Embed Size (px)
Citation preview

American Journal of Medical Genetics 14:773-782 (1983)
The Kenny-Caffey Syndrome: Growth Retardation and Hypocalcemia in a Young Boy
W. K. Lee, A. Vargas, J. Barnes, and A. W. Root
Departments of Pediatrics and Radiology, University of South Florida College of Medicine, Tampa, and the All Children’s Hospital, St. Petersburg, Florida
A 2-year-old black boy with the Kenny-Caffey syndrome was first evaluated because of growth retardation and hypocalcemia. Hypothalamic-pituitary function was normal. Basal serum somatomedin C levels were normal for age, but did not increase during short-term administration of human growth hormone. Serum immunoreactive parathyroid hormone levels remained inappropriately low during spontaneous and induced hypocalcemia, indicating that hypocalcemia was the consequence of hypoparathyroidism. The manifestations of 15 patients with this syndrome are tabulated.
Key words: growth retardation, hypocalcemia, hypoparathyroidism, Kenny-Caffey syndrome, medullary stenosis, autosomal-dominant inheritance, X-linked dominant inheritance
INTRODUCTION
The Kenny-Caffey syndrome is characterized by intrauterine and postnatal growth retardation, uniformly small and slender long bones with medullary stenosis, and diaphyseal cortical thickening, hypocalcemia, and hyperphosphatemia [Kenny et al, 1966; Caffey, 19671. We began evaluation of a black male with this syndrome at 2 8/12 years and have attempted to define the causes of growth retardation and hypocalcemia in this patient. We present these data and review the literature on this syndrome.
Received for publication July 17, 1982; revision received October 4, 1982.
Address reprint requests to Dr. Allen W. Root, All Children’s Hospital, 801 Sixth Street South, St. Petersburg, FL 33701.
0 1983 Alan R. Liss, Inc.

774 Leeet al CLINICAL REPORT
The patient was the product of a nonconsanguineous union, delivered vaginally at 38 weeks’ gestation to a gravida I mother following a pregnancy complicated by transient vaginal bleeding in the fourth month. Birth weight was 2.6 kg (5th centile) length 46 cm (5th centile), occipitofrontal head circumference (OFC) 34.5 cm (50th centile). Large fontanelles and separation of the cranial sutures were noted, but computerized scan of the head was normal. At 10 weeks the infant had several brief tonic convulsions and was hospitalized. OFC was 39 cm and fontanelles and cranial sutures were widely open. Serum calcium levels were low (3.5-8.3 mg/dl), and serum phosphate concentrations (4.7-8.9 mg/dl) were normal to high. The serum magnesium value was 2.6 mg/dl (normal range 1.8-2.6). Despite low serum calcium levels, the patient had no further seizures. A second computerized scan showed wide separation of the metopic and other cranial sutures and large fontanelles but no other anomalies. The persistently low serum calcium and high serum phosphate levels and an inappropriately low serum concentration of immunoreactive parathyroid hormone (iPTH) 168 pg/ml (normal 164-457 pg/ml; Upjohn Laboratory, Kalamazoo, Michi- gan) led to the diagnosis of hypoparathyroidism. He received ergocalciferol (28,000 unitdday), elemental calcium (345 mg/day), and phenobarbital. At 7 months the boy sustained a fracture of the middle of the left femur. He continued to receive ergocal- ciferol and calcium, and the fracture healed normally. However, the mother inadver- tently increased the dose of ergocalciferol to 200,000 unitdday .
At 2 8/12 years the child was noted to be hypercalcemic (12.4 mg/dl) and he was referred to us. On examination he was an active, intelligent, immature-appearing black boy with height of 77 cm (height age: 13 months); weight 9.15 kg (weight age: 13 months); OFC 49.5 cm (25th centile for age) (Fig. 1). The anterior fontanelle measured 10 x 6 cm, the posterior fontanelle 3.5 X 3.5 cm. Metopic and sagittal sutures were widely separated. On ophthalmological study his eyes were normal. He had 20 teeth with much caries. Except for hypercarotenemic palms and soles, he was otherwise normal.
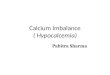
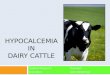
Two weeks after discontinuing all medication, the child was reevaluated. Skull films showed a large anterior fontanelle with widely separated metopic suture. The calvaria was thin, and the diploic space was absent (Fig. 2). Medullary stenosis with relative cortical thickening of the diaphyses was noted in all tubular bones (Fig. 3). Bone age was 2 1 months.
Following infusion of Na2EDTA (50 mg/kg over 2 h) [Tsang et al, 19761, total and ionized serum calcium values declined, but serum immunoreactive parathyroid hormone (iPTH) (midregion assay) levels did not increase above basal values (Table I) and there was no increase in urinary excretion of cyclic adenosine monophosphate. Basal concentrations of thyroxine (9.1 pg/dl), triiodothyronine (143 ng/dl) and TSH (1.1 pU/ml) were normal. There was normal diurnal variation of serum cortisol levels (a.m. 21.1 pg/dl; p.m. 3.9 pg/dl) and a normal cortisol secretory response to insulin hypoglycemia (2 1.1-38.9 pg/dl). The patient was insulin-sensitive. After intravenous injection of regular insulin (0.1 unitdkg), the glucose concentration declined from 63 mg/dl to a low of 26 mg/dl 20 min after injection and was 37 mg/dl 1% hours after injection. The peak growth hormone secretory response to insulin hypoglycemia was subnormal (< 3 ng/ml); that to arginine infusion was low normal with a peak of 5.5 ng/ml (normal > 5 ng/ml). Somatomedin C levels ranged between 0.16 and 0.26 U/ ml (Nichols Institute, Los Angeles; normal for age: 0.12-1.5). Chromosomes (Giemsa banding) were normal (46,XY).

Kenny-Caffey Syndrome 775
Fig. 1. Patient at 2 8/12 years of age.
Fig. 2. The calvaria was thin and lacked diploic space.
Lateral skull radiograph showing large anterior fontanelle with widely separated metopic suture.

776 Leeet a1
Fig. 3. Radiograph of tibia and fibula demonstrating cortical thickness in diaphyses and marked medullary stenosis.
TABLE I. Effect of NazEDTA on Calcium Homeostasis
Serum levels in relation to infusion of 50 mg/Kg Na2EDTA over 2 hours
Patient - Ih Oh + % h + I h + 2 h f 3 h + 4 h Total calcium (mg/dl) 9.6 9.1 8.2 7.7 7.4 7.1 7.1
iPTH (pg/ml)a 168 <125 <125 <125 < 125 <125 <125
Total calcium 9.3 If: 0.4b 8.1 * 0.88 8.1 If: 0.9 8.5 f 0.7 8.6 f 0.5 Ionized calcium 4.2 f 0.4 2.8 f 1.2 3.0 +_ 0.6 3.4 & 0.8 3.9 t 0.6 iPTH 98 f 52 140 f 72 134 f 87 113 * 74 92 * 46
Ionized calcium (mgfdl) 5.4 4.2 2.8 3.0 3.0 3.2 3.5
Control individuals (N = 16)
aMethod of Root et al [ 19741. bff + 1 SD.

Kenny-Caffey Syndrome 777
Dihydrotachysterol (DHT) 0.2 mg thrice daily maintained serum total calcium levels of 8-11.4 mg/dl and ionized calcium values of 3.58-4.62 mg/dl during the first year of observation. Serum iPTH levels were never greater than 125 pg/ml despite intermittent hypocalcemia. Several serum calcitonin levels were less than 50 pg/ml (Bioscience Laboratory, Van Nuys, California; normal < 450 pg/ml). Serum 25- hydroxyvitamin D values ranged between 14.4 and 25.9 ng/ml, and 24,25-dihydroxy- vitamin D concentrations between 1.2 and 2.8 ng/ml during the period of observation. On two occasions when not receiving DHT serum concentrations of 1,25-dihydroxy- vitamine D (Bioscience Laboratory) were 52 and 40 pg/ml (normal 20-76 pg/ml); total serum calcium concentrations were 9.4 and 7.1 mg/dl respectively.
After 12 months of observation height and weight continued to deviate from normal with a height velocity of 4.4 cm/yr and weight velocity of 0.35 kg/yr (Fig. 4). At 3 8/12 years the patient was reevaluated. He was hypomagnesemic (0.7 mEq/ L), but serum concentrations of magnesium returned to normal (1.5-1.9 mEq/L) after administration of magnesium (266 mg/day orally). During this period DHT was discontinued and the child became hypocalcemic while eumagnesemic. Serum iPTH values were undetectable at this point. After readministration of DHT, serum calcium levels rose to normal. Basal somatomedin C concentration was 0.35 U/ml and did not change after three injections of human growth hormone (0.1 U/kg).
Skeletal roentgenograms and serum concentrations of calcium were normal in mother and father.
DISCUSSION AND LITERATURE REVIEW
The manifestations of 15 patients with the Kenny-Caffey syndrome are presented in Tables I1 and I11 [Boynton et al, 1979; Caffey, 1967; Frech and McAlister, 1968; Kenny and Linarelli, 1966; Majewski et al, 1981; Wieland et al, 1981; Wilson et al, 19741.
Growth Retardation The birth weight and length of our patient were at the 5th centile for gestational
age; postnatally the growth rate was slow (Fig. 4). In 3/11 patients the birth weight was < 2.5 kg and length < 45 cm. Twelve patients were proportionally dwarfed later in life, two had micromelic dwarfism [Weiland et al, 19811, and one (Table 11: AM) was of normal height (75 cm) at 1 year [Majewski et al, 19811. The reported adult heights of affected subjects ranged from 121 to 149 cm [Boynton et al, 1979; Kenny and Linarelli, 1966; Majewski et al, 19811.
In our patient the growth hormone secretory response to arginine infusion was normal. Basal somatomedin C levels were low normal and did not increase during short-term administration of human growth hormone. The significance of this obser- vation is uncertain, as low basal somatomedin C values may not increase after short- or long-term administration of somatotropin, even in hyposomatotropic patients in whom there is increase in linear growth velocity during long-term administration of this material [Kemp et al, 19811.
Majewski et a1 [1981] recorded normal growth hormone secretion in two patients (Table 11: GS, BS). One patient (Table 11: US) with a borderline growth hormone secretory response was treated with 4 units of human growth hormone twice weekly for 9 months without acceleration of linear growth velocity [Majewski et al,

778 Lee et a1
Fig. 4. Growth chart of the patient.

TABLE
11.
Rep
orte
d Pa
tient
s W
ith K
enny
-Caf
fey
Synd
rom
e*
Caf
fey,
19
67;
Ken
ny a
nd
Wils
on
Boy
nton
W
iela
nd
Lina
relli
, Fr
ech
and
et a
l, et
al,
Maj
ewsk
i et a
l, et
al,
Pres
ent
1966
M
cAlis
ter.
1968
19
74
1979
19
81
1981
re
uort
Patie
nt
M
FD
LL
LR
1 4
GS
BS
US
AH
M
H
DB
SM
TM
D
B Se
x F
M
F M
M
MF
M
MM
F
M
F F
M
Chr
onol
ogic
age
(yea
rs)
39
3.3
1 19
13
19
37
16
.5
7.5
1 31
54
6
7 2
Pren
atal
ons
et o
f gro
wth
+
+
+
Del
ayed
clo
sure
of a
nter
ior
+ +
+ +
-+
+-
+
+ +
R
efra
ctio
n an
omal
ies
of
HH
N
H
HH
HM
M
MH
H
N
-
--
-
-
-
- -
reta
rdat
ion
Prop
ortio
nate
ly d
war
fed
++
+
+ +
+ +
+ +
* +
+ M
DM
D
+
font
anel
le
eyes
M
icro
phth
alm
ia
Nor
mal
inte
llige
nce
Sym
ptom
atic
hypo
calc
emia
A
nem
ia
Del
ayed
bon
e ag
e C
ortic
al th
icke
ning
with
m
edul
lary
sten
osis
of
the
tubu
lar b
ones
C
alva
rial t
hick
ness
: Th
ick-
Tk;
Thin
-Tn
Cal
varia
: Dip
loic
spa
ce
++
+
+
++
-
+
+ +
+
Tk
Tk
-
+ + + + + + -
-
Tn
Tk
++
+ +
?+
- -
++
+-
++
+
++
- -
++
+
+-
- +
-
+ +
+-
+
++
++
-+
NN
NN
Tk
+ +
++
+ +
+ +
++
+
P?
-
-
+ fn
Y
-
E
Tk
B 9
Tn
8
1
fn
*Nor
mal
gro
wth
at
12 m
onth
s; H
, hyp
erop
ia; M
, myo
pia;
N, n
orm
al;
MD
, mic
rom
elic
dw
arfis
m;
+, pr
esen
t; -,
abs
ent;
Bla
nk, n
ot s
tate
d.

780 Leeet a1
TABLE 111. Major Manifestations of Individuals With the Kenny-Caffey Syndrome
Number of patients affected/Total
Prenatal onset of growth delay Proportional shortness of stature Delayed closure anterior fontanel Refraction anomalies Microphthalmia Normal intelligence Symptomatic hypocalcemia Anemia Delayed bone age Cortical thickening with medullary
Calvaria: Abnormality of thickness Calvaria: Presence of Diploic Space
"Two with micromelia, one normal. bEight with hyperopia, three with myopia. 'One with cortical thickening only. dFive thick. two thin.
stenosis of the tubular bones
3/11 12/15= 9/11 11/13b 6/11 11/13 11/15 5/11 61 10 14/15'
7/l ld 219
19811. Thyroid function has been normal in all patients studied [Majewski et al, 198 11. Although the TSH secretory response to thyrotropin-releasing hormone was exaggerated in two patients (Table 11: BS, US), the data suggest that in most patients with the Kenny-Caffey syndrome growth retardation does not begin prenatally and is probably not due to dysfunction of the hypothalamic-pituitary unit.
Hypocalcemia Episodic symptomatic hypocalcemia was present in 11 115 patients, with onset
from the first few days or weeks of life to the 4th decade [Boynton et al, 1979; Frech and McAlister, 1968; Majewski et al, 1981; Wilson et al, 19741. Basal serum iPTH concentrations in our patient were usually undetectable; when measurable, they were inappropriately low for the concurrent low serum calcium levels. There was no iPTH secretory response to EDTA-induced hypocalcemia, which is consistent with hypo- parathyroidism. In infancy, the serum magnesium concentration of our patient was normal. At 3 8/12 years he was hypomagnesemic, but restoration of the eumagne- semic state did not increase serum calcium or iPTH values, indicating that the hypomagnesemia resulted from hypoparathyroidism [Anast et al, 1972; Tsang, 19721. Boynton et a1 [1979] described a 19-year-old hypocalcemic patient (Table 11: 4) in whom no parathyroid tissue could be identified at postmortem search of the neck. Wieland et a1 [1981] reported one patient (Table 11: SM) with an undetectable serum iPTH level; another subject (TM) had elevated iPTH concentrations in a radioim- munoassay detecting predominantly the biologically active intact hormone, but unde- tectable in an assay recognizing the carboxyl-terminal fragment. Both patients in this report [Weiland et al, 19811 had normal serum 25-hydroxyvitamin D and 1,25- dihydroxyvitamin D concentrations. Levels of 1,25-dihydroxyvitamin D were normal in our patient. Majewski et a1 [1981] reported normal iPTH and calcitonin secretory responses in 5/6 patients after intravenous calcium administration. In one patient (Table 11: AH) the calcitonin level was slightly elevated. In our patient serum

Kenny-Caffey Syndrome 781
calcitonin levels were normal. These data suggest that in most patients hypocalcemia is attributable to partial or complete hypoparathyroidism.
Other Manifestations
Delayed closure of the anterior fontanelle and widely separated metopic sutures were present in 9/11 patients. Three patients had myopia, eight patients had hyper- opia, one had strabismus, and six had microphthalmia. Intelligence was normal in 11/13 patients. In two unrelated patients (Table 11: LR, BS) the intelligence quotient ranged between 65 and 70 points.
Anemia was recorded in 5/10 patients; two patients responded well to treatment with iron. The role of medullary stenosis in the development of anemia in this disease is unknown, but the two are not necessarily related (Table 11); nor is there a specific relationship between hypoparathyroidism and medullary stenosis.
Six patients had retarded bone ages. Cortical thickening at the diaphyses and medullary stenosis of the tubular bones were present in 13 patients. The degree of cortical thickening and the severity and pattern of the medullary stenosis varied between patients. In some patients there was severe medullary stenosis in the upper limbs, and the lower limbs were only mildly involved. In other patients medullary stenosis was present in the lower limbs whereas the upper limbs were apparently normal [Majewski et al, 19811. Roentgenograms of the calvaria also demonstrated variable abnormalities ranging from thickness to thinness of the calvaria with and without diploic spaces and sclerosis [Caffey, 1967; Frech and McAlister, 1968; Majewski et al, 1981; Wilson et al, 19741.
Thus, patients with the Kenny -Caffey syndrome have a variable phenotype; most have proportionate growth retardation usually of postnatal onset, delayed closure of fontanelles, prominent metopic sutures, eye abnormalities, medullary stenosis and cortical thickening of tubular bones of varying severity, and hypocalcemia secondary to hypoparathyroidism. The syndrome has been transmitted from affected mothers to children of both sexes in three families [Kenny and Linarelli, 1966; Majewski et al, 19811, indicating that this is a dominant trait and that the disease is compatible with reasonably long-term survival and normal reproductive capability. The manifestations in males and females are similar favoring autosomal inheritance, although X-linked dominant inheritance cannot be excluded.
REFERENCES
Anast CS, Mohs JM, Kaplan SL, Burns TW (1972): Evidence for parathyroid failure in magnesium deficiency. Science 177:606-608.
Boynton JR, Pheasant TR, Johnson BL, Levin DB, Straton BW (1979): Ocular findings in Kenny’s syndrome. Arch Ophthalmol 97:896-900.
Caffey J (1967): Congenital stenosis of medullary spaces in tubular bones and calvaria in two propor- tionate dwarfs-mother and son; coupled with transitory hypocalcemic tetany. Am J Roentgen01 loo: 1-1 1.
Frech RS, McAlister WH (1968): Medullary stenosis of the tubular bones associated with hypocalcemic convulsions and short stature. Radiology 91:453-461.
Kemp SF, Rosenfeld RG, Lin F, Gaspich SF, Hintz RL (1981): Acute somatomedin response to growth hormone: Radioreceptor assay versus radioimmunoassay. J Clin Endocrinol Metab 52:616-621.
Kenny FM, Linarelli L (1966): Dwarfism and cortical thickening of tubular bones. Am J Dis Child 111:201-207.

782 Leeet a1
Majewski F, Rosendahl W, Ranke M, Nolte K (1981): The Kenny syndrome-A rare type of growth deficiency with tubular stenosis, transient hypoparathyroidism and anomalies of refraction. Eur J Pediatr 136:21-30.
Root AW, Gruskin A, Reber RM, Stopa A, Duckett G (1974): Serum concentrations of parathyroid hormone in infants, children and adolescents. J Pediatr 85:329-336.
Tsang RC (1972): Neonatal magnesium disturbances. Am J Dis Child 124:282-293. Tsang RC, Chen IW, McEnergy IP, Brown DR, Johnson JR and Lesniewicz J (1976): Parathyroid
Wieland P, Fischer JA, Heller R, Fanconi A, Prader A (1981): Severe dwarfism associated with
Wilson MG, Maronde RF, Mikity VG, Shinno NW (1974): Dwarfism and congenital medullary stenosis
function tests with EDTA infusions in infancy and childhood. J Pediatr 88:250-256.
hypocalcemia and unusual parathyroid hormone findings. Pediatr Res 15: 1191A.
(Kenny syndrome). Birth Defects 10: 128-132.