Embed Size (px)
Citation preview

T H E N O S E T I P 1
By DAVID MATTHEWS, M.D. , M.CH., F.R.C.S.
The Hospital for Sick Children, Great Ormond Street, London
THIS paper concerns correction of deformities associated with cleft lip and palate and with cosmetic corrections. I t does not include reconstruction following trauma.
THE TIP IN CLEFTS
One hundred and thirty cases had 163 operations performed upon them at T h e Hospital for Sick Children, London, between January 196o and July I966. All the operations were secondary to primary closure of the lip and nostril performed either at T h e Hospital for Sick Children or elsewhere. T h e operations have been analysed and an attempt made to evaluate the results (Fig. I).
REPAIR OF NOSE TIP--CLEFT LIP AND PALATE (13 ° CASES)
The Hospital for Sick Children--January 196o to July 1966
Average Method Number Age
28 9"2 33 7"3
"Flying Bird"
Lateral advancement (Broomhead)
Lateral Z-plasties (Matthews)
Inroll
Columellar advancement
Abbe and tip advancement
Ant. septal straightening
Reversed cartilage graft
Composite graft
17
31
7
14
25
5
3
Total number of separate operations 163
6. 7
5"6
5"3
9"0
7"6
15"o
12"5
FIG. I Summary of operations used to correct the nose tip in cases of cleft lip and palate.
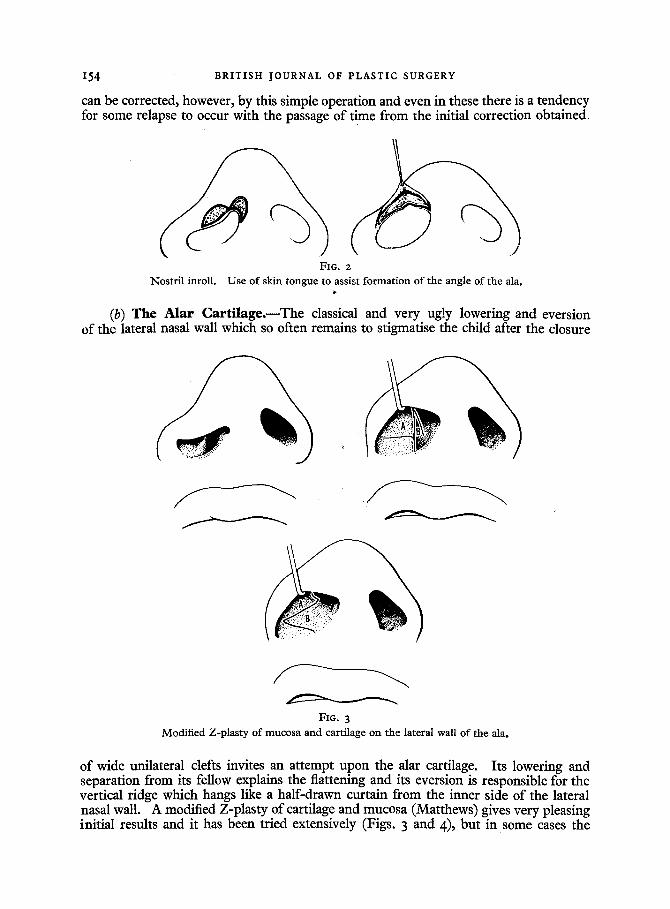
(a) Nos t r i l I n r o l l . - - T h i s is the simplest operation undertaken and like all inroll operations is basically modelled on Joseph's procedure. Usually there is an advantage in keeping the central tongue of superfluous skin and setting this into a notch created by incising the lower margin of the alar cartilage at.its angle (Fig. 2). In this way the angle can be raised more nearly to approach the level of the opposite side and a more normally acute angle can also be produced. Only very minor degrees of abnormality
1 Part of the McIndoe Memorial Lecture delivered at The Royal College of Surgeons of England, 24th November i966.
153
154 BRITISH JOURNAL OF PLASTIC SURGERY
can be corrected, however, by this simple operation and even in these there is a tendency for some relapse to occur with the passage of time from the initial correction obtained.
FIG. 2
Nostril inroll. Use of skin tongue to assist formation of the angle of the ala.
(b) The Alar Car t i lage . - -The classical and very ugly lowering and eversion of the lateral nasal wall which so often remains to stigmatise the child after the closure
FIG. 3 Modified Z-plasty of mucosa and cartilage on the lateral wall of the alao
of wide unilateral clefts invites an attempt upon the alar cartilage. Its lowering and separation from its fellow explains the flattening and its eversion is responsible for the vertical ridge which hangs like a half-drawn curtain from the inner side of the lateral nasal wall. A modified Z-plasty of cartilage and mucosa (Matthews) gives very pleasing initial results and it has been tried extensively (Figs. 3 and 4), but in some cases the

THE NOSE TIP 155
results have been disappointing in the long term because of the appearance of secondary distortion in the growing cartilages subsequent to operation. For this reason if this operation is used for vertical shelf correction it should not be performed before adolescence (Fig. 5)- A second and safer method of dealing with the lateral wall is by a rotation flap of cartilage and mucosa (Broomhead) (Fig. 6). The advantage of this
A FIG. 4 B Result of lateral alar Z-plasty.
A FIG. 5 B Alar Z-plasty combined with alar shortening.
operation over the Z-plasty is that it does not involve cutting the cartilage. It produces some very nice results but its shortcoming, as with the others, is a tendency for relapse towards the original deformity with the passage of time. The later the operation is undertaken the less is this tendency and it undoubtedly has a lasting place in the surgeon's armamentarium for dealing with this deformity (Fig. 7).
But with experience over the years it has become apparent that the best operation and the most widely applicable to the average, and the severe case, is the so-called "f lying b i rd " procedure in which the angles and lateral crura of the alar cartilages are exposed on both sides and sutured together as necessary to equalise the tip (Fig. 8).

156 BRITISH JOURNAL OF PLASTIC SURGERY
A FIG. 6 B Rotat ion flap of cartilage and muco~a on lateral alar wall (Broomhead) :
(a) incisions ; (b) on completion.
A FIG. 7 B
Result o f use of rotation flap on lateral alar wall.
FIG. 8 " F l y i n g b i rd" incision with suture of alar cartilages.
THE NOSE TIP I 5 7
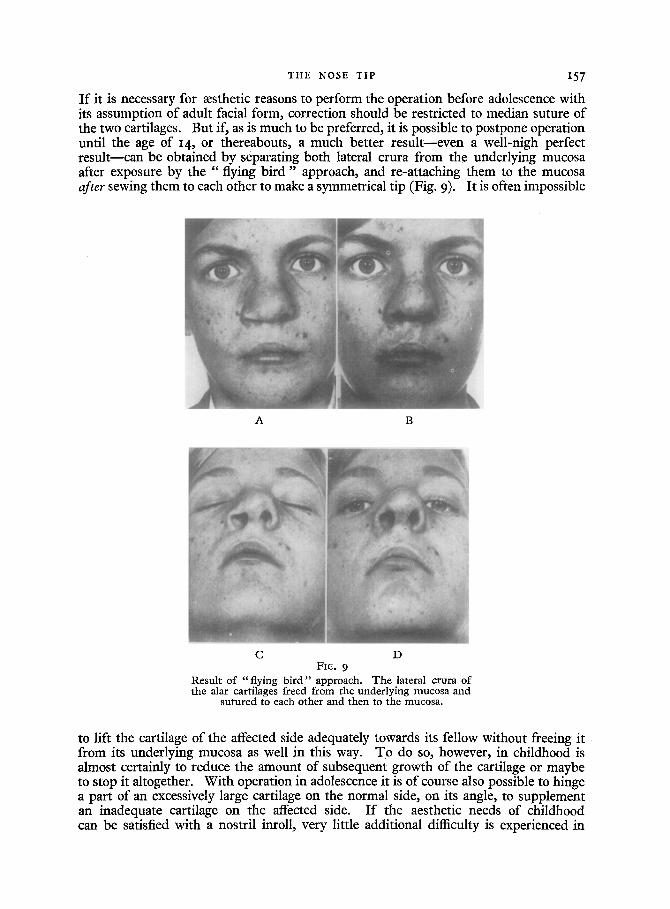
I f it is necessary for msthetic reasons to perform the operation before adolescence with its assumption of adult facial form, correction should be restricted to median suture of the two cartilages. But if, as is much to be preferred, it is possible to postpone operation until the age of 14, or thereabouts, a much better result--even a well-nigh perfect result--can be obtained by separating both lateral crura from the underlying mucosa after exposure by the "flying b i r d " approach, and re-attaching them to the mucosa after sewing them to each other to make a symmetrical tip (Fig. 9). It is often impossible
A B
C D FI6. 9
Resu l t o f " f l y i ng b i r d " approach. T h e lateral crura o f the alar cartilages freed f rom the under ly ing mucosa and
su t u r ed to each o ther and t hen to the mucosa .
to lift the cartilage of the affected side adequately towards its fellow without freeing it from its underlying mucosa as well in this way. To do so, however, in childhood is almost certainly to reduce the amount of subsequent growth of the cartilage or maybe to stop it altogether. With operation in adolescence it is of course also possible to hinge a part of an excessively large cartilage on the normal side, on its angle, to supplement an inadequate cartilage on the affected side. I f the aesthetic needs of childhood can be satisfied with a nostril inroll, very little additional difficulty is experienced in

158 BRITISH JOURNAL OF PLASTIC SURGERY
FIG. IO
Bilateral case treated by "f lying b i r d " approach.
FIG. I I FIG. I2 Fig. I I .--Bilateral case. Elongation of colurndla by winged flaps inset after lengthening the medial crura. Fig. i2 . - -Gase result after lengthening of medial crura.

THE NOSE TIP I59
performing a "flying b i r d " operation later. This is the best compromise. A Z-plasty of the alar base to turn it inwards and elevate it for symmetry can of course be combined with all these operations, and has been incorporated with them on many occasions. It is an integral part of the overall atempt to achieve symmetry of the whole nostril.
A
B FIG. I3, AandB
Case result after alar cartilage suture. Columellar advancement and Abbe flap.
Of the 29 bilateral clefts in the series 8 were satisfactorily treated by the same "flying bird" procedure, and are of course easier to deal with than the unilateral cases because the deformity is symmetrical (Fig. IO) ; 7 needed the combination of suture of the cartilages with advancement of the columella (Matthews) (Figs. II and I2) and 14 needed cartilage suture, columeUar advancement and an Abbe flap as well at the

160 BRITISH JOURNAL OF PLASTIC SURGERY
FIG. I3, C
same time (Fig. 13). Even with this extensive procedure it is simpler to get a good result in bilateral cases than in the asymmetrical unilateral case.
(c) The Septum.--Operations on the tip in cleft cases may also need to be accompanied by corrective procedures on the anterior cartilaginous part of the septum and these can be undertaken simultaneously without risk if a few simple precautions are taken. The cartilage should be exposed by lifting the perichondrium from only one side, and the risk of damage to the contralateral mucosa minimised by standing it away by the injection of local ana:sthetic. Part of the cartilage can then be safely resected to relieve the tension causing the deflection. The remaining framework can also be thinned by paring it down to straighten convexities, or when necessary it can be completely divided either through the columellar strut or on the bridge-line, provided it is afterwards transfixed by a catgut stitch. The reason why such liberties can be taken is because of the preservation of the perichondrial-cartilaginous adhesion on the contralateral side. Half the maxillary spine can also be safely removed with an osteotome or nibblers if it is deviated, as is so often the case. The spine should never be removed completely, since its absence causes some ugliness from retraction of the naso-labial angle.
(d) Compos i te Graf t . - -These have been required on only three occasions to make good losses of the alar base (Fig. 14).
(e) Reversed Cartilage Graf t . - -This is useful for the restoration of the convexity to a collapsed lateral nostril wall. It is equally useful for collapse and flattening which results from other causes besides clefts, and overcomes the tiresome inspiratory obstruction some patients experience from congenital inadequacy of the lateral crura of the alar cartilages. A piece of auricular cartilage is taken through a post-auricular approach and inserted subcutaneously from a small incision in the nostril fold. The cartilage is sprung in under slight tension so that its natural curvature is reversed (Fig. 15). I f it is put in with normal curvature the cartilage is not strong enough to hold the nostril aperture open. Enough cartilage can easily be taken from one ear for both nostrils without causing deformity (Fig. 16).

THE NOSE TIP 16I
FIG. 14 Composite graft. Used to restore alar base.
Reversed cartilage graft. FIG. 15
Auricular cartilage inserted under tension and against its normal curvature through an incision lateral to the alar base.
FIG. 16 Reversed cartilage graft. Case result.
162 BRITISH JOURNAL OF PLASTIC SURGERY
THE COSMETIC T I P
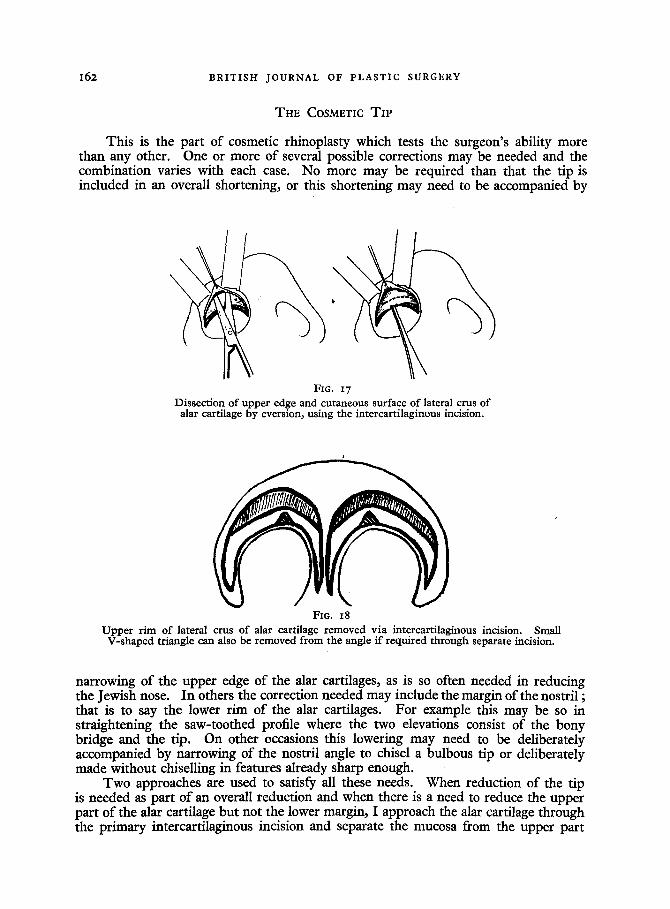
This is the part of cosmetic rhinoplasty which tests the surgeon's ability more than any other. One or more of several possible corrections may be needed and the combination varies with each case. No more may be required than that the tip is included in an overall shortening, or this shortening may need to be accompanied by
FIG. 17 Dissection of upper edge and cutaneous surface of lateral crus of
alar cartilage by eversion~ using the intercartilaginous incision.
FIG. 18 Upper rim of lateral crus of alar cartilage removed via intercartilaginous incision. Small
V-shaped triangle can also be removed from the angle if required through separate incision.
narrowing of the upper edge of the alar cartilages, as is so often needed in reducing the Jewish nose. In others the correction needed may include the margin of the nostril ; that is to say the lower rim of the alar cartilages. For example this may be so in straightening the saw-toothed profile where the two elevations consist of the bony bridge and the tip. On other occasions this lowering may need to be deliberately accompanied by narrowing of the nostril angle to chisel a bulbous tip or deliberately made without chiselling in features already sharp enough.
Two approaches are used to satisfy all these needs. When reduction of the tip is needed as part of an overall reduction and when there is a need to reduce the upper part of the alar cartilage but not the lower margin, I approach the alar cartilage through the primary intercartilaginous incision and separate the mucosa from the upper part
THE NOSE T I P I 6 3
A B
C D
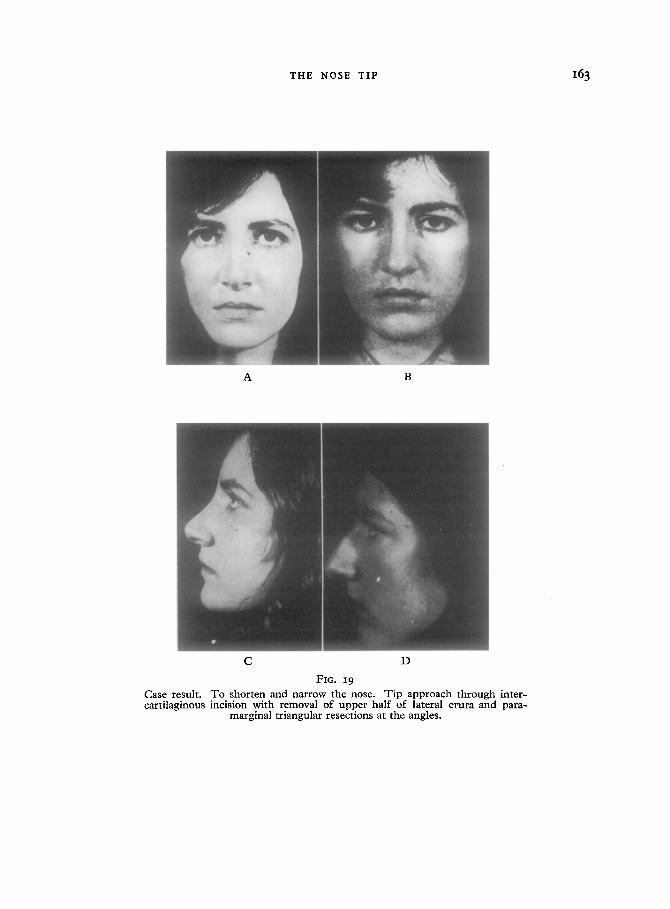
FIG. 19
Case result. To shorten and narrow the nose. Tip approach through inter- cartilaginous incision with removal of upper half of lateral crura and para-
marginal triangular resections at the angles.

I6 4 BRITISH JOURNAL OF PLASTIC SURGERY
A B
C D
FIG. 2o Case result. To shorten and produce retrouss6 tip. T ip approach through intercartilaginous incision with removal of only the outer part of the upper margin of the lateral crura. No paramarginal triangular excisions required.
THE NOSE T I P 16 5
of the cartilage after everting it (Fig. x7). This involves no sacrifice of mucosa and allows removal of the upper half of the alar cartilage from the midline as far laterally as is required. This operation can of course be combined with a small paramarginal apical V-shaped resection of cartilage and mucosa to give fractional narrowing of the tip as well (Figs. I8, I9 and 20).
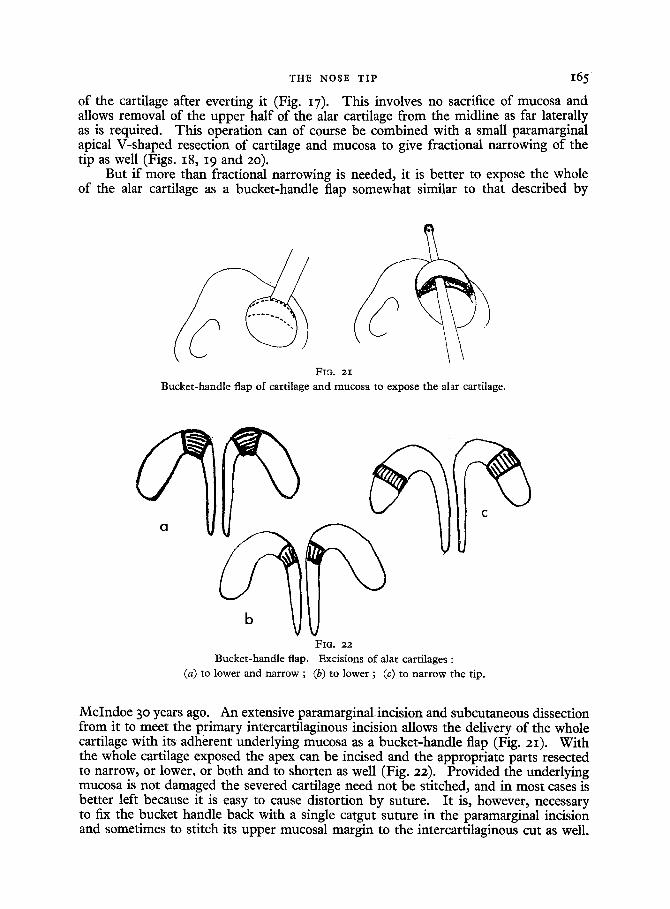
But if more than fractional narrowing is needed, it is better to expose the whole of the alar cartilage as a bucket-handle flap somewhat similar to that described by
FI,9. 2I
Bucke t -hand le flap o f cartilage and mucosa to expose the alar cartilage.
FIG. 22
Bucke t -hand le flap. Excis ions o f alar cart i lages :
(a) to lower and nar row ; (b) to lower ; (c) to na r row the tip.
McIndoe 30 years ago. An extensive paramarginalincision and subcutaneous dissection from it to meet the primary intercartilaginous incision allows the delivery of the whole cartilage with its adherent underlying mucosa as a bucket-handle flap (Fig. 2z). With the whole cartilage exposed the apex can be incised and the appropriate parts resected to narrow, or lower, or both and to shorten as well (Fig. 22). Provided the underlying mucosa is not damaged the severed cartilage need not be stitched, and in most cases is better left because it is easy to cause distortion by suture. It is, however, necessary to fix the bucket handle back with a single catgut suture in the paramarginal incision and sometimes to stitch its upper mucosal margin to the intercartilaginous cut as well.

I66 BRITISH JOURNAL OF PLASTIC SURGERY
A B
C D
FIG. 23 Case result. To correct " saw too th" bridge-line and narrow the tip. Bucket-
handle approach to tip. Cartilage treated as in Figure 2z (a).

THE NOSE TIP I 6 7
A B
C D
FIG. 2 4
Case result. To achieve maximum reduction of all elements in the nasal framework. Tip approached with bucket-handle flap and treated as in Figure zz (a) as well as by removal of the upper half of the lateral crura and a thin
piece of the lower margins of the lateral and medial crura.
It is also a help, for modelling with precision, to pack the nostrils with tulle gras for 24 hours. Its stickiness provides an ;.nternal splint which facilitates the creation of the desired shape (Figs. 23 and 24).





























