Embed Size (px)
Citation preview

Journal of Plastic, Reconstructive & Aesthetic Surgery (2014) 67, 1669e1679
The myocutaneous trapezius flap revisited:A treatment algorithm for optimal surgicaloutcomes based on 43 flap reconstructions
Anil Can a,b, Dennis P. Orgill b, J.O. Dietmar Ulrich c,Marc A.M. Mureau a,*
a Department of Plastic and Reconstructive Surgery, Erasmus MC, University Medical CenterRotterdam, Rotterdam, The Netherlandsb Division of Plastic and Reconstructive Surgery, Brigham and Women’s Hospital, Harvard MedicalSchool, Boston, MA, USAc Department of Plastic and Reconstructive Surgery, Radboud University Nijmegen Medical Center,Nijmegen, The Netherlands
Received 2 March 2014; accepted 29 July 2014
KEYWORDSTrapezius;Myocutaneous flap;Treatment algorithm;Surgical outcome
* Corresponding author. Department2040, 3000 CA Rotterdam, The Nether
E-mail address: m.mureau@erasmu
http://dx.doi.org/10.1016/j.bjps.2014.01748-6815/ª 2014 British Association of P
Summary Background: Because the vascular anatomy of the trapezius flap is highly variable,choosing the most appropriate flap type and design is essential to optimize outcomes and mini-mize postoperative complications. The aim of this study was to develop a surgical treatmentalgorithm for trapezius flap transfers.Methods: The medical files of all consecutive patients with a myocutaneous trapezius flapreconstruction of the head, neck, and upper back area treated at three different universitymedical centers between July 2001 and November 2012 were reviewed.Results: There were 43 consecutive flaps performed in 38 patients with a mean follow-up timeof 15 months (range, 1e48 months). Eleven patients had a mentosternal burn scar contracture(12 flaps), 12 patients (13 flaps) presented with cancer, and 15 patients (18 flaps) weresuffering from chronic wounds due to failed previous reconstruction (n Z 6), osteoradionecro-sis (n Z 1), chronic infection (n Z 3), bronchopleural fistula (n Z 3), and pressure sores(nZ 2). The mean defect size was 152 cm2. Sixteen flaps were based on the superficial cervicalartery (SCA; type 2), 16 were based on the dorsal scapular artery (DSA; type 3), one was basedon the intercostal arteries (type 4), and 10 flaps were based on both the DSA and SCA.Recipient-site complications requiring reoperation occurred in 16.3%, including one total flapfailure (2.6%).
of Plastic and Reconstructive Surgery, Erasmus MC, University Medical Center Rotterdam, PO Boxlands. Tel.: þ31 10 703 4638; fax: þ31 10 703 2693.smc.nl (M.A.M.Mureau).
7.044lastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved.

1670 A. Can et al.
Conclusions: The trapezius myocutaneous flap is a valuable option to reconstruct various headand neck and upper back defects. Based on our data, a surgical treatment algorithm was devel-oped in an attempt to reduce variation in care and improve clinical outcomes.ª 2014 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Introduction
Although there is ample experience with reconstruction ofextensive head and neck defects after oncologic resections,trauma, and burns, it still remains a challenge to achieveacceptable functional and esthetic results. Over the pastyears, free tissue transfer has come forward as a highlyreliable and first-choice method to repair most complexhead and neck defects.1 However, if reconstruction in-volves external skin defects, the use of locoregional flaps isaesthetically preferable to free flaps because of theircloser similarity in skin color, texture, and thickness.1e3 Inaddition, sometimes the use of free flaps is contraindicateddue to significant preoperative comorbidity, previous sur-gery, or radiation therapy, which considerably increases therisks of postoperative complications.1
The pectoralis major myocutaneous pedicled flap isconsidered the regional “workhorse” flap for head and neckreconstruction.4 Recently, however, there has been arevival of interest in the pedicled trapezius flap, which hasproven to be a valuable alternative for the reconstructionof various head and neck defects. Four different types oftrapezius flaps have been described in literature: the su-perior, the lateral island, the vertical, and the lower island(posterior) muscle or myocutaneous flap.5e8 The trapeziusmyocutaneous flap is an easy to harvest, thin, reliable,well-vascularized, and large flap located far away from thearea involved, allowing a wide arc of rotation. Further-more, the flap can be extended with the use of a tissueexpander, providing a thin, large, and pliable skin islandwith excellent functional and aesthetic outcomes.9
Because the vascular anatomyof the trapezius flap is highlyvariable, choosing themost appropriate flap type and design isessential to optimize outcomes and minimize postoperativecomplications. The purpose of this article is to describe asurgical treatment algorithm for trapezius flap transfers,based on clinically relevant parameters. This will help recon-structive surgeons to select themost appropriateflap typeanddesign for various external skin defects in the head and neckarea, with the ultimate aim to improve clinical outcomes.
Patients and methods
Patient characteristics
This study is a retrospective review of three academiccenters (Erasmus MC, Rotterdam, The Netherlands; Uni-versity Hospital Aachen, Germany; and BWH, Boston, MA,USA). From July 2001 to November 2012, 38 consecutivepatients underwent 43 trapezius flap reconstructions. In
one 5-year-old girl without any risk factors, a plannedtransfer of the trapezius flap was aborted due to infectionof a previously placed submuscular tissue expander.Consequently, she was excluded from this study.
The hospital records of all these patients were reviewedretrospectively and patient characteristics, operative de-tails, and follow-up data were recorded in a standardizedform (Table 1). After data evaluation, a surgical treatmentalgorithm was developed based on defect size, localization,previous treatment, and complexity.
Flap anatomy
The anatomy of the trapezius muscle has been previouslydescribed in detail.6,10e12 It is a large and thin muscle, witha unique triangular shape and substantial length. It origi-nates from the medial third of the superior nuchal line ofthe occipital bone, the external occipital protuberance,the ligamentum nuchae, the spinous processes of the sev-enth cervical vertebra, and all the thoracic vertebrae, andinserts into the lateral third of the clavicle, the medialborder of the acromion, and the entire length of thescapular spine.6 The muscle suspends the shoulder girdleand assists in raising and rotating the shoulder. It is inner-vated by the accessory nerve.
According to the findings of Haas and Weiglein, there areat least two dominant pedicles: the superficial branch ofthe transverse cervical artery (superficial cervical artery:SCA) and the deep branch of the transverse cervical artery(dorsal scapular artery: DSA), and some minor pedicles (theoccipital artery and the intercostal perforators).10 Theanatomy of the transverse cervical artery (TCA) and theDSA in the posterior triangle is highly variable. The TCAenters the trapezius muscle at the base of the neck anddescends vertically along the deep surface of the trapeziusmuscle. It arises directly from the thyrocervical trunk in themajority of cases and runs across the posterior triangle ofthe neck where it divides into a superficial branch (SCA),which crosses over the levator scapulae, and a deep branch(DSA), which runs deep to the levator scapulae with itsmajor branch penetrating between the rhomboid muscles.The SCA gives rise to a descending and an ascending branch,which supply the upper and lower portions of the trapeziusmuscle, respectively.10 Figure 1 shows the vascular anat-omy of the trapezius muscle and depicts the wide range ofvarious trapezius flap classifications in the literature.
Surgical techniques
Four different trapezius myocutaneous flaps have beendescribed in the literature: the superior trapezius, the

Table 1 Patient, treatment, and follow-up details of 38 cases treated with 43 myocutaneous trapezius flaps.
Patient details Treatment details Follow-up details
Case Age,sex
Indication Defect location Flap type (V/T) Flap Size(cm2)
RT Complication,reoperation or tumorrecurrence
Follow-up(months)
1. Oncology
5 31, F Osteosarcoma 6th rib R(chest wall)
SCA þ DSA-V 12 � 4 No MRSA infection,empyema, reoperation
5
12 58, M Nerve sheath tumor T8-9 (chest wall) SCA þ DSA-V 12 � 4 Preop Metastasis, reoperation 1024-R 82, M SCC metastasis Posterior neck Type 3 DSA-V 4 � 8 No None 2925-L 82, M SCC metastasis Posterior neck Type 3 DSA-V 5 � 5 No None 2929 59, M Microcystic adnexal
carcinomaPosterior scalp Type 3 DSA-V 12 � 7 No Hematoma, reoperation 10
4 92, M SCC recurrence Vertex Type 3 DSA-V 20 � 12 Pre- andpostop
Wound infection,reoperation
2
6 68, M Sarcoma recurrence Supraclavicular L Type 2 SCA-T 5 � 4 Preop None 3611 47, F Sarcoma recurrence Paraspinal T4-5 Type 3 DSA-V 20 � 5 No None 113 74, M SCC recurrence Preauricular L Type 2 SCA-V 22 � 10 Preop Reoperation (to improve
outcome)6
16 42, M BCC recurrence Posterior neck R Type 3 DSA-VY 25 � 15 No Reoperation (to improveoutcome)
41
17 67, M Sarcoma recurrence Upper back L Type 3 DSA-V 8 � 6 Pre- andpostop
Wound infection,reoperation, tumorrecurrence
11
21 77, M SCC recurrence Temporal L Type 3 DSA-V 20 � 13 Preop Reoperation, tumorrecurrence
8
27 83, M SCC recurrence Ear R Type 3 DSA-V 11 � 13 No Urosepsis 1 (D)2. Chronic wounds
3 55, V Breakdown LD flap Mandible L Type 3 DSA-V 18 � 5 Preop Reoperation (to improveoutcome)
25
19-R 79, F Necrosis LD flap Spine T4-T6 Type 4Intercost.perf.
12 � 4 Preop Metastasis of lungcarcinoma
1
20-L 79, F Necrosis LD flap Spine T4-T6 SCA þ DSA-V 12 � 4 Preop Metastasis of lungcarcinoma
1
23 63, M Partial necrosisCP flap
Ear L Type 3 DSA-V ? Preop Hematoma, reoperation 32
26 66, M Dehiscence SC flap Mastoid L Type 3 DSA-V 30 � 7 Preop Hematoma, paresis n VII,dehiscence, reoperation
8 (D)
30 55, V Infection PM flap Neck L Type 2 SCA-V 14 � 8 Preop Total flap necrosis,reoperation
4 (D)
31 79, M Necrosis SC flap Face R Type 3 DSA-V 9 � 6 No None 11
22 40, F Osteoradionecrosis Post. neck Type 3 DSA-V ? Preop None 8
1 60, M Chronic infection L post. neck Type 3 DSA-V 12 � 5 Pre- andpostop
Metastasis of melanoma 1
10 41, M Chronic infection Sub-occipitaloccipital
Type 2 SCA-V 12 � 4 Preop Hematoma 1
14-R 70, M Chronic infection Back T2 SCA þ DSA-V 12 � 4 Preop Seroma donor-site,reoperation
12
15-L 70, M Chronic infection Back T2 SCA þ DSA-V 12 � 4 Preop Reoperation 12
2 61, M Bronchopleuralfistula
L post. Thorax(5/6 rib)
SCA þ DSA-V 15 � 4 No None 1
9 68, F Bronchopleuralfistula
Post Back L SCA þ DSA-V 12 � 4 Preop None 9
18 50, F Bronchopleuralfistula
Back L(med.scapula)
SCA þ DSA-V 12 � 4 Preop Recurrentbronchopleural fistula,reoperation
24
7-R 54, M Chronic pressure sore Midback SCA þ DSA-V 12 � 4 No None 38-L 54, M Chronic pressure Midback SCAþDSA-V 12 � 4 No None 3
(continued on next page)
Trapezius flap treatment algorithm 1671

Table 1 (continued )
Patient details Treatment details Follow-up details
Case Age,sex
Indication Defect location Flap type (V/T) Flap Size(cm2)
RT Complication,reoperation or tumorrecurrence
Follow-up(months)
sore28 73, V Chronic pressure
soreOccipital Type 3 DSA-V 19 � 8 No Necrosis donor-site,
reoperation6
3. Postburn
32 21, M Scar contracture Axilla L Type 2 SCA-V,pre-expanded
49 � 15 n/a Dehiscense donor-site 3
33 5, M Scar contracture Mentosternal Type 2 SCA-V,pre-expanded
30 � 10 n/a None 48
34 39, F Scar contracture Mentosternal Type 2 SCA-V,pre-expanded
26 � 10 n/a None 43
35 51, F Scar contracture Mentosternal Type 2 SCA-V 32 � 11 n/a None 3836 64, M Scar contracture Mentosternal Type 2 SCA-V 28 � 11 n/a None 3537-R 37, F Scar contracture Mentosternal Type 2 SCA-V,
pre-expanded27 � 11 n/a Hematoma 26
38-L 37, F Scar contracture Mentosternal Type 2 SCA-V,pre-expanded
27 � 11 n/a None 26
39 31, M Scar contracture Mentosternal Type 2 SCA-V 25 � 9 n/a None 2640 6, F Scar contracture Mentosternal Type 2 SCA-V,
pre-expanded24 � 8 n/a Scar contracture,
reoperation22
41 7, M Scar contracture Mentosternal Type 2 SCA-V,pre-expanded
26 � 9 n/a None 18
42 6, F Scar contracture Mentosternal Type 2 SCA-V,pre-expanded
23 � 8 n/a None 15
43 8, F Scar contracture Mentosternal Type 2 SCA-V 22 � 7 n/a None 14
V, Vertical. T, Transverse. L, Left. R, Right. BCC, basal cell carcinoma. SCC, squamous cell carcinoma. LD, Latissimus Dorsi. CP, Cer-vicopectoral. SC, Supraclavicular. PM, Pectoralis Major. (D), Deceased. n/a, not applicable. ?, unknown.
1672 A. Can et al.
lateral island trapezius, and the vertical and the lowertrapezius island myocutaneous flap (LTIMF).5e8 However,classifying flaps by their vascular pedicle and categorizingthem into vertical or transverse flaps is a more efficient andlogical way.10
According to Haas and Weiglein, a trapezius flap can beelevated on four different pedicles:
Figure 1 Overview of the wide range of various trapeziusflap classifications in the literature, including the classificationused in the present study (types 1e3).
Type 1: Based on the occipital artery, usually includingthe superior descending part of the muscle with atransverse skin paddle orientation.Type 2: Based on the ascending or descending branch ofthe SCA, including parts of the middle transverse fiberswith a transverse or vertical skin paddle orientation.Type 3: Based on the DSA, including the inferiorascending fibers with a vertical paddle orientation.Type 4: Based on the intercostal arteries in a turnovertechnique.
A myocutaneous flap based on the occipital artery (type1) is rarely indicated. Flaps based on the SCA (type 2) orDSA (type 3) are among the most frequently used flaps inclinical practice for various indications. A turnover muscleflap of the ascending part (type 4) could be a good treat-ment option for soft tissue defects of the middle and upperthoracic spine.
Type 2 flap
DesignIf the trapezius flap is based on the ascending branch of theSCA, it can be harvested as either a myocutaneous or anosteomyocutaneous flap, including a segment of the scap-ular spine. If it is based on the descending branch, it canonly be raised as a myocutaneous flap. The skin island can
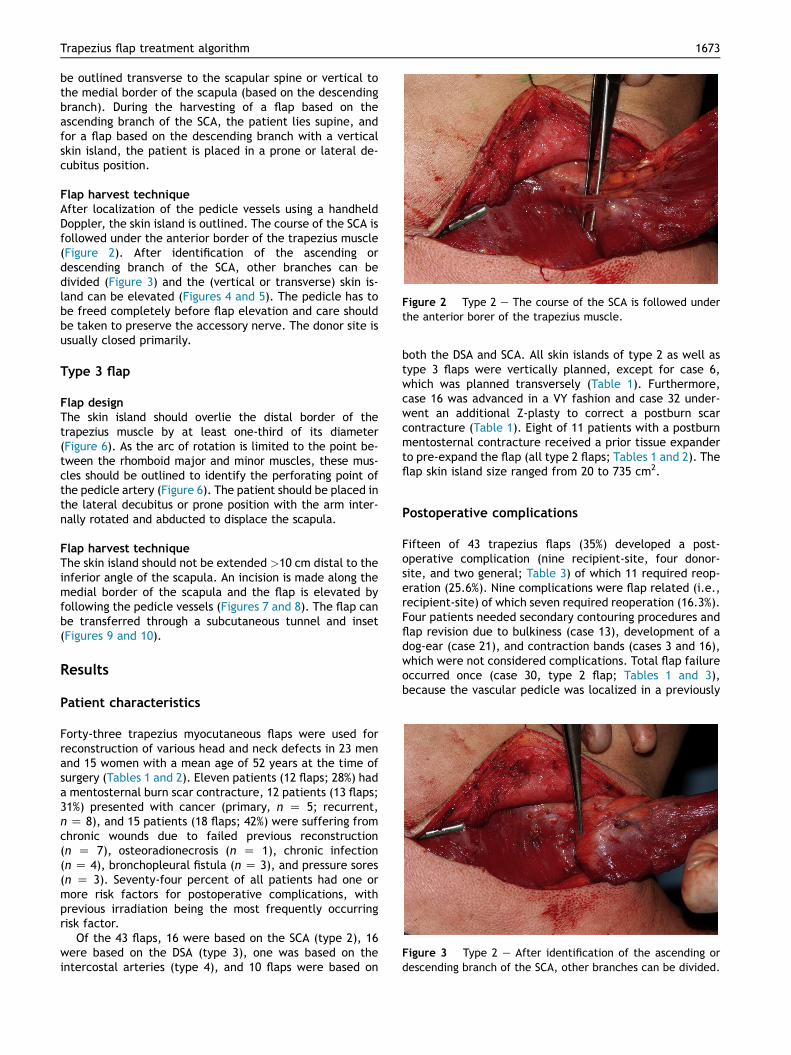
Figure 2 Type 2 e The course of the SCA is followed underthe anterior borer of the trapezius muscle.
Figure 3 Type 2 e After identification of the ascending ordescending branch of the SCA, other branches can be divided.
Trapezius flap treatment algorithm 1673
be outlined transverse to the scapular spine or vertical tothe medial border of the scapula (based on the descendingbranch). During the harvesting of a flap based on theascending branch of the SCA, the patient lies supine, andfor a flap based on the descending branch with a verticalskin island, the patient is placed in a prone or lateral de-cubitus position.
Flap harvest techniqueAfter localization of the pedicle vessels using a handheldDoppler, the skin island is outlined. The course of the SCA isfollowed under the anterior border of the trapezius muscle(Figure 2). After identification of the ascending ordescending branch of the SCA, other branches can bedivided (Figure 3) and the (vertical or transverse) skin is-land can be elevated (Figures 4 and 5). The pedicle has tobe freed completely before flap elevation and care shouldbe taken to preserve the accessory nerve. The donor site isusually closed primarily.
Type 3 flap
Flap designThe skin island should overlie the distal border of thetrapezius muscle by at least one-third of its diameter(Figure 6). As the arc of rotation is limited to the point be-tween the rhomboid major and minor muscles, these mus-cles should be outlined to identify the perforating point ofthe pedicle artery (Figure 6). The patient should be placed inthe lateral decubitus or prone position with the arm inter-nally rotated and abducted to displace the scapula.
Flap harvest techniqueThe skin island should not be extended >10 cm distal to theinferior angle of the scapula. An incision is made along themedial border of the scapula and the flap is elevated byfollowing the pedicle vessels (Figures 7 and 8). The flap canbe transferred through a subcutaneous tunnel and inset(Figures 9 and 10).
Results
Patient characteristics
Forty-three trapezius myocutaneous flaps were used forreconstruction of various head and neck defects in 23 menand 15 women with a mean age of 52 years at the time ofsurgery (Tables 1 and 2). Eleven patients (12 flaps; 28%) hada mentosternal burn scar contracture, 12 patients (13 flaps;31%) presented with cancer (primary, n Z 5; recurrent,n Z 8), and 15 patients (18 flaps; 42%) were suffering fromchronic wounds due to failed previous reconstruction(n Z 7), osteoradionecrosis (n Z 1), chronic infection(n Z 4), bronchopleural fistula (n Z 3), and pressure sores(n Z 3). Seventy-four percent of all patients had one ormore risk factors for postoperative complications, withprevious irradiation being the most frequently occurringrisk factor.
Of the 43 flaps, 16 were based on the SCA (type 2), 16were based on the DSA (type 3), one was based on theintercostal arteries (type 4), and 10 flaps were based on
both the DSA and SCA. All skin islands of type 2 as well astype 3 flaps were vertically planned, except for case 6,which was planned transversely (Table 1). Furthermore,case 16 was advanced in a VY fashion and case 32 under-went an additional Z-plasty to correct a postburn scarcontracture (Table 1). Eight of 11 patients with a postburnmentosternal contracture received a prior tissue expanderto pre-expand the flap (all type 2 flaps; Tables 1 and 2). Theflap skin island size ranged from 20 to 735 cm2.
Postoperative complications
Fifteen of 43 trapezius flaps (35%) developed a post-operative complication (nine recipient-site, four donor-site, and two general; Table 3) of which 11 required reop-eration (25.6%). Nine complications were flap related (i.e.,recipient-site) of which seven required reoperation (16.3%).Four patients needed secondary contouring procedures andflap revision due to bulkiness (case 13), development of adog-ear (case 21), and contraction bands (cases 3 and 16),which were not considered complications. Total flap failureoccurred once (case 30, type 2 flap; Tables 1 and 3),because the vascular pedicle was localized in a previously

Figure 4 Type 2 e Elevation of myocutaneous trapezius flap.
Figure 5 Type 2 e Inset of myocutaneous trapezius flap.
1674 A. Can et al.
irradiated area. Subsequently, the defect was successfullyclosed with a free anterolateral thigh (ALT) flap. A 70-year-old male patient (cases 14 and 15, flap type 2/3; Tables 1and 3) developed a chronic seroma in a heavily irradiatedarea. For this reason, an additional latissimus dorsi flapreconstruction was performed to bring the nonirradiatedtissue into the area. Furthermore, a 50-year-old female(case 18, type 2/3 flap; Tables 1 and 3) presented withrecurrence of a non-collapsible bronchopleural fistula dueto radiation and inflammatory fibrosis, which could not besealed using bronchoscopic techniques and coverage with atrapezius flap. Subsequently, the defect was closed with aleft serratus anterior flap. An 83-year-old male patient withurosepsis, who subsequently developed treatment-relatedprimary diastolic heart failure and fluid overload, died 1month postoperatively (case 27; Table 1). Another six pa-tients needed reoperation due to hematoma (cases 23 and29), wound infection (cases 4, 5, and 17), and woundcontraction (case 40). Donor-site dehiscence occurredtwice (cases 26 and 32) and donor-site necrosis once (case28).
We could not find a statistically different recipient-sitecomplication rate between flap types 2, 3, and 2/3 (chi-squared test, p Z 0.60). Flap type 4 was excluded from thisanalysis because it was used only once. Furthermore, weobserved no statistically significant differences in majorrecipient-site complications between defect localizationsor indication for surgery (Table 2).
Literature review
Different opinions on the vascular anatomy of the trapeziusflap and its modifications have led to a wide range ofvarious, confusing classifications (Figure 1). A PubMedsearch of the English literature revealed 13 papers with 242different cases of trapezius flap reconstructions (Table4).13e26 In an analysis of 30 superior trapezius flaps byAviv et al., no major flap complications were reported,whereas Netterville et al. reported major complications intwo (7%) of 28 superior flaps.13,14 The LTIMF, based on theTCA, was reported with 7% major flap failures (>20% flap
Figure 6 Type 3 e The skin island should overlie the distalborder of the trapezius muscle by at least one-third of itsdiameter.

Figure 7 Type 3 e Incision along the medial border of thescapula.
Figure 9 Type 3 e Trapezius flap transfer through subcu-taneous tunnel.
Trapezius flap treatment algorithm 1675
loss) and 6.5% minor flap failures in a series of 45 cases byUrken et al.17 All but one flap failed in patients who un-derwent prior neck dissection. Chen et al. reported thatthe extended vertical lower trapezius island myocutaneousflap can be performed safely in patients undergoing irra-diation or chemotherapy (provided that the vascular bundleis present), with a complication rate of 0%.18e23 Elshaeret al. used the extended LTIMF based solely on the DSA intheir series of postburn axillary contracture repair.25 Therewere no major complications reported. Zheng et al. re-ported the use of the extended lower trapezius myocuta-neous flap in burn scar reconstruction of the face and neckin 11 children (12 flaps). No major complications were re-ported, except for mild necrosis in one case.26
Surgical treatment algorithm
Which trapezius flap type is indicated depends on thelocalization of the defect, bone involvement, and priorneck dissection, as is depicted in the proposed algorithm(Figure 11). Soft tissue defects of the anterior neck, lowerneck, and intraoral mucosa are typical indications for flapsbased on the ascending branch of the SCA (type 2a). In the
Figure 8 Type 3 e Trapezius flap elevation by following theDSA pedicle.
case of small bone defects (e.g., mandible), a combinedosteomyocutaneous flap based on the ascending branch ofthe SCA may be indicated.27 In the case of larger bonydefects, the vascularization cannot be guaranteed.
Typical indications for flaps based on the descendingbranch of the SCA (type 2b) are soft tissue defects of theposterior neck and defects of the cervical spine. Further-more, when the accessory nerve has already been dividedduring neck dissection, a flap based on the descending partof the SCA is preferred. Flaps based on the DSA (type 3) aretypically used for defects of the contralateral side of thelower neck and upper thoracic spine. In the case of a softtissue defect of the middle and lower thoracic spine, a type4 flap is used based on the intercostal arteries.
Particularly in flap types 2 and 3, tissue expanders canbe placed in a submuscular plane to enlarge the size of theflap prior to transfer, if time allows, providing a thin skinisland with less risk of skin necrosis of the lower part.
Discussion
The purpose of this study was to evaluate surgical outcomesof trapezius myocutaneous flap reconstructions and to
Figure 10 Type 3 e Trapezius flap inset and primary donor-site closure.
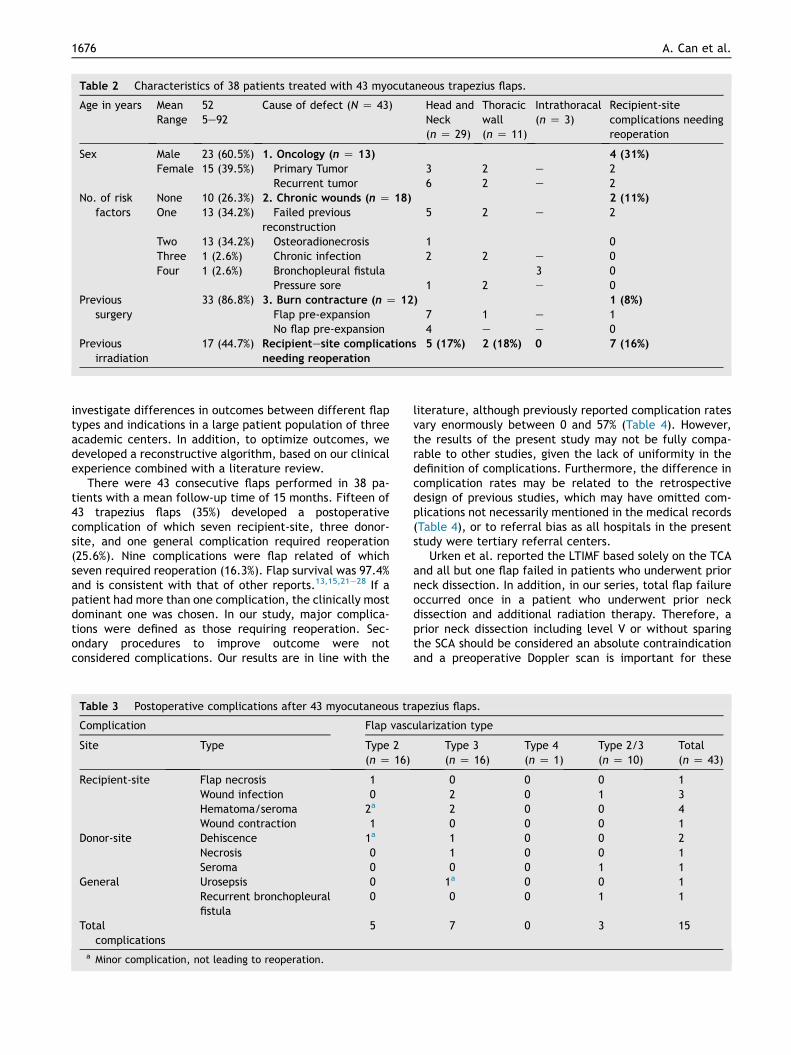
Table 2 Characteristics of 38 patients treated with 43 myocutaneous trapezius flaps.
Age in years MeanRange
525e92
Cause of defect (N Z 43) Head andNeck(n Z 29)
Thoracicwall(n Z 11)
Intrathoracal(n Z 3)
Recipient-sitecomplications needingreoperation
Sex Male 23 (60.5%) 1. Oncology (n Z 13) 4 (31%)
Female 15 (39.5%) Primary Tumor 3 2 e 2Recurrent tumor 6 2 e 2
No. of riskfactors
None 10 (26.3%) 2. Chronic wounds (n Z 18) 2 (11%)
One 13 (34.2%) Failed previousreconstruction
5 2 e 2
Two 13 (34.2%) Osteoradionecrosis 1 0Three 1 (2.6%) Chronic infection 2 2 e 0Four 1 (2.6%) Bronchopleural fistula 3 0
Pressure sore 1 2 e 0Previous
surgery33 (86.8%) 3. Burn contracture (n Z 12) 1 (8%)
Flap pre-expansion 7 1 e 1No flap pre-expansion 4 e e 0
Previousirradiation
17 (44.7%) Recipientesite complications
needing reoperation
5 (17%) 2 (18%) 0 7 (16%)
1676 A. Can et al.
investigate differences in outcomes between different flaptypes and indications in a large patient population of threeacademic centers. In addition, to optimize outcomes, wedeveloped a reconstructive algorithm, based on our clinicalexperience combined with a literature review.
There were 43 consecutive flaps performed in 38 pa-tients with a mean follow-up time of 15 months. Fifteen of43 trapezius flaps (35%) developed a postoperativecomplication of which seven recipient-site, three donor-site, and one general complication required reoperation(25.6%). Nine complications were flap related of whichseven required reoperation (16.3%). Flap survival was 97.4%and is consistent with that of other reports.13,15,21e28 If apatient had more than one complication, the clinically mostdominant one was chosen. In our study, major complica-tions were defined as those requiring reoperation. Sec-ondary procedures to improve outcome were notconsidered complications. Our results are in line with the
Table 3 Postoperative complications after 43 myocutaneous tr
Complication Flap vasc
Site Type Type 2(n Z 16)
Recipient-site Flap necrosis 1Wound infection 0Hematoma/seroma 2a
Wound contraction 1Donor-site Dehiscence 1a
Necrosis 0Seroma 0
General Urosepsis 0Recurrent bronchopleuralfistula
0
Totalcomplications
5
a Minor complication, not leading to reoperation.
literature, although previously reported complication ratesvary enormously between 0 and 57% (Table 4). However,the results of the present study may not be fully compa-rable to other studies, given the lack of uniformity in thedefinition of complications. Furthermore, the difference incomplication rates may be related to the retrospectivedesign of previous studies, which may have omitted com-plications not necessarily mentioned in the medical records(Table 4), or to referral bias as all hospitals in the presentstudy were tertiary referral centers.
Urken et al. reported the LTIMF based solely on the TCAand all but one flap failed in patients who underwent priorneck dissection. In addition, in our series, total flap failureoccurred once in a patient who underwent prior neckdissection and additional radiation therapy. Therefore, aprior neck dissection including level V or without sparingthe SCA should be considered an absolute contraindicationand a preoperative Doppler scan is important for these
apezius flaps.
ularization type
Type 3(n Z 16)
Type 4(n Z 1)
Type 2/3(n Z 10)
Total(n Z 43)
0 0 0 12 0 1 32 0 0 40 0 0 11 0 0 21 0 0 10 0 1 11a 0 0 10 0 1 1
7 0 3 15

Table 4 Literature review of trapezius flap reconstruction outcomes by flap type.
Flap type No. Indication Minorcomplication
Majorcomplication
Reoperation
Type 1 Occipital Superior
Aviv et al.13 30 Primary tumor 2 0 0Netterville et al.14 28 NR NR 2 (7%) NR 7%
Type 2/SCA Lateral (TCA)
Netterville et al.14 24 NR NR 5 (21%) NR 21%LTIMF (TCA)
Mathes and Stevenson15 13 Chronic infection (n Z 2) 0 0 0 0%Primary tumor (n Z 4) 0 0 0ORN (n Z 3) 0 0 0Failed previousreconstruction (n Z 4)
0 0 0
Cummings et al.16 14 NR NR 57% NR 57%Urken et al.17 45 NR 6.5% 7% NR 7%Extended vertical LTIMF (TCA)
1 Chen et al.18 11 Recurrent tumor 1 0 0 0%2 Chen et al.19 8 Recurrent tumor 2 0 0 0%3 Chen et al.20 4 Primary tumor 1 0 0 0%5 Chen et al.21 8 Primary tumor 1 0 0 0%6 Chen et al.22 18 Primary tumor 3 0 0 0%7 Chen et al.23 11 Primary tumor 2 0 0 0%Extended vertical TMF (TCA)
Ugurlu et al.24 9 Failed previousreconstruction (n Z 4)
0 0 0 11%
Tumor recurrence (n Z 5) 2 1 1Present study 2 Recurrent tumor 0 0 0 12.5%
2 Chronic wound 1 1 112 Burn contracture 1 1 1
Type 3/DSA Extended LTIMF (DSA)
Elshaer25 8 Burn contracture 2 0 0 0%Zheng et al.26 11 Burn contracture 1 0 0 0%Present study 3 Primary tumor 0 1 1 25%
6 Recurrent tumor 0 2 27 Chronic wound 0 1 1
Type 2/3DSA/SCA
Present study 2 Primary tumor 0 1 1 10%8 Chronic wound 0 0 0
Type4/intercostals
Present study 1 Chronic wound 0 0 0 0%
NR, not reported.
Trapezius flap treatment algorithm 1677
patients undergoing this procedure.28 Ugurlu et al. pro-posed that an extended vertical trapezius myocutaneousflap based solely on the TCA could be used as a salvageprocedure for failure of previous flap procedures and tumorrecurrence.24 Because the extended flap is a peninsularflap, a longer well-perfused flap can be used, without thegreat risk of total flap failure. However, the peninsulardesign of the flap requires a secondary operation to correctthe dog-ear.
The reconstruction of head and neck defects with a localflap in combination with planned radiation therapy maydelay wound healing, and a free flap may not always befeasible or preferable in patients with a poor general con-dition or a poor prognosis.1 In these instances, regional flapsurgery may be the first choice. The trapezius flap is a goodalternative to the pectoralis major or supraclavicular flap,and it is preferred over local flaps. The main disadvantages
of the trapezius flap include the required position changeduring surgery, its unreliable vascularization after level Vneck dissection, and the possible requirement of a skingraft to close the donor site in the case of a large skin is-land. Traditionally, the pectoralis major flap is the first-choice regional flap in head and neck surgery, because itis conveniently located anteriorly and requires no positionchange. However, the pectoralis flap has a more limited arcof rotation, more flap bulkiness, and negative estheticconsequences for the donor site in females, and possibilityfor secondary contracture of the pedicle or gravitationaldisplacement with time.4
Conclusions
Trapezius myocutaneous flaps based on SCA and DSA have alow donor-site morbidity and a reliable vascularization, and

Figure 11 A surgical management algorithm for trapezius flap transfers, based on our experience with 43 cases and a literaturereview.
1678 A. Can et al.
ensure skin coverage in the head and neck area withreasonable skin color match. As with any musculocutaneousflap, tissue expanders can be employed to enlarge the flapprior to transfer if time allows. Donor-site problems arerarely significant.
Our study clearly shows that these flaps are particularlyuseful in patients who have experienced previous radiationinjury, or who are ineligible for free flap surgery for headand neck reconstruction.
Conflict of interest
None.
Funding
None declared.
Ethical approval
Not required.
References
1. Krijgh DD, Mureau MA. Reconstructive options in patients withlate complications after surgery and radiotherapy for head and
neck cancer: remember the deltopectoral flap. Ann Plast Surg2013 Aug;71(2):181e5.
2. Hofer SO, Mureau MA. Pedicled perforator flaps in the head andneck. Clin Plast Surg Oct 2010;37(4):627e40 [vi].
3. MureauMA,PoschNA,MeeuwisCA,Hofer SO. Anterolateral thighflap reconstructionof largeexternal facial skindefects: a follow-up study on functional and aesthetic recipient- and donor-siteoutcome. Plast Reconstr Surg Apr 2005;115(4):1077e86.
4. van Rossen ME, Verduijn PV, Mureau MA. Survival of pedicledpectoralis major flap after secondary myectomy of musclepedicle including transection of thoracoacromial vessels: doesthe flap remain dependent on its dominant pedicle? J PlastReconstr Aesthet Surg Mar 2011;64(3):323e8.
5. Demergasso F, Piazza MV. Trapezius myocutaneous flap inreconstructive surgery for head and neck cancer: an originaltechnique. Am J Surg Oct 1979;138(4):533e6.
6. Baek SM, Biller HF, Krespi YP, Lawson W. The lower trapeziusisland myocutaneous flap. Ann Plast Surg Aug 1980;5(2):108e14.
7. Tan KC, Tan BK. Extended lower trapezius island myocutaneousflap: a fasciomyocutaneous flap based on the dorsal scapularartery. Plast Reconstr Surg Apr 2000;105(5):1758e63.
8. Mathes SJ, Nahai F. Classification of the vascular anatomy ofmuscles: experimental and clinical correlation. Plast ReconstrSurg Feb 1981;67(2):177e87.
9. Ulrich D, Fuchs P, Pallua N. Preexpanded vertical trapeziusmusculocutaneous flap for reconstruction of a severe neckcontracture after burn injury. J Burn Care Res MareApr 2008;29(2):386e9.
10. Haas F, Weiglein AH. Trapezius flap. In: Wei FC, Mardini S,editors. Flaps and reconstructive surgery. Saunders; 2009.p. 249e69.

Trapezius flap treatment algorithm 1679
11. Navarro-Vila C, Borja-Morant A, Cuesta M, Lopez de Atalaya FJ,Ignacio Salmeron J, Barrios JM. Aesthetic and functionalreconstruction with the trapezius osseomyocutaneous flap anddental implants in oral cavity cancer patients. J Craniomax-illofac Surg Dec 1996;24(6):322e9.
12. Yang D, Morris SF. Trapezius muscle: anatomic basis for flapdesign. Ann Plast Surg Jul 1998;41(1):52e7.
13. Aviv JE, Urken ML, Lawson W, Biller HF. The superior trapeziusmyocutaneous flap in head and neck reconstruction. ArchOtolaryngol Head Neck Surg Jul 1992;118(7):702e6.
14. Netterville JL, Panje WR, Maves MD. The trapezius myocuta-neous flap. Dependability and limitations. Arch OtolaryngolHead Neck Surg Mar 1987;113(3):271e81.
15. Mathes SJ, Stevenson TR. Reconstruction of posterior neck andskull with vertical trapezius musculocutaneous flap. Am J SurgOct 1988;156(4):248e51.
16. Cummings CW, Eisele DW, Coltrera MD. Lower trapezius myo-cutaneous island flap. Arch Otolaryngol Head Neck Surg Oct1989;115(10):1181e5.
17. Urken ML, Naidu RK, Lawson W, Biller HF. The lower trapeziusisland musculocutaneous flap revisited. Report of 45 cases anda unifying concept of the vascular supply. Arch OtolaryngolHead Neck Surg May 1991;117(5):502e11.
18. Chen WL, Zhang B, Wang JG, Yang ZH, Huang ZQ, Zhang DM.Reconstruction of large defects of the neck using an extendedvertical lower trapezius island myocutaneous flap followingsalvage surgery for neck recurrence of oral carcinoma. J PlastReconstr Aesthet Surg Mar 2011;64(3):319e22.
19. Chen WL, Li J, Yang Z, Huang Z, Wang J, Zhang B. Extendedvertical lower trapezius island myocutaneous flap in recon-struction of oral and maxillofacial defects after salvage surgeryfor recurrent oral carcinoma. J Oral Maxillofac Surg Feb 2007;65(2):205e11.
20. Chen WL, Deng YF, Peng GG, et al. Extended vertical lowertrapezius island myocutaneous flap for reconstruction of
cranio-maxillofacial defects. Int J Oral Maxillofac Surg Feb2007;36(2):165e70.
21. Chen WL, Yang ZH, Zhang DM, Huang ZQ, Fan S, Wang L.Reconstruction of major full cheek defects with combinedextensive pedicled supraclavicular fasciocutaneous island flapsand extended vertical lower trapezius island myocutaneousflaps after ablation of advanced oral cancer. J Oral MaxillofacSurg May 2012;70(5):1224e31.
22. Chen WL, Yang ZH, Li JS, Huang ZQ. Reconstruction of thetongue using an extended vertical lower trapezius islandmyocutaneous flap after removal of advanced tongue cancer.Br J Oral Maxillofac Surg Jul 2008;46(5):379e82.
23. Chen WL, Li JS, Yang ZH, Huang ZQ, Wang JQ. Extended ver-tical lower trapezius island myocutaneous flap for repairingextensive oropharyngeal defects. J Oral Maxillofac Surg Jun2009;67(6):1349e53.
24. Ugurlu K, Ozcelik D, Huthut I, Yildiz K, Kilinc L, Bas L. Extendedvertical trapezius myocutaneous flap in head and neck recon-struction as a salvage procedure. Plast Reconstr Surg Aug 2004;114(2):339e50.
25. Elshaer WM. Extended lower trapezius island myocutaneousflap in the repair of postburn axillary contracture. PlastReconstr Surg Jun 2004;113(7):2076e81 [discussion2082e2074].
26. Zheng XY, Guo X, Wang TL, Wang JQ. Extended lower trapeziusmyocutaneous flap in burn scar reconstruction of the face andneck of children. Pediatr Surg Int Dec 2011;27(12):1295e300.
27. Conley J. Use of composite flaps containing bone for majorrepairs in the head and neck. Plast Reconstr Surg May 1972;49(5):522e6.
28. Urken ML. Trapezius system. In: Urken ML, Cheney ML,Blackwell KE, Harris JR, Hadlock TA, Futran N, editors. Atlas ofregional and free flaps for head and neck reconstruction: flapharvest and insetting. 2nd ed. Lippincott Williams & Wilkins;2011. p. 27e46.





























