Embed Size (px)
Citation preview

The Healthcare Analytics Summit 2021VirtualSept. 21 – 23, 2021 (half-day sessions)
▪ Industry-Leading Featured Speakers
▪ Steve Kerr
▪ Rana el Kaliouby, PhD
▪ Vin Gupta, MD, MPA, MSc
▪ Chris Chen, MD
▪ Amy Compton-Phillips, MD
▪ Brent C. James, MD, Mstat
▪ Sadiqa Mahmood, DDS, MPH
▪ 21 Educational Breakout Sessions
▪ CME Accreditation for Clinicians
▪ Analytics and AI Showcases, Networking, and More
▪ Virtual Platform optimized for a live experience
“The virtual experience was beyond any other that
I've attended. You all did a wonderful job of creating
an "in-person" feel and I appreciate that as a learner.
The virtual platform was very intuitive and fun.”
Visit hasummit.com to register and learn more

Vitalware User Group 2021
This year's User Group will include:
•CEU opportunities
•Industry education
•New Vitalware product features, tips &
tricks
•Prizes and awards
Please Note: This event is open to
Vitalware clients ONLY. Please
reach out to your Client Success
Executive to register.

New Trends In Hospital Charge
Capture

William L MalmND,CRCR,CMAS,CHIAP
Vice President, Revenue Transformation


Description of Session
• New Trends We’re Seeing in Hospital Charge Capture will show a direction toward enhanced use of data analytics. With an increasing focus on cost and capped reimbursements data analytics provide that insight into management of revenue cycle to attain, maintain or regain your optimal level of performance. We will cover levers that can be manipulated to attain optimal charge capture.

Agenda
Today we will cover:
▪ Overview of Charge Capture and identification of weak links
▪ Understand the move to non-hospital services
▪ Review People – Process and Technology Approach

Objectives
Today we will cover:
▪ Be able to state two people criteria
▪ Be able to state two process criteria
▪ Be able to state two technology criteria

Overview of Charge Capture

Revenue Cycle Flow

Trends
• New trends revolve around going back to basics and adding data analytics
• Breaking down the silos
• Move the action steps to the earliest point in the revenue cycle
• Focus on Clinical Revenue Cycle (CRC) processes
• Reconciling policies and procedures to processes (many of which may be outdated)
• Create control points – very similar to accounting
Trends
• Move from Patient Financial Services to Patient Access
• Additional focus on data analytics • Identification of patterns of behavior
• Enhanced audit / agreed-upon-procedure
• Focus on Net Patient Service Revenue and Cost to Deliver services to ensure that bottom line
• Enhanced audits / technology for root cause remediation to avoid increased costs / charge leakage
• Charge Capture objective is 1-3% of Net Patient Service Revenue

The Revenue Cycle Interdependencies
People
ProcessTechnology


People – Process & Technology

Process is only as strong as the weakest link !
Pt Access
Clinical Revenue
Cycle
Revenue Integrity
Patient Financial Services

People
• Human intervention and creation of the revenue cycle can only be supplemented by technology
• See trends toward moving the educational components closer to the beginning of the revenue cycle
• Great focus is now occurring with Patient Access and their personnel
• Professional Organization – National Association of Healthcare Access Management (NAHAM)
• Provides excellent training and education opportunities to improve Patient Access
• Provides certification

People
• Focus on an area where errors that lead to initial denials and failed claims originate – Patient Access• HFMA stated that up to 40% of claims can have registration related errors
• Clinicians:• Clinical departments and/or staff are seldom included in the full scope
of revenue cycle discussions and plans
• New trends include a concept of a clinical revenue cycle
• Focus on documentation and clinical activities associated with charge capture
• Clinical staff will need to be continuously educated and monitored, through audit, to enhance their documentation skills

People
• Clinicians:• Some areas of clinical focus would include personnel from:
• Nursing
• Cardiac Cath / EP Lab
• Mid-level practitioners
• Peri-Op services
• Pharmacy
• Clinical Documentation Improvement Specialists
• Managed Care
• Social Services
• Radiology
• Laboratory
• Emergency Services / Observation

People
• Clinicians:• While the prior was a partial listing the clinical group needs to focus
on whatever area responsible for documentation and charge capture.
• Other non-clinicians should be included as well in a Clinical Revenue Cycle (ex supply chain)
• HIM / Coding:• This group are also Subject Matter Experts (SME) like the CRC
personnel
• Coding is based upon well documented standards that require complete sufficient and accurate documentation
• Coding personnel can risk over / under coding based on interpretation

People
• Revenue Integrity• Key components for this group are charge capture and pre-billing
edits
• Reconciliation and charge capture audits limit the leakage that diminishing the bottom line
• RI staff are also specialty trained • May have coding experience or clinical background
• May have compliance background
• May have billing experience and/or denial experience
• Professional Organizations' such as HFMA, AHIA and NAHRI are focused on the revenue cycle and outcomes and offer training and education

People
• Information Technology• Provides an essential skillset
• IT services are the essential link for all processes within the revenue cycle
• IT personnel create documentation templates
• IT personnel create “documentation driven charging”
• One of the silo concerns is that historically IT has created processes that work for the software but may not be complementary to the human processes
• Including IT on any team will provide value

People
• Key to any performance improvement plan are two groups that are rather new to revenue cycle
• Six Sigma groups:• Determine the cause of the underperformance or error
• Create sound remediation plans
• Execute and monitor these plans
• Project Management Organization• Implements the root cause remediation and performance
improvement using documented implementation plans to ensure all aspects are covered and performed

Key People Strategies
• Integrated team bringing skills together for synergistic result
• On-going education, training and cross training
• Continued second person review to identify weaknesses and re-train as required
• Personnel are able to identify root cause issues with limited data and therefore should have the authority to recommend a root cause remediation process

Key People Strategies
• Human capital is the weakest link in the revenue cycle therefore:• Constant review at control points is necessary
• The next step in the revenue cycle should review the prior step to ensure that the personnel have completed their required component
• Failure(s) identified should immediately be assessed as a group and root cause identified
• Retention efforts are key to ensuring a growing revenue cycle • Constant turnover expends resources and leaves the cycle more prone to error
• Focus on putting the right person in the right role at the right time for the right reason

Labor is More than Just FTE Counts

Labor Management
• Labor management is key to the revenue cycle
• Frequently cost savings result in FTE reduction
• Want to focus on training, retaining and managing roles that are consistent to the objective
• Labor management focuses on efficiency not just reduction by matching acuity and effort to a specific role
• Outsourcing can be considered but still must be managed by the facility. Complete outsourcing can lead to lost opportunities.

Accounting Internal Controls for Revenue Cycle
Patient Access
Control Point/Assess
CRCControl
Point/Assess
RI
Control Point /Assess

Internal Controls Necessary with People
• Human nature is to experience errors and failures• High volumes, client facing pressure to complete
• Complex software and incomplete training
• Patient care comes first so documentation may be incomplete prompting groups such as CDI to follow up
• Each step in the revenue cycle must review the work of the prior step• Nursing confirms the demographics and account information
• Failure to perform this task could result in the wrong patient information being used in the care of the patient (i.e. allergy concern)

Internal Controls Necessary with People
• Each step in the revenue cycle must review the work of the prior step• Clinical revenue cycle will review documentation provided in the
record by the nursing and professional staff
• Clinical revenue cycle will need to be completed before moving on to HIM coding
• For each action step in the revenue cycle an internal control point must follow in which that step is reviewed PRIOR to moving to the next phase
• Ex: Pilots have a checklist – if one thing on the list is missed they start the checklist all over again

People – Process & Technology

The Revenue Cycle Interdependencies
People
ProcessTechnology

Process
• People require structure to reach the same objective no matter how they approach it
• Process(es) such as policies and procedure provide these structures
• Patient Access:• Processes such as policies and procedures for eligibility check,
authorizations
• Processes to confirm that the patient identification is confirmed to prevent medical errors further downstream
• Key to any process is a policy and procedure

Process is comprised of policy and procedures
Consistent application and
outcomes
Procedure
Policy

Policies and Procedures
• The policy and procedure acts as a standard for which to measure the outcome• Policy is higher level and provides guidance
▪ Webster states: ▪ “a definite course or method of action selected from among alternatives and in
light of given conditions to guide and determine present and future decisions
▪ b : a high-level overall plan embracing the general goals and acceptable procedures especially of a governmental body”
• Policy sets the “standard” and provides the benchmark from which to measure the success of the process
• Key to auditing and internal controls

Charge Capture Audithttps://vitalware.com/resources/articles/how-to-design-a-hospital-charge-capture-audit

Policy Example
Policy: Point of Service Cash Collection• Point of service collection is a patient friendly method as defined by
HFMA to ensure that collections occur as early in the revenue cycle as possible
• Point of service collections decrease post service costs to collect
• Point of service cash collection shall occur at the time of registration or arrival for surgical service
• This should include all acceptable copayments, deductibles or portion of a self pay requirement
• Daily POS cash should strive for 98% or greater based on the services rendered at that location.
• All patient access staff are accountable for following this policy and any associated procedures

Policy Example
• Point of Service Cash Collection▪ NAHAM has a number of point of service cash collection examples
▪ These provide a national guidance on best practice opportunities for cash collections.
• Auditing POS Cash will use the audit cycle against the policy and the findings to determine if in fact the process works or requires additional intervention

Policy Example - Emergency
POLICY:
• In 2008, under the Outpatient Prospective Payment System, CMS stated the following guidelines for charging and billing Evaluation and Management Levels within the ED. Our policy is to follow these guidelines and ensure that all of the points specified are documented within the medical record and the level assigned will be commensurate with the guidelines stated by CMS. The following CMS guidelines will be followed for all facility level E & M in the Emergency Department and for all payors within the Health system.
• “In the absence of national guidelines, we will continue to regularly reevaluate patterns of hospital outpatient visit reporting at varying levels of disaggregation below the national level to ensure that hospitals continued to bill appropriately and differentially for these services. In addition, we note our expectation that hospitals’ internal guidelines would comport with the principles listed below.
• The coding guidelines should follow the intent of the CPT code descriptor in that the guidelines should be designed to reasonably relate the intensity of hospital resources to the different levels of effort represented by the code (65 FR 18451).
Charge Capture Process
• Policies and procedures that are key to the process of charge capture would include, not limited to:• Medical necessity
• Charge capture
• Charge reconciliation
• Documentation (inpatient and outpatient)• Input from CDI and coding

Policy Driven Charge Capture Process

People – Process & Technology

The Revenue Cycle Interdependencies
People
ProcessTechnology

Technology
• Technology is the last of the 3 interdependencies
• This is the piece that performs in a predictable and sustained fashion without variance
• Unlike people and process, technology only performs as it is told to do or designed to do
• It is essential that technology NOT drive the process but have the process designed to incorporate the benefits of technology• If processes are created just to make the technology work then likely
the process will not be sustained.

Types of Technology
• Technology can be divided into a couple pillars• CDM / Chargmaster Maintenance
• One source knowledge centers to look up and obtain current coding and regulatory data
• Rules or AI based charge capture technology• Stand alone technology
• Stand alone technology supplemented by seasoned consultants
• Technology in which daily reports of aberrancies are reviewed by certified auditors.
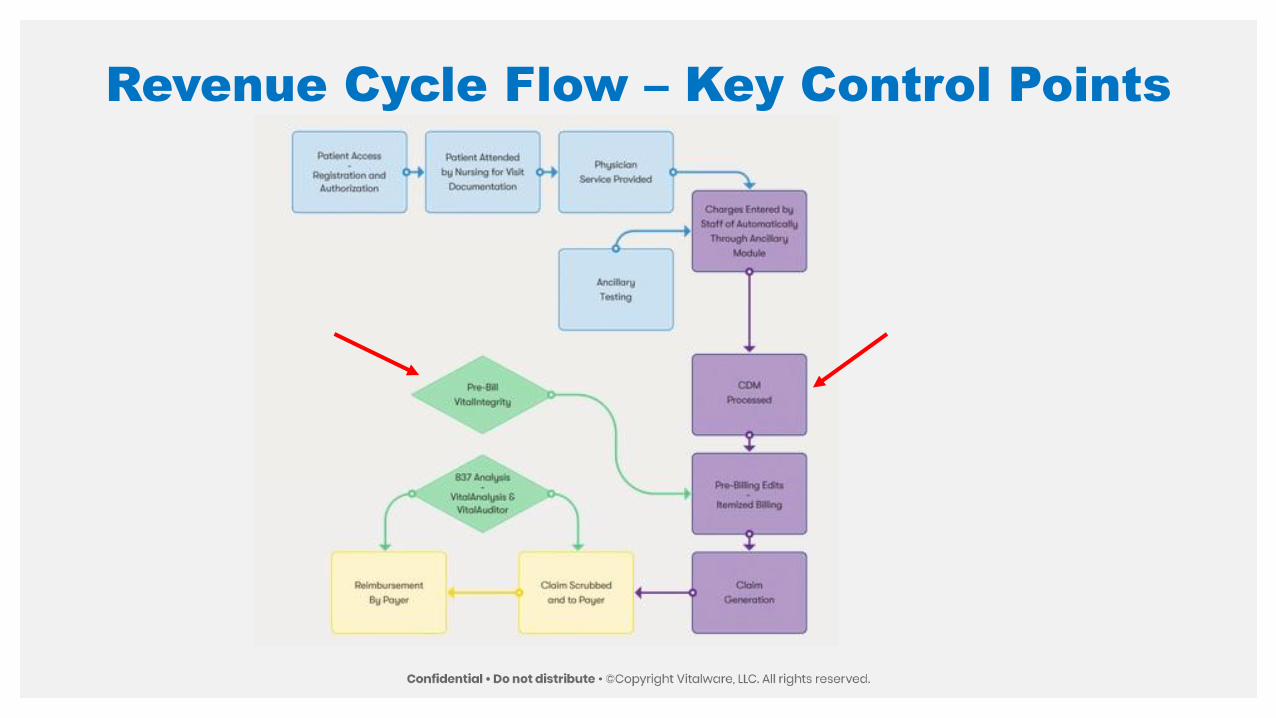
Revenue Cycle Flow – Key Control Points

CDM – Internal Control Point
• CDM is the first line of defense for charge capture
• In the 2005 Supplemental OIG Guidance for Hospitals, they indicated that a poorly maintained CDM could lead to patterns of charge capture over / under charges• “Outdated CDMs create significant compliance risk for hospitals.
Because the Healthcare Common Procedure Coding System (HCPCS) codes and APCs are updated regularly, hospitals should pay particular attention to the task of updating the CDM to ensure the assignment of correct codes to outpatient claims. This should include timely updates, proper use of modifiers, and correct associations between procedure codes and revenue codes.”

CDM – Internal Control Point
• The CDM software maintains the chargemaster in a more compliant state by scrubbing it at regular intervals.• Outdated codes
• Deleted codes
• Pricing disparities
• Many different organizations, including CMS make the CDM public therefore errors could be made public
• Risk areas continue to be high volume area such as:• Pharmacy
• Supply Chain
• Operating Room Service

Technology and Risk Areas
• Operating Room Services• Preference cards are a know cause of charging errors
• Preference cards not reconciled with the CDM may create “in lieu” of charging where the preference selection charges an item but it is not linked to the correct item in the CDM
• Charges for items never used – charging by exception can charge for the whole list when many were never utilized or documented creating a charge error

Technology and Risk Areas
• Supply Chain• Technology should be used to compare Make, Model, Manufacturer
to HCPCS code assignments
• Example: Vitalware frequently finds that non-vascular ablation catheters (GI) are coded as vascular ablation catheters
• Example: Frequently find pacemakers using the inaccurate HCPCS Code
• Pharmacy• CDM frequently contains J codes for oral medications where the J
code is simply for injectable version
• Find inaccurate multiplier in the CDM converting dispensing dose to HCPCS billing unit

CDM – Technology but People and Process
• CDM management tool is as successful as the people and the policies / procedures that guide the process
• For this reason, even with technology an outside review is encouraged at specific intervals to ensure that the CDM is 100% accurate and complete
• CDM must have personnel that are familiar and embody the processes consistent with the clinical operations• Ex: The CDM person should know about the clinical operations of the
ED with understanding of the documentation process and IT document driven charges and how they connect with CDM and ultimately appear on a claim

Charge Capture Technology
• Many vendors have charge capture technology• Consignment based – pay for what is found but no desire of vendor to
fix the concerns found
• Non-consignment / subscription based – pay flat fee and there is no charge per finding.
• Charge capture technology must consume 100% of the daily charges• Rules based is the standard of the industry
• These rules are based on national standards of targets and triggers with combinations that can create a million combinations

Targets and Triggers
• Trigger is a CPT/HCPCS/ICD-10CM or ICD-10PCS code that appears on the claim that looks for a specific target that it needs to match to
• If the Target is missing from the claim, but is expected to be there based on the Trigger. If the Target is missing then the rule fires.
• In many cases the combination is multiple triggers and multiple targets creating a many-to-many review of the charges to ensure completeness

Ex: Amniotic Membrane Missing Device
TargetTrigger(s)

Technology Supports People & Process
People and Process are the
foundation
Build the technology around
the foundation
Amend the new people-process-
technology to ensure optimal
benefit
Re-educate constantly to
ensure alignment

Technology Benefits
• Technology allows for constant auditing of charges to minimize charge leakage and maximize compliance
• The result will be enhanced complete clean claim
• Revenue Integrity teams can they “slice and dice” by service area, high dollar, high volume, gross, directionally correct net, prior area of concern and many more options.
• Patterns of behavior are identified easily
• Promotes root cause analysis and remediation and not just continue to work the same error day by day

Example: Service Area Summary

High Dollar / High Volume
• High Dollar:• In the prior slide we note that one case where the charge stands out
at $23,534.
• An auditor will need to address this particular concern with the goal of a complete clean claim being submitted
• High Volume:• In the prior slide we not that 112 of these were attributed to IV therapy
• This could indicate a pattern of behavior
• The team needs to investigate why there are 112 of these – is it a system created issue, documentation issue, coding issue.
• By using the six sigma technique of 5 Why’s this could be identified• https://sixsigmapool.com/5-whys-analysis/

Summary

Summary
• Current and future trends will depend upon alleviating silos and focusing on the interdependencies of People-Process and Technology
• With continuing focus on decrease revenue these new processes will have to encompass cost management as well• Supply chain offers significant opportunities and cost management in
the supply chain is a trend that is likely going to continue
• Facilities tend to run from “fire to fire” and frequently don’t complete the full implementation

• Integrating technology (CDM / Charge Capture) into processes and people management will allow for sustainable outcomes• Allows for consumption of 100% of daily charges
• Identifies patterns that can create lost charges
• Enhance compliance by making compliance more transparent and hep to demonstrate where medical necessity may be required
• Key Takeaway – sustainable processes involving skilled personnel and state of the art technology for a best of breed outcome.































