Embed Size (px)
Citation preview

Kameron Leigh Matthews MD JDChief Medical Officer, UI Health Mile Square Health Center
Associate Medical Director, UI Health PlusAssistant Professor of Clinical Family Medicine
University of Illinois at Chicago
The (Near) Future of Healthcare Delivery
What are ACOs, PCMHs, and Value-based Performance?
Disclosures
• No Financial Relationships

Objectives
• To define the “accountable care organization,” its associated models of payment and care delivery, and review an example of its implementation.
• To discuss the commonly adopted components of the Patient-Centered Medical Home and its impact on the achievement of improved patient outcomes.
• To describe trends in value-based purchasing (pay-for-performance) models and their impact on quality and efficiency measures.

Accountable Care Organizations
• An ACO is a network of doctors and hospitals that shares financial and medical responsibility for providing coordinated care to patients in hopes of limiting unnecessary spending.
• Formalized under the Affordable Care Act for Medicare entities
• Now implemented with Medicaid and commercial sector
• Modeled after Kaiser Permanente and Geisinger Health System.

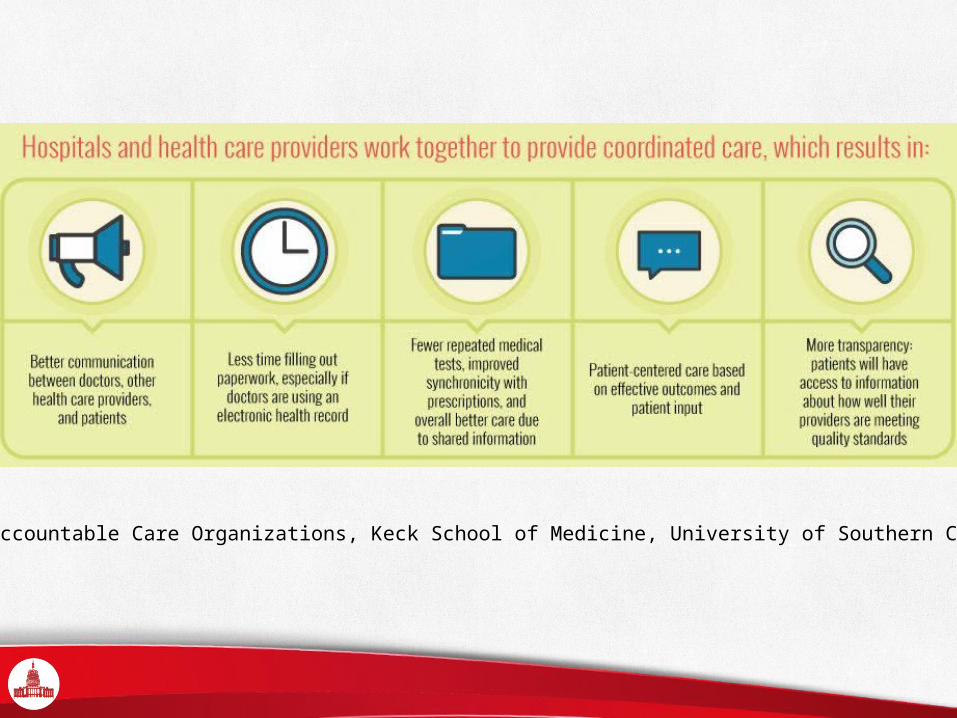
Source: Accountable Care Organizations, Keck School of Medicine, University of Southern California

ACOs - Key Elements
• Provider Led• Primary Care at the helm• Hospitals, Community Health Centers, specialists,
urgent care centers• Accountability for Patient Outcomes• Care Coordination and case management• Tied to payment
• Potential for shared savings• Reduced expenditures for a defined population by
diminishing the link between payments and volume and intensive of services provided

How Does It Work?
• Similarities to HMOs/capitated models?• Goal of cost savings• More focus on quality of care and population
health• Less focus on restrictions to utilization of health
care services• Larger groups of patients for risk distribution while
also making appropriate clinical decision making.

UI Health Plus - Illinois Accountable Care Entity

Patient-Centered Medical Home
• A health care delivery model that places the patient at the center of team-based care that is coordinated and proactively managed.
• Certification by National Committee for Quality Assurance (NCQA) or Joint Commission
• Standards with specific requirements and levels of accreditation.

PCMH Standards
• Patient-centered access and communication• Population health management through Patient
tracking and registry function• Care management and Patient self-management
support• Coordination including Test tracking and Referral
tracking• Performance measurement and quality improvement

PCMH Critical Factors• Same day appointments for routine and
urgent care• Timely clinical advice by telephone.• Patient care team meetings or other
structured communication process focused on individual patient care

PCMH Critical Factors• Clinical decision support for mental health
or substance use disorders• Monitoring of total patient population • Medication reconciliation and tracking• Registry tracking and “Closing the Loop”• Lab tests• Imaging• Referrals

Outcomes
• Consistent improvement of quality outcomes• Hoff, T.,W.Weller, and M. Depuccio. 2012. “The Patient-Centered
Medical Home: A Review of Recent Research.” Medical Care Research and Review 69: 619–44.
• Mixed results for multiple variables• ED visits• Inpatient admissions• Average length of stay• Costs/Medicare payments• Utilization of testing• Patient experience
May 2015

Outcomes
• Improvement also associated with higher risk patient populations• Chronic conditions
• Coles, ES, et al. Health Affairs. 2015; 34 (1): 87-94.• Van Hasselt, M. et al. Health Serv Res. 2015 Feb; 50 (1): 253-72
• Minimizes redundant care• Question remains as to whether a net costs savings is
associated with the model• Do any improvement in medical expenditures
outweigh the operating costs on the practice side?• Long term outcomes beyond time-limited studies

Herbert PL et al. “Patient-Centered Medical Home Initiative Produced Modest Economic Results For Veterans Health Administration, 2010-12” Health Affairs, 33, no.6 (2014):980-987
Patient Aligned Care Teams in the Veterans Health Administration accounted for a discounted investment through FY 2012 was $774 million (primarily for new personnel) and an additional $23 million for training. The investment was offset by an estimated $596 million in discounted costs of utilization that was avoided because of PACT, for a net loss of $178 million.

Value-Based Performance
• Payment for achievement of specific quality outcomes and care coordination goals
• Distinct from a fee-for-service model• Recommended by the Institute of Medicine
• "Rewarding Provider Performance: Aligning Incentives in Medicare". (2006) The National Academies Press.


Outcomes
• Mixed results for quality outcomes• Improvement in primary care settings
• Lemak CL et al. “Michigan's Fee-For-Value Physician Incentive Program Reduces Spending And Improves Quality in Primary Care”. Health Affairs, 34, no.4 (2015):645-652
• Poor evidence in hospitals• Slower spending increases• Annual savings
January 2014

Disparities in effects on disadvantaged patient populations• Provider organizations that serve lower income patient
populations typically have lower average quality performance and lower average PMPM quality incentive payments.• Lower initial capitation payments makes it difficulty for
low-performing providers to initiate the improvement efforts
• Redistribution of resources away from those organizations that need them most.
• Recommendation: stronger incentives for higher risk subgroups of patients.
Damburg CL et al. “Pay-For-Performance Schemes That Use Patient And Provider Categories Would Reduce Payment Disparities”. Health Affairs, 34, no.1 (2015):134-142

Summary
• Innovation in payment models is necessary to control health care costs
• Traditional models based on services do not impact quality outcomes
• Primary care plays a critical role to improving quality.• Models minimizing the divide between primary care
and specialty care provide continued hope for achieving the triple aim: improving quality of care, addressing the patient experience, while decreasing costs.