Embed Size (px)
Citation preview

The Kidney Dialysis Case
Limited Resource: Kidney Dialysis machine
Demand vastly exceeds supply
Purely ‘medical’ criteria are insufficient
Goal is to make good (fair/just) distribution decisions
Simple Case
Illustrates relevant principles/considerations that apply generally in health care allocation
Makes concrete what is ‘hidden’ behind QALY/health economics algorithms
Maximizing Outcomes & Fairness can give us completely different prioritizations.
Can conflict when non-linear relationship between resource/input and desired outcome.
(not a direct more resources in, more benefit out)
Outcome-maximizing demands concentrating resource in most-outcome generating
location, fairness demands either even spread or allocation to the worst off.
True of almost any social policy outcome.
Risk of Systematic Bias
People explicitly & implicitly favor those like themselves.
•Seemingly ‘neutral’ criteria can be strongly biased if unjust background
Quality Adjusted Life Years (QALYS)
A measure of the state of health of a person or group in which the benefits, in terms of
length of life, are adjusted to reflect the quality of life. One QALY is equal to 1 year of life in
perfect health. …calculated by estimating the years of life remaining for a patient following a
particular treatment or intervention and weighting each year with a quality of life score (on

a zero to 1 scale). It is often measured in terms of the person's ability to perform the
activities of daily life, freedom from pain and mental disturbance.
Persad, Wertheimer, Emmanuel
Evaluated 8 allocation principles grouped into 4 categories: treating people equally, favoring
the worst-off, maximizing total benefits, and promoting & rewarding social usefulness.
No 1 principle is sufficient to incorporate all morally relevant considerations.
Individual principles must be combined into a multiprinciple allocation system.
Complete lives system
Health: “Species typical” functioning. Functioning normally for some appropriate reference
class (e.g. a gender specific subgroup) of a species. Health is the absence of significant
pathology
Various socially controllable factors contribute to maintaining normal functioning in a
population and distributing health fairly in it, such as:
•Traditional public health and medical interventions
•Social determinants of health
•Income and wealth
•Education
•Control over life and work.
Technological imperative
Tendency to give the best care that is technically possible even it ifs costs are high
(Fuchs 1968)
The pursuit of the most advanced technology and the
desire to implement it without regard to cost.
Use of these medical technologies becomes: self-propagating, requisite, uncritically
accepted
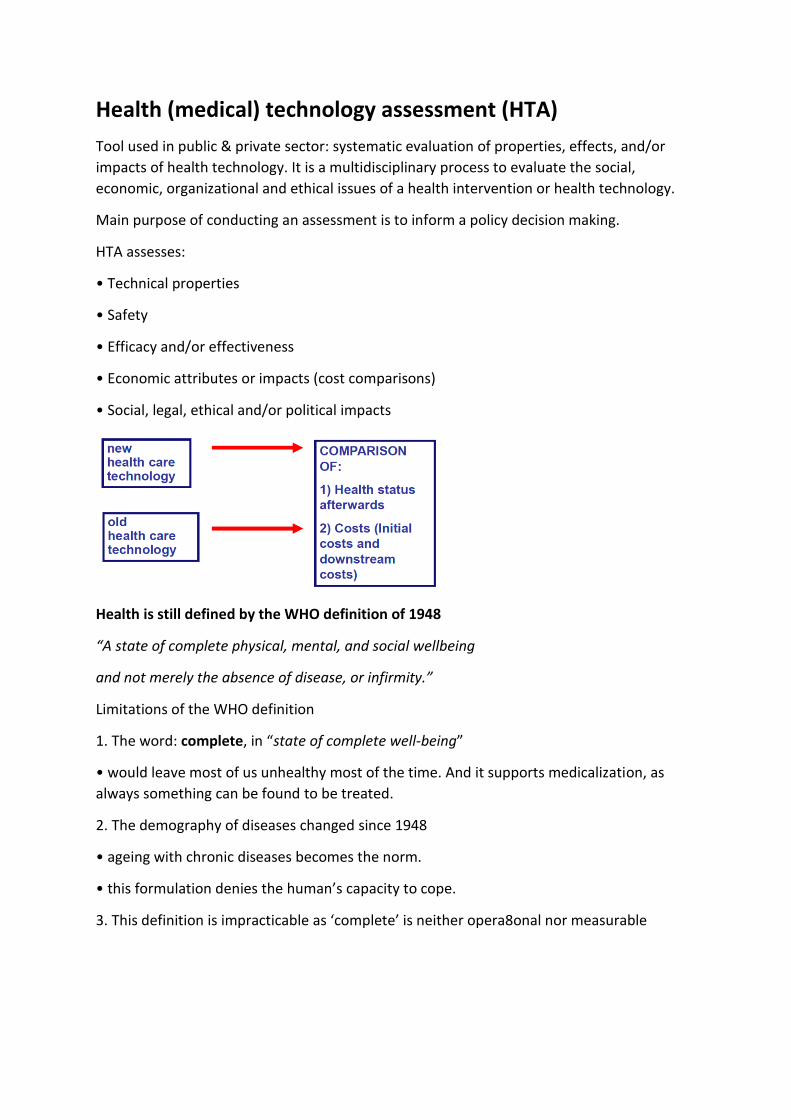
Health (medical) technology assessment (HTA)
Tool used in public & private sector: systematic evaluation of properties, effects, and/or
impacts of health technology. It is a multidisciplinary process to evaluate the social,
economic, organizational and ethical issues of a health intervention or health technology.
Main purpose of conducting an assessment is to inform a policy decision making.
HTA assesses:
• Technical properties
• Safety
• Efficacy and/or effectiveness
• Economic attributes or impacts (cost comparisons)
• Social, legal, ethical and/or political impacts
Health is still defined by the WHO definition of 1948
“A state of complete physical, mental, and social wellbeing
and not merely the absence of disease, or infirmity.”
Limitations of the WHO definition
1. The word: complete, in “state of complete well-being”
• would leave most of us unhealthy most of the time. And it supports medicalization, as
always something can be found to be treated.
2. The demography of diseases changed since 1948
• ageing with chronic diseases becomes the norm.
• this formulation denies the human’s capacity to cope.
3. This definition is impracticable as ‘complete’ is neither opera8onal nor measurable

Nieuw voorstel:
“Health as the ability to adapt and to self manage, in the face of social, physical and
emotional challenges”
What is enhancement?
Strictly speaking, enhancement includes any activity by which we improve our bodies,
minds, or abilities –things we do to enhance our well-being and our capacities.
Narrower definition of Enhancement
Human enhancement involves boosting our capabilities and overcome the limitations of the
body, beyond the species-typical level or statistically-normal range of function for an
individual
Often compared to therapy: Therapy aims to fix something that has gone wrong, while
enhancement interventions aim to improve t the state of an organism beyond its normal
healthy state.
Some of our basic capacities may be altered through technology:
Nanotechnology (boosted immune system)
Genetic manipulation
Cybernetics
Pharmacological enhancement
Prosthetics/exoskeletons
Mind uploading/computer brain interfaces
Which capacities?
Mood
Memory
Intelligence
Physical capacities
Moral capacities
Emotions
Extension of human lifespan/non-human abilities (night-vision, etc.)
And more
Enhancement vs. Therapy
Current therapies and future enhancements interventions do not always map onto
this distinction easily (e.g. palliative care, fertility treatments, abortion, plastic
surgery, euthanasia)
Unclear how to classify interventions that reduce probability of disease/death (e.g.
vaccination)

capacities vary continuously not only within a population but also within the lifespan
of a single individual.
When we mature, our physical and mental capacities increase; and as we grow old,
they decline
Health and Disease
Why is the reference class needed? Well the question is healthy, compared to who?
Normal in one group can be abnormal in another.
Woman with the average testosterone level of a man=diseased
Man with average level of testosterone for a man=healthy
So we need something more specific than normal for the WHOLE species.
Three viewpoints:
1. Bioconservative position:
Enhancement is acceptable as long as it seeks to treat disease and disability with the goal of
improving deficient function to normal levels.
2. Liberal Position
Enhancement is acceptable, even when it attempts to improve patient functionality over
and above what is normal
3. Transhumanist position:
Enhancement is strongly accepted in the hopes that humans will achieve enhanced intellect,
eliminate suffering, increase physical strength, achieve freedom from disease, etc.
Critics of enhancement argue it will:
a. Alter or destroy human nature
b. That altering human nature is a bad thing
Defenders of enhancement respond:
a. Human nature is a varied concept, is maleable, changing, etc. And it contains good and
bad elements
b. It is not a bad thing to alter or destroy human nature-we might change it for the better!
c. Most of what human beings do with any technology is unnatural in some sense, yet these
uses are accepted as benefits, not harms.
Mood Enhancement: Authenticity & Identity
What matters in life is not simply enjoying pleasant experiences. We also want our
experiences to bear the right sort of relation to reality.

This point is connected to one’s view of happiness & the good life
Positional Goods: goods whose value to those who have them depends upon others not
having them.
Deep Brain Stimulation
Deep brain stimulation (DBS) involves implanting electrodes within certain areas the brain.
Electrodes produce electrical impulses that regulate abnormal impulses/ the electrical
impulses can affect certain cells and chemicals within the brain.
Amount of stimulation in deep brain stimulation is controlled by a pacemaker-like device
placed under the skin in patient’s chest.
Wire that travels under the skin connects this device to the electrodes in the brain
What is it used for?
Essential tremor
Parkinson's disease
Dystonia
Epilepsy
Tourette syndrome
Chronic pain
Obsessive compulsive disorder
DBS is also being studied as an experimental treatment for major depression, stroke
recovery, addiction and dementia.
Personality Change & Authenticity
1. Yves Agid described that up to 65% of the married (or living with a partner) PD
patients experienced a conjugal crisis after the operation. Different reasons could be
found for this, but personality changes could clearly play a role (Agid2006).
2. Increased Impulsivity (hypersexuality, compulsive eating, and pathological gambling)
3. Key to note that personality changes were likely already taking place as a
consequence of the disease state.
An intervention like DBS that seems to majorly improve QoL on one dimension (like
reduction of PD tremors or symptoms of severe OCD) can potentially decrease QoL in other
areas, both for the person getting the treatment and for those around him or her.
This treatment improves QoL along different dimensions for different people ands they
value these changes or disvalue them to different extents.

Sometimes the impact of the intervention is so strong that people experience it as changing
their ability to control their lives or truly live as themselves.
QoLValue Conflicts: Privacy and Security, Surveillance Technologies Privacy violations Come in multiple forms:
Deepest secrets shared—things you’ve done you’re ashamed of, crimes committed, health conditions.
Being watched, when vulnerable, without your knowledge.
Blackmail—the threat to release info etc to certain people.
Government possessing certain information
Information that could be used to harm you. What is a privacy violation? In general, privacy violations at the core: when information about a person is shared with people that the person would not want the info shared with. People who possess, collect, process, and use information about you: • Family members—parents, children, siblings • Friends • Neighbors • Employer • Government • Retailers • Service providers • Health care providers • Insurers • Other institutions—universities Reasonable expectation of privacy
Meant as guide to contexts where your information has special protections.
Used to be interpreted as: expectation of privacy within home; none outside home.
But then interpreted as:Sometimes extending outside the home (e.g. to phonebooth)
And also reduced right to privacy within the home (e.g. helicopter observing marijuana plants)
No longer so useful—technology changes our expectations of privacy, we expect certain privacies outside home and have lost some inside home (e.g. internet monitoring). Foreseen and unforeseen privacy harms Foreseen:
Electronic medical records
Centralizing info, making access easier.
Computerized face recognition
Technology to read and record license plates Unforeseen:
Credit card usage, mobile phone location info. Information used in unexpected ways.
Tax returns, oyster card Electronic Medical Records in NL

Problems:
Centralized access means more attractive to criminals
Any health care provider with access to system could access any patient records (or last five visits)
Encryption quality criticized Advantages
Easier to access more data
Easier for more people to access data
Potentially: easier to restrict data to particular people?
Can make data available for limited time
Easier to make only certain data available
Can track who accesses what data
Solove: privacy problems can be produced by
“Information processing” and exclusion—someone (the government, the health system) having more info about you and what’s going, and control over than info, than you have. You can’t fix errors in the data; you can’t predict who knows what, you can’t influence how the data is used.
Aggregation—how can the info be combined with other info in a way that might be harmful
Distortion—how can just some of the info—“only part of the story”—pose a harm?
The potential for secondary use—national ID cards.
Just the knowledge of surveillance. Inhibition of activities: movement, speech, purchases, socializing, friendships
How much do people really care about privacy? Sceptic: Not much. People say they care. Then choose convenience over privacy Privacy advocates respond: People don’t really have a choice. People don’t know what is being done with data. People don’t fully realize consequences of sharing data So, despite sceptics, privacy is likely to be a value that people take seriously, into the future. Value tensions / conflicts: Value tensions occur when supporting one value in a technology challenges another value. They can occur within a single individual, between an individual and a group, or across different groups. Resolving value conflicts

Sometimes we willingly give up access to information:
To government (police, FBI), in exchange for security
To government (income info), in exchange for services that support our well-being Welfare, social security
To health organizations in exchange for services that support our well-being
We consent to giving access to information to certain people for certain uses.
Transitions in healthcare & food systems
1. The discussion with regard to a new definition of health is an inextricable part of the current transition in the healthcare system
2. Transition of the healthcare system is closely related to developments in medicine and medical technology and in hygiene and sanitation, but also to changes within the food system
3. Stakeholders do not only feel the consequences of transitions in socio-technical systems but also can be active in changing socio-technical systems
4. Stakeholders that are part of the existing socio-technical system differ in their role and possible transformative actions with those involved in experiments (niches)
Multi-Level Perspective (MLP) Landscape: long-term developments, trends and major crises Regimes: mainstream, established / dominant practices, structures and cultures Niches: innovations or radically new practices, ideas or organizing principles
Transitions:

Transformation processes in which society changes in a fundamental way over a generation or more
Radical shifts from one system to another Transition s-curve:
Transitions happen when:
There is sufficient pressure from the landscape
Regimes become unstable and open for change
Niche-innovations are sufficiently developed
What is Transition Management?
A practical approach to guide transitions towards sustainability
Aimed at mobilizing different people, organisations and networks for sustainable system innovation
Characteristics of a transition:
Radicalshift (fromonesystem toanother)
Long-term process(20-50 years)
High levels of complexity and uncertainty
Multi-actor (science, policy, firms, ngo’s, users, etc.)

Transition Management: characteristics
Combining a long-term vision with short-term objectives
Thinking in terms of: •Multi-domain (e.g. within the healthcare sector) •Multi-actor(science, industry, ngo’s, users, etc.) •Multi-level(niches, regimes, landscape)
Learning-by-doing and doing-by-learning
Aiming for system optimization and system innovation
Keeping a large number of options open Transition management: 4 main aspects of approach
Develop a guiding vision of a sustainable future
Build up a long-term “transition agenda” (including shared objectives and transition paths)
Create space for experimenting and learning(in ‘niches’, pilot projects or ‘transition experiments’)
Facilitate reflection(“are we still doing the right things?”)
Ongoing transition in Dutch healthcare
Neighbourhood Care
“Buurtzorg” is an innovative approach to homecare
Founded in 2006 by a former community nurse, now 800 independent teams with 9000 nurses
Agitated against the bureaucratic way Dutch homecare was (is) organised
Developed the “Self-Managed Team” approach
Scaled up from successful ‘transition experiment’ to mainstream model in long-term care
Conceptual framework to study processes & strategies for ‘scaling-up’
Deepening: learning about new practices, structure and culture within a specific context (niche-development)
Broadening: repeating and connecting radically new practices, structure and culture in different contexts (linking different niches)
Scaling-up: embedding in dominant practices, structure and culture at the level of a societal system; influencing the regime or mainstream (societal embedding)

Deepening: Learning and experimenting activities of Buurtzorg
Starting with a societal challenge: better healthcare, lower costs
Demonstrating societal costs & benefits with Societal Business Case Broadening: Repeating and connecting activities of Buurzorg
Translation to other healthcare domains (e.g. mental healthcare, welfare, youth care, maternity care)
International expansion of Buurtzorg Scaling-up: Societal embedding activities of Buurtzorg
Influencing different elements of the healthcare system: national policy, education, starting a new healthcare insurance, etc
Food & health It is difficult to isolate the impact of food intake from other factors (e.g. physical
exercise, drinking, smoking habits)
Scientific progress in nutrition research leads to more nuanced conclusions Health enhancing measures are difficult due to the complicated relationship between food & health
Role of government in health enhancing policy is mostly indirect
Decreasing trust in science and experts from the 1970s onwards complicated health enhancing policy
Relation between food consumption and health not straightforward:
Difficult to isolate the impact of food intake from other factors (e.g. physical exercise, drinking, smoking habits)
Scientific progress in nutrition research leads to more nuanced conclusions This complicates health enhancing measures