Embed Size (px)
Citation preview

11/13/2009
1
The Neurological Control of Movement
Mary ET Boyle, Ph.D.Department of Cognitive Science
UCSD
Levels of Control of Movement
• A change in the place or position of the body or a body part.Movement y y p
• When neurological control of movement is working correctly we can … do anything!
• If not, movement disorders such as myasthenia gravis, movement apraxia, ALS, Parkinson’s disease, and Huntington’s disease.

11/13/2009
2
Levels of Control of Movement: Simple to Complex
The simplest movements are reflexive reactions
withdrawing your hand after touching a hot stove or blinking when something
more complex than reflexes, but less complex than other skills
maintaining posture, sitting, standing, walking, and eye movement
withdrawing your hand after touching a hot stove or blinking when something gets in your eye
complex movements can be learned
playing the violin, riding a bike, and operating exercise equipment

11/13/2009
3
Stimulation of Movement
Most basic level of control is the spinal cord (e.g., spinal reflexes, such as the withdrawal reflex, are solely controlled by the spinal cord).spinal cord).
Next level involves brain stem structures in the hindbrain and midbrain (e.g., visual pursuit of a light stimulus).

11/13/2009
4
Highest level of control Highest level of control involves the cerebral cortex and structures such as the dorsolateralprefrontal cortex, the primary and secondary motor cortex, and the motor cortex, and the somatosensory cortex.
Basal Ganglia (main components: striatum, pallidum, substantia nigra, and subthalamic nucleus)
Influences movement by smoothing out and refining it(gets rid of extraneous movement and acts to (gets rid of extraneous movement and acts to ensure that the selected movement occurs with sufficient, but not excessive, force); also responsible for muscle tone and postural adjustments.
The corpus striatum and Huntington’s disease – leads to substantial
enlargement of the lateral ventricles

11/13/2009
5
Cerebellum
Plays a central role in l i di d translating uncoordinated
movements into a skilled action;
receives feedback from sensory receptors that monitor movement and brain stem structures that initiate movement.

11/13/2009
6
Three types of muscle tissue in the body:

11/13/2009
7
11/13/2009
8
extension
Contraction of triceps muscle
(extensor)
flexion
Contraction of the biceps muscle
(flexor)
movement away from the
body
brings the extended
limb back toward the body
Skeletal muscle
Muscle fibers
Myofibrils
MyofilamentsyMyosin
(thick filaments)
Actin
(thin filaments)
11/13/2009
9
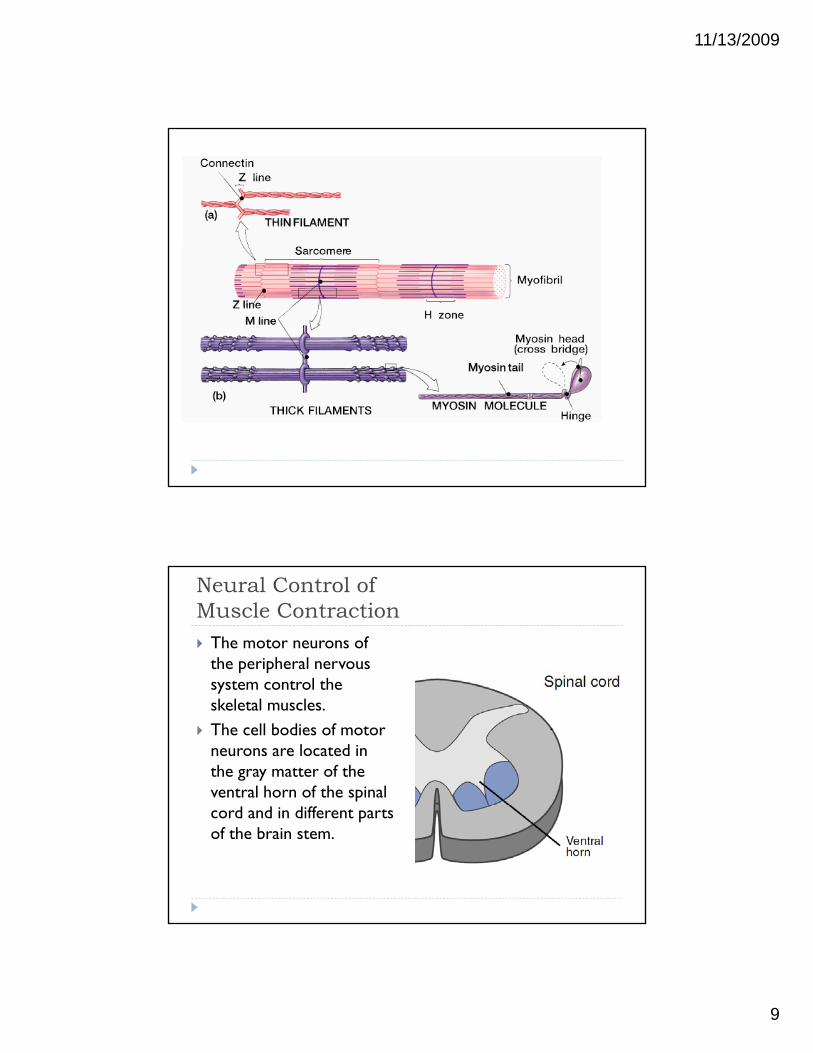
Neural Control of Muscle Contraction The motor neurons of
the peripheral nervous system control the system control the skeletal muscles.
The cell bodies of motor neurons are located in the gray matter of the ventral horn of the spinal cord and in different parts of the brain stem.

11/13/2009
10

11/13/2009
11
Motor Neurons: Transmission of a Neural Impulse
Transmission of a neural impulse from motor neuron to muscle fiber at the neuromuscular junction—similar to th t i i f l i l b t the transmission of neural impulses between neurons
Motor neuron releases ACh into the synaptic cleft.
ACh binds to receptor proteins on the postsynaptic membrane (the muscle fiber).
EPSPs are then produced; upon sufficient excitation, an action potential is generated.
Neuronal voltage gated calcium channel
Skeletal muscle di h l
ACH
sodium channel
Potassium channel
ACH receptor

11/13/2009
12
As the action potential travels down the muscle fiber, it increases the permeability of the fiber membrane to Ca2+ ions, which causes myosin headswhich causes myosin heads to form cross bridges with actin filaments.
The myosin heads pivot, causing the myosin and actin filaments to slide past one another.
The Motor Unit
A motor neuron and the muscle fibers it controls form a
Each branch of an axon synapses with a single muscle
muscle fibers it controls form a motor unit
synapses with a single muscle fiber.

11/13/2009
13
Patellar Reflex
The reflex in which tapping the tendon of pp gthe knee stretches one of the muscles that extends the leg, and the resulting muscle contraction causes the leg to kick outward.
Muscle spindle—A structure embedded within an extrafusal muscle fiber than enables the CNS to contract a muscle to counteract the stretching of the extrafusal muscle fiber.
Intrafusal muscle fiber— A muscle fiber that extends the length of the muscle spindle that is surrounded by annulospiral endings (sensory receptors in the central part of the muscle fiber).
11/13/2009
14
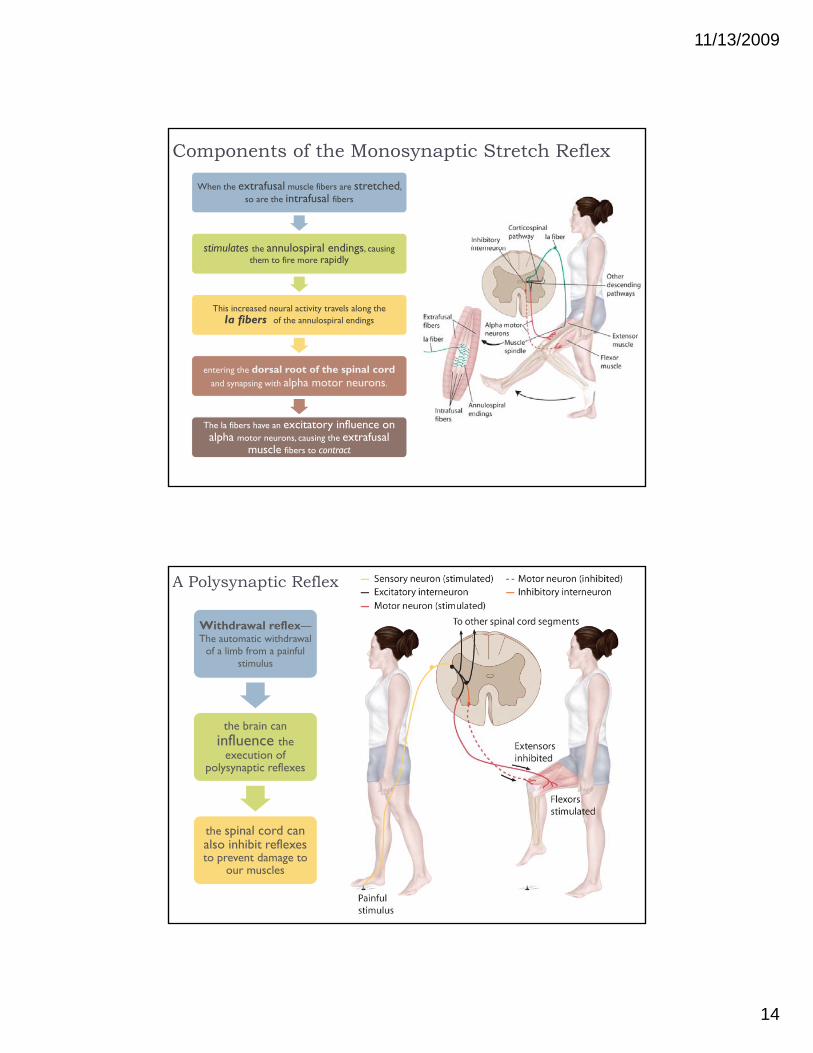
Components of the Monosynaptic Stretch Reflex
When the extrafusal muscle fibers are stretched, so are the intrafusal fibers
stimulates the annulospiral endings causing stimulates the annulospiral endings, causing them to fire more rapidly
This increased neural activity travels along the Ia fibers of the annulospiral endings
i h d l t f th i l d entering the dorsal root of the spinal cord and synapsing with alpha motor neurons.
The Ia fibers have an excitatory influence on alpha motor neurons, causing the extrafusal
muscle fibers to contract
A Polysynaptic Reflex
Withdrawal reflex—The automatic withdrawal
of a limb from a painful stimulus
the brain can influence the
execution of polysynaptic reflexes
the spinal cord can also inhibit reflexes to prevent damage to
our muscles

11/13/2009
15
Golgi Tendon Organs
Receptor located among the fibers of tendons that measures the total amount of force exerted by
the muscle on the bone to which the tendon is attached
Enables motor system to control extent of muscle contraction.
Strength of muscle contraction reflects the force exerted by the muscle on the bone—the
f f greater the contraction of the muscle fibers, the greater the force on the bone.
With too much force, Golgi tendon organs reduce the contraction of extrafusal muscle
fibers, resulting in the muscle exerting less pressure on the tendon and bone.
Renshaw Cells
An inhibitory interneuron excited by an alpha motor neuron that causes it to stop firing, p g,preventing excessive muscle
contraction.
C b t l d Combats muscle damage that can result from fatigue, which results from muscles
contracting often in a short period of time.

11/13/2009
16
Gamma Motor NeuronsA neuron that synapses with intrafusalmuscle fibers to produce continuous
muscle tension.
Continuous activity of gamma motor neurons produces a constant contraction
of extrafusal muscle fibers
(muscle tone)
This muscle tone is maintained at all times, except during REM sleep.
The gamma motor system also gives us the ability to anticipate certain
movements and react quickly.
Brain Control of Voluntary Movement
• Hierarchically organized• Starts at dorsolateral prefrontal cortex.• Decision maker• Decision maker
• Sensory input primarily integrated by the posterior parietal cortex.
• Learning changes the locus of control over the movements.
• Subcortical control. More efficient.

11/13/2009
17
Dorsolateral Prefrontal Cortex The top executive in the perception-action cycle in
nonhuman primates and humans.
cells in this area integrate sensory information
across time with motor across time with motor actions needed to deal
with the information
Secondary Motor Cortex
Cortical area consisting of the supplementary motor and the premotor areasand the premotor areas.
Supplemental motor area --involved in the
planning and
sequencing of voluntary movementsvoluntary movements(internally generated
stimuli)Premotor cortex plans and sequences externally guided
movements.
Receives input mostly from the visual cortex

11/13/2009
18
Supplemental motor area Part of the secondary motor cortex.
receives input from pthe posterior
parietal cortex and the somatosensory
cortex
Because most movements are guided by both intentions and external stimuli, the connections between the supplementary motor area and the premotor cortex coordinate movement planning.
Cortical Control of Movement
Primary motor cortex:initiates voluntary movements
Directly involved in the control of motor neurons.
Stimulation results in movements involving groups of muscles – not individual muscles.

11/13/2009
19
Mirror Neurons
Neurons in the primate premotor cortex that are activated by performing an action or by watching another monkey or person performing an action. Also seems to exist in humans, in Broca’s area and the
primary motor cortex. Humans learn many actions through the observation and
imitation of the actions of others and the mirror neuron system provides a possible mechanism through which observation can be translated into action.
Plasticity of the Primary Motor Cortex
The primary motor cortex shows great plasticity in its response to sensory and motor changes.
Any body part has multiple and widely distributed representations in the topography of the primary motor cortex.

11/13/2009
20
Plasticity of the Primary Motor Cortex
Though the exact mechanism for this plasticity is not known, one possibility is long-term potentiation (LTP), a long-lasting increased excitability in a specific neural circuit caused by repetitive stimulation. May represent learning at the cellular level.
D d NMDA i i d GABA Dependent on NMDA receptor activation and GABAAreceptor inhibition; weakened by the drug scopolamine.
Primary Somatosensory Cortex
The sensory receptors in the muscles and joints send information about the external environment to the
d h i i l somatosensory cortex and the posterior parietal cortex.
It then goes to the dorsolateral prefrontal cortex, the secondary motor cortex, and then the primary motor cortex.
The primary motor cortex then becomes aware of the f h l h b i d d h status of the muscles that must be activated and the
location of the body parts that must be moved in order to exert the right amount of force.
11/13/2009
21
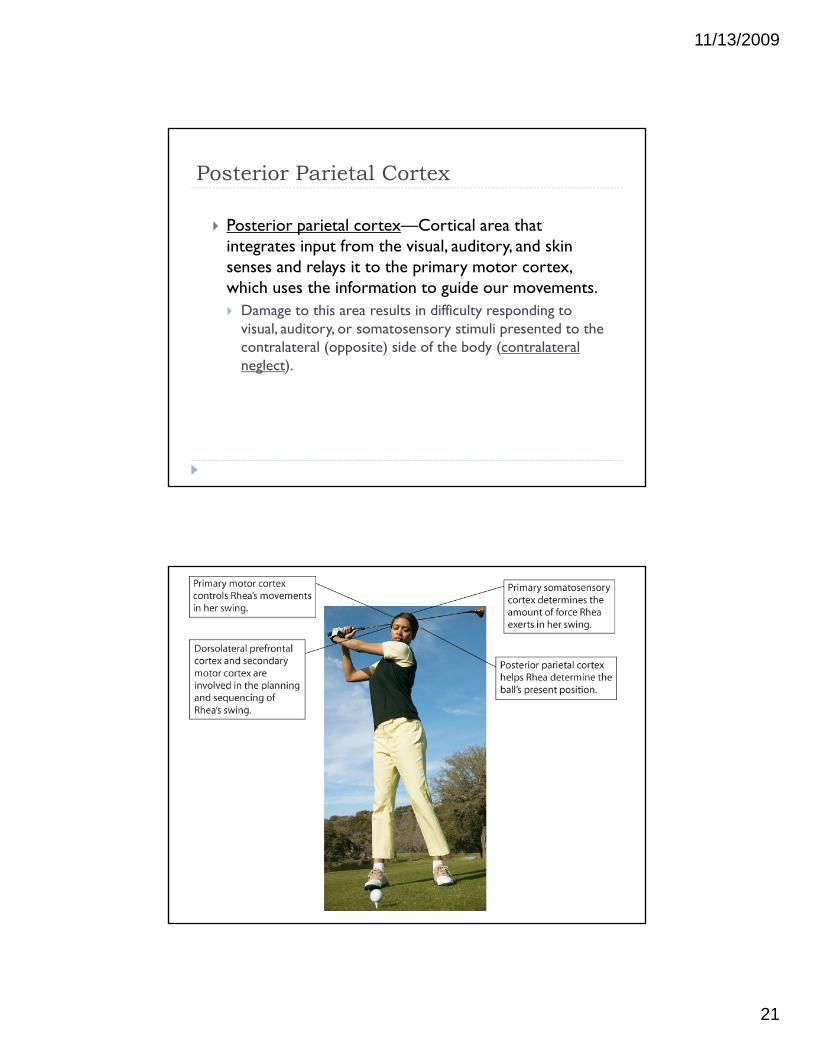
Posterior Parietal Cortex
Posterior parietal cortex—Cortical area that integrates input from the visual auditory and skin integrates input from the visual, auditory, and skin senses and relays it to the primary motor cortex, which uses the information to guide our movements. Damage to this area results in difficulty responding to
visual, auditory, or somatosensory stimuli presented to the contralateral (opposite) side of the body (contralateral neglect)neglect).

11/13/2009
22
Other Movement Disorders
Apraxia—A movement disorder characterized by missing or inappropriate actions not caused by paralysis or any other motor impairmentor any other motor impairment.
Constructional apraxia—A disorder characterized by difficulty drawing pictures or assembling objects.
Limb apraxia—An impairment in the voluntary use of a limb caused by damage to the left parietal lobe or the corpus callosum.
Apraxia of speech—A disorder characterized by difficulty speaking clearly, caused by damage limited to Broca’s area.
Motor Pathways
The primary motor cortex uses information from the posterior parietal cortex, somatosensory cortex, and secondary motor cortex to initiate movement.
From the primary motor cortex and other cortical areas, two fiber tracts travel through the midbrain and hi db i d i h h PNS i d hindbrain and connect with the PNS in order to produce movement.

11/13/2009
23
Tracts Originating in the Motor Cortex
Corticospinal tract—Motor pathway that controls movements of fingers, hands, arms, trunk, legs, feet. Lateral corticospinal tract—The axons of the corticospinal
tract that cross over in the medulla to connect to the opposite side of the spinal cord, controlling the movement of the fingers, hands, arms, lower legs, and feet on the opposite side of the b dbody.
Ventral corticospinal tract—The noncrossing axons that control the movements of the trunk and upper legs on the same side of the body.
Corticobulbar tract—A motor pathway that controls movements of the face and tongue.
Tracts Originating in the Primary M t Motor Cortex

11/13/2009
24
Tracts Originating in the Subcortex
Ventromedial tract—One of four motor pathways originating in different parts of the subcortex that control movements of the trunk and limbs.
Vestibulospinal tract—A ventromedial tract that plays a central role in posture.T l A d l h l Tectospinal tract—A ventromedial tract that controls upper trunk (shoulder) and neck movements and coordinates the visual tracking of stimuli.
Tracts Originating in the Subcortex
Lateral reticulospinal tract—A ventromedial tract that activates the flexor muscles of the legs.
Medial reticulospinal tract—A ventromedial tract that activates the extensor muscles of the legs.
Rubrospinal tract—A motor pathway that controls f h h d l l l d movements of the hands, lower arms, lower legs, and
feet.

11/13/2009
25
Tracts Originating in the Subcortex

11/13/2009
26

11/13/2009
27
The Cerebellum
The brain area responsible for developing rapid, coordinated responses or habits.
Located behind and beneath the cerebral cortex; outer surface is extremely convoluted; represents 10% of the brain’s mass, but contains more than half of its neurons.
Ballistic movement—A habitual, rapid, well-practiced movement that does not depend on sensory feedback; controlled by the cerebellum.

11/13/2009
28
The Cerebellum
Input to/output from the cerebellum is conveyed by large bundles of axons called peduncles.
Integrates information about motor activity, balance and head position, limb position and extent of muscle contraction and determines whether ongoing movements
d i ti f th i i t d d are deviating from their intended course. If movements begin to deviate, the cerebellum can correct
them by sending signals to other structures, such as the deep cerebellar nuclei.
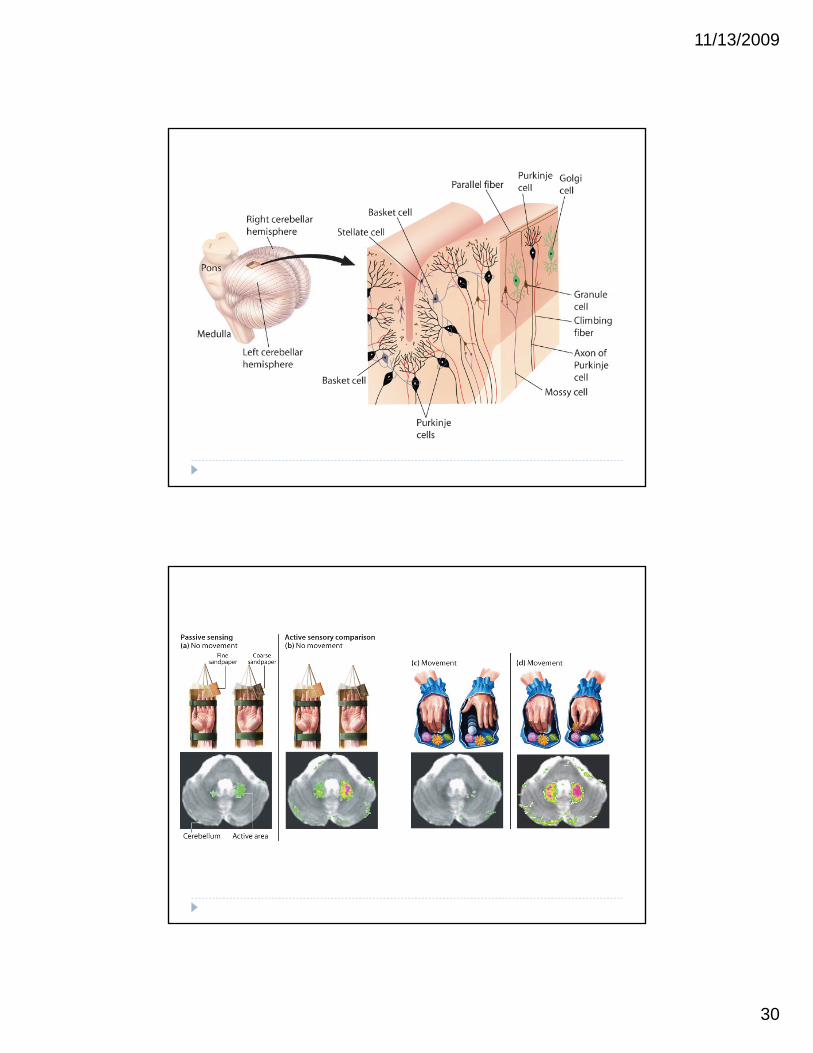
The Cerebellum Purkinje cells–An output cell from the cerebellar cortex,
which has an exclusively inhibitory effect. B k t ll A b ll th t h i hibit Basket cell—A cerebellar neuron that has an inhibitory
influence on Purkinje cells.

11/13/2009
29
Consequences of Cerebellar Damage
Difficulty maintaining a stable posture, making movements such as walking unsteady, slurred speech, and uncoordinated eye movements.
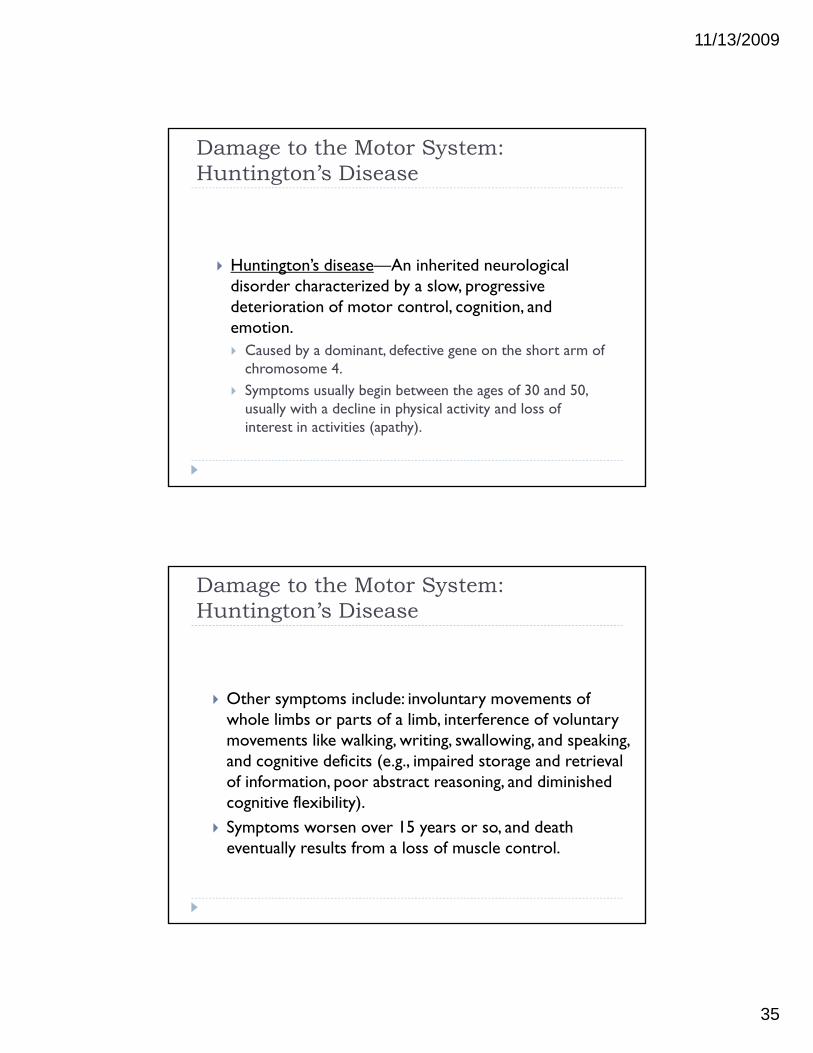
Research suggests that the cerebellum plays a significant role in cognitive behaviors in addition to its role in fine-tuning motor movements and in motor learning.
Neurons in the cerebellum are sensitive to alcohol; alcohol intoxication can lead to signs of cerebellar malfunction.
See Scientific American Spotlight “Probing Cerebellar Function”
11/13/2009
30

11/13/2009
31
The Basal Ganglia
Basal Ganglia—Group of structures that integrates movement and controls postural adjustments and muscle tone. Consists of three subcortical nuclei:
Caudate nucleus (part of neostriatum) Putamen (part of neostriatum) Putamen (part of neostriatum)
Globus pallidus (paleostriatum)
Corpus striatum—Part of the basal ganglia consisting of the caudate nucleus and putamen.
The Basal Ganglia
Integrates movement through interconnections with the primary motor cortex, the cerebellum, substantia nigra, red nucleus, and other motor centers in the brain.
Damage to the basal ganglia results in impairments in l l i bili l i d muscle tone, postural instability, poorly integrated
movements, and difficulty performing voluntary movements (e.g., standing and walking).

11/13/2009
32
The Basal Ganglia
Damage to the Motor System: Parkinson’s Disease
Parkinson’s disease—A degenerative neurological disorder characterized by rigidity of the limbs and muscle tremors. Bradykinesia—A movement disorder characterized by
slow movement. Festination—A tendency in a movement disorder to speed
up a walking pace to running. Other symptoms include: difficulty in speaking, lack of y p y p g,
facial expression, apathy, lack of spontaneous blinking, cognitive deficits (e.g., problems with learning, memory, attention, and judgment).

11/13/2009
33
Damage to the Motor System: Parkinson’s Disease
First signs of the disease may include a tremor in one hand or some stiffness in the muscles of a leg
Over time, tremors and rigidity worsen; movement becomes increasingly impaired.
Motor disturbances are caused by the degeneration of the DA-producing cells of the substantia nigra that synapse with the basal ganglia.
Damage to this nigrostriatal dopaminergic system leads to the bradykinesia, whereas the rigidity and tremors are believed to result from excessive activity in a neural loop extending from the ventrolateral thalamus to the primary motor cortex.
Damage to the Motor System: Parkinson’s Disease Suggested causes: Genetic basis E h liti Encephalitis Arteriosclerosis Carbon monoxide or manganese poisoning Trauma to the head Syphilitic damage to the brain Environmental toxins

11/13/2009
34
Damage to the Motor System: Parkinson’s Disease
Possible treatments: Levodopa—L-dopa; a drug converted to DA in the brain,
increasing levels of DA depleted by the disease. Effective in decreasing rigidity and improving movement, but less
effective in reducing tremors. High dosages can result in schizophrenic-like symptoms.g g p y p
Damage to the Motor System: Parkinson’s Disease
Possible treatments: Thalamotomy—Psychosurgical treatment that relieves
tremors and improves rigidity; does not relieve bradykinesia. Pallidotomy—Psychosurgical treatment that reduces tremors,
rigidity, and bradykinesia. Deep brain stimulation Deep brain stimulation Transplantation of fetal tissue into the corpus striatum (highly
controversial)
11/13/2009
35
Damage to the Motor System: Huntington’s Disease
Huntington’s disease—An inherited neurological disorder characterized by a slow, progressive deterioration of motor control, cognition, and emotion. Caused by a dominant, defective gene on the short arm of
chromosome 4chromosome 4. Symptoms usually begin between the ages of 30 and 50,
usually with a decline in physical activity and loss of interest in activities (apathy).
Damage to the Motor System: Huntington’s Disease
Other symptoms include: involuntary movements of whole limbs or parts of a limb, interference of voluntary movements like walking, writing, swallowing, and speaking, and cognitive deficits (e.g., impaired storage and retrieval of information, poor abstract reasoning, and diminished cognitive flexibility)cognitive flexibility).
Symptoms worsen over 15 years or so, and death eventually results from a loss of muscle control.

11/13/2009
36
Damage to the Motor System: Huntington’s Disease
Inability to control voluntary movements is caused by atrophy of the cerebral cortex and basal ganglia.
The death of neurons in the basal ganglia decreases GABA and ACh levels, which increases activity in the nigrostriatal dopaminergic pathway. This causes the
f h i l h appearance of the involuntary movements that characterize the disease.
Terms
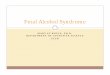
Opposing action of skeletal muscles can be illustrated in the e tensi n and fle i n f a limbthe extension and flexion of a limb.
Contracting an extensor muscle produces extension of the limb (movement away from the body).
Contracting a flexor muscle causes flexion (brings the extended limb back toward the body).
Muscles that work in opposition to each other (e g Muscles that work in opposition to each other (e.g., biceps and triceps) are called antagonistic muscles; muscles whose contraction results in the same movement are called synergistic muscles.

11/13/2009
37
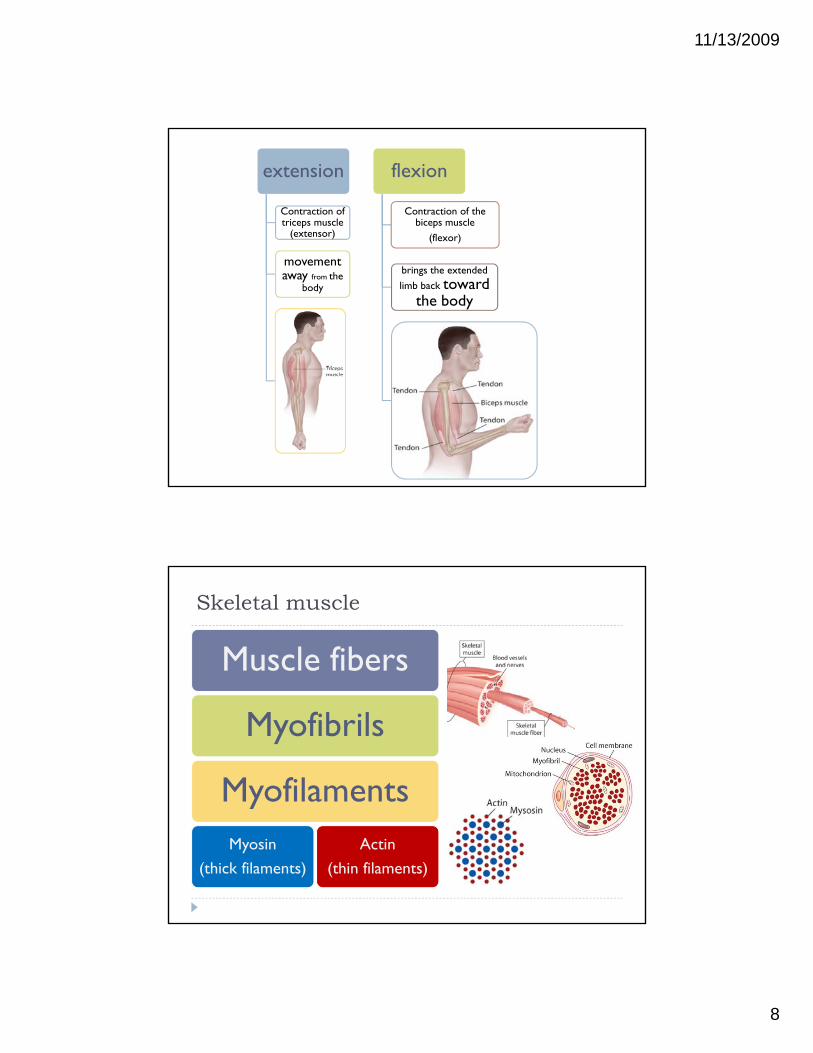
Muscle fibers—One of the units comprising a skeletal muscle; about 10 to 100 micrometers in diameter.
Myofibrils—One of the units comprising a muscle fiber; cylindrical structures about 1 to 2 micrometers across.
Myofilament—A component of a myofibril.
There are two kinds of myofilament in myofibrils: Myosin—The protein component of thick myofilaments. Actin—The protein component of thin myofilaments.
Sarcomere—The functional unit of a myofibril, consisting of overlapping bands of thick myosin filaments and thin actin filaments.actin filaments. This gives skeletal muscles a striped appearance, which is why
they are sometimes called striated muscles.

11/13/2009
38
Alpha motor neurons—Motor neurons with a long axon that leaves the ventral root of the spinal cord or b i d i h i di id l l fibbrain stem and synapse with individual muscle fibers. Their axons conduct information rapidly (220 m/second).
Extrafusal muscle fiber—A muscle fiber controlled by an alpha motor neuron.
Neuromuscular junction—A specialized synapse between an alpha motor neuron and an extrafusal
fmuscle fiber. Motor end plate—The flattened area of an extrafusal
muscle fiber where a motor neuron and the muscle fiber synapse.
The Motor Unit
Each branch of an axon synapses with a single muscle fiber.
Collectively, a motor neuron and the muscle fibers it controls form a motor unit (an alpha motor neuron and the muscle fibers it controls).
When the axon of an alpha motor neuron has few When the axon of an alpha motor neuron has few branches and controls only a few muscle fibers, fine motor control is possible.
When the axon has many branches and controls many muscle fibers, gross limb movement is possible.

11/13/2009
39
Muscle Adaptation
Different types of muscles facilitate diverse abilities: Slow-twitch muscle—A muscle fiber that contracts and fatigues
slowly; produces slower contractions that can be maintained for long periods of time without fatiguing.
Fast-twitch muscle—A muscle fiber that contracts and fatigues quickly; produces rapid contractions that tire quickly.
I t di t t it h l A l fib th t t t t Intermediate-twitch muscle—A muscle fiber that contracts at a lower rate than fast-twitch and a higher rate than slow-twitch muscles; produces contractions of moderate speed and duration.
We use primarily slow or intermediate-twitch muscles when we stand or walk; fast-twitch muscles when we run.
Reflex Control of Movement
Reflex—A simple, automatic response to a sensory stimulus.
Patellar reflex—A reflex in which tapping the tendon of the knee stretches one of the muscles that extends the leg, and the resulting muscle contraction causes h l ki k dthe leg to kick outward.
Most reflexes are produced by the spinal cord without involvement of the brain.

11/13/2009
40
Monosynaptic Stretch Reflex
Monosynaptic stretch reflex—A spinal reflex with a single synapse between the sensory receptor and the muscle effector. Muscle spindle—A structure embedded within an
extrafusal muscle fiber than enables the CNS to contract a muscle to counteract the stretching of the extrafusal
l fibmuscle fiber. Intrafusal muscle fiber—A muscle fiber that extends the
length of the muscle spindle that is surrounded by annulospiral endings (sensory receptors in the central part of the muscle fiber).
Monosynaptic Stretch Reflex
When the extrafusal muscle fibers are stretched, so are the intrafusal fibers; stimulates the annulospiral endings, causing them to fire more rapidly.
This increased neural activity travels along the Ia fibers (or axons) of the annulospiral endings, entering the dorsal
f h i l d d i i h l h root of the spinal cord and synapsing with alpha motor neurons.
The Ia fibers have an excitatory influence on alpha motor neurons, causing the extrafusal muscle fibers to contract.

11/13/2009
41
Primary Motor Cortex: Organization
Organization of the Primary Motor Cortex The movement of different body parts is elicited by
stimulation of different regions of the primary motor cortex. There is greater cortical representation of some body parts
than of others. Body parts that produce precise movements (e g hands and Body parts that produce precise movements (e.g., hands and
mouth) have greater representation than do parts that produce gross movements (e.g., arms and legs).