Embed Size (px)
Citation preview

The Internotional Journal of Periodontics & Restorative Dentistry

333
Surgical Crown-LengtheningProcedure to Entiance Esttietics
Gad C. Bensimon. DDS'
This arfide prGS&nts ttie rotionaie for fhe use of a preproslhetic surgicalcrown-lengttiening procedure, porticulariy in the anterior region whereestheiics is of great concern. Clinical cases illusfrate fhe procedure anddemor^strate how if can be used to provide enough sound tooth structurefo restore teeth wifhauf impingement on the biologic width, at fhe samefime reducing a "gingival smiie"and creating new popillae.Ont J Periodontics Restorative Dent 1999:19:333-341.)
'Postgraduate Student, Deportment of Periodontics. ColumbiaUniversity, New York: and Private Practice Limited to Periodontics,Slrosbourg, France.
Reprint requests: Or G, C Bensimon, 3 Ailée de la Robertsau, Ó7000
Strasbourg, France.
Restoration of fractured, severeiydecayed, partiaiiy erupted (de-iayed passive eruption), worn, orpooriy restored teeth is a com-mon problem faced by the gen-eral dentist. The preservation ofthe bioiogic width is often diffl-cuit, in the maxillary anteriorteeth, deoiing with the estheticsof a "gingival smile" probiem orioss of papiliae is a chaiienge toail therapists. The ciinical cosespresented in this article will iiius-trate ttie crown-iengthening pro-cedure, a surgicai techniquethat heips resolve these prob-iems. The rationaie and themethod for reoreating papiiiaewiii be iiiustrated.
The most common surgicalmodoiity used to increase theclinicai crown length is the api-oally positioned flap in conjunc-tion with resective osseous sur-gery. This technique wiil increosethe clinical crown length andmaintain the existing attachedgingiva, and the dentoglngivalcomplex will be re-formed, Re-sective osseous surgery designedto expose adequate clinical
Volume 19, Number 4.1999

334
crown iengfh provides for fheproper placemenf of margins,enhanoes fhe refenfion,' andcreates a periodontal environ-ment in which piaque controiprocedures can be more effec-tively performed,^
Rosenberg and Garber^have outiined the facfors thotshould be taken into accountprior to tooth-iengthening proce-dures. The restorative factors fhatshould be considered ore: (1)esfhetics, C'2)form. ("clj function, (4)refenfion, and (5) marginal seol.The iimif ing factors thaf should beconsidered are: f/J crown-fo-rootrafio. (2) mainfainabilify, (3) esthef-ics, (4) locafion of furcafions, (5)predicfobiiity, (0^ footh-arch relo-fionship, and (7) comparison otodjacenf periodontium.
Anatomic factors
Biologic width
Gargiuio ef ai'̂ described thedimensions and reiafions of fhedentogingivol junction in humons:fhe biologic widfh is fhe zone offhe root surface coronal fo fhealveolar crest fo which fhe junc-tionai epifhelium and connecfivetissue ore attached: it overages2,04 mm,This dimension may varyfrom toofh to footh, buf if is pre-senf in all heaithy denfifions.^
The resforatian of a foothwithout regord to the biologicwidth may result in a poor peri-adontoi response. The margin otthe restoration may become an
iotrogenic facfor and initiate gin-gival infiammafion ond bonerésorption. The finish line of fheresforative margin shouid nofimpinge on the supracrestal con-necfive fissue and fhe juncfionolepifheiium,''''
Surgical crown iengfheningwiii provide enough sound toofhsfruofure to restore fhe foofhwithout impingement on the bio-logic width, A minimum of 3 mmcoronai to the alveoiar cresf isnecessory^: 1 mm for fhe re-formation of the connecfive fis-sue aftachment. i mm fo receivethe junctionai epithelium, and 1mm for the re-formaflon of a gin-givai sulcus in which fhe marginof the resforafion will be piaoed.
The orown-lengfhening pro-cedure aims af the reestablish-menf of a healfhy periodontiumaf a mere apicol level, as theosseous resecf ive surgery is com-bined with on apical shift of thegingival margin. The establish-ment of a good reiationship be-tween fhe margins of the resforo-tion, the bone, and fhe soff fissueshouid produce a clinical condi-tion fhat can be more easilymainfained by the patient andthedentolteom.
Osseous arohifeofure
Reshaping the alveolar crest andreesfoblishing a normal fiberarrangemenf is a prerequislfe fora complefe. funcfional recuper-afion of fhe periodonfium,^ In fhecase of fhe crown-lengthening
The infernationol Journoi of Periodontics a Restorotive Dentistry

335
technique, osseous surgery isneeded to recreate and main-tain a physiologic gingival archi-tecture, described by Prichard^°OS 'one in which the interdentalarea is conical and coronallypositioned to the buccal and iin-gua! (or palotal) plotes of bone,which have a paroboiic shapeand flow smoothly from the inter-dental area; an interdental areathat follows the shape ot thecementoenameljunction."Thesefactors wiil allow a ttiin, scalloped,knife-edged gingival contourwith pyromid-shaped papillaetfiatfill the interproximol space.
Osseous resective proce-dures used in periodontal ther-apy have been shown to be effi-cient in stabilizing periodontaidestruction.1' When osseousresective procedures dre used incombinotion with an apioaliypositioned flap for pocket reduc-tion or elimination, much ot thepocket regrovi/th has been attrib-uted, as stated by Ochsenbein,'^to ttie "dynamic behavior of ttiegingiva that prefers to live at ornear the cemento-enamel junc-tion and that always seems deter-mined to return to ¡ts originai pre-operative architectural form."
To what, then, can the goodlong-term results of crown-lengthening procedures beattributed?
Ochsenbein's statement hasbeen supported by Mothersonand Zander,^^'^ who performedinterdental osteoplasty and os-seous resection on monkeys.Theirresults showed that the surgically
creafed pattern was maintainedas healing occurred. The soft tis-sue overlying the radicular boneto I lowed the bony profile.Regording the interdental area,the surgically creoted osseouscontour was maintained whenosseous resection wos performed.The interdentai soft tissue mor-phology was influenced by theamount of space between thecontact area and the alveolorprocess.
Thus, the other factor that willinfluence the gingival morphol-ogy, especially the interdentalpapillae, is the shape and size ofthe interdental space and thecementoenamei junction (CEJ).In cases of crown-lengtheningprocedures, the surgical treat-ment is usually followed by a pros-thetic treatment that creates anew environment witti new crov/nmorphology ond new contactpoints.Tbis can explain the stabil-ity otttie surgical results.
Tissue management
Management of the vestibularHap
Crown lengthening daes notinvolve Itie use ot a simple full-thickness (mucoperiosteal)inverse beveled flap to gainaccess to the bone, but rather apartiai-futi thickness flap that canbe extended to a partial-tull-par-tial thickness positioned flap,^^Once an adequate amount otbone has been exposed, sharp
Volume i 9, Number 4,1999

33Ó
dissection is agoin employed toallow for better Hop positioning.
The fiop is scaiioped. A newmarginal fissue is formed by thisinitiai incision, ond the newiy cre-ated papillae are thinned to athickness of approximateiy 1,5mm. This thinning eiiminates thickgingivol morgins and iarge trian-gulor pieces of interdentai tissue.A thick tissue would be difficuit totrim properiy once the fiap hasbeen raised ond freed.
Proper piaoement ot the ini-tiol incision is oriticai and dependson the amount of available kera-tinized gingiva. The initiol incisionpiacement has been clossitiedoccording to the omount of ker-otinized tissue present":
• Class i: keratinized gingiva ismore than odequate. Buccaiincision Is ploced 1 to 3 mmfrom the crest of gingiva andfiop is positioned opioally,
• Ciass li: kerotinized gingiva isadequote. Crestai incisionand flap apicaiiy positionedto the crest of bone.
• Ciass Hi: keratinized gingiva isinodequote. Sulculor incisionand tlap apicaiiy positioned 1to 2 mm below crest of bonefo increose the zone of kero-tinized gingiva.
When making the initiai inci-sion, the clinician should antici-póte the final underlying osseouscontour.The common mistake ofremoving most if not ali of theexisting keratinized gingiva shouldbe avoided. Concerning the
anterior region more thon onyother orea, an incision thot willleove bone exposed shouid beavoided. If necessory, intemaiiybeveied verticai releasing inci-sions may be pioced at the lineongle ot the adjocent tooth toimprove visibiiity and access.Thefiap is then elevated to the ieveiof the muoogingivoi junctionusing o periosteal eievator.
Management of the palatalflap
The partial-thickness palatal flapis used.'^ Since the paiatal fiopoannot be positioned apicaiiy itis impartant to evoiuote thetopogrophy of the underiyingbone ond to determine the thick-ness of the polatal tissues beforeany incisions are made; this isaccompiished by periodontolprobing and sounding after localanesthesia. The sounding wiiiallow the surgeon to differentiotebetween dense fibrotic tissue andeniarged tissue caused by os-seous irreguiarities.The tissue thick-ness and the amount of bonethat has fo be removed to ex-pose enough root surface are thedetermining factars for incisionpiacement, A more exaggeratedincision is needed it extensiveosseous resection is necessary.The most common mistake is tocreóte o fiop that is either tooiong or too short.
Using a # 15 blade an inter-naiiy beveled incision is made tothe oiveolar bone. Again, the
surgeon must anticipate thefuture contigurotion of the cre-stai bone. After a shorp dissec-tion porallel to the bone, asplit-fuli thickness flap is ele-voted. The connective tissuefibers still attoched to the rootsurfaces ore severed and thecollar of interdental and supro-gingival tissue is removed.The so-caiied secandary polotai fiap isremoved as well.
With the 2 flaps raised, scaiing,root pianing, ond degranulationare completed. It is important toobtain a olean surgical fieldbefore storting the osseous resec-tion since the exoct bony config-uration or smail bony defects canbe hidden by residual fibers orbleeding.
Management of the bone:Osseous resection
To achieve a gingival contourtightiy adopted to the alveolorbone ond opicai to the presurgi-cai locatian, the osseous phose ofthe surgicai crown-lengtheningprocedure uses the techniquesof osteopidsty and astectomy^'
To determine the amount ofaiveolor bone that hos to be re-moved, several factors must beconsidered; the height of the od-jacent teeth (to avoid compro-mising their periodontium by cre-otlng a precipitous change in theosseous morphology), the amountof roof thaf has to be denuded,ond the crown-to-root ratio asmeosured radiographicoiiy.
The Internationai Journal of Periodontics & Restorotive Dentistry

337
The crown-lengthening pro-cedure In an anterior segment Jsone of the cases in which theosseous surgical phase can beperformed "ideolly" and shouldresult in o positive osseous archi-tecture with the interproximolbone coronal tc the buccal ondpalatal radicular bone at a moreapical level,
A small # 2 or 4 round bur in ahigh-speed hondpiece is used tooutline the bone at the ccrrectlevel, with nc contact with theteeth.This first step facilitates thebone removal facially and lin-gually using hand chisels.This willrecreate the parabolic osseousform capable of supparting asimilar gingival architecture,
Osteoplasty is used to elimi-nate ony exostoses or thick bonymargins and to achieve properosseous term. It includes thetechniques of vertical groovingand radicular blending, as inresective osseous surgery forpocket elimination. Verticalgrooving, using a water-cooled #8 bur in a high-speed hand-piece, wili reduce the buccoiin-gual thickness of the interdentalbone. Radicular blending usingthe same bur will recreate anevenly tîawing osseous form.
Using Ochsenbein chisels, tfiefinal osseous recontouring wilf beperformed at the line angles ofttie teeth to remove any residualbony spicules. It is important tacheck whether the minimum of 3mm of root surface coronal tathe alveolar cresf has been ob-toined for each taoth.
Sutures
At ttiis stage ttie area is rinsed andthe daps are allowed to tall backagainst the bcne.The buccal flapis repositioned cr positioned api-ccily if necessary, in any case, thegingival margin should rest pas-sively at the crest of the bone wittithe new papiliae positioned inter-proximally permitting primary clo-sure. A new dissection of the flapbeyond the mucogingival junc-tion may be necessary
The provisionoi prosthesis isreplaced to evaluate the degreeof crown lengthening achieved,Pressure is then applied withmoistened sterile gauze for a fewminutes to check the adaptationof the flaps, which are suturedinto position with a continuoussling suturing technique,The buc-cai fiap is positioned apicaliythrough the use cf pericsteai ver-tical or horizontai mattress sutures,and the paiatal flap is positionedthrough ttie use of horizontai oroblique mattTess sutures. Pressureis again applied, this time to pre-vent any hematoma formationthat could result ¡n partial necro-sis of the fiap. Temporary re-cementation of the provisionalprosthesis is followed by theplacement of a periodontaldressing.
Postoperative care
An ice pack should be appliedpostoperatively Anaigesics areprescribed. The potient is
instructed to rinse with chlorhex-idine during the first postopera-tive week and after the removalof the dressing for a period of 3weeks. Antibiotics can be pre-scribed, especiaily when exten-sive osseous surgery has beenperformed. At 1 week after thesurgery the dressing and suturesare removed. New oral hygieneinstructions are given.
The provisional prothesis isreiined after a healing period of 3to 4 weei<s. At this time the pros-thetic margins are relocated api-caiiy and siightly supragingivally.^Refinement of the tooth prepa-rotion should be pertormed 4weeks later (8 to 10 weei<s afterthe surgicai procedure): this wiliprovide for the prcper placementct the margin of the restoration inreiaticn tc the new gingival sui-cus. Depending on the estheticneeds, the margin can be placedat the gingival crest or 0.5 mminto the healthy gingival suicus. Itdoes not have to be placed atthe same level all around thetooth; a combination of supragin-gival, crestal, and intracrevicularmargins can be piaced aroundthe same tooth.2'
Volume 19, Number 4.1999
338
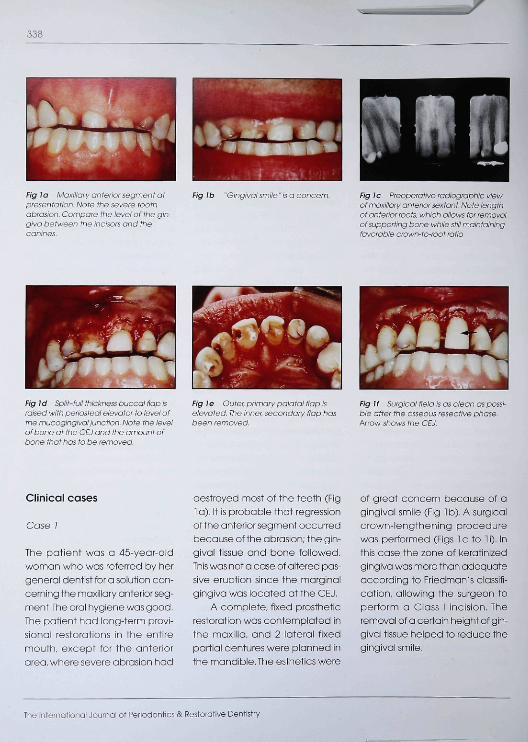
mvss»Fig ¡o Maxillary anterior segment atpresentation. Note the severe toothabrasion. Compare the level of the gin-giva between the incisors and thecanines.
Fig Ib "Gingival smile ' is a concern. Fig ¡c Preoperative radiographie viewof maxiiiary anferior sextant Note lengthaf anterior rcofs. which allows for removalaf supporting bone white still maintainingfavorable crown-to-root ratio.
Fig Id Split-full !li:ci<r>(í7,5 Ijuccal nap israised with penasteai eievator to level ofthe mucogingival junction. Ncte fhe levelof bone at the CE J and the amount ofbone that has to be removed.
Fig fe Outer, primary palatal fiopiselevated. The inner, secondary flap hasbeen removed.
Fig If Surgical field is as clean as possi-ble after fhe asseous resecfive phase.Arrow shows the CEJ.
Clinical cases
Case /
The patient wos a 45-year-oidwoman who was referred by hergênerai dentist for a solution con-cerning the maxillary anterior seg-ment.The orai hygiene was good.The patient had long-term provi-sional restorations in the entiremouth, except for the anteriorarea, where severe abrasion had
destroyed most of the teeth (Fig1 a), it is probable that regressionof the anterior segment occurredbecause of the abrasion; the gin-givai tissue and bone foiiowed.This was not a case of aitered pas-sive eruption since the marginalgingivo was iocated otthe CEJ,
A complete, fixed prostheticrestoration was oontempiated inthe moxlila, and 2 laterai fixedpartial dentures were planned inthe mandibie,The esthetics were
of great concern because of agingivai smiie (Fig 1 b). A surgicalcrown-iengthening procedurewas performed (Figs 1 c to 1 i). Inthis cose the zone of keratinizedgingiva was more than adequateaccarding to Friedmon's oiassifi-cation, aiiowing the surgeon toperform a Ciass I incision. Theremoval of a certain height of gin-givoi tissue helped to reduce thegingivoi smiie.
The international Journal of Periodontics & Restorative Dentistry

339
Fig Jg At 2 weete ofrer removoi ofdressing tiealing is very good. Note ftiepreser)oe of the newly formed papiiiae.
Fig lh Final prosthesis in place. Notethe position of the potient's lips in rela-tion to the size and form of the teeth.
Fig a F¡naiprosthesis i yearattersurgery.
Case 2
The potient, a 52-year-old woman,was referred by her gênerai den-tist affer he had carried out fhe ini-fiai preparofion phase. A com-piefe. fixed prosthetic restorafionwas confemplafed in the maxilla,and 2 lateral fixed partial dentureswere planned in the mandible.The patient had long-term provi-sional restorations (Fig 2a) andshowed good oral hygiene.
On fhe anterior maxillaryfeefh. the referring denfisf wasconcerned abouf fhe loss ofpapillae. He was not safisfed wifhthe gingival morphology; fhe
thick gingival contour and thetotal absence of papillae—insfead, there were interproximaigingival craters formed by buccaiand palatal "wolls"—did nofseem fo be conducive fo peri-odonfal health or orol hygieneprocedures. Pockets overoging 4mm could be probed interproxi-mally. The gingiva presented a"negative arohif ecfure," compo-rable fo fhe negafive osseousarchifecfure thaf is usually foundduring periodontol surgery Foodimpoction occurred very often,Esfhefics were also of greaf con-cern for 2 reasons: the smileshowed foo much gingiva and
there were large interdentalspaces wifh no papillae,
A surgicol crov/n-lengfheningwas ftierefore performed (Figs 2bfo 2d), The prosfhetic freafmentcreafed a new environmentcontact points, and crown mor-phology that influenced fhe gin-gival archifecfure. especially theinferdenfal papillae. Af 12 weeksposfsurgery the final restorafivephase began. The resforafionmargins could be placed prop-erly in reiafion fo the new gingivalsulous (Figs 2e and 2f),
These 2 cases demonsfrafethat fhe surgical crown-lengfti-ening procedure can be used
Volume 19, Number 4,1999

340
Fig 2a Maxiliary anterior segment wifh provisianal prosthesis atpresentation. Note tafol absence of papillae^ marginal gingivaappears as a straight horizontal line. Gingival craters are pre-sent in eactt interdental area, Ttie zane of i<erafinized gingiva ismore ttian adeauate aaaarding ta Friedman's dassification.
Fig 2b Initial buccal inai^an is scalloped and inverseiybeveled, w/ffi no vertical incisians ta thin the new papillae,
Fig 2c Osseaus surgery has been completed with a high-speed, water-cooied round bur to outline the bone at the cor-rect level. This facilitates removal of bone with hand ahiseis.
Fig2d AI I month after the surgery the healing is very good.Note the presence of the newiy formed papillae and theamount of lengthening obtainod.
successfully to allow, facilitdte, orenhance a prosthetic treatment.This procedure provides rapid, sta-ple results and should be includ-ed in treatment planning moreoften. Omitting a crown-length-ening procedure when it is nec-essary will leod to inflammation.
gingivai recession or eniarge-ment, bone résorption, visiblemargins, and unesthetic results;using the procedure wiil add onlyone step to the treotment, andwill be of great benefit to thepatient and the dental team.
Acknowledgments
The author wishes to thank his teaohers atColumbia University and at StrasbourgUniversity. A specioi thani( you goes tomy late friend Dr B. Mosi<ow. Specialthanks also to Dr Alain Azuelos for theprosthetic management of case 1 andto Dr René Serfaty for the prosthetic man-ogement of case 2.
The Internotionai Journal of Periodontios & Restorative Dentistry

341
F^ 2e New provisional prosti^esis is fabricated 4 weeks aftersurgery It IS adapted to the new gingivai environment, prosthet-ic riKiigira are relocated opicaliy and slightly supragingivaity.
Fig2t Completed case at a maintenance visit 1 year later.
References
1. Willey RL. Retention in the preporationof teeth for cost restorotian.JProsthetDent 1976,35:526.
2. BurchJ.Tenrulestbrdevelopingcrowncontours in restorations. Dent CiinNorth Am 197l; l5:6l l-6!8.
3. Rosenberg MM, Gorber DA. To of tilengthening procedures. CompendCantin Educ Dent 198O;1:161-172.
4. Gargiula AW, Wentz FM, Orbon B.Dimensions of ttie dentogingival junc-tioh in humans. J Periodontol 1961:32:2Ó1.
5. MaynardJGJr.WiisonRD Physioiogicaldimensions of the periodontium signif-icant to the restorative dentist JPeriodontol 1979:50:170-174.
6. keough BE, ef ol. Periodontol prostfie-sis: Prosthetic rrxinogement for patients\witti advanced periodontal disease.In: Olark JW (ed). Clinical Dentistry.Philadelphia: JB üppincott, 1981.
7. Nevins M. Skurow HM.The introcrevic-ular restorative margin, the biologicwidth, and the maintenance of thegingivol margin. Int J PeriodonticsRestorative Dent 198<1.4(3).31-49.
8. Nev/comb G. The relationship be-tween the location of subgingivolcrown morgins and gingival inflam-mation.J Peiodontol 1974:45:151-154.
9. Carranza R Carranza F Jr. Periodontaidisease iocal therapy. Inf Dent J1957:7:209.
10 PriohardJ.Gingivoplastygingivecto-my ond osseous surgery. J Periodontoi1961:32:275.
11 Kramer GM.The case for osteotomy—A time-tested theropeutic modolrty inseiected periodontitis sites, int JPeriodontics Restorative Dent 1995:15:229-237.
12. Ochsenbein C. Current status otosseous surgery. JPeriodonioi 1977:48'577-586.
13. MathersonD.ZanderH.Aneuaiuationof osseous surgery in monkeysiabstroot 325). intemational Asso-ciation for Dentai Research, 1903:117.
14 Zander H.MathersonD.The effect ofosseous surgery on interdentai tissuemorphology in monkeys (abstract326J. International Association forDental Research. 1963:117.
15. MdtfiersonDG.Anevoiuationofheoi-ing toilowing osseous periodonfolsurgery in monkeys. Int J PeriodonticsRestorotive Dent 1988:8(5).9-39.
16 GoidmanHM.ShumanA.isenPergG.An Atlos of the Surgical Managementof Periodontoi Diseose. Cnicago:Quintessence. 1982.
17. Friedman N, Levine HL. Muoogingivalsurgery: Current stotus. J Periodontoi1964,35:5.
18. Stamieno H Jr Paiotai tlap surgery:Mucosol ttap (split thickness) and itsadvantages over the muooperiostealflap. J Periodontoi. 1969:40547-552.
19. Friedman N. Periodontol osseoussurgery: Osfeaplosty and osteoecto-my.J Periodonto! 1955:26:257.
20. De Waai H, Casfeiiucci G.The impor-tance af restorative margin place-ment to the biaiagic widtti and peri-odontal health. Part II.Int jPeriodontiosRestorative Dent 199d: 14:71-83.
21. DeWaalH, CastellucciG.TIieimpor-tonce of restorative margin place-ment to the biologic widtti and peri-odontal health. Part I. Int J PeriodpnticsRestorative Dent 1993:13:461-471.
Volume 19, Number 4,1999





























