Embed Size (px)
Citation preview

POSTGRAD. MED. J. (I961), 37, 703
THE MOTILITY OF THE SMALL INTESTINEA. M. CONNELL, M.B., CH.B., B.Sc.
Member of the Medical Research Council's Gastroenterology Research Unit, Central Middlesex Hospital, London, N.W.Io.
'Every point of the intestine is in a state ofactivity, which can be played upon and modified byimpulses arriving at it from all positions of the gut,above and below'-Bayliss and Starling, I899.ALTHOUGH the dynamic state of the intestinalmusculature was well appreciated by Bayliss andStarling at the end of the last century, subsequentprogress in our understanding of the mechanismscontrolling intestinal motility has been dis-appoifitingly slow. Progress has been delayed bya confused nomenclature. The terms 'motility',' peristalsis' and 'tone' are often used in-discriminately and without precise definition. Forexample, the term ' motility' is used to describe avariety of different features of the intestinal move-ments, including the rate of passage of food andother materials along the alimentary tract, theappearances of the gut on direct observation or atfluoroscopy, the 'tone ' or rigidity of the bowelwall and the pressures developed in the lumen ofthe bowel. The result is that references to bowelmovements in clinical writings are frequently sovague and imprecise as to be, at times, meaning-less. Progress in this field of study has also beenhindered by difficulties in methodology. Patientsand subjects always dislike swallowing tubes andas it has until recently been necessary to pass atube into the small intestine to obtain informationabout bowel movements, there has been a naturalreluctance on the part of clinical physiologists tosubject their patients to this discomfort. Further-more, the nausea and distress caused by thepresence of a tube in the alimentary tract mayvitiate studies using these methods.The advent of the ingestible telemetering cap-
sule, however, has for the first time made itpossible to obtain quantitative data from thealimentary tract without the use of tubes and itseems likely that the prototypes undergoingdevelopment at present herald a new era in thestudy of gastrointestinal function. It is thereforean appropriate time to examine existing knowledgeabout the motility of the small intestine in man.
Methods of StudyIn animals a great deal of information has been
obtained about intestinal movements by directobservations of loops of bowel of which theThiry-Vella (Thiry, I864; Vella, I888) is the bestknown. Alternatively, recordings have been madefrom balloons or other devices introduced intofistulous openings in the alimentary tract.
In man, direct observation can be made, butonly at surgery where the situation is complicatedby the effects of trauma and anesthesia, or of thelimited area of bowel exteriorized to form acolostomy or ileostomy. However, a number ofindirect methods are available. These include theuse of X-rays, the detection of intestinal soundsby a microphone on the abdominal wall, recordingof intestinal electropotentials, the recording of walltension by large balloons and the recording ofintra-luminal pressures by open-ended tubes orminiature transducers. There is no ideal method,and each method can only give information abouta limited aspect of motility so that in any givenstudy the method used must be selected withconsideration to the particular aspect of motilityabout which information is desired. For example,radiology remains the best method of timingintestinal transit but even cineradiography is oflimited value in investigating other aspects ofmotility and while the large balloon remains thebest method of assessing the 'tone' or rigidityof the bowel wall it does not accurately recordintra-luminal pressure. A review of the methodsof measurement of gastrointestinal motility inman has recently been published by Farrar andDavidson (I960).Large Balloons
For many years the large balloon has had anhonoured place in the study of intestinal motilityand much of the information we now have hasbeen obtained by this method. Balloon-manometersystems have certain well-known disadvantageswhich have been discussed by Quigley and Brody(I952), Lorber and Shay (I954), and more re-cently by Chaudhary and Truelove (I96I). Un-happily, the impression has been created that theconsiderable amount of data accumulated by thismethod is invalid. However, in spite of theavailability of newer and more refined methods,
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

704 POSTGRADUATE MEDICAL JOURNAL December 1961
.iiii~iii aiP
,. .4........
4 ~ift~"'*@I;:: II·:ivj;:ij:
......
·:;::-r;7;i·::···:::;;
Its-~E 5E~'";l- -a:: - ;;~"""·":WL.
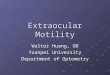
FIG. i.-Diagrammatic representation of the structure of the radio pill. (By courtesy of the Editorof the British Communicatiens and Electronics.)
the large balloon remains a useful method in thestudy of intestinal motility. By virtue of itsstimulant effect on the bowel it provides a base-lineof activity against which the effects of drugs canbe assessed and it is still the only method ofdetermining the rigidity or 'tone' of thebowel wall.
Small BalloonsMany of the disadvantages of the large balloon
system result from the insensitive water mano-meters usually employed. Many of the disadvan-tages can be overcome if a smaller balloon with anoptical recording system is used. Code, Hightowerand Morlock (1952) described a small balloon(3 cm. in diameter) recording on an optical mano-meter and Hightower (1952) showed good correla-tion between this device and a pressure transducerin all areas of the gastrointestinal tract with theexception of the pyloric antrum.
Miniature BalloonsAtkinson, Edwards, Honour and Rowlands
(1957) introduced a miniature balloon (7 mm. byio mm.) recording on a metal capsule opticalmanometer (Rowlands, Honour, Edwards andCorbett, 1953). An almost exact comparison existsbetween tracings obtained with a miniature balloonand an open-ended tube (Edwards and Rowlands,I960; Connell, 1g96a) and a miniature balloon and
a radio pill recording from the same segment ofgut (Connell and Rowlands, i960) provided thatthe balloon is not squeezed by the bowel wall.These miniature balloons record true intraluminalpressures, do not act as a stimulus to motility andcannot be blocked by the bowel content.
Open-ended TubesOpen-ended tubes, which may be either air-
filled (Rowlands, Honour, Edwards and Corbett,1953) or fluid-filled (Smith, Texter, Stickley andBarborka, 1957), measure true intraluminal pres-sures, but plugging of the catheter with mucuscan be troublesome and result in damping or dis-tortion of the record. To overcome this, mostinvestigators keep the tubes patent by introducingair or fluid continuously into the recording systemat a very slow rate (Quigley and Brody, 1952).Electromagnetic Pressure TransducersA miniature pressure transducer in the bowel
records true intraluminal pressures and, providedthe response characteristics of the recording systemare satisfactory, is free of the difficulties due todamping or distortion which occur using open-ended tubes. A pressure transducer was intro-duced by Abbott, Hartline, Hervey, Inglefinger,Rawson and Zetzel (I943), but failed to be acceptedinto general use, probably on account of technicaldifficulties. A miniature manometer, however,
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

December i961 CONNELL: The Motility of the Small Intestine 705
devised by Gauer and Gienappe (1950) for cardio-vascular research has been used with good resultsin the study of alimentary motility, including thesmall intestine (Quigley and Brody, i952; Code,Wilkinson and Sauer, 1954).Radio PillThe discomforts and obvious disadvantages of
oro-nasal intubation have stimulated the develop-ment of radio telemetering capsules for studyingthe gastrointestinal tract (Mackay and Jacobson,1957; Farrer, Zworykin and Baum, 1957; Connelland Rowlands, 1960). The pressure-sensitivecapsule devised by the Medical Research Councilis illustrated in Fig. i (Rowlands and Wolff, i960).One end of the pill-housing is formed by a perspexdiaphragm to which a ferrite disc is attached.When the diaphragm bends the disc is movedand this changes the inductance and hence thefrequency of oscillation of the transmitter. Thefrequency change is transmitted and picked up bya suitable aerial. The power supply is a batterywith a life of up to 8o hours. In later models theswitching device illustrated in this pill has beenreplaced by a peg which on removal permits con-tact between two wires. For accurate recording itis necessary to screen the patient and receivingsystem against unwanted electronic interference.
This technique permits quantitative recordingof small intestinal intraluminal pressures withoutany discomfort to the patient. Moreover, when thepill changes its position with reference to theaerial the strength of the signal received alsochanges. By recording variations in signal strengthinformation is provided about movements of thecapsule not necessarily associated with changes inintraluminal pressure (Connell and Rowlands,i96i). At the same time, information about gastro-intestinal transit can be obtained by following themovements of the pill fluoroscopically using animage intensifier. This may become the method ofchoice in small intestinal studies in spite of thedisadvantages of expense and the fact that recordscan be obtained from only one position in theintestine at a time. The problem of localizing thepill can largely be overcome by the judicious useof contrast media and fluoroscopy (Ridgeway andSmith, i961; Connell, I96ib).X-rays
Although radiology permits simultaneous visual-ization of the activity of several areas of the in-testinal tract, the method suffers from some seriouslimitations. Outstanding among these are the lackof any continuous record from which to makequantitative measurements, the fact that one seg-ment of gut may obscure another and the shorttime available for study due to the radiation hazard
even when an image intensifier is used. X-raystudies, however, can supplement and illustrateother techniques and they also provide the onlymeans of estimating intermediate transit times.
Abdominal SoundsCannon (1905) first used intestinal sounds as a
measure of total intestinal activity. Although thismethod has been used to estimate the gross effectof drugs on motility (Farrar and Inglefinger, 1955;Du Pleissis, 1954), it is not an accurate index, asthe intensity and quality of the sound depend notonly on the contraction of the intestinal muscle,but also on the relative proportions of gas and fluidin the bowel and the distance of the active loopfrom the surface. Intestinal movements frequentlyoccur without the production of any sound(Louckes, Quigley and Romans, 1953).Electropotential Recording
Electropotential changes have been recordedfrom the small intestine of dogs (Armstrong,Milton and Smith, I956) and from the intestinalmuscle of the exteriorized ileum in conscious men(Daniel and Bogoch, 1959). Action potentialshave been described in association with forcefulsegmental contractions, but changes in electricalactivity occur in the absence of pressure changes.However, it is clear that much further work isnecessary to establish the significance of thesepotentials.Pressure Patterns from the Small IntestineDuodenum and JejunumA typical record of the pressure changes of the
upper small intestine obtained using miniatureballoons is illustrated in Fig. 2. The waves illus-trated here are of short duration (2 to 6 seconds),of varying amplitudes (up to 75 cm. of waterpressure) and occur in rhythmic sequence at arate of i i to I2 per minute. Larger, slower waveslasting from o seconds to 8 minutes may alsooccur, but with less regularity. They may havesuperimposed faster components. The proportionof slow waves is greatest in the duodenum and theybecome less prominent both in number and sizein the jejunum (Inglefinger and Abbott, 1940).
While there is general agreement about thedescription of the waves of the small intestine,there is confusion about their nomenclature.Inglefinger and Abbott (I940) described the smallfast waves as ' S ' waves in distinction to largeslower waves, which they called ' L ' waves. Smithand others (I957) divided the waves into 'A' wavesof less than 30 seconds duration and ' B ' waves ofmore than 30 seconds duration. Foulk, Code, Mor-lock and Bargen (I954), on the other hand, adoptedthe classification devised by Templeton and
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

706 POSTGRADUATE MEDICAL JOURNAL December i961
40 1
FIG. 2.-Rhythmic fast waves from the duodenum recorded by a miniature balloon. Thesecorrespond to S Waves (Inglefinger and Abbott, '943), A waves (Smith and others, 1957)and Type I (Foulk and others, 1954). Verticals equal I-minute intervals.
Lawson (I 93 ) to describe the motility of the colonin dogs. In this scheme fast waves are calledType I and the slower waves Types II or III.Type III is a base-line rise with superimposedwaves. This classification was also used by Fink(1959) and Oddone, de la Pierre, Bertero and Jona(1959). Andrew (1954) gave the slow waves a func-tional significance and called them' tetany ' waves.Farrar and Bernstein (I958), however, noting thatnone of the published classifications had provedsatisfactory, did not attempt any classification ofwaves into distinct types. This is, undoubtedly,a realistic view, but it is essential for furtherprogress that an agreed nomenclature of motilityshould be established.
In a normal record there are periods of activityalternating with periods of inactivity, but therecorded duration of activity of the upper smallintestine differs considerably in various publica-tions (Table i). Some of the differences may bedue to different methods of recording, but other,and possibly more important, reasons are theinterval since the previous meal (Foulk, Code,Morlock and Bargen, I954) and the exact methodof analysis. In this latter respect Fink (i959)showed that the percentage of the total time ofobservation occupied by active and inactiveperiods was approximately the same. On the otherhand, where the duration of each wave wasmeasured and the sum of these durations used tocompute percentage activity the mean was only12%. There is, therefore, a variation betweenobservers depending on the criterion of ' activityselected.The duration of activity is the same in normal
subjects, patients with duodenal ulcer in remission,patients with ulcerative colitis (Foulk, Code, Mor-lock and Bargen, I954), patients with duodenal
TABLE I
PercentageAuthor Method of Duration of
Recording Activity
Foulk, Code, Mor- Balloons, 3 cm. 34 (fastinglock and Bargen (i954) diameter 24 hours)
62 (fasting5-12 hours)
Smith, Texter, Stick- Open-ended 14 (fasting)ley and Barborka tubes(I957)
Oddone, de la Pierre, Small balloons 25Bertero and Jona (2 cm. dia-(I959) meter)
Fink (I959) Open-ended < 30-65tubes
Barbero, Chin Kim Open-ended 23and Davis (1958) (chil- tubesdren)
diverticula and patients with cholelithiasis (Fink,I959). Smith and others (I957) report an in-creased duration of activity in patients with duo-denal ulcer who are experiencing symptoms. Theduration of activity was found to be diminished inpatients with idiopathic steatorrhcea (Fink, I959;Inglefinger and Moss, I943), but not in childrenwith cceliac disease (Barbero, Chin Kim and Davis,I958).There is complete agreement that the rate of
rhythmic contractions of the duodenum is between8 and I2 cycles per minute and that the predom-inant frequency is i i per minute. The frequency ofcontraction of the jejunum is not altered inasymptomatic duodenal ulcer or in ulcerativecolitis (Foulk, Code, Morlock and Bargen, I954).
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

December 1961 CONNELL: The Motility of the Small Intestine 707
cm AH20
40
30
20
10
0
FIG. 3.-Large waves with superimposed fast components from the terminal ileum recorded byminiature balloon. These correspond to L waves (Inglefinger and Abbott, 1943), B waves(Smith and others, I957), Type III (Foulk and others, I954) and tetany waves (Andrew, 1954).Verticals represent X-minute intervals.
IleumLess information is available about the motility
of the terminal ileum and some of the data havebeen obtained by recording through ileostomystomas where it is doubtful if conditions are thesame as in the intact bowel. Recording by an open-ended tube passed through the mouth, Fink (I959)showed that the activity of the terminal ileum wascharacterized by low-amplitude rhythmic waves,present for 50 to 90% of the time of study. Largesimple waves were less frequently seen than in theduodenum, but so-called Type III waves werefrequently seen (Fig. 3). Inglefinger and Abbott(1940) found essentially similar patterns of activityand we have seen in recent studies, using theradio pill, rhythmic fast waves at a rate of six perminute occurring continuously for 21 hours in anormal subject. During this time no forwardmovement of the pill occurred. Farrer and Bern-stein (1958), recording from a radio capsule in theterminal ileum, also found, in contrast to Fink(I959), that the rate of rhythmic contractions ofthe ileum was slower than in the duodenum. Asimilar observation was made by Code, Rogers,Schlegel, Hightower and Bargen (1957), whostudied the motility of the terminal ileum throughileostomies in two subjects.The balance of evidence is that in man the rate
of rhythmic contraction decreases progressively onmoving from the duodenum to the ileum. Thesame gradient was noted in rabbits by Alvarez(19I5), who claimed that the rate of rhythmic con-traction of any segment of the small intestinevaried inversely with its distance from the pylorus.Douglas and Mann (i939a) made similar observa-
tions on dogs. The rate of rhythmic contractionis very constant at any one site and is not affectedby eating, sleep, vagotomy and splanchnicectomy(Douglas and Mann, I939a) or psychic influences(Castleton, 1934).
Douglas (I949), in an attempt to explain thedifferent rates of contraction of different parts ofthe small intestine, showed that the rate of rhyth-mic contraction of a length of jejunum could bereduced by any procedure which divided the in-trinsic nerve supply of the segment from that ofmore proximal segments. He concluded that therate of contraction of the jejunum was influencedby the duodenum. Armstrong, Milton and Smith(1956) noted that the rate of the slow componentsof electropotential records from the small intestineof dogs also decreased from duodenum to ileum.At any one site, however, the rate of the slowcomponents was very similar to the rate of rhyth-mic contraction. Subsequently, on the basis of thiswork, Milton and Smith (I956) suggested that theslow component of the electrical record was thefactor which controlled the frequency of rhythmiccontraction of the bowel. They also showed thatthe slow component of the duodenum and upperjejunum was influenced by discharge from an areain the region of the bile duct, but ectopic foci ofslow electropotential waves may be artificially pro-duced. On this basis, they postulated a pace-making area in the duodenum analogous to thoseof the cardiac muscle.While there is evidence that the rate of con-
traction of the upper small intestine is controlledfrom the duodenum, Daniel, Carlow, Wachter,Sutherland and Bogoch (I959) showed that the
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

708 POSTGRADUATE MEDICAL JOURNAL December 1961
distal small intestine is independent of duodenalcontrol and it seems likely that local pacemakerareas exist throughout the length of the gut whichimpart a distinct rhythm to segments of gutimmediately distal to them.
Basal Pressure in the Small IntestineThe basal pressure in the jejunum was recorded
by Abbott and others (I943) at between 8 and iocm. of water. Kewenter and Kock (i960) re-corded basal pressures in the duodenum of be-tween 6 and 10 cm. of water. These authorsconsidered that the hydrostatic pressure of thebody tissues and the 'tone' of the abdominalmuscles provided the greater part of this pressure.Fink (1959), although noting individual variations,showed a correlation between body weight andbasal pressure. Confirmation that the ' tone 'of the bowel wall contributed very little to the basalpressure was provided by Edwards and Rowlands(196i) who demonstrated that the basal pressuresin the cadaver were in the same range as in theliving subject, and that the pressure recorded wasdirectly related to the distance of the recordingpoint from the body surfaces. All these authorsused either open-ended tubes, miniature balloons,or electromagnetic transducers. Using large bal-loons, however, the 'tone' of the bowel wallcontributes a much greater proportion to the basalpressure.
Correlation of Pressure Records with X-rayAppearancesAt present there is no clear picture of what the
various types of waves on the pressure recordsrepresent in terms of the observed contractions ofthe intestinal wall. Inglefinger and Abbott (1940)outlined their balloons with barium and showedthat both large and small waves were associatedwith contractions passing caudally over the balloon.The small waves were associated with narrow in-dentations on the balloon surface while the largewaves lasting up to one minute might compress theballoon in its length. In a similar study Chapman,Pelazzo, Taylor and Proudfoot (1949) reported thatlow amplitude rhythmic waves corresponded toring-like contractions lasting 5 to 10 secondsrunning caudally over the balloons. Thesecontractions may have moved the balloons andbarium slightly but barium was never propelledforwards. They were, therefore, not propulsivewaves. Movements of the barium were associatedwith slow sustained contractions which might lastup to two minutes. In ileostomies, Posey andBargen (I95i) noted expulsion of fluid faeces in thepresence of both small and large waves (Types I,II and III). However, in the presence of smallwaves the faeces welled passively from the stoma,
whereas with large waves (Types II and III)they were expelled with force. Solid stool wasexpelled only in association with large waves.Fink (I959) showed a relationship between the rateof transit of a balloon and the proportion of large(Type III) waves in the record. The evidence isthat the low amplitude rhythmic waves may eitherrepresent stationary annular contractions or pro-pagated waves with no propulsive force. Peri-stalsis, therefore, in the sense of a propagatedcontraction should not necessarily be correlatedwith transport of chyme. On the other hand,transport does occur frequently, but not univer-sally (Daniel, Sutherland and Bogoch, I959) inassociation with more prolonged powerful rises inintraluminal pressure. Propulsion depends notonly on the nature of the wave form but also on thesize and nature of the bolus, the resistance to flowand the strength of the contraction. The radiopill has several times been seen to undergo rapidforward movements during the decline in pressureof a powerful wave, as it is thrust away from thegrip of the constricting contraction ring. Radio-logically, forward movement of chyme usuallyoccurs in 'squirts ' and such a rapid movementcould be produced either by a sudden strong con-traction of a segment of bowel with low resistanceto escape of the content distally, or by a rapidperistaltic wave.
Transit Times in the Small IntestineThe classical methods of estimating transit such
as the ingestion of carmine markers and the use ofglass beads are not only crude but applicable onlyto the study of mouth-to-anus times. Smallintestinal transit in man necessitates the use ofcontrast radiology in one form or another, the useof tubes, or the study of patients with ileostomies.Most markers, especially barium, can give informa-tion only about the rate of passage of the first andlast traces of the material but a more usefulmeasurement is that of the time of passage of themain concentration. As barium sulphate pro-bably stimulates bowel activity (Childrey, Alvarezand Mann, 1930) its rate of passage is not an indexof the transit time of ordinary meals, but for mostpurposes this is adequate. The rate of passagethrough the upper small intestine is more rapidthan through the lower. Using balloons outlinedby barium Inglefinger and Abbott (1940) showedthat the rate of passage of the balloon through theduodenum is five minutes, through the jejunum,two hours, and through the ileum, three to sixhours. Van Liere, Stickney and Northup (1945)obtained similar results in dogs. The rate ofpassage through the duodenum is extremely rapid.We have found that a radio pill passes from thepylorus to the fourth part of the duodenum in a
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

December i961 CONNELL: The Motility of the Small Intestine 709
0.8
0.6
0.4
FIG. 4.-Duodenal motility recorded by radio pill. Inthe time occupied by a wave (arrowed) the pillhad an uninterrupted movement from the positionof the pylorus to the fourth part of the duodenum.The dots represent i-minute intervals.
few seconds (Fig. 4) confirming the view ofDouglas (1948) that the function of the duodenumis transport and not trituration. At the other endof the small intestine the rate of transit is parti-cularly slow. A radio pill may remain for severalhours in the terminal ileum although rhythmicwaves may be recorded almost continuouslythroughout this period. Hertz (1913) and Op-penheimer (I940), in studies with barium, alsocommented on the delay in the terminal ileumalthough contractions occurred almost contin-uously. Many of these passed along the ileumtowards the colon. Hertz (I913) believed that' ileal stasis is a normal physiological condition ofthe utmost importance for adequate digestion'.
Both Hertz (I913) and Oppenheimer (1940)also described powerful peristaltic waves whichoccurred at irregular intervals and propelled thecontents of the terminal ileum into the cacum.These waves were associated with relaxation of theileocacal sphincter. They were much more
frequently seen immediately after meals (Hertz,1913) and it is known that evacuation of an estab-lished ileostomy occurs at infrequent intervals,usually after meals.
Factors Affecting Intestinal MotilityNervous Control of Intestinal MlovementThe gut has both an extrinsic supply via anto-
nomic nervous pathways and an intrinsic supplyin the plexuses in the gut wall, which permit com-plicated movements even when the extrinsic supplyis completely removed. The intricate nervous net-work in the wall of the intestine is often describedas being concentrated into two relatively distinct
plexuses, but the anatomical picture is, in fact,less simple and Garven (I957) describes at leastfive distinct plexuses. There is evidence that thereis a functioning protoplasmic syncytium includingboth the nervous networks and the smooth musclecells (Boeke, i940).
Bayliss and Starling (I899) originally postulateda neurogenic basis for the peristaltic reflex and,although this was disputed by Alvarez (1950),recent anatomical and physiological studies havestrengthened the original concept. Bulbring, Linand Schofield (1958) have shown that, althoughthe peristaltic reflex is not abolished by extrinsicdenervation of the small intestine, it can be pre-vented by local anesthesia, asphyxiation or re-moval of the mucous membrane. These experi-ments provide evidence that there are within thebowel wall intrinsic reflex arcs consisting of at leasttwo neurones: a sensory neurone with a nerveending on the mucosa and a motor neurone in-nervating the muscle cell.On the basis of their work on the peristaltic
reflex, Bayliss and Starling (I899) formulated alaw of the intestine which stated that a contractionof the bowel was associated with a distal relaxation.It is not always realized that the law is only validwithin the conditions of the experimental situationin which it was first established; that is, on dis-tension of the denervated intestine of a dog with aballoon. The ' law ' does not hold universally andPosey and Bargen (1951), using balloons, wereunable to confirm it in man.
Extrinsic Nervous ControlAfferent Pathways from the Small Intestine.
Afferent impulses arising in the gut result in reflexalteration in the function of various organs (Whit-teridge, I956). Extensive sensory pathways fromthe intestine have been described, and Paintal(I954) and Iggo (I957) have described sensoryreceptors in the small intestine. Agostoni, Chin-nock, Daly and Murray (I957) have shown that90% of the fibres of the vagus are afferent. Afferentpathways also occur in the sympathetic system.
Efferent Pathways to the Small Intestine. Muchof our information about the autonomic control ofintestinal motility has been obtained from animalexperiments. From the earlier studies emerged thegeneral concept that the parasympathetic outflowwas motor and the sympathetic outflow inhibitoryto the intestine. However, experimental physi-ologists, even using the most elegant techniques,recognize the necessarily artificial nature of theexperimental situation and the inherent capricious-ness of the results of nerve section or nerve stimula-tion. The response to nerve section will dependalmost entirely on the state of the bowel at thetime of section. For example, section of a motor
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

710 POSTGRADUATE MEDICAL JOURNAL December i961
nerve produces negligible effects unless the nerveis' tonically ' active (Youmans, 1952). Stimulationof nerves can be even more confusing. Garry andGillespie (1955) indicated some of the reasons forthe confusion when they showed that the responseof the gut varies with the frequency and strengthof stimulation to the extent of reversing theoriginal response. Animal studies, therefore, mustbe interpreted with caution.
Effect of the Vagus. In common with the generalview that the vagus is motor to the small intestine,Harper, Kidd and Scratcherd (I959) showed thatstimulation of either the central or peripheral endof the vagus resulted in an increase in the tone ofthe small intestine and in the amplitude of thecontraction. Division of the nerve did not in-fluence the rate of rhythmic contraction of thesmall intestine of the dog (Douglas and Mann,I939a), although Alvarez, Hosoi, Kiyoshi, Over-gard and Ascanio (I929) found that vagotomyalways reduced the rate in rabbits. In man,vagotomy results in little disturbance of smallintestinal function, although diarrhkea and occasion-ally steatorrhcea may result (Kay, i960). Thereis, however, no experimental evidence that this is aresult of a direct effect on the small intestine.
Effect of the Sympathetic Outflow. Section of thesympathetic nerves also results in very little altera-tion in small intestinal function. Douglas andMann (I939a) found no alteration in the rate ofrhythmic contraction of the small intestine of thedog following splanchnicectomy, although one dogdid develop diarrhoea. Ivy, Grossman and Bach-rach (1950) observed no ill effects following pre-ganglionic sympathectomy in dogs, but bloodydiarrhoea and ulceration of the stomach and smallintestine with a high mortality occurred followingremoval of the cceliac ganglia. In man, Bingham,Inglefinger and Smithwick (1950) studied themotility of the small intestine both radiologicallyand manometrically following bilateral-thoraco-lumbar sympathectomy for hypertension andfound no significant effect on motility. There wasan increase in the frequency of bowel action inone-fifth of the patients studied and three of i00patients complained of persisting severe diarrhoea.Some looseness of the bowels following sym-pathectomy was also noted by Ross and Brolsma(195i), but no patients had serious gastro-intestinal sequelae.The minimal effects of sympathectomy and
vagotomy on small intestinal function in man sup-port the modern concept that the sympathetic andparasympathetic outflows, rather than mediatingopposing and antagonistic impulses, exert a con-tinuous and complementary regulatory action,which integrates the function of the small intestineand permits a smooth response to the diversity of
stimuli to which it is exposed. This regulatoryfunction is largely carried out by utilizing a seriesof reflex pathways, some of which include thecentral nervous system, while others are largely inthe intrinsic nerve networks.
Intestino-intestinal ReflexesThe intestino-gastric reflexes, which effect in-
hibition of gastric motility following upper in-testinal distension, are probably mediated throughthe vagus (Thomas and Mogan, I931). On theother hand, intestino-intestinal inhibitory reflexeswhich have been extensively studied in Thiry andThiry-Vella loops in dogs, are independent of thevagus (Youmans, I944). As a result of thesereflexes, distension of one segment results in ageneralized inhibition of motility of the wholesmall intestine. There is agreement that both theafferent and efferent pathways are in the thoraco-lumbar system and that the central connections arein the spinal cord from the seventh thoracic tosecond lumbar segments (Youmans, i944; Changand Hsu, I942; Morin and Vial, I934). Thesestudies do not discount the possibility that sub-sidiary pathways may exist in the intrinsicplexuses.. These observations underline the self-perpetuating nature of the distension of intestinalileus and offer an explanation of the beneficialeffects of decompression by suction.
Reflex Responses to FeedingThe increase in small intestine activity after
eating was first described by MacEwan(I904) whowatched the writhing movements of the terminalileum through a cwecal fistula. He noted that theresponse was too quick to be explained by peri-stalsis spreading along the intestine and attributedit to a reflex. Since then other workers havedemonstrated increased ileal activity followingmeals (Daniel and others, I959; Kewenter andKock, i960) associated with occasional relaxationof the ileocaecal valve and discharge of the ilealcontents into the cacum (Hertz, I913).
Gregory (1950) showed that this reflex could beelicited in dogs by placing small quantities of foodin the stomach, by distending it with a balloon oreven by sham feeding. Douglas and Mann (1940)elicited the reflex by placing food in the duodenum.Gregory's experiments led him to the view that thereflex was dependent' on the integrity of thethoraco-lumbar outflow but Douglas and Mann(i939b, 1940) held that the response depended onthe continuity of the intestine and that the in-creased activity was transmitted mechanically alongthe bowel wall. This latter explanation, however,would not account for the cephalic phase of thereflex. The response is independent of the vagusnerves (Douglas and Mann, i939b) but can be
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

December I961 CONNELL: The Motility of the Small Intestine 711I
T MrYPENDRI '
O. / o0 I 0.
/ *.* ** *.. e *. ...\..'' ~} .''/*/e . ......0.2
FIG. 5.-The motility of the ileum recorded by radio pill. At the first arrow this normal subject wastold that his lunch was being prepared and at the second arrow he began to eat his lunch.The dots represent i-minute intervals.
abolished by atropine (Daniel and others, i959).Fig. 5 shows the effects of food on the smallintestine and demonstrates the cephalic phase ofthe reflex in a normal man. Post-prandialsymptoms are prominent in many gastro-intestinaldisorders and some of these symptoms may have abasis in a disorganization or incoordinationof the gastro-ilio-colic reflexes.
Effect of DrugsThe effect of a drug on the pressure patterns
can only give an approximate index of the likelyclinical effect as the relationships between in-testinal pressures and clinical symptomatology arenot established, but if a drug fails to produce anyeffect on a pressure record it is unlikely that it willbe useful in clinical practice. Certain proprietarypreparations tested by Rowlands, Chapman,Taylor and Jones (i95oa) did not affect smallintestinal motility, and no subsequent clinicalevidence has been advanced to indicate that thesedrugs have any therapeutic value. The difficultiesof assessing the effect of drugs in the alimentarytract are made even more formidable in that placebotablets may result in a decrease in small intestinalactivity (Chapman, Rowlands, Taylor and Jones,i950). Unwarranted claims about the effective-ness of drugs may be made either because of failureof adequate experimental control or because of un-warranted interpolation from the experimentalresult into clinical practice. The problemsassociated with the measurement of the effects ofdrugs on the gastrointestinal tract have recentlybeen reviewed by Rowlands (i959).
Drugs Inhibiting Motility. Chapman, Rowlandsand Jones (i950) showed that atropine andbelladonna alkaloids result in a much greaterdecrease in upper small-intestinal motility thanplacebo preparations. The most striking fall is in
propulsive motility. All forms of motility in theterminal ileum are reduced by atropine (Code andothers, I957). Banthine also produces a decreasein propulsive and total contractions and causes adecrease in tone. It has a more rapid effect andreduces motility to a greater degree than tincture ofbelladonna (Chapman, French, Hoffman andJones, 1952) and delays the transit time throughthe small intestine (Lepore, Golden and Flood,195I). Other drugs which cause reduction insmall intestinal motility are tetraethylammonium(Chapman, Stanbury, Jones and Dennison, 1948),amphetamine (Elsom, Glenn and Drossner, 1939),ephedrine (Posey, Bargen, Dearing and Code,1948), and adrenaline (Bargen, Wesson andJackman, 1940). The effect of the sympatheticamines, however, is biphasic as following a shortperiod of relaxation there is frequently a reboundphase of increased activity (Dreyer, 1954). Thiseffect was initially demonstrated in the cat in-testine but also occurs in the human intestine(Daniel, Sutherland and Bogoch, 1959).
Drugs Stimulating Motility. The injection ofprostigmine results in a moderate increase in thefrequency and amplitude of the propagated wavesin the small intestine (McMahon, Code, Sauer andBargen, 1949; Kewenter and Kock, i960). Thatthese waves are propulsive has been demonstratedby barium studies (Liljedahl, Mattsson and Per-now, 958a) and by direct observation ofileostomies(Schwartz, Reingold and Necheles, 1942). Mech-olyl also causes an increase in propulsive motilityin adults (Ginsberg and Miller, 1953) and inchildren (Barbero, Chin Kim and Davis, 1958).
Morphine. The effect of morphine on the smallintestine has been reviewed by Vaughan Williams(I954). Manometrically, in the jejunum, morphineproduces a rise in base-line sustained over severalminutes on which fast waves may be superimposed
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

712 POSTGRADUATE MEDICAL JOURNAL December I961
(Rowlands, Chapman, Taylor and Jones, 195ob;Kewenter and Kock, i960). Similarly, in theterminal ileum it does not reduce the total activity,but increases the percentage of rhythmic smallwaves and almost eliminates the large waves (Code,Rogers, Schlegel, Hightower and Bargen, I957).Daniel, Sutherland and Bogoch (I959) showed thatthe morphine-induced spasm is abolished byatropine, but not by vagotomy or by large dosesof hexamethonium. Morphine does not, however,stimulate either the human or dog ileum in vitro.These authors conclude that the spasm could beproduced both through a direct effect on smoothmuscle and by a central effect mediated by theautonomic nerves. It is also known that morphineincreases the transit time of the small intestine(Rowlands, Chapman, Taylor and Jones, I95ob;Grebell, I958), but this is not due to a generalizeddepression of small intestinal motility, but to thereduction in propulsive activity (Vaughan Williamsand Streeten, 1950), together with spasm prevent-ing the onward passage of chyme. VaughanWilliams and Streeten (1950) showed that in con-scious dogs morphine is a more powerful inhibitorof intestinal propulsion than amidone and thatpethidine has the least effect.
Unfortunately, no drug is available whose soleeffect is to increase the normal segmenting activityof the small intestine. On theoretical grounds it islikely that such a drug would be of great valueclinically in controlling intestinal hurry. At presentthe nearest approach to the ideal is morphine andits derivative, codeine, which is widely used forthis purpose.
5-hydroxytryptamine (5 H.T., Serotonin). Fol-lowing the discovery that argentaffin tumours con-tained large quantities of serotonin it was postu-lated that the diarrhea associated with the con-dition was the result of the excess circulating hor-mone. This finding stimulated investigation intothe effects of 5 H.T. on the intestinal musculature.In vitro, Bulbring and Lin (1958) demonstratedthat 5 H.T. derived from the intestinal mucosais released from the ileum of the guinea pig inresponse to a rise in intraluminal pressure. Applic-ation of 5 H.T. to the mucosal surface of thebowel resulted in an increase in peristalsis, where-as application to the serosal surface diminishedperistalsis. They postulated that serotonin sensi-tized pressure receptors in the intestinal mucosa.Experiments in the intact animal (Bulbringand Crema, 1959) gave less definite results.Intraluminal application failed to give aresponse and intravenous administration in-creased segmenting movements, but not pro-pulsion. They attributed the failure to obtain aresponse in the intact animal partly to excessivedesensitization of the sensory nerve ending and
partly to the destruction of 5 H.T. by amineoxidase. In man, when given orally even in largedoses, 5 H.T. has no effect (Hendrix, Atkinson,Clifton and Inglefinger, i957; Connell, Rowlandsand Wilcox, I960) on intestinal motility, but whenadministered intravenously a temporary rise inbase-line with superimposed fast waves has beennoted (Hendrix, Atkinson, Clifton and Inglefinger,1957). Haverback and Davidson (I958) obtaineda similar response with the serotonin precursor,5-hydroxytryptophan, and showed that the effectcould not be inhibited by atropine, but was an-tagonized by 2-bromolysergic acid diethylamide(BOL). Daniel, Honour and Bogoch (i960), re-cording both mechanical and electrical responsesto intravenous serotonin, confirmed these findingsand concluded that the effect of serotonin on thesmall intestine was a direct one and not mediatedby any other known intestinal stimulant. In spiteof these studies, the exact role of 5 H.T. in gastro-intestinal physiology remains in doubt.
Substance P. Substance P is a pharmacologicallyactive material distinct from histamine, serotoninor acetylcholine, which can be extracted from theintestinal wall with a motor effect on isolatedintestinal muscle (Pernow, I95I). Liljedahl,Mattsson and Pernow (i958b) have shown thatinjection of substance P results in an increase insmall intestinal movements, producing more pro-pulsive activity than prostigmine. It is claimedthat greater quantities of substance P than normalcan be extracted from the small intestine of patientswith the dumping syndrome (Wallensten, Garsten,Johnson and Salzman, I959). It is difficult to see,however, how significant progress in our under-standing of the role of this material can be madeuntil it is prepared in purer form, if, indeed, thepharmacological actions described are, in fact, theeffect of a single substance.
Motility and AbsorptionIt is frequently assumed that altered states of
intestinal motility affect absorption from the gut,but there is little experimental evidence for this.In an attempt to determine the relationship,Cummins and Almy (1953) estimated the uptakeof glucose and methionine from the bowel by adirect method during periods of normal motilityand periods of hypermotility induced by urecholineand physostigmine. They rather hesitantly con-cluded that absorption of these substances wasincreased during periods of increased activity.Grossier and Farrar (i960), using both the radiopill and tube methods, attempted to correlate theuptake of 24Na and small intestinal motility, butwere able to show no more than a possible re-lationship between segmental activity and 24Nauptake. Conversely, Higgins, Code and Orvis
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

December i961 CONNELL: The Motility of the Small Intestine 7
(1956) in a careful study reported a decrease in therate of absorption of deuterium-labelled water and24Na following reduction of small intestinal motilityby banthine. Rapid transit is frequently in-criminated as a cause of malabsorption, althoughevidence on the point is almost non-existent.
There is a generalized reduction in the pressurechanges of the small intestine in idiopathicsteatorrhoea in relapse (Inglefinger and Moss, 1943;Fink, 1959) although Barbero, Chin Kim andDavis (1958) were unable to show any differencein the pressure patterns of coeliac children as com-pared with normal. There is also a delay in thetransit of barium through the small intestine insprue (Golden, I950). Although in our ownlaboratory we have confirmed the marked decreasein intra-luminal pressure changes in idiopathic
steatorrhcea we have at the same time noted phasicalterations on signal strength of the radio pilloccurring continuously over long periods indicat-ing gentle rocking movements of the pill. Thesecan be confirmed fluoroscopically. The intestinein idiopathic steatorrhcea is not totally inactive butperhaps it is not generating sufficient power toproduce normal segmenting movements (Connell,Misiewicz and Rowlands, I96i). It is not possibleto say whether this is a primary or secondary effect,but the interesting observation of Schneider,Bishop and Shaw (i960) that gluten inhibitsperistalsis in smooth muscle in vitro tends tosupport the secondary nature of the musculardefect in steatorrhcea. This aspect of intestinalmotility is particularly poorly studied and onewhich will almost certainly repay further work.
REFERENCESABBOTT, W. O., HARTLINE, H. K., HERVEY, J. P., INGLEFINGER, F. J., RAWSON, A. J., and ZETZEL, L. (1943): Intubation
Studies of the Human Small Intestine: XXI. A Method for Measuring Intraluminal Pressures and its Applicationto the Digestive Tract, J. clin. Invest., 22, 22i.
AGOSTONI, E., CHINNOCK, J. E., DALY, M. DE BURGH, and MURRAY, J. G. (1957): Functional and Histological Studiesof the Vagus Nerve and its Branches to the Heart, Lungs and Abdominal Viscera of the Cat, 7. Physiol., 135, i82.
ALVAREZ, W. C. (I915): The Rate of Rhythmic Contraction in the Small Intestine of the Rabbit, Amer. J. Physiol.,37, 267., HosoI, KIYOSHI, OVERGARD, A., and ASCANIO, H. (1929): The Effects of Degenerative Section of the Vagi and theSplanchnics on the Digestive Tract, Ibid., 90, 631.(I950): The Muscular Versus the Nervous Origin of the Rhythmic Contractions of the Gut, chapter X, in 'AnIntroduction to Gastroenterology ', 4th edition. London: Heinemann.
ANDREW, R. (1954): Gastric, Duodenal and Jejunal Motility in Man: Physiological Studies by Balloon Kymography,Aust. J. exp. Biol., 32, 479.
ARMSTRONG, H. T., MILTON, G. W., and SMITH, A. W. (1956): Electropotential Changes in the Small Intestine,J. Physiol., 131, I47.ATKINSON, M., EDWARDS, D. A. W., HONOUR, A. J., and ROWLANDS, E. N. (1957): Comparison of Cardiac and Pyloric
Sphincter, Lancet, 273, 918.BARBERO, G. J., CHIN KIM, I., and DAVIS, J. (1958): Duodenal Motility Patterns in Infants and Children, Paediatrics,
22, 1054.BARGEN, J. A., WESSON, H. R., and JACKMAN, R. J. (1940): Studies in the Ileocecal Junction, Surg. Gynec. Obstet.,
7I, 33-BAYLISS, W. M., and STARLING, E. H. (1899): The Movements and Innervation of the Small Intestine, J. Physiol., 24, 99.BINGHAM, J. R., INGLEFINGER, F. J., and SMITHWICK, R. H. (1950): The Effects of Sympathectomy on the Motility
of the Human Gastrointestinal and Biliary Tract, Gastroenterology, I5, 6.BOEKE, J. (1940): ' Problems of Nervous Anatomy '. London: Oxford University Press.BULBRING, E., LIN, R. C. Y., and SCHOFIELD, G. (1958): An Investigation of the Peristaltic Reflex, in Relation to
Anatomical Observations, Quart. J. exp. Physiol., 43, 26., (I958): The Effect of Intraluminal Application of 5-Hydroxytryptamine and 5-Hydroxytryptophan on Peri-stalsis: The Local Production of 5-HT and its Release in Relation to Intraluminal Pressure and Propulsive Activity,J. Physiol., 140, 381., and CREMA, A. (1959): The Action of 5-Hydroxytryptamine, 5-Hydroxytryptophan and Reserpine on IntestinalPeristalsis in Anaesthetized Guinea Pigs, Ibid., 146, 29.
CANNON, W. B. (1905): Auscultation of the Rhythmic Sounds Produced by the Stomach and Intestines, Amer. J.Physiol., I4, 339.CASTLETON, K. B. (1934): An Experimental Study of the Movements of the Small Intestine, Ibid., 107, 641.CHANG, P. Y., and Hsu, F. Y. (1942): Localization of the Intestino-intestinal Reflex Arc, Quart. Y. exp. Physiol., 31, 311.CHAPMAN, W. P., STANBURY, J. B., JONES, C. M., and DENNISON, A. Y. (1948): The Effect of Tetraethyl Ammonium
on the Small Bowel in Man, 3. clin. Invest., 27, 346., PELAZZO, W. L., TAYLOR, A., and PROUDFOOT, W. (1949): Multiple Balloon Kymograph Recording of IntestinalMotility in Man with Observations on the Correlation of the Tracing Patterns with Barium Movements, Ibid.,28, 1517., ROWLANDS, E. N., TAYLOR, A., and JONES, C. M. (1950): Multiple Balloon Kymograph Recording of Variationsin Motility of the Upper Small Intestine in Man During Long Observation Periods Before and After PlaceboAdministration, Gastroenterology, 15, 341.
,, and JONES, C. M. (I950): Multiple Balloon Kymographic Recording of the Comparative Action of OralAdministration of Atropine, Tincture of Belladonna and Placebos on the Motility of the Upper Small Intestinein Man, New Engl. J. Med., 243, I.
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

714 POSTGRADUATE MEDICAL JOURNAL December I961
--, FRENCH, A. B., HOFFMAN, P. S., and JONES, C. M. (I952): Multiple Balloon Kymograph Recording of the Effectof Banthine, Belladonna and Placebos on Upper Intestinal Motility, Ibid., 246, 435.
CHAUDHARY, N. A., and TRUELOVE, S. C. (I96I): Colonic Motility: A Critical Review of Methods and Results, Amer.J. Med., 31, 86.
CHILDREY, J. H., ALVAREZ, W. C., and MANN, F. C. (1930): Digestion: Efficiency with Various Foods and underVarious Conditions, Arch. intern. Med., 46, 361.
CODE, C. F., HIGHTOWER, N. C., and MORLOCK, C. G. (I952): The Motility of the Alimentary Tract in Man, Amer.J. Med., 13, 328., WILKINSON, G. R., and SAUER, W. G. (1954): Normal and Some Abnormal Colonic Motor Patterns in Man,Ann. N. Y. Acad. Sci., 58, 317.
--, ROGERS, A. G., SCHLEGEL, J., HIGHTOWER, N. C., and BARGEN, J. A. (1957): Motility Patterns in the TerminalIleum: Studies in Two Patients with Ulcerative Colitis and Ileal Stoma, Gastroenterology, 32, 65I.
CONNELL, A. M., ROWLANDS, E. N., and WILCOX, P. B. (I960): Serotonin, Bananas and Diarrhcea, Gut, I, 44., (960): Wireless Telemetering from the Digestive Tract, Ibid., I, 266.
-(96a): The Motility of the Pelvic Colon: Motility in Normals and in Patients with Asymptomatic DuodenalUlcer, Ibid., 2, I75.(I96Ib): Localization of Ingested Telemetering Capsules, Lancet, i, 557.
, and ROWLANDS, E. N. (i96i): Clinical Application of Radio Pill for Measuring Gastro-intestinal Pressure, in' Proceedings of the Third International Conference on Medical Electronics ', p. I26. London:, MIsIEwICz, J. J., and ROWLANDS, E. N. (1961): In preparation.
CUMMINS, A. J., and ALMY, T. P. (1953): Studies on the Relationship between Motility and Absorption in the HumanSmall Intestine, Gastroenterology, 23, 179.
DANIEL, E. E., SUTHERLAND, W. H., and BOGOCH, A. (1959): Effects of Morphine and other Drugs on the Motility ofthe Terminal Ileum, Ibid., 36, 510.
--, and BOGOCH, A. (1959): The Mechanism of the Spasmogenic Action of Morphine on the Small Intestine ofMan and Dog, in' Proceedings of the World Congress of Gastroenterology, Washington, 1958 ', p. 138. Baltimore:Williams and Wilkins., CARLOW, D. R., WACHTER, B. T., SUTHERLAND, W. A., and BOGOCH, A. (1959): Electrical Activity of the SmallIntestine, Gastroenterology, 37, 268.
--, HONOUR, A. J., and BOGOCH, A. (1960): Antagonism of Serotonin Induced Contraction and Electrical Activity inthe Ileum, Ibid., 39, 62.
DOUGLAS, O. M., and MANN, F. C. ( 939a): An Experimental Study of the Rhythmic Contractions in the Small Intestineof the Dog, Amer. J. dig. Dis., 6, 3 8.
( 939b): The Activity of the Lower Part of the Ileum of the Dog in Relation to the Ingestion of Food,Ibid., 6, 434.
(940): The Gastro-ileac Reflex: Further Experimental Observations, Ibid., 7, 53.(1948): The Activity of the Duodenum, J. Physiol., 107, 472.(I949): The Decrease in Frequency of Contraction of the Jejunum after Transplantation to the Ileum, Ibid.,10o, 66.
DREYER, N. B. (I954): Rebound Effects on the Cat's Intestine, Arch. int. Pharmacodyn., 97, 54.Du PLEISSIS, D. J. (I954): Clinical Observations on Intestinal Motility, S. Afr. med. J., 28, 27.EDWARDS, D. A. W., and ROWLANDS, E. N. (1960): An Air Filled Metal Capsule Optical Manometer System, in ' Pro-
ceedings of the Second Internation Conference on Medical Electronics, Paris, 1959 ', p. 307., -((1961): Unpublished studies.
ELSOM, K. A., GLENN, P. M., and DROSSNER, J. L. (I939): Intubation Studies of the Small Intestine: The Effect ofPitressin and Amphetamine (Benzedrine) Sulphate on Motor Activity of Small Intestine and Colon, Amer. J.dig. Dis., 6, 593.
FARRAR, J. T., and INGLEFINGER, F. J. (1955): Gastrointestinal Motility as Revealed by Study of Abdominal Sounds,Gastroenterology, 29, 789.
-, ZWORYKIN, V. K., and BAUM, J. (1957): Pressure Sensitive Telemetering Capsule for the Study of Gastro-intestinal Motility, Science, 126, 975.
--, and BERNSTEIN, J. S. (1958): Recording of Intraluminal Gastrointestinal Pressures by a Radio TelemeteringCapsule, Gastroenterology, 35, 603.
-, and DAVIDSON, M. (I960): The Measurement of Gastrointestinal Motility in Man, in 'Methods on MedicalResearch ', 8, 200.
FINK, S. (1959): The Intraluminal Pressures in the Intact Human Intestine, Gastroenterology, 36, 66i.FOULK, W. T., CODE, C. F., MORLOCK, C. G., and BARGEN, J. A. (1954): A Study of the Motility Patterns and the
Basic Rhythm of the Duodenum and Jejunum in Human Beings, Ibid., 26, 6oi.GARRY, R. C., and GILLESPIE, J. S. (I955): The Responses of the Musculature of the Colon of the Rabbit to Stimulation,
in vitro, of Parasympathetic and of the Sympathetic Outflows, J7. Physiol., x28, 557.GARVEN, H. S. D. (1957): 'A Student's Histology '. Edinburgh: E. and S. Livingstone.GAUER, 0. H., and GIENAPPE, E. A. (1950): A Miniature Pressure Recording Device Devised for Cardio Vascular
System Research, Science, 112, 404.GINSBERG, M., and MILLER, J. M. (1953): Physiologic Observations on a Segment of Normal Human Jejunum, Gastro-
enterology, 24, 307.GOLDEN, R. (1950): Some Clinical Problems in Small Intestinal Physiology: Mackenzie-Davidson Memorial Lecture,
Brit. J. Radiol., 23, 390.GREBELL, F. S. (I958): Some Radiological Observations on the Effect of Morphine Sulphate on the Gastrointestinal
Tract in Man, Ibid., 31, 534.GREGORY, R. A. (1950): Some Factors Influencing the Passage of Fluid Through Intestinal Loops in Dogs, J. Physiol..
III, 119.
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

December I961 CONNELL: The Motility of the Small Intestine 715
GROSSIER, V. W., and FARRAR, J. T. (I960): Absorption of Radioactive Sodium from the Intestinal Tract of Man:I. Effect of Intestinal Motility; II. Effect of an Organomercurial, 3J. clin. Invest., 39, I607.
HARPER, A. A., KIDD, C., and SCRATCHERD, T. (1959): Vago-vagal Reflux Effects on Gastric and Pancreatic Secretionand Gastrointestinal Motility, J. Physiol., 148, 417.
HAVERBACK, B. J., and DAVIDSON, J. D. (I958): Serotonin and the Gastrointestinal Tract, Gastroenterology, 35, 570.HENDRIX, J. R., ATKINSON, M., CLIFTON, J. A., and INGLEFINGER, F. J. (1957): The Effect of 5-Hydroxytryptamine in
Intestinal Motor Function in Man, Amer. J. med., 23, 886.HERTZ, A. F. (I913): The Ileo-Caecal Sphincter, J. Physiol., 47, 54.HIGGINS, J. A., CODE, C. F., end ORVIS, A. L. (i956): The Influence of Motility on the Rate of Absorption of Sodium
and Water from the Small Intestine of Healthy Persons, Gastroenterology, 31, 708.HIGHTOWER, N. C., JR. (1952): Comparison of Intraluminal Pressures and Motility Patterns in the Gastrointestinal
Tract of Human Beings when Recorded by Balloons and Direct (Electrical Transducer) Pressure System, Fed.Proc., Ix, 69.
IGGO, A. (1957): Gastrointestinal Tension Receptors with Unmyelinated Afferent Fibres in the Cat, Quart. J. exp.Physiol., 42, I30.
INGLEFINGER, F. J., and ABBOTT, W. 0. (1940): Intubation Studies of the Human Small Intestine: The DiagnosticSignificance of Motor Disturbance, Amer. J. dig. Dis., 7, 468., and Moss, R. E. (1943): The Motility of the Small Intestine in Sprue, J. clin. Invest., 22, 345.
IvY, A. C., GROSSMAN, M. I., and BACHRACH, W. H. (I950): Peptic Ulcer, Chapter XII, in 'Role of the NervousSystem ', p. 412. Philadelphia: The Blakiston Co.
KAY, A. W. (I960): Some Surgical Aspects of the Malabsorption Syndrome, Brit. med. J., i, I291.KEWENTER, J., and KOCK, N. G. (i960): Motility of the Human Small Intestine: A Method for the Continuous
Recording of Intraluminal Pressure Variations, Acta chir. scand., 119, 430.LEPORE, M. J., GOLDEN, R., and FLOOD, C. A. (195I): Oral Banthine, an Effective Depressor of Gastrointestinal
Motility, Gastroenterology, 17, 551.LILJEDAHL, S. O., MATTSSON, O., and PERNOW, B. (I958a): Cineroentgenography of the Intestine with Special Reference
to the Effect of Stimulating Agents upon Motility, Acta Radiologica, 49, 348.--, -, (I958b): The Effect of Substance P. on Intestinal Motility in Man, Scand. Y. clin. Lab. Invest., 10, i6.LORBER, S. H., and SHAY, H. (1954): Technical and Physiological Considerations in Measuring Gastrointestinal
Pressures in Man, Gastroenterology, 27, 478.LOUCKES, H., QUIGLEY, J. P., and ROMANS, W. E. (1953): Sounds at the Pyloric Sphincter, Fed. Proc., 12, 91.MACEWAN, W. (1904): The Function of the Caecum and Appendix, Lancet, ii, 995.MACKAY, R. S., and JACOBSON, B. (1957): Endoradiosonde, Nature, 179, 1239.MCMAHON, J. M., CODE, C. F., SAUER, W. G., and BARGEN, J. A. (1949): A Study of the Action of Prostigmine on the
Bowel of Human Beings, Gastroenterology, 12, 970.MILTON, G. W., and SMITH, A. W. M. (1956): The Pacemaking Area of the Duodenum, J. Physiol., 132, 1oo.MORIN, G., and VIAL, J. (1934): Reactions Respiratoires et Circulatoires provoqu6es par la Distension brusque de l'in-
testine chez le Chien, Arch. int. Physiol., 38, 428.ODDONE, I., DE LA PIERRE, M., BERTERO, R., and JONA, E. (i959): Prime Osservazioni sulla Duodenografia, ' Estratto
da Minerva medica ', p. I.OPPENHEIMER, A. (1940): The Ileo-caecal Region, Radiology, 34, 545.PAINTAL, A. S. (1954): The Response of Gastric Stretch Receptors and Certain Other Abdominal and Thoracic Vagal
Receptors to some Drugs, J. Physiol., 126, 271.PERNOW, B. (1951): Substance P Distribution on the Digestive Tract, Acta physiol. scand., 24, 97.POSEY, E. L., BARGEN, J. A., DEARING, W. H., and CODE, C. F. (1948): The Effects of So-called Antispasmodics on
Intestinal Motility, Gastroenterology, II, 344., (195I): Observations of Normal and Abnormal Human Intestinal Motor Function, Amer. J. med. Sci.,221, I 0.
QUIGLEY, J. P., and BRODY, D. A. (1952): Physiologic and Clinical Considerations of Pressures developed in the DigestiveTract, Amer. J. Med., 13, 73.
RIDGEWAY, M., and SMITH, A. N. (I96I): The Management of Recording Pressure Changes in the GastrointestinalTract using Telemetering Capsule, J. roy. Coll. Surg. Edin., 6, 192.
Ross, J. R., and BROLSMA, M. P. (I951): Splanchnicectomy: Its Clinical Effects on the Gastrointestinal Tract, Gastro-enterology, 17, 389.
ROWLANDS, E. N. (1959): Measurement of the Effect of Drugs on the Gastrointestinal Tract, in ' Quantitative Methodsin Human Pharmacology and Therapeutics ', p. 31. Oxford, London, New York and Paris: Pergamon Press., CHAPMAN, W. P., TAYLOR, A., and JONES, C. M. (i95oa): Multiple Balloon Kymograph Recording of the Actionof Syntropan and of Trasentin on the Motility of the Upper Small Intestine in Man, Surg. Gynec. Obstet., 91, 513., , -, (I95ob): Multiple Balloon Kymograph Recording of the Comparative Action of Morphine andPlacebos on the Motility of the Upper Small Intestine in Man, Ibid., 91, 129.
--, HONOUR, A. J., EDWARDS, D. A. W., and CORBETT, B. D. (1953): Metal Capsule Optical Manometer for measuringPressures in the Human Gut with an open-ended Tube, Clin. Sci., 12, 299., and WOLFF, H. S. (i960): The Radio Pill, British Communications and Electronics, 7, 598.
SCHNEIDER, R., BISHOP, H., and SHAW, B. (i960): The Inhibition of the Peristaltic Reflex by Substances from ProteinSources, Brit. J. Pharmacol., 15, 219.
SCHWARTZ, A. H., REINGOLD, I., and NECHELES, H. (1942): Study of the Mechanism of Action of Prostigmin on In-testinal Motility in Human Beings and in the Dog, Surgery, II, 746.
SMITH, H. W., TEXTER, E. C., STICKLEY, J. H., and BARBORKA, C. J. (1957): Intraluminal Pressures from the UpperGastrointestinal Tract: II. Correlations with Gastro Duodenal Motor Activity in Normal Subjects and Patientswith Ulcer Distress, Gastroenterology, 32, 1025.
TEMPLETON, R. D., and LAWSON, H. (1931): Studies in the Motor Activity of the Large Intestine: I. Normal Motilityin the Dog, recorded by the Tandem Balloon Method, Amer. if. Physiol., 96, 667.
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from

716 POSTGRADUATE MEDICAL JOURNAL December x961
THIRY, L. (1864): Uber eine Neue Methode den Dumdamrn zu Isolieren, S.-B. Akad. Wiss. Wien., math.-nat. Kl.,50, 77.
THOMAS, J. E., and MOGAN, C. H. (1931): The Enterogastric Reflex, Proc. Soc. exp. Biol. Med., 28, 968.VAN LIERE, E. J., STICKNEY, J. C., and NORTHUP, D. W. (1945): The Rate of Progress of Inert Material Through the
Small Intestine, Gastroenterology, 5, 37.VAUGHAN WILLIAMS, E. M. (1954): The Mode of Action of Drugs Upon Intestinal Motility, Pharmacol. Rev., 6, I59.
, and STREETEN, D. H. P. (1950): The Action of Morphine, Pethidine and Amidone upon the Intestinal Motilityof Conscious Dogs, Brit. J. Pharmacol., 5, 584.
VELLA, L. (i888): Neues Varfahren zur Gewinnung reinen Darmsaftes und Feststellung seine Physiologischen Einger-schaften, ' Moleschott's Untersuchungen zur Naturlehre der Menschen med der Thiere ', 13, 40.
WALLENSTEN, S., GARSTEN, P., JOHNSON, M., and SALZMAN, G. F. (i959): The Dumping Syndrome: I. Roentgencinemato-graphic Study of the Motility of the Small Intestine in the Dumping Syndrome following Partial Gastrectomy,Acta chir. scand., II8, 117.
WHITTERIDGE, D. (1956): The Effects of Distension of Viscera, ' Lectures on the Scientific Basis of Medicine', Vol.IV, 1954-55, p. 305. London: Athlone Press.
YOUMANS, W. B. (I944): The Intestino-intestinal Inhibitory Reflex, Gastroenterology, 3, I114.(1952): Neural Regulation of Gastric and Intestinal Motility, Amer. J. med., 13, 209.
Protected by copyright.
on Novem
ber 23, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.434.703 on 1 Decem
ber 1961. Dow
nloaded from