Embed Size (px)
DESCRIPTION
Our mission is to enhance your ability to practice equine medicine by providing the latest info you need.
Citation preview
Vol 6 Issue 2 2016www.modernequinevet.com
Recommendation helps find early PPIDTaking a good skin sample for the labTechnician Update: Successful management of pleural pneumonia
Equine VetThe Modern
BEVA Congress:
Kickstartwound healing
2 Issue 2/2016 | ModernEquineVet.com
Table of ConTenTs
EndocrInologyTest recommendation helps find early PPId ..............................................................10
dErMaTologySkin sampling: Prep it right for the lab .........................................................................12
TEchnIcIan uPdaTESuccessful management of pleural pneumonia .......................................................14
nEwShappy or angry? your horse Knows ..............................................3Fda approves dewormer for use in Broodmares ................18qPcr confirms EhV-5 in horses with respiratory distress .............................................................................19
Share this issue with your colleague. he or She can sign up here FrEE.
LEGAL DISCLAIMER: The content in this digital issue is for general informational purposes only. PercyBo Publishing Media LLC makes no representations or warranties of any kind about the completeness, accuracy, timeliness, reliability or suitability of any of the information, including content or advertisements, contained in any of its digital content and expressly disclaims liability of any errors or omissions that may be presented within its content. PercyBo Publishing Media LLC reserves the right to alter or correct any content without any obligations. Furthermore, PercyBo disclaims any and all liability for any direct, indirect, or other damages arising from the use or misuse of the information presented in its digital content. The views expressed in its digital content are those of sources and authors and do not necessarily reflect the opinion or policy of PercyBo. The content is for veterinary professionals. ALL RIGHTS RESERVED. Reproduction in whole or in part without permission is prohibited.
Kick start wounds to aid healing
coVEr STory:
4Cover photo courtesy of R. Jim Schumacher
SaleS: Matthew Todd • [email protected]
eDIToR: Marie rosenthal • [email protected]
aRT DIRecToR: Jennifer Barlow • [email protected]
conTRIbUTIng wRITeRS: Paul Basillo • Kathleen ogle
coPY eDIToR: Patty wall
Published by
p E r c y b omedia publishing
Equine VetThe Modern
aDveRTISeRSShanks Veterinary Equipment ................................. 3Merck animal health ................................................. 5Standlee Premium western Forage ........................ 7
avalon Medical ............................................................ 8Electric hoof Knife ...................................................... 9aaEVT ...........................................................................15
PO Box 935 • Morrisville, PA 19067Marie Rosenthal and Jennifer Barlow, Publishers

ModernEquineVet.com | Issue 2/2016 3
Horses appear to be able to distinguish between an-gry and happy human facial expressions, according to a recent study.
psychologists studied how 28 horses reacted to seeing photographs of positive versus negative hu-man facial expressions. The horses were recruited from five riding or livery stables in Sussex and Sur-rey, UK, between April 2014 and February 2015. They were shown happy and angry photographs of two unfamiliar male faces. The experimental tests examined the horses' spontaneous reactions to the photos, and the experimenters were blinded to which photographs they were displaying to avoid influencing the horses.
When viewing angry faces, horses looked more with their left eye, a behavior associated with per-ceiving negative stimuli. Their heart rate also in-creased more quickly and they showed more stress-related behaviors. The researchers concluded that this response indicated that the horses had a func-tionally relevant understanding of the angry faces they were seeing.
“What's interesting about this research is that it shows that horses have the ability to read emotions across the species barrier. We have known for a long time that horses are a socially sophisticated species but this is the first time we have seen that they can distinguish between positive and negative human facial expressions,” said Amy Smith, a doctoral stu-dent in the Mammal Vocal communication and cognition research Group at the University of Sus-sex who co-led the research.
“The reaction to the angry facial expressions was particularly clear — there was a quicker increase in their heart rate, and the horses moved their heads to look at the angry faces with their left eye,” said Ms. Smith
research shows that many species view negative events with their left eye because the right brain hemisphere processes threatening stimuli and in-formation from the left eye is processed in the right hemisphere.
A tendency for viewing negative human facial expressions with the left eye specifically has also been documented in dogs. MeV
Happy or angry? Your Horse Knows
news noTes
For more information:
Smith AV, Proops L, Grounds K, et al. Functionally relevant responses to human facial expressions of emotion in the domestic horse (Equus caballus). Biology Letters, 2016 DOI: 10.1098/rsbl.2015.0907 www.shanksvet.com • [email protected]
Lifting Large Animals Since 1957
Shut
terst
ock/
Foto
kosti
c
B y M a r i e r o s e n t h a l , M S
When evaluating a wound, consider the stage the wound is in — inflammatory, debridement, repair or maturation — and how a veterinarian can kick start it into the next phase before beginning treatment, suggested a panel of experts at the british Equine Vet-erinary Association (bEVA) con-gress.
“Wound healing doesn’t move steadily from one phase to the next, and there are often overlap-ping phases. Think about what the impediments are to moving that wound to the next stage,” sug-gested Patrick Pollock, phD, se-
nior veterinary clinician Equine Surgery of the Weiper’s centre Equine Hospital, School of Vet-erinary Medicine at the University of Glasgow. Impediments, such as infection, hypergranulation and repeated trauma, should be man-aged before the wound can prog-ress to the next healing stage.
“I think as a profession, we don’t do wounds very well. We tend to think about what we can buy to put on the wound or what dressings we have in our cup-board instead of thinking two basic questions: What stage is the wound in and what are the things
Imag
es co
urte
sy of
R. Ji
m Sc
hum
ache
r
CoVer sTory
4 Issue 2/2016 | ModernEquineVet.com
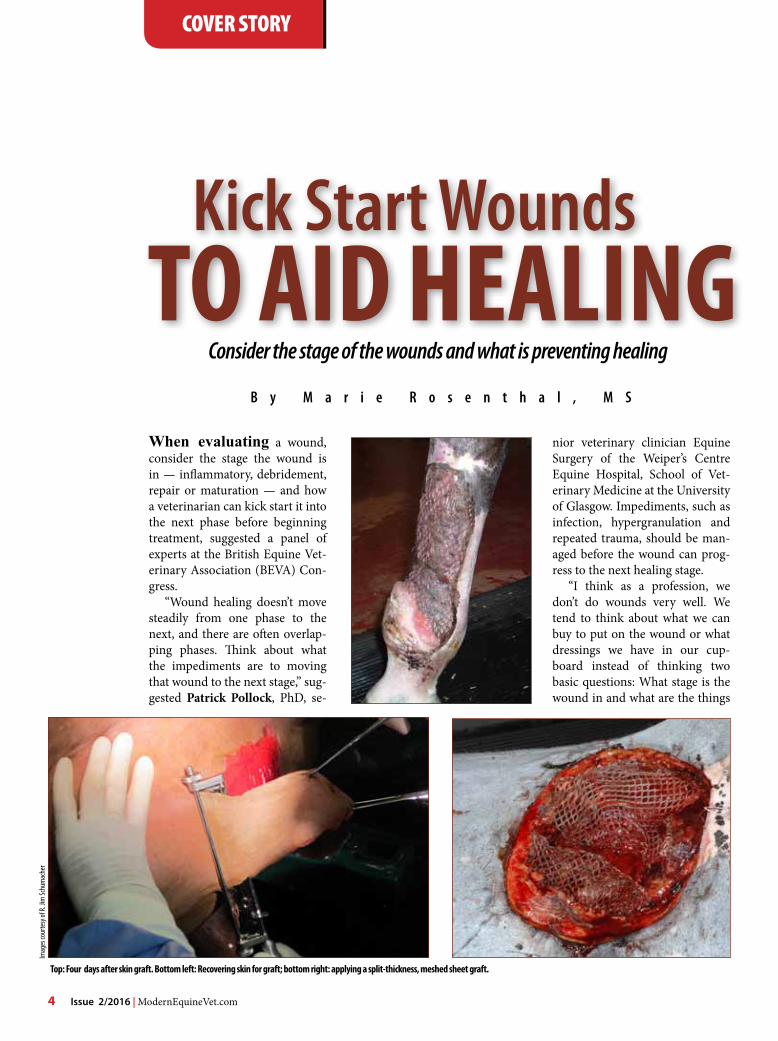
Top: Four days after skin graft. bottom left: Recovering skin for graft; bottom right: applying a split-thickness, meshed sheet graft.
Kick Start woundsTo aID HealIng
Consider the stage of the wounds and what is preventing healing

1 UC Davis (Nicola Pusterla) & Merck Animal Health. Infectious Upper Respiratory Surveillance Program. Ongoing Research 2008-present.
2 Townsend HGG. Onset of protection against live-virus equine influenza challenge following vaccination naive horses with a modified-live vaccine. Unpublished data.
Visit us online to learn more about Merck Animal Health and the equine products and programs that help you keep horses healthy.
The Science of Exceptional
The Science of Healthier Animals
2 Giralda Farms • Madison, NJ 07940 • merck-animal-health-usa.com • 800-521-5767Copyright © 2016 Intervet Inc., d/b/a/ Merck Animal Health, a subsidiary of Merck & Co., Inc.All Rights reserved. 51358 2/14/ EQ-1244
Stop flu where it starts.
Trust Flu Avert® I.N. for superior protection against relevant flu strains threatening the U.S. horse population.1
• Just ONE dose required - An ideal first flu vaccine for young horses - Provides protection at the site of infection
and long-lasting immunity• Proven safe and effective - Intranasal application leaves no risk for
injection site reactions to interfere with training or competing
• Rapid onset of protection - Onset of flu protection within five to
seven days following one dose – no matter when your horse was last vaccinated for flu.2
Now that’s exceptional.
To aID HealIng

that are stopping the wound from healing,” he said.
Many wounds need to be irri-gated and debrided, and most vet-erinarians turn to a “fancy piece of equipment” to accomplish this — a hose. Using a hose is some-what controversial, because some experts recommend sterile iso-tonic saline solution for lavaging and debriding the wound, but the panel seemed in agreement that a hose can be a useful and inexpen-sive method for wound cleaning.
“It seems reasonable to ac-complish what needs to be done cheaply rather than going to ster-ile saline physiological solutions,” said Debra Archer, bVMS, phD, certES(Soft Tissue), DEcVS, MrcVS, professor and head of Equine Surgery at the University of Liverpool.
Dr. pollock said that the large quantities of sterile fluids that are needed to manage a large wound might not be practical in the field. “I think the reality is that we live in the real world, and people keep horses in places where getting a lot
of sterile solution is difficult,” he said. “Tap water is certainly clean enough to put onto a wound … the necrotic debris and the con-tamination that you remove is far more detrimental to the wound than tap water.”
Many topical medications and bandages aid wound healing. In addition to traditional bandages, Dr. pollock discussed medical grade honey. Manuka medical grade honey not only keeps the wound moist, but also debrides the wound and aids wound heal-ing. “We use quite a lot of honey, and we use medical grade honey,” he said, “because we’ve seen some research that indicated you could get into trouble using household honey [due to contamination],” Dr. pollock said.
“owners are desperate to go to the store, buy a jar of honey and slap it on the wound with that. It is just that some honeys can be contami-nated during processing,” he said.
“There is a lot of work to do about honey, but my opinion, based on its use, is that it is ex-
CoVer sTory
6 Issue 2/2016 | ModernEquineVet.com
EA2
DISCOVER THE DIFFERENCE FOR YOUR HORSE OR FIND A STANDLEE DEALER ATWWW.STANDLEEFORAGE.COM
Standlee grows and manufactures the highest quality forage products available, which equine veterinarians and nutritionists strongly recommend feeding your horse.
Choose the best for your horse by feeding Standlee Premium Western Forage®.
Standlee carries Alfalfa, Timothy Grass, Orchard Grass, Alfalfa/Timothy Grass and Beet Pulp pellets.
TYPICAL COMPETITOR ALFALFA PELLETS STANDLEE PREMIUM ALFALFA PELLETSVS
HAY THERE!WHICH PELLETS WOULD YOU CHOOSE FOR YOUR HORSE?
Proud sponsor of:
an equine wound before and after the application of RediHeal, which provides a healing scaffold for the wound.
Imag
es co
urte
sy of
Avalo
n Med
ical
tremely good,” he said.However, because it does de-
bride tissue, honey should not be used during the repair stage when the wound begins to build the ma-trix for new skin; a veterinarian should recommend something else, such as a hydrogel bandage, which keeps the wound moist without the debriding properties.
“If I have granulation tissue, I would not use honey,” Dr. pollock said, “I would switch to hydrogel bandages.”
There was a discussion about packing large wounds, and again there can be disagreement among veterinarians about which wounds should be packed. It can be diffi-cult to pack a chest wound, for instance and keep it airtight, ex-plained Safia Barakzai, bVSc, MSc, cert ES (Soft Tissue), DESTS, DEcVS, MrcVS, a spe-cialist in Equine Surgery and se-nior lecturer in Equine Surgery at the royal (Dick) School of Vet-erinary Studies at the University of Edinburgh. Dr. pollock suggested using plastic food wrap to help keep the packing materials in and the wound airtight.
“Deep puncture wounds will also require systemic antibiotics because of the concern of infec-tion,” Dr. barakzai added.
Keep a close eye on puncture wounds, they warned because they can become contaminated, fill with fluid or lead to secondary conditions, such as pleuritis, de-pending on where they are located on the body.
Some wounds are too large to heal by secondary intention and skin grafting might be necessary, according to Jim Schumacher, DVM, MS, professor in the De-partment of Large Animal clini-cal Sciences, college of Veterinary Medicine, University of Tennessee.
There is a case to be made for grafting fresh wounds and a case

EA2
DISCOVER THE DIFFERENCE FOR YOUR HORSE OR FIND A STANDLEE DEALER ATWWW.STANDLEEFORAGE.COM
Standlee grows and manufactures the highest quality forage products available, which equine veterinarians and nutritionists strongly recommend feeding your horse.
Choose the best for your horse by feeding Standlee Premium Western Forage®.
Standlee carries Alfalfa, Timothy Grass, Orchard Grass, Alfalfa/Timothy Grass and Beet Pulp pellets.
TYPICAL COMPETITOR ALFALFA PELLETS STANDLEE PREMIUM ALFALFA PELLETSVS
HAY THERE!WHICH PELLETS WOULD YOU CHOOSE FOR YOUR HORSE?
Proud sponsor of:

CoVer sTory
8 Issue 2/2016 | ModernEquineVet.com
to be made for grafting granulat-ing tissue, he said. Grafts take better on fresh wounds, but a lot more skin needs to be harvested to graft a very large fresh wound, he explained. “The advantage to wait-ing until it begins to granulate is that the wound contracts making it much smaller, so less skin needs to be harvested,” he said.
Medical doctors tend to pre-fer grafting human wounds when they are fresh to preserve joint movement, but contraction is good in horses, he said. “body and neck wounds of horses heal pri-marily by contraction.”
In addition, grafting can kick start a wound that is not progress-ing to the next stage, he said. “I
think applying a graft to a wound that is not healing very well adds elements to the healing, like cyto-kines, thus stimulating contrac-tion and epithelialization,” Dr. Schumacher said.
In one case he discussed, the horse had been badly burned in a barn fire and required large grafts, even after waiting for the forma-
Imag
es co
urte
sy of
Dr. P
atric
k Poll
ock.
Progression of wound treated with manual debridement with a hose and a honey dressing, the first to last picture are 4 weeks apart.
HORSES • COWS • GOATS • SHEEP
“Hoof Trimming Just Got Easier”
Better Hoof HealthHassle Free Trimming
Smoother ResultsEasy & Pain-Free
Lightweight & Durable
877-320-8203ElectricHoofKnife.US
ModernEquineVet.com | Issue 2/2016 9
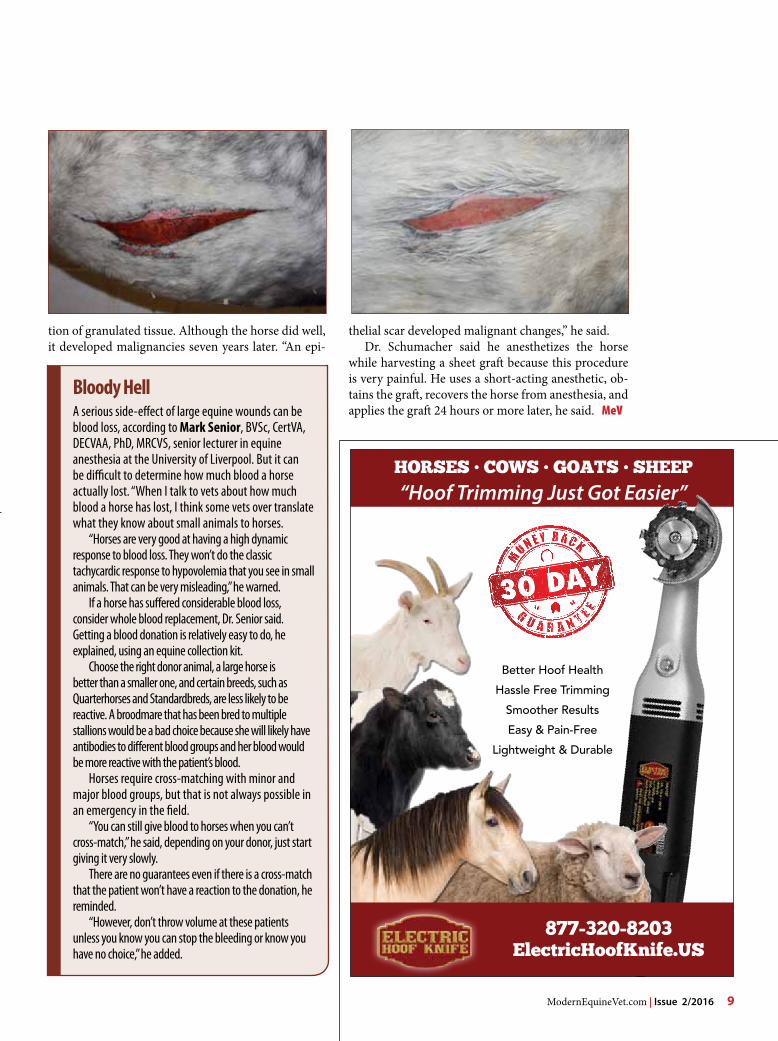
bloody HellA serious side-effect of large equine wounds can be blood loss, according to Mark Senior, BVSc, CertVA, DECVAA, PhD, MRCVS, senior lecturer in equine anesthesia at the University of Liverpool. But it can be difficult to determine how much blood a horse actually lost. “When I talk to vets about how much blood a horse has lost, I think some vets over translate what they know about small animals to horses.
“Horses are very good at having a high dynamic response to blood loss. They won’t do the classic tachycardic response to hypovolemia that you see in small animals. That can be very misleading,” he warned.
If a horse has suffered considerable blood loss, consider whole blood replacement, Dr. Senior said. Getting a blood donation is relatively easy to do, he explained, using an equine collection kit.
Choose the right donor animal, a large horse is better than a smaller one, and certain breeds, such as Quarterhorses and Standardbreds, are less likely to be reactive. A broodmare that has been bred to multiple stallions would be a bad choice because she will likely have antibodies to different blood groups and her blood would be more reactive with the patient’s blood.
Horses require cross-matching with minor and major blood groups, but that is not always possible in an emergency in the field.
“You can still give blood to horses when you can’t cross-match,” he said, depending on your donor, just start giving it very slowly.
There are no guarantees even if there is a cross-match that the patient won’t have a reaction to the donation, he reminded.
“However, don’t throw volume at these patients unless you know you can stop the bleeding or know you have no choice,” he added.
tion of granulated tissue. Although the horse did well, it developed malignancies seven years later. “An epi-
thelial scar developed malignant changes,” he said.Dr. Schumacher said he anesthetizes the horse
while harvesting a sheet graft because this procedure is very painful. He uses a short-acting anesthetic, ob-tains the graft, recovers the horse from anesthesia, and applies the graft 24 hours or more later, he said. MeV
10 Issue 2/2016 | ModernEquineVet.com
endoCrinology
B y T o m r o s e n t h a l
The Equine Endocrinology Group (EEG) has issued new rec-ommendations that veterinarians conduct the thyrotropin-releasing hormone (TrH) stimulation test to determine the levels of the adre-nocorticotropic hormone (AcTH) in horses to better diagnose horses with early signs of pituitary pars in-termedia dysfunction (ppID).
recent advancements in test-ing now enable the TrH stimula-tion test to more clearly identify the levels of AcTH in horses, ac-cording to Nicholas Frank, DVM, phD, DAcVIM, professor and de-partment chair at the cummings School of Veterinary Medicine at Tufts University, who serves as the coordinator for the five-year-old EEG.
The TrH stimulation test should be conducted by veterinarians from mid-November to mid-July, said Dr. Frank. reference ranges for the TrH stimulation test have not been established from mid-July to mid-November. A baseline blood sam-ple should first be obtained, imme-diately followed by 1 mL of IV TrH. A second sample is collected exactly 10 minutes later.
If the results from the laborato-ry show the horse’s hormone level at 10 minutes is above 110 pg/mL, then, according to EEG guidelines, the horse is positive for ppID, for-
merly called equine cushing’s dis-ease.
Dr. Frank said the EEG, which is comprised of clinicians and re-searchers from different countries, is continuing its research to determine the hormone levels indicating ppID at other months of the year to reflect horses’ seasonal endocrine activity. The EEG will be assembling again this summer to develop guidelines for diagnosing insulin dysregulation, a key component of equine metabol-ic syndrome (EMS) in horses.
The TrH stimulation test should not necessarily be admin-istered during a horse’s annual wellness exam, but when the horse shows early signs of early ppID, Dr. Frank said. He noted that the traditional resting AcTH test, while valuable in the diagnosis of moderate or advanced ppID, is not effective in diagnosing early ppID. The TrH stimulation test should replace the resting AcTH Test for early diagnosis of ppID in younger horses.
clinical signs of ppID can be found in horses from 10 years old until the end of a horse’s life. Dr. Frank said veterinarians should keep ppID in the back of their minds when examining a horse. The signs of early ppID are:
• Decreased athletic performance,
• Change in attitude/lethargy, • Delayed haircoat shedding, • Regional hypertrichosis, • Change in body conformation, • Regional adiposity and • Laminitis.
Steve Grubbs, DVM, phD, DAcVIM equine technical man-ager for boehringer Ingelheim Vetmedica Inc. (bIVI), the manu-facturer of prascend, said early signs of ppID may overlap other endocrine diseases, such as EMS. If a horse has delayed or localized shedding, abnormal sweating and/or laminitis the animal may have ppID. However, because ppID his-torically has not been considered in the initial list of differential diag-noses, especially in younger horses, experts believe the disease may go undiagnosed and untreated. A change in paradigm is needed, he said.
“The mental picture of ppID is that old horse with extremely long hair that just lacked shed-ding,” Dr. Grubbs said. “When we think about the early subtle signs, we have to rethink this. Look back over the years how we probably missed the subtle signs of ppID because we weren’t considering it, because we just didn’t know.”
Dr. Grubbs advised, “put ppID on your differential list.” To de-
identifies early PPIdTRH Stimulation Test
ModernEquineVet.com | Issue 2/2016 11
identifies early PPId
tect the subtle signs of ppID, “you have to actually put your hands on the horse. you can be looking
at the horse for other reasons. If you’re not thinking of early signs of ppID, you would miss it.” The
For more information on the EEG, including the Recommendations for the Diagnosis and Treatment of Pituitary Pars Intermedia Dysfunction (PPID) visit http://sites.tufts.edu/equineendogroup/
For more information:
early clinical signs of ppID should be in the back of a veterinarian’s mind regardless of the age of the horse, he said. If those early clini-cal signs are spotted, the TrH stimulation test can confirm ppID cases. Earlier diagnosis would re-sult in treatment administered earlier in the disease.
Dr. Grubbs said the top signs of early ppID that help him recognize the disease are decreased athletic performance and delayed hair coat shedding, which occurs all over the horse’s body in advanced ppID, but occur in patches and specific areas, such as on the sides of the neck and along the jugular groove in early disease.
He acknowledged the difficulty in detecting early ppID because the signs can indicate other conditions. However, the TrH simulation test recommended by the EEG can lead to early detection of ppID.
Dr. Frank said that if left un-treated, ppID can trigger endo-crine laminitis in horses.
“If caught early, ppID can be managed,” he said.
Dr. Grubbs said a survey by bIVI of 900 horses that were tested for ppID found that the ages of horses that tested positive ranged as young as 5 years old to 30 years old. The highest percentage of horses with ppID was in the 15- to 20-year-old range. In the study, the clinical signs with the highest predictability of ppID were abnor-mal sweating and delayed hair coat shedding.
Dr. Frank suggested that vet-erinarians keep early ppID in the differential for horses showing the symptoms at approximately 10 years old. MeV
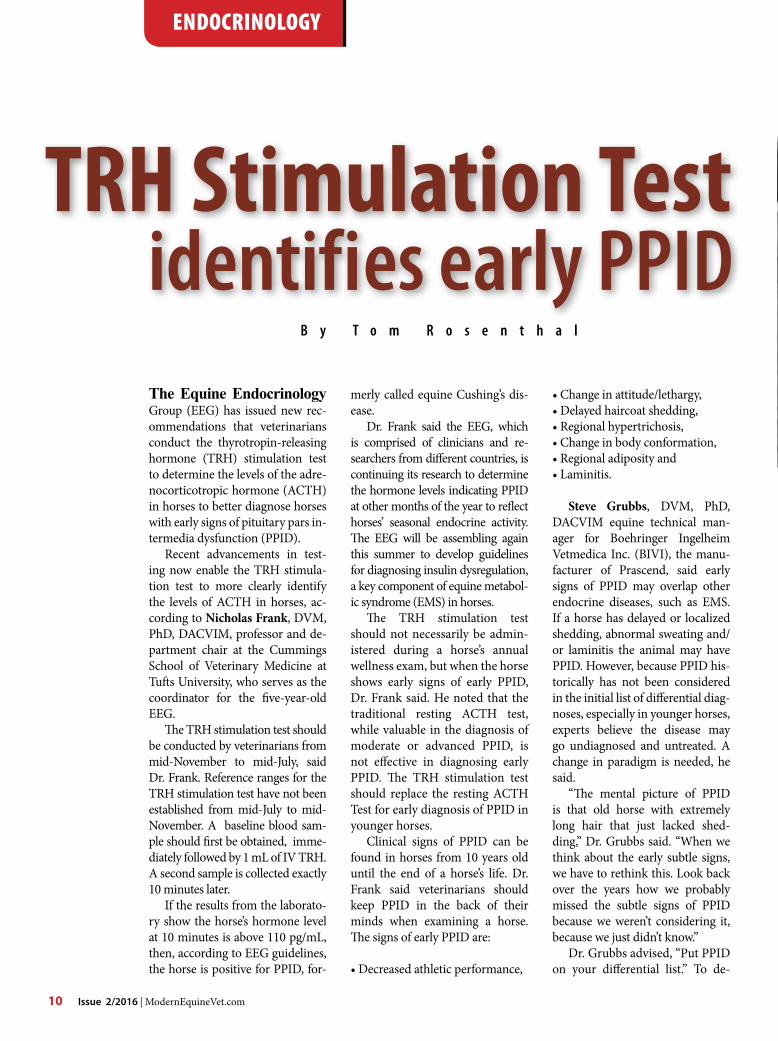
The top horse has early pituitary pars intermedia dysfunction; the bottom horse has late PPID.
Imag
es co
urte
sy o
f BIV
I.
TRH Stimulation Test

12 Issue 2/2016 | ModernEquineVet.com
derMaTology
“As an anatomical pathology resident, I spent time reading biop-sy specimens that had been submit-ted to UGA’s pathology lab,” said Susan L. White, DVM, DAcVIM, professor emeritus of large animal medicine at the University of Geor-gia. “I have seen a lot of cases where the submitting veterinarian marks an X on a diagram of the animal on the submission sheet and sends it in. That is not helpful when a pa-thologist is trying to provide useful information.”
Punch BiopsyDr. White explained that obtaining a skin biopsy early in the disease progression is advantageous. by the time a veterinarian evaluates a horse with a dermatologic issue, all too often the disease has been pres-ent for some time and may have been treated with multiple topical or systemic therapies by the owner.
The earlier the biopsy is taken, the more likely a primary lesion will be available for sampling.
“rule No. 1 is to biopsy a pri-mary lesion,” Dr. White said at the 61st AAEp Annual convention in Las Vegas. “During your physical examination ask the owner to assist
you in identifying primary lesions as biopsies from excoriated or trau-matized lesions are not likely to be informative.” In addition, she recommended asking the owner about any anti-inflammatory drugs given to the animal, particularly corticosteroids.
A disposable biopsy punch that is 8 mm or larger will give the veterinarian a significantly larger sample when compared with the 6-mm punch that is often used in small animal medicine. The archi-tecture of a skin biopsy specimen is markedly fragile, so Dr. White rec-ommended treating the punch as a circular scalpel.
“While applying gentle pres-sure, turn the biopsy punch in one direction only,” she explained. “you do not want to distort the architec-ture.”
Dr. White recommended ob-taining multiple punch biopsies
Skin Sampling
Pathologists tend to agree that context is the key to correct interpretation of skin samples.
B y P a u l B a s i l i o
Send in the crusts.Often, horses will have disease processes that involve crusts or exfoliative material. These may be important in rendering a diagnosis.
“The exfoliative layers of the epidermis or crusts may come off in the process of biopsying the lesion,” Dr. Susan L. White said. “You want to include those in your formalin container so they can be examined as well.”
One easy way to take care of these small pieces is to use microscope lens paper that is used for cleaning the objectives on the microscope. The crusts can be folded into a little package, which can then be submersed in formalin until the paper is saturated. That can be submitted to the diagnostic laboratory. Ph
oto c
ourte
sy of
Dr. S
usan
Whit
e.
Prep it right for the lab
rule no. 1 is to biopsy a primary lesion, but this can be difficult, especially if the owner has already treated the horse.
ModernEquineVet.com | Issue 2/2016 13
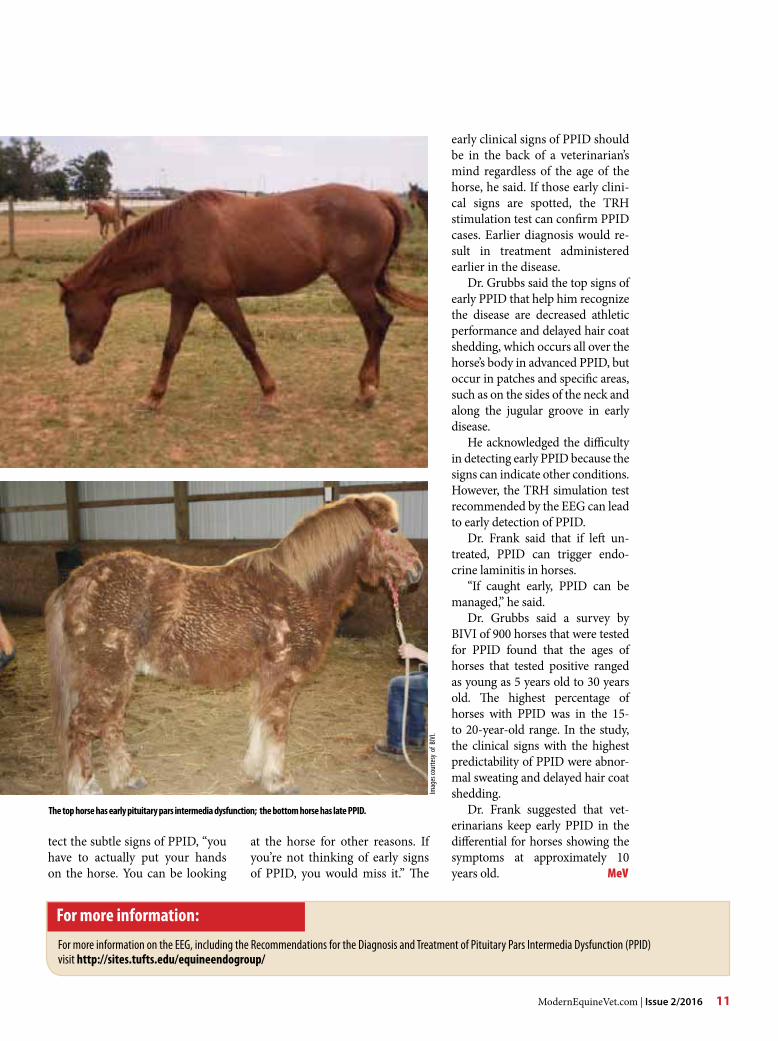
Tools necessary for doing a punch biopsy
when submitting samples. Most di-agnostic laboratories will allow ex-amination of up to three punch bi-opsy specimens for one charge for one submission at one time. Many laboratories do not have a limit for the number of biopsy specimens that can be submitted for a case.
“This allows the opportunity to examine several specimens in cases where there is difficulty dif-ferentiating a primary lesion from a progression of lesions on different parts of the animal.”
The tissue in a skin biopsy specimen will degrade or necrose in short order. In a situation where numerous specimens are required, place each sample in formalin right after it is removed, instead of lining up each sample and placing them in formalin at once, she recom-mended.
Wrapping small specimens in lens paper and labeling it with a pencil before placing it in formalin (pen ink will disappear) can help keep things organized, according to Dr. White.
Incisional biopsy “With an incisional biopsy, you can go deeper within the tissue, and include an area that extends into the subcutaneous tissue,” Dr. White said. “In some instances, you can go even deeper into the fascia and muscle planes if you have an eroding or proliferating lesion.”
For elliptical biopsy specimens, the strong elastic collagen in equine skin will contract quite a bit when it is placed in formalin, which de-stroys the delicate architecture of the sample that the pathologist needs to examine.
“It’s like writing a message on a piece of tinfoil and then crum-pling it up and trying to read it,” Dr. White said. “To avoid this, take the biopsy specimen, place it on heavy paper, cardboard, or even a tongue depressor, and pin it with 25-gauge
needles. Wait about 30 seconds for the subcutaneous tissue to adhere to the material you’ve pinned it to, then place the entire piece in a for-malin container.”
Dr. White recommended ob-taining an elliptical specimen that includes some normal skin in ad-dition to the abnormal skin. This can give the pathologist a clean normal-to-abnormal junction to examine.
“you want about one-third nor-mal skin to two-thirds abnormal skin
in your incisional biopsy,” she said.
Excisional biopsyIn patients with pustules or small nodules, excisional biopsies may be indicated to remove the lesion as well as examine it. Include a margin of normal skin in the specimen for complete examination purposes.
In instances where a neoplastic process is concerned, it is impor-tant to identify whether any tumor cells were left behind or if the mar-gins are clean. MeV
Im
ages
cour
tesy
of D
r. Sus
an W
hite.
Make sure you provide some normal skin as well as abnormal skin to give the pathologist a clean normal-to-abnormal junction to examine.
Prep it right for the lab

14 Issue 2/2016 | ModernEquineVet.com
By Andrea Whittle
A 4-year-old Thorough-bred gelding came into the hospital as an emer-gency referral. He had won a race two weeks pri-or and had exercised four
days before being referred into the hospital. He was febrile prior to admission with a history of depression. The referring veterinarian had been called out to look at him for three days prior to admission for suspected pneumonia and chose to refer him when evidence of pleural effusion was seen on an ultrasound examina-tion. He was being treated with antibiotics, nonsteroi-dal anti-inflammatory drugs (NSAIDs), IV fluids and periodic distal limb cryotherapy.
Upon arrival at the hospital a full physical exam was performed. This horse was reluctant to walk forward when first unloaded. A considerable amount of dark, blood tinged, malodorous nasal discharge was seen from the left nostril. He had an exaggerated respira-tory effort with an abdominal component, was nostril flaring with a resting respiratory rate of 40 beats per minute (bpm) and had an occasional, non-productive, cough. His mucous membranes were bright pink with a prolonged capillary refill time of 3 seconds. Thoracic auscultation revealed harsh sounds bilaterally. His GI system was hypomotile although he passed normal manure during the examination. The reluctance to move was not associated with increased digital puls-es; his legs were cool to palpate with mild distal limb edema. His heart rate was 64 bpm with bilateral jugu-lar vein fill, a catheter from the referring veterinarian was in place and patent with swelling at the insertion site. His temperature was 101.5° F on admission and he was 1,000 lb on weigh tape.
The ultrasound examination of the thoracic region showed significant changes to the lung surface and the presence of pleural fluid. The right side showed areas of consolidated lung with evidence of pleural effusion and diffuse comet tails elsewhere. The left side showed extensive pleural effusion with fluid present 2” above the point of shoulder. After the ultrasound he was se-dated (xylazine 80 mg and butorphanol 0.5 cc) for an upper airway evaluation and trans-tracheal wash via a 1.5 meter endoscope. This is accomplished using a tri-ple guarded aspiration catheter (Mila EMAc800) and saline diluent. There was a large yield of thick, almost
The successful management of pleural pneumonia
blood tinged nasal discharge
AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For more inf or mat ion vist www.aae vt.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.
TeChniCian updaTe
black fluid with a foul odor. This was submitted to the laboratory for cytology and culture.
A replacement catheter was placed in the rJV; the area was clipped and blocked (Lidocaine) ready for placement of a 14G Arrow over-the-wire catheter, the catheter placed by the referring veterinarian was re-moved. A complete blood count, creatinine and elec-trolyte panel were submitted at admission. The white blood cell count was elevated at 15,800 with 78% seg-mented leukocytes, 20% lymphocytes and 2% bands. The fibrinogen was 800 mg/dL, pcV 39.9% and total protein 6.1 g/dL. His creatinine was 1.0 mg/dL.
He was continued on an antibiotic regime of potas-sium penicillin, gentamicin with metronidazole. Ad-ditional treatments included flunixin, pentoxyfylline and omeprazole with probiotics. Firocoxib (0.27 mg/kg IV load dose then 0.09 mg/kg IV SID) was added for additional NSAID coverage alongside the flunixin.
Due to his reluctance to move freely a fentanyl transdermal patch (75 µg patch) was placed over the left cephalic vein and secured with conform and Elas-tikon. This was removed after 72 hours and was the only patch used. We placed Soft ride boots on both front feet as a precautionary measure although he never showed signs of being foot sore and never had elevated digital pulses.
The tracheal aspirate grew Escherichia coli and

AAEVT MembershipBi-Annual NewsletterWeekly “HoofBeats” Email NewsblastFull access to www.aaevt.org, including the Career Center and the LibraryUp-to-date information on the AAEVTDiscounted registration for AAEVT Regional Meetings and the annual AAEP/AAEVT ConventionNTRA, Working Advantage and Platinum Performance BenefitsThe opportunity to participate in the AAEVT Online Certification Program or to become a member of the AEVNT Academy-Specialty in Equine Veterinary Nursing Scholarship opportunities. AAEVT’s Equine Manual for Veterinary Technicians (Blackwell Publishing 20% discount on purchase price)Opportunity to attend Purina’s Annual Equine Veterinary Technician Conference - All Expenses paid!
•••••
•••
••
•
AAEVT ObjectivesProvide opportunities for CE, training, communication, and networkingEducate the equine veterinary community and the public about our professionInform Members of issues affecting our professionAssist in providing the best medical care to improve the health and welfare of the horse
••••
AAEVT Online Equine Certification ProgramA three course, 10 module, equine-only online program offered through ACTGeared toward Credentialed Veterinary Technicians, Assistants, Support staff, & StudentsAreas of study include: equine medical terminology, anatomy and physiology, parasitology, laboratory, diagnostics, equine basics (breeds, wellness, husbandry,) diagnostic procedures, emergency medicine, restraint, pharmacology, surgical assistance and anesthesia, equine office proceduresA certificate of completion is awarded to those who: Successfully complete required courses Complete the list of required skills (per a supervising DVM who is an AAEP member) Attend an AAEVT regional CE symposium and participate in the we labsThose individuals who successfully complete the programs will be recognized as AAEVT Certified Equine Veterinary Technicians / AAEVT Certified Equine Veterinary Assistants depending on their current designation. The certificate is recognized by the AAEVT and the AAEP but does not grant the credentialed status by the AVMAFor more information go to www.aaevt.4act.com or call 800-357-3182
•••
•
•
•
For mo re in f o r mat i on vi st www.aae vt.org*American Association of Equine Veterinary Technicians and Assistants
AAEVT Mission Statement: To promote the health and welfare of the horse through the education and professional enrichment of the equine veterinary technician and assistant.
AAEV T M E M b E r s h i pMembership in the AAEVT is open to all veterinary technicians, assistants, support staff and those employed in the veterinary health care industry worldwide. Student membership is open to those currently enrolled in an AVMA/CVMA accredited veterinary technology program.
16 Issue 2/2016 | ModernEquineVet.com
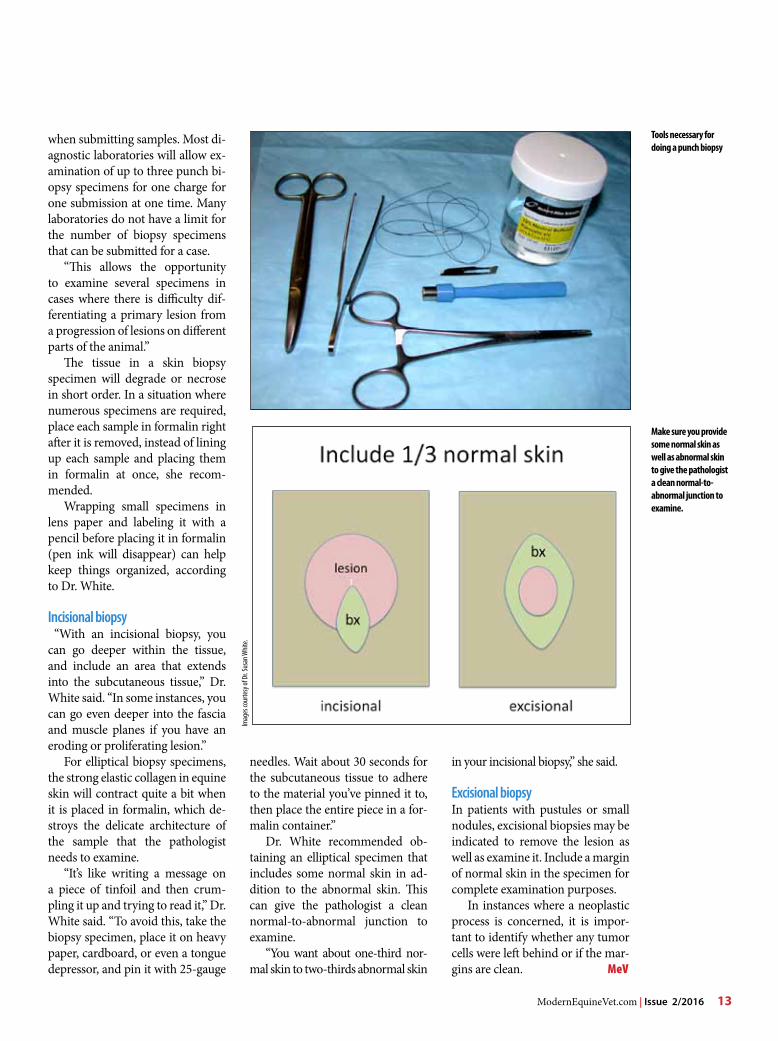
Streptococcus zooepidemicus; the pleural fluid also grew E. coli. The sensitivity results from these cultures necessitated a change in antibiotics on day 3; the genta-micin was discontinued and replaced with enrofloxa-cin.
The accumulation of pleural fluid was greater on the left side, our next procedure was the placement of an indwelling thoracic drain on the left hand side. An area was identified on ultrasound, clipped and scrubbed in preparation for the placement of a 28 Fr Trocar. The insertion site was blocked, subcutaneous and up to 1” deep with lidocaine prior to a final prep scrub and cut down with a #15 blade. The thoracic drain was placed and secured with a finger trap suture. A sterile pleural fluid sample was taken for cytology and culture be-fore a Heimlich valve was placed and the chest was al-lowed to freely drain, 4.5 L of fluid were collected. This drain continued to drip and stayed patent for 4 days. The drain was removed on day 4, the site was sutured closed with absorbable suture, padded with gauze and an Elastikon wrap was placed around the abdomen.
Ultrasounds were repeated every day and the deci-sion was made on day 2 to place a 28 Fr thoracic drain in the right side of the chest as well. The procedure was undertaken in the same manner as before with addi-tional sedation (total 260 mg xylazine and 0.8 cc butor-phanol). The right side drained 8 L of fluid.
Ultrasound evaluation of the right side of the chest showed strands of fibrin around the drain insertion site and these eventually clogged the drain on its third day. The 28 Fr drain site was locally blocked (lido-caine), the drain was removed and replaced with a 30Fr thoracic drain; this drain initially gave 5.5 L of fluid then maintained a steady drip for several days. The drain was removed on day 7 when the ultrasound showed only a small pocket of fluid ventral to the drain with significant fibrin strands and a pocket of walled off fluid caudoventrally between ribs 10 and 11. The
left side of the chest showed a fluid pocket ventral to the previous drain site between IcS 5 and 8.
one of the biggest nursing challenges with cases of pleural pneumonia is their reluctance to eat and drink. Depression, anorexia, often due to oral medications, and reluctance to move around, usually related to tho-racic pain, are all factors to consider.
our patient was initially very sore and unwill-ing to move around the stall, this gradually resolved with the firocoxib and the fentanyl patch, As soon as he was willing to leave the stall he was taken out for short walks to a grassy area, he wouldn’t always graze but he was much brighter after any time spent outside watching activity around the clinic. our technicians would groom him outside and let him walk around if he wanted to.
Feeding these cases can be difficult, it requires pa-tience and often access to many different feeds to try. The approach that worked well in this case was to of-fer small amounts of a feed that he liked frequently throughout the day and night on an opposite schedule to all of his oral medications. The technicians would check his vitals Q4hrs and would offer small feeds every time they went into his stall. If there was grain left in the bucket it would be thrown away, the bucket cleaned and small amounts of fresh offered. He start-ed to eat a little better and we were able to schedule feeds to better suit the rest of the barn. Feeding him last out of the horses in his immediate area seemed to increase his appetite. He would eat and drink well im-mediately after his time outside, the technicians made sure that he had fresh water and a small feed to come in to. We also used a grain-free water flavoring (Horse Quencher) to encourage water intake. He always had access to grass hay and alfalfa offered in the morning and evening.
His thoracic drains were monitored for placement and patency Q15 minutes – Q1hr and his legs were
The ultrasound examination of the thoracic region showed significant changes to the lung surface and the presence of pleural fluid. The right side (left image) showed areas of consolidated lung with evidence of pleural effusion and diffuse comet tails elsewhere. The left side (right image) showed extensive pleural effusion with fluid present 2” above the point of shoulder.
Imag
es co
urte
sy of
Andr
ea W
hittle
TeChniCian updaTe
ModernEquineVet.com | Issue 2/2016 17
frequently washed to keep them free of drainage to prevent scalding. He had his Soft rides removed daily to check for rubs and sores; the sole support pads were replaced approximately every 4 days.
He was discharged to farm care on day 7 with an IV catheter in place, we planned an antibiotic switch to doxycycline after 7 days. bloodwork was to be repeated every 7 days.
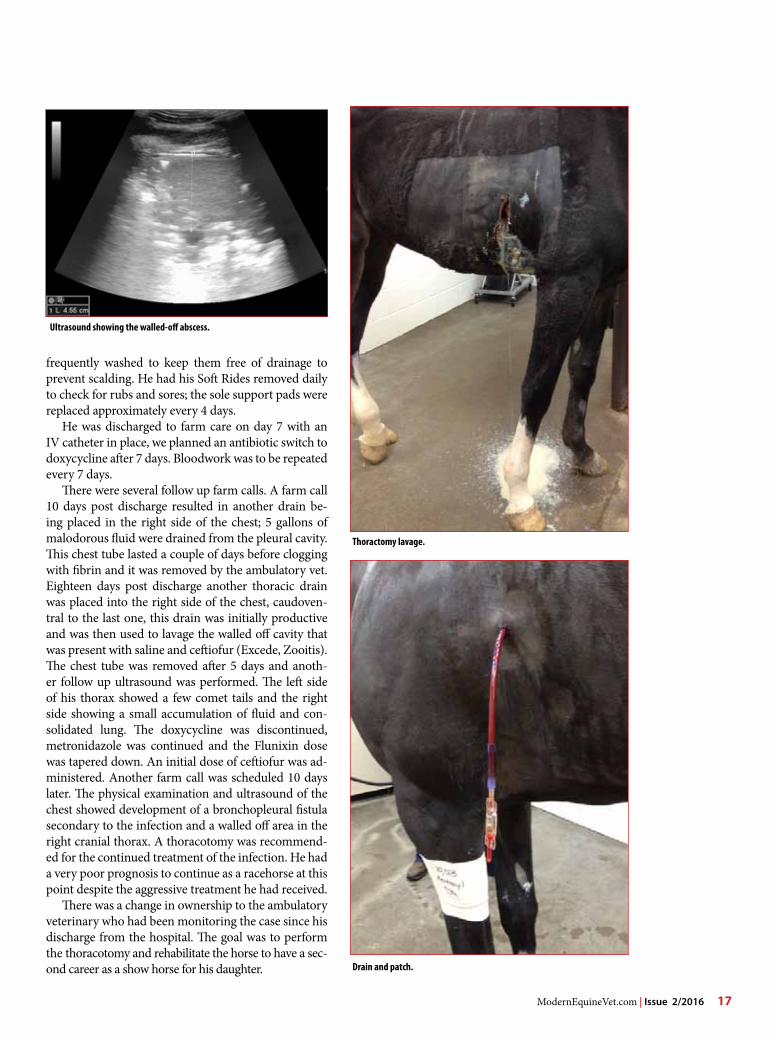
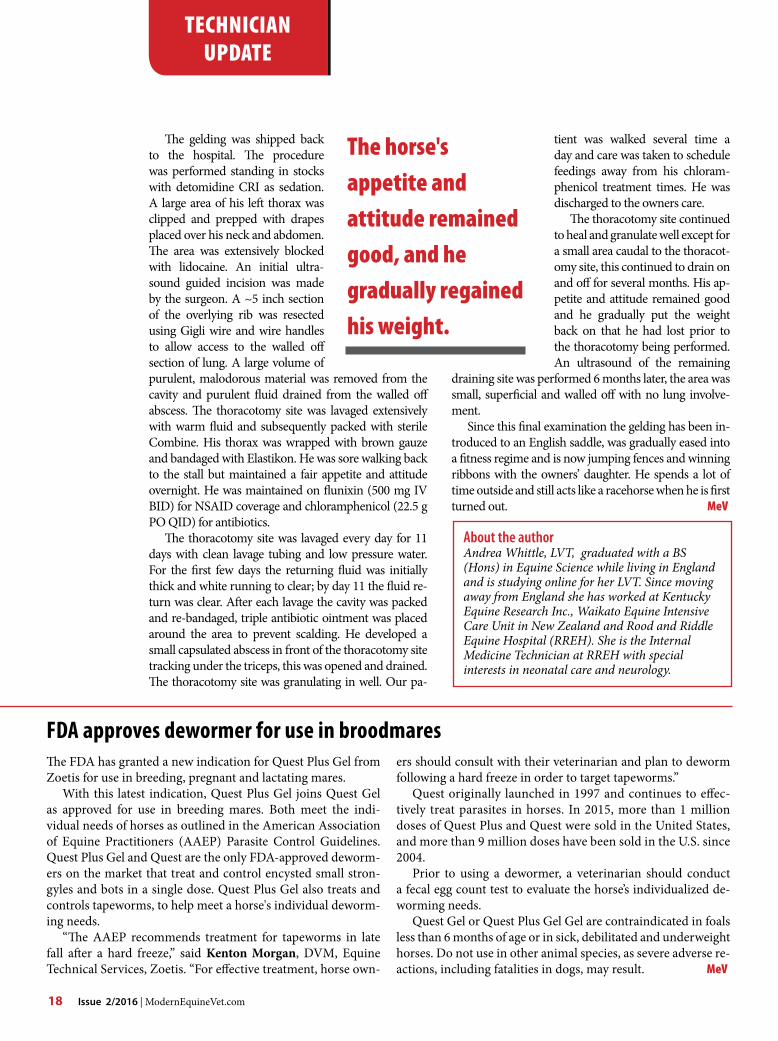
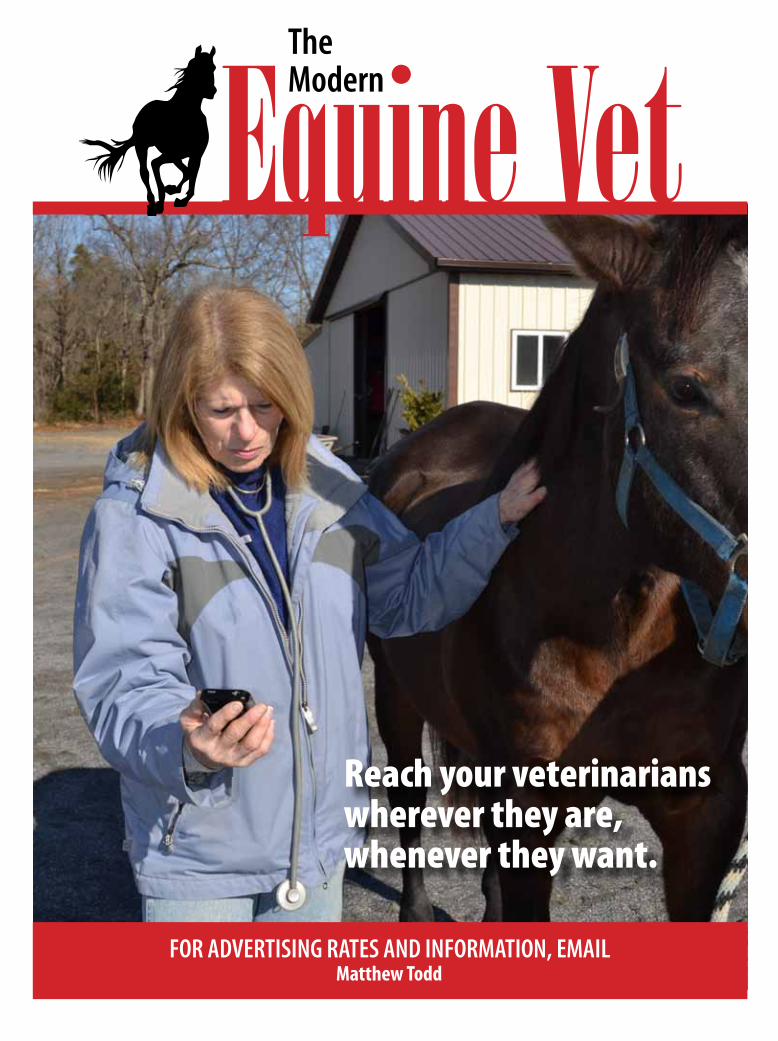
There were several follow up farm calls. A farm call 10 days post discharge resulted in another drain be-ing placed in the right side of the chest; 5 gallons of malodorous fluid were drained from the pleural cavity. This chest tube lasted a couple of days before clogging with fibrin and it was removed by the ambulatory vet. Eighteen days post discharge another thoracic drain was placed into the right side of the chest, caudoven-tral to the last one, this drain was initially productive and was then used to lavage the walled off cavity that was present with saline and ceftiofur (Excede, Zooitis). The chest tube was removed after 5 days and anoth-er follow up ultrasound was performed. The left side of his thorax showed a few comet tails and the right side showing a small accumulation of fluid and con-solidated lung. The doxycycline was discontinued, metronidazole was continued and the Flunixin dose was tapered down. An initial dose of ceftiofur was ad-ministered. Another farm call was scheduled 10 days later. The physical examination and ultrasound of the chest showed development of a bronchopleural fistula secondary to the infection and a walled off area in the right cranial thorax. A thoracotomy was recommend-ed for the continued treatment of the infection. He had a very poor prognosis to continue as a racehorse at this point despite the aggressive treatment he had received.
There was a change in ownership to the ambulatory veterinary who had been monitoring the case since his discharge from the hospital. The goal was to perform the thoracotomy and rehabilitate the horse to have a sec-ond career as a show horse for his daughter.
Ultrasound showing the walled-off abscess.
Drain and patch.
Thoractomy lavage.
18 Issue 2/2016 | ModernEquineVet.com
The gelding was shipped back to the hospital. The procedure was performed standing in stocks with detomidine crI as sedation. A large area of his left thorax was clipped and prepped with drapes placed over his neck and abdomen. The area was extensively blocked with lidocaine. An initial ultra-sound guided incision was made by the surgeon. A ~5 inch section of the overlying rib was resected using Gigli wire and wire handles to allow access to the walled off section of lung. A large volume of purulent, malodorous material was removed from the cavity and purulent fluid drained from the walled off abscess. The thoracotomy site was lavaged extensively with warm fluid and subsequently packed with sterile combine. His thorax was wrapped with brown gauze and bandaged with Elastikon. He was sore walking back to the stall but maintained a fair appetite and attitude overnight. He was maintained on flunixin (500 mg IV bID) for NSAID coverage and chloramphenicol (22.5 g po QID) for antibiotics.
The thoracotomy site was lavaged every day for 11 days with clean lavage tubing and low pressure water. For the first few days the returning fluid was initially thick and white running to clear; by day 11 the fluid re-turn was clear. After each lavage the cavity was packed and re-bandaged, triple antibiotic ointment was placed around the area to prevent scalding. He developed a small capsulated abscess in front of the thoracotomy site tracking under the triceps, this was opened and drained. The thoracotomy site was granulating in well. our pa-
tient was walked several time a day and care was taken to schedule feedings away from his chloram-phenicol treatment times. He was discharged to the owners care.
The thoracotomy site continued to heal and granulate well except for a small area caudal to the thoracot-omy site, this continued to drain on and off for several months. His ap-petite and attitude remained good and he gradually put the weight back on that he had lost prior to the thoracotomy being performed. An ultrasound of the remaining
draining site was performed 6 months later, the area was small, superficial and walled off with no lung involve-ment.
Since this final examination the gelding has been in-troduced to an English saddle, was gradually eased into a fitness regime and is now jumping fences and winning ribbons with the owners’ daughter. He spends a lot of time outside and still acts like a racehorse when he is first turned out. MeV
about the authorAndrea Whittle, LVT, graduated with a BS (Hons) in Equine Science while living in England and is studying online for her LVT. Since moving away from England she has worked at Kentucky Equine Research Inc., Waikato Equine Intensive Care Unit in New Zealand and Rood and Riddle Equine Hospital (RREH). She is the Internal Medicine Technician at RREH with special interests in neonatal care and neurology.
TeChniCian updaTe
The horse's appetite and attitude remained good, and he gradually regained his weight.
The FDA has granted a new indication for Quest plus Gel from Zoetis for use in breeding, pregnant and lactating mares.
With this latest indication, Quest plus Gel joins Quest Gel as approved for use in breeding mares. both meet the indi-vidual needs of horses as outlined in the American Association of Equine practitioners (AAEp) parasite control Guidelines. Quest plus Gel and Quest are the only FDA-approved deworm-ers on the market that treat and control encysted small stron-gyles and bots in a single dose. Quest plus Gel also treats and controls tapeworms, to help meet a horse's individual deworm-ing needs.
“The AAEp recommends treatment for tapeworms in late fall after a hard freeze,” said Kenton Morgan, DVM, Equine Technical Services, Zoetis. “For effective treatment, horse own-
ers should consult with their veterinarian and plan to deworm following a hard freeze in order to target tapeworms.”
Quest originally launched in 1997 and continues to effec-tively treat parasites in horses. In 2015, more than 1 million doses of Quest plus and Quest were sold in the United States, and more than 9 million doses have been sold in the U.S. since 2004.
prior to using a dewormer, a veterinarian should conduct a fecal egg count test to evaluate the horse’s individualized de-worming needs.
Quest Gel or Quest plus Gel Gel are contraindicated in foals less than 6 months of age or in sick, debilitated and underweight horses. Do not use in other animal species, as severe adverse re-actions, including fatalities in dogs, may result. MeV
FDa approves dewormer for use in broodmares

ModernEquineVet.com | Issue 2/2016 19
related to respiratory disease).They took blood, nasal swabs and bAL fluid sam-
ples to test for the presence of EHV-5 and the viral load by qpcr.
The highest rate of detection of EHV-5 was in the EMpF group in which 91% of blood samples, 82% of nasal swabs and 92% of bAL samples were positive for EHV-5. Viral loads in blood were significantly higher in the EMpF group compared with the other groups. The viral load in nasal secretions was significantly higher in EMpF cases than in the two other lung dis-ease groups.
After the EMpF group, the control group had the highest rate of detection in nasal swabs (72%). The high rate of detection in the control group may be reflective of that population or indicate a wider prevalence of latent infection in healthy horses, the researchers said. When both blood and nasal secretions were EHV-5 positive (regardless of the viral load), the sensitivity for that horse having EMpF was 90% and the specificity 89.8%.
one horse in the IAD group was positive for EHV-5 bAL fluid with all other positive bAL samples being in the EMpF group. MeV
Detection of equine herpes vi-rus-5 (EHV-5) in bronchoal-veolar lavage (bAL) samples is consistent finding in horses with suspected equine mul-tinodular pulmonary fibrosis (EMpF), according to a recent study by researchers at the Uni-versity of california Davis.
The diagnosis of EMpF re-quires histological examination of lung tissue, obtained either by percutaneous lung biopsy or at post mortem examination.
“Although histopathological confirmation through a lung biopsy is considered the gold standard for EMpF diagnosis, results of qpcr testing of bALF or a combination of whole blood and nasal secretions should be regarded as clini-cally useful in support of this diagnosis,” the research-ers wrote. “The latter testing may be relevant when dealing with horses in respiratory distress, for which invasive procedures, such as bAL fluid collection or lung biopsies may be detrimental to their health.”
Due to the potential risks of lung biopsy, a positive result for EHV-5 in respiratory secretions detected by quantitative polymerase chain reaction (qpcr) is of-ten used to support diagnosis, but its efficacy has never been tested, according to Dr. Nicola Pusterla, phD, professor of Medicine and Epidemiology at Uc Davis college of Veterinary Medicine, and an expert in her-pesviruses.
Dr. pusterla and his colleagues looked at respiratory samples from confirmed cases of EMpF and compared them with cases with other lung pathology and normal horses. Seventy adult horses of varying ages and breeds were included in the study.
based on clinical findings, bAL cytology, thoracic imaging and histopathology of lung tissue, the horses were divided into four groups: EMpF, inflammatory airway disease (IAD), non-EMpF interstitial lung dis-ease and the control (horses euthanized for reasons not
qPcR of bal confirms eHv-5 in horses with respiratory distress
Imag
e cou
rtesy
of D
r. Pus
terla
.
gross necropsy showing the consolidated and nodular appearance of the lungs from a horses with eMPF.
Pusterla N, Magdesian K. G., Mapes S. M. et al. Assessment of quantitative polymerase chain reaction for equine herpesvirus-5 in blood, nasal secretions and bronchoalveolar lavage fluid for the laboratory diagnosis of equine multinodular pulmonary fibrosis. Equine Vet J. 2016 Jan 18 [Epub ahead of print].http://onlinelibrary.wiley.com/doi/10.1111/evj.12545/abstract
For more information:
news noTes
reach your veterinarians wherever they are, whenever they want.
For adVErTISIng raTES and InForMaTIon, EMaIlMatthew Todd
Equine VetThe Modern





























