Embed Size (px)
Citation preview
THE NATIONAL MEDICAL JOURNAL OF INOlA VOL. S, NO.3. 145
Classics in Indian Medicine
C. GopalanDr C. Gopalan has spearheaded the campaign against undernutritionin India for nearly four decades. His contributions towards thecause of betterment of the nutritional status of the poor havebenefited India and other developing countries and have inspiredmovements for the eradication of undernutrition among them.
Nearly 40 years ago, after a brilliant academic career at theMadras Medical College leading to a Doctoral Degree in Medicine,Dr Gopalan was poised for a lucrative practice as a clinician.Around that time India was rocked by the worst famine in itshistory-the Bengal famine-in which several thousand peopledied of starvation. The impact of the famine moved Dr Gopalanto combat undernutrition among the poor.
He founded the National Institute of Nutrition in India in 1960and was its Director till 1974. The institute is now recognized tobe one of the best of its kind in the world and has made majorcontributions towards understanding nutritional problems affectingthe poor.
As Director-General of the Indian Council of Medical Research(1974-79), he provided a new orientation to medical research inthe country and encouraged investigation into problems on communi-cable diseases and those related to poverty and undernutrition.
Dr Gopalan initiated the series of Asian Congresses of Nutritionin 1970. He was primarily responsible for the formation of theFederation of Asian Nutrition Societies. He has also been Presidentof the International Union of Nutritional Sciences and was the firstChairman of the Regional Advisory Committee on Medical Researchfor South East Asia (WHO, SEARO).
Dr Gopalan's research contributions include over 200 papersand over a dozen books on nutrition.
He is a Fellow of the Royal Society. At present he is the Director-General of the Nutrition Foundation of India.
KWASHIORKOR AND MARASMUS:EVOLUTION AND DISTINGUISHING FEATURES
C.GOPALANNutrition Research Laboratories, Indian Council of Medical Research, Hyderabad
Reprinted from Calorie deficiencies and protein deficiencies. Edited by R. A. McCance and E. M. Widdowson. 1968:4~0.

146
Nearly 14 years ago, an international group ofscientists met in Jamaica to discuss what was thentermed the problem of "Protein Malnutrition". Inthese intervening years a great deal has beenwritten on the subject, but is evident that con-siderable controversy and confusion still surroundmany aspects of this problem.
An important step in our better appreciation ofthe problem in recent years is the recognition thatin all considerations of protein adequacy thequestion of calorie intake is of the utmost impor-tance. Professor Platt has forcefully reminded usof the old dictum that proteins and calories areclosely interdependent. He has deplored thetendency to equate the term kwashiorkor withprotein malnutrition, and has advocated theconcept of protein-calorie deficiency, whichwill include in its ambit such different clinicalsyndromes as marasmus and kwashiorkor andmarasmic kwashiorkor.
Protein-calorie deficiency leads to two distinctclinical syndromes-kwashiorkor and marasmus.In recent years there have been some extremelyelegant experimental studies which have con-vincingly shown how variations in the caloricintake modify and condition the effects of proteindeficiency. It has been now clearly demonstratedthat syndromes analogous to marasmus andkwashiorkor can be produced in experimentalanimals by appropriate dietary manipulations.
On the basis of experimental studies it has
TABLE I KWASHIORKOR AND MARASMUS: SALIENT FEATURES
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 5, NO.3
now been postulated that a deficiency of proteinwith adequate or more than adequate caloriesleads to kwashiorkor, while deficiency of caloriesleads to marasmus. The protein-calorie ratio inthe diet is held to be of crucial significance inthis regard. Some workers speak of a spectrum ofprotein-calorie malnutrition, one end of whichis represented by marasmus, and the other bykwashiorkor.
The application of experimental results to humansituations is often a difficult exercise and has to beattempted with considerable caution and cir-cumspection. The observations which I intend topresent pertain to poor Indian communitiesamong whom both marasmus and kwashiorkor arefrequently encountered. These observations willshow that the current hypotheses which seek toexplain the differential pathogenesis of marasmusand kwashiorkor, purely on the basis of differ-ences in the protein-calorie ratio in the diets inthese two states, do not meet all the facets of thesituation.
SALIENT DISTINGUISHING FEATURES
The clinical pictures of classical marasmus andclassical kwashiorkor are too well known torequire elaborate description here. In Table I, Ihave broadly outlined some differences in thebiochemical and pathological features of thesetwo states. The peak age-incidence of marasmus is
Marasmus Kwashiorkor
Age of maximal incidenceEmaciationOedemaFatty infiltration ofliverSkin changesSerum albuminSerum enzymes:
LipaseAmylaseEsterase
Serum lipids:Triglycerides NormalCholesterol NormalNon-esterified fatty acids Elevated
Blood sugar NormalResponse to epinephrine ExaggeratedSerum urea NormalCopper in serum NormalHaircopper NormalUrinary urea/total urine nitrogen Above 65%Increase in body weight after high protein
and calorie intake during the first4weeks
6-18 months+++AbsentOto ±InfrequentAlmostnormal
12-48months-r to + ++ to + + ++++FrequentMarkedly lowered
Normal Markedly loweredNormal LoweredSlightly lowered Lowered
Poor
NormalLoweredElevatedNormalLoweredLoweredLoweredLoweredBelow 50%
Satisfactory

CLASSICS IN INDIAN MEDICINE
generally lower than that of kwashiorkor though,apparently, this is not the case in Jamaica. Thereduction in serum protein and serum albuminlevels is of a somewhat lower order in marasmusthan in kwashiorkor. Serum lipase, amylase andesterase concentrations are better preserved inmarasmus than in kwashiorkor. Liver biopsiesreveal that the liver is more or less normal inmarasmus, in contrast to kwashiorkor wheremarked fatty change is a characteristic feature.Total 24-hour urinary nitrogen, as well as the ratioof urea nitrogen to total nitrogen, are significantlyhigher in marasmus than in kwashiorkor. Bloodurea and blood cholesterol are significantlyreduced in kwashiorkor as compared to marasmus.Non-esterified free fatty acid levels are, appa-rently, elevated in both conditions. Ferritin ispresent in serum in kwashiorkor, but not inmarasmus. My colleague, Dr. S. G. Srikantia, willdiscuss this observation in greater detail at a laterstage in this colloquium. The fasting blood sugarlevels are apparently normal in both conditions,but the response to epinephrine is poor in kwashi-orkor but not in marasmus.
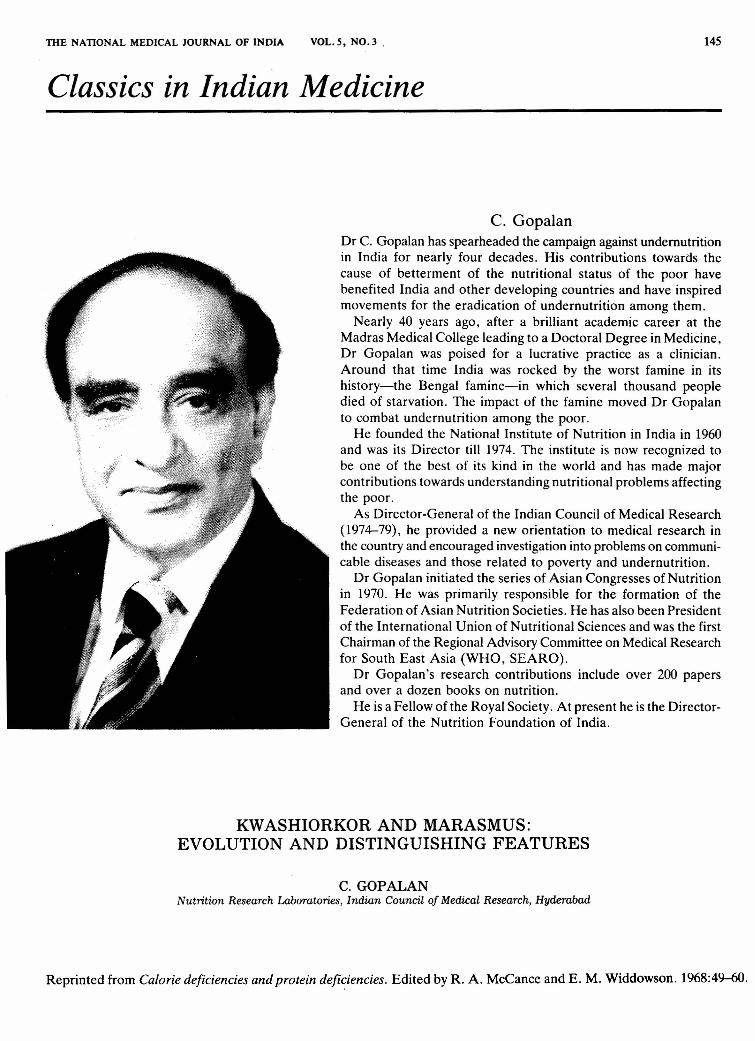
A comparison of the non-essential amino acidratios in marasmus and kwashiorkor, using theone-dimension chromatography technique ofWhitehead and Dean (1964), failed to reveal anyconsistent difference between the two conditions.The ratio was either normal, raised or lowered inkwashiorkor, and in some cases of kwashiorkorthe ratios actually increased after treatment (Fig.1). In marasmus the values did not appear to beraised. So we do not subscribe to the claim thatthis test is of diagnostic value. The alanine-glutamine ratio was low in kwashiorkor andincreased after treatment. The picture wasexactly opposite in the case of marasmus.
The total 24-hour hydroxyproline excretion inurine was reduced in cases of kwashiorkor. How-ever, the value, when expressed in terms ofcreatinine, was not significantly different from
8 111 r:__« " ---~ 9.,' <; _------- .• 1
~ -1· -; ---
~ ~ 7 .•....•
aJU i ...2(j)«5i .•.... .' .········/4~ ~ .•.•.......•...•.• --." .........•................... /.'"
0« 3-L ""'--. "~_"."5~~ j ----"."..- --..~-- .,.,....0- - '--. ."I-- -- • ...",QaJ 1~~a::w Ii' i I I
3
o 4 8 12 16 20 24 28 32DAYS OF TREATMENT
FIG.1. Non-essential/essential amino acid ratio infive children during treatment for kwashiorkor
147
that obtained in normal children. We are, there-fore, of the view that this reflects only changes inbody weight and does not indicate a specificchange in collagen metabolism.
Most of the differences between kwashiorkorand marasmus which I have listed above can bedirectly related to the central fact that in maras-mus the functional integrity of the liver is rela-tively better preserved than in kwashiorkor.
It will thus be clear that marasmus andkwashiorkor, in their classical forms, are twoclearly distinguishable syndromes. The importantquestion is whether they represent two distinctand different diseases with different aetiologicalbackgrounds and calling for different methods ofapproach with regard to prevention and control,or whether they represent two distinct facets ofthe same disease. Our observations bearing on thequestion of evolution and natural history of thesetwo syndromes, as they occur in our region, maythrow light on this question.
EVOLUTION
Conclusions as to the evolution of kwashiorkoror marasmus have generally been based on his-tories obtained from cases of kwashiorkor, or onanimal experiments. It is obvious that reliableinformation on the evolution of these states will bepossible only through field studies of com-munities among whom kwashiorkor and maras-mus are common.
Many of you here are aware of the extensive sur-vey of the incidence of protein -calorie deficiencywhich we carried out some years ago in four SouthIndian States (Someswara Rao et al., 1959). Thatsurvey revealed that among the poorest sections ofthe populations, 1-2 per cent of children of pre-school ages suffered from frank signs of'kwashior-kor at any given time. The incidence of frankmarasmus in the same community was twice ashigh. That survey, however, did not provide directinformation as to the evolution of these syn-dromes.
We have recently undertaken an intensive studyof a poor rural community. Nearly 2,000 childrenbelow 5years of age have been examined. In a rep-resentative sub-sample of this group, careful dietsurveys were carried out by trained investigators.The salient results of these studies have been setout in Table II.
A comparison of the weights ofthese children atdifferent ages with corresponding data for Ameri-can children shows the extent of growth retarda-tion in this group. The daily protein intake variedfrom 1.9g.zkg.in infancy to around 1.5g'/kg. in thefourth and fifth years. The protein was almost sol-ely derived from cereals (rice and/or millet) in thelater age group, while in the earlier age groupbreast milk contributed a significant proportion.In terms of "reference protein", therefore, the pro-

148 THE NATIONAL MEDICAL JOURNAL OF INDIA VOL.5, NO.3
TABLE II PROTEIN AND CALORIE INTAKES OF POOR SOUTH INDIAN CHILDREN
Age group Number Mean Reported Protein intake Calorie intakesurveyed weight normal
(kg.) American g'/24 hr. g'/kg./ kcal.! kcal./kg.weight (kg.) 24 hr. 24 hr. 124hr.
6-12 months 126 6.7 9.6 12.6 1.9 593 901-2 years 418 7.8 11.4 13.5 1.7 645 812-3 years 328 9.1 13.6 19.9 2.2 868 963-4 years 394 10.7 15.7 19.4 1.8 904 844-5 years 578 12.4 17.4 18.9 1.5 858 71
tein intake in the latter age group was about 1.0g.lkg. These figures would appear just adequate interms of actual body weights, but are clearly lowerthan the latest recommendations of the W.H.O'/F.A.O. Expert Group (1965),when expressed interms of "ideal body weight".
The daily caloric intake ranged from around 90kcal.!kg. body weight in the earlier age group toaround 80 kcal.!kg. in the later age group. Theseintakes are clearly less than the figure of 100--110kcal.!kg.,which is generally considered adequate.Thus, even on the basis of the actual body size ofthe children, the caloric intake must be consi-dered inadequate. In the light ofthese figures forcaloric intake the protein inadequacy of the dietsmust, in fact be considered to be greater than theprotein intake figures alone would indicate.
The calories obtained from protein accountedfor 8 per cent of total calories-a percentage thatcould be expected of dietaries which are almostsolely based on rice, wheat or millets.
Two salient features which emerge from theforegoing observations are: firstly, there is aremarkable attempt to restrict body growth to alevel which will be in keeping with the availabilityof protein and calories. Growth retardation inthese children is an attempt at adaptation to theprotein-calorie deficiencies; secondly, and this ismore important from the practical standpoint, themain bottleneck in the current dietary situation iscalorie inadequacy. An increase of about 30 percent in the intake of even cereal-based diets wouldnot only correct the calorie inadequacy but alsopromote a better utilization of dietary protein,without distorting the present protein-calorieratio. The prevailing picture of protein-caloriemalnutrition in these communities would therebybe considerably mitigated. It is essential toemphasize this point in these days of unceasingquest for protein concentrates and protein iso-lates.
Twenty-three frank cases of kwashiorkor wereseen among the group of 1,800children below 5years, giving a prevalence of 1.3 per cent. This issimilar to the prevalence rate of kwashiorkorobserved in our more extensive earlier survey.The number of cases of marasmus in this group
depends on the criteria employed. Practically allchildren in the community showed growth retar-dation associated with varying degrees of emacia-tion. Twoto three per cent of children showed par-ticularly severe degrees of emaciation and couldbe designated as cases of marasmus. The bodyweights of the children with kwashiorkor (afterdisappearance of oedema), and with marasmus,were nearly 60 per cent of the average weights forthe corresponding age groups in the community.
The important point I wish to emphasize here isthat the most careful investigations failed to showthat the dietary pattern of the children whodeveloped kwashiorkor or marasmus was qualita-tively different from those of other children in thecommunity. They had all subsisted on the sametype of cereal-based diets as the rest of the chil-dren in the community. The quantities consumedwere at the lower limits of the range of intakesobtaining in the community. In particular, we arein a position to state categorically that there wasno evidence whatsoever that the children whodeveloped kwashiorkor had been "force-fed" orthat their mothers had tended to "push" starchyfoods. On the contrary, we found that some ofthesechildren, for some weeks prior to the onset offrank kwashiorkor, had subsisted on even smallerquantities of the same cereal-based diets that theyhad previously taken. Thus, if there was anychange at all in the diet, it was in the direction offurther restriction of calories and proteins with-out any change in the protein-calorie ratio.
As far as this community was concerned, there-fore, the development of the two forms ofprotein-calorie malnutrition could not be explained onthe basis of the hypothesis: predominant caloriedeficiency-marasmus; predominant proteindeficiency with adequate or more than adequatecalories-kwashiorkor.
We have also made a longitudinal study of nearly300 children from birth for periods extending upto 3years. Ninety ofthese children have now beenfollowed up for over 3 years. These children alsobelonged to the same poor socio-economic group.They are visited at fortnightly intervals in the firstyear and at monthly intervals thereafter. Theobject of this study was to elucidate the natural

CLASSICS IN INDIAN MEDICINE
history of protein-calorie malnutrition in thecommunity and to assess the possible contributoryrole of dietary factors and infections in this pro-cess. Out of the 90children followed up for 3years,seven developed frank signs of kwashiorkorduring the study.
The dietary patterns of these children con-formed to the picture presented earlier; the dietin all cases could be considered protein-caloriedeficient. The growth was apparently satisfactoryup to about the fourth month; thereafter, thegrowth curve levelled off and varying degrees ofemaciation were found in all the children. Insome, the emaciation was so marked as to justifythe designation "marasmus". Some childrenshowed "moon face" and dyschromotrichia, a pic-ture which would correspond to what some work-ers call "pre-kwashiorkor"-a rather misleadingname, since these children on follow-up did notnecessarily develop kwashiorkor. Some childrendeveloped frank signs of kwashiorkor (Figs. 2 and3). The growth pattern and the dietary pattern ofthe children who developed kwashiorkor and ofthose who did not, were not materially different.There was no evidence that children whodeveloped kwashiorkor had been either force-fedor having a diet any different from that of otherchildren in the community. Five of the seven chil-dren who developed kwashiorkor had recurrentbouts of diarrhoea and dysentery for some days,resulting in loss of appetite and further restrictionof their diets. These children were fed their usualdiets but in smaller quantities. In one case anattack of chicken-pox preceded the developmentof kwashiorkor. In another, the development ofkwashiorkor was gradual and could not be attri-buted to any special factors.
These longitudinal studies again confirmed thatthere was no striking qualitative differences inthe dietary pattern or in the protein-calorie ratioof diets between cases of marasmus and kwashior-kor on the one hand and the undernourished chil-dren in the community on the other. It would seemthat cases-of marasmus and kwashiorkor were theend results of more severe degrees of the sametype of protein-calorie deficiency prevalent in therest of the community. .
In extensive nutrition surveys among commun-ities ofpoor children subsisting on almost uniformprotein-calorie-deficient diets, kwashiorkor,marasmus and "nutritional dwarfism" are oftenfound to coexist. It is our experience that in sucha malnourished community, roughly 1-1.5 percent of children below 5 years show evidence ofkwashiorkor, about 2-3 per cent are franklymarasmic and the rest show varying degrees ofgrowth retardation and emaciation. Further,marasmic children may develop kwashiorkor(marasmic kwashiorkor) and children withkwashiorkor may present the picture of marasmus
149
F. No. tcI
11
10
~ACEMOON FACE
HAIR OISCOLOURAnON
DYSENTERY,
MOTHER'SPREGNANCV
l' ~OREWEANING SUPPLEMENTARY
FEEDS
60 120 180 240 300 360 420 480 540 600 660 720 780 840 900 960 1020DAYS
FIG.2. Evolution of kwashiorkor in a child
\0MOON FACE AND
F. No. 1sa OISCOLOURATION Of HAIR
fMOTHER'S PREGNANCY
o 60 120 180 240 300 360 420 480 540 600 660 720 780 840DAYS
FIG. 3. Evolution of kwashiorkor in a second child
after shedding their oedema. Marasmus andkwashiorkor thus coexist in the same community.Marasmus and kwashiorkor can also be seen in thesame child while continuing on the same diet, atdifferent points of time.
It will thus be clear that marasmus andkwashiorkor, as they are seen in our area, are notthe same as experimental marasmus andkwashiorkor, induced by caloric deficiency orforce-feeding respectively. I am aware, however,that human counterparts of experimental "maras-mus" induced in animals through feeding low-calorie diets, and of experimental "kwashiorkor"induced through force-feeding protein-deficientdiets, exist in other situations. Marasmus has beenfrequently seen in children fed on small quan-tities of milk. It is also probable that Jamaicankwashiorkor, which has been reported to beassociated with a high caloric intake, and whosepeak age incidence has been claimed to be similarto marasmus (Garrow, 1966),may be looked uponas the human counterpart of "experimentalkwashiorkor" brought about by force-feeding. Iconsider, however, that the great majority of casesof kwashiorkor in India, probably in Indonesiaand possibly in the Middle East, cannot beexplained on this basis. We have necessarily toenlarge our concept of the pathogenesis ofkwashiorkor.
PATHOGENESIS OF KWASHIORKOR: A HYPOTHESIS
It may be expected that when a child is sub-jected to the stress of protein-ealorie deficiency

150
its tissues respond to the stress in a manner thatwould enable it to "adapt" itself to the deficiency.In fact, growth retardation and restriction of'phys-ical activity are obvious clinical manifestations ofsuch adaptation. The preservation of functionaland structural integrity of the liver may be consi-dered as yet another instance of adaptation. Thebiochemical mechanisms at the cellular levelwhich are involved in such adaptation and theprecise role of hormonal and other factorstherein, still require to be carefully elucidated.Waterlow (1959)has shown in experiments withlabelled amino acids that in animals on a low-protein diet, liver protein becomes more highlylabelled than in animals on a normal diet. In afurther extension of this work, Waterlow andStephen (1966)showed that the rat adapts itselftoa low protein diet by an alteration in the pattern ofprotein synthesis. They demonstrated that proteinturnover was "maintained at more or less normallevels in those organs which may be consideredmost essential for life at the expense ofthose suchas muscles and skin, which are less essential".Other biochemical evidence of such adaptation tolow-protein diets have also been provided byMariani, Spadoni and Tomassi (1963),who foundan increase in the activity of amino acid activatingenzymes in the liver of animals on protein-defi-cient diets.
Children in a poor community subsisting on pro-tein-calorie-deficient diets may be expected torepresent various stages of such adaptation,depending on the degree and duration of protein-calorie deprivation. "Nutritional dwarfism" maybe considered to represent the relatively mildereffects of such adaptation, while marasmus maybe considered to reflect the extreme effects of thatprocess, the farthest limit is what Garrow (1959)picturesquely called the "contraction of themetabolic frontiers".
As was pointed out earlier, the hormonal factorsinvolved in such adaptation are as yet unclear.Waterlow and Stephen (1966) have suggested apossible role of insulin. Platt, Heard and Stewart(1964)have adduced evidence of decreased insu-lin activity in young pigs on a protein-calorie-defi-cient diet. The results of studies on cortisol levelsin kwashiorkor are apparently conflicting.Pimstone and co-workers (1966) have reportedraised growth hormone levels in kwashiorkor. Onthe other hand, Monckeberg and co-workers (1963)obtained good response in cases of marasmusafter injection of growth hormone and suggestedthat in this syndrome there is an endocrine-con-trolled adaptation to the shortage of food. Themetabolic adjustments geared to protect the liver-in marasmus at the expense of muscle are shownby the observation that it is extremely difficult toget a marasmic child under treatment to put onweight.
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 5, NO.3
It may be postulated that there may sometimesbe a failure of adaptation. Kwashiorkor may beconsidered such a failure of adaptation. Thebiochemical mechanisms which are usuallyinvoked to protect the essential tissues like theliver, pancreas and intestines at the expense ofless essential muscle, have failed; functional andstructural damage to the liver follows, and thesigns and symptoms of kwashiorkor which arelargely attributable to this become evident.
What are the factors that bring about suchdysadaptation? One may postulate that force-feed-ing or the administration of excess calories in theface of protein deficiency may be one such factor.This will explain "experimental kwashiorkor"induced by force-feeding and the Jamaicankwashiorkor associated with excessive caloriesand unaccompanied by emaciation. On the otherhand, dysadaptation may also be brought about bya sudden further exaggeration or by continuedprolongation of the stress of protein-calorie defi-ciency. This sequence will explain thepathogenesis of cases of kwashiorkor as seen inour country. Most of the cases of kwashiorkor hereare likely to be cases of marasmic kwashiorkorassociated with a considerable degree of musclewasting and emaciation.
It may be expected that in a poor communityexposed to the stress of'protein-calorie deficiencythe great majority of the children will need todevelop a mild degree of adaptation (nutritionaldwarfism), but a considerable number will showthe extreme results of adaptation (marasmus) anda small number will show the effects of dysadapta-tion (kwashiorkor). This is generally the picturewhich is seen in poor Indian communities.
Though this hypothesis would appear to belargely based upon circumstantial evidence, Iwould like to mention some experimental resultsthat lend support to it. It has been shown byRamalingaswami, Deo and Sood (1961)that "ex-perimental kwashiorkor can be induced in mon-keys in a matter of a few weeks by force-feedingthem a protein-deficient diet". On the other hand,we had shown earlier (Srikantia and Gopalan,1959)that kwashiorkor can be induced in monkeyswithout force-feeding, provided the animals aremaintained for prolonged periods of time on pro-tein-calorie deficient diets. The details of thisstudy will be presented later in this colloquium byDr Srikantia.
We have shown that marasmic children havelevels of plasma cortisol significantly higher thanthose in children suffering from kwashiorkor (un-published data), and we have also observed thatthe administration of cortisol to monkeys force-fed low protein diets postpones considerably thedevelopment of fatty livers. More clinical andexperimental studies are obviously necessarybefore the validity of this "adaptation" hypothesis

CLASSICS IN INDIAN MEDICINE
is established. We have some studies under way toexamine these aspects of the problem.
REFERENCESGarrow, J. S. (1959). J. CUn. Invest., 38,1241.Garrow, J. S. (1966). Lancet, 2, 592.Mariani, A., Spadoni, M. A., and Tomassi, G. (1963). Nature,
Lond., 199,373. -Monckeberg, F., Donoso, G., Oxman, S., Pak, N., and Meneghello,
J. (1963). Pediatrics, 31, 58.Pimstone, B. L., Wittmann, W., Hansen, J. D. L., and Murray, P.
(1966). Lancet, 2, 779.Platt, B. S., Heard, C. R. C., and Stewart, R. J. C. (1964). In
Mammalian Protein Metabolism, vol. 2, p. 446, eds. H. N. Munroand J. B. Allison. New York and London: Academic Press.
Ramalingaswarni, V., Deo, M. G., and Sood, S. K (1961) In Meet-ing Protein Needs oflnfants and Children, p. 365. N atn. Acad.ScL Washington, D.C.
Someswara Rao, K, Swaminathan, M. C., Swarup, S., andPatwardhan, V. N. (1959). Bull. Md. Hlth. Orq., 20, 603.
Srikantia, S. G., and Gopalan, C. (1959). J. Appl. Physiol., 14,828.Waterlow, J. C. (1959). Nature, Lond., 184, 1875.Waterlow, J. C., and Stephen, J. M. L. (1966). Br. J. Nutr., 20, 461.Whitehead, R. G., and Dean, R. F. A. (1964). Am. J. Clin. Nutr.,
14,313.W.H.O.IF.A.O. (1965). Report of a Joint F.A.O.IW.H.O. Expert
Group on Protein Requiremtns, Tech. Rep. Ser. Wid. Hlth.Org. No. 301.
151
This paper, published nearly a quarter of a century agoand still widely quoted, had a very important influence onall of us working on childhood malnutrition. After 1935,when Williams described the development of kwashiorkorin a west African child displaced from the breast by a newbaby and put to feed on starchy paps, most of us believedthat the underlying cause of the syndrome was proteindeficiency. In the minds of many this belief was elevatedto the status of a' dogma, according to which protein wasthe most important limiting factor in the diets of ThirdWorld children. Consequently, an enormous amount oftime and money was devoted to the development of protein-rich supplements for young children. To the world at largethe scientific validity of this policy appeared to be guaranteedby the support that it received from the Protein AdvisoryGroup of the United Nations.
Gopalan 's paper showed very clearly that the theoreticalbasis of this activity was untenable, although he was carefulto caution against generalizing to the world as a wholefrom his results in India. His was the first community studyinvolving a population of children large enough to producea number of cases of kwashiorkor and marasmus. Up tothat time almost all the work on these conditions had beenhospital-based and little attention had been given to theirevolution and natural history. Measurements of food intakeshowed that the cereal-based diet of these village childrenwas marginally deficient in both energy and protein by the
standards current at that time. Moreover-and this is thekey point-there was no difference, quantitatively orqualitatively, in the diets of the children who developedkwashiorkor on the one hand and marasmus on the other.
The hypothesis that kwashiorkor represents a break-down of adaptation does not take us very much furtherbecause, in my opinion, a marasmic child can hardlybe regarded as adapted. However, that is a question ofterminology; the important point of principle that emergedfrom Gopalan's study was that the different clinical picturesare to a large extent determined by differences in the hostresponse rather than in the nutritional environment. Suchan interpretation is consistent with the well recognizedvariability in the energy and protein requirements ofindividual children, although the basis of this variability isstill unknown.
This paper of Gopalan's, therefore, had an impact inthree ways: it showed the artificiality of regarding mal-nutrition, as it evolves in a community, as a single-factordisease; it restored the balance when the pendulum hadswung too far towards exaggerating the importance ofprotein; and it displayed the dangers of basing public healthpolicy on inadequate scientific evidence.
J. c. WATER LOW
London School of Hygiene and Tropical MedicineLondon, UK