Embed Size (px)
Citation preview

Shiga Toxin-Producing
Escherichia coli:
The Human Health Perspective
P. I. Tarr
Division of Gastroenterology and Nutrition
Washington University School of Medicine
NOTE: Some slides could include data that have not yet been published, or subject to peer review, and should not be quoted and should be considered to be preliminary
Perspective
E. coli O157:H7: ~ .9/100,000 people/year (MMWR Morb Mortal Wkly Rep 2011;60:749-55)
HUS: 500-750 cases per annum, 90% < 18 yo
Rare infections need good systems, protocols,
and vigilance
• How can we optimally diagnose this infection?
• Can we attenuate human illnesses?
• What misconceptions do we need to address?

Time is not on your side!
-3 -2 -1 0 1 2 3 4 5 6 7
Diarrhea
Bloody
diarrhea

First Contact (frequently ER) Profile:
Memorial Day to Thanksgiving
Holtz, et al, Gastroenterology. 2009 ;136:1887
Klein, et al, J Pediatr. 2002;141:172

Strategic Microbiology
• Culture!
(C. difficile optional –
await bacterial
culture)
• Hustle stool to the lab

First Medical Contact
Microbiologic Evaluation is
CRITICAL

Stool
Broth
Incubate O/N
Shiga Toxin EIA
Microbiologic Evaluation is Critical
Agar vs. Assay

Pediatrics. 1987;80:37
J Infect Dis. 1990;162:553
J Pediatr. 1998;132:777
J Infect Dis. 2001;183:1063
J Pediatr. 2002;141:172
Foodborne Pathog Dis. 2006;3:88
Epidemiol Infect. 2007 Mar 5 (epub)1-7
Arch Pediatr Adolesc Med. 2011;165:884-9.
Agar detects only O157:H7, but this single
serotype remains the nearly exclusive (>95%)
cause of HUS in US, UK, Canada, Japan, and
South America
How much HUS do non-O157:H7
STEC cause in US?
83 patients with HUS, (1987-91), nationwide surveillance (Banatavala, et al*).
70 patients had stool cultures with growth, median of 8 days after illness onset.
30 patients had STEC; 25 of these were O157 (overall O157 rate: 35%) (only 1/3 of HUS patients have O157:H7 if cultured on admission with HUS**, but 96% are + if cultured early in illness)
Of 5 patients from whom non-O157:H7 STEC were recovered, 4 had serology, and
3 of these 4 had evidence of a recent infection with E. coli O157.
Of 31 cases from whom no STEC were recovered, 21 had antibodies to O157. (Sera obtained up to 80 days after illness onset, well after seropositivity peak***, so this rate is possibly low.
Little room left for non-O157:H7 STEC to cause HUS
in US
*J Infect Dis. 2001;183:1063 ** J Infect Dis 1990;162:553 *** J Infect Dis 2002;186:566

Recent Study of HUS
50 children with diarrhea – associated HUS, from 10
centers in US (UC Davis, Seattle, Indiana, Little Rock,
Milwaukee, Albuquerque, Columbus, Cincinnati, St.
Louis) and 1 in Scotland (Glasgow) (Hickey, et al*)
Years: 2008-2009.
27+ for O157, 1 + for O121:H19, All other were negative
*Arch Pediatr Adolesc Med. 2011;165:884

Shiga toxin–producing Escherichia coli (STEC) isolates by method of
initial detection and STEC serotype, Connecticut, 2000–2009.
Hadler J L et al. Clin Infect Dis. 2011;53:269-276
© The Author 2011. Published by Oxford University Press on behalf of the Infectious Diseases
Society of America. All rights reserved. For Permissions, please e-mail:

Connecticut 2000-2009
• 499 broth + EIAs
• 163 were O157:H7 (33%)
– 10% HUS rate
• 229 were non-O157:H7 STEC (46%);
– 0.4% HUS rate
• 78 (16%) were not + at State Laboratory
• 29 (6%) no STEC recovered
Clin Infect Dis 2011;53:269

O157/non-O157 Acuity Pyramid
HUS 95/5 - 99/1 in multiple studies
Seattle Children’s Hospital Emergency Room
19911: 13/5
1998-20012: 28/11
Statewide, MT (1998-2000)3 and CT (2000-2009) 4
MT : 32/50 (#2 was O26, with 16 isolates)
CT: 163/229 (#2 was O111, with 44 isolates) 1Gastroenterology. 1993;105:1724; 2J Pediatr. 2002;141:172; 3 J Infect Dis.2003;188:719; 4Clin Infect Dis 2011;53:269

Toxin Screening misses O157:H7
(i.e., sorbitol MacConkey
agar is more sensitive)
• Klein, E, et al, J Peds 2002; 172;
• Emerg Infect Dis. 2000 Sep-Oct;6(5):530-3.
• Eur J Clin Microbiol Infect Dis. 2003
Nov;22(11):689-92. Epub 2003 Oct 23.
• Emerg Infect Dis. 2007 Feb;13(2):318-21.
• J Clin Microbiol. 2007 Oct;45(10):3377-80. Epub
2007 Aug 1. PubMed PMID: 17670920;
• J Clin Microbiol. 2003 Jun;41(6):2650-3.
Toxin Assays Slow
Diagnosis of O157:H7
• Not read daily in many centers
• Often sent to commercial laboratories
• Isolation devolves to state PHL
• State of isolation isn’t always state of
presentation or residence
• Specimen transport issues

Why rapidly diagnose O157?
• E. coli O157:H7 thrombotic complications,
epidemics; other serotypes rarely do
• Syndromic profiling helpful, but clinician needs
+ or - culture result ASAP
• HD needs isolate
• Intervention appears possible
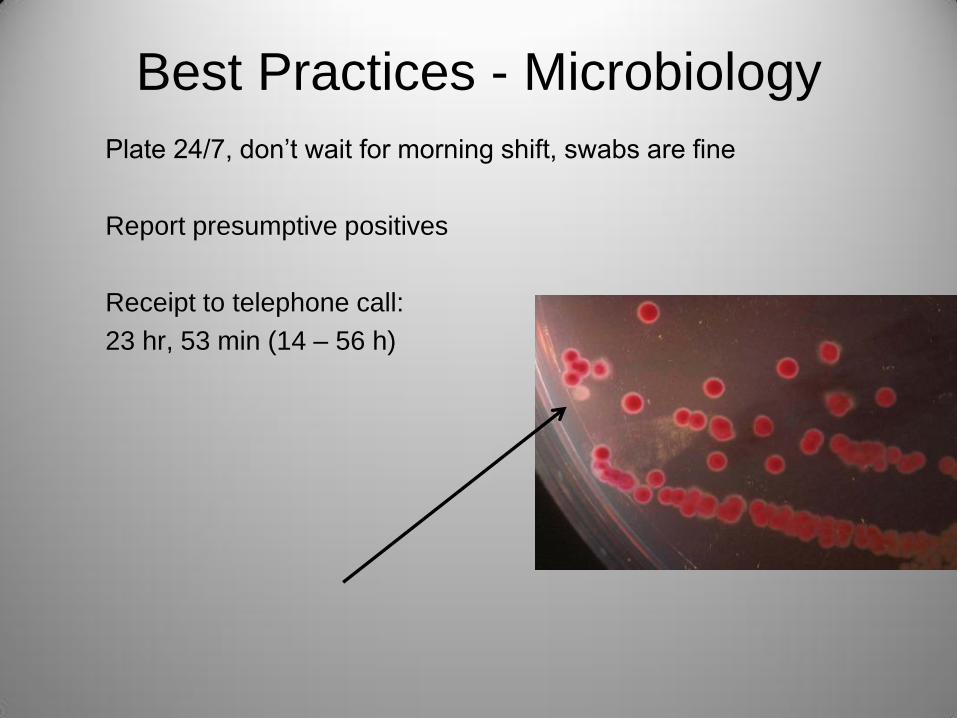
Best Practices - Microbiology
Plate 24/7, don’t wait for morning shift, swabs are fine
Report presumptive positives
Receipt to telephone call:
23 hr, 53 min (14 – 56 h)

CDC Guidelines
Recommendations for Diagnosis of Shiga Toxin--Producing
Escherichia coli Infections by Clinical Laboratories LH Gould, C Bopp, N Strockbine, R Atkinson, V Baselski, B Body, R Carey, C Crandall, S Hurd, R Kaplan, M Neill, S
Shea, P Somsel, M Tobin-D'Angelo, P M Griffin, P Gerner-Smidt
“All stools submitted for testing from patients with acute community-
acquired diarrhea … should be cultured for O157 STEC on selective
and differential agar.”
Best practice: Agar and toxin assay
MMWR Recomm Rep. 2009;58(RR-12):1-14
What’s the rush?

Control
Uncomplicated
Pre-HUS
38
Fra
gm
en
t 1
+2
(n
mo
l/L) A
Control
Uncomplicated
Pre-HUS
112
t-P
A a
ntig
en
(n
g/m
L) D
Control
Uncomplicated
Pre-HUS
20
50
PA
I-1
act
ivity
(IU
/mL
) B
Control
Uncomplicated
Pre-HUS
710
log
D-d
ime
er
(lo
g n
g/m
L)
E
Control
Uncomplicated
Pre-HUS
010
t-P
A/P
AI-
1 c
om
ple
xes
(ng
/mL
)
C
Control
Uncomplicated
Pre-HUS
1000
3000
PA
P c
om
ple
xes
(ng
/mL
)
F
D-dimer Before HUS
*
*
NEJM 2002; 346:23

Child at Presentation
• Little or no toxin in stool
• Coagulation system activated, but CBC normal
• Pathogen still present in stool
• Kidneys not yet injured
What’s a provider to do?

Admit, Isolate
Inpatient (contact) precautions:
dedicated equipment, gowns, gloves
Outpatient advice:
“Wash your hands well!”
Werber, et al, Clin Infect Dis. 2008;46:1189-96.

0 10 20 30 40 50 60 70
OR
1997-1999 , n=71
Withhold antibiotics
N Engl J Med. 2000;342:1930-6.

• Antibiotics are a risk for HUS in MN
Smith, K, et al, Pediatr Infect Dis J. 2011 Sep 1
• Antibiotics are commonly prescribed
36%, US and Scotland (Hickey, et al, Arch Pediatr Adolesc Med. 2011; 165:884)
23%, Minnesota (Smith, K, et al, Pediatr Infect Dis J. 2011 Sep 1)
44% in a multi-state CDC analysis (Nelson, et al, Clin Infect Dis. 2011;52:1130)

Volume Expand
• Comfort
• Vascular protection in view of HUS risk
• q12 h CBC (drop the hemoglobin)
• daily BUN, creatinine, electrolytes
• K is OK if K is normal or low
• Wait for platelets to rise
(single determination rarely sufficient)

0.5 0.5
1.4
2.3
5.14.9
5.5 5.6
6.0
5.6
4.3 4.3 4.2
2.9 2.8 2.7 2.7 2.7 2.8
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Day of Illness
0.4 0.3 0.4
1.3
1.9
2.22
1.3
0.90.7 0.6
2 3 4 5 6 7 8 9 10 11 12
Day of Illness
Non-oligoanuric
Oligoanuric
creatinine creatinine

0.5 0.5
1.4
2.3
5.14.9
5.5 5.6
6.0
5.6
4.3 4.3 4.2
2.9 2.8 2.7 2.7 2.7 2.8
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Day of Illness
0.4 0.3 0.4
1.3
1.9
2.22
1.3
0.90.7 0.6
2 3 4 5 6 7 8 9 10 11 12
Day of Illness
Non-oligoanuric
Oligoanuric
creatinine creatinine
Oakes RS, Kirkham JK, Nelson RD, Siegler RL. Duration of oliguria and anuria as predictors of chronic renal-related sequelae in post-diarrheal hemolytic uremic syndrome. Pediatr Nephrol. 2008;23:1303–8.
Loirat C. [Post-diarrhea hemolytic-uremic syndrome: clinical aspects]. Arch Pediatr. 2001;8 Suppl 4:776s–84s.
Siegler RL, Pavia AT, Christofferson RD, Milligan MK. A 20-year population-based study of postdiarrheal hemolytic uremic syndrome in Utah. Pediatrics. 1994;94:35–40.
Siegler RL, Milligan MK, Burningham TH, Christofferson RD, Chang SY, Jorde LB. Long-term outcome and prognostic indicators in the hemolytic-uremic syndrome. J Pediatr. 1991;118:195–200.
Garg AX, Suri RS, Barrowman N, Rehman F, Matsell D, Rosas-Arellano MP, et al. Long-term renal prognosis of diarrhea-associated hemolytic uremic syndrome: a systematic review, meta-analysis, and meta-regression. JAMA. 2003;290:1360–70.
Robson WL, Leung AK, Brant R. Relationship of the recovery in the glomerular filtration rate to the duration of anuria in diarrhea-associated hemolytic uremic syndrome. Am J Nephrol. 1993;13:194–7.
Tonshoff B, Sammet A, Sanden I, Mehls O, Waldherr R, Scharer K. Outcome and prognostic determinants in the hemolytic uremic syndrome of children. Nephron. 1994;68:63–70.
Huseman D, Gellermann J, Vollmer I, Ohde I, Devaux S, Ehrich JH, et al. Long-term prognosis of hemolytic uremic syndrome and effective renal plasma flow. Pediatr Nephrol. 1999;13:672–7.
Mizusawa Y, Pitcher LA, Burke JR, Falk MC, Mizushima W. Survey of haemolytic-uraemic syndrome in Queensland 1979-1995. Med J Aust. 1996;165:188–91.
Spizzirri FD, Rahman RC, Bibiloni N, Ruscasso JD, Amoreo OR. Childhood hemolytic uremic syndrome in Argentina: long-term follow-up and prognostic features. Pediatr Nephrol. 1997;11:156–60.
Gianantonio CA, Vitacco M, Mendilaharzu F, Gallo G. The hemolytic-uremic syndrome. Renal status of 76 patients at long-term follow-up. J Pediatr. 1968;72:757–65.
Gianantonio CA, Vitacco M, Mendilaharzu F, Gallo GE, Sojo ET. The hemolytic-uremic syndrome. Nephron. 1973;11:174–92.
Dolislager D, Tune B. The hemolytic-uremic syndrome: spectrum of severity and significance of prodrome. Am J Dis Child. 1978;132:55–8.
de Jong MC, Monnens LA. Recurrent haemolytic uraemic syndrome. Padiatr Padol. 1976;11:521–7.
Mencia B. S., Martinez de Azagra A, de Vicente A. A., Monleon L. M., J. CF. Uremic hemolytic syndrome. Analysis of 43 cases. An Esp Pediatr 1999;50:467–70.
Good
Bad

Variable Good
outcome
Poor outcome P
Presentation Day 2 Day 3 0.066
First culture Day 2 Day 3 0.02
First IV
started
Day 3
(0-4)
Day 4.5
(2-9)
0.01
First Cultue
obtained
Day 2
(0-4)
Day 3
(2-9)
0.02
Culture + Day 4 (2-4) Day 7 (3-9) 0.001
What variables are associated with good outcomes?
Pediatrics. 2005;115:e673-80

Copyright ©2005 American Academy of Pediatrics
Fig 2. Volume and characteristics of fluids that were administered during first 4 days of
illness
Pediatrics. 2005
Jun;115(6):e673-80

Copyright restrictions may apply.
Hickey, C. A. et al. Arch Pediatr Adolesc Med 2011;165:884-889.
Logistic Models

Detection Acceleration
Every second counts:
presentation specimen
(come in now)
Specimen inoculation (swab OK)
Inoculation interpretation
(don’t worry about H7, coli confirmation)
Report health department (do it now)
4H Management
• Hospitalize
• Hydrate
• Hold antibiotics
• Health Department





























