Embed Size (px)
Citation preview

The Narcotic Epidemic: Our
Response
Ronald E. Delanois, M.D.
Nicole E. George, D.O.
Jennifer I. Etcheson, M.D., M.S.
Chukwuweike U. Gwam, M.D.

• History of the opioid problem
– Nationally
– Statewide (Maryland)
– Institutionally (Sinai Hospital)
• Orthopaedics & the opioid
epidemic
• Opioid Rx at Sinai Hospital
• Sinai Hospital: addressing the
opioid problem
– Pre-/Peri-operative
– Intra-operative
– Post-operative
Outline

• 2005: national market campaign
to eliminate pain
– Based on the premise that physicians
are not treating pain adequately
• 2010: CMS established Value-
Based purchasing
– Value tied to patient perception of
care (HCAHPS)
– Pain control major component of
HCAHPS
• Providers ↑↑↑ opioid prescriptions
• Opioid epidemic
History of the Problem

• Drug overdose deaths in
the U.S. have tripled
since 2000
– 52,404 drug overdose
deaths in 2015
• Opioid-related overdoses
accounted for 63.1% of
these deaths
– 33,091 opioid-related
overdose deaths in 2014
– ~50% involved
prescription opioids
• Prescription opioid
addiction costs the U.S.
economy $78.5
billion/year
U.S. Opioid Epidemic

Opioid Epidemic in Maryland

• Orthopaedic surgeons
rank 3rd with respect to
writing opioid
prescriptions.
• Account for 7.7% of opioid
prescriptions among all
U.S. physicians.
– #1= PCPs (28.8%)
– #2= Internists (14.6%)
Opioids in Healthcare

• Patient-controlled analgesia (PCA)
– Intravenous or epidural
– Morphine, fentanyl,
hydromorphone
• Opioid Medications
– Short-acting (i.e. morphine,
fentanyl, oxycodone IR,
hydromorphone)
– Long-acting (i.e. Oxycontin)
How Was Pain Historically Controlled in
Orthopaedics?

• 20-30 Rx/day x 12
months
• 4800-7200 Rx/year
• 90 pills/Rx
Narcotic Prescriptions at Sinai
Hospital: 2014

• 2014: Sinai Hospital/RIAO sought to ↓ opioid
prescribing
– How do patients rate their pain?
– What other modalities can be utilized to ↓ postop pain?
What is Sinai Hospital Doing to
Combat the Opioid Epidemic?

1. Questionnaire (to identify
patients at risk of opioid
addiction)
2. Patient education
3. 90-day pain contracts with
patients
4. Staff education
5. Care coordination
6. Partnerships with PCPs &
pain management providers
7. Premedication
Sinai Hospital: Addressing the Narcotic Problem
(Pre-operative)

• Preoperative total joint
education class
• Education on the consequences
of opioid misuse & opioid
addiction
Patient Education

• Implemented to identify
patients at risk for opioid
addiction
Questionnaire

• In order for patients to receive
preoperative and postoperative
opioids for pain control
• Establishes
– Rapport
– Plan of care
– Consequences
• Patients must follow rules or
opioid prescribing ceases
Pain Contracts
• Standardized pain
protocol
• Frequent pain
assessments
• Pain medication
administered based on
pain scores (vs.
scheduling the pain
meds)
Staff Education

• Care coordination team
– 1 patient educator
– 4 nurses
• 1 nurse is designated as the
nurse navigator
• Surgery scheduler
• Orthopaedic surgery team
• Floor supervisor RN
Care Coordination

• Primary care physicians
• Physical therapists
• Anesthesiology team
• Pain control specialists
Partnerships with Other Providers

• To decrease postoperative
opioid requirements
• Regimen consists of:
– Gabapentin
– Celebrex
– Oxycodone IR (5mg)
Premedication
1. Opioid-sparing approach
2. Multimodal pain control
Sinai Hospital: Addressing the Narcotic Problem
(Intra-operative)

• Shift in pain control
method from:
– General anesthesia→
– Spinal anesthesia→
– Peripheral nerve blocks &
adjuvant agents
• Opioids & patient
experience
– Press-Ganey survey scores
related to patient pain scores
Opioid-Sparing Analgesia

• Acetaminophen
• NSAIDs
• Local anesthetics
• GABA agents
• Muscle relaxants
• Others
– Anticonvulsants
– Antidepressants
– Antihistamines
– Psychostimulants
– Anti-spasmodics
Premedication/Adjuvant Pain Control

• Randomized-control trial
– 140 patients undergoing primary unilat. total knee arthroplasty (TKA)
– Local infiltration analgesia (LIA) ± liposomal bupivacaine (LB)
• Endpoints
– Pain scores
– Opioid consumption
– Time to first opioid rescue
– Patient safety
• LIA with LB resulted in significantly improved postop pain, opioid
consumption, & time to first opioid rescue
• No unexpected safety concerns with use of LB
Multimodal Pain Control: Exparel

Multimodal Pain Control: Adductor Canal Block
• Adductor canal block (ACB)
– A peripheral nerve block
– Low incidence of complications
– Excellent pain relief
• Retrospective review
– 110 patients undergoing TKA
– Multimodal periarticular analgesia (MPA) ± ACB
– Pts who received both MPA and ACB had shorter LOS (2.44 vs. 1.98
days)

• NSAIDs
– Celebrex
– Diclofenac vs. ketorolac
• Spinal anesthesia
• Gabapentin
Multimodal Pain Control: Others

1. Interdisciplinary
partnerships
2. HealthLoop
Sinai Hospital: Addressing the Narcotic Problem
(Post-operative)

• Orthopaedic
surgeons
• Anesthesiologists
• PM&R specialists
• PCPs
• Nurses
• Pharmacists
• Social workers
Interdisciplinary Partnerships

• Interactive patient-provider
software platform
• Total joint arthroplasty patients
– Enrolled 14 days prior to surgery
– Continues through 21 days post-
surgery
• 97% patient enrollment at Sinai
Hospital
Patient Engagement Tool

• Nationwide, orthopaedists have
decreased opioid prescribing by 13.4%
from 2014 to early 2017.

• 2014:
– 20-30 Rx/day x 12 mos
– 4800-7200 Rx/year
– 90 pills/Rx
• 2017:
– 1-2 Rx/day x12 mos
– 240-480 Rx/year
– 60 pills/Rx
– ↓↓ # opioid Rx by
22.5x (2250%) since
2014
Narcotic Prescriptions at Sinai
Hospital: How Have We Done?

• Rudd RA, Seth P, David F, Scholl L. “Increases in Drug and Opioid-Involved
Overdose Deaths— United States, 2010-2015.” Weekly. December 2016: 65(50-
51);1445–1452. <https://www.cdc.gov/mmwr/volumes/65/wr/mm655051e1.htm>.
• Schuchat A, Houry D, Guy Jr. G. “New Data on Opioid Use and Prescribing in the
United States.” JAMA. 2017;318(5):425-426.
<https://jamanetwork.com/journals/jama/fullarticle/2643332>.
• Gostin LO, Hodge JG, Noe SA. “Reframing the Opioid Epidemic as a National
Emergency.” JAMA. 2017;318(16):1539-1540.
<https://jamanetwork.com/journals/jama/fullarticle/2652445>.
• Edlund MJ, Martin BC, Russo JE, DeVries A, Braden JB, Sullivan MD. “The role of
opioid prescription in incident opioid abuse and dependence among individuals with
chronic noncancer pain: the role of opioid prescription.” Clin J Pain. 2014
Jul;30(7):557-64.
References

• Pts with chronic non-cancer-related pain who took
opioids for >90 days (even at low doses) have a
substantially higher odds (O.R., 14.92) of developing
opioid use disorder compared with those who were
not prescribed opioids.
Orthopaedics & the Opioid Epidemic

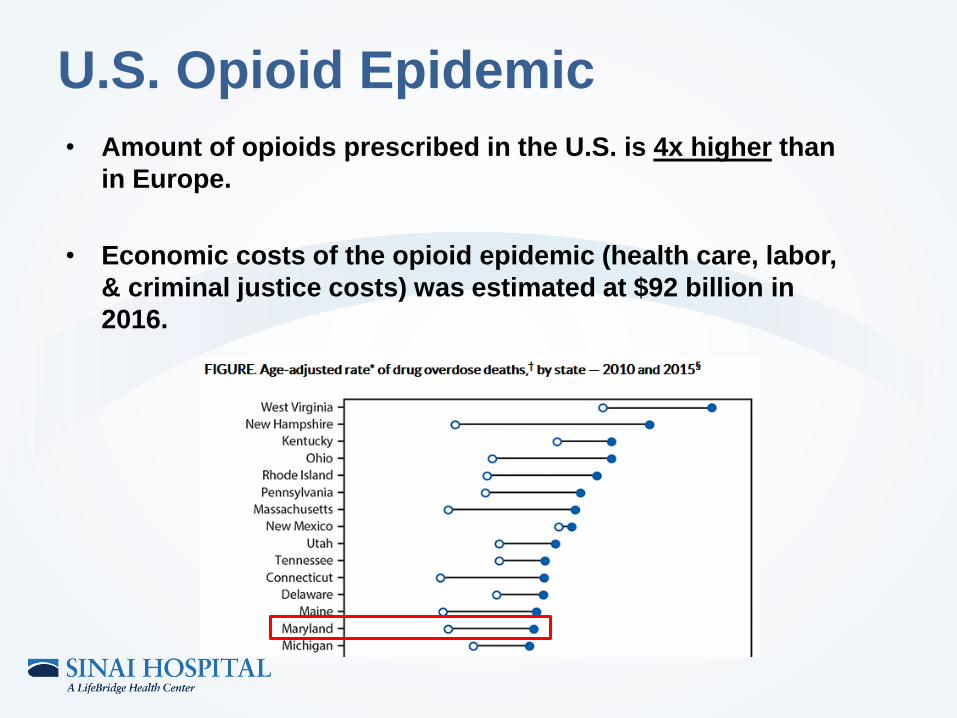
• Amount of opioids prescribed in the U.S. is 4x higher than
in Europe.
• Economic costs of the opioid epidemic (health care, labor,
& criminal justice costs) was estimated at $92 billion in
2016.
U.S. Opioid Epidemic

The Opioid Epidemic in Maryland
• In 2011, Maryland
declared a public health
emergency due to the
opioid epidemic.
• In the first 8 months of
2016, there were 1,468
opioid-related overdose
deaths.

Total number of drug- and alcohol-related intoxication
deaths by selected substances, Maryland 2007-2016
The Opioid Epidemic in Maryland

The Opioid Epidemic in Maryland
Number of Opioid-Related Deaths Occurring
in Maryland from January through March of
Each Year
Number of Prescription Opioid-Related
Deaths Occurring in Maryland from January
through March

2014
No.
(Rate)
2015
No.
(Rate)
% change in
rate
(2014 to 2015)
Natural & semi-synthetic opioids 388 (6.2) 398 (6.5) +4.8%
Methadone 153 (2.4) 182 (2.9) +20.8%
Synthetic opioids (other than
methadone)
230 (3.8) 357 (5.8) +52.6%
Heroin 313 (5.2) 405 (6.6) +26.9%
Number and rate of drug overdose deaths in Maryland, 2014 & 2015





























