Embed Size (px)
Citation preview

The Next Big Thing
Dr Anne WeaverConsultant in Emergency Medicine & Pre-hospital Care
Clinical Director for TraumaRoyal London Hospital

Things to share with you
• Good conference / interesting journal• Recent research – PROPPR, FIinTIC, EFIT, Cryostat 1&2, ITACTIC• Platelet storage • TXA, DOACS • The next big thing• New gadgets / monitors

Vicky

THOR / RDCR networkTransfusion journal annual supplement

International stats
• Trauma – 4th leading cause of death globally• 40% trauma deaths due to bleeding• 2 million / yr worldwide• Massive transfusion - 50% mortality• Acute traumatic coagulopathy - 30% trauma pts• ATC - 4 fold increase mortality

UK stats – trauma haemorrhage
• 4700 / yr major haemorrhage (1550 dead)• 1300 / yr massive haemorrhage (585 dead)• Deaths 50% in 24hrs (50% in first 4 hrs)• 50% needed urgent surgery• £85 million / yr

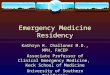
Acute Traumatic Coagulopathy

Trauma
TRAUMA INDUCEDCOAGULOPATHY
Shock
Acidemia
ACUTE TRAUMATIC COAGULOPATHY
Platelet dysfunction
↑ activatedProtein C
Neuro-endocrine axis
Fibrinolysis↑ Thrombin
Hemodilution
Hypothermia
Fibrinolysis
↓Fibrinogen
Resuscitation related

Catastrophic haemorrhage in PHC• C ABC• Tourniquets• Novel haemostatic agents• Handling and packaging• Splinting• Permissive hypotension• Damage control resuscitation / surgery – thoracotomy / REBOA• Blood product transfusion• TXA administration

“CODE RED”pre-alert system
Often for non-compressible haemorrhage
Make a clinical judgment of injury loadDetermine the presence of shock – physiologyActivation of Massive Haemorrhage Protocol


2.8 units pRBCtransfused
On-scene time 37 mins Hb 14.0
pH 7.07 BE – 12.8

Pre-hospital PRBC trials
• PRBC• Improved outcomes• 6hr survival• 24hr survival• Reduced blood product transfusion in 24hrs• Improved BE / acid base balance on admission• Feasible – Scandinavia / Australia / US / UK• Low wastage

Does 1:1 improve outcome?
Kashuk et al. J Trauma 2009; 65: 261-71
Borgman et al. J Trauma 2007; 63:805–813

Plasma
• Contains plasma proteins, clotting factors, fibrinogen• Volume resuscitation• Haemostatic resuscitation• Restores glycocalyx• Available as:
• Fresh Frozen Plasma (FFP) – thawed for use (delay)• Lyophilised / freeze dried plasma – reconstituted, not licensed in UK• Liquid plasma – never frozen, contains platelets, 7 day shelf life

Pre-hospital plasma in practice
• Trials in US - PAMPER, COMBAT, PUPTH• Feasible but high wastage due to short shelf-life – extended to 5 days
in April 2016• Wales & Thames Valley AA – thawed plasma• France, Germany, Kent / Surrey & Sussex – freeze dried plasma• If born after 1st Jan 1996 – to avoid CJD, cannot have UK plasma –
give DOB if known in pre-alert.

VS.

PROPPR (plasma, platelet, RBC) trial
• Multi-centre RCT• 1:1:1 vs 1:1:2• Low numbers• No stat sig difference in 24 hr or 30 day mortality• Higher rate of haemostasis• Reduced numbers of death due to exsanguination• UK National guidelines changed on this basis last year (2015)• MHPs should be aligned to this ratio

Platelets
• We were told: “Stored at room temperature, constant agitation”
• We weren’t told: that they have better function at 4C
• Shortened time in circulation but that’s ok for severe bleeding
• Cold platelets might be useful in trauma

Fibrinogen

Impact of fibrinogen levels on outcomes after acute injury in patients requiring a massive transfusion.Inaba K et al. J Am Coll Surg. 2013 Feb;216(2):290-7.
Fibrinogen > 180 mg/dl, Fibrinogen 180 – 100 mg/dl, Fibrinogen < 100 mg/dl

Hyperfibrinolysis

Fibrinogen concentrate or cryoprecipitate
• Fibrinogen• Takes a while to mix esp high
dose• Expensive• Only contains fibrinogen• Easy to carry / store at room
temp• Not currently licensed in UK
• Cryoprecipitate• Has to be thawed but is “ready
mixed”• Contains other factors vWf, XIII,
fibronectin• Relatively cheap• Research re shelf-life of pre-
thawed cryo - up to 14/7

Fibrinogen RCT

http://efit1trial.co.uk/


CRYOSTAT
a

CRYOSTAT Mortalitya
Standard: Y 6/21 : 28%Early CRYO: 2/20 : 10%

CRYOSTAT 2

Tranexamic Acid


Tranexamic acid - standard practice
• 1 g bolus followed by 1 g infusion over 8 hrs• Benefit if given within 3 hrs• Optimal results if within 1 hr• Maximal effect for SBP <75mmHg• Potentially harmful if delayed >3hrs• Trial data showed no increase in arterial or venous thrombosis

Royal London research team data
• First dose of TXA is effective for most patients• Visible reduction in hyperfibrinolysis on ROTEM• 2nd dose (infusion) may not be required in many cases• If hyperfibrinolysis persists – need to provide more substrate ie Fg• Code Red pts who receive TXA have 10% VTE rate (much higher than
control group)
• Suggestion from US group that TXA should be more targeted than current practice and guided by ROTEM / TEG.
Moore E et al Transfusion 2016;56(Suppl 2):S115-118

iTACTICImplementing Treatment Algorithms for the Correction of Trauma Induced Coagulopathy
Prospective, randomised controlled trialBleeding trauma patients
ROTEM / TEG vs conventional clotting tests (CCT)

ROTEMTM
TEG®
Visco-elastic assays

5 minute diagnosis
ATC

iTACTICImplementing Treatment Algorithms for the Correction of Trauma Induced Coagulopathy
FIBRINOGENIf FIBTEM CA5 < 10mmGive additional 4g equivalent of fibrinogen (As Cryoprecipitate or Concentrate)
PLATELETSIf (EXTEM CA5 - FIBTEM CA5) < 30mmGive 1 additional pool of platelets
PLASMAIf EXTEM CA5 >40mm AND EXTEM CT >80sGive 4 additional units of plasma
TRANEXAMIC ACIDIf EXTEM LI30 <85% Give additional 1g IV bolus of tranexamic acid

NOACS / DOACS(Non-vitamin K dependent / Direct oral anti-coagulants)
Eg Dabigatran, Rivaroxaban

Novel anti-coagulants

Dabigatran antidote – Idarucizumab (Pradaxa, Praxbind)• Available in a pharmacy near you??• Better if it was in a cupboard in resus or in your Thomas pack……• Interim results of a phase III trial – Pollock et al. 2015• Immediate reversal of dabigatran by binding to drug & metabolites• IV drug – 5g ( 2 x 50 ml bolus over 20 minutes)• £2400• Dose can be repeated• May need blood product support to control bleeding

Blood product transfusion in PHC
• Ratios debate• ABO compatability and availability• Temperature – storage of components• Safety – leuco-reduction• Cold storage – loss of platelet function??• Feasibility – packaging, licensing, cold chain, traceability

Treating blood failure – we need a fluid that can……
• Repay oxygen debt – PRBC, crystalloid• Stop proteolysis - plasma• Repair glycocalyx – plasma, platelets• Treat coagulopathy – plasma, cryo, TXA, platelets
• And restores volume as quickly as possible……

The Next Big Thing
• 1:1:1• Plasma: PRBC: platelets• Through one IV line• No mixing with water• Leuko-depleted with platelet
sparing filter
• No UK production chain currently……

Transfusion. 2016:56;S190-S202• US Army data• WB superior or equivalent to blood product txn• 4C platelets have better function than 22C plt

Norway (PHC and special forces)
• Military-civilian co-operation• Freeze dried plasma – 2013• PRBC – 2014• Whole blood – 2015 (Special forces only)• Warm, whole blood donation to “buddy”• Pre-screened personnel• Fit to continue special ops work after donation• Developed protocol for Emergency Donor Panels
• Rapid blood group – 40s• Blood borne virus screen – 60s

New gadgets / monitoring
• Compensatory Reserve Index monitoring (Convertino – physiologist)• In development• Could be used to select Special Forces recruits with better reserve• Red / amber / green indicator• Accurate predictor of reserve• Could be added to traditional monitors
J App physiol 2013;115:1196-1202.
• ROTEM sigma model• Easier to use than previous Delta version• Perhaps much smaller version in future for PHC use

Ongoing work for bleeding patients
• Research trials – rapidly translate to clinical practice• Whole blood – bench work prior to RCT in civilian pre-hospital care
setting• Improve processes & procedures
• Ambulance service dispatch and advice to bystanders• “Right turn resuscitation” – direct to theatre• Hospital design – RAPTOR suites
• Mass Casualty events• Stock planning / product type• Emergency Donor panels


ROYAL LONDON HOSPITAL MTC CODE RED MORTALITY