disability-based discrimination, unless doing so would constitute a “fundamental alteration” the nature of the service, program, or activity
The Olmstead Plaintiffs and Their Claim
Photo credit: Atlanta Legal Aid Society

Figure 3
• Unjustified institutional isolation of people with disabilities is a form of discrimination under the ADA
– in order to receive needed medical services, people with disabilities must, because of those disabilities, relinquish participation in community life that they could enjoy given reasonable accommodations, while people without disabilities can receive needed medical services without similar sacrifice
• Community-based services must be offered, if appropriate, if a person with a disability does not oppose moving from an institution to the community, and if the community placement can be reasonably accommodated, considering the state’s resources and the needs of other people with disabilities
• The reasonable modification standard would be met if a state demonstrates that it has a comprehensive, effectively working plan for placing qualified people with disabilities in less restrictive settings and a waiting list that moves at a reasonable pace
The Supreme Court’s Decision in Olmstead

Figure 4
Private Insurance, 8%
NOTE: Total LTSS expenditures include spending on residential care facilities, nursing homes, home health services, and home and community-based waiver services. Expenditures also include spending on ambulance providers and some post-acute care. This chart does not include Medicare spending on post-acute care ($73.3 billion in 2012). All home and community-based waiver services are attributed to Medicaid. SOURCE: KCMU estimates based on CMS National Health Expenditure Accounts data for 2012.
As the Primary Payer for Long-Term Services and Supports, Medicaid Plays a Key Role in Community Integration
Medicaid, 50%
Other Public and Private,
22%
Out-of-Pocket,
19%
Total National LTSS Spending in 2012 = $294 billion
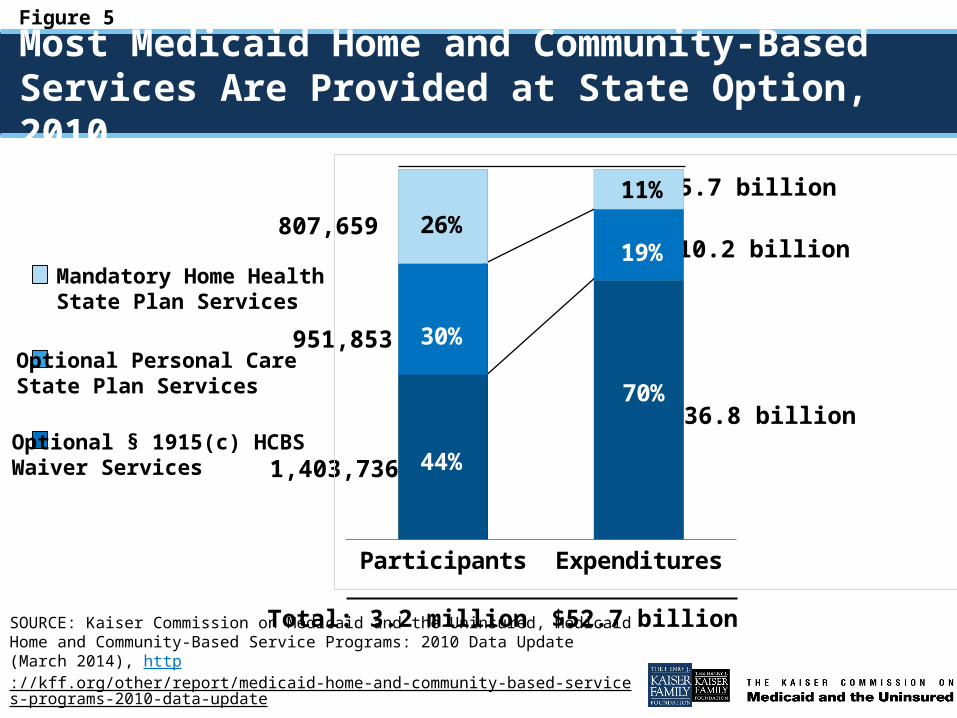
Figure 5
Most Medicaid Home and Community-Based Services Are Provided at State Option, 2010
3.2 million $52.7 billion
807,659
951,853
1,403,736
$5.7 billion
$10.2 billion
$36.8 billion
Mandatory Home Health State Plan Services
Optional Personal Care State Plan Services
Optional § 1915(c) HCBS Waiver Services
SOURCE: Kaiser Commission on Medicaid and the Uninsured, Medicaid Home and Community-Based Service Programs: 2010 Data Update (March 2014), http://kff.org/other/report/medicaid-home-and-community-based-services-programs-2010-data-update.
Total:
Participants Expenditures
26%11%
30%
19%
44%
70%

Figure 6
NOTE: “Aged/Disabled” comprises the following enrollment groups: aged, aged/disabled, and physically disabled. “Other” comprises the following enrollment groups: children, individuals with HIV/AIDS, individuals with mental health needs, and individuals with traumatic brain and spinal cord injuries. Percentages may not sum to 100 due to rounding. SOURCE: Kaiser Commission on Medicaid and the Uninsured, Medicaid Home and Community-Based Service Programs: 2010 Data Update (March 2014), http://kff.org/other/report/medicaid-home-and-community-based-services-programs-2010-data-update.
Medicaid § 1915(c) HCBS Waivers Can Be Capped, Resulting in Waiting Lists, 2002-2012
53% 47% 45%
64%
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Other
Aged/Disabled
Intellectual/Developmental Disability
28%
53% 47% 45%53% 53%
68% 64% 61%
62% 63%
58% 3% 1%
1%
6%5%
6%
6%
10%
8%
9%
10%
192,447 180,347 206,427 260,916 280,176 331,689 393,096 365,553 428,571Total: 511,174 523,710
43% 51%53%
41% 42%
26%30%
29%
29% 32%
28%

Figure 7
SOURCE: Kaiser Commission on Medicaid and the Uninsured, Faces of People on HCBS Waiver Waiting Lists (March 2014), http://kff.org/medicaid/report/medicaid-beneficiaries-who-need-home-and-community-based-services-supporting-independent-living-and-community-integration/.
Medicaid HCBS Waiver Services Play An Important Role in Supporting Beneficiaries’ Community Integration
CurtisAge 20
Topeka, KS
MargotAge 38
Charlotte, NC
CarolynAge 25
Miami, FL
Residence Lives with his mother Lives with a friend Lives with her mother
Time on Waiting List
Recently started receiving services after 12 year wait
Still waiting 18 months after inter-state move to be near family
Received services after waiting for 9 years
Health Mental retardation, autism, and sensory integration issues
Cerebral palsy with spastic quadriplegia
Chromosomal condition affecting growth, mobility, behavior, and intellectual functioning
Situation Attendant services help with basic living skills at home and in the community; will eventually need group home residential placement
Has master’s degree in social work but unable to work due to health; has had 6 inpatient hospitalizations since her move, which she believes were preventable with sufficient home health aide hours
Needs behavioral therapist and job coach to succeed at sheltered workshop and attendant services and wheelchair ramp to facilitate community access
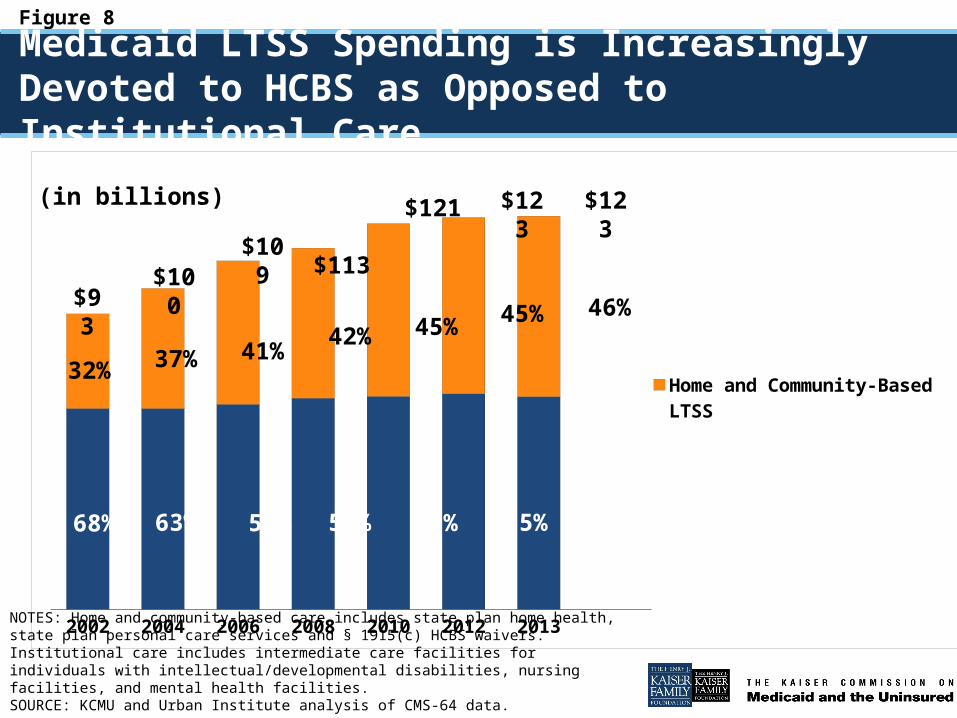
Figure 8
2002 2004 2006 2008 2010 2012 2013
Home and Community-Based LTSSInstitution-Based LTSS
$93$100
$113$121 $123 $123
68%
37%
63%
42%
58% 55%
45%
32%
55%
45%
54%
46%
Medicaid LTSS Spending is Increasingly Devoted to HCBS as Opposed to Institutional Care
NOTES: Home and community-based care includes state plan home health, state plan personal care services and § 1915(c) HCBS waivers. Institutional care includes intermediate care facilities for individuals with intellectual/developmental disabilities, nursing facilities, and mental health facilities.SOURCE: KCMU and Urban Institute analysis of CMS-64 data.
(in billions)
$109
41%
59%

Figure 9
Seniors Non-Elderly People with Disabilities
51%
21%
49%
79% Predominantly Community-Based CarePredominantly Institutional Care
1.9 million 1.6 million
NOTE: Individuals who used both institutional and community-based services in the same year are classified as using institutional services in this figure. SOURCE: KCMU and Urban Institute estimates based on MSIS and CMS-64 FY 2010 data.
Among Beneficiaries Who Use LTSS, a Larger Share of Non-Elderly People with Disabilities Live in the Community Than Seniors

Figure 10
• Recent case themes, highlighting Medicaid’s key role in Olmstead implementation, include:
– providing community-based services instead of institutionalization;
– providing services in the most integrated setting to enable people with disabilities to interact with non-disabled peers to the fullest extent possible;
– providing community-based services to prevent institutionalization for people at risk;
– replacing sheltered workshops with supported employment; and
– eliminating disability-based discrimination within the Medicaid program
Olmstead Implementation 15 Years After the Supreme Court’s Decision
SOURCE: Kaiser Commission on Medicaid and the Uninsured, Olmstead’s Role in Community Integration for People with Disabilities Under Medicaid: 15 Years After the Supreme Court’s Olmstead Decision (June 2014), available at http://kff.org/medicaid/issue-brief/olmsteads-role-in-community-integration-for-people-with-disabilities-under-medicaid-15-years-after-the-supreme-courts-olmstead-decision/.

Figure 11
NOTE: Total counts equal the number of states that are approved by CMS to participate in the option as of Nov. 2014. States with pending state plan amendments or demonstration proposals are not captured in this figure. Washington is approved for both capitated and managed fee-for-service financial alignment demonstrations. SOURCES: CMS, Medicaid.gov, and state websites.
Medicaid Offers A Number of Options for States to Increase Beneficiary Access to HCBS
45
2116 15
12
4

Figure 12
SOURCE: Kaiser Family Foundation, Faces of Dual Eligible Beneficiaries (July 2013).
Medicaid Plays a Key Role in Community Integration
WandaAge 78
Tulsa, OK
VirginiaAge 72
Oklahoma City, OK
DonAge 41
Owossa, MI
Residence Lives in subsidized senior housing Lives alone at home Lives in an apartment
Health Muscular and skeletal problems, degenerative joint disease in lower back, hip replacement, and poor circulation in legs
Uterine cancer, hypertension, acid reflux, hernia, poor circulation in legs
Developmental disabilities, impulse control disorder, neuroleptic malignant syndrome
Medicaid’sRole in LTSS
Helped her transition from nursing home to community after two year stay post-surgery; case manager coordinates in-home aide and transportation services
Provides regular home visits by nurse and personal care aide
Enables him to self-directs his LTSS by hiring his own in-home caregivers and move from group home to his own apartment

Figure 13
NOTES: *MI has 1 waiver for seniors and people with physical disabilities and another waiver for people with I/DD. **Analysis includes states with § 1115 or § 1915(b)/(c) capitated MLTSS waivers. Other states may have capitated MLTSS programs through § 1932 state plan or § 1915(a) waiver authority. SOURCE: KCMU analysis of approved waiver terms and conditions, available at www.medicaid.gov.
State Interest in Delivering LTSS Through Capitated Managed Care Waivers Is Increasing
WY
WI
WV
WA
VA
VT
UT
TX
TN
SD
SC
RI PA
OR
OK
OH
ND
NC
NY
NM
NJ
NH
NV NE
MT
MO
MS
MN
MI*MA
MD
ME
LA
KY KS
IA
IN IL
ID
GA
FL
DC
DE
CT
CO CA
ARAZ
AK
AL
HI
MLTSS waiver includes seniors, people with physical disabilities, and people with I/DD (5 states)MLTSS waiver includes seniors and people with physical disabilities (13 states)
No MLTSS waiver** (31 states plus DC)

Figure 14
• Expanding Medicaid financial eligibility criteria (NJ, NY, RI, VT)
• Providing HCBS to people at risk of institutionalization (AZ, DE, HI, NY, RI, TN, VT)
• Allowing spouses as paid caregivers (AZ, VT)
• Including financial incentives for health plans to provide increased HCBS (HI, IL*, OH, TN) or provisions that increase state funding of HCBS (KS, VT)
• Requiring health plans to have strategies for NF to community transitions or NF diversion (KS, NJ, NM)
Some Managed LTSS Waiver Provisions Are Aimed at Increasing Beneficiary Access to HCBS
NOTE: *IL’s provision is in concurrent § 1115A authority. SOURCE: KCMU analysis of approved MLSS §1115 and §1915(b)/(c) waiver terms and conditions, available at www.medicaid.gov.

Figure 15
• Some existing quality measures, such as the National Core Indicators, ask beneficiaries to rate aspects of their services, such as:
– The extent of community integration where they live, work, and spend leisure time
– Opportunities to exercise choice and self-determination
• Some of the financial alignment demonstrations for dual eligible beneficiaries require states to report on measures related to LTSS rebalancing, such as:
– The number or percent of beneficiaries living in institutional or community-based settings
– The number or percent of beneficiaries transitioning between institutional and community-based settings
– The number or percent of beneficiaries experiencing a decrease in authorized personal care hours.
• LTSS rebalancing measures remain a gap in evaluating HCBS quality, and additional work is needed and underway in this area.
Some LTSS Rebalancing Measures Exist, But Further Development is Needed
Figure 16
• The ACA’s new and expanded options to rebalance LTSS spending toward HCBS can be incorporated into states’ Olmstead plans
- Money Follows the Person and Community First Choice include enhanced federal funding
- The Balancing Incentive Program includes reforms such as the development and expansion of no wrong door/single entry point systems and core standardized assessments to achieve greater equity among different populations receiving Medicaid HCBS
• CMS’s new definition of “home and community-based setting” seeks to ensure the fullest integration for people with disabilities
• CMS’s 2013 guidance on Medicaid managed LTSS waivers specifies that these delivery systems reforms must be administered consistent with Olmstead and the ADA’s community integration mandate
Looking Ahead, Medicaid Will Continue to Offer States Options to Facilitate Community Integration

Figure 17
For more information on Medicaid and health reform, visit…
www.kff.org





























