Embed Size (px)
Citation preview

2/22/2013
1
WOUND CARE 101 A PLETHORA OF TIPS FOR EVERYDAY
Regina F. Holmes MSN, RN, FNP-BC, CWOCN
WOC SPECIALTY NURSING ADVOCATES FOR QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS IN PATIENT CARE
•WOC nursing is a specialty recognized by the American Nurses Association (WOCN®, 2010a).
•WOC nurses provide expert clinical care to patients with wounds, pressure ulcers, fistulas, drains, stomas & continence disorders (WOCN®-WOCNCB®, 2008).
–Improves healing outcomes
–Builds a formulary of products to streamline consistent care for patients with WOC issues (e.g., dressings, supplies, modalities, equipment)
–Develops protocols for cost-effective resource utilization
–Provides proactive risk management
•Designs/participates in initiatives to improve patient care such as:
–Pressure ulcer prevention programs.
–Catheter associated urinary tract infection (UTI ) prevention programs.
–Surgical site infection prevention programs.

2/22/2013
2
Elijah
http://www.bing.com/videos/search?q=ostomy&view=detail&mid=0842E987AB863D297E510842E987AB863D297E51&first=0&FORM=NVPFVR
Objectives for today:
1. Identify Common wounds
2. Identify Common Skin Rashes
3. Pharmacological Interventions
4. Treatment Modalities
Factors Impacting Wound Healing
Infection
Local or systemic
Mobility/pressure
Unable to do pressure relief measures
Devices (splints, cast, etc)
Co-morbid disease processes
DM, Cardiac, Respiratory, Autoimmune, Anemia,SCA
2/22/2013
3
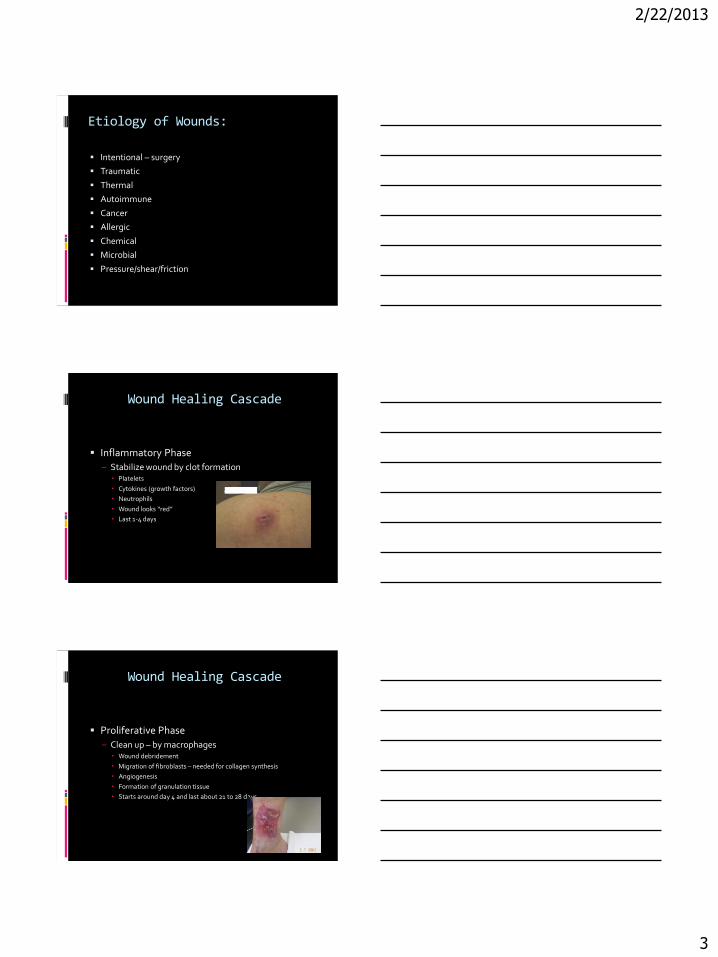
Etiology of Wounds:
Intentional – surgery
Traumatic
Thermal
Autoimmune
Cancer
Allergic
Chemical
Microbial
Pressure/shear/friction
Wound Healing Cascade
Inflammatory Phase
– Stabilize wound by clot formation Platelets
Cytokines (growth factors)
Neutrophils
Wound looks “red”
Last 1-4 days
Wound Healing Cascade
Proliferative Phase
– Clean up – by macrophages Wound debridement
Migration of fibroblasts – needed for collagen synthesis
Angiogenesis
Formation of granulation tissue
Starts around day 4 and last about 21 to 28 days

2/22/2013
4
Wound Healing Cascade
Maturation Phase
– Final closure Continued formation of granulation tissue
Progressive epithelialization from margins
Simultaneous synthesis and breakdown of collagen
Collagen becomes organized in bundles to increase tensile strength of new tissue
Last from day 21-28 until about 3 months
NOTE: Scar tissue will never be as strong as normal tissue, about 80% strength at 3 months.
Examples of Wound Types: Cancer Allergic
Chemical Microbial
Types of Wounds:

2/22/2013
5
Types of Wounds:
Acute or Chronic?
Acute are either traumatic or surgical
Chronic wounds
Classification of Wounds
Partial Thickness
- can go into dermal layer but not through
Full thickness
- can go through all layers, even into bone

2/22/2013
6
IAD:
Do not use a pressure ulcer classification system to describe wounds other than pressure ulcers. Educate the professional on differentiating pressure ulcers from other types of wounds (e.g.venous ulcers, arterial ulcers, neuropathic ulcers,traumatic
IAD:
venous ulcers, arterial ulcers, neuropathic ulcers,
incontinence-associated dermatitis, skin tears, and
intertrigo).”
Copyright EPUAP/NPUAP Nov 2009 from NPUAP.org
IAD risk factors:
Chronic exposure to moisture
Fecal and urinary incontinence
Use of a containment device
Alkaline pH (soaps, ammonia, moist skin)
Overgrowth or infection with pathogens
Friction
2/22/2013
7
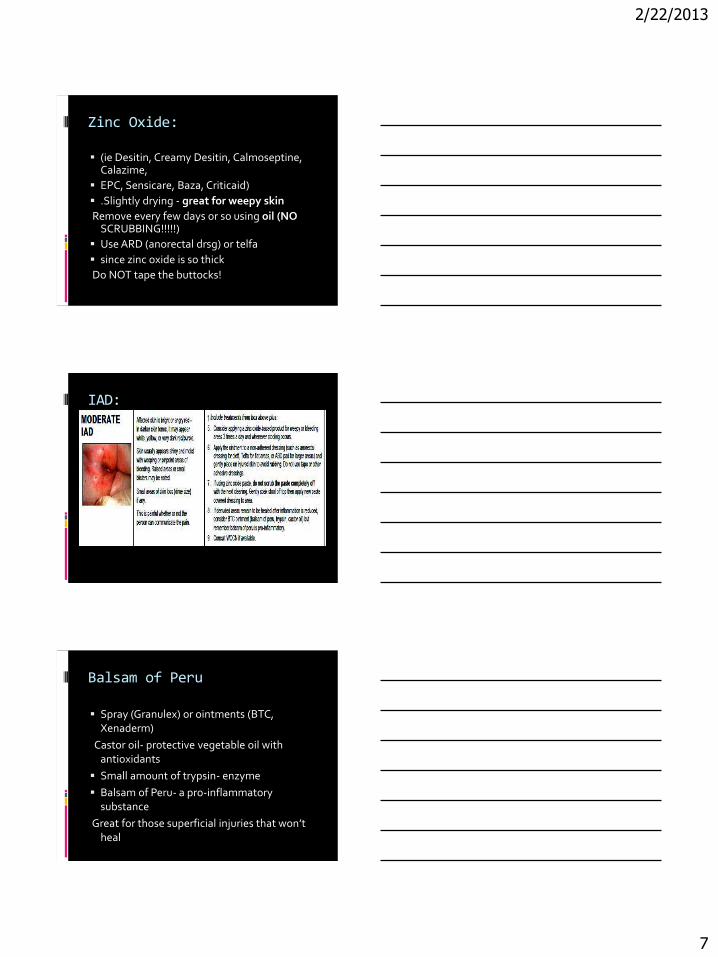
Zinc Oxide:
(ie Desitin, Creamy Desitin, Calmoseptine, Calazime,
EPC, Sensicare, Baza, Criticaid)
.Slightly drying - great for weepy skin
Remove every few days or so using oil (NO SCRUBBING!!!!!)
Use ARD (anorectal drsg) or telfa
since zinc oxide is so thick
Do NOT tape the buttocks!
IAD:
Balsam of Peru
Spray (Granulex) or ointments (BTC, Xenaderm)
Castor oil- protective vegetable oil with antioxidants
Small amount of trypsin- enzyme
Balsam of Peru- a pro-inflammatory substance
Great for those superficial injuries that won’t heal

2/22/2013
8
Balsam of Peru
because the person doesn’t have a very active
immune response
(inflammation- first phase of healing)
. Avoid on highly inflamed skin!
Treatment
Friction damage/Skin Tears
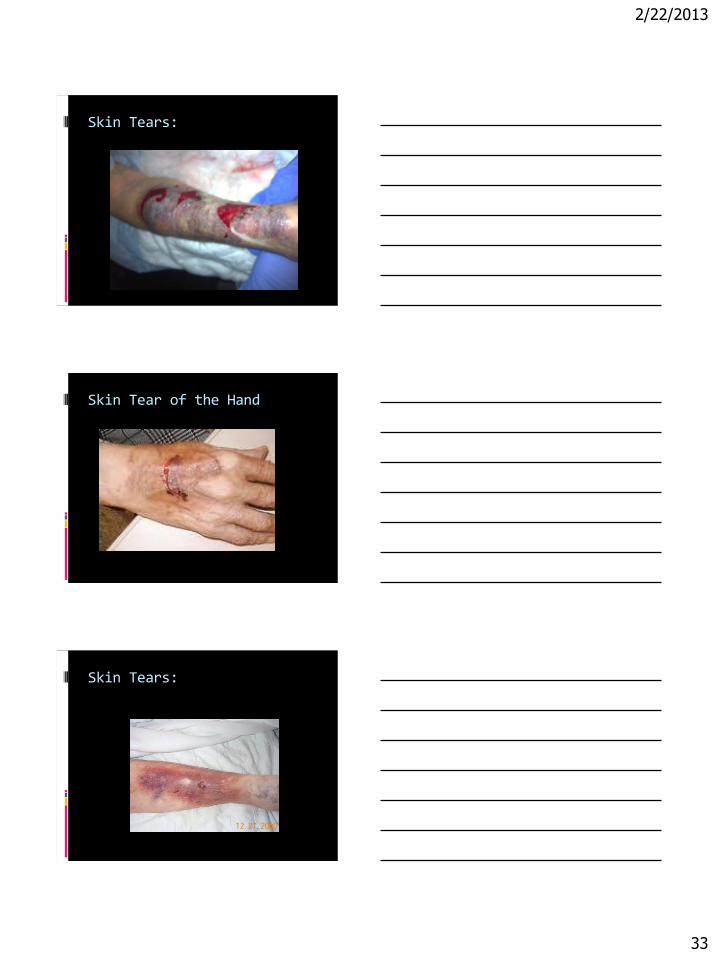
May be treated with soft silicone or low tack foam dressings. Hold in place with stocking-like products or cotton gauze wraps. They tended to achieve wound closure within 7 to 10 days. cleaning with normal saline, control of bleeding, and clots removal. Skin flaps should be approximated if possible. Dressing applied depends on wound characteristics.
Pressure Ulcers
2/22/2013
9
Background and Significance
Pressure ulcers are becoming common. According to Heath Cost and Utilization Project(HCUP) developing before or after hospitalization increased by 80% between 1993- 2006(Russo,Steiner, & Spector, 2008).
Pressure ulcer related cost:
Inpatient stays with diagnosis of Pressure Ulcers totaled 11 billion in 2006.
Average Length of stay is 5 days costing $ 10,000,
Average pressure ulcer related stay is 13-14 days costing $16,755-$20,438
More likey to be discharged to a long term care facility(3 times the rate of other dx)
Overall Principles of Effective Wound management
Identify and Correct exologic(environmental) factors
Systemic support for wound healing
Evidenced based topical Therapy

2/22/2013
10
Background and Significance
56.5 % are > 65 years
Paralysis and spinal cord injuries were most common in younger adults with the diagnosis of pressure ulcers (Russo et al., 2008).
Background and Significance
Pressure ulcers are areas of localized injury to the skin/or underlying tissue usually over a bony prominance, as a result of pressure , or pressure in combination
with shear.”(NPUAP/EPUAP,2009).
Pressure Ulcers
In 2007 the National Pressure Ulcer Advisory Panel(NPUAP) redefined and updated the definitions of pressure ulcer and the stages of pressure ulcers, including the original 4 stages and added 2 new stages; deep tissue injury and unstagable pressure ulcers (WOCN PU Guidelines ,2008).

2/22/2013
11
NPUAP Pressure Ulcer Staging
Suspected Deep Tissue Injury:
Purple or maroon localized area of discolored intact skin or blood filled blister due to damage to underlying soft tissue from pressure and/or sheer. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. NPUAP 2007
DTI:
Stage I:
Intact skin with nonblanchable redness of a localized usually over a bony prominance. Dark skin My not have visible blanching; its color may differ from surrounding skin.
NPUAP 2007

2/22/2013
12
Stage I
Stage II:
Partial thickness loss of dermis presenting as a shalloe open ulcer with red pink wound bed, without slough. May also present as an intact or opened/ruptured blister.
NPUAP 2007
Stage II

2/22/2013
13
Stage III:
Full thickness tissue loss. Subcutaneous fat may be visible but bone,tendon, or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining or tunneling.
NPUAP 2007
Stage III
Stage IV:
Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may be present on some parts of the wound bed. Often includes undermining or tunneling.
NPUAP 2007

2/22/2013
14
Stage IV
Unstagable:
Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed.
Copyright: NPUAP 2007
Unstagable

2/22/2013
15
LEVD:
An estimated 7 million adults in the US have a venous disorder such as venous insufficiency. These under-recognized vascular problems result in severe skin damage and ulcerations of the lower legs, produce pain, and restrict mobility.
LEVD:
Available data indicate that $3 billion is spent annually on leg ulcer care. Approximately 7 out of every 10 individuals with a previous venous leg ulcer (VLU) will experience a new one each year
LEVD:
Assessment
• Four key areas to assess are the
limb, skin, circulation, and wound.

2/22/2013
16
LEVD Risk Factors:
• 20 – 50% risk of developing a
venous leg ulcer (VLU) if varicosities left
unattended/untreated.
• Restricted ankle movement and
reduced calf muscle pump power.
• Injection drug use.
Triggers:
• External events or exacerbating factors
associated with ~75% of VLUs
– Cellulitis
– Penetrating injury/trauma
– Contact dermatitis
– Rapidly aggravating leg edema
– Burns, Dry skin with itching
– Insect bites
Factors impeding healing
Factors impeding healing
• Pain
• Co-morbid conditions
– Cardiac, rheumatoid arthritis, lymphedema, obesity,
lower extremity arterial disease
• Ulcer deeper than 2 cm

2/22/2013
17
Factors Impeding Healing:
History of debridement
• Presence of multiple VLUs
• Below normal hemoglobin counts
• Short walking distance < 200 m
• Smoking
• Higher disease severity including lipodermatosclerosis
Factors Impeding Healing
• Medications: corticosteroids and
immunosuppressive agents
• Older age
• Ulcer chronicity > 4 weeks
• Venous refill time < 20 seconds
Venous Dermatitis
• Eczema
– Elevated homocysteine (Hcy) levels
(hyperhomocysteinemia
• LOE = C
– Associated with increase severity of
disorder and VLUs

2/22/2013
18
Factors contributing to ulcer: Factors contributing to ulcer
recurrence
Body mass index (BMI) ≤ 20 kg/m2
Malnutrition
Depression
Decreased physical activity
Lack of leg elevation
Not wearing compression, Cardiac disease
Diagnostics:
– Duplex scanning with ultrasound, with or without color,
is the most reliable, noninvasive test to diagnose
Diagnostics:
anatomical and hemodynamic abnormalities and to detect reflux in any venous segment
• Photoplethysmography (PPG), air plethysmography (APG)
– Assess perfusion status to rule out combined disease
• Ankle brachial index
2/22/2013
19
ABI
http://www.youtube.com/watch?feature=player_detailpage&v=5Wclloi-qjU
Diagnostics:
• Skin temperature (increased temperature associated with
VLUs, infection, non-healing) (LOE = C)
Prevention of VLUs and progression of CVD: • Aggressive treatment of:
– Varicosities
• Weight management, physical activity,
foam sclerotherapy
– Cellulitis and acute dermatitis
– Pain

2/22/2013
20
Prevention of VLUs and progression of CVD: • Compression:
– Recurrence rates are lower in persons wearing high compression
(e.g., 40–50 mm Hg) hosiery compared
to medium (e.g., 30–40 mm Hg) compression hosiery;
Offer strongest compression tolerable
Prevention of VLUs and progression of CVDs – Adherence rates are significantly higher
with
moderate compression than with high-compression
Adjunctive Therapies
• Subfascial endoscopic perforator
(SEPS) surgery:
– there is some positive evidence about
the effects of surgical interventions
such as SEPS on preventing VLU
recurrence.

2/22/2013
21
Medicatins:
• Horse chestnut seed oil (Aesculus
hippocastanum L).
oral or topical phlebotonics.
• Micronized purified flavonoid
fraction (MPFF).
Patient Education:
Use compression therapy for the
remainder of their life.
• Use highest compression possible or
tolerated.
• Avoid mechanical trauma to the lower
leg.
• Discuss medication options with PCP
Devitalized tissue:
Devitalized tissue
• No one method of debridement has
been shown to be optimal for LEVD
ulcers.
• There is evidence to support the use
of larval (maggot) therapy to remove
necrotic tissue compared to different
types of debridement techniques.
2/22/2013
22
Topical dressings • There is insufficient evidence to
determine whether honey dressings
are beneficial in decreasing wound
healing rates compared to usual
care (e.g., compression and nonadherent
dressings).
Infection • The offending organism, through culture,
needs
to be determined for appropriate treatment. It is
important to consider the growing concern
regarding antibiotic resistance
Infection:
• Quantitative swab cultures have been
demonstrated to be a reasonable alternative to tissue biopsy in clinical practice for chronic wounds of which venous ulcers are included, to rule out infection

2/22/2013
23
Infection:
Antibacterial preparations should only be used in cases of clinical infection and not for bacterial colonization.
No conclusive studies to guide definitive topical antibiotic choice, dose and duration.
Use of newer, relatively nontoxic antimicrobials (e.g.,cadexomer iodine or silver dressings) over topical antibiotics
Nutrition:
Oral zinc sulfate does not appear to aid in the healing of leg ulcers in individuals with normal zinc levels. There is also limited evidence of benefit in people with LEVD who have low serum zinc. Thus, further research is needed to determine the benefits of zinc in patients
Compression:
• Multi-layer systems are more effective than single-layer systems
Examples of compression: Profore,Unna’s Boot
Juxta Lite
Trental (pentoxifylline).
– Dosages of 400 mg orally three times per day can accelerate healing of venous ulcers

2/22/2013
24
Example of 4 layer Compression:
Juxta- Lite
<iframe width="640" height="360" src="http:" frameborder="0" allowfullscreen></iframe>
IPC:
(IPC) may be used for patients who are immobile or who need higher levels of compression than that which can be provided with
stockings or wraps, such as those with extremely large
legs or who are intolerant of stockings or wraps.
2/22/2013
25
Medications:
Trental (pentoxifylline).
– Dosages of 400 mg orally three times per day can accelerate healing of venous ulcers
Granulocyte-macrophage colony stimulating factor (GMCSF).
A cytokine with pleiotropic functions) peri-ulcer injection
Medications:
• Horse chestnut seed extract (Escin/Aescin). Dosages of 300 mg containing 50 mg of the active ingredient
escin, twice daily – short term use
• Sulodexide (a glycosaminoglycan composed of low
Medications:
• Sulodexide (a glycosaminoglycan composed of low
molecular weight heparin (80%) and dermatan sulfate
(20%).
– Available orally and intramuscularly

2/22/2013
26
Surgical Options:
• Superficial venous surgery consists of
perforator ligation, minimally invasive surgery
(endoscopic) and invasive (open) surgery.
Superficial venous surgery combined with
compression compared to compression alone is as equally effective at increasing healing rates at 24 weeks.
Adjunctive Therapies:
• Biologic skin substitutes (BSSs).
• Whirlpool : insufficient evidence to support the use of whirlpool
• Laser therapy—low level (LLLT).
US
– There is limited evidence to support the use of LLLT.
• Electromagnetic therapy.
Adjunctive Therapies:
Negative pressure wound therapy (NPWT)
• Hyperbaric oxygen therapy (HBOT).

2/22/2013
27
Patient Education and Follow up:
Educate patients about wearing compression for a lifetime, smoking cessation, physical activity/exercising,
avoiding trauma/leg crossing, and following healthy diet
weight management and nutrition.
assess adherence ,condition of stockings, bandages, and wraps.
Lower Extremity Arterial Disease Lower extremity arterial disease (LEAD)
commonly referred to as PVD,PAD ,POAD, refers to disorders affecting the leg arteries.
CVD is the number one killer in the U.S., with 8-10 million people afflicted with LEAD. A disease often silent until a limb or life-threatening event occurs.
Lower Extremity Arterial Disease Based on ABI <0.9 LEAD is present in 29% of
patients 70 years or older and in 29% of patient 50-69 years who use tobacco or have Diabetes.
Uder diagnosed, under treated due to asymptomatic and atypical symptoms( absence of claudification).
Increased risk of CV and Cerebrovascular morbidity and mortality

2/22/2013
28
Lower Extremity Arterial Disease Lower Extremity Arterial Disease (LEAD)is
chronic and 90% of patients will have a progression of the disease in 5 years (Notcolff et al., 2002). The most common cause is atherosclerosis which is characterized by plaque formation ,thought to be triggered by vascular injury and inflammation.
Lower Extremity Arterial Disease Stenosis results from plaque formation and
over time results in ischemia. LEAD is associated with degenerative disorders such as collagen abnormalities, vasculitic disorders, systemic disorders such as Lupus, and Rheumatoid arthritis. Lower extremety circulatory problems can occur when other conditions are present: protein C deficientcy and Raynaud’s disease.
Risk Factors:
Advanced age
Smoking
Diabetes
Dyslipidemia
Hpypertension
Hyperhomocysteinemia
CRI, Family HX of CVD, Ethnicity

2/22/2013
29
Risk Factors
Periodontal Disease
Biomarkers associated with LEAD: CRP, Fibrinogen,D-Dimer,
Assessment:
Functional ability
Pain history:
Intermittent Claudication
Exacerbating Factors: elevation and exercise
Alleviating factors: rest,dependency
ALI (6 Ps)verses CLI
ABI
>1.3 Elevated (non-compressable
>1.0 Normal
<0.9 LEAD
<0.6-0.8 Borderline
<0.5 Severe Ischemia <0.4 Critical limb Ischemia
Toe Pressures <30 (<50 DM) = CLI
2/22/2013
30
ABI
>1.3 Refer further vascular testing
>1 Blood Flow sufficient to heal
<0.9 LEAD: Conservative therapy
<0.6-0.8 Borderline perfusion : vascular referral if no response in 2-4 weeks
<0.5 Severe Ischemia : Vascular
ABI:
Maintain stable dry black eschar
<0.4 CLI : Urgent Vascular evaluation
Medications:
Statins
Cilostazol 100mg BID
ACE inhibitors
Ramipril
ASA
Thienopyridines
Clopidogrel 75 mg maybe > effective than ASA

2/22/2013
31
Surgical Options:
Bypass/Angioplasty
Skin Grafting
Amputation
Where do diabetic ulcers occur? Diabetic ulcers tend to occur in the following
areas:
– Areas most subjected to weight bearing, such as the heel, plantar metatarsal head areas, the tips of the most prominent toes (usually the first or second), and the tips of hammer toes (Ulcers also occur over the malleoli because these areas commonly are subjected to trauma.)
– Areas most subjected to stress, such as the dorsal portion of hammer toes
Diabetic or Pressure?
The etiologies of diabetic ulceration include neuropathy,7 arterial disease,8 pressure,9 and foot deformity.10

2/22/2013
32
Not just traditional pressure With damage to the nervous system, a
person with diabetes may not be able to feel his or her feet properly. Normal sweat secretion and oil production that lubricates the skin of the foot is impaired. These factors together can lead to abnormal pressure on the skin, bones, and joints of the foot during walking and can lead to breakdown of the skin of the foot.
Diabetic or pressure?
SKIN TEARS
2/22/2013
33
Skin Tears:
Skin Tear of the Hand
Skin Tears:

2/22/2013
34
Skin Tear:
Skin Tears:
Skin Tears:

2/22/2013
35
Classification of Skin Tears:
What to do?
Step 1: Predicting Risk
It is critical to predict and identify those at
high risk for skin tears so that an appropriate
prevention program can be implemented before
injury occurs (Bank & Nix, 2006; Carville et
al., 2007; LeBlanc et al., 2008). Older adults are
at high risk for the development of skin tears
Prevention Strategies:
Step 2: Prevention Strategies
Most skin tears occur accidentally during routine
patient care activities. Education and involvement
of family and caregivers in the prevention
of skin tear development is imperative.

2/22/2013
36
Treatment:
Step 3: Treatment
Although prevention of skin tears should remain
the primary focus, evidence-based wound
care principles should be used when a skin tear
develops. The same principles used for other
wounds should be employed when treating
skin tears.
Treatment :
Skin tears should be treated in a systematic
way to include cleansing with normal saline,
controlling bleeding, removing a clot, and selecting
an appropriate dressing to address
the wound characteristics.
Initial Treatment: Replace the skin flap, if possible, by gently
rolling the skin flap over the wound. Best
practice supports that a skin flap be approximated
if possible, and a hydrogel,
alginate, foam, soft silicone, or nonadherent
dressings be applied over the
replaced flap, depending on the wound
characteristics (LeBlanc & Christensen,
2005; LeBlanc et al., 2005
2/22/2013
37
Dressing Selection :
Based on Characteristics:
Transparent
Nonadherent
Foam
Silicone
Hydrogel or sheets
alginate
How to Care for Wound with A Skin Flap? A skin flap
may not cover the entire wound, but
should be positioned to increase the
chance for it to “take” onto the wound
bed. The skin flap can be approximated
by using a moistened cotton tip applicator
and gently “rolling” the skin flap into
place. If the skin flap is not viable, debride
MRSA UPDATE IDSA 2012
For a cutaneous abscess, incision and drainage is the primary treatment (A-II). For simple abscesses or boils, incision and drainage alone is likely to be adequate, but additional data are needed to further define the role of antibiotics, if any, in this setting.

2/22/2013
38
Finger Abscess
http://www.youtube.com/watch?v=aHA44fYCzCk&feature=player_detailpage
Antibiogram
MRSA UPDATE
Antibiotic therapy is recommended for severe or extensive disease (involving ultiple sites of infection) associated cellulitis, signs and symptoms of systemic illness, associated comorbidities or immunosuppression, extremes of age, abscess in an area difficult to drain (eg, face, hand, and genitalia), associated septic phlebitis, and lack of response to incision and drainage alone (A-III).
For outpatients with purulent cellulitis (eg, cellulitis associated with purulent drainage or exudate in the absence of a drainable abscess), empirical therapy for CA-MRSA is recommended pending culture results. Empirical therapy for infection due to β-hemolytic streptococci is likely to be unnecessary (A-II). Five to 10 days of therapy is recommended but should be individualized on the basis of the patient's clinical response

2/22/2013
39
MRSA CONT.
For empirical coverage of CA-MRSA in outpatients with SSTI, oral antibiotic options include the following: clindamycin (A-II), trimethoprim-sulfamethoxazole (TMP-SMX) (A-II), a tetracycline (doxycycline or minocycline) (A-II), and linezolid (A-II). If coverage for both β-hemolytic streptococci and CA-MRSA is desired, options include the following: clindamycin alone (A-II) or TMP-SMX or a tetracycline in combination with a β-lactam (eg, amoxicillin) (A-II) or linezolid alone (A-II).
MRSA CONT.
For outpatients with nonpurulent cellulitis (eg, cellulitis with no purulent drainage or exudate and no associated abscess), empirical therapy for infection due to β-hemolytic streptococci is recommended (A-II). The role of CA-MRSA is unknown. Empirical coverage for CA-MRSA is recommended in patients who do not respond to β-lactam therapy and may be considered in those with systemic toxicity. Five to 10 days of therapy is recommended but should be individualized on the basis of the patient's clinical response
The use of rifampin as a single agent or as adjunctive therapy for the treatment of SSTI is not recommended (A-III).
MRSA CONT
For hospitalized patients with complicated SSTI (cSSTI; defined as patients with deeper soft-tissue infections, surgical/traumatic wound infection, major abscesses, cellulitis, and infected ulcers and burns), in addition to surgical debridement and broad-spectrum antibiotics, empirical therapy for MRSA should be considered pending culture data. Options include the following: intravenous (IV) vancomycin (A-I), oral (PO) or IV linezolid 600 mg twice daily (A-I), daptomycin 4 mg/kg/dose IV once daily (A-I), telavancin 10 mg/kg/dose IV once daily (A-I), and clindamycin 600 mg IV or PO 3 times a day (A-III). A β-lactam antibiotic (eg, cefazolin) may be considered in hospitalized patients with nonpurulent cellulitis with modification to MRSA-active therapy if there is no clinical response (A-II). Seven to 14 days of therapy is recommended but should be individualized on the basis of the patient's clinical response.
2/22/2013
40
MRSA
Cultures from abscesses and other purulent SSTIs are recommended in patients treated with antibiotic therapy, patients with severe local infection or signs of systemic illness, patients who have not responded adequately to initial treatment, and if there is concern for a cluster or outbreak (A-III).
For children with minor skin infections (such as impetigo) and secondarily infected skin lesions (such as eczema, ulcers, or lacerations), mupirocin 2% topical ointment can be used (A-III). 10. Tetracyclines should not be used in children <8 years of age (A-II).
MRSA
In hospitalized children with cSSTI, vancomycin is recommended (A-II). If the patient is stable without ongoing bacteremia or intravascular infection, empirical therapy with clindamycin 10–13 mg/kg/dose IV every 6–8 h (to administer 40 mg/kg/day) is an option if the clindamycin resistance rate is low (eg, <10%) with transition to oral therapy if the strain is susceptible (A-II). Linezolid 600 mg PO/IV twice daily for children ≥12 years of age and 10 mg/kg/dose PO/IV every 8 h for children <12 years of age is an alternative (A-II).
Recurrent SSTIs Preventive educational messages on personal
hygiene and appropriate wound care are recommended for all patients with SSTI. Instructions should be provided to:
i. Keep draining wounds covered with clean, dry bandages (A-III).
ii. Maintain good personal hygiene with regular bathing and cleaning of hands with soap and water or an alcohol-based hand gel, particularly after touching infected skin or an item that has directly contacted a draining wound (A-III).

2/22/2013
41
Recurrent SSTIs CONT.
Avoid reusing or sharing personal items (eg, disposable razors, linens, and towels) that have contacted infected skin (A-III).
13. Environmental hygiene measures should be considered in patients with recurrent SSTI in the household or community setting:
i. Focus cleaning efforts on high-touch surfaces (ie, surfaces that come into frequent contact with people's bare skin each day, such as counters, door knobs, bath tubs, and toilet seats) that may contact bare skin or uncovered infections (C-III).
What is the management of MRSA pneumonia? Pneumonia For hospitalized patients with severe community-acquired
pneumonia defined by any one of the following: (1) a requirement for intensive care unit (ICU) admission, (2) necrotizing or cavitary infiltrates, or (3) empyema, empirical therapy for MRSA is recommended pending sputum and/or blood culture results (A-III).
For health care–associated MRSA (HA-MRSA) or CA-MRSA pneumonia, IV vancomycin (A-II) or linezolid 600 mg PO/IV twice daily (A-II) or clindamycin 600 mg PO/IV 3 times daily (B-III), if the strain is susceptible, is recommended for 7–21 days, depending on the extent of infection.
In patients with MRSA pneumonia complicated by empyema, antimicrobial therapy against MRSA should be used in conjunction with drainage procedures (A-III).
CALCIPHYLAXIS

2/22/2013
42
Dermatologic Delimas
Steven Johnson’s Syndrome
SJS
SJS

2/22/2013
43
SJS:
What id this?
Shingles

2/22/2013
44
Herpes:
Opthalmic :
Psoriasis:

2/22/2013
45
Finger Abscess
http://www.youtube.com/watch?v=aHA44fYCzCk&feature=player_detailpage
Overall Principles of Effective Wound management Identify and Correct exologic factors
Systemic support for wound healing
Evidenced based topical Therapy
Treat the Whole patient, not the hole in the patient!!!

2/22/2013
46
Wound Management
3 requirements for wound healing
– Etiology-what “caused” the wound. Try to correct or manage the cause.
– Systemic- is the pt ‘able” to heal? Education to pt to improve healing ability.
– Topical- what dressing or topical treatment is applied to the wound . Based on DIPAMOPI.
Etiology
Determine the cause
Correct or manage the cause
– Pressure-support surfaces, turning, etc
– Venous stasis-compression
– Arterial-vascular consult
– Surgical-NA
– Diabetic-glucose control, offloading
– Atypical-varies, referral to dermatology (?)
– Skin tears-improve skin integrity, pad items
Systemic Support
Nutrition-protein 1.2-1.5g/kg/d & calories 30cc/kg/d
Perfusion-decrease reducible factors
BMI-appropriate wt/ht
Activity-
Glucose management
Hydration-30cc/kg/d typical
Immune system
Manage co-morbidities

2/22/2013
47
Debridement options
Surgical converts chronic wound to acute
wound
best option for full thickness wounds with abscess, sepsis, etc.
Debridement options
Conservative sharp Using scalpel, scissors and/or
pickups/forceps
Best option for patient with loose avascular tissue who is a not good candidate for surgical debridement
NC nurse practice act governs who can do this
Contraindications: clotting disorder, systemic infection
Debridement options
Chemical (Dakin’s solution) Use of non-enzymatic solutions
to promote breakdown of necrotic tissue
Indicated for wound with necrosis and odor
Some confusion of what “1/4 strength” really means
Note: Dakin’s solution loses potency in 24-48 hrs

2/22/2013
48
Debridement options
Surgical converts chronic wound to acute
wound
best option for full thickness wounds with abscess, sepsis, etc.
Debridement options
Conservative sharp Using scalpel, scissors and/or
pickups/forceps
Best option for patient with loose avascular tissue who is a not good candidate for surgical debridement
NC nurse practice act governs who can do this
Contraindications: clotting disorder, systemic infection
Debridement options
Hydrotherapy
Whirlpool
Best for burns
Con: possible spread of infection
Pulsatile lavage
8-15 psi to soften and remove necrotic tissue, debris, bacteria
Effective on slough, but not on eschar
2/22/2013
49
Debridement options
Autolytic
Utilizes WBC and enzymes in wound fluid to digest necrotic tissue
Safe, non-invasive Will usually see significant progress within 72 hours
Debridement options
Mechanical debridement:
NON-SELECTIVE and PAINFUL
Use of saline moistened gauze that is allowed to dry on the wound bed, typically 4-8 hours after application
As gauze dries, necrotic tissue (and unfortunately viable tissue) adheres to the gauze
When gauze dressing is removed, the necrotic tissue (and unfortunately the adherent viable tissue) is removed as well
Identify Infection
Tissue biopsy
Most accurate
Most difficult and invasive
Fluid aspiration
Most effective in sterile cavity infections
Swab culture
Only as effective as the operator
Don’t culture “pus” – only clean tissue
Must express fluid from “clean tissue” in wound bed

2/22/2013
50
Identify and treat infection
All open wounds are contaminated - but…not all wounds are infected
“Bacterial load or bioburden” – may
be too high to allow healing but not “really” infected
Can treat topically
Infection (colony counts > 100,000)
needs to be promptly detected and properly eliminated
Maintain moist wound surface
Moist wound surface promotes cell migration
Moist wound surface prevents cell death (that occurs when wound dries out)
Protect From Trauma
Healing or newly healed tissue is fragile
50% of normal skin strength at 2 weeks
80% of normal within 3 months
NEVER as strong as original
Infection – delays healing
sudden failure to progress can indicate new infection
Repeated injury - delays healing
Scar tissue does not have normal cell regeneration properties

2/22/2013
51
Insulate
Maintain normal temperature
Negative effects of sub-normal temperature
vasoconstriction
cellular activity declines
Wound Care Product Selection
Pick the product that meets the most acute need at each level of healing
If no progress is seen within 2 weeks, re-assess and modify approach
Every wound care product is GREAT for SOME WOUNDS, BUT--- no one product is GREAT for EVERY WOUND
Advanced Therapies: Ultrasonic Debridement
Ultrasonic-assisted wound debridement
Low frequency US – cleaves through necrotic tissue and biofilm
“painless”
Types of wounds
Any chronic wound
Pressure ulcers
Diabetic ulcers
Venous ulcers
Burns
Surgical wounds
*Sonoca by Söring

2/22/2013
52
Advanced Treatments: Vacuum Assisted Closure Systems
Wound VAC Must have “relatively” clean wound
bed
Must have some depth
Must be free of infection or at least under treatment
Can be used at home, in hospital or in extended care facilities
Advanced Therapies: Hyperbaric Oxygen
Medical application Other conditions treated:
Autism
Cerebral palsy
Multiple sclerosis
Attention deficit disorder
Fibromyalgia
Chronic fatigue
Crohn’s disease/colitis
MI
Mitochondrial disorders
Ammonia toxicity
Carbon monoxide inhalation
Advanced Treatments: Bioengineered Altered Tissue: Skin
Equivalents
Graft Jacket.
derived from human dermis and
contain collagen fibers
If the wound is like a “crater”, the
Ulcer Repair Matrix (sheet form)
may be used to graft the wound
and aid in the body’s repair.
If the wound is a “tunneling”
wound, the GRAFTJACKET®
XPRESS Scaffold can be used
by applying the graft by syringe
into the wound and filling the
“tunnel”.
2/22/2013
53
Vacuum Assisted Closure Systems
Blue Sky Must have “relatively” clean wound
bed
Works well with wounds with depth but little open surface area
Instead of foam, uses a suction tubing
Advanced Treatments: Growth factors
Regranex only FDA-approved prescription
medicine that contains platelet-
derived growth factor
Contraindications:
patients with known skin cancers
at the site of application
wounds that are stitched or stapled
patients sensitive to any
components of this product (e.g.,
parabens)
Advanced Treatments: Growth factors
Autologous Platelet Collection System uses 55 ml of patient’s whole
blood
Centrifuge separates blood – isolating plasma into:
Platelet poor
Platelet rich
Platelet “rich” is put into wound
Cell Factor Technologies, Inc GPS Platelet Concentration System

2/22/2013
54
Advanced Therapies: Hyperbaric Oxygen
Origin of HBO therapy In US: Mid-to-late 1930s
Treat “bends”
Developed in Milwaukee
Medical application Mid-1960’s gained favor
Typical wound conditions:
Burns
Surgical
Infections
Diabetic ulcers
Crushing injuries
Bone fractures
Advanced Treatments: Bioengineered Altered Tissue: Skin
Equivalents
Non-autologous grafts Neonatal foreskins
Interwoven into some form of matrix that either dissolves or becomes incorporated into body tissue
Most sent frozen
Most common: Apligraft, Dermagraft and Graft Jacket
Advanced Treatments: Bioengineered Altered Tissue: Skin
Equivalents

2/22/2013
55
Advanced Treatments: Bioengineered Altered Tissue: Skin
Equivalents
Transcyte Nylon mesh fabric which has
human fibroblast
Cryopreserved
High levels of protein and growth factors
Nylon is not biodegradable
Advanced Treatments: Bioengineered Altered Tissue: Skin
Equivalents
Advanced Treatments: Bioengineered Altered Tissue: Skin
Equivalents
OASIS comprised of porcine-derived
acellular small intestine
submucosa
compatible with human tissue
unique because it is a complex
scaffolding
provides an optimal environment
- restoration of tissue structure
and function. indicated for partial and full
thickness wounds and skin loss
injuries as well as superficial and
second-degree burns.

2/22/2013
56
Advanced Therapy: Anodyne
Anodyne Therapy Use of infrared light emitting
diodes (LED)
Penetrates up to 5 cm of tissue depth
Improves circulation
Reduces pain and stiffness
Reduces muscle spasms
Works well with neuropathic ulcers
Advanced Therapies: Probiotics
Probiotics means "for life"
refers to concentrated supplements of beneficial or good bacteria
Over use of antibiotics have weakened immune systems
Probiotics - the good friendly bacteria, promotes the body's natural immunity
keeps us healthy and helps our digestion
necessary to keep the bad bacteria level lower
There are many “good bacteria” available
Examples of Probiotics
Colloidal silver
Oregano
Aloe vera
Calcium magnesium powder
Omega 3 Fish Oil
Reference list
Available on request