Embed Size (px)
Citation preview

The Journal of Continuing Education in the Health Professions, Volume 14, pp. 83-89 . Printed in the U.S.A. Copyright 0 1994 The Alliance for Continuing Medical Education and the Society of Medical College Directors of Continuing Medical Education. All rights reserved.
Original Article
The Interactive Videoconference: An Effective CME Delivery System
CAROL L. HAMPTON, M.M.S. Director of Instructional Development Office of Medical Education
PAUL E. MAZMANIAN, PH.D. Assistant Dean of Medical Education Office of Medical Education
THOMAS J. SMITH, M.D. Assistant Professor of Medicine and Health Administration Massey Cancer Center
Medical College of Virginia Virginia Commonwealth University Richmond, VA
Abstract: Today satellite television is readily available to many hos- pitals, where it can prove an eflicient means of delivering continuing medical education (CME)-particularly in rural areas.
Since there is little research in CME on the effectiveness of video- conferencing, this paper was written to describe a case study focus- ing on that issue. An interactive videoconference on breast cancer was presented to health care professionals in their community hos- pital settings. Results of a test given before and after the broadcast indicated a 21 percent increase in knowledge among participants. Key Words: videoconferencing, interactive television, continuing medical education (CME), continuing nursing education (CNE), change, breast cancer
The State of Current Research Videoconferencing effectively links people at different sites through audio and visual communication. Yet today few medical-school-based CME providers produce television conferences of any type, and those that do gen- erally produce only a small number of programs.lt2
This may explain, in part, why there is a dearth of reported studies on videoconferencing as an effective delivery system for continuing medical ed- ucation. McLaughlin and Donaldson3 reviewed CME literature from 1984 to
83

Humpton et ul
1988-selecting studies that included an evaluation component-but did not report any studies that evaluated videoconferencing. Davis, et a14 reviewed the literature from 1975 to 1991 but reported no studies which included videoconferencing as an effective intervention in CME.
What literature does exist on videoconferencing focuses more on the me- chanics of delivery than the effectiveness of technique.5-11 Furthermore, while several studies do report knowledge gain after a videoconference, the target population is undergraduate or graduate medical or nursing students rather than practitioners.12.13
Yet many experts stress the need for a change in educational methods. Manning14 says telecommunications technology should be used to make knowledge more accessible to health professionals and to link continuing ed- ucation information more directly to individual practices. Leist and Kristofcols suggest that CME delivery systems and programs should be in- creasingly responsive, more timely, and geographically closer to participants.
Study Description This study was developed and produced by the Virginia Hospital Television Network of the Office of Medical Education at the Medical College of Virginia (MCV)/Virginia Commonwealth University. Produced in collabo- ration with the MCV Massey Cancer Center, it was supported in part by an educational grant from Health and Sciences Network. The program was ap- proved for appropriate continuing education credit for physicians, family practitioners, pharmacists and other health care professionals.
“Management of Early Stage Breast Cancer: Asymptomatic Mass” was chosen as the subject of the videoconference because breast cancer is a com- mon lethal disease.I6 The National Institutes of Health (NIH) has formulated clear management guidelines for the treatment of breast cancer which it re- leased in 1988 and again in 1990. Another reason for the selection of this topic is that there is a wide variation in the care given to breast cancer pa- tients, and some of the treatment is at odds with the published guide- lines. 1731 8
Since NIH guidelines contain information related to various levels of cancer care and since that care is often provided by a team in a community hospital setting, the targeted audience was multidisciplinary: physicians, nurses, and other health care professionals. The reported audience included 277 practitioners at 99 sites; in addition, 50 sites indicated they had video- taped the program for later use. The videoconference was also televised by the Health and Sciences Network to its approximately 750 subscriber hos- pitals.
84

The Interactive Videoconference
The project components were a live videoconference broadcast, printed instructional materials, and a pre- and post-test of participants’ knowledge. The broadcast was a full-motion color video originating from a TV studio, transmitted up to a satellite, and then beamed down to multiple sites. Its one- hour format included 35 minutes of preproduced video presentations by health care professionals, patient interviews, and closeup views of radio- graphic images, tumor specimens, and the mammographic screening pro- cess. The remaining 25 minutes were allotted to interactive discussion, during which remote-site participants could phone in questions and receive answers on television from the MCV faculty members in the studio.
The program moderator was a faculty member from MCV’s Department of Family Practice who was familiar with the instructional objectives and skilled in clarifying questions from the primary care perspective. He had re- hearsed in order to become comfortable with the television medium and his role as moderator.
The designated teleconference coordinator at each participating hospital received a package of printed instructional materials two weeks prior to the broadcast. This included two tests of six identical questions reflecting es- sential elements in the NIH guidelines. The post-test contained one more question than the pre-test; it asked participants if they planned to make any changes in their practice as a result of what they had learned in the video- conference.
The cooperation of local site coordinators was an essential component of this program. Coordinators were expected to promote the videoconference, schedule the meeting room, copy handouts, collect attendance data, admin- ister the tests and complete the evaluation. The research findings of Chute, et al.19 and Moore, et al.11 support the importance of the coordinator’s role.
Study Results Sixty-nine useable sets of completed pre- and post-tests were sent back from 21 sites, representing a 25 percent return rate. Nurses returned 30 tests, physicians returned 22, and other health care professionals returned 17 tests.
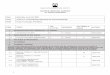
The post-test, taken immediately after participation in the videoconfer- ence, demonstrated a 21 percent increase in knowledge over the pre-test, taken before the conference began. Table 1 summarizes the pre-test/post-test data. Each group of participants showed an increase in correct answers on each of the six questions, except for the other health professionals group which scored the same on one question and lower on another question. Overall, the physicians scored highest on the pre-test. The nurses demon- strated the most gain from pre-test to post-test, while the other health pro-
85

Hampton et a1
n = 69
22 MDs
30 Nurses
17 Other Health Profs.
TOTALS
Table 1 Videoconference: Pre-test/Post-test Data Summary
Pre-test Post-test # Questions # Correct % # Correct % Increase %
Possible Answers Correct Answers Correct in # of Increase Correct Answers
132 63 47% 85 64% 23 17%
180 53 29% 102 57% 49 28%
102 36 35% 51 50% 15 15%
414 151 36% 238 57% 87 21%
The pre-test and post-test each contained six identical questions. Each group of participants showed an increase in correct answers in each of the six questions, except for the other health pro- fessionals group which scored the same on one question and lower on one question.
fessionals showed a mixed response, scoring an increase in correct answers on some questions but not on others.
Thirty-three participants-10 physicians, 12 nurses, and 11 other health care professionals-indicated they would make changes in their practice as a result of the videoconference. The physicians said they would pay more at- tention to ink marking of the pathology specimen, dye for tumor localization on the mammogram, and team management for treatment. Nurses indicated they would promote mammograms, encourage more frequent self breast ex- aminations, and provide the patient more information about treatment.
Discussion Data from this small study suggest that change in testable knowledge can oc- cur among health care practitioners at community hospitals as a result of videoconferencing. While the authors feel the study was successful in demonstrating this point, it did raise related questions which are worthy of further investigation.
For instance, in addition to effectiveness, this CME format probably has an economic advantage as well. Although this study did not document fi- nancial benefits, it seems likely that videoconferencing is a more cost-ef- fective way of delivering continuing medical education than physically moving people.20 Therefore videoconference production and transmission
86

The Interactive Videoconference
costs should be balanced against the lost productive time and travel costs in- curred when a number of participants must leave their community hospitals in order to reach a distant CME location. Existing literature has reported cost benefit effectiveness in distance learning projects,20 but it has focused on corporate rather than medical training.
In this Virginia study, participants from states as distant as Texas and Nebraska were provided an educational opportunity they might otherwise not have had. This suggests that current medical information delivered by videoconferencing may prove valuable to practitioners in geographically iso- lated areas.
Although this study did not document change within the workplace af- ter the videoconference, that subject is also worthy of future investigation. When one person leaves the hospital to attend a CME conference, the group remaining does not participate in the learning activity. Therefore, involving members of several professions in the same learning activity on site, within their common work setting, may help them to make positive change.21.22
Practical Recommendations The following recommendations are gleaned from this study, the literature, and the authors’ collective experience. As videoconferencing and the ready availability of new communication technology continue to grow, these sug- gestions to faculty and planners should make CME both more accessible and more effective in the future.
1. Identify objectives and write test questions simultaneously. This saves time and helps to assure that the program focuses on the most essential information. 2. Design program and support materials so they are easy for the site coordinator to use and understand. This is particularly important when research is involved. 3. Maximize visual opportunities. Television may be an excellent medium for medical education since, as Dwyer documents? it pro- vides multiple opportunities to increase learning through visualization. 4. Creatively apply instructional technology to deliver CME. This is especially important for program planners as information technology systems are e ~ p a n d e d ~ ~ 7 ~ 5 and become more readily accessible in hospitals, physicians’ offices, schools, and homes.
87

Hampton et a1
References 1. Mazmanian, PE, Hamson, RV, Osborne, CE. Diversity across medical schools; pro-
grams. enrollment , and fees for continuing medical education. J Cont Educ Health Prof 1990; 10: 23-33.
2. Survey for 1990-91 : descriptive results. Survey Subcommittee of the Society of Medical College Directors of Continuing Medical Education (RV Hamson, Chairman), April, 1992.
grams: a selected literature, 1984-88. J Cont Educ Health Prof 1991; 11:65-84.
of CME: A review of 50 randomized controlled trials. JAMA 1992; 268:9: 11 11-1 117.
primer, 2nd edition. New York: Praeger, 1992.
gram in a hospital library. Bull Med Libr Assoc 1987; 75:2:128-132.
Cont Educ Nurs 1985; 16:2:47-52.
Biocommun 1992; 19:4:26-30.
ment of participant responses. J Biocommun 1984; 11:3:5 - 8.
education preferences of physicians and nurses in rural areas. Modius 1986; 7:3:53- 58.
11. Moore, DM. Burton, JK, Dodl, NR. The role of facilitators in Virginia’s electronic classroom project. Am J Distance Educ 1991; 6:3:29-39.
12. Dohner, CW, Zinser, E, Cullen, T, Schwarz, MR. Teaching basic science and clinical medicine at a distance: an evaluation of satellite communication. Distance Education
13. Fry, CF, Baer. C, Cornett, S. Interactive television in nursing continuing education. J
14. Manning, PR. Continuing education needs of health care professionals. Bull Med
15. Leist, JC, Kristofco, RE. The changing paradigm for continuing medical education:
3. McLaughlin, MS, Donaldson, JF. Evaluation of continuing medical education pro-
4. Davis, DA, Thomson, MA. Oxman, AD, Haynes, RB. Evidence for the effectiveness
5. Piemme, TE. In: Rosof, AB, Felch, WC (eds.) Continuing medical education: A
6. Sutton, LS, Phillips, FM, Winfield, SR. Managing a satellite communications pro-
7. Treloar, LL. Facts about teleconferencing for staff development administrators. J
8. Benschoter, RA, Benson, SJ. Satellite system addresses rural health problems. J
9. Burleson, MA, Sugimoto, T. Cancer education via videoteleconferencing: an assess-
10. Lockyer, JM, Parboosingh, IJ, McDowell, AC. Teleconferencing and the continuing
1985; 6: 114-33.
Cont Educ Nursing 1976;7:3:26-32.
Libr Assoc 1990; 78:2:161-164.
impact of information on the teachable moment. Bull Med Libr Asso 1990; 78:2:173- 179.
16. American Cancer Society. Cancer facts and figures-1992. Atlanta 1992. 17. Kosecoff J. Kanouse DE, Brook RH. Changing practice patterns in the management
of primary breast cancer: consensus development program. Health Serv Res 1990;
18. Nattinger AB, Gottlieb MS, Veum J, Yahnke D, Goodwin JS. Geographic variation 2 5 : 5: 809-823.
in the use of breast-conserving treatment for breast cancer. N Engl J Med 1992;
19. Chute, AG. Balthazar, LB, Poston, CO. Learning from teletraining. Am J Distance 326:17:1102-1107,
Educ 1988; 2:3:55-63.
88

The Interactive Videoconference
20. Chute, AG. Teletraining: needs, solutions and benefits. In: International
21. Cervero, RM. Effective continuing education for professionals. San Francisco:
22. Berwick, DM. The double edge of knowledge (editorial). JAMA 1991; 266:6:841-
23. Dwyer, FM. Strategies for improving visual learning. Learning Service, State
24. Dede, CJ. Emerging technologies: impacts on distance learning. Ann Am Acad Pol
25. Borow, W. Medical television: prescription for progress (commentary). JAMA 1993;
Teleconferencing Association Yearbook 1990. Washington, D.C.: ITCA, May 1990.
Jossey-Bass Inc., 1988.
842.
College, PA: Learning Service, 1978.
SOC Sci 1991; 514:146-158.
270: 13: 1601 - 1602.
89