Embed Size (px)
Citation preview

The Impact of the American Recovery and The Impact of the American Recovery and p yp yReinvestment Act Funding Upon the Federal Reinvestment Act Funding Upon the Federal
Rural Community Health Center ProgramRural Community Health Center ProgramRural Community Health Center ProgramRural Community Health Center Program
PresenterPresenterPresenterPresenterMichael ShambaughMichael Shambaugh--Miller, Ph.D.Miller, Ph.D.
Department of Health Services Research and AdministrationDepartment of Health Services Research and AdministrationCollege of Public HealthCollege of Public Health
University of Nebraska Medical CenterUniversity of Nebraska Medical Center
CoCo--AuthorsAuthorsKate Hanson, M.A. Dept. of EpidemiologyKate Hanson, M.A. Dept. of Epidemiology
Jess Behrens M A Dept of HSRAJess Behrens M A Dept of HSRAJess Behrens, M.A. Dept. of HSRAJess Behrens, M.A. Dept. of HSRA
Nebraska Center for Rural Health Research

Rural Health Care Before the Advent of R H C Pthe Federal Rural Health Clinic Program

ARRA Funding RationaleARRA Funding RationaleARRA Funding RationaleARRA Funding Rationale
Th A i R d R i ATh A i R d R i AThe American Recovery and Reinvestment Act The American Recovery and Reinvestment Act provides $2 billion to be invested in Community provides $2 billion to be invested in Community Health CentersHealth Centers an unprecedented opportunity toan unprecedented opportunity toHealth Centers,Health Centers, an unprecedented opportunity to an unprecedented opportunity to serve more patients, stimulate new jobs, and meet the serve more patients, stimulate new jobs, and meet the significant increase in demand for primary health caresignificant increase in demand for primary health caresignificant increase in demand for primary health care significant increase in demand for primary health care services among the Nation's uninsured and underserved services among the Nation's uninsured and underserved populations. Over the next two years Recovery Act populations. Over the next two years Recovery Act p p y yp p y y(ARRA) funding will be invested in Community Health (ARRA) funding will be invested in Community Health Centers to support critically needed health care services, Centers to support critically needed health care services, renovations and repairs and investments in health renovations and repairs and investments in health information technology. information technology.

QuestionQuestionQuestionQuestion
Did the funding go to areas where the need has Did the funding go to areas where the need has been demonstrated as critical through secondary been demonstrated as critical through secondary g yg ymethods methods –– not just the expressed need found in not just the expressed need found in the grant applications from the states receivingthe grant applications from the states receivingthe grant applications from the states receiving the grant applications from the states receiving awards.awards.

Study ApproachStudy ApproachStudy ApproachStudy Approach
Find alternate methods of measuring the need Find alternate methods of measuring the need for expanded services or new services.for expanded services or new services.pp
V l bl C i i A l iV l bl C i i A l iVulnerable Communities AnalysisVulnerable Communities AnalysisShambaughShambaugh--Miller, 2001Miller, 2001
FQHC Placement MeasurementFQHC Placement MeasurementSwann and Griffin, 2006Swann and Griffin, 2006

Vulnerable Communities ModelVulnerable Communities ModelVulnerable Communities ModelVulnerable Communities Model
Original useOriginal useTo develop an alternative model for determining To develop an alternative model for determining p gp gareas that are financially risky for primary care areas that are financially risky for primary care practitioners.practitioners.ppUsing updated variables will recalculate the VC’s for Using updated variables will recalculate the VC’s for the entire nationthe entire nationthe entire nationthe entire nation

Health Service Communities Vulnerable by Principal Components Analysis and
Areas Vulnerable by Population DensityResults of first VC run using2000 Census data y p y2000 Census data.
Study RegionAreas vulnerable by population densityHSC Vulnerable by Principal Components AnalysisBorder statesStudy states
N
EW
S
0 700 1400 Miles
Source: U.S. Census, 2000

Optimal Placement MethodOptimal Placement MethodOptimal Placement MethodOptimal Placement Method
Locations are chosen based on competitions ofself-submitted proposals which do not necessarilyself submitted proposals, which do not necessarilyinclude the location that is best for the overallsystem, or that would lead to a better geographicdispersion of resources (National Center fordispersion of resources (National Center forPrimary Care).

Optimal Placement MethodOptimal Placement MethodOptimal Placement MethodOptimal Placement Method
Developed an optimization model that maximizesthe coverage of the weighted demand in thethe coverage of the weighted demand in thepopulation, limited by the overall budget and the capacity levels of each facility and service.

Optimal Placement MethodOptimal Placement MethodOptimal Placement MethodOptimal Placement Method
Used statistical methods on national health survey databases to determine predictors of somedatabases to determine predictors of some healthcare measures, and used these predictors with Census data to estimate need within each countycounty.

Optimal Placement MethodOptimal Placement MethodOptimal Placement MethodOptimal Placement Method
ddFindingsFindingsFigure shows that much of this unmet demand is in southern states such as Alabama, Georgia, and Mississippi. Third, they found the MUA constraint did d h l b f CHC b l h ddid reduce the total number of CHCs, but only had a big impact on a few states; namely Colorado, New Mexico North Dakota Texas and West VirginiaMexico, North Dakota, Texas, and West Virginia.Of these, the western states all gained CHCs in the MUA constrained solution compared to the notMUA-constrained solution compared to the not-constrained solution.

Optimal Placement MethodOptimal Placement MethodOptimal Placement MethodOptimal Placement Method
Th h f h f f fThere was therefore some shift of CHCs from urban to rural areas. Clearly the value of MUA is to ensure that these populations get preference. One of the bene¯ts of the national CHC location model is that it allows for quantifying the services delivered, enabling policy makers to weigh the cost and bene¯t of their decisions such as requiring CHC locations be in MUA q gcounties or that a certain percentage of locations be in rural communities.

Optimal Placement MethodOptimal Placement MethodOptimal Placement MethodOptimal Placement Method
Wh ki i b h d l d hWhen making comparisons between the model and the current CHC locations, it is clear that the current location and service decisions are not the most cost-efficient. Locations and services chosen by our model offered improvements in all measures of 15 - 20%, such as for encounters per year.Thier solutions better target uninsured and rural populations, even though this was not an explicit goal of the optimizationeven though this was not an explicit goal of the optimization model. Results also show that it is important to choosepnot only locations, but also the services and capacities of the locations.
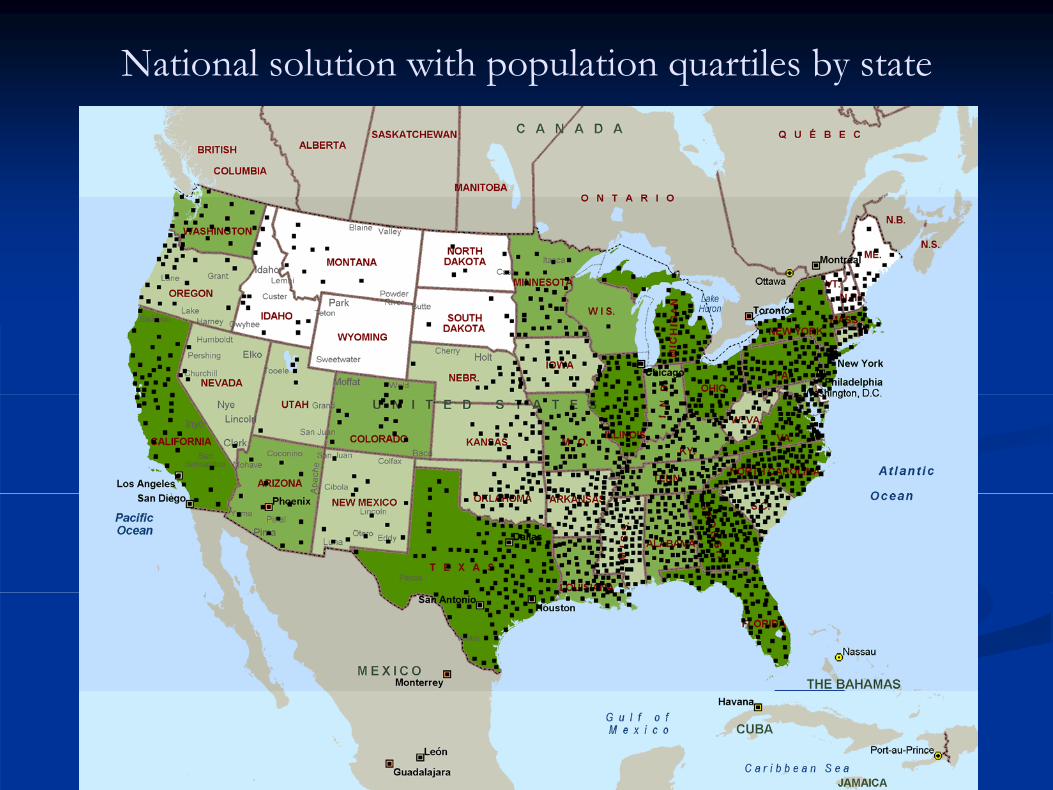
National solution with population quartiles by state

Current locationsOf CHC’s in relationTo Vulnerable Communities

Next StepsNext StepsNext StepsNext Steps
L ARRA f d d CHC’ h f d d dL ARRA f d d CHC’ h f d d dLocate ARRA funded CHC’s that were funded under Locate ARRA funded CHC’s that were funded under two categoriestwo categories
E d d dE d d dExpanded needExpanded needNew facilityNew facility
D t i hi h f iliti i d f di dD t i hi h f iliti i d f di dDetermine which facilities received funding and were Determine which facilities received funding and were either in recognized VC or in Optimal Locations.either in recognized VC or in Optimal Locations.U i th R l H lth k l l t th j bU i th R l H lth k l l t th j bUsing the Rural Healthworks program, calculate the job Using the Rural Healthworks program, calculate the job creation and financial impact of the grant funding upon creation and financial impact of the grant funding upon the local service areasthe local service areasthe local service areas.the local service areas.Policy recommendationsPolicy recommendations

SourcesSourcesSourcesSources
Optimization of Community Health Center Locations and Service Offerings with Statistical gNeed EstimationPaul M Griffin Christina R Scherrer Julie LPaul M. Griffin, Christina R. Scherrer, Julie L. Swann
(Special Issue on Healthcare Engineering)Submitted August 2006 Accepted May 2007Submitted August 2006, Accepted May 2007

SourcesSourcesSourcesSources
U S H l h d H S iU S H l h d H S iU.S. Health and Human ServicesU.S. Health and Human Serviceshttp://www.hhs.gov/recovery/hrsa/healthcentergrants.htmlhttp://www.hhs.gov/recovery/hrsa/healthcentergrants.html
Health Services at Risk in “Vulnerable” Rural PlPlacesMichael D. Shambaugh-Miller, ABD, Julie A. Stoner, PhD L i G P l PhD K ith J M ll PhDPhD, Louis G. Pol, PhD, Keith J. Mueller, PhDRural Policy Brief, Volume Seven, Number Five (PB2002 5) O t b 2002 RUPRI C t f R l(PB2002-5) October 2002 RUPRI Center for Rural Health Policy Analysis

Contact InformationContact InformationContact InformationContact Information
Michael ShambaughMichael Shambaugh--Miller, Ph.D.Miller, [email protected]@unmc.edu
UNMC College of Public Health UNMC College of Public Health –– Dept. of Health Dept. of Health gg ppServices Research and AdministrationServices Research and Administration
402402 559559 52605260402402--559559--52605260www.unmc.edu/nebraskawww.unmc.edu/nebraska