Embed Size (px)
Citation preview

THEMETABOLICDEMANDSOFCULTURALLY-SPECIFIC
POLYNESIANDANCES
by
WeiZhu
Athesissubmittedinpartialfulfillmentoftherequirementsforthedegree
of
MasterofScience
in
HealthandHumanDevelopment
MONTANASTATEUNIVERSITYBozeman,Montana
November2016

©COPYRIGHT
by
WeiZhu
2016
AllRightsReserved

ii
TABLEOFCONTENTS
1.INTRODUCTION.........................................................................................................1
HistoricalBackground...............................................................................................1StatementofPurpose...............................................................................................3SignificanceofStudy.................................................................................................3Hypotheses...............................................................................................................4Limitations................................................................................................................5Delimitations.............................................................................................................5
2.REVIEWOFTHELITERATURE.....................................................................................6
Introduction..............................................................................................................6HealthStatusinNHOPI.............................................................................................6PA–AStrategyforBetterHealthOutcomes.............................................................9
PhysicalActivityandHealthOutcomes............................................................9PhysicalInactivityinHawaiianPopulations...................................................11
PolynesianDanceStudy..........................................................................................12DancingasaformofPA.................................................................................12ThePolynesianDances..................................................................................14MetabolicDemandsofPolynesianDance......................................................15
Summary.................................................................................................................17
3.THESISMANUSCRIPT...............................................................................................18
Introduction............................................................................................................18Methodology..........................................................................................................22
Participants....................................................................................................22Procedures.....................................................................................................23PolynesianDancesTested..............................................................................23DanceTestingProtocol...................................................................................25MeasurementofCardiometabolicDemands.................................................26MeasurementofBloodLactate.....................................................................27DataProcessingandCalculations..................................................................27StatisticalAnalyses.........................................................................................29
Results.....................................................................................................................30CharacteristicsofParticipants........................................................................30CardiorespiratoryResponsestoPolynesianDancing.....................................31AerobicandAnaerobicContributionstoTotalAEE........................................34

iii
TABLEOFCONTENTSCONTINUED
Discussion...............................................................................................................38METValuesacrossthePolynesianDancesTested.........................................38GenderComparisonsforMETValues............................................................40AerobicAEE....................................................................................................41AnaerobicAEE................................................................................................42LimitationsandFutureResearch...................................................................43
Conclusions.............................................................................................................44
4.CONCLUSIONS.........................................................................................................46
REFERENCES................................................................................................................48
APPENDIXA:IRBapprovedInformedConsentDocument..........................................53

iv
LISTOFTABLES
Table Page
1.DescriptivestatisticsforPolynesiandancestudyparticipants....................31
2.CardiorespiratoryresponsesandbloodlactateconcentrationforeachofeightPolynesiandances...........................................................33
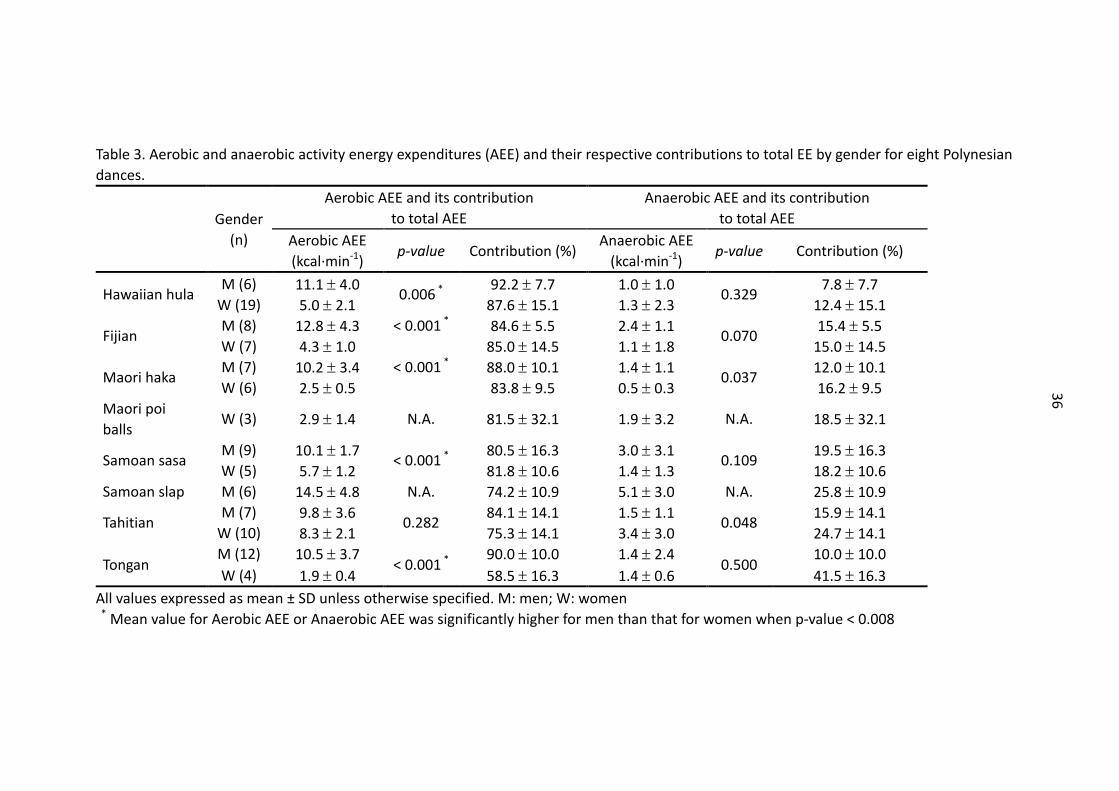
3.Aerobicandanaerobicactivityenergyexpenditures(AEE)andtheirrespectivecontributionstototalEEbygenderforeightPolynesiandances........................................................................36

v
LISTOFFIGURES
Figure Page
1.Metabolicequivalents(MET)foreightPolynesiandancesbygender....................................................................................................35
2.AerobicandanaerobiccontributionstothetotalactivityenergyexpenditureforeightPolynesiandances.Figure2(a):absoluteaerobicandanaerobicAEE(kcals·min-1);Figure2(b):relativeaerobicandanaerobicAEEtototalAEE(%)...............37

vi
NOMENCLATURE
Cardiacrehabilitation(CR):isabranchofrehabilitationmedicineandphysicaltherapydealingwithoptimizingphysical function inpatientswith cardiacdiseaseor recentcardiacsurgeries.
Cardiometabolic disorders: a cluster of diseases of cardiovascular disease (CVD),diabetes,andobesity.
Dance therapy: is the psychotherapeutic use of movement and dance to supportintellectual,emotional,andmotorfunctionsofthebody.
Danceroutine:Eachculturaldanceroutineismadeupofdancemovesfromaspecificculture.Atypicaldanceroutinelastsbetween3and5minutes.
Exerciseprescription: refers to thespecificplanof fitness-relatedactivities thataredesignedforimprovingphysicalfitnessandhealth.Itincludesthefrequency,intensity,durationandmodofexercise.
Metabolic demand (ormetabolic cost, energy expenditure, exercise intensity): theenergy consumption of particular physical activities, usually expressed as MET.Moderateintensityactivityrefersto3to5.9MET.
MetabolicEquivalent(MET):isdefinedastheratioofmetabolicrateduringaspecificphysical activity to a reference metabolic rate at rest, set by convention to 3.5mL·kg−1·min−1ofoxygenuptake.TheMETisusedtoexpresstheintensityofactivitiesinawaycomparableamongpersonswhovaryinbodymass.
Oxygenuptake(VO2):therateofoxygenutilizationbytheworkingmuscletissueduringexercise.
Physicalactivity(PA):isdefinedasanybodilymovementproducedbythecontractionofskeletalmusclesthatresult inasubstantial increase incaloricrequirementsoverrestingenergyexpenditure.
PhysicalActivityReadinessQuestionnaire(PAR-Q):Ahealthscreeningquestionnairedesigned to determine whether or not you should see a doctor beforestarting/resumingphysicalactivity.

vii
ABSTRACT
It is suggested that dancing is a form of exercise that induces favorablephysiologicalandpsychologicaleffectscomparable toaerobicexercise training.ThecurrentstudysoughttomeasurethemetabolicdemandsforseveralPolynesiandances(i.e.,Hawaiianhula,Fijian,Maorihakaandpoiballs,Samoansasaandslap,Tahitian,andTongan),andtoevaluatepossiblegenderdifferencesinthesemeasuresinagroupofexperiencedPolynesiandancers.Thirtyparticipants(13menand17women)weretested through a dance testing protocol, using indirect calorimetry. Metabolicdemands were evaluated in units of metabolic equivalent (MET), as well as bothaerobicandanaerobicactivityenergyexpenditure (AEE)contributions to totalAEE.Onesamplet-testwasusedtocomparethemeanMETvaluesforeachculturaldanceto the cutoff values (3-MET and 6-MET, respectively) for moderate and vigorousphysical activity.Genderdifferenceswereexaminedusing independent t-tests. ThemeanMETvaluesforall,butMaoripoiballsdance,weresignificantlygreaterthan3.0METs.ThemeanMETvalues forSamoansasa,SamoanslapandTahitianwerealsosignificantlygreaterthan6.0METs.Themen’sMETvaluesforHawaiianhula,Samoansasa,Tongan,Fijian,andMaorihakawereallsignificantlygreater(P<0.001)thanthecorrespondingvaluesforwomen,whiletheTahitianMETvaluesweresimilar(P=0.526)between both genders. Aerobic and anaerobic AEE contribute 83.4% and 16.6%,respectively,onaverage, forPolynesiandances,withHawaiianhulabeingthemostaerobic(88.7%and11.3%,respectively)andSamoanslapbeingtheleastaerobic(74.2%and25.8%,respectively).TheaerobicAEEformenwassignificantlygreaterthanthatforwomenfortheHawaiianhula,Samoansasa,Fijian,Maorihaka,andTongan(P<0.001),whilenosignificancegenderdifferencewasobserved inanaerobicAEE(P=0.087-0.989).ThepresentstudyindicatedthatthePolynesiandanceofvariousformsmetthecurrentPArecommendations,andthuscanbeusedasanappropriatemodeof aerobic exercise to increase regular physical activity in the ethnic minorities inHawaiiandthesouthPacificforhealthpromotionanddiseaseprevention.

1
CHAPTERONE-INTRODUCTION
HistoricalBackground
Thegrowingpopularityofrecreationalandcompetitivedancinghasparalleled
the growing knowledge documenting the potential health benefits of dance
(Belardinellietal.2008).Dancetherapy,asfirstintroducedtopatientsparticipatingin
cardiac rehabilitation (CR) programs, uses movement to support the physical and
emotionalwell-beingofpatientsandhasbeenprovento improveexercisecapacity
and quality of life. Different forms of dance (i.e., Waltz, Latin, and aerobic dance
training),havebeenimplementedasphysicalactivityinterventionstrategiesinboth
CVDpatientsandhealthypopulations.Forexample,Waltzdancewascompared to
aerobicexercisetrainingandwasreportedtoresultinthesamebeneficialeffects,such
asimprovedfunctionalcapacityandendothelium-dependentdilationinpatientswith
chronicheart failure (Belardinellietal.2008).Aerobicdancetraininghasalsobeen
showntoreducelow-densitylipoproteincholesterol(LDL-C)andtriglyceridelevels,as
wellasloweringsystolicanddiastolicbloodpressure,inhypertensivepatients(Maruf
etal.2014).FavorablepsychologicaleffectshasalsobeenreportedbyDomeneand
hisgroup(2014)inLatinpartneredsocialdance.
DancetherapywasintroducedtoaCRprograminHawaii.TheHulaEmpowering
LifestyleAdaptationStudy(theHELAStudy)(Looketal.2012)isaprojectfundedby
theNationalInstituteonMinorityHealthandHealthDisparities.Theprojectaimedto

2
developacommunity-basedphysicalactivityCRprogramintegratinghuladancing,an
indigenousculturalpractice,asaformofphysicalactivity(PA).Thispracticenotonly
improved functional capacity of participants, but also enhanced their sociocultural
bonds anddeepened their appreciationof theHawaiian culture (Maskarinec et al.
2015b).Therefore,itisreasonabletopredictthatthesetraditionalculturedancescan
beregardedasaneffectiveexercisemodalityforgeneralhealthpromotionforpeople
ofallagesinNativeHawaiiansandotherPacificIslanders.
Polynesiandances,suchastheHawaiianhula,weredevelopedthroughoutthe
Pacific Islands where the Polynesians originally settled. Each Polynesian culture
tendedtohaveitsownculturally-specificdances,themostwell-knownofwhichare
taughtinschoolsandgroupexerciseclasses,practicedbymenandwomenofallages,
and are popular with all ethnicities (Look et al. 2012). Some of themost popular
PolynesiandancesincludethosefromtheHawaiian,Fijian,Maori,Samoan,Tahitian,
andTongancultures.Asaculturally-relatedPA,Polynesiandancecouldbeusedasan
alternativeformofaerobicexerciseforCVDpatientsandforthegeneralpublic.
The application of basic exercise prescription principles (i.e., duration and
frequencyofpreformingthesekindsofdances)isdifficult,however,withoutknowing
the metabolic demands of these dances. Although the metabolic demands of a
comprehensivevarietyofactivitieshavebeenlistedintheCompendiumofPhysical
Activities (Ainsworth et al. 2011), the number of culturally-based activities is very
limited, andmany of those values were based on self-reported exertion levels or

3
unpublished thesis data, without directly measuring oxygen uptake (VO2). To our
knowledge, only one study (Usagawa et al. 2014) has objectively measured the
metabolic demands of hula, one of the Polynesian culture dances. Usagawa and
colleagues(2014)determinedthemetaboliccostofhulatobe5.7to7.5metabolic
equivalents (METs), which is classified as equivalent tomoderate-to-high intensity
exercise.However,hulaisjustoneofmanypopularPolynesiandances.Themetabolic
costs of all other commonly practiced and performed Polynesian dances are
completelyunknown.Duetothelimitedresearchinthisfield,thepresentstudyaims
atdeterminingthemetabolicdemandsofseveralculturally-specificPolynesiandances
thataremostcommonlypracticedandperformedatthePolynesianCultureCenteron
theislandofOahuinHawaii,USA.
StatementofPurpose
Theprimarypurposeofthisstudyistodetermineandcomparethemetabolic
demands of several culturally-specific Polynesian dances within experienced
Polynesiandancers. The secondarypurpose is to compare theexercise intensityof
eachculturaldancewiththecurrentPAguidelinesformoderate(3-MET)andvigorous
(6-MET)intensityexercises.
SignificanceofStudy
Due to limited research in this field, thepresent studywill provideobjective

4
measures on the metabolic demands of several commonly practiced Polynesian
dancesthatarespecifictosixdifferentPolynesiancultures:Hawaiian,Fijian,Maori,
Samoan,Tahitian,andTongan.Inaddition,theresultsfromthisstudywillbeofvalue
tohealthpractitioners,coachesandhealthinterventionresearcherstoprescribePA
dosage for CVD patients and the general public using Polynesian dance as an
alternativeformofPA.
Hypotheses
ItishypothesizedthattheMETvalueforatleastoneofthePolynesiandances
tobetestedissignificantlydifferentfromtheotherPolynesiandances:
H01:μMET1=μMET2=μMET3=μMET4=μMET5=μMET6=μMETn
HA1:μMET1≠μMET2≠μMET3≠μMET4≠μMET5≠μMET6≠μMETn
WhereμMET1toμMETnarethepopulationmeanMETvaluesforthentypesofPolynesian
dance.
It isalsohypothesizedthatallPolynesiandancestobetestedwillhavemean
METvalues≥3.0METs:
H02:μMETi<3.0METs
HA2:μMETi≥3.0METs
Where:μMETirepresentsthepopulationmeanMETvalueforeachPolynesiandanceto
betested.

5
Limitations
One limitation of the present study is that the Polynesian dances tested are
dependent upon the skill and experience of each study volunteer. As currently
designed,thisstudywillrequestthateachsubjectperformeachPolynesiandanceof
interest,buteachsubjectmaynotbeabletoperformallthedanceroutines.Whilean
aprioriattemptwillbemadetorecruitsubjectswhocanperformalltheculturaldance
routines, the success of this plan will be unknown until the study is completed.
Therefore,itispossiblethattherewillbemissingdataforsomedancestobetested.
Delimitations
The scope of inference for this study is delimited to experienced Polynesian
dancersduetonon-randomsampling.

6
CHAPTERTWO-REVIEWOFTHELITERATURE
Introduction
NativeHawaiiansandotherPacificIslanders(NHOPI)sufferadisproportionately
higher prevalence of cardiometabolic disorders when compared to the general
populationoftheUnitedStates(Mauetal.2009).Physical inactivityandsedentary
lifestyleinthispopulationisanindependentriskfactorforthehigherprevalenceof
cardiovascular diseases (CVD), obesity, andmetabolic syndrome (Grandinetti et al.
2015).CulturaldancesofPolynesia,suchasthehulafromtheHawaiianculture,could
be adopted as culturally-specific form of physical activity (PA) for general health
promotion(Maskarinecetal.2015b).However,itisnecessarytoprescribethedoseof
PA by exercise intensity, duration and frequency, while the knowledge about the
energyexpenditureofthesePolynesiandancesisverylimited.Currently,onlythehula
hashadenergyexpenditureobjectivelyevaluatedforexerciseprescription(Usagawa
etal.2014),whilenootherPolynesiandanceshavebeenmeasureddirectly.Thelack
of research in the determination ofmetabolic demands for Polynesian dances has
promptedthecurrentstudy.
HealthStatusinNHOPI
NHOPI refer to those of indigenous ancestry on the islands of Polynesia,
Melanesia and Micronesia (Mau et al. 2009). This population consists of Native

7
Hawaiians, Caucasians, Blacks, Latinos, and Asian Americans (mainly Japanese,
Filipinos,ChineseandKoreans).
NHOPIhavebeencategorizedashigh-riskpopulationsthataremostsusceptible
to cardiometabolic disorders of CVD, diabetes, and obesity in the United States
(Usagawa et al. 2014). It is worthwhile mentioning that the mortality rate in this
populationareamongthehighestintheUnitedStates(Johnsonetal.2004). Inthe
NHOPI,CVDistheleadingcauseofmortality,whichaccountsfor55%ofalldeaths.
DiabetesstandsoutasamajorriskfactorofCVDinthispopulation.Itisreportedthat
CVDratesarefour-foldhigherinthosewithdiabetesthanthosewithout(Alulietal.
2010). Hawaiians have also been reported to have a higher incidence of type 2
diabetes (Maskarinec et al. 2015a), which could result from central obesity and
physicalinactivity(Grandinettietal.1999).
AreNHOPIgeneticallymoresusceptibletocardiometabolicdiseases?Mauetal.
(2009) found that CVD risk factors, such as high cholesterol concentration,
hypertension,andelevateddiastolicbloodpressureweresignificantlyrelatedtothe
degreeofHawaiianancestry.Accordingtoageneticstudy(Grandinettietal.2006),
prolongedheart-ratecorrectedQTinterval,whichhasbeenblamedforthecauseof
sudden death and increased mortality, was observed in populations of Filipino,
Japanese andHawaiian ancestry, compared to Caucasian populations. Besides, the
oddsofdiabetesdiagnoseswerereported70%higheramongAsianAmericansthan
whitesinHawaii,afteradjustmentforage,genderandBodyMassIndex(BMI)(Kinget

8
al. 2012). Grandinetti et al. (1998) also found that the prevalence of glucose
intolerancewas significantly higher amongNativeHawaiians thanwhites.And it is
interestingtonotethatfullHawaiianssufferedahigherprevalenceofdiabetesthan
part-Hawaiians(Mauetal.2009),suggestingapossiblegeneticfactor.Furthermore,
theprevalenceforoverweightandobesityinthispopulationhit84%(Duncanetal.
2015),comparedto69%ofnationallevel(Ogdenetal.2014).BMIwashigherinboth
NativeHawaiiansandamongotherethnicmixturesthathadNativeHawaiianancestry
(Grandinettietal.1999).Additionally,increasedBMIandwaisttohipratio(WHR)were
significantlyassociatedwithpercentageHawaiianancestry(Grandinettietal.1999).
Collectively,thisevidencesuggestedthattheremightbesomegeneticlinkbetween
Hawaiianancestryandtheonsetofcardiometabolicdiseasesinthispopulation.
However, unhealthy lifestyles were also reported to be responsible for the
higherprevalenceofcardiometabolicdisordersinthispopulation(Kimetal.2013).A
prospectivestudy(Maskarinecetal.2007)indicatedthatduetoahighfrequencyof
smokingandalcoholuse,NativeHawaiianshadthehighestchronicdiseaseriskscores
comparedtootherethnicgroups.ApproximatelyoneinthreeNativeHawaiianswere
smokers,comparedto15%ofadultsmokersintheUSpopulation(Johnsonetal.2004).
Over 51% of Native Hawaiians reported drinking alcohol, slightly higher than the
averagerateof48.6%inthegeneralpopulationoftheUnitedStates(Johnsonetal.
2004).Althoughgeneticinfluencescouldbeacontributingfactortotheonsetoftype
2diabetes(Mauetal.2009),Steinbrecheretal.(2011)investigatedthepreventable

9
proportionoftype2diabetesriskinmultiethnicpopulationofHawaii.Theyfoundthat
beingoverweightandphysicallyinactive,aswellassmokingandhavingahighmeat
consumption,weretheprimaryrisksofdiabetesinallethnicgroups.Indeed,Kimetal.
(2008) found thatNativeHawaiiansandFilipinoshavehigher consumptionof local
ethnicfoods,suchasLaulau,Kaluapig,PoiandPortuguesesausage,Pinacbet,Sinigang
andDinengdeng,andthatthepreferenceofconsumingthesetraditionalfoodswas
positivelyassociatedwithtype2diabetesduetothehighenergydensity.
PA–AStrategyforBetterHealthOutcomes
PhysicalActivityandHealthOutcomes
Physicalactivityisdefinedasanybodilymovementproducedbythecontraction
ofskeletalmusclesthatresultsinasubstantialincreaseincaloricrequirementsover
restingenergyexpenditure (Caspersenet al. 1985). PAplays a fundamental role in
healthmaintenanceandinreducingtherisksofchronicdiseases.
ThatPApromoteshealthandfitnesshasbeenrecognizedforcenturiesandis
nowawidelyacceptedconcept.RegularPAhasshort-termbenefits,suchasincreased
energyexpenditure, increased insulinsecretionand insulinsensitivitypost-exercise,
improvedsleepquality,andlong-termbenefits,includingahealthierheart,improved
fitnesslevel,aswellashavinglesschanceofbeingobeseanddevelopingdiabetesand
otherchronicdiseases(JAMAPatientPage2000).Thereisageneralconsensusinthe
literaturethatregularPAisassociatedwithalowerBMI(Okeyoetal.2009),reduced

10
cardiovascular risk (Hegde and Solomon 2015), decreased cancer risk (Thune and
Furberg2001),aswellasabettercognitivefunction(Domeneetal.2014).Inaddition,
there is a graded dose-response relationship between PA and overall health
(Kesaniemietal.2001).Furthermore,itisbelievedthatlifestyleinterventionismore
effective in preventing diabetes and CVD risks, such as hypertension and
hyperlipidemia,thanpharmaceuticaltherapies(Aasetal.2006).Lastly,bothleisure
timeandoccupationalPAwerereportedtohaveagradeddose-responseassociation
withloweroverallcancerrisk(ThuneandFurberg2001).
Physical inactivity has been amajor concern in the past 50 years as people
adoptedmoresedentarytasksasoneoftheirlifestylechangesinthemodernsociety.
WhileitiswelldocumentedthatlessPAisstronglyassociatedwithanincreasedrisk
of all-cause mortality in apparently healthy individuals (Szostak & Laurant 2011),
sedentarytimeisnowbelievedtobeanindependentriskfactorforchronicdiseases
andmortality(Culletal.2015).Boothetal.(2000)foundthatsedentarylifestylescould
beresponsibleforat leastone-thirdofall-causemortality inU.S.adults.Decreased
dailyPAwasalsoreportedtohaveastrongdose-responserelationshipwithmetabolic
disorders(Kesaniemietal.2001).A6-yearlongitudinalstudy(Menaietal.2015)found
that the time spent in watching television and using a computer had a strong
associationwithincreasedBMIandpercentbodyfat.
PhysicalInactivityinHawaiianPopulations
According to the 2008 Guidelines of Physical Activity (USDHHS 2008), the

11
minimaldoseof150minperweekofmoderateintensity,aerobicactivityperformed
inepisodesofatleast10minutesaregenerallyrecommendedintheadultpopulation
tomaintainbodyweightandpreventweightgain,reducecardiovascularriskfactors,
andtoimprovecardiorespiratoryfitnessandoverallwell-being.
However,itisreportedthat59.1%ofmenand64.1%ofwomenoftheNHOPI
(versus51.6%ofmenand56.7%ofwomenoftheoverallU.S.population)didnotmeet
thefederallyrecommendedlevelsofPA(CentersforDiseaseControlandPrevention
(CDC) 2004; USDHHS 2008). Physical inactivity results in the excessive storage of
caloriesinthebody,whichinturnleadstoahigherprovenanceofobesity,diabetes
andmetabolicsyndrome(Szostak&Laurant2011).Physicalinactivityalsoundermines
one’scardiopulmonaryfitness,withelevatedrestingheartrate(RHR)asanindicative
factor.Grandinettietal.(2015)investigatedamultiethniccohortinHawaii,including
Native Hawaiian, Japanese, Filipino, Caucasian, and mixed ethnic ancestries, and
reportedthatthosewithincreasedRHRandwhowerealsolessphysicallyactivewere
morelikelytodevelopinsulinresistance.ElevatedRHRhasalsobeenidentifiedasan
independentriskfactorforCVDandmortality(RuizOrtizetal.2010).
Since regularPA, especiallymoderate-intensity aerobic exercise, can improve
functionalcapacityandserveasanalternativetreatmentforspecificcardiorespiratory
andmetabolic diseases similar to pharmacological treatments (Faude et al. 2015),
increasingPAshouldresultinbeneficialhealthoutcomesintheNHOPI.

12
PolynesianDanceStudy
DancingasaFormofPA
Dancinginvolvesrhythmicmovementsofthebodywithmusic.Itisreportedthat
dancing has a similar effect on health as traditional aerobic exercise training (i.e.,
treadmill,stationarybicycle,andstepmachine)(Belardinellietal.2008)andtherefore
canberegardedasanalternativeculturally-specificPA.
Dance therapy, as first introduced to patients participating in cardiac
rehabilitation (CR) programs, uses dance movements to support the physical and
emotionalwell-beingofpatientsandhasbeenprovento improveexercisecapacity
andqualityoflife(Belardinellietal.2008).Differentformsofdance,suchasWaltz,
Latin,andaerobicdancetraining,havebeenusedasinterventionstrategiesinboth
CVDpatientsandhealthypopulations.
Belardinellietal.(2008)examinedthebenefitsandsafetyofWaltzdancingin
patientswith chronic heart failure. They compared aWaltz dance protocolwith a
supervised aerobic exercise training and a control group. The results of the study
showed that Waltz dancing was safe and that both functional capacity and
endothelium-dependentdilation improvedsignificantly inbothtraininggroups(i.e.,
Waltzdancingandaerobictraining),whiletherewasalsonodifferencebetweenthe
two groups. Another randomized study (Maruf et al. 2014) identified that aerobic
dancetrainingfor12weekshelpedreduceLDL-Candtriglyceridelevels,andlowered
systolicanddiastolicbloodpressureinhypertensivepatients.Domeneandhisgroup

13
(2014) investigated the effects of Latin partnered social dance using an Exercise
Benefits/BarriersScale(EBBS),andreportedapositivepsychologicaloutlookwithLatin
dance participation. Collectively, these studies demonstrate that dance, as an
alternativeformofaerobicexercise,hasbeneficialeffectsoncardiorespiratoryfitness,
metabolicprofiles,andpsychologicalhealthinbothCVDpatientsandhealthyadults.
Dance therapy has been introduced to a CR program in Hawaii. The Hula
EmpoweringLifestyleAdaptationStudy(theHELAStudy)(Looketal.2012)isaproject
fundedbytheNationalInstituteonMinorityHealthandHealthDisparities.Theproject
aimed todevelopacommunity-basedphysicalactivityCRprogram integratinghula
dancing,anindigenousculturalpractice,asphysicalactivity(PA).Thispracticenotonly
improved functional capacity of participants, but also enhanced their sociocultural
bondsanddeepenedtheirappreciationofHawaiianculture(Maskarinecetal.2015b).
Therefore, it is reasonable to predict that these traditional culture dances can be
regarded as an effective exercise modality for people of all ages in the NHOPI
populationasaformofgeneralhealthpromotion.
ThePolynesianDances
Polynesian dances, such as the hula,were developed throughout the Pacific
Islandswhere thePolynesiansoriginally settled.EachPolynesianculture tended to
haveitsownculturally-specificdances,themostwell-knownofwhicharetaughtin
schoolsandgroupexerciseclasses,practicedbymenandwomenofallages,andare
popularwithallethnicities(Looketal.2012).SomeofthemostpopularPolynesian

14
dancesincludethosefromtheHawaiian(indigenouspeoplesoftheHawaiianIslands),
Fijian (indigenous peoples of the Fiji Islands), Maori (indigenous peoples of New
Zealand),Samoan(indigenouspeoplesoftheSamoanIslands),Tahitian(indigenous
peoples of Tahiti), and Tongan (indigenous peoples of The Kingdom of Tonga, a
collection of 177 islands) cultures.Hula, for instance, is aHawaiian-specific dance,
whichcanbeeitherHulaAuana,wherethedanceisaccompaniedbychantandstring
instruments,ortheHulaKahiko,wherethedanceisaccompaniedbychantandancient
drums.Meke,atraditionalstyleofdanceinFiji,isoftenreferredtoasaspiritdance
whichinvolvesquickupperandlowerbodymovementsandjumping.Whilemostof
thePolynesianculturaldances involvebothmenandwomendancingtogether, the
Maori have a clear gender differenceon choreography. For instance, the haka is a
Maori battle dance, traditionally only performedbymenwho standwith hips and
kneesinaslightlyflexedposition.Thisdanceincludesfootmovementsthatresemble
stompingwithhandandarmmovementsthatslaptheuppertorsoandlegs.Dancers
oftenperformthisdanceinaheightenedarousalstateinferringintimidation.Thepoi
balldance,however,ismorecommonforMaoriwomen,wherepoiballsareattached
to one or both ends of a rope and are swung around in different movements
throughoutthedance.TheSamoanculturehastwomajorculturally-specificdances:
Taupo,whichisoftenreferredtoastheprincessdance,andSasa,whichincludesupper
body movements with clapping and slapping mimicking the beat of a drum. The
TahitianOridanceismadeupofquickbodilymovementsfeaturedbywomen’squick

15
hip movements (Tamure) and men’s quick knee movements (Pa oti). The Tongan
culturehasthreemajortypesofdance:Nafa(drummer),Taualunga(woman’sgraceful
dance) andMa’ulu’ulu. TheMa’ulu’ulu, usually performedwhile sitting, has upper
bodymovementscharacterizedbyarmandhandmovementsalongwith torsoand
headmovements.AdvancedPolynesiandanceroutinesrequirecomplexmovements,
advanced technique and aesthetics, as well as a high physiological capacity
(Koutedakis&Jamurtas2004).
Nowadays,manyoftheseculturally-specificdancesaretaughtinschoolsorto
exercisegroupsandarecommonlypracticedbymenandwomenofallages,aswellas
withallethnicities(Looketal.2012).Asaculturally-relatedPA,Polynesiandancecould
bemoreattractiveandmoreadherent to theseat-riskpopulations than traditional
aerobicexercise(Maskarinecetal.2015b).
MetabolicDemandsofPolynesianDance
Althoughthemetabolicdemandsofacomprehensivevarietyofactivitieshave
beenlistedontheCompendiumofPhysicalActivitiesbyAinsworthetal.(2011),the
numberofculturally-specificdanceactivitiesisverylimited.Toourknowledge,there
isonlyonestudy(Usagawaetal.2014)thathasobjectivelydeterminedtheenergy
expenditure of hula, one of the Polynesian culture dances. They determined the
metabolic equivalent (MET) value via direct measurements of oxygen uptake and
reported that the hula dance expends 5.7 to 7.5METs,which can be classified as
equivalenttomoderate-to-highintensityphysicalactivity(MVPA).

16
WhilehulaisprobablyoneofthemostwidelyrecognizedPolynesiandances,it
isnottheonlyPolynesiandancethat iscommonlypracticedandperformed.Atthe
Polynesian Culture Center on the island of Oahu (Hawaii), some other Polynesian
culturaldancesarefrequentlyperformedtothepublicatthe“Ha:BreathofLife”show,
whichincludesHawaiian,Fijian,Maori,Samoan,Tahitian,andTonganculturedances.
Sofar,thephysiologicaldemandsofthesedancesarecompletelyunknown.
Energyexpenditureofdancevarieswiththeintensityofbodymovements,the
dominanceoftheupperand/orlowerbodylimbs,theskilllevelofthedancers,aswell
as the fitness level of the dancers. According to previous literature,most types of
dance requireat leastamoderate intensity (3.0METs).One study (Massiddaetal.
2011) reported the competitive Latin American dance to be MVPA, where Latin
partneredsocialdancewasdeterminedtorequire5.1and7.3METswhenperformed
moderatelyorvigorously,respectively(Domeneetal.2014).Salsadancingrangesfrom
3.9 to 5.5 METs (Emerenziani et al. 2013), while Waltz dancing was 4.1 METs
(Belardinelli et al. 2008). Finally, recreational ballroom dance (Mixture of Waltz,
Foxtrot,Swing,andCha-Cha)costsanaverageof6.1METsforatotaltestingduration
of30mins(Lankfordetal.2014).
AssumingthattheexerciseintensityofPolynesiandancesisatleastatmoderate
level, thenpracticing these culturally-specificdanceswould contribute favorably to
meeting the U.S. National PA Guidelines (≥150 mins/week of moderate intensity,
aerobicactivity). Therefore, itwouldbeuseful toexamine theexercise intensityof

17
eachtypeofthecommonlypracticedPolynesiandances,andeventuallyprovidemore
information for exercise prescription to the at-risk populations in Hawaii and
throughoutPolynesia.
Summary
AlthoughtheCompendiumofPhysicalActivitiesliststheenergyexpenditurefor
awidevarietyofPAs,thereareaverylimitednumberofculturally-basedactivities.
ManyofthereportedMETvalueswerebaseduponself-reporteddataandnotdirect
measuresofoxygenuptake.Thus,themetabolicdemandsofmostPolynesiandances
areunknown.Thecurrentstudyisdesignedtofilltheobviousgapintheliteratureby
objectivelymeasuringtheexerciseintensityfortheseculturaldances,whichcouldbe
usedthroughmoreappropriateexerciseprescriptionsfortheat-riskNHOPIpopulation.

18
CHAPTERTHREE-THESISMANUSCRIPT
POLYNESIANDANCEASAFORMOFPHYSICALACTIVITY:EXERCISEINTENSITY,ENERGY
EXPENDITURE,ANDENERGYSYSTEMCONTRIBUTIONS
Introduction
NativeHawaiiansandotherPacificIslanders(NHOPI)sufferadisproportionately
high prevalence of cardio-metabolic disorders when compared with the general
population of the United States (U.S.) (Mau et al. 2009). Physical inactivity and
sedentary lifestyle are believed to be independent risk factors contributing to the
higherprevalenceofcardiovasculardiseases(CVD),obesity,andmetabolicsyndrome
(Grandinettietal.2015)intheNHOPIpopulation.Itisreported,forexample,that59.0%
ofmenand64.2%ofwomenoftheNHOPIdidnotmeetthefederallyrecommended
levelsofPA(USDHHS2008;CDC2004).However,thereisageneralconsensusinthe
literature that regularmoderate-to-vigorous intensity physical activity (MVPA) that
satisfiestheU.S.FederalPAGuidelines isassociatedwitha lowerBMI(Okeyoetal.
2009), reduced cardiovascular risks (Hegde and Solomon 2015), improved glucose
tolerance (Slentzetal.2016),aswellasabettercognitive function (Domeneetal.
2014). Thus, by encouraging regular MVPA in this population, the NHOPI could
improveboth cardiovascular andmetabolic fitness levels, aswell asdecrease their
risksformanychronicdiseases.Assuch,MVPAisbeingusedasanequivalentmethod

19
oftherapyforcardiometabolicdiseasesthathassimilarbenefitsaspharmacological
treatments(Faudeetal.2015).
Polynesian dances, such as the well-known Hawaiian hula, refer to a large
collectionofdancesthatareeachspecifictothePolynesiancultures(e.g.,Hawaiian,
Fijian,Maori,Samoan,Tahitian,Tongan,etc.)andPacificislandsonwhichtheywere
developed.SomeofthemostpopularPolynesiandancesaretaughtinschoolsandare
practiced bymen andwomen of all ages and ethnicities (Look et al. 2012). Thus,
PolynesiandancingcouldbeconsideredaculturallyspecifictypeofPAfortheat-risk
NHOPIpopulation.Waltz, aerobicdance, and Latinpartnered social dancehaveall
beenstudiedas intervention tools for increasingMVPA invariouspopulations,and
werefoundtoimprovethefunctionalcapacityandendothelium-dependentdilation
(Belardinellietal.2008),bloodlipidprofileandbloodpressure(Marufetal.2014),as
wellaspsychologicaloutlookfortheparticipants(Domeneetal.2014).Thus,dancing
is considered to be a form of PA that can induce similar physiological effects as
traditional aerobic exercise training (Belardinelli et al. 2008). As a matter of fact,
“dancetherapy”hasbeenintroducedtopatientswithcardiovascularandmetabolic
diseases and has become popular in recent years (Faude et al. 2015). The Hula
EmpoweringLifestyleAdaptations(HELA)study, forexample,successfullyusedhula
dancing, a culturally-relevantdance tonativeHawaiians, as ameans for increasing
MVPAandimprovehealthbenefitsincardiacrehabilitationprogramparticipants(Look

20
et al. 2012). Thus, dancingmay be an effective form of PA for promoting healthy
outcomesinpopulationsthatarereceptivetodancingactivities.
Unfortunately,thereisrelativelylittleobjectiveinformationavailableaboutthe
cardiometabolic consequences of regular dancing, whichmakes the application of
basicexerciseprescriptionprinciples(i.e.,determiningthe“dose”ofexercise)difficult
without knowing the metabolic demands (or exercise intensity, as commonly
expressed with metabolic equivalents (MET) or energy expenditure (EE)) for each
Polynesiandance. Forexample, thereare very fewMETvalues for culturally-based
activitieslistedintheCompendiumofPhysicalActivities(Ainsworthetal.2011),and
noneofthesevalueswerebasedupondirectmeasuresofoxygenuptake(VO2).Sofar,
thehulaistheonlyPolynesiandancetohavedirectMETintensitymeasuresreported
in the literature (5.7 and7.6METs for lowandhigh intensitydances, respectively)
(Usagawa et al. 2014). To our knowledge, the MET intensity for other Polynesian
danceshasneverbeenassessedobjectively(e.g.,usingindirectcalorimetry).Thus,the
lackofMETintensityevaluationsformostPolynesiandancesmaybeadeterrentto
theiruseasMVPAinterventiontoolsfortheNHOPIandotherhighriskpopulations.
WhiletheaerobicdemandsforPolynesiandancingareweaklyunderstood,the
anaerobic energy demands of Polynesian dancing are completely undocumented.
Accordingtotheliterature,thetraditionalstrategyfordeterminingPAMETintensities
istoaveragethelastseveralminutesofdirectly-measuredoxygenconsumptionfora
steady-state bout lasting 3-10 mins. While this strategy provides the information

21
needed to assess aerobic exercise intensity, no information is provided about
anaerobicenergyexpenditureoranaerobicwork intensity.Blood lactatemeasures,
however, takenduring thesamesteady-statebouthavebeenused toestimate the
anaerobic EE for both low and high intensity activities (e.g., weight lifting, rock
climbing,andrunning)(Scott2006;Bertuzzietal.2007;Duffieldetal.2005).Given
thatmanyPolynesiandancesarenotpurelysteady-stateactivities,itmaybeusefulfor
healthcare professionals to know both the aerobic and anaerobic contributions to
whole-body EE (Scott 2005). However, to our knowledge, there have been no
publishedevaluationsofboththeaerobicandanaerobicEEcontributionsforanytype
ofdancing.
Thus, the primary purpose of this study was to measure and compare the
metabolic demands (both aerobic and anaerobic) for several popular forms of
Polynesiandanceascommonlypracticedandperformedbyaconveniencesampleof
experienced Polynesian dancers. When expressed as METs, these results can be
compared to the 2008 U.S. Physical Activity Guidelines (USDHHS) to determine
whether dance intensity exceeds the commonly-used intensity thresholds for
moderate(3.0METs≤“moderate”<6.0METs)orvigorousintensity(≥6METs)PA.We
hypothesized that all of the Polynesian dances tested would exceed the 3-MET
threshold, while some of the dances (but not all) would also exceed the 6-MET
threshold. Since some Polynesian dances are choreographed by gender (withmen
tendingtohavemoreenergeticappearingroutines),wealsohypothesizedthatthe

22
MET intensity for themen’sdanceswouldbe significantlyhigher than that for the
women’s dances. Finally, given the complete lack of information regarding the
anaerobiccontributiontototalEEofdancing,wealsosoughttodescribehowboth
aerobicandanaerobicenergysystemscontributetototalEEofPolynesiandancing.
Methodology
Participants
Participantsofthisstudywereexperienceddancersworkingfull-timeorpart-
time (within thepast12months)performing the“Hā:BreathofLife”showfor the
Polynesian Culture Center on the island of Oahu (Hawaii, USA). Inclusion criteria
included:1)Menandwomenaged18-64years;2)NativeHawaiiansandotherethnic
groupsinHawaiicommonlyidentifiedasNHOPI;3)Thosewhocouldperformatleast
oneofthePolynesiandancesofinteresttothisstudy.Exclusioncriteriaincluded:1)
Pregnantwomen;2)Thosewhoself-identifiedashavinguncontrolledchronicdiseases
ororthopedicconditionsthatcouldadverselyaffectcardiometabolicmeasurements
ortheparticipant’sabilitytodance;3)Thosewhohadcontraindicationstoperforming
MVPA. The study protocolwas approved by the BrighamYoungUniversity (BYU) –
Hawaii (Laie, Oahu) Institutional Review Board. Participants read and signed the
informed consent form that fully described the risks and benefits associated with
participatinginthisstudy.

23
Procedures
Participants who satisfied both inclusion and exclusion criteria were further
screenedwiththePhysicalActivityReadinessQuestionnaire(PAR-Q)tohelpidentify
andexcludethosewithcontraindicationstoMVPA.Demographicandanthropometric
data, suchasage,gender,bodyheightandmass, self-reportedethnicity,aswellas
totalyearsofPolynesiandanceexperience,werecollectedatthebeginningofeach
test session. Prior to their visit, participants were instructed to wear appropriate
clothing and footwear for dancing, to be rested and well hydrated, and to avoid
caffeineintakeatleast2–3hourspriortotesting.Bodyheightwasmeasuredbarefoot
usingaportablestadiometer(InvictaModel#IP0955;InvictaPlasticsLimited,Leicester,
England)tothenearest0.1cm,andbodymasswasobtainedtothenearest0.1kg
usingadigitalscale(Tanitamodel#BF-683W;TanitaCorporationTokyoJapan).These
dataweresubsequentlyusedtocalculatebodymassindex(BMI,kg/m2)asbodymass
(kg)dividedbybodyheight(m)squared.
PolynesianDancesTested
ThePolynesiandancestestedbythisstudywerethosecommonlypracticedand
performedbyexperienceddancersinthe“Hā:BreathofLife”showatthePolynesian
CultureCenter(Laie,Oahu,Hawaii).Thethemeofthisshowwastohighlightspecific
Polynesianculturesbycombiningtraditionalstoriesabouteachculture’soriginwith
traditionalmusicanddancing.Assuch,thisshowfocusedonsixpopularPolynesian
cultures and their respective dances: 1) The Hawaiian hula (both traditional and

24
contemporaryforms)fromtheislandsofHawaii;2)TraditionalFijiandancefromthe
islandsofFiji;3)Maoridances(thehakaforbothmenandwomen,aswellaspoiballs
forwomen)fromNewZealand;4)Samoansasa(menandwomen)andslap(menonly)
dancesfromtheislandofSamoaandAmericanSamoa;5)TraditionalTahitiandance
fromtheislandsofTahiti;6)TraditionalTongandancefromtheislandsofTonga.
TheHawaiianhula, tellsastorywithacombinationofsmoothlycoordinated
hand,head,andlowerbodymotionswhileinastandingposition.Thetraditionalhula
isperformedtoachantandtraditionalHawaiianinstruments(suchasdrums)andis
characteristic of the hula style prior to Westernization of the islands. The
contemporaryhula,incontrast,isperformedtomusicwithmoderninstruments(such
as guitar). TraditionalFijian dance reflects the spiritworld, and is characterizedby
quickupperandlowerbodymovementswithsomejumping.TheMaorihakadance
(forbothmenandwomen)isatraditionalancestralwar(battle)danceduringwhich
dancers perform in a heightened arousal state inferring intimidation. The men
includedmoresquattingmovements,whilethewomenperformedasupportinghaka
witharmmovements,withoutthelargelowerbodysquattingtypemovements.The
Maoripoiballsdance(forwomen),usingpoiballs (twopaddedballsattachedbya
string)asaperformanceequipment,integratesstory-telling,singinganddancing.The
Samoanculturehastwomainformsofdance:thesasa(forbothmenandwomen)and
slap (only formen), both ofwhich depict everyday life activities. Sasa is generally
performedbyalargegroupofpeople,usuallyinaseatedposition,whilesomeparts

25
ofthedancerequirestandingup.Slapistraditionallyperformedbymenandrequires
strengthandstability,duringwhichdancersforcefullyslaptheirhandsontheirown
bodies,insyncwitheachother,withhandsclappingandfeetstampingforwardsand
backwards.TraditionalTahitiandanceisperformedbymenandwomentogetheror
separately, and is characterized by a rapid hip-shaking motion to percussion
accompaniment(i.e.,drums)atafastrhythm.ThetraditionalTongandancefeatures
story-telling through lots of hand and feet gestures. The graceful movements of
womendancerscontrastwiththegreatvigorofthemendancers.Thetempoofallthe
dancemusic used in the “Hā: Breath of Life” show is approximately 130 beat per
minute(bpm),withtheexceptionofthecontemporaryHawaiianhula(80bpm)and
theSamoanslap(180bpm).
DanceTestingProtocol
Participants were tested either individually (i.e., they were the only dancer
tested)oringroupsoftwoorthreewithalldancersbeingtestedsimultaneously.The
group limit of three dancers was set to match the amount of testing equipment
available.Alldancetestingwasperformedinalargeballroomwithhardwoodflooring
on the campus of BYU-Hawaii. Participants, wearing all of the measurement
equipment,beganthetestingwith5minutesofquietsittingforthedeterminationof
sittingrestingmetabolicrate(RMRorVO2REST)andrestingbloodlactateconcentration
([LAREST]). Next, participants were given another 5minutes to warm-up using self-
directedactivities(i.e.,walking, flexibilityexercises,dancing,etc.).Next,asthefirst

26
piece of dance music began, the participants started the first dance routine and
continued for4.5–5.0minutesbeforeanother5minutesofquietsittingrest.The
individualmusicpieceslastedfrom1.5–3.5minuteseach,soeachdancetestingbout
requiredthemusicpiecetobelooped2–3timestoprovidecontinuousmusicfor4.5
–5.0minutes.EventhoughPolynesiandancingdoesnotusuallylastlongerthanthe
longestmusicpiece(i.e.,3.5minutes),thedurationofdancetesting(4.5–5.0minutes)
was considered necessary to provide the best opportunity for steady-state
cardiorespiratoryandbloodlactatemeasures.Inaddition,whendancingasagroupof
2or3simultaneously,thedancersperformedthesamechoreography.Finally,while
mostoftheparticipantsdancedtothe“Hā:BreathofLife”showmusic,afewdancers
brought theirownmusic fordancingwhichwas characteristicof the samecultural
dancestyleandtempoas thatused in theshow.This testingprocess (i.e.,dance5
minutesandrestfor5minutes)wasthenrepeatedforasmanyoftheculturaldances
thattheparticipantscouldperformwithoutself-reportingunduefatigue.Theorder
for performing the dance types was randomly assigned prior to the start of each
testingsession.
MeasurementofCardiometabolicDemands
Thetestingwasconductedunderroomtemperaturebetweenand20–21°C,
relativehumidityof57–71%,andatanaltitudewithin10mabovesealevel.Each
participantwasfittedwithaheartratemonitorcheststrap(PolarElectroInc.,NY,USA)
and a small backpack that carried a portable indirect calorimetry metabolic

27
measurementsystem(OxyconMobile®;VIASYS,SanDiego,CA,USA).Themetabolic
systemwascalibratedpriortoeachtestaccordingtothemanufacturer’sinstructions.
During all testing, participants wore a facemask affixed with an adjustable fabric
headpiecewhichcontainedtheflowtachometerandexpiredgassamplingtubesfor
themetabolicsystem.Heartrate(HR)dataweretransmittedtothemetabolicsystem,
while the real-time respiratory gas measures for oxygen consumption and carbon
dioxideproduction(VCO2)wererecordedcontinuously(breath-by-breath)throughout
theparticipant’srestinganddancetestingwithoutrecalibration.Thebreath-by-breath
samplingby themetabolic systemwas thenusedtosummarizeall cardiometabolic
dataatone-minute sample intervals for subsequentanalyses.The totalmassofall
testingequipmentcarriedbyparticipantswhendancingwas1.5kg.
MeasurementofBloodLactate
Fingertipbloodsamplesweredrawnforlactateanalysis(LactatePlusTM,Nova
BiomedicalUK,Chesire,UK)rightafterRMRmeasurement(whilestillsitting),aswell
as immediately followingeachdanceroutinetocharacterizetheanaerobicexercise
intensity.
DataProcessingandCalculations
Aerobic EECalculations. TheMET (dimensionless)wasused to represent the
aerobic exercise intensity while aerobic activity energy expenditure (aerobic AEE;
kcals·min-1)was calculated to represent thenet aerobic energyproduced from the

28
oxidativesystem.Todeterminethesevariables(METandaerobicAEE),the1-minute
sampleaverageddatafromtheportablemetabolicsystemwereaveragedoverthelast
2minutesforeachdancebout,includingabsoluteVO2(mL·min-1),VCO2(mL·min-1),HR
(beat·min-1),andrespiratoryexchangeratio(RER).First,relativeVO2wascalculatedas:
relative VO2 (mL·kg-1·min-1) = absolute VO2 (mL·min-1)/mass (kg), wheremass was
eithertheparticipant’sbodymass(forRMRmeasurement)orthesumofbodymass
andthe1.5kgequipmentmass(fordancetesting).RelativeVO2wasthentransformed
toMETas:MET=relativeVO2/3.5.AerobicAEEfordancingwascalculatedas:Aerobic
EE(kcals·min-1)=[(EEfordance)–(EEforRMR)],wherebothEEvalueswerecalculated
usingWeir’sequation,EE (kcal·min-1)=3.9xVO2 (mL·min-1)+1.1xVCO2 (mL·min-1)
(Weir1949).
Anaerobic EE Calculations. Anaerobic AEE, or the net anaerobic energy
produced from the glycolytic system,was estimated by the accumulation of blood
lactateconcentration([LA])aboverestingvalues(i.e.,[LAREST]),where1.0mmol·L-1was
assumedtobeequivalenttoarelativeVO2of3.0mLO2·kg-1·min-1(diPrampero1981).
ThisVO2equivalentwasthentransformedintoanaerobicAEE,withaunitofkcals·min-
1,usingacaloricequivalentof20.9kJ(5kcals)perliterofO2(Bertuzzietal.2013).If
thisVO2equivalentwasnegative(i.e.,[LAREST]>[LA]),thentheanaerobicAEEduring
dancewasconsideredtobe0kcals·min-1.Itwasalsoassumedthatthecontributionof
alacticmetabolismduringtheseactivitieswasnegligiblebecausetheATP-PCrsystem

29
ispredominantlyusedduringhigh-intensity(3–5timesthepoweroutputthatelicits
VO2MAX),short-duration(10–15seconds)exercises(Bertuzzietal.2013).
TotalEECalculations.TotalAEEwasthencalculatedasthesumofbothaerobic
AEE (from measured VO2) and anaerobic AEE (from [LA]) contributions. The
contributionofbothaerobicandanaerobicmetabolismsforeachtypeofdancewas
expressedinbothabsolute(kcals·min-1)andrelativeunits(%oftotalAEE).
StatisticalAnalyses
Intraclasscorrelations(ICC)forreliabilitywerecomputedbetweenthelasttwo
minutesoftherawcardiometabolicmeasures:VO2,CO2,andHR(Baumgartnerand
Jackson1995).Descriptivestatisticswerepresentedasmean±SDunlessotherwise
specified.Aone-wayANOVAwithTukey’sHSDpost-hocanalysiswasusedtoevaluate
thedifferencesinMETvaluesacrossdances,whileonesamplet-testswereusedto
comparethemeanMETvaluesforeachtypeofdancetothe3-METand6-METMVPA
thresholds.GenderdifferencesinaerobicandanaerobicEE,aswellastheirrespective
contributionstototalEE,wereexaminedusingindependentt-tests.Allstatisticaltests
wereevaluatedforsignificanceatthe0.05alphalevel,whileaBonferronicorrection
wasusedtocorrectthe0.05alphaforgroupsofsimilartests.Assuch,thet-testsfor
gendercomparisonshadanadjustedalphaof0.008(0.05/6tests),whilethealpha
level was adjusted to 0.006 (0.05 / 8 tests) for the 3-MET and 6-MET threshold
comparisons. All statistical analyses were conducted using SPSS 13.0 for windows

30
(SPSSInc.,Chicago,USA).
Results
CharacteristicsofParticipants
Thedemographicandanthropometricstatisticsforthe13menand17women
participantsarelistedinTable1,suchasage(Mean±SD;22.8±3.1yrs),bodymass
index (BMI; 27.6 ± 5.5 kg·m-2), and Polynesian dance experience (6.6 ± 7.3 yrs).
According to BMI classification standards for adults (American Colleage of Sports
Medicine 2014), the men were represented within all BMI categories from
underweight to obese while the women were classified within normal weight,
overweight,andobesecategories(seeTable1).Inaddition,themeanBMIvaluesfor
menwassignificantlyhigherthanthoseforwomen(P=0.018).Therewerenogender
differencesinrestingHR(HRREST)orVO2REST,butwomenhadsignificantlylower[LAREST]
(1.0±0.4vs.1.5±0.5mmol·L-1;P=0.011),andself-reportedmorePolynesiandance
experiencethanmen(8.9±7.9vs.3.5±5.4yrs;P=0.043).Theself-reportedethnicity
fortheparticipantswasverydiversewith16participantsreportingacombinationof1
–3specificPolynesianethnicities(i.e.,Hawaiian,Fijian,Maori,Samoan,Tahitian,and
Tongan), five others reporting either Asian (n = 2) or Polynesian (n = 3), and the
remainderreportingacombinationof≥1Polynesianwith≥1non-Polynesianethnicity
(White/Caucasian,German,Japanese,orSwedish).

31
Table1.DescriptivestatisticsforPolynesiandancestudyparticipants.
Allsubjects(n=30)
Men(n=13)
Women(n=17)
Age(years) 22.8±3.1 24.1±2.9 21.8±2.9Bodyheight(cm) 168.5±9.7 175.1±9.6 163.5±6.4Bodymass(kg) 79.1±20.6 93.0±23.4 68.4±9.1BMI(kg·m-2) BMIClassificationsa 27.6±5.5 30.2±6.7 25.6±3.3
Underweight 1 1 0 Normal 9 3 6 Overweight 13 3 10 Obese 7 6 1HRREST(beat·min-1) 77.6±12.4 75.2±16.6 79.0±9.5VO2REST(mL·kg-1·min-1) 3.9±1.0 3.9±1.0 4.0±1.1LAREST(mmol·min-1) 1.2±0.5 1.5±0.5 1.0±0.4Danceexperience(years) 6.6±7.3 3.5±5.4 8.9±7.9Allvaluesexpressedasmean±SDunlessotherwisespecified.BMI:bodymassindex.TheparticipantwasconsideredunderweightwhenBMI<20.0;normalweightwhen20≤BMI<25;overweightwhen25≤BMI<30;andobesewhenBMI≥30.HRREST:restingheartrate;VO2REST:restingoxygenuptake;LAREST:restingbloodlactateconcentrationaBMIclassificationareindicatedasthenumberofparticipants
CardiorespiratoryResponsestoPolynesianDancing
Prior to summarizing the cardiometabolic data, the last twominutesof data
were evaluated for intraclass reliability. First, repeatedmeasures ANOVA found no
significantdifferencesbetweenthelasttwominutesofcardiometabolicdata(P=0.17
–0.95).Additionally,theICCcalculationswereconsistentlyhighinmagnitudewithall
values>0.90.GiventhelackofsignificantdifferencesandhighICCvalues,thelasttwo
minutes of cardiometabolic were averaged for all subsequent analyses. Table 2
summarizes the cardiorespiratory and blood lactate responses for each of the
Polynesiandancesevaluated.ApreliminaryanalysisfoundthatmeanMETvaluesfor

32
thetraditionalhula(5.8±1.9;n=6)andcontemporaryhula(6.7±2.6;n=19)were
statisticallysimilar(P=0.436),sothesedatawerepooledandreferredtoas“hula”for
allsubsequentanalyses.Giventhevariedsamplessizesacrossdances(n=3forpoi
ballston=25forhula),theunequalvariances(SD=1.0to3.1METs),aswellasthe
slightly skeweddistributions for somesamples, the sampleswere transformedand
analyzedwiththeplannedOne-wayANOVA.TheANOVAresultsforthetransformed,
however,didnotdifferfromusinguntransformeddata.Thus,theresultsoftheANOVA
withuntransformeddataarereported.TheANOVAcomparingmeanMETacrossthe
danceswassignificant(P=0.001),withonlyMaoripoiballs(lowestmeanMETat3.7)
andSamoanslap(highestmeanMETat9.6)beingstatisticallydifferent.Asshownin
Table 2, percentHRMAX ranged between 64.2% (Tongan) and 79.5% (Tahitian); RER
ranged from 0.81 (Maori poi balls) to 0.95 (Tahitian); and blood lactate from 1.8
mmol·L-1(Maorihaka)to5.2mmol·L-1(Samoanslap).Interestingly,Tahitianhadboth
thehighestpercentHRMAX(79.5%),andthehighestRERvalue(0.95),andamoderately
high[LA] (3.8mmol·L-1),whileSamoanslaphadthehighest [LA] (5.2mmol·L-1)but
neitherthehighestpercentHRMAX(76.7%)northehighestRER(0.93).ThemeanMET
valuesforalldancestested,butMaoripoiballsdance(P=0.168),weresignificantly
greaterthan3.0METs(P=0.003forMaorihaka;P<0.001forHawaiianhula,Samoan
sasaandslap,Tahitian,Tongan,andFijian).ThemeanMETvaluesforSamoansasa,
SamoanslapandTahitianwerealsosignificantlygreaterthan6.0METs(P=0.037,P=
0.001andP<0.001,respectively).

33
Table2.CardiorespiratoryresponsesandbloodlactateconcentrationforeachofeightPolynesiandances.
Dance(n)VO2
(mL·kg-1·min-1) MET HR(beat·min-1) PercentHRMAX(%) RERLA
(mmol·L-1)
Hawaiianhula(25) 22.7±8.4 6.5±2.4*† 138.1±20.3 69.7±10.3 0.82±0.07 2.2±1.9
Fijian(15) 24.5±9.3 7.0±2.6*† 140.7±12.9 71.3±7.4 0.84±0.06 2.4±1.2
Maorihaka(13) 20.8±10.9 5.9±3.1*† 127.1±15.1 64.6±8.2 0.82±0.09 1.8±1.0
Maoripoiballs(3) 13.0±3.7 3.7±1.0 130.4±29.9 65.7±15.2 0.81±0.05 2.7±2.9
Samoansasa(14) 23.1±4.1 6.6±1.2*†‡ 145.6±14.2 73.1±6.7 0.87±0.07 3.0±1.6
Samoanslap(6) 33.6±5.1 9.6±1.5†‡ 150.5±16.5 76.7±8.1 0.93±0.05 5.2±2.0
Tahitian(17) 28.9±6.4 8.3±1.8†‡ 156.9±23.0 79.5±11.3 0.95±0.07 3.8±2.5
Tongan(16) 20.9±8.1 6.0±2.3*† 127.4±23.8 64.2±12.2 0.88±0.06 2.1±1.3
Allvaluesexpressedasmean±SDunlessotherwisespecified.n:samplesize;VO2:oxygenuptake;MET:metabolicequivalent;HR:heartrate;PercentHRMAX:Percentofage-predictedmaximalHR,calculatedasPercentHRMAX=(HR/age-predictedmaximalHR)x100;RER:respiratoryexchangeratio;LA:bloodlactate*Meanvalueformenwassignificantlyhigherthanthatforwomen†significantly≥3METs‡significantly≥6METs

34
GiventhatfiveoftheeightPolynesiandances(i.e.,allbutTahitian,Samoanslap,
andMaoripoiballs)includedgender-specificdancechoreographywithidenticalmusic,
itwasofinteresttocompareMETvaluesbygender.However,splittingtheMETdata
inTable2bygendercreatedsomeextremedifferences insamplesizeandunequal
variances.Thus, inadditiontotheplannedt-tests,theSatterthwaiteApproximation
(Satterthwaite 1946) was used which is a method for handling two-sample
comparisonswith different sample sizes and (or) unequal variances. The statistical
results for this technique,however,were identical to theoriginally-planned t-tests.
Thus,theresultsofthet-testsarereported.WhencomparingtheMETvaluesbetween
menandwomenusingindependentt-tests,themen’sMETvaluesforHawaiianhula,
Samoansasa,Tongan,Fijian,andMaorihakawereallsignificantlygreater(P<0.001;
seeFigure1)thanthecorrespondingvaluesforwomen,whiletheTahitianMETvalues
weresimilar(P=0.526)betweengenders(seeFigure1).
AerobicandAnaerobicContributionstoTotalAEE
CalculationresultsforbothaerobicandanaerobicAEEforbothmenandwomen
are shown in Figure 2(a), while the respective contributions of the aerobic and
anaerobicAEEtothetotalAEEareshowninFigure2(b).AccordingtoFigure2,aerobic
AEEwasthepredominantenergysourceforallPolynesiandancestested.Theaverage
contributionofaerobicAEEtototalAEEwas83.4±14.4%witharangeof74.2±10.9%
(Samoanslap)to88.7±13.7%(Hawaiianhula).Incontrast,themeancontributionof
anaerobicAEEwas16.6±14.4%,witharangeof11.3±13.7%(Hawaiianhula)to25.8

35
±10.9%(Samoanslap).ThesamecalculationsforaerobicandanaerobicAEE,aswell
as the contribution of these AEE sources relative to total AEE, are summarized by
gender in Table 3. The aerobic AEE formenwas significantly higher than that for
womendancingtheHawaiianhula,Samoansasa,Fijian,Maorihaka,andTongan(P=
0.006forHawaiianhula;P<0.001fortheotherfourtypesofdance).Foranaerobic
AEE,incontrast,therewerenosignificantdifferencebetweenmenandwomenforthe
sixdancesperformedbybothgenders(P=0.037–0.500).
1 2 3 4 5 6 7 8 9 10 11 12
METs
Fijian
MaoriHaka
Hawaiianhula
Samoansasa
Tahitian
Tongan
Dances
Men Women
Figure 1.Metabolic equivalents (MET) for eight Polynesian dances by genderwithreferencetothe3-METand6-METthresholdscommonlyusedtodefinemoderateandvigorousexerciseintensities,respectively.Allvaluesexpressedasmean±SD.
36
Table3.Aerobicandanaerobicactivityenergyexpenditures(AEE)andtheirrespectivecontributionstototalEEbygenderforeightPolynesiandances.
Gender(n)
AerobicAEEanditscontributiontototalAEE
AnaerobicAEEanditscontributiontototalAEE
AerobicAEE(kcal·min-1)
p-value Contribution(%)AnaerobicAEE(kcal·min-1)
p-value Contribution(%)
HawaiianhulaM(6) 11.1±4.0
0.006*92.2±7.7 1.0±1.0
0.3297.8±7.7
W(19) 5.0±2.1 87.6±15.1 1.3±2.3 12.4±15.1
FijianM(8) 12.8±4.3 <0.001* 84.6±5.5 2.4±1.1
0.07015.4±5.5
W(7) 4.3±1.0 85.0±14.5 1.1±1.8 15.0±14.5
MaorihakaM(7) 10.2±3.4 <0.001* 88.0±10.1 1.4±1.1
0.03712.0±10.1
W(6) 2.5±0.5 83.8±9.5 0.5±0.3 16.2±9.5Maoripoiballs
W(3) 2.9±1.4 N.A. 81.5±32.1 1.9±3.2 N.A. 18.5±32.1
SamoansasaM(9) 10.1±1.7
<0.001*80.5±16.3 3.0±3.1
0.10919.5±16.3
W(5) 5.7±1.2 81.8±10.6 1.4±1.3 18.2±10.6Samoanslap M(6) 14.5±4.8 N.A. 74.2±10.9 5.1±3.0 N.A. 25.8±10.9
TahitianM(7) 9.8±3.6
0.28284.1±14.1 1.5±1.1
0.04815.9±14.1
W(10) 8.3±2.1 75.3±14.1 3.4±3.0 24.7±14.1
TonganM(12) 10.5±3.7
<0.001*90.0±10.0 1.4±2.4
0.50010.0±10.0
W(4) 1.9±0.4 58.5±16.3 1.4±0.6 41.5±16.3Allvaluesexpressedasmean±SDunlessotherwisespecified.M:men;W:women *MeanvalueforAerobicAEEorAnaerobicAEEwassignificantlyhigherformenthanthatforwomenwhenp-value<0.008

37
Hula Sasa Slap Tahitian Tongan Fijian Haka Poi balls
Polynesian Dances
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
AEE(kcal·m
in-1)
SD f or Total AEE Anaerobic AEE Aerobic AEE
(a)
Hula Sasa Slap Tahitian Tongan Fij ian Haka Poi balls
Polynesian dances
0
20
40
60
80
100
Perc
ent o
f Tot
al A
EE (%
)
Anaerobic AEE (%) Aerobic AEE (%)
(b)
Figure2.Aerobicandanaerobiccontributionstothetotalactivityenergyexpenditurefor
eightPolynesiandances.MeanvaluesforaerobicandanaerobicAEE,aswellasstandard
deviationsfortotalAEE,areshowninFigure2(a,top)wherethetotalAEEisthesumof
bothaerobicandanaerobicAEE.Therespectivecontributionsasapercentofthetotal
AEEfortheaerobicandanaerobicsystemsareshowninFigure2(b,bottom).

38
Discussion
The present study provides insight into both aerobic and anaerobic metabolic
demandsforseveralpopularformsofPolynesianculturaldance.Ourresultsindicatethat
allPolynesiandancestested(exceptforMaoripoiballs)haveMETintensitiesthatexceed
the3-METMVPAthreshold,andthusmaybeconsideredanappropriateexercisemodality
fortheat-riskNHOPIpopulationtomeetthecurrentrecommendationsforPA(USDHHS
2008).However,itwasalsoclearthatthemen’sdancestendedtohavemuchhigherMET
valuesthanthewomen’sdances(i.e.,Hawaiianhula,Fijian,Maorihaka,Samoansasa,and
Tongan) so both gender and the type of Polynesian dance should to be considered
togetherwhendesigningadance-specificPAintervention.
METValuesacrossthePolynesianDancesTested
ThemeanMETvalues for thePolynesiandancesevaluatedby this study ranged
broadlyfromalowof3.7METsforMaoripoiballsandahighof9.6METsfortheSamoan
slap(seeTable2).Interestingly,theMaoripoiballsandSamoanslapwerealsotheonly
twodancesspecifictoonegender(womenandmen,respectively).ThemeanMETvalues
fortheothersixdancesweremoresimilar(5.9–8.3METs;seeTable2),butincludedboth
menandwomendancers.Whencomparedtothe3-METand6-METthresholdsforMVPA,
all,butMaoripoiballsdance,exceeded3.0METs,whileSamoansasa,Samoanslapand
traditionalTahitianexceeded6.0METs.Thus,thehypothesisthatallPolynesiandances

39
testedwouldexceedthe3-METthresholdwasnearlysatisfied,whilethehypothesisthat
onlysome(notall)ofthedanceswouldexceedthe6-METthresholdheldtrue.
ComparableMETdataforPolynesiandancingisrelativelyscarceinthepublished
research literature.TheHawaiianhula, forexample,appearstobetheonlyPolynesian
dancepreviouslyreporteduponwithdirectmeasuresofoxygenuptake.Usagawaetal.
(2014) evaluated the Hawaiian hula (described by the authors as a combination of
traditional and contemporary forms of hula) in competitive Polynesian dancers and
reportedmeanMETvaluesof5.7and7.6METsforslowtempo(low-intensity)andfast
tempo (high-intensity) hula, respectively. The present studymeasured traditional and
contemporaryhulaseparatelyandfoundthesetwosub-stylesofhulatobestatistically
similar(5.8and6.7METs,respectively;P=0.436).Regardless,bothoftheseevaluations
for hula, whether the style was traditional, contemporary, or some combination,
consistently report the intensity to exceed the 3-MET threshold but not the 6-MET
threshold.
Focusing on ballroomdancing, Lankford et al. (2014) reported that the exercise
intensityoffourdancestyles(5.3,5.3,6.4,and7.1METsforwaltz,foxtrot,chacha,and
swing,respectively)withrecreationaldancersalsoexceededthe3-METthreshold.Recent
workfromourownlab(Zhuetal.2016)focusedonevaluatingthemetabolicdemandsfor
Tinikling,atraditionalPhilippinebamboodance.Usingmostlymiddle-agedadultswitha
recreationalfamiliarityofthedancestyle,TiniklinghadameanMETintensityof6.9METs
whichexceededthe6-METthreshold(P=0.0015).Thecommonalityamongstthesedance

40
studies is that MET values were based upon the indirect calorimetry technique for
assessing aerobicmetabolic demands. However, despite the different types of dances
reported upon (Polynesian, ballroom, Tinikling), the different populations assessed
(competitiveandprofessionaldancers,aswellascollege-agedandmiddle-ageddancers),
theresultsconsistentlysuggestthatmanyformsofdancehaveametabolicdemandthat
easilyexceedsthe3-METthreshold,whilesomealsoexceedthe6-METthreshold.
GenderComparisonsforMETValues
The result of the present study supported our second hypothesis that theMET
intensitiesforsomeofthemen’sdanceswouldbesignificantlyhigherthanthoseforthe
women’sdances(seeFigure1).FiveofthesixPolynesiandancesperformedbybothmen
and women (i.e., Hawaiian hula, Fijian, Samoan sasa, Maori haka, and Tongan) had
gender-specificchoreographywhiledancingto identicalmusic.Forexample,theMaori
haka(atraditionalbattledance)hasmenandwomenperforminginaheightenedarousal
state that encourages yellingwith exaggerated facial expressions. However, themen’s
hakaemphasizeshigh-intensityupperandlowerbodymotions,whilethewomen’shaka
involves relatively quiet standing and less exaggerated upper body motions. These
choreographydifferencesexplainwhywomen’shakahadametabolicdemandofonly3.2
METswhilethemen’shakaaveraged8.3METs.Tahitianwastheonlydancethathadno
significant gender difference inMET values, and could also be classified as vigorous-
intensityPAforbothgenders.

41
Thelowermetabolicdemandsexhibitedbythewomendancersmightalsodueto
thewomendancersreportingmorePolynesiandanceexperiencethanthemen(8.9vs.
3.5 yrs, P = 0.043). This observation is consistent with the women hula dancers in
Usagawa’sstudy(2014)whostartedtrainingattheageof5whilemendancersstartedin
lateadolescenceorearlyadulthood.Assuch, it ispresumedthatmoreyearsofdance
experience would lead to higher dancing skill levels and possibly more energetically
efficientdancemovements.However,thisexplanationseemsunlikelygiventhecontrast
inchoreographybetweenmenandwomendancersdescribedabove.Whileamovement
analysiswasnotperformedonthesedancers,thevisualappearanceofthemen’sdance
choreographyoftenappearedmorehighly energetic (i.e., jumping, stomping,dynamic
largerangeofmotiongestures)whilethewomen’sdancesappearedrelativelysubdued
(i.e.,smoothandgracefulbodymotionswithoutjumpingorstomping).Finally,themen
in thepresent studyalsohada significantlyhigherBMI (30.2kg·m-2) than thewomen
dancers(25.6kg·m-2)whichcouldhaveincreasedtheaerobicenergycostformensimply
because of having more body mass when dancing. While having a higher BMI most
certainlycontributedtoahigherabsoluteenergeticcostsfordancing,itisstillmorelikely
that differences in dance choreography between genders was the primary cause for
genderdifferencesamongstfiveofthePolynesiandancestestedinthisstudy.
AerobicAEE
As for aerobic AEE,we observed themean values for theHawaiian hula, Fijian,
Maorihaka,Samoansasa,Samoanslap,aswellas the traditionalTahitianandTongan

42
dancestorangebetween6.5and14.5kcal·min-1(seeFigure2a).Previousdancestudies,
suchasLankfordetal.’srecreationalballroomdancestudy(2014),reportedthatwaltz,
foxtrot,chacha,andswingcostanaverageof5.9kcal·min-1.ForLatinAmericandancing,
Massiddaetal.(2011)reportedmetabolicratesof9.9,8.3,6.6,8.5,and8.3kcal·min-1for
cha cha, samba, rumba, paso doble, and jive, respectively. Emerenziani et al. (2013)
measuredtheAEEinthreedifferentformsofsalsadance:typicalsalsalesson(5.6and4.5
kcal·min-1),ruedadecasinolesson(6.8and5.3kcal·min
-1),andsalsadancingatnightclub
(7.1and4.2kcal·min-1),formenandwomen,respectively.Thesedataarecomparableto
ourfindingsforHawaiianhula(6.5kcal·min-1),Samoansasa(8.6kcal·min
-1),Tahitian(8.9
kcal·min-1),Tongan(8.3kcal·min
-1),Fijian(8.8kcal·min
-1),andMaorihaka(6.7kcal·min
-1),
thoughthepresentstudyistheonlyonetohavealsoassessedtheanaerobicenergycost.
AnaerobicAEE
Itiswellknownthattheaerobicandanaerobicenergycontributionstototalenergy
expenditure during PA will change in response to exercise intensity and duration
(NummelaandRusko1995),aswellaswithexercisemodalities(Scott2005).Unlikemany
classicformsofaerobicexercise(e.g.,walking,jogging,bicycling),manyPolynesiandances
arenotpurelysteady-stateactivitiesduetochangesinchoreographythatcorrespondwith
changesinmusictempoandduration.Thus,abetterunderstandingoftheaerobicand
anaerobicenergysystemcontributionstototalenergyexpenditureduringdancemaybe
important for correct administration and structuring of exercise prescription. To our
knowledge,thisisthefirststudytoevaluatethebothabsolute(kcals·min-1)andrelative

43
(%oftotalAEE)aerobicandanaerobicAEEduringdancingexercise.Inshort,thecurrent
studyfoundthataerobicenergywaspredominantlyusedforallPolynesiandancestested.
Onaverage,aerobicandanaerobicAEEcontribute83.4%and16.6%,respectively,tototal
AEE for Polynesian dances (see Figure 2b). Across dances, theHawaiian hula had the
highestaerobicenergycontribution(88.7%aerobicand11.3%anaerobicforatotalAEE
of7.7kcal·min-1),whileSamoanslaphadthelowestaerobicenergycontribution(74.2%
aerobic and25.8%anaerobic for a total AEEof 19.6 kcal·min-1). These aerobic energy
contributionsarecomparabletootherenduranceexercises,suchas1500mtrackrunning
(77%and86%formenandwomen,respectively),3000mtrackrunning(86%and94%for
men and women, respectively) (Duffield et al. 2005), and 2000 m rowing (87%) (de
CamposMello et al. 2009). By referring to findings of our study (i.e., the aerobic and
anaerobic AEE contributions to total AEE), health practitioners and researchers could
design interventionprogramsusingoneormore formsof Polynesiandance thathave
absoluteorrelativeaerobicAEEequivalenttotraditionalexercisemodalities(e.g.,Samoan
slapvs.men’s1500mtrackrunning,Hawaiianhulavs.2000mrowing,etc.).
LimitationsandFutureResearch
OnelimitationofthisstudyisthatourparticipantswereallexperiencedPolynesian
dancers.Noviceorbeginnerdancersmayhaveverydifferentcardiometabolicresponses
totheseformsofdance.Whilethedependenceofcardiometabolicresponsesondance
experiencehasbeensuggested(Bertuzzietal.2007),thetopicdoesnotseemtohave
been studied or reported upon in the literature. Second, all the dance testing was

44
performedforadurationof4.5–5minstoensurethattheparticipantsreachedsteady-
stateforrespiratorygasanalysis.However,factorssuchasexercisedurationmayinfluence
the metabolic fate of blood lactate concentration (Gastin 2001), and therefore, the
anaerobic AEE estimates from our study only stands for 4.5 – 5minutes steady-state
measurement,andnotgeneralizabletoanylongerdurationofPolynesiandancing.Other
studylimitationsincludethesmallsamplesizesforsomeofourdancedata(e.g.,n=3for
theMaori poi balls dance), and that an objectivemeasure of aerobic fitness, such as
maximaloxygenuptake(VO2MAX),wasnotmeasuredforourdanceparticipants.
Futureresearchshouldconsiderusingdancerswithamorediverserangeofdance
experienceand skill toprovideamorecompleteunderstandingof theenergy cost for
Polynesiandancing.Also,variousdurationsofdancingexerciseshouldalsobeaddressed
in future studies to provide better evidence of the energy system contributions to
Polynesiandancing. Finally, the current study’s analysisofbothaerobic andanaerobic
contributionstototalenergyexpenditureshouldbeexpandedtoothertypesofdanceto
determinethegeneralizabilityofourobservations.
Conclusions
ThepresentfoundthattheaverageMETintensityformostofthePolynesiandances
evaluated(Hawaiianhula,Samoansasaandslap,Fijian,Maorihaka,andTongan,butnot
Maoripoiballs)exceededthe3-METthreshold.However,whenevaluatedbygender,the
men’sMETvaluesweresignificantlyhigherthanthewomen’svaluesforallbuttraditional

45
Tahitiandance.Thus,whiletheseresultssupporttheuseofPolynesiandancingasameans
topromoteincreasedMVPAforhealthpromotionanddiseasespreventionfortheNHOPI
population,thecardiometabolicdosetobeexpectedwillvarybetweenPolynesiandances,
as well as between genders. Regardless, the present study can serve as a starting
referencefortheprescribeduseofPolynesiandancingbyhealthpractitioners,coaches,
exercisephysiologistandresearchers.

46
CHAPTERFOUR-CONCLUSIONS
The present study provides insight into both aerobic and anaerobic metabolic
demandsforseveralpopularformsofPolynesianculturaldance.Ourresultsindicatethat
theaverageMETintensityformostofthePolynesiandancesevaluated(Hawaiianhula,
Samoansasaandslap,Fijian,Maorihaka,andTongan,butnotMaoripoiballs)exceeded
the3-METMVPAthreshold,andthusmaybeconsideredanappropriateexercisemodality
fortheat-riskNHOPIpopulationtomeetthecurrentPArecommendations. Itwasalso
clearthatthemen’sdancestendedtohaveamuchhigherMETvaluethanthewomen’s
dances(i.e.,Hawaiianhula,Samoansasa,Fijian,Maorihaka,andTongan),andtherefore,
bothgenderandthetypeofPolynesiandanceshouldtobeconsideredtogetherwhen
designingadance-specificPAintervention.
Also,thisstudyisthefirsttoreporttherespectiveaerobicandanaerobicenergy
expendituresfordancingexercise.Wefoundthataerobicenergywaspredominantlyused
forallPolynesiandancestested,andthatthecontributionofaerobicAEEtototalAEEfor
alldancestestedaresimilartotraditionalenduranceexercises(i.e.,running,rowing,etc.).
GiventhatmanyPolynesiandancesarenotpurelysteady-stateactivitiesduetochanges
in choreography that correspondwith changes inmusic tempo and duration, findings
abouttheaerobicandanaerobicAEEcouldbeimportantforcorrectadministrationand
structuringofexerciseprescriptionusingoneormoreformsofPolynesiandance.
Theresultsofourstudy,however,arelimitedtoexperiencedPolynesiandancers,
whoweretestedforadurationof4.5-5minutes.Futureresearchshouldconsiderusing

47
dancers with a more diverse range of dance experience and skill to provide a more
completeunderstandingoftheenergycostforPolynesiandancing.Also,variousdurations
ofdancingexerciseshouldbeaddressedtoprovidebetterevidenceoftheenergysystem
contributionstoPolynesiandancing.Finally,thecurrentstudy’sanalysisofbothaerobic
andanaerobic contributions to total energyexpenditure shouldbeexpanded toother
typesofdancetodeterminethegeneralizabilityofourobservations.
Thus,whilethecurrentstudysupportstheuseofPolynesiandancingasameansto
promote increasedMVPAforhealthpromotionanddiseasespreventionfortheNHOPI
population,thecardiometabolicdosetobeexpectedwillvarybetweenPolynesiandances,
as well as between genders. Regardless, the present study can serve as a starting
referencefortheprescribeduseofPolynesiandancingbyhealthpractitioners,coaches,
exercisephysiologistandresearchers.

48
REFERENCES
AasA-M,SeljeflotI,TorjesenPA,etal(2006)Bloodglucoseloweringbymeansof
lifestyleinterventionhasdifferenteffectsonadipokinesascomparedwithinsulin
treatmentinsubjectswithtype2diabetes.Diabetologia49:872–880.doi:
10.1007/s00125-006-0205-8
AinsworthBE,HaskellWL,HerrmannSD,etal(2011)2011CompendiumofPhysical
Activities:asecondupdateofcodesandMETvalues.MedSciSportsExerc43:1575–
1581.doi:10.1249/MSS.0b013e31821ece12
AluliNE,ReyesPW,BradySK,etal(2010)All-causeandCVDmortalityinNative
Hawaiians.DiabetesResClinPract89:65–71.doi:10.1016/j.diabres.2010.03.003
AmericanColleageofSportsMedicine(2014)ACSM’sGuidelinesforExerciseTestingand
Prescription,9thedn.PA:LippincottWilliams&WilkinsWoltersKluwer,Philadelphia
BaumgartnerTA,JacksonAS(1995)Measurementforevaluationinphysicaleducation
andexercisescience,5thedn.WI:Brown&benchmarkPublishers,Madison
BelardinelliR,LacalapriceF,VentrellaC,etal(2008)Waltzdancinginpatientswith
chronicheartfailure:newformofexercisetraining.CircHeartFail1:107–114.doi:
10.1161/CIRCHEARTFAILURE.108.765727
BertuzziR,NascimentoEMF,UrsoRP,etal(2013)Energysystemcontributionsduring
incrementalexercisetest.JSportsSciMed12:454–460.
BertuzziRCdeM,FranchiniE,KokubunE,KissMAPDM(2007)Energysystem
contributionsinindoorrockclimbing.EurJApplPhysiol101:293–300.doi:
10.1007/s00421-007-0501-0
BoothFW,GordonSE,CarlsonCJ,HamiltonMT(2000)Wagingwaronmodernchronic
diseases:primarypreventionthroughexercisebiology.JApplPhysiolBethesdaMd1985
88:774–787.
CaspersenCJ,PowellKE,ChristensonGM(1985)Physicalactivity,exercise,andphysical
fitness:definitionsanddistinctionsforhealth-relatedresearch.PublicHealthRepWash
DC1974100:126–131.
CentersforDiseaseControlandPrevention(CDC)(2004)PhysicalactivityamongAsians
andnativeHawaiianorotherPacificislanders--50StatesandtheDistrictofColumbia,
2001-2003.MMWRMorbMortalWklyRep53:756–760.

49
CullBJ,HaubMD,RosenkranzRR,etal(2015)TheSeatedInactivityTrial(S.I.T.):Physical
ActivityandDietaryOutcomesAssociatedWithEightWeeksofImposedSedentaryTime.
JPhysActHealth.doi:10.1123/jpah.2015-0096
deCamposMelloF,deMoraesBertuzziRC,GrangeiroPM,FranchiniE(2009)Energy
systemscontributionsin2,000mracesimulation:acomparisonamongrowing
ergometersandwater.EurJApplPhysiol107:615–619.doi:10.1007/s00421-009-1172-9
diPramperoPE(1981)Energeticsofmuscularexercise.RevPhysiolBiochemPharmacol
89:143–222.
DomenePA,MoirHJ,PummellE,EastonC(2014)Physiologicalandperceptualresponses
toLatinpartneredsocialdance.HumMovSci37:32–41.doi:
10.1016/j.humov.2014.06.009
DuffieldR,DawsonB,GoodmanC(2005)Energysystemcontributionto1500-and3000-
metretrackrunning.JSportsSci23:993–1002.doi:10.1080/02640410400021963
DuncanKL,LassetterJH,VanServellenG,etal(2015)Therelationshipbetweenselect
demographiccharacteristicsandbodymassindexamongNativeHawaiianandother
PacificIslandercaregivingadults.JTranscultNursOffJTranscultNursSocTranscultNurs
Soc26:31–38.doi:10.1177/1043659614523998
EmerenzianiGP,GuidettiL,GallottaMC,etal(2013)Exerciseintensityandgender
differenceof3differentsalsadancingconditions.IntJSportsMed34:330–335.doi:
10.1055/s-0032-1323722
FaudeO,ZahnerL,DonathL(2015)[Exerciseguidelinesforhealth-orientedrecreational
sports].TherUmschRevThérapeutique72:327–334.doi:10.1024/0040-5930/a000683
GastinPB(2001)Energysysteminteractionandrelativecontributionduringmaximal
exercise.SportsMedAucklNZ31:725–741.
GrandinettiA,ChangHK,ChenR,etal(1999)Prevalenceofoverweightandcentral
adiposityisassociatedwithpercentageofindigenousancestryamongnativeHawaiians.
IntJObesRelatMetabDisordJIntAssocStudyObes23:733–737.
GrandinettiA,ChangHK,MauMK,etal(1998)Prevalenceofglucoseintoleranceamong
NativeHawaiiansintworuralcommunities.NativeHawaiianHealthResearch(NHHR)
Project.DiabetesCare21:549–554.
GrandinettiA,LiuDM,KaholokulaJK(2015)Relationshipofrestingheartrateand
physicalactivitywithinsulinsensitivityinapopulation-basedsurvey.JDiabetesMetab

50
Disord14:41.doi:10.1186/s40200-015-0161-2
GrandinettiA,SeifriedSE,ChowDC,etal(2006)Associationbetweenangiotensin-
convertingenzymegenepolymorphismsandQTdurationinamultiethnicpopulationin
Hawaii.AutonNeurosciBasicClin130:51–56.doi:10.1016/j.autneu.2006.03.012
HegdeSM,SolomonSD(2015)InfluenceofPhysicalActivityonHypertensionand
CardiacStructureandFunction.CurrHypertensRep17:588.doi:10.1007/s11906-015-
0588-3
JAMAPatientPage(2000)Thebenefitsofregularphysicalactivity.JAMA283:3030.
JohnsonDB,OyamaN,LeMarchandL,WilkensL(2004)NativeHawaiiansmortality,
morbidity,andlifestyle:comparingdatafrom1982,1990,and2000.PacHealthDialog
11:120–130.
KesaniemiYK,DanforthE,JensenMD,etal(2001)Dose-responseissuesconcerning
physicalactivityandhealth:anevidence-basedsymposium.MedSciSportsExerc
33:S351-358.
KimH-S,ParkS-Y,GrandinettiA,etal(2008)Majordietarypatterns,ethnicity,and
prevalenceoftype2diabetesinruralHawaii.NutrBurbankLosAngelCtyCalif24:1065–
1072.doi:10.1016/j.nut.2008.05.008
KimY,WilkensLR,ParkS-Y,etal(2013)Associationbetweenvarioussedentary
behavioursandall-cause,cardiovasculardiseaseandcancermortality:theMultiethnic
CohortStudy.IntJEpidemiol42:1040–1056.doi:10.1093/ije/dyt108
KingGL,McNeelyMJ,ThorpeLE,etal(2012)Understandingandaddressingunique
needsofdiabetesinAsianAmericans,nativeHawaiians,andPacificIslanders.Diabetes
Care35:1181–1188.doi:10.2337/dc12-0210
KoutedakisY,JamurtasA(2004)Thedancerasaperformingathlete:physiological
considerations.SportsMedAucklNZ34:651–661.
LankfordD,BennionT,KingJ,etal(2014a)TheEnergyExpenditureofRecreational
BallroomDance.
LankfordD,BennionT,KingJ,etal(2014b)TheEnergyExpenditureofRecreational
BallroomDance.
LookMA,KaholokulaJK,CarvhaloA,etal(2012)Developingaculturallybasedcardiac
rehabilitationprogram:theHELAstudy.ProgCommunityHealthPartnershResEduc

51
Action6:103–110.doi:10.1353/cpr.2012.0012
MarufFA,AkinpeluAO,SalakoBL(2014)Arandomizedcontrolledtrialoftheeffectsof
aerobicdancetrainingonbloodlipidsamongindividualswithhypertensionona
thiazide.HighBloodPressCardiovascPrevOffJItalSocHypertens21:275–283.doi:
10.1007/s40292-014-0063-2
MaskarinecG,CarlinL,PaganoI,etal(2007)Lifestyleriskfactorsforchronicdiseaseina
multiethnicpopulation:ananalysisoftwoprospectivestudiesovera20-yearperiod.
EthnDis17:597–603.
MaskarinecG,JacobsS,MorimotoY,etal(2015a)DisparityindiabetesriskacrossNative
HawaiiansanddifferentAsiangroups:themultiethniccohort.Asia-PacJPublicHealth
Asia-PacAcadConsortPublicHealth27:375–384.doi:10.1177/1010539514548757
MaskarinecG,LookM,TolentinoK,etal(2015b)PatientperspectivesontheHula
EmpoweringLifestyleAdaptationStudy:benefitsofdancinghulaforcardiac
rehabilitation.HealthPromotPract16:109–114.doi:10.1177/1524839914527451
MassiddaM,CugusiL,IbbaM,etal(2011)EnergyexpenditureduringcompetitiveLatin
Americandancingsimulation.MedProblPerformArt26:206–210.
MauMK,SinclairK’imi,SaitoEP,etal(2009)Cardiometabolichealthdisparitiesinnative
HawaiiansandotherPacificIslanders.EpidemiolRev31:113–129.doi:
10.1093/ajerev/mxp004
MenaiM,CharreireH,Kesse-GuyotE,etal(2015)Determiningtheassociationbetween
typesofsedentarybehavioursandcardiometabolicriskfactors:A6-yearlongitudinal
studyofFrenchadults.DiabetesMetab.doi:10.1016/j.diabet.2015.08.004
NummelaA,RuskoH(1995)Timecourseofanaerobicandaerobicenergyexpenditure
duringshort-termexhaustiverunninginathletes.IntJSportsMed16:522–527.doi:
10.1055/s-2007-973048
OgdenCL,CarrollMD,KitBK,FlegalKM(2014)Prevalenceofchildhoodandadult
obesityintheUnitedStates,2011-2012.JAMA311:806–814.doi:
10.1001/jama.2014.732
OkeyoOD,AyadoOLO,MbagayaGM(2009)Physicalactivityanddietaryfatas
determinantsofbodymassindexinacross-sectionalcorelationaldesign.EastAfrJ
PublicHealth6:32–36.
RuizOrtizM,RomoE,MesaD,etal(2010)Prognosticvalueofrestingheartrateina

52
broadpopulationofpatientswithstablecoronaryarterydisease:prospectivesingle-
centercohortstudy.RevEspCardiol63:1270–1280.
SatterthwaiteFE(1946)AnApproximateDistributionofEstimatesofVariance
Components.BiomBull2:110–114.doi:10.2307/3002019
ScottCB(2006)Contributionofbloodlactatetotheenergyexpenditureofweight
training.JStrengthCondResNatlStrengthCondAssoc20:404–411.doi:10.1519/R-
17495.1
ScottCB(2005)Contributionofanaerobicenergyexpendituretowholebody
thermogenesis.NutrMetab2:14.doi:10.1186/1743-7075-2-14
SlentzCA,BatemanLA,WillisLH,etal(2016)Effectsofexercisetrainingalonevsa
combinedexerciseandnutritionallifestyleinterventiononglucosehomeostasisin
prediabeticindividuals:arandomisedcontrolledtrial.Diabetologia.doi:
10.1007/s00125-016-4051-z
SteinbrecherA,MorimotoY,HeakS,etal(2011)Thepreventableproportionoftype2
diabetesbyethnicity:themultiethniccohort.AnnEpidemiol21:526–535.doi:
10.1016/j.annepidem.2011.03.009
SzostakJ,LaurantP(2011)Theforgottenfaceofregularphysicalexercise:a“natural”
anti-atherogenicactivity.ClinSciLondEngl1979121:91–106.doi:10.1042/CS20100520
ThuneI,FurbergAS(2001)Physicalactivityandcancerrisk:dose-responseandcancer,
allsitesandsite-specific.MedSciSportsExerc33:S530-550-610.
UsagawaT,LookM,deSilvaM,etal(2014)Metabolicequivalentdeterminationinthe
culturaldanceofhula.IntJSportsMed35:399–402.doi:10.1055/s-0033-1353213
USDHHS2008physicalactivityguidelinesforAmericans.
WeirJBDB(1949)Newmethodsforcalculatingmetabolicratewithspecialreferenceto
proteinmetabolism.JPhysiol109:1–9.
ZhuW,HeilD,Alforque-TanR,AngostaA(2016)TheMetabolicEquivalentforTinikling:A
PhilippineFolkloricDance.MedSciSportsExerc48:846.

53
APPENDIXA
IRBAPPROVEDINFORMEDCONSENTDOCUMENT

54
PartA:ApplicationInformation
1. TitleofStudy: ThePolynesianDanceStudy
2. PrincipalInvestigator:JoelReece 3. Contact Person (if different
fromPI):
Title:
AssistantProfessor
Dept:
ExerciseandSportScience
Title:
Dept:
Address(+zip):
55-220KulanuiSt.#1968
Address(+zip):
Phone:
675-3353
Email:
Phone:
Email:
4. Co-Investigator(s)(name&affiliation):
Eli Lankford Brigham Young University Idaho, Daniel Heil Montana State
University,WeiZhuMontanaStateUniversity
5. ResearchOriginatedBy(checkone):
Faculty Student Staff
6. ResearchPurpose(checkallthatapply):
Grant
HonorsThesis
Thesis
Other
Dissertation ORCAScholarship
CourseProject:Whichcourse?
7. CorrespondenceRequest:
Mail CallforPick-Up
PartB:ResearchStudySynopsis
1. ShortStudyDescription:
The primary purpose of this study is to determine themetabolic demands of
dancefrom6differentPolynesiancultures.Participantswillperformdancesfrom
anyofthe6culturaldancestheydesire(i.e.,Samoan,Hawaiian,Tongan,Fijian,
Mauri,andTahitian).Alldanceswillbeperformedwhileparticipantsarewearing
a breath-by-breath analyzer during the duration of the dance session. The
analyzerwillrecordheartrate,oxygenintakeandCO2output.Participantswillalso
wearsmallelectronicactivitymonitors(1oneachwrist;1oneachankle;1onthe
hip)sothatwepredictthemetabolicdemandsofPolynesiandancesinthefuture,
such as for a group intervention. The primary outcome for these datawill be
energyexpenditure.
2. StudyLength:Whatisthedurationofthestudy?
October2015-February2016
3. LocationofResearch:
a. Wherewilltheresearchtakeplace?BYUHcampus,Ballroom
b. WillthePIbeconductingand/orsupervisingresearchactivityatanysites
notunderthejurisdictionoftheBYUHIRB? Yes|No

55
PartB:ResearchStudySynopsis(continued)
4. SubjectInformation:
a. NumberofSubjects:75
b. GenderofSubjects:Maleandfemale
c. AgesofSubjects:18-64
5. PotentiallyVulnerablePopulation(checkallthatapply):
Children
CognitivelyImpaired
Prisoners
Faculty’sOwnStudents
PregnantWomen
Institutionalized
Other.Pleasedescribe
6. Non-EnglishSpeakingSubjects:
WillsubjectswhodonotunderstandEnglishparticipateintheresearch:
Yes|No
Ifyes,pleaseprovidethefollowinginformation:
a. Describeyourresourcestocommunicatewiththesubjects:
b. Intowhatlanguage(s)willtheconsentformbetranslated:
7. AdditionalSubjectConcerns:
Arethereculturalattitudes/beliefsthatmayaffectsubjectsinthisstudy?
Yes|No
Ifyes,pleasedescribeattitudesandhowtheymayaffectsubjects.
Culturaldanceactivitywillbeusedtocollectdata.Itispossiblethatsome
maybesensitivetousingculturedancetocollectdata.Onlyvolunteers
willingtodancefordatacollectionwillbeinvolved.
8. DisseminationofResearchFindings:
a. Willtheresearchbepublished? Yes|No
Ifyes,whereifknown?
Peerreviewedjournal
b. Willtheresearchbepresented? Yes|No
Ifyes,whereifknown?
RegionalandNationalconferences
9. ExternalFunction:
Areyouseekingexternalfunding? Yes|No
Ifyes,pleaseprovidethefollowinginformation:
a. Whatagency?
b. Haveyoureceivedfunding? Yes|No Ifyes,dollaramount?
10. MethodofRecruitment(checkallthatapply):
Flyer
ClassroomAnnouncement
LettertoSubject
ThirdParty
Random
Other

56
PartB:ResearchStudySynopsis(continued)
11. PaymenttoSubject:
Willthesubjectbecompensatedforparticipation? Yes|No
Ifyes,pleaseprovidethefollowinginformation:
a. Amount:
b. FormofPayment:
Cash
Voucher
Check
1099
GiftCertificate
Other
c. Willpaymentbeprorated? Yes|No
Ifyes,pleaseexplain:
d. Whenwillthesubjectsbepaid?
EachVisit StudyCompletion Other
12. ExtraCredit:Willsubjectsbeofferedextracredit? Yes|No
Ifyes,describethealternative:
13. Risks:Identifyallpotentialrisks/discomfortstosubjects.
Nomorethanminimalrisk/discomfort.Therisksinvolvedforparticipatinginthis
studymay includemilddiscomfortduringandafterdance. Thesediscomforts
may includeshortnessofbreath, tiredor sore legs,but thesediscomfortsare
common for anyone who participates in moderate intensity exercise. The
participantsmayalsofeelslightdiscomfortwhilewearingtheequipment(head
strap and face mask, back pack with Oxycon Mobile sensors and heart rate
monitor),butthesediscomfortsaremostlyduetothenoveltyofwearingthis
type of equipment during exercise. All attemptswill bemade to ensure that
participantsarecomfortablewithwearingthemeasurementequipmentbefore
anytestingoccurs.
14. Benefits:a. Aretheredirectbenefitstoparticipants? Yes|No
Ifyes,pleaselistthem.
b. Aretherepotentialbenefitstosociety?Yes
Ifyes,pleaselistthem?
c. IncreasedinformationonwhetherPolynesiandanceisaneffectiveform
ofcardiorespiratoryexercise.
57
PartB:ResearchStudySynopsis(continued)
15. StudyProcedures:a. Whatwillbethedurationofthesubjects’participation?60-90minutes
b. Willthesubjectsbefollowedaftertheirparticipationends? Yes|No
Ifyes,pleasedescribe?
c. Describethenumber,durationandnatureofvisits/encounters?
2visits.Visit1:60-90minutes.Eachsubjectwillbescreenedforparticipation
by completing a Physical Activity Readiness Questionnaire (PARQ). Next,
participants will complete a second brief demographic questionnaire, be
measuredforheightandweight,andbefitfortheequipment.Visit2:Body
compositiontest15-30minutes.
d. Whichofthefollowingdescribethestudy? Therapeutic
Non-therapeutic
e. Listallproceduresthatwillbeperformedtogeneratedatafortheresearch.
A questionnaire will include gender, ethnicity, date of birth, and dance
experience.Otherdatawillincludeaccelerometerdata(wrist,ankle,andhip
monitors), oxygen uptake, CO2 output, heart rate. Blood lactate
measurementswillbetakenafterdancingusingafingerprick.
f. Listallprocedures/questionnairesdonesolelyforthepurposeofthe
researchstudy.
PARQ.Questionnaireforgender,ethnicity,dateofbirth,danceexperience.
Accelerometerdata,oxygenuptake,CO2output,heart rate.Blood lactate
measurementswillbetakenafterdancingusingafingerprick.
g. Listallprocedures/questionnairesparticipantsalreadydoregardlessof
research.
16. InformedConsent:
AreyourequestingWaiverorAlterationofInformedConsent? Yes|No
Ifyes,pleaseprovidethefollowinginformation:
a. Filloutandattachthewaiverofinformedconsent.
b. Brieflydescribeyourprocesstoobtainconsent:
All subjects will be asked to read the informed consent form. Prior to
signing the informed consent form, all subjects will receive verbal
explanation.Priortoparticipation,writtenconsentwillbeobtained.

58
PartB:ResearchStudySynopsis(continued)
17. Confidentiality: a. Arethesubjects’socialsecuritynumbers,BYUHIDnumbersorany
identifiers(otherthanstudynumbersandinitials)beingsentoffsite?
Yes|No
Ifyes,describeandexplainreasons.
b. Willanyentityotherthantheinvestigativestaffhaveaccesstomedical,
healthorpsychologicalinformationaboutthesubject? Yes|No
Ifyes,pleaseindicatewho?
c. Brieflydescribeprovisionsmadetomaintainconfidentialityofdata,
includingwhowillhaveaccesstorawdata,whatwillbedonewiththe
tapes,etc.
DatawillbefiledinalockedcabinetinJoelReece’sofficewithaccesstohim
andprimaryresearchersonly.Atthetimeofparticipationsubjectswillbe
givenasubjectnumbertoidentifyanydatalinkedwiththem. Anystudents
involvedwillonlyhaveaccesstodatawithanidentifyingsubjectnumber.
AnyadditionaldatawillbestoredontheViasysmetabolicsystemcomputer
software;thissoftwareisaccessiblebypasswordonly.
WilltherawdatabemadeavailabletoanyoneotherthePIandimmediatestudy
personnel? Yes|No
If yes, describe the procedure for sharing data. Include with whom it will be
shared,howandwhy.
Ifdataispublishedandpeerswouldliketodofollow-upstudies.Rawdatamaybe
sent,butnoidentifyingnameswillbegiven,onlysubjectnumbers.
PartC:
The attached investigation involves the use of human subjects. I understand the
university’spolicyconcerningresearchinvolvinghumansubjectsandIagree:
1. Toobtainvoluntaryandinformedconsentofsubjectswhoaretoparticipateinthis
project.
2. Toreport to the IRBanyunanticipatedeffectsonsubjectswhichbecomeapparent
duringthecourseof,orasaresultof,theexperimentationandtheactiontaken.
3. Tocooperatewithmembersofthecommitteechargedwithcontinuingreviewofthis
subject

59
4. Toobtainpriorapprovalfromthecommitteebeforeamendingoralteringthescope
oftheprojectorimplementingchangesintheapprovedconsentdocument.
5. Tomaintainthedocumentationofconsentformsandprogressreportsasrequiredby
institutionalpolicy.
6. Tosafeguardtheconfidentialityofresearchsubjectsandthedatacollectedwhenthe
approvedlevelofresearchrequiresit.
Signature*ofthePrincipalInvestigator:___________JoelReece__________________
Date:___________10/7/15___________________
FacultySponsorSignatureNecessaryforAllStudentSubmissions
“IhavereadandreviewedthisproposalandcertifythatitisreadyforreviewbytheIRB
Board.Ihaveworkedwiththestudenttopreparethisresearchprotocol.Iagreetomentor
thestudentduringtheresearchproject.”
CommitteeChair/FacultySponsor(Pleasesignandprint):
____________________________________
Thesis/Dissertation–DateofApprovalbytheProposalReviewCommittee:
____________________________________
Ifsubmittingbyemail,pleasecheckthisboxtoverifythatyouarethePIlistedonthis
applicationandagreetofollowtheitemslistedabove.
PartD:SynopsisoftheProposal
PartD,1-9,shouldonlybe5pagesorless(notincludinginstruments,consentforms,etc.).
Pleaseuse12ptfont,pagenumbersandtheheadingsnotedbelow.
1. SpecificAims
1) Determine the average metabolic cost of Polynesian dance using 6 different
cultures(i.e.,Hawaiian,Tongan,Fijian,Samoan,Mauri,Tahitian).
2) Determinetheaveragemetaboliccost foreachtypeofPolynesiandanceand if
therearemetabolicdifferencesamongculturaldances.
3) Determine the specific metabolic cost of different dances for each cultural
Polynesiandancewhereapplicableandiftherearemetabolicdifferencesamong
dances.
4) Determineifthereisametaboliccostdifferencebetweenmalesandfemaleswhile
performingtheirrespectiveculturaldances.
5) Collectelectronicactivitymonitordataatthewrists,ankles,andthehip,foruse

60
inpredictingthemetabolicrateduringPolynesiandanceforfuturedancestudies.
2. Hypothesis
It is hypothesized that Polynesian dance will have a similar metabolic cost across
cultures.
3. BackgroundandSignificance
The popularity of dance is growing (2, 9, 16, 18), alongwith the knowledge of its
potentialhealthbenefits(3-6,10,12-14,17).Thispopularitycanbeseeninelitelevels,
suchDanceSportbeingconsideredasanadditiontothesummerOlympicGames(18)
and at the beginner level in the streets (9). According to Bauknecht (2), ballroom
dancinghasbeenrevivedinAmericawithsuchshowsas,SoYouThinkYouCanDance
onFoxandDancingwiththeStarsonABC. Healthbenefitsfromdancehaveincluded
increasedbonedensity (13), fitness (3,5,10,12),happiness (4),andpsychological
wellbeing(14).Withthisincreasinginterestarounddanceitisimportanttoevaluate
metabolicdemandsofdancetodeterminepotentialhealthbenefitsassociatedwith
uniquetypesofdance.
Metabolic demands for dance have previously been evaluated in general dance,
ballroomdance,AnishinaabeJingledance,andCaribbeandance(1).Themetabolic
costofdancehasawiderangedependingonthetypeofdance.Forexample,slow
ballroomdance(e.g., foxtrot) ismeasuredat3.0metabolicequivalenttasks(METs)
comparedto11.3METsincompetitiveballroomdance.Withthewidevariabilityof
intensitiesindance,itisimportanttounderstandthemetaboliccostofvariouscultural
Polynesiandance.ByunderstandingthemetaboliccostofPolynesiandance,potential
healthbenefitsandappropriatetrainingprogramsforperformerscanbeidentified.
For example, besides potentially improving dance performance, knowing the
metabolic cost of dance may encourage healthier behavior change to decrease
sedentarytime,increasephysicalactivitywithdance,andleadtoadecreaseofdisease
inareaswherePolynesiandancecanbepracticed.
4. DescriptionofSubjects
Approximately75volunteerparticipants(18yearsandolder)thatareexperiencedin
performingatleastoneculturalroutinetomusicfromtheBreathofLifeHashowat
thePolynesianCulturalCenterwillbe recruited.Prior toparticipation,dancerswill
complete a physical activity readiness questionnaire (PAR-Q) to screen for
contraindicationstomoderate-to-vigorousexercise,aswellassignaconsentform.A
questionnaire evaluating dance experience, demographic statistics, and perceived
functionalabilitywillbecompleted.
5. Confidentiality

61
AllparticipantswillbeassignedasubjectIDnumber.Onlyconsentformswillinclude
the names of participants. All other datawill be kept in a locked filing cabinet or
passwordprotectedsoftware.
6. MethodorProcedures
AlldatawillbecollectedonthecampusofBYU-Hawaiiintheballroomdancehallwith
hardwoodflooring.Priortodancing,ethnicity,height,age,gender,andweightwillbe
recorded.Eachparticipantwillthenbefittedfortwotypesofmeasurementdevices:
1)Portablemetabolicmeasurementsystem(OxyconMobile),and2) fiveelectronic
physicalactivitymonitors(Actical).
MetabolicSystem:TheOxyconMobilehasbeenvalidatedthroughconcurrentstudies
withtheDouglasbagmethod. ItiscommonlyacceptedthattheDouglasbagmethod
is the gold standard for obtaining accurate oxygen consumption (11). The Oxycon
Mobile has been tested against the Douglas Bagmethod in studies such as Hans
Rosdahl (15). The study indicates thatwith theOxyconMobile oxygen uptake is
obtainedthroughbreath-by-breathanalysisandcanbedeterminedwithahighdegree
of validity. The portable metabolic system is worn on a vest with two analyzers
mountedtothebackofthevest.Amaskwithstrapsfasteningitaroundtheheadis
alsowornwithasampletubeattachedtotheanalyzers.
Physical Activity Monitors: The Actical is an accelerometry-based physical activity
monitorthatcanbewornonthewrist,ankle,orhipoftheparticipanttoquantifybody
movement.TheActicalisverysmall(thesizeasmallwristwatch)andlightweight(<20
grams),andhasbeenvalidatedforuseinpredictingtheenergycostofmanyactivities
(including total daily energy expenditure). However, the Actical has never been
validatedforpredictingtheenergycostofPolynesiandance.UseoftheActicalsinthis
studywillallowustoevaluatetheenergycostofPolynesiandanceinthefuturewith
theneedfortheportablemetabolicsystem.
After fitting the participant with these devices, participants will sit quietly for 5
minutestomeasuresittingrestingmetabolicrate.Next,theparticipantswillspend
another 5 minutes engaging in self-directed warmup activities that may include
walkingarounddancehall,flexibilityexercises,aswellasdancing.Next,thefirstpiece
of dancemusic will begin and the participant, along with up to 2 other research
participants,willbeginthefirstdanceroutine(asagrouporindividuallydependingon
participants). After 5minutes of continuous dancing, themusic will stop and the
participantswillbeinstructedtositonachairforanother5minutes.Theparticipants
willthenrepeatthisprocess(i.e.,5minutesofdancefollowedby5minutesofquiet
sitting)forasmanyculturaldancesastheyknow.Participantswhocannotdancetoa
62
specificculturedancewillcontinuetosituntilthebeginningofthenextculturethey
arefamiliarwith.Ifnootherculturedancesareknown,participantscanbedismissed
orcanwaituntilalltheroutinesarecompleted.Finally,immediatelyfollowingeach5-
minutedanceroutine,afingertipbloodsamplewillbedrawnforlactateanalysisusing
standardsamplingmethodology.Incombinationwithmeasuresofoxygenuptakeand
heart rate,measuresofblood lactate areused to characterize the intensityof the
danceexercise.
DanceRoutine:Eachculturaldanceroutineismadeupofdancemovesfromaspecific
culture. While a typical dance routine lasts between 3 and 5 minutes, all dance
routinesinthisstudywilllast5minutestoensurethatallthephysiologicalmeasures
of interest (e.g., oxygen uptake, heart rate, blood lactate) achieve a physiological
plateau.ThemusicplayedforeachdanceroutinewillbeplayedtotheBreathofLife
showtoensureaconsistenttempo.
BodyComposition:Subjectswillbeaskedtocompleteabodycompositiontestusing
theBodpod,within2weeksofdancetesting.Thisisanoninvasivemeasurementusing
airdisplacementlastingapproximately15minutes.Standardprotocolofnoteatingor
exercising2hourspriortotestingwillbefollowed.
7. DataAnalysis
Descriptive statistics of height, age,weight, and BMIwill be presented by gender.
Descriptivestatisticsofmetaboliccosts foreachculturaldanceroutineandtypeof
dancewithinculturalroutinewillalsobepresentedbygender.Repeatedmeasures
ANOVAwillbeemployeddodetermineifdifferencesinmetaboliccostexistamong
culturaldanceroutineswithfollow-upposthoctestswhennecessary. Independent
samplet-Testswillbeemployedtodetermineifdifferencesexistbetweenmalesand
femalesforeachculturaldanceroutine.ReliabilityofActicalmeasurementscompared
to theOxyconMobilemeasurementswill be determinedwith regression analysis.
Finally, standard step-forward multiple regression procedures will be used to
determinethebestpredictionofdanceenergycostusingtheActicalmonitors.
8. Risks
Thisstudywillhavenomorethanminimalrisk.Toensurethis,participantswillallbe
screenedwithaphysicalactivityreadinessquestionnaireandbeaccustomedtothe
culturaldancetheywillperform.
9. Benefits
Benefitsof thestudywillbe increasedknowledgeof thecardiovascularbenefitsof
Polynesiandance.

63
10. Compensation
Nocompensationwillbegivenbytheresearchersforparticipatinginthisstudy.
11. References1. Ainsworth,BarbaraE.,etal."2011CompendiumofPhysicalActivities:asecond
updateofcodesandMETvalues."Medicineandscience in sportsandexercise
43.8(2011):1575-1581.
2. Bauknecht, S.. Popularityof TVdance shows inspiresnew interest inballroom,
salsa.PittsburghPost-Gazette(2009).
3. Cobo,JuanRuiz,S.RosRuiz,andMohamedFaroukAllam."Danceforyourhealth."
JournalofPreventiveMedicineandHygiene52.2(2015).
4. FitnessandWellness;Studiesconfirmsballroomdancing isgoodforhealthand
happiness.(2005,June).WorldDiseaseWeekly,799. RetrievedFebruary1,2010,
fromResearchLibrary.(DocumentID:854598061).
5. Flores,R.Dance forHealth: improving fitness inAfricanAmericanandHispanic
adolescents.March-April1995.110(2)189-193,(1994).
6. Hanna,J.L.Thepowerofdance:healthandhealing.JAltCompMed.1:323-331,
1995.
7. Heil,D.P.,PredictingActivityEnergyExpenditureUsingtheActicalActivityMonitor.
ResearchQuarterlyforExerciseandSport77(1),64-80.(2006)
8. Heil,D.P.,KlippelN.J.Validationofenergyexpenditurepredictionalgorithmsin
adultsusingtheActicalelectronicactivitymonitor.MedicineandScienceinSports
andExercise:35(5), S284(2003).
9. Hipp, J. Aaron, et al. "Taking physical activity to the streets: the popularity of
CicloviaandOpenStreets initiatives in theUnitedStates."American Journalof
HealthPromotion28.sp3:S114-S115(2014).
10. Keogh,JustinWL,etal."Physicalbenefitsofdancingforhealthyolderadults:a
review."JAgingPhysActiv17.4,479-500(2009).
11. Liddell,F.D.K.Estimationofenergyexpenditurefromexpiredair.JApplPhysiol.
18:25-29,(1963).
12. Lima,M.M.S. Ballroom dances as a therapy for the elderly in brazil. American
JournalofDanceTherapy,29(2),129(2007).
13. Matthews,B.L.,K.L.Bennell,H.A.Mckay,K.M.Khan,A.D.G.Baxter-Jones,R.L.
MirwaldandJ.D.Wark.Dancingforbonehealth:a3-year longitudinalstudyof
bonemineralaccrualacrosspubertyinfemalenon-elitedancersandcontrols.Ost
Int.17:1043-1054,(2006).
14. Quin,E.,Frazer,L.,&Redding,E. (2007).Thehealthbenefitsofcreativedance:Improving children's physical and psychological wellbeing. Education& Health,
25(2),31-33.
15. Rosdahl, H., Lindberg, T., Edin, F., & Nilsson, J. TheMoxusModular metabolic
systemevaluatedwithtwosensorsforventilationagainsttheDouglasbagmethod.

64
EuropeanJournalofAppliedPhysiology,113(5),1353-67(2013).
16. Sun, Yamei. "LineDance:AnOpportunity forWomen’sHealthandEquality:An
Analysis Based on Line Dance Surveys of China in the 21st Century."Women,
IdentitiesandCulture1.1(2015).
17. Ward,S.Healthandthepowerofdance.JournalofPhysicalEducation,Recreation
&Dance,79(4),33(2008).
18. World Dance Sport Federation. The aspirations. Retrieved August 8, 2015
https://www.worlddancesport.org/About/Olympic/The_Aspirations.
19. Qualifications20. Four qualified professionals with experience in energy expenditure, dance,
physicalactivity,bodycomposition,andaccelerometry.
Includethefollowinginformationasnecessaryintheappropriateappendix.
AppendixI–ConsentDocument
AppendixII–Questionnaires,Surveys,Instruments,Interviewquestion,etc.

65
AppendixI
ConsenttobeaResearchSubjectforthe
PolynesianDanceStudy
Introduction
ThisresearchstudyisbeingconductedbyDr.JoelReece(BYUH),Dr.EliLankford(BYUI),
Dr.DanielHeil (MontanaStateUniversity), andWei Zhu (MontanaStateUniversity) at
BrighamYoungUniversity–Hawaiitodeterminethemetabolicdemandsofdancefrom6
differentPolynesiancultures.Youwereselectedtoparticipatebecauseyouareabilitiesin
Polynesiandances.
Procedures
You will be asked to participate for 60-90 minutes. First you will be screened for
participationbycompletingaPhysicalActivityReadinessQuestionnaire(PARQ).Nextyou
will complete a second brief demographic questionnaire, bemeasured for height and
weight,andbefitfortheequipment.
The questionnaire will include gender, ethnicity, date of birth, dance experience, and
perceivedfunctionalability.Otherdatawillincludeaccelerometerdata(wrist,ankle,and
hipmonitors),oxygenuptake,CO2output,heartrate.Bloodlactatemeasurementswillbe
takenafterdancingusingafingerprick.Withintwoweeksaftertestingyouwillbeasked
tocompleteabodycompositiontest.
Risks/Discomforts
Therearenomorethanminimalrisksforparticipationinthisstudy.However,youmay
feelphysicaldiscomfortfromthefingerpricktomeasurebloodlactateand/orperforming
thedances.
Benefits
There are no direct benefits to subjects. However, it is hoped that through your
participation researchers will learn more about the metabolism that occurs during
Polynesiandancing.
Confidentiality
Allinformationprovidedwillremainconfidentialandwillonlybereportedasgroupdata
with no identifying information. All data will be kept in a locked storage cabinet or
passwordprotectedandonlythosedirectlyinvolvedwiththeresearchwillhaveaccessto
them. The results of this studywill likely bepublished, butno identifying variablesof
individualparticipantswillbereleased.
Compensation
Nocompensationforparticipationwillbeawarded.

66
Participation
Participationinthisresearchstudyisvoluntary.Youhavetherighttowithdrawatanytime
orrefusetoparticipateentirelyatanytime.
QuestionsabouttheResearch
Ifyouhavequestionsregardingthisstudy,youmaycontactDr.JoelReeceat(808)-675-
QuestionaboutyourRightsasResearchParticipants
Ifyouhavequestionsyoudonotfeelcomfortableaskingtheresearcher,youmaycontact
Dr.BoydTimothy,IRBChair,(808)675-3931,[email protected]
Ihaveread,understood,andreceivedacopyoftheaboveconsentanddesireofmyown
freewillandvolitiontoparticipateinthisstudy.
Signature:_______________________________
Date: _______________________________

67
AppendixII
Questionnaires
SubjectID:_____________
Sex
BirthDate
Height
Weight
Ethnicity
Dancestoperform:
Fijian Tongan Samoan
Hawaiian Mauri Tahitian
DanceExperience:
Beginner Intermediate Expert
HowmanymonthshaveyouperformedPolynesiandance?
PerceivedFunctionalAbility(PFA)
Supposeyouweregoingtoexercisecontinuouslyonan indoortrackfor1mile.Which
exercisepaceisjustrightforyou–nottooeasyandnottoohard?
1. Walkingataslowpace(18minutespermileormore)
2. Walkingataslowpace(17-18minutespermile)
3. Walkingatamediumpace(16-17minutespermile)
4. Walkingatamediumpace(15-16minutespermile)
5. Walkingatafastpace(14-15minutespermile)
6. Walkingatafastpace(13-14minutespermile)
7. Joggingataslowpace(12-13minutespermile)
8. Joggingataslowpace(11-12minutespermile)
9. Joggingatamediumpace(10-11minutespermile)
10. Joggingatamediumpace(9-10minutespermile)
11. Joggingatafastpace(8-9minutespermile)
12. Joggingatafastpace(7-8minutespermile)
13. Runningatafastpace(7minutespermileorless)
How fast could you cover adistanceof 3miles andNOTbecomebreathlessoroverly
fatigued?Berealistic
1. Icouldwalktheentiredistanceataslowpace(18minutespermileormore)
2. Icouldwalktheentiredistanceataslowpace(17-18minutespermile)
3. Icouldwalktheentiredistanceatamediumpace(16-17minutespermile)
4. Icouldwalktheentiredistanceatamediumpace(15-16minutespermile)

68
5. Icouldwalktheentiredistanceatafastpace(14-15minutespermile)
6. Icouldwalktheentiredistanceatafastpace(13-14minutespermile)
7. Icouldjogtheentiredistanceataslowpace(12-13minutespermile)
8. Icouldjogtheentiredistanceataslowpace(11-12minutespermile)
9. Icouldjogtheentiredistanceatamediumpace(10-11minutespermile)
10. Icouldjogtheentiredistanceatamediumpace(9-10minutespermile)
11. Icoldjogtheentiredistanceatafastpace(8-9minutespermile)
12. Icouldjogtheentiredistanceatafastpace(7-8minutespermile)
13. Icouldruntheentiredistanceatafastpace(7minutespermileorless)
(George, J.D. et al. Non-exercise VO2MAX estimation for physically active college
students.MedicineandScienceinSportsandExercise.29,415-423,1997)

69
PHYSICALACTIVITYREADINESSQUESTIONNAIRE(PAR-Q)
Name:________________________________Date:____________________
PAR-Q isdesignedtohelpyouhelpyourself.Manyhealthbenefitsareassociatedwith
regularexercise,andthecompletionofPAR-Q isasensible firststeptotake ifyouare
planningtoincreasetheamountofphysicalactivityinyourlife.
Formostpeople,physicalactivityshouldnotposeanyproblemorhazard.PAR-Qhasbeen
designed to identify the small number of adults for whom physical activity might be
inappropriateorthosewhoshouldhavemedicaladviceconcerningthetypeofactivity
mostsuitableforthem.
Commonsense isyourbestguide inansweringthesefewquestions.Pleasereadthem
carefullyandchecktheYESorNOoppositethequestionifitappliestoyou.
YES NO
[] [] 1.Hasthedoctoreversaidyouhavehearttrouble?
[] [] 2.Doyoufrequentlyhavepainsinyourheartandchest?
[] [] 3.Doyouoftenfeelfaintorhavespellsofseveredizziness?
[] [] 4.Hasadoctoreversaidyourbloodpressurewastoohigh?
[] [] 5.Hasyourdoctorevertoldyouthatyouhaveaboneorjointproblemsuch
asarthritisthathasbeenaggravatedbyexercise,ormightbemadeworse
withexercise?
[] [] 6.Isthereagoodphysicalreasonnotmentionedherewhyyoushouldnot
followanactivityprogramevenifyouwantedto?
[] [] 7.Areyouoverage65andnotaccustomedtovigorousexercise?
Ifyouanswered“YES”tooneormorequestions…
Ifyouhavenotrecentlydoneso,consultwithyourpersonalphysicianbytelephoneorin
personBEFOREincreasingyourphysicalactivityand/ortakingafitnesstest.Tellhim/her
whatquestionsyouansweredYEStoonPAR-Q,orshowyourdoctoryourcopyofthis
form.
Ifyouanswered“NO”tooneormorequestions…
You have a reasonable assurance of your present suitability for a graduated exercise
programoranexercisetest.
NOTE:Postponeexercisetestingifyousufferfromminorillnesssuchasacommoncold.
Signature:___________________________ Date:_______________________

70
BRIGHAM YOUNG UNIVERSITY- HAWAII
Institutional Review Board MEMORANDUM Application Approval Notification TO: Joel Reece FROM: Boyd Timothy, IRB Chair
Brigham Young University – Hawaii 808-675-3931 [email protected]
SUBJECT: IRB Application Number: # (15-11)
The Polynesian Dance Study Approval Date: October 9, 2015 Expiration Date: October 8, 2016 Application Type: New Research Type: Non-exempt Application Review Type: Expedited The Institutional Review Board (IRB) of Brigham Young University – Hawaii approved your application. The research was approved in accordance with 45 CFR 46 of Federal Policy for the Protection of Human Subjects, and the University’s IRB policies and procedures. The IRB approves waiver of signed informed consent as per criteria in 45 CFR 46.116(d). Please reference the IRB application number (above) in any future communication regarding this research. Recruitment/Consent: For research requiring written informed consent, the IRB-approved and stamped informed consent document is enclosed. The IRB approval expiration date has been stamped on the informed consent document. Please keep copies of the consent forms used for this research for three years after the completion of the research.