Embed Size (px)
Citation preview
The Irish Training Programme:
A self-sufficient, low cost, high quality system
Professor Richard VellemanEmeritus Professor of Mental Health Research,
University of Bath, UK and Senior Research Consultant, Sangath Community NGO, Goa, India
1

2

3

4

5
Alcoholism: A Comparison of Treatment and Advice,
with a Study of the Influence of Marriage
(Maudsley Monograph) Hardcover – 1 Jan 1978By Jim Orford & Griffith Edwards

6
Wilson, C. and Orford, J. [1978] Children of alcoholics: report of a preliminary study and comments on the literature.
Quarterly Journal of Studies on Alcohol, 39, 121-142.
7
8

50 families of drug misusers Impact Effects Coping Help received Support AttributionsPlus: Parents vs partners
9

10

11
Orford, J., Natera, G., Davies, J., et al (1998a) Stresses and strains for family members living with drinking or drug problems in England and Mexico. Salud
Mental, 21, 1-13.
12
Orford, J., Natera, G., Davies, J., et al (1998b) Tolerate, engage or withdraw: a study of the structure of family coping in England and Mexico. Addiction, 93 (12), 1799-1813.
Orford, J., Natera, G., Davies, J., et al (1998c) Social support in coping with alcohol and drug problems at home: findings from Mexican and English families. Addiction Research, 6(5), 395-420.
Orford, J., Natera, G., Velleman, R., et al (2001) Ways of coping and the health of relatives facing drug and alcohol problems in Mexico and England. Addiction, 96, 761-774.
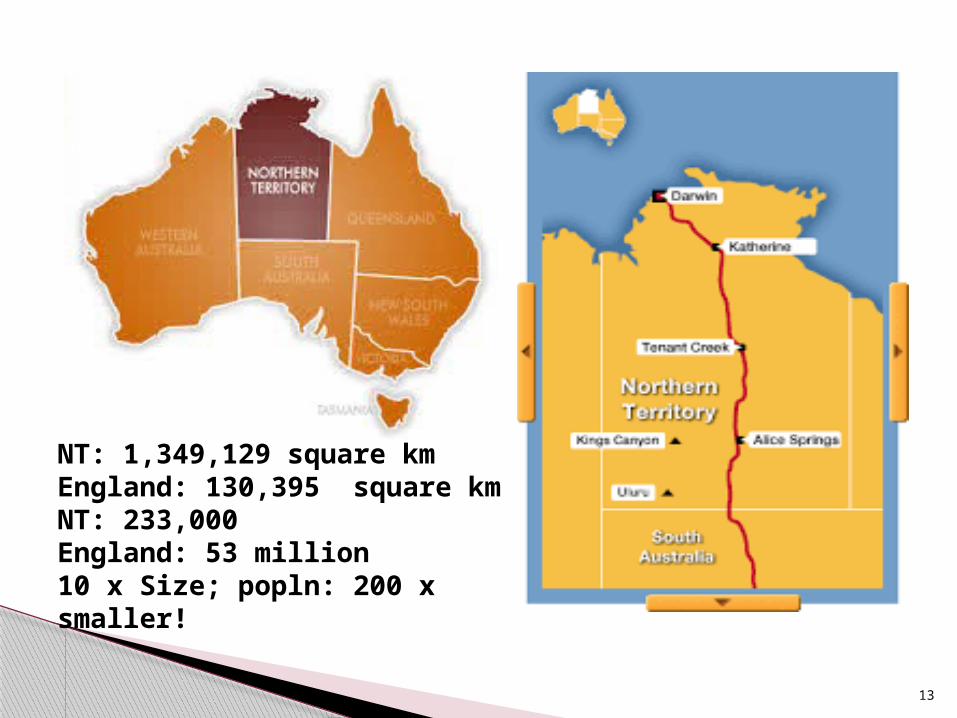
NT: 1,349,129 square km England: 130,395 square kmNT: 233,000 England: 53 million10 x Size; popln: 200 x smaller!
13

14

15

Jim Orford, Guillermina Natera, Alex Copello, Carol Atkinson, Mercela Tiburcio, Richard Velleman, Ian Crundall, Jazmin Mora, Lorna Templeton & Gwen Walley.(2005) Coping with Alcohol and Drug Problems: The Experiences of Family Members inThree Contrasting Cultures. London; Routledge.
16

17

18

19

20

21
22
Four highly contrasting geographical / cultural areas. People say extraordinarily similar about what it is like to live with someone who has an addiction problem, seemingly irrespective of where they come from. Common experiences included:◦ How difficult it is to live with someone (as a spouse, or as a
parent or as a child) when that person misuses substances. ◦ The various impacts that the user has on their lives: the users
changeable moods, or their aggression, or their violence, or their disruption of family or social occasions, or the impact on the family’s finances or of their worries over the users failing health.
◦ How this has affected them as family members, who have to worry and often bear the brunt of any changes in the substance misuser.
◦ How they often become anxious, or depressed, or how the worry seems to lead to effects on their physical health too: their sleep is disturbed, or their eating is disrupted or they develop headaches or gastric problems.
What do family members say- the similarities?
23

◦ how they cope or deal with these difficulties. From a careful examination of what they say about how they cope, it seems that there are 3 main ways that people cope with living with a drug or alcohol or gambling misuser. Some people use mainly one of three ways, others move from one way to another (as it is very difficult for family members to know how best to deal with such a situation).
The 3 ways of coping that people use are:◦ ‘Standing up to’ - Trying to get involved in changing the
relative’s drinking or drug use or gambling;◦ ‘Putting up with’ – tolerating the drinking or drug use or
gambling;◦ ‘Distancing from / Gaining independence’ – Withdrawing,
or trying to distance oneself from the drinking or drug use or gambling.
The amount and type of social support that people receive is really an important influence: that if they get more support (of the right type: i.e. that they find supportive), then it becomes easier to bear the problems resulting from living in this type of environment. AFINet developed a simple model developed directly from the things that family members have said.
24

Developed from what family members told the AFINet group in various research studies:
Families experience stress as a result of someone else’s problem drinking or drug use; this has an impact on them.
The strain of dealing with the substance misuse leads to physical and psychological ill health.
The strain is influenced/mediated by:◦ Method(s) of coping◦ Level and quality of social support
The stress-strain-coping-support (SSCS) model
25

Here it is in a diagram:
Strain: usually
physical and psychological
health problems
How the family member copes with
(responds to) the situation
The level and quality of social support
available to the family member
and
Family members
are stressed
due to the impact of
a relative’s substance
misuse
26
Contrast with other Models
Lots of other models can appear to blame the families, or to pathologise them (eg co-dependency, family therapy).
SSCS model does not: we are interested in empowering / enabling FMs.
A) Family members are at the heart of the response.
And B) SSCS model also considers how harms to individuals and families can be reduced. This led to the development of 5 Step.
27

One Way
No Entry
No Trespassing
No Loitering
28

29
5-Steps

Derives from the SSCS model and what family members have told us.
The 5-Steps are:1. Let the family member tell their story- listen &
reassure.2. Provide relevant information.3. Discuss ways of coping and responding.4. Explore sources of support.5. Arrange further help if needed.
The 5-Step Method
30
Several research studies in the UK and Italy, including one randomised controlled trial.
Research in primary care, and also statutory and non-statutory drug and alcohol services. Has been used within ethnic minority groups.
Mixed method research, involving both questionnaires and interview data.
Data from many hundred family members. One pilot study of the 5-Step Method with
groups. One 12-month follow-up study,
demonstrating further improvements.
How do we know the 5-Step Method helps family
members?
31

For family members: A positive and significant change in coping behaviour. Reduction in symptoms (physical and psychological). Links between coping and health. Lessening of the impact of the problem. Indirect impact on children and others in the family. 5-
Step Method is being piloted in Northern Ireland with children and young people, AND with parental mental health issues as well as substance misuse.
For practitioners: Confidence in working with family members. Awareness of the importance of working with family
members.
Research Evidence
32

o Different to other ways of working with families e.g. it’s empowering, enabling, non-pathologising & focuses on the family member in their own right.
o Is evidence-based, in 2 ways: it is both developed from evidence, and then has evidence that it is effective.
o Provides a structure to guide the work. o Applicable in a range of settings, including NGO/
voluntary, primary health, specialist health, and private.o Flexible in application e.g. number/frequency of
meetings, number of family members, length of sessions.o Modes of delivery, e.g. 1:1, self-help, telephone, groups. o Practitioners may need to consider additional training &
interventions for work with couples, children or families. o The steps should be worked through in order.
Key Principles
33

34

where does this take us on our journey?
35

36

We know a lot now about how family members are affected if a relative develops an addiction –related problem – alcohol, drugs, gambling and so on.
We have developed a way of helping that family members like and appear to help them, and that practitioners like to deliver –
a way of helping that is flexible, and responsive, and above all, aims to empower, to enable FMs to start to feel stronger again, to start to feel that they can feel a sense of greater control over their own lives.
And we have written these results up in both scientific journals and in professional magazines and spoken about them at conferences.
BUT – SO WHAT!
37

International Organisation:AFINet: Addiction & the Family InternationalWebsite: www.Afinetwork.info
74 members from almost 20 countries inclAustralia, NZ, Hong Kong, India, Iran, South Africa, Nigeria, Brazil, Mexico, USA, Canada
38

39

June 2011 Megan O’Leary from the FSN
“The FSN is very interested in looking at the possibility of introducing the 5-Step Method in Ireland. The stress-strain-coping support-model reflects the approach that the FSN takes to drug use and the family and much of the work involved with the 5-Step Method is already undertaken within the family support groups. The use of the method would formalise this approach and ensure consistency across the country.”
40

41

Step 1: Train practitioners in the 5-Step Method; they practice it until they are ready to submit audio-recordings of sessions covering all 5 Steps; these are assessed against criteria for delivery of the Method; once they meet the required level, they are Accredited as 5-Step Method Practitioners.
The three broad steps are:
42
Step 2: Train these Accredited 5-Step Practitioners to deliver training to other practitioners in the 5-Step Method; they practice it; when ready DVD recordings of all components of a 2-day training course training practitioners in the 5-Step method are assessed against further criteria (related to training instead of 5-Step practice); once they meet the required level, Accredited as a 5-Step Method Trainer.
43

Step 3: Train Accredited Practitioners to become Accredited Assessors ie listen to audio-tapes of 5-Step Method sessions, rate practitioners, and decide to Accredit (or not) these practitioners. We train people to become Accredited Assessors by getting them to rate tapes that we have already rated. They continue to do this until they can reliably obtain the same ratings as we give. Once they can, they become Accredited 5-Step Method Assessors.
44

Once a place has Accredited Trainers and Accredited Assessors, that place is self-sufficient, and we (AFINet-UK – formerly known as the UK ADF Group) only need to have periodic visits to
a) offer 'master-classes', b) answer questions; and c) do any quality assurance assessments as seem appropriate/ needed.
45

46

Allow family member to describe situation and tell their story .
Identify relevant stresses and how the FM has been affected
Identify relevant stresses and how others have been affected
Normalise the experience of FMs giving the FM an indication that they are not alone with their experiences
Cover appropriately the Beginning and Ending of the session (introduction and purpose of 5 step, confidentiality; summarised main FM issues, use of handbook, next steps, practical issues of contact and date of next session).
Step 1 – Assessment Criteria. Listen, reassure and explore concerns
Eliciting the story. (pages 18 – 24 Professional’s HandBook)
47

Room set up effectively and sessions well planned. Participants know what to expect and training has a logical well timed format.
Factual information is effectively presented. Variety of presentation methods used to maintain
group focus; Training plan adhered to. Exercises adequately explained /facilitated and
feedback given to participants to review and improve their skills.
Presenter’s behaviour models 5 step and general counselling skills. Presenters work well together.
Exercises are effective at training participants to use 5 step competently and to be assessed.
Summary of the criteria related to 5-Step Method Training
48

Ireland has Accredited 5-Step Method Practitioners,
and Accredited 5-Step Method Trainers and Accredited 5-Step Method Assessors.
Ireland is self-sufficient in maintaining the 5-Step Method
And we (AFINet-UK, the old UK ADF Group) only are needed to have periodic visits to help ensure that all is going smoothly.
Where are we now?
49

50

At first it was to better understand what affected family members were going through.
Then it was to develop a way of helping them, so that they could feel more empowered and in control of what felt like an uncontrollable situation.
Then is was to give these ideas away – to empower not only affected family members, but practitioners, and organisations, so that they, too, need not be dependent on us – the ‘experts’ – to skill them up to help these affected family members.
51

52

53

54

To develop a self-sufficient, low cost, high quality system for the continued replication of the 5-Step Method; To have ‘given the 5-Step Method away’, whilst still ensuring that what people were delivering WAS a good quality version of the 5-Step Method.
55