Embed Size (px)
Citation preview

Journal of Clinical Periodontology: 1976: 3: 110-122
Key words; occliisal trauma - healthy periodontium.Accepted for publication: June 29, 1975.
The influence of traumafrom occlusion on reduced but healthy
periodontal tissues in dogs3AN LINDHE AND INGVAR ERICSSON
Department of Periodontology, Faculty of Odontology, University of Gothenburg,Gothenburg, Sweden
Abstract. The experiments were performed in five dogs fed a soft diet which alloweddental plaque accumulation. Experimental periodontal breakdown was introduced onDay 0. After ISO days trauma from occlusion was produced in P and P4, i.e. themandibular fourth premolars, in the manner described by Svanberg & Lindhe (1973). OnDay 280 the periodontal pockets around 4P and P were eliminated. A notch wasprepared in the root at the level of the bottom of the surgically eradicated pocket. Inaddition, the occlusal trauma in the P region was deleted. From Day 280 to Day 370the teeth of the animals were brushed twice a day. The animals were then sacrificed,radiographs of the premolar regions were taken, and tissue sections comprising P P jM(and P3P4MJ were produced and subjected to microscopic analysis. The results indicatethat jiggling type occlusal trauma and tooth hypermobility are not factors which detri-mentally affect healing following periodontal surgery.
Results from analyses of human autopsy creased tooth mobility (the post-traumaticmaterial have suggested that trauma from phase). The traumatic phase is characterizedocclusion is a co-destructive factor in perio- by an osteoclastic alveolar bone resorption,dontitis (for review see Svanberg 1974a). gradually increasing width of the perio-Thus trauma produced by occlusal forces dontal membrane, and by a periodontalmay alter the pattern ol: spread of the ligament tissue in which there is an in-plaque-induced inflammation, thereby pro- creased number of vessels exhibiting en-ducing angular osseous defects and infra- hanced permeability to plasma and leuko-hony pockets (Glickman 1967). Experiments cytes. During the post-traumatic phase thein monkeys and dogs with normal gingiva vascularity (and permeability) of the en-or overt gingivitis have revealed that trauma larged periodontal membrane tissue is nor-from occlusion of the jiggling type induces mal. Furthermore, there is no obvious re-a series of adaptive alterations within the tention of leukocytes within the periodontalperiodontal tissues (Wentz et al. 1958, ligament, nor are there signs of increasedSvanberg & Lindhe 1973, Svanberg 1974b). osteoclastic activity. During the post-Under certain experimental conditions, traumatic phase the periodontal tissues be-jiggling forces produce one phase of in- come adapted to the altered functionalcreasing tooth mobility (the traumatic demands (Svanberg & Lindhe 1973, Svan-phase) and one phase of permanently in- berg 1974b).

INFLUENCE OF TRAUMA FROM OCCLUSION ON HEALTBY PERIODONTIUM 111
Lindhe &, Svanberg (1974) have pre-sented data indicating that the jiggling typeocclusai trauma, if occurring concomitantlywith an ongoing experimentally inducedprocess of periodontal tissue breakdown,may cause: (1) an increased rate of apicaldowngrowth of pocket epithelium, and (2)infrabony pocket formation. In someaspects the results of this study supportfindings reported from examinations of hu-man autopsy material (for review see Svan-berg &. Lindhe 1973). Thus, for example,Glickman & Smulow (1965, 1967) statedthat the periodontal tissues at the pressureside of teeth subjected to periodontitis andtrauma from occlusion could be consistentlycharacterized by the presence of angularbony defects and infrabony pockets. Thiswould imply (GHckman 1967) that, whenthe chronic inflammatory lesion producedby the bacterial plaque reaches the majorsupporting tissues, trauma from occlusionmay become a co-destructive factor in perio-dontitis.
The aim of the present investigation wasto study what remaining influence traumafrom occlusion may have on the process ofperiodontal breakdown once the causativefactors of infectious origin have beeneliminated.
Material and Methods
The experiments were performed in fivedogs (Beagles), which at the start of thestudy were 10-12 months old. During apre-experimental period of several weeks,the teeth of the dogs were first carefullyscaled and polished with rubber cups andpumice, and then subjected twice a day tometiculous toothbrushing. At the initiationof the experiment (Day 0), none of thedogs exhibited clinical signs of gingivitis.Throughout the study the animals were feda diet which allows gross plaque formation(Hamp et al. 1973).
PEPIGDONTJrii
Fig. 1. Outline of the experiment. Periodontalbreakdown was induced on Day 0 and traumafrom occlusion (T.O.) was introduced on Day180. On Day 280 periodontal pockets wereeliminated and T.O. deleted on the controlside. The experiment was terminated on Day370.
Planung des Experimentes. Experimenlelle Pa-rodontolyse wurde am Tage 0 induziert. Dazukam am Tage 180 Trauma durch Okklusion(T.O.). Am Tage 280 wurden die Taschen ent-fernt und das Trauma durch Okklusion an derKontrollseile aufgehoben. Tag 370, Abschlussdes Experimentes.Plan de ['experience. Une destruction paro-dontale etait produite au jour 0 et un trauma-tisme occlusai (T.O.) introduit au jour 180.Au jour 280, les culs-de-sac etaient elimines,et T.O. supprime du cote temoin. L'experiencese lerminait au jour 370.
On Days 0, 180, 280 and 370 (Fig. 1)the periodontal tissues of the ^P- and P^-regions were studied using the followingcriteria:
1: Gingival inflammation. The state of thegingiva was assessed according to the cri-teria of the Gingival Index system (Loe &Silness 1963). Separate scorings were madefor the mesial, distal, buccal and lingualaspects of the gingiva, and a mean scorefor the tooth was then calculated. In ad-dition, clinical colour photographs weretaken.
2: Plaque. The amounts of plaque on themesial, distal, buccal and lingual surfacesof the two teeth were estimated accordingto the Plaque Index system (Silness & Loe1964). A mean score for each tooth wascalculated.
3: Tooth mobility. Tg^ -values for ^P and

LINDHE AND ERICSSON
P4 were assessed in accordance with amethod described by Miihlemann (1954).
4: Alveolar hone topography. Standard-ized roentgenograms of the marginal al-veolar bone were produced in accordancewith a modification of a method describedby Eggen (1969) and Lindhe et al. (1973).
Immediately following the clinical exam-ination on Day 0, inflammation was in-duced in the periodotital tissues around^P and P , according to a technique de-scribed by Ericsson et al. (1975). A scalpelwas introduced 2 to 3 mm into the perio-dontal ligament around the entire root sur-face of the two teeth. Narrow, infrabonypockets of standardized depth (1 mm) wereprepared on the mesial and distal aspectsof 4P and P^. Approximately 1 mm of themarginal alveolar bone was then removedfrom the buccal and lingual areas of thesame teeth. A copper band was cementedto ^P and P^ in order to prevent reattach-ment of the periodontal tissues. The cop-per bands were removed 21 days later, anda ligature of cotton floss was placed aroundthe teeth at the level of the cemento-enamel junction.
Six months later (Fig. 1), trauma fromocclusion was produced by the installationof cap splints and bar devices as describedby Svanberg & Lindhe (1973) On bothsides of the maxilla the animals were sup-plied with cap splints fitted with obliqueplanes which made primary contacts withthe two lower fourth premolars ( P and P )before centric occlusion was established.Following installation of the cap splints, theincisors did not make contact in occlusion.Thus, when the mandible, after havingmade primary contact in the posterior pre-molar region, was moved further towardsthe centric occlusion, P and P^ were sub-jected to excessive horizontal forces andtilted in a mesial-buccal direction. On bothsides of the mandible, the canines ( C andCj) and the first molars ( M and Mj) were
fitted with crowns and connected with alingua! bar. A spring (Dentaurum Ltd®,Germany: Spring-hard wire diam. 0.55 mm)was attached to each of the lingual bars,and was also introduced through chan-nels (running in a buccal-Iingual direction)in the crowns of P and P4. When theanimal disoccluded the teeth, the springspulled ^P and P4 back to their originalpositions. The masticatory movements re-sulted in jiggling forces acting upon thelower fourth premolars. It should be stress-ed that: (1) the anatomy of the temporo-mandibular joint of the dogs permits theanimal to exercise hinge-axis movementsonly, and (2) the obhque planes of thecap splints were adjusted in such a way thatthey made simultaneous and even contactwith 4P and P4.
On Day 280, wben a severe periodontallesion had been established (Ericsson et al.1975), the oblique plane of the cap sphnton the right side of the maxilla was re-moved. The premolars and first molars onboth sides of the mandible (jM ^P gP ^Pand Pg P3 Pj M]) were then scaled andpolished with rubber cups and pumice. Thechronically inflamed periodontal tissuesaround ^P and P^ were eliminated usinga surgical approach originally described byWidman (1918), the so-called modifiedWidman flap procedure (Ramfjord & Nissle1974). During surgery a notch was care-fully prepared in the root surface at thelevel of the bottom of the clinically de-tectable infrabony pocfet. This notch servedas a reference point for measurements tobe made later on histological sections inthe microscope. The flaps were sutured.The sutures were removed 2 weeks later.
From Day 280 to the termination of theexperiment on Day 370 (Fig. 1) the teethof the dogs were subjected to careful me-chanical tooth cleaning twice a day. Par-ticular care was taken to clean the inter-radicular area of ^P and P^.

INFLUENCE OF TRAUMA FROM OCCLUSION ON HEALTHY PERIODONTIUM 113
At the end of the experiment the dogswere sacrificed with an overdose of Pento-thal (Pentothalsodium®, Abbott), the man-dibles dissected and divided along the mid-line. Radiographs of the premolar regionon both sides were taken on a skull-table.
TEST CONTROL
fT- .JE. ...BC
Fig. 2. Schematic drawing illustrating the me-sial aspect of the test (left) and control (right)tooth regions. In the microscopic sections thefollowing distances were assessed: 1) Notch (A)lo apical cells of the junctional epithelium(JE); 2) Bone crest (BC) to JE; and 3) A toBC. In the control gronp BC was alwayslocated coronally of A. In the test group, ECwas located close to A. See also Fig. 8.Schenialische Darsteltung der mes'talen Teileder Testbereiche (links) iind der KontroU-bereiche (rechts). In den mikroskopischenSchnitten wurden folgende Abstcinde gemes-sen: I) Kerbe (A) ~ apikale Zellen des Epithel-ansatzes (JE); 2) Knochenkanun (BCj - JE;3) A~BC. In der Kontrollgruppe war BC im-mer coronal von A lokalisiert. In der Test-gruppe war BC in der'Nahe von A lokalisiert.Siehe auch Abb. 8.
Dessin schematique illustrant I'aspect me-sial des regions des dents exp crime ntales(test = cote gauche) et temoins (control =cote droit). Sur les coupes microscopiques, lesdistances suivantes ont ete mesurees: 1) Rai-nure (A) — cellules apicales de Vattachementepithelial (JE); 2) Crete osseuse (BC) - JE; 3)A ~ BC. Dans le groupe temoin, BC etait tou-jours situe du cote coronaire de A. Dans legroupe experimental, BC etait situe pres de A.Voir aussi Pig. 8.
Specimens containing the distal portion ofthe third premolar, the fourth premolar andthe mesial portion of the first molar ( MP 3P and Pg P^ Mj), were harvested, fixed
in formahn, decalcified in a solution ofequal volumes of 50 % formic acid and15 % sodium fomate; they were then de-hydrated and embedded in paraffin. Mesio-distal sections were cut with the microtomeset at 7 am and were stained in hematox-yhn-eosin. From each biopsy five sections,20 [im apart, were used for determining thefollowing distances (Fig, 2) on the mesialaspect of 4P and P^:
1) The apical border of the notch (A) tothe most apical cells of the junctionalepithelium (JE);
2) The marginal bone crest (BC) to JE;3) A to BC;4) The length of the junctional epithelium
(EA).Using microscopic projection, the sec-
tions were magnified (X 98.4) and theirimages depicted on a white paper screen.The size of the periodontal ligament area(PLA) on the mesial side of ^P and P^ wasdetermined by the use of a planimeter(9527-12 Jngut® Polar Compensating Plani-meter, Ingut Ltd., Sweden), as describedin detail by Svanberg & Lindhe (1973). Thetotal vascular cross section area (VCA)within the PLA was also assessed planime-trically. In addition, the value of VCA/PLAX 100 for each specimen was calculated.The number of osteoclasts present on thealveolar bone surface bordering the PLAwas determined.
Results
Gingival Conditions and Amount of PlaqueAt the start of the study, the gingivaearound the test and control teeth werenormal and no plaque could be detectedon the gingival third of the tooth surfaces(Table 1). Following termination of the

114 LINDHE AND ERICSSON
of the test and control teeth
der Testzdhne und der
Table 1. The average values of GI, PII and tooth mobility (T^^on Day 0, 180, 280 and 370Die durchschnittliehen Werte von GI, Pll und ZahnmobilitatKontrollzahne an den Tagen 0, ISO, 280 und 370Valeurs moyennes de GI (Indice Gingival) et Pll (Indice Plague) et mobilite dentaire (des dents experimentales (test) et des dents temoins (control) aux jours 0, 180, 280 et 370
Parameter
Days
0
ISO
280
370
TestX
0
2.8
3.0
0.2
GI
ControlX
0
2.8
3.0
0.2
TestX
0
2.4
3.0
0
P!I
ControlX
0
2.4
3.0
0
TestX
3.4
9.6
25.7
42.4
s.e.
0.5-1c
1.3Hc
3.8—[c
6.8—1
T500 (1/100 mm)
ControlX
r-3.1c[—9.9
c[—24.2cL-5.4
s.e.
0.3
0.7
1.5
1.1
Level ofsignificance
NS
NS
NS
P<0.001
= P< 0.001.
tooth cleaning procedures and the applica-tion of cotton floss ligatures, large amountsof plaque rapidiy accumulated in the poste-rior premolar regions. The gingival condi-tion gradually deteriorated. On Days 180and 280 the gingivae around ^P and P^exhibited clinical signs of severe chronicinflammation. Following scaling, periodon-tal pocket elimination and the reinstitutionof daily tooth cleanings on Day 280, theclinical symptoms of gingivitis almost en-tirely disappeared in a very short periodof time. Thus, on Day 370, only one dogexhibited minute signs of gingivitis in the4P and P^ region; a mean GI of 0.2 (testand control) was calculated.
Tooth MobilityImmediately before the induction of perio-dontal inflammation, the T,^g values (Table1) of the test and eontrol teeth were 3.4(± 0.5) and 3.1 (± 0.3). After 6 monthsof experimental periodontitis, the Tg d valuesexhibited a small but significant increasefrom 3.4 to 9.6 (test) and from 3.1 to 9.9(control). After the installation of the capsplints and the bar devices there was a very
pronounced increase of the mohility of ^Pand P^ (Fig. 3). The T^^g values calculatedfrom measurements on Day 280 vv-ere 25.7
™ « MTOOTH MOBILITY
E3 CONTROL
1 5f
Fig. 3. Diagrammatic presentation of theaverage mobility of the test and control teeth(T ny) calculated from measurements with theperiodontometer on Days 180, 280 and 370.Das Diagramm zeigt durchschnittliche Mo-bilitat der Testzdhne und der Kontrollzdhne(T^oo)' «" ^^" Tagen 180, 280 und 370 mitdem Periodontometer gemessen.Diagramme represcntant la mobilite moyennedes dents experimentales (test) et temoins (con-trol) calculees (T^^^) a partir des mesuresfaites avec le periodontometre aux jours 180,280 et 370.

INFLUENCE OF TRAUMA FROM OCCLUSION ON HEALTHY PERIODONTIUM 115
(test) and 24.2 (control). The removal ofthe oblique plane on Day 280 resulted ina reduction of tooth mobility in the con-trol teeth. On Day 370 the average mobilityvalue of the control teeth did not signif-icantly differ from the corresponding valueon Day 0. In the test teeth, however, therewas a further increase of the mobilitytowards the end of the study. At the ter-mination of the experiment the mean T-y^value of the control teeth was 5.4 as com-pared with 42-4 for the test teeth.
Fig. 4. Radit ^ , i . , ^after 180 days of experimental periodontalbreakdown. Note the marked "horizontal" al-veolar bone loss.Rontgenaufnahme vom P^ Bereicb nach 180Tagen mil experimentellem parodontalen Ab-hau. Man hemerke den ausgesprochenen "hori-zontalen" Knochenverlust.Radiographie de la region P^ apres 180 joursde destruction parodontalc experimentale. No-ter la resorption osseiise "horizontale" mar-quee.
Fig. 5. Radiograph obtained after 280 days ofexperimental periodontal breakdown and 100days after the initiation of trauma from oc-elusion. Note the marked horizontal alveolarbone loss but also the angular bony defects(arrows).Rontgenaufnahmc nach 280 Tagen mil ex-perimentellem parodontalen Abbau und 100Tage nach Anbringen des okklusalen Traumas.Man bemerke den ausgesprochenen horizonta-len Knochenverlust sowie die anguldren Kno-chendefekte (Pfeile).Radiographie faite apres 280 jours de des-truction parodontale experimentale et 100jours apres le debut du traumatisme occlusal.Not^r la resorption osseuse alveolaire marquee,mais aussi les lacunes osseuses triangiilaires(voir fleches).
Alveolar Bone TopographyAfter 6 months of experimental perio-dontitis, the level of the marginal alveolarbone had been moved around 4 mm api-cally. The marginal crest of the alveolarbone had an uneven and indistinct appear-ance (Fig. 4). From roentgenographs ob-tained on Day 280, it could be seen thatthe jiggling forces had produced a marked

LINDHE AND ERICSSON
t.
Fig. 6. Radiograph of a control tooth regionobtained at the end of the experiment. Notethe distinctly outlined marginai alveolar bonecrest and the narrow periodontal ligamentspace,Rontgenaufnahmen eines Konlrollbereichesbeiin Abschluss des Experimentes. Man be-achte den scharf gezeichneten Knochenkammund den engen Desmodontalspalt.Radiographie de la region d'une dent te-moin, faite a la fin de I'experience. Noter lescontours nets de la crete osseusa alveolaire etla minceur de I'espace desmodontal.
cone-shaped widening of the marginal perio-dontal ligament space; this was especiallypronounced around the mesial root. In ad-dition, the periapical ligament space wasalso somewhat widened (Fig. 5). The re-moval of the oblique plane from the capsplint (i.e. the elimination of jigglingforces) and the treatment of the periodontalinflammation resulted in alterations in theperiodontal tissues which, in roentgeno-graphs, were characterized hy the reestab-
Fig. 7. Radiograph of a test tooth region ob-tained at the end of the experiment. Note thedistinctly, outlined marginal alveolar bone crestbut also the widened periodontal ligamentspace; tbis was especially pronounced at themesial root (arrows).Rontgenaufnahnie elnes Testbereiches beim Ab-schluss des Experimentes. Man beachte denscharf gezeichneten Knochenkamm, aber auchden erweiterten Desmodontalspalt, besondersan der mesialen Wurzel (Ffeilc).Radiographie de la region d'une dent ex-perimentale, faite a la fin de I'experience.Noter la nettete du contour de la crete alveo-laire, mais aussl Velargissement de I'espace des-modontal, particulierement prononce au niveaude la racine mesiale (voir fleches).
lishment of a narrow periodontal .ligamentspace and the presence of a distinct andradiopaque marginal termination of the al-veolar bone (Fig. 6). On radiographs ob-tained from the test tooth regions at theend of the study, the marginal terminationof the alveolar bone exhibited an even andrather distinct outline (Fig. 7). The perio-
INFLUENCE OF TRAUMA FROM OCCLUSION ON HEALTHY PERIODONTIUM 117
dontal ligament space, however, still ap-peared markedly widened, not only in themarginal but also in the apical regions.
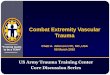
F(^. 5. Micrograph illustrating the mesial perio-dontal ligament from the control (C) and test(T) tooth regions in one dog. Note that: (1)the periodonta! ligament in the test section ismuch wider than in the control section, (2) thebone crest (BC) in the control section (in rela-tion to the notch = A) is located at a morecoronal level than in the test section, (3) theapical cells of the junctional epithelium (JE)are in hoth test and control sections locatedabove the apical border of the notch (A), and(4) the distance between JE and BC is thesame in the test and control sections.Die Mikroaufnahme zeigt das incxiale Desmo-dont im Kontrollbereich (C) und im Testbe-reich (T) hei dem gleichen Hund. Man be-ackte, (1) dass das Dcsmodont im Testbereichesviel weiler isl als im Kontrolibereich, (2) dassder Knochenkamm (BC) im Konlroltbereich(beziiglich der Kerhe A) koronaler liegt als imTestbereich, (3) dass die apikalen Zellen desEpithelansatzes (JE) im sowohl Kontrollbe-reich als auch im. Testbereich oberhalb derapikalen Grenze der Kerbe (A) liegen und (4),dass der Abstand JE~BC in beiden Bereichengleich ist.
Histological FindingsThe gingival tissues of four out of five dogshad a rather uniform appearance. The oralepithelium was well keratinized and thejunctional epithelium was smooth withoutsigns of rete peg formations. The connec-tive tissue was almost devoid of inflam-matory cells but characterized by the pres-ence of a dense collagenous network. In onedog the very marginal part of the gingiva(on test as well as control regions) con-tained a small zone of round cell accumula-tions. In no section did the periodontalligament tissue harbour infiltrates of leuco-cytes. The periodontal ligament tissue onthe pressure side of the test teeth har-boured a large number of small-sized « 10|.im in diameter) vascular units. In the con-trol teeth, the vasculature of the sameregion was mainly composed of largervascular units.
The most apical cells of the junctionalepithelium were, in the control as well as inthe test teeth, always located at a levelmarginal to the apical border of the notch(A) (Fig. 8). The dentin surface of thepart of the notch which made contact withthe junctional epithelium did not displaysigns of cementum formation. The part ofthe notch, however, which faced connectivetissues was always lined with newly formedcellular cementum (Fig. 8). Connective tis-
Coitpe montranl le desmodonte dii cotemesial des regions des dents temoins (C) etexperimentales (T) chez un des chiens. Noterque (1) le desmodonte de la coupe experimen-tale est beaucoup plus large que dans la coupetemoin, (2) la crete osseuse (BC) de la coupetemoin (par rapport a la rainure A) est siiueea un niveau se rapprochant plus de la. cou-ronne que dans la coupe experimental^, (3) lescellules apicales de Vattachement. epithelial (JE)sont situees, et dans les coupes temoins et dansles coupes experimentales, au dessus du bordapical de la rainure (A), et (4) la distance en-tre JE et BC est la meme dans les coupestemoin et experimentale.

118 LINDHE AND ERICSSON
Table 2. The average distance (in units) be-tween 1) the apical border of the notch (A)and the apical cells of the junctional epithelium(JE), 2) the bone crest (BC) to the junctionaiepithelium (JE), 3) the apical border of the notch(A) to the bone crest (BC) and 4) the averagelength of the epithelial attachment (EA) onthe mesial surface of the teethDurchschnittlicher Abstand (in Einheiten)zwischen 1) apikaler Begrenzung der Ker-be (A) und den apikalen Zellen des Epithel-ansatzes (JE), 2) Knochenkamm (BC) und demEpithelansatz (JE), 3) apikaler Begrenzung derKerbe (A) und dem Knochenkamm (BC) und4) die durchschnittUche Ldnge des Epithelan-satzes auf der mesialen Oberfldche der ZdhneDistance moyenne (en unites) 1) entre lebord apical de la rainure (A) et les cellulesapicales de I'attachement epithelial (JE), 2)entre la crete osseuse (BC) et I'attaehementepithelial (JE), 3) entre le bord apical de larainure (A) et la crete osseuse (BC); et 4)longueur moyenne de I'attachement epithelial(EA) sitr la face mesiale des dents
Test Control
Distances x ± s.e. x ± s.e. Level ofl m significance
A-JE 441 75.0 774 63.5 P<O.OiBC-JE 474 64.1 422 56.0 NSA-BC - 3 6 85.3 351 62.1 F<0.01EA 1880 130 1550 110 NS
sue fibres seemed to terminate in this ce-mentum.
The average distance (Fig. 2) betweenthe apical border of the notch (A) and themost apical cells of the junctional epi-theliutn (JE) was 441 ^m in the test teethand 774 im in the controls (Tahle 2). Thisdifference is statistically significant at the1 % level.
In both the test and control teeth theaverage distance between the bone crest(BC) and the apical border of the dento-gingival epithelium (JE) was around 440|xm.
Jn the control teeth the bone crest (BC)was consistently located on a level marginal
to the apical border of the notch. In thetest teeth, however, the bone crest in threedogs out of five was located at a level api-cal to the notch. The difference betweenthe test and control teeth regarding thelocation of the bone crest (BC) in relationto the notch (A) was statistically significant(P < 0.01).
The results from the determinations ofthe periodontal ligament area (PLA), thevascular cross-section area (VCA) and thenumber of osteoclasts are given in Table 3.On the average, the PLA as well as theVCA of the test teeth was twice the sizeof the controls. The vascular cross-sectionarea per periodontal ligament area, how-ever, was similar in test and control teeth(17 % and 14 %, respectively). There was asignificantly larger number of osteoclastspresent on the alveolar bone surface bor-dering the PLA of the lest teeth than inthe corresponding area of the control teeth(8.25 and 0.13).
Discussion
In the present study periodontal disease wasinduced around single posterior premolarsby allowing plaque to accumulate aroundcotton fioss ligatures placed around theneck of the teeth. Earlier studies in the dog(Lindhe •& Svanberg 1974, Ericsson et al.1975) have shown that 6 months of plaqueaccumulation of this kind will result in aperiodontal lesion characterized by "hori-zontal" alveolar bone loss, apical down-growth of the dento-gingival epitheliumand suprabony pocket formation. If underotherwise identical experimental conditionstrauma from occlusion of the jiggling typeis introduced as a co-factor, the rate ofprogression of periodontal breakdown seemsto increase and angular osseous defectscombined with infrabony pockets will result(Svanberg & Lindhe 1974, Lindhe & Svan-berg 1974).

INFLUENCE OF TRAUMA FROM OCCLUSION ON HEALTHY PERIODONTIUM 119
Table 3. The average periodontal ligament area (PLA), vascular cross-section area (VCA) andnumber of osteoclasts on the alveolar bone surface bordering PLA of the test and controlteethDurchschnittlicher Raum der Desmodontalspalien (FLA), Gefassquerschnittsfldche (VCA) undAnzahl der Osteoklasten auf den aiveoldren Knochenoberfliichen, die die Alveole bei Test- undKontrollzdhnen begrenzenSuperficie moyenne du desmodonte (PLA), siiperficie de la section des vaisseaux (VCA) etnombre d'osteoclastes a la surface de I'os alveolaire bordant le desmodonte des dents experi-mentales et temoins
Parameters Test ControlX s.e.
Level ofsignificance
RatioTest/ControlX s.e.
Periodontal ligamentarea (PLA)
Vascular cross-sectionarea (VCA)
VCA/PLA X 100 {%)Number of osteoclasts
767.3
129.4178.25
87
18
0.8
386.5
57.2140.13
25
6
0.09
F < 0.01
F < O.OOi
P < 0.001
2,0
2.3
0.3
0.4
In order to evaluate further the relativeimportance of plaque and the "co-destruc-tion factor" in periodonta! disease, a studywas performed in dogs with experimentallyinduced periodontal breakdown. Plaque wasremoved and pathologically deepened pock-ets were surgically eliminated, but jigglingtrauma was allowed to persist during heal-ing. The results demonstrated that, providedplaque and inflamed periodontal tissueswere removed and a proper oral hygieneregimen was established, healing also oc-curred in cases where jigghng forces wereacting on hypermobile teeth. This indicatesthat microbiai plaque is the main causativefactor not only in gingivitis and early perio-dontitis (Lindhe et al. 1973) but also in theprogressive lesion where trauma from oc-clusion may act as a "co-destructive" com-ponent. It should he observed that healingafter periodontal treatment occurred whenthe test teeth were still in the so-calledtraumatic phase (Svanberg & Lindhe 1973),i.e. exhibited increasing tooth mobility, in-creased osteoclastic activity and a largenumber of small-sized vessels within theperiodontal ligament of the zone of "co-
destruction". This implies that, in the perio-dontal ligament area, tissue alterationscaused by trauma from occlusion do notinterfere with the regeneration and thereorganisation of the epithelial and con-nective tissue components of the gingiva.This interpretation is supported by obser-vations reported by Waerhaug (1955). Hestudied the pathogenesis of pocket forma-tion in traumatic occlusion in dogs andstated: "The area of principal fibers be-tween the alveolar crest and the deepestline of the epithelial cuff represents a safetyzone. This band of tissue follows the move-ments of the tooth and will not be injuredby the same trauma that causes injury tothe periodonta] membrane within the al-veolus." As a matter of fact, in the pres-ent study, the distance between the apicalcells of the junctional epithelium and thealveolar crest (BC to JF; Table 2), i.e. the"safety zone", was the same in the test andnon-jiggled control teeth.
In the present experiment, healing of theperiodontal tissues was documented clin-ically as well as by microscopic analyses ofbiopsy preparations. The clinical data

120 LINDHE AND ERICSSON
showed that at the termination of theexperiment: (1) the gingiva around thetest teeth was normal (GI = 0 in four dogs;GI = 1 in one dog), and (2) the marginaltermination of the alveolar bone in theroentgenographs exhibited an even and dis-tinct outline. In the histological sections(except in one dog which showed clinical aswell as histological signs of overt gingivitis),there were no signs of round-cell infiltra-tion in the supraalveolar connective tissueor in the periodontal ligament in either thetest or control tooth regions. The junctiona!epithelium was smooth and without retepegs. Collagen fibres were inserted in thenewly formed cementum apical to the junc-tional epithelium. In this respect the resultsof this study corroborate data presented byGlickman et ai. (1966). They studied theeffect of occlusai forces on healing follow-ing muco-gingival surgery and reported thattrauma from occlusion "did not influencethe healing of the gingiva in terms of theformation of a normal gingival sulcus andzone of attached gingiva."
The findings of the present experimentsalso support observations made in clinicalstudies reported by Nyman et al. (1975)and Rosling et al. (1975). They showed thatonce plaque and chronically inflamed perio-dontal tissues had heen removed and pro-vided the dentitions were kept up to a pro-per standard of oral hygiene, normal heal-ing of periodontal tissues always occurred,even around teeth which were subjected tojiggling forces.
The histometric analysis of the perio-dontal tissues revealed various differencesbetween the test and control teeth. Thus,in the test teeth (1) the size of the perio-dontal ligament area, as well as the vascularcross-section area, was twice as large and(2) the number of osteoclasts was severaltimes as high as in the control teeth. Sim-ilar findings were reported by Glickmanet al. (3966). Three months after periodon-
tal surgery, the periodontal tissues of dogteeth subjected to occlusai trauma werecharacterized hy a widened periodontalligament with increased vascularity. Glick-man et al. (1966) also noted that the gin-gival segment of the alveolar bone in thepressure zone was thinner due to increasedosteoclastic activity. In the present materiala similar thinning of the bone was noted inthe jiggled teeth. In the most coronal partof the marginal bone this thinning resultedin a reduction of the height of a thin al-veolar bone crest. Therefore in the controldogs the bone crest was always located ata level marginal to the apical border of thenotch, whereas in the test dogs the bonecrest was located at or slightly apical tothe notch. The difference in location of thebone crest between the test and controlteeth may, therefore, be regarded as aconsequence of different functional de-mands. Since, however, the apical cells ofthe junctional epithelium in the controlteeth were located more coronally than inthe test teeth, it may be argued that in thecontrol teeth, but not in the jiggled testteeth, a reattachment resulted followingperiodontal treatment. The design of thepresent experiment does not allow a de-tailed analysis of this problem.
Zusammenfassung
Die Einwirkung traumatisicrendcr Ocklusionauf reduzierfes aber gesundes parodonlales Ge-webe bei HiindenDie Versuche wurden an fiinf Hunden vorge-nommen die mit weicher Kost gefiittert wor-den waren um Ansammlung dentaler Plaque(weicher Belage) zu erraoglichen. Experimen-telle Parodontolyse wurde am Tage 0 induziert.Nach 180 Tagen wurden die Zahne 4P und P4,also die mandibularen vierten Pramolaren, demTrauma durch Okklusion ad modum Svanberg& Lindhe (1973) ausgesetzt. Die Wurzel wurdein der Hohe des Bodens der chirurgisch be-seitigten Tasche mit einer Kerbe als Messindi-kator versehen, Gleichzeitig wurde der Anlasszur traumatisierender Okklusion an P beseitigt.

INFLUENCE OF TRAUMA FROM OCCLUSION ON HEALTHY PERIODONTIUM 121
Vom Tage 280 bis zum Tage 370 wurden dieZahne der Versuchstiere zweimal taglich gerei-nigt. Dann wurden die Tiere geopfert. Der Be-reich der Pramolaren wurde mit Rontgenauf-nahmen untersucht, Gewebeschnitte der Region3P 4P jM (sowie P., P^ M ) hergestellt und mi-kroskopisch analysiert.
Die Resultate zeigen, dass okklusales Trau-ma mit Vor- und Zuriickverschiebung derKrone (Schaukeltyp) sowie Hypermobiiitat vonZahnen keinen Aniass zu Heilungsstorungennach parodontaler ChLnirgie geben.
Influence des Iraumalismes occlusaux sur lestissus parodontaux affaihiis, inais non palho-logiques, chez le chienCes experiences ont ete effectuees sur cinq chi-ens recevant une nourriture moUe qui permet-tait l'accumulation de la plaque dentaire. Unedestruction experimentale du parodonte a eteintroduite au jour 0. ISO jours plus tard, untraumatisme occlusal a ete produit au niveaude ,P et P4, c.-a-d. au niveau des quatriemespremolaires inferieures, suivant la methodedecrite par Svanberg & Lindhe (1973). Au jour280, on a procede a l'eradication chirurgicaledes culs-de-sac existant autour de 4P et P4. Unerainure devant servir de repere a ete faite dansla racine au niveau du fond du cul-de-sac. Deplus, dans la region de 4P, le traumatisme oc-clusal a ete supprime. Du jour 280 au jour 370,les dents des animaux ont ete brossees deuxfois par jour. Les animaux ont ensuite etesacrifies, les regions des premolaires ont eteradiographees, et des coupes comprenant jP 4P^M (et Pg P^ M ) ont ete preparees et etu-diees au microscope. II ressort des resultats decette etude que le traumatisme occlusal detype "jiggling" (va-et-vient) et i'exagerationde la mobilite dentaire ne sont pas des fac-teurs agissant au detriment de la cicatrisationapres les interventions de chirurgie parodon-tale.
References
Eggen, S. (1969) Standardiserad intraorai ront-genteknik. Sveriges Tandliikarfdrbunds Tid-ning 17, 867-872.
Ericsson, L, Lindhe, J., Rylander, H. & Oka-moto, H. (1975) Experimental periodontalbreakdown in the dog. Scandinavian Journalof Dental Research 83, 189-192.
Giickman, I. (1967) Occlusion and periodon-tium. Journal of Dental Research 46, suppl.1, 53-59.
Giickman, I. & Smulow, J. B. (1965) Effect ofexcessive occlusal forces upon the pathwayof gingival inflammation in humans. Journalof Periodontology 36, 141-147.
Giickman, 1. & Smulow, J. B. (1967) Furtherobservations on the effects of trauma fromocclusion in humans. Journal of Perio-donlology 38, 280-298.
Giickman, I., Smulow, J. B., Voge!, G. &Passamonti, G. (1966) The effect of occlusalforces on healing following mucogingivalsurgery. Journal of Periodonlology 31, 319-325.
Hamp, S.-E., Lindhe, J. & Loe, H. (1973) Longterm effect of chlorhexidine on developinggingivitis in the Beagle dog. Journal of Perio-dontal Research 8, 63-70.
Lindhe, J., Hamp, S.-E. & Loe, H. (1973) Ex-perimental periodontitis in the Beagle dog.Journal of Periodontal Research 8, 1-10.
i-l-indhe, J. & Svanberg, G. (1974) Influence oftrauma from occlusion on progression ofexperimental periodontitis in the beagle dog.Journal of Clinical Periodontology 1, 3-14.
Loe, H. & Silness, J. (1963) Periodontal diseasein pregnancy. L Prevalence and severity.Acta Odontologica Scandinavica 21, 533—551.
Miihlemann, H. R. (1954) Tooth mobility. Themeasuring method. Initial and secondarytooth mohility. Journal of Periodontology25, 22-29.
Nyman, S., Rosling, B. & Lindhe, J. (1975) Ef-fect of professional tooth cleaning on healingafter periodontal surgery. Journal of Clin-ical Periodontology 2, 80-86.
Ramfjord, S. P. & Nissle, R. R. (1974) Themodified Widman flap. Journal of Perio-dontology 45, 601-607.
Rosiing, B., Nyman, S. & Lindhe, J. (1975)Effect of plaque control on bone regene-ration within periodontally treated intrabonypockets. In manuscript.
Silness, J. & Loe, H. (1964) Periodontal diseasein pregnancy. 11. Correlation between oralhygiene and periodontal condition. ActaOdontologica Scandinavica 22, 121-135.
Svanberg, G. (1974a) Experimental traumafrom occlusion in the dog. Thesis. Universityof Gothenburg, Sweden.
Svanberg, G. (1974h) Influence of trauma fromocclusion on the periodontium of dogs withnormal or inflamed gingivae. OdontologtskRevy 25, 165-178.

L I N D H E AND ERICSSON
Svanberg, G. & Lindhe, J. (1973) Experimentaltooth hypermobility in the dog. A method-ological study. Odontologisk Revy 24, 269-282.
Svanberg, G. & Lindhe, J. (1974) Vascularreactions in the periodontal ligament inci-dent to trauma from occlusion. Journal ofClinical Periodontology 1, 58--69.
Waerhaug, J. (1955) Pathogenesis of pocketformation in traumatic occlusion. Journal ofPeriodontology 26, 107-118.
Wentz, F. M., Jarabak, J. & Orban, B. (1958)Experimental occlusal trauma imitating cus-pal interferences. Journal of Periodontology29, 117-127.
Widman, L. (1918) The operative treatmentof pyorrhea alveolaris. A new surgicalmethod. Svensk Tandldkare Tidskrift 16, 3 -80.
Address:
Department of PeriodontologyFaculty of OdontologyFackS-400 33 Gothenburg 33Sweden