Embed Size (px)
Citation preview
Social Science & Medicine 59 (2004) 377–387
ARTICLE IN PRESS
*Tel.: +45-3
E-mail addr
0277-9536/$ - se
doi:10.1016/j.so
The health-promoting family: a conceptual framework forfuture research
Dr. Pia Christensen*
The National Institute of Public Health, Svanem^llevej 25, 2100 Copenhagen Ø, Denmark
Abstract
There has so far only been little research attention given to how families actively engage in promoting their health in
everyday life. In this paper a theoretical framework is proposed for studies of the ‘health-promoting family’ with
particular focus on children’s health and well-being. This paper sets out a conceptual model for understanding how the
family can play a part in promoting both the health of children and children’s capacities as health-promoting actors. It
draws on contemporary social science approaches to health, the family and children, suggesting a new emphasis on the
family’s ecocultural pathway, family practices and the child as a health-promoting actor.
r 2003 Elsevier Ltd. All rights reserved.
Keywords: Family health; Child health; Health promotion; Health-promoting family
Introduction
This paper addresses what has remained a somewhat
neglected area: how, in their everyday life, families
engage in promoting the health of their members
(Sindal, 1997). To date only a small amount of research
has been directly concerned with how family members
(including children) actively engage in promoting,
developing and sustaining their health (Hogg, Barker,
& McGuire, 1996). My aim is to present a theoretical
model for future studies of the ‘health-promoting family’
with particular focus on children’s health and well-
being. This paper will be restricted to discussion of the
main theoretical components for such a model, thus
identifying a framework within which future methodo-
logical and empirical work can be located.
The health-promoting family
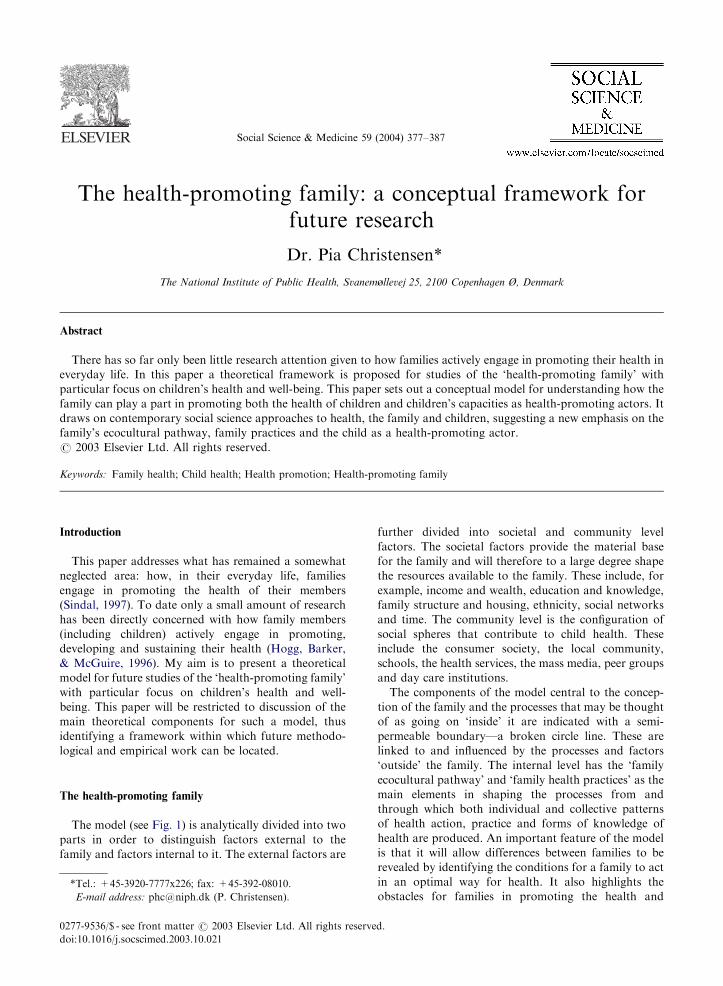
The model (see Fig. 1) is analytically divided into two
parts in order to distinguish factors external to the
family and factors internal to it. The external factors are
920-7777x226; fax: +45-392-08010.
ess: [email protected] (P. Christensen).
e front matter r 2003 Elsevier Ltd. All rights reserve
cscimed.2003.10.021
further divided into societal and community level
factors. The societal factors provide the material base
for the family and will therefore to a large degree shape
the resources available to the family. These include, for
example, income and wealth, education and knowledge,
family structure and housing, ethnicity, social networks
and time. The community level is the configuration of
social spheres that contribute to child health. These
include the consumer society, the local community,
schools, the health services, the mass media, peer groups
and day care institutions.
The components of the model central to the concep-
tion of the family and the processes that may be thought
of as going on ‘inside’ it are indicated with a semi-
permeable boundary—a broken circle line. These are
linked to and influenced by the processes and factors
‘outside’ the family. The internal level has the ‘family
ecocultural pathway’ and ‘family health practices’ as the
main elements in shaping the processes from and
through which both individual and collective patterns
of health action, practice and forms of knowledge of
health are produced. An important feature of the model
is that it will allow differences between families to be
revealed by identifying the conditions for a family to act
in an optimal way for health. It also highlights the
obstacles for families in promoting the health and
d.

ARTICLE IN PRESS
Fig. 1. Model of the health-promoting family.
P. Christensen / Social Science & Medicine 59 (2004) 377–387378
well-being of children and the barriers to enabling the
child’s development as a health-promoting actor during
their growing up.
At the centre of the model, and a primary concern of
research, are the health practices of the family. By this is
meant all those activities of everyday life that shape and
influence the health of family members. These include
the traditional health practices around food and healthy
eating, physical activity, alcohol and smoking, care and
connection, and in addition other key factors that can be
shown to affect young people’s health and well-being.
WHO (2001) suggested five factors important to young
people’s health. These include: meaningful relationships
with adults and peers; parental structure and boundaries
for behaviours; encouragement of self-expression; op-
portunities for participation with their contributions
being valued; educational, economic and social oppor-
tunities and minimal risk of injury, exploitation, or
disease. Childhood research supports these findings
whilst stressing children’s own experiences, perspectives
and actions. For example, Christensen (1998) suggests
that children wish for families in which they have
opportunities to participate in everyday life, and in
which they feel that they are able to contribute
to and manage their own health and well being, as well
as that of other family members. De Winther, Baerveldt,
and Kooistra (1999) have argued that ‘child participa-
tion’ needs to be linked with ‘enablement’. They argue
for the importance of gaining meaningful social
experiences (e.g. at school and in their neighbourhood)
for children to develop the self-respect and social
competence that allows them to work better for their
own health and well-being. Important work by Burton
(Skinner, Burton, & Manlove, 2000) points out the value
of ‘mattering’ for children, the experience that they
matter to other people, and Christensen (2002) has
highlighted the importance of ‘someone being there for
you’ for children and young people in their relationships
with parents and friends. Work on children and risk (for
example, Green, 1997) suggests putting an emphasis on
‘risk management’ as well as risk behaviour, acknowl-
edging how children and young people (including their
families) actively balance and handle different risks in
their everyday life.
The model suggested in this paper focuses on the
health of children. It suggests two main outcomes of the
health-promoting practices of families: the health status
of children (as measured, for example, by morbidity
rates); and the child as a health-promoting actor. Whilst
child health status is a traditional outcome measure of
health research, the idea of the child as a health-
promoting actor is new. The model suggests that the

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387 379
degree to which children act in ways that promote (or
demote) their own health is an important aspect of
family life. It suggests that children should be seen as
actors in their own right and that research should ask
how children become involved in and, indeed, pro-active
in health practices during growing up.
This is currently work in progress and for the scope of
this paper only the main elements of the child as a
health-promoting actor are indicated here. For the child
to develop independent agency in relation to their own
(and others) health and well-being the key aspects
suggested are: self care (physically, emotionally and
socially), personal care and hygiene, keeping fit and
active (physically and mentally), developing and main-
taining connections (including relations of care, respon-
sibility and obligation) with parents and peers,
balancing and managing everyday risks, developing
knowledge and health-related skills and competencies,
developing positive values and meaningful goals for own
health, well being and health behaviours, and the ability
to consult and use health care services.
The ecocultural pathway
The model suggests a way of looking at family health
practices within the broad range of activities that
families engage in. This part of the model is referred
to as ‘the family ecocultural pathway’. This concept is
drawn from Weisner and his colleagues and is a method
of conceptualising the ways in which families engage
with and utilise the resources at their disposal (see, for
example, Weisner, 1998, 1996; Gallimore, Weisner,
Kaufman, & Bernheimer, 1989). The ecocultural ap-
proach suggests that families have their own goals and
values that they pursue through their daily routines.
Through daily practices and activities they may be more
or less successful in meeting their goals. These goals may
or may not include health or may balance health against
other goals. However the daily routines followed by
families have implications for the health of each family
member. Some families will follow routines that to a
greater extent than other families will support their
health and well being. This ecocultural approach is an
important step forward in looking at family health.
Instead of being concerned to link health to different
types of family (e.g. one or two parent families), it rather
concentrates on what families actually do in their
everyday life—their practices. The ecocultural pathway
includes all the family goals, values and practices and
thus forms the broad milieu within which health
practices take place. Health-related practices are there-
fore only a part of the picture and have to be understood
in this broader context. Families have to balance the
individual and shared goals and needs of family
members with health and well being, and integrate these
in the overall goals of the family. For example, the
business of earning a living may influence diet or
exercise.
Influences on the family
Of course families in different socio-economic situa-
tions have very different resources at their disposal and
this may also result in different ecocultural pathways.
To a large degree socio-economic position may shape
the resources available to the family, including, for
example, income and wealth, education and knowledge,
social networks, time, and emotional energy. Thus
factors such as occupation and whether the family has
one or two working parents are important in determin-
ing the level of resources available. However, it is also
crucial to look at how the family makes use of the
resources available to them and how this forms part of
their cultural pathway to health. Different families
construct their ecocultural pathway in different ways,
even though their socio-economic situation may be
similar. It is important therefore to look at both the
resources available to families and how families handle
these resources—that is how they construct their
ecocultural pathway. This ecocultural pathway thus acts
as a mediator between family health practice and the
socio-economic position of the family. Another factor
that shapes family health practices is their history across
generations. A child’s health status is also determined by
the child and family history of health and illness and
genetic dispositions of the parents. The model therefore
also draws attention to the importance of investigating
the family history of health practices, for example family
eating patterns, involvement in physical activity, atti-
tudes to health services and so on. Finally, there is a host
of community spheres that influence and shape chil-
dren’s health. These include the consumer society, the
local community, schools, the health services, the mass
media, peer groups and day care institutions. These
enter into family life in two ways. Sometimes they are
mediated through parents but in contemporary society
children also have independent access to such spheres.
These may be important also in their peer relationships.
Overall then this model sets out a way of looking at
the family as a health-promoting environment. In the
following section I will further develop its theoretical
underpinnings.
Health promotion and the family
I take as my starting point the problem identified in
more recent studies of child health. This is the tendency
of conventional approaches to child health to focus on
negative rather than positive factors and outcomes for
children and young people’s health and well-being. De

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387380
Winther (1997) argues that concerns about the well-
being of children over time have given prominence to
explanations of causality on an individual rather than on
a societal level. This is coupled with seeking to identify
health-damaging effects and negative outcomes for
children rather than identifying those factors that
promote their health or reduce the risk of negative
outcomes. A number of researchers have made similar
calls for the need to uncover positive indicators of child
well-being and place these alongside the medical and
epidemiological questions about child health outcomes.
Ben-Arieh and Wintersberger (1997) and Zubrick,
Silburn, Vimpani, and Williams (1999), for example
argue for the importance of an ecological perspective
that take into account factors operating within the
family household and the neighbourhood as well as
those operating on a broader societal level. In relation to
this debate Barnes (2001) argues that research needs to
develop indicators that relate to children’s well-being in
the present. This in turn will allow children’s own
subjective experiences of well-being to be reflected in the
development and shaping of the concepts that are used
to measure their well-being.
This issue is salient to the broader debate within
health promotion about whether health should be
defined negatively or positively. An important distinction
has to be drawn between disease prevention and health
promotion (Breslow, 1999). Health debates have been
marked by both of these dimensions, especially in relation
to the WHO’s broad definition of health (WHO, 1986).
Over the years this definition has been marked by a pull
and push effect that has taken various forms and reflected
different interests. The importance of a positive approach
to health is now generally recognised and it is given a
prominent position in current thinking. Breslow (1999)
has very importantly suggested the need to pay particular
attention to the Ottawa Charter’s explicit definition of
health as a resource for everyday life, and consequently
the need to shift the focus of health-promoting strategies
to ‘capacity building for health’ He argues:
To reach the full potential of living, it is becoming
clear the specific capacities must be developed and
maintained. This is clearly beyond disease prevention
and illustrates the importance of considering the
nature of health promotion (Breslow, 1999, p. 1031).
The notion of ‘the health-promoting family’ can be
usefully understood within Breslow’s advocacy of the
idea of ‘capacity building for health’. Whilst parents are
not the only ones involved in building children’s
capacity for health, they are nevertheless key mediators
in the process. In understanding the health-promoting
family it will, therefore, be important to identify the
factors that act as key resources in child health. This
involves looking at the health-related practices of
parents as they are embedded in their everyday life. It
also involves working through how children engage in
their own health and well-being, how they develop the
skills that enable them to do so, and how children
contribute to the health and well-being of their family
and others to whom they socially relate. Taken together
this approach would explore the environment in which
children live, looking at the base it forms for their health
choices and also, perhaps, how it may be improved and
changed (cf. Kickbusch, 2002), to take into account
children’s perspectives and active participation in their
own and their family’s health.
The family
The family and family life has long been recognised as
a complex historical, social and cultural phenomenon.
As a context defining a multiple set of everyday living
arrangements and different ways of organising personal
intimate relationships, the trend in family studies has
been away from the use of the family as a generic term
towards more fluid conceptualisations of the family (e.g.
Holland, Mauthner, & Sharpe, 1996; Carsten, 1998;
Simpson 1998; Cheal, 2002). This is of importance when
considering the family as a health-promoting environ-
ment. In an in-depth study of the nature of, and
processes involved in, the communication of health
messages to and within families Holland, et al. (1996,
p. 83) conclude that:
The family is clearly a complex site for the reception,
transmission and communication of health informa-
tion...individual health beliefs and health-related
behaviour are related to a number of factors related
to family life.
They suggest that these determining factors include
family structure, employment patterns, gender and age
role differences, the stage of parenting, family dynamics
and parenting styles, communication patterns, power
relations and decision-making processes.
Their findings suggest that understandings of the
health-promoting family must work with a concept of
the family that can handle great complexity and
diversity. Recent developments within the sociology of
the family have taken up the challenge both of
representing greater family complexity and employing
wider notions of what the family is. They do this by
focusing more attention on what families actually do
(Cheal, 2002; Silva & Smart, 1997). This can be
contrasted to previous research that has centred mainly
on two approaches: family structure and family func-
tions. The structural approach led to identifying
different ‘types’ of family defined by social positions or
roles. A family structure is typically defined by who the
family members are and by their relationship to each

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387 381
other, for example in terms of marriage and parenthood
(Cheal, 2002, p. 7). However this approach cannot
account very well for the activities that family members
do together, or for the meanings and results of these
activities. The second approach, by focusing on family
functions, offered a way of looking at the activities that
families do together in order to meet their needs within a
context of assumed mutual responsibility. Within this
approach family functions could be based on externally
observed and defined activities, such as involvement in
food production, distribution and consumption or in the
care of children or elderly family members. However,
this approach tended to stress the positive benefits of
families (that is what people do together and especially
what they do to support each other), but left more or
less unanswered questions about why not all families
function well (ibid).
Recognition of the shortcomings of both the structur-
al and functional approaches to the family signalled an
important step forward for the study of the family: the
move toward studying the interactions and transactions
of family life through the study of family practices
(Morgan, 1996, 1997). The family is no longer to be
conceived of as a static or concrete social unit. The
notion of family practices carries with it a sense of
‘action’ and ‘doing’ rooted in the everyday. In their
everyday character these practices also carry a sense of
regularity and repetition. Family practices are linked to
wider notions of parenthood, kinship and marriage and
the expectations and obligations associated with these.
They link history and biography because practices are
historically constituted and shaped at the same time as
they are woven into and constituted from elements of
individual biographies (Mills, 1959, in Morgan, 1996).
This theoretical approach is a very promising one for
the study of family and child health (1). One especially
useful way of focusing on family practices is provided by
the ‘ecocultural’ view of the family developed by
Weisner and colleagues in USA. This is designed as a
flexible tool for understanding a wide range of different
family circumstances in different social and cultural
settings. At its heart is a concern with everyday routines:
‘Cultural pathways are made up of everyday routines
of life and routines are made up of cultural activities
(bedtime, playing video games, home work, watching
TV, cooking dinner, etc.). Activities are useful units for
cultural analysis because they are meaningful units for
parents and children to understand, they are amenable
to ethnographic fieldwork, systematic observation and
interviewing methods. They are what children and
adults experience and they crystallize the important
aspects of culture’ (Weisner 2002, p. 276).
The ecocultural approach places a strong emphasis on
how families sustain their everyday routines. It therefore
asks in detail how the resources available to families and
the constraints and opportunities faced by families are
managed and how they contribute to sustainability. It
suggests that three factors are especially important. The
first is termed ‘ecological fit’. It refers to the relationship
of the family to important matters such as earning a
living, neighbourhood safety and transportation, etc. It
recognises the effect that each of these can have on
aiding or disrupting the daily routines of a family and
the goals they are pursuing through them. It draws
particular attention to how families are able to balance
issues of income, neighbourhood, transport etc. with the
effort of sustaining their daily routines. The second
factor is termed ‘meaningfulness’. This refers to the
moral and cultural significance of the daily routines to
the family members. If these ‘make sense’ and are valued
by family members, this helps them to sustain routine
everyday activities. Finally, there is a factor termed
‘congruence’. This refers to the balance between the needs
and goals of family members. If there is congruence then
they will be met not completely but sufficiently. No one
person’s needs will dominate the others (2).
It is notable that this approach to the family is very
compatible with the idea of health as a resource for
living. Health practices are woven into the everyday life
of families as they try and establish sustainable routines.
In the flow of everyday life, health practices may or may
not be separated out as distinct, however, from a
research viewpoint it is necessary to foreground health
practices analytically whilst simultaneously recognising
that they are woven into family routines. This allows for
recognition that, for example, some families may be able
to establish routines that allow for the successful
integration of health practices and goals into their
everyday life. However, health may also come into
conflict with other goals and needs. For example, getting
the material resources needed for the family may disrupt
everyday health practices.
This approach, then, enables a detailed view of the
processes involved in promoting health in families
because it assumes that all families, whatever their
background or circumstances, can be involved in health-
promoting activities. This takes an important step away
from the conventional emphasis on family type and
notions of the ‘problem family’. It allows a focus on the
dynamics and family practices, asking whether they
promote or hinder the development of good health and
well-being in children. This is underscored by a concern
with children’s own part in shaping themselves as
health-promoting actors. It is of course expected that
families with fewer resources (biologically, socially,
culturally and materially) may have the most difficulties
or obstacles in achieving and sustaining health and well-
being for its members. However, the approach taken
allows the health practices of the family to be
analytically separated from the issue of resources (3).
Furthermore, within this approach the notion of the
family ceases to be seen as a bounded unit and is

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387382
recognised as constituted not only through sets of
ongoing relations between family members—through
internal connections—but also through connections
external to the family. These are the social relations
that cut across the family and connect its members to
work, school and other social and material settings.
Both adults and children (women and men, boys and
girls) establish such networks of connections. The
importance of connections across these boundaries was
shown in a study of farming families in the UK
(Christensen, Hockey, & James, 1997, 1998). Men and
women drew up the boundaries of family and commu-
nity in different ways. This revealed a complexity
around the relation between self, family and community
that became articulated at times of family crisis such as
the onset of illness. This perspective proved an
important one to understand the ways in which families
provide help and support in case of illness.
Health socialisation and the place of children
During industrialisation (1800–1900) the notion of
child socialisation changed dramatically. Childhood
became constituted through notions of the intimate
and private sphere of the family and ideas about the
importance of children’s learning and nurturing. Mod-
ern childhood was constituted through the formation of
specific social worlds, such as the way motherhood
pivoted around the dyadic relationship between mother
and child during infancy. It also included the separation
of play, school and work and the exclusion of children
from the work force (Alanen, 1988). Childhood became
a quarantine period when particular protective care was
necessary. Since the child was seen as not yet part of
society he/she was on the receiving end of care, learning
and protection. Emergent notions of this new social
world developed into a number of practices and schemes
to monitor child health and well-being, childcare and
Fig. 2. The social settings involved in children’s
training. This involved the development of particular
professional expertises in relation to children, such as in
the emergence of pediatrics (Armstrong, 1983). At the
same time the family became a key social institution in
society with the primary task of undertaking the proper
development and sustenance of both child and parental
health and well-being (Crawford, 1994). This gave
emphasis to the importance of primary socialisation
and the transmission of health knowledge and behaviour
from the mother (or parents) to the child. This
positioned mothers as especially responsible in provid-
ing for the child. At the same time childhood was
characterised by relations of dependency, constituting
children as the more or less passive recipients of care.
In contemporary, post-industrial times socialisation
theories have shifted, stressing the interactive character
of the socialisation process. This constitutes the child as
developing through active engagement with the
health knowledge and actions of adults. The increased
institutionalisation of modern childhood, which has
taken place over the last decades, has led to the
recognition of the school and other day care institutions
as contributing to children’s health and well-being
through the stake that educators and pedagogues have
in the socialisation of children. However, as recent
detailed research has shown, the discrepancies between
health socialisation practices at home and those at
school have important implications for children’s
acquisition of self-care practices (Mayall, 1993, 1996).
What goes on in one context is not necessarily carried
over and built on in the other, and vice versa. More
recently, children’s health has been recognised as a
plural construct, produced at the interface between the
child, family, friendships and peer groups, school, day-
care institution, media (especially TV), the consumer
society, and health care services (see Fig. 2). This
interplay of many different social actors and contexts
creates a health universe of competing values and
standards that renders outmoded the idea of a one-
development as health-promoting actors.

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387 383
way transmission of health, practices and values. This
underlines the idea that contemporary societies require
children to create meanings for themselves.
Although the family can still be seen as central, when
it comes to health more recent research has emphasised
the pluralistic character of children’s health. As a
consequence the view of children as primarily dependent
in the different contexts of their everyday life such as
that of the family, school and after school institution is
changing (Corsaro, 1997). Recent important work
within health promotion is exploring new directions
for child health practice and policy through adopting the
notion of the social ecology of child health and well-
being. This refers to the nested arrangement of family,
school, neighbourhood and community contexts (Earls
& Carlson, 2001).
Children and young people are growing up in a
society undergoing great change. This has created
environments where they meet with many different and
often contradictory health and life quality values and
practices. Parents cease, therefore, to be regarded as
having the only, or perhaps even the primary, influence
on children’s health and successful development in
youth. Of course parents retain a central role in
providing care and support, and in strengthening and
monitoring children/young people in their growing up.
However, the interactive and pluralistic character of
health means that children have in a larger measure than
before to create meaning for themselves and to develop
their own positive health practices. In this process
parents may now be seen as very important mediators in
children’s health actions rather than being seen as
having the main direct influence upon them.
Shifting perspectives on children and child health
When considering the move towards understanding
the child as an health-promoting actor we are dealing
not only with understanding how children’s socialisation
take place but also with how children are seen.
Traditionally in child health research the perspective
has been to understand the child as an object, that is as a
person acted upon by others and broadly shaped by
influences in its social and material environment, rather
than as a subject acting in the world (Kalnins, McQueen,
Backett, Curtice & Currie, 1992; Christensen, 1998;
Woodhead & Faulkner, 2000). This notion of the child is
still widely persuasive in studies that see child health and
well-being primarily as an outcome of external influ-
ences, including genetic disposition/composition, passive
socialisation and specific structural factors.
This approach emphasises children’s dependency in
their relations with adults and renders them relatively
passive in relation to external influences. The tendency
to neglect children’s own experiences, understandings
and actions, and the failure to see children as social
persons in their own right, has led to an emphasis on
what could be called an ‘‘adultist’’ perspective in child
health research (Ridge, 2002). In the first place, this has
emphasised the key role of adults in children’s health.
Although research has argued for the greater scope in
recognising children’s agency and subjectivity in health,
children are primarily seen as modelling parental
behaviour (Jackson & Henriksen, 1997). Real agency
in health has been delegated to responsible adults and is
closely associated with parental roles. As primary
models for their children, it is mothers’ health status,
beliefs, behaviour and practices that are usually linked
with those of the child. This may be extended to include
other significant adults (such as fathers and teachers)
who through their engagement and care are designated
as active, responsible agents. Adults status, and in
particular the parental child/adult relationship, is seen in
normal circumstances as the guarantor of children’s
health and welfare. Indeed parenting has been identified
as the single largest variable implicated in childhood
illnesses and child accidents. Much important work
investigating the impact of risk factors on children’s
academic and psychological functioning (Rutter, 1979;
Sameroff, Bartko, Baldwin, Baldwin, & Seifer, 1998) has
shown that it is a number of risk factors that best
explains individual differences in children’s develop-
mental outcomes, i.e. it is the cumulative effect rather
than the unique effects of any particular factor.
Second, this ‘adult’ view is reflected in the epidemio-
logical concern with child health as a precursor to the
future general health of the population. Renewed
interest in a life-course perspective on health thus
recognises human health as shaped over time through
genetic factors, family, socio-economic and material
living conditions and personal lifestyles (Barker, 1992;
Ross & Wu, 1995; Power & Hertzman, 1997; Lynch,
Kaplan, & Salonen, 1997). In this vein the health
characteristics of childhood are employed as statistically
predictive of adult health (McCarthy, 2002), just as
paternal living conditions and lifestyle can be shown
statistically predictive of the health of the next genera-
tion. The prenatal period is seen to play an important
role in diseases being clinically detected later in life.
Research findings published during the last decade
suggest the scope for exploring such links in more detail
(Kuh & Ben-Shlomo, 1997; Ben-Shlomo & Kuh 2002;
Berkman & Kawachi, 2000).
However, in this perspective children’s health and
well-being appear primarily as serving the need to
understand the natural course of adult illness better.
Whilst this clearly expresses a legitimate concern with
the future health of children as adults, it draws attention
away from the value of children’s health and well being
for children—as living in the present and in their
transitions from childhood to adulthood. Indeed the
implications of specific factors for children’s health in

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387384
the present are met with the argument that these may be
serious in themselves but are even more important as
precursors of problems in adulthood and for the next
generation (see, for example, Hoghughi, 1998; Kolvin,
Muller, Scott, Gatzanis, & Fleeting, 1990).
This problem is reflected in the conventional focus on
young people’s risk-behaviour and is highlighted by the
rather sparse literature on the health, well-being and
health behaviours of middle childhood. This conven-
tional focus neglects children and young people’s
positive health behaviours and fails to recognise them
as a base which could be built upon by health
promotion. The potential for this approach is shown
in Nichter’s (2000) large scale, in-depth study of
American teen-age girls and dieting. She argues that
health promotion needs to support the strategies that the
girls employ for maintaining their health in the present
and suggests that this will be conducive to long term
success. For example, she suggests that the girls’ idea of
‘watching what you eat’ forms a positive counter to the
dieting messages and programmes that dominate the
media.
A third problem flowing from seeing children as
objects rather than subjects is the over-reliance in
research on objective measures of child health. Too
little attention is paid to the processes that lie behind the
statistical associations found. Research evidence shows
that it is necessary to look at children’s own active role
in forming and shaping their lives. For example, Joshi,
Cooksey, Wiggins, McCullock, Verropoulou, and
Clarke (1999) have recently argued that a reliance on
the statistical analysis of longitudinal data is insufficient
for an understanding of why some children do well and
some do badly even when the social and economic
circumstances of their lives are very similar. In their
study Joshi and colleagues wished to quantify the impact
of changing family forms of Britain through investigat-
ing their outcome for children’s development and well-
being. The study used longitudinal data on children aged
5–17 years old. A particular focus was how children
living in families with a single parent compared to
households with two parents. The researchers did find
significant difference on several dimensions of children’s
well-being when they made a crude comparison between
children who lived with both their biological parents and
children living in other family arrangements. However
the relationship between family type, housing and
children’s well being was mediated in complex ways by
levels of human, economic and social capital. For
example, low income was one of the most powerful
associations with children doing badly. But low income
was both a precursor to and a consequence of marital
breakdown (and thus of children not living with both
their biological parents).
Furthermore, the research found great variations
within the same family types. Some children seemed to
be badly affected by family breakdown but many were
not. The researchers concluded that although they did
not wish to argue that divorce was a life event that did
not affect children, they warned against conventional
assumptions that children from broken homes are
necessarily vulnerable or victims. They found that
children’s resilience was an important aspect of how
and why some children did well when others were
observed to be more vulnerable even within the same
family. This was an aspect that could not be explained
by the family type that the child lived in (see also
McMunn, Nazroo, Marmot, Boreham, & Goodman,
2001). This latter point indicates the importance of
exploring in more detail the differences among children
and in particular the influence of their own agency for
maintaining their well-being, including the resources
that children who do well are able to draw upon for their
support through hardship and difficulties.
Such a refocusing will undoubtedly require more
qualitative and ethnographic work allied to quantitative
investigation, resulting in a mixed method approach in
child health. For example, much previous research has
both assumed and emphasised the important role of
parents for children’s health, well-being and behaviour.
It thus reflects the main concerns of developmental
research with investment in children (and their prospec-
tive futures) at home, school and in the community
rather than with how children contribute to their
families and communities through ‘the flows of moral
and material capital between the generations from child
to parents as well as parents to children’ (Weisner,
2001). More recent research, in particular ethnographic
and qualitative work, has, however, helped to illuminate
how a focus on children’s specific contributions can
provide important insights into the dynamics of family-
based health and health care (Christensen, 1998; Back-
ett, 1992a). Such studies have begun to demonstrate that
even early in their lives children actively contribute to
health-promoting activities in the family (Backett,
1992a, b; Backett-Milburn, 2000; Brannen & Storey,
1996; Brannen, Heptinstall, & Bhopal 2000), at school
(Prout, 1988; Mayall, Bendelow, Barker, Storey, &
Veltman, 1999; Christensen, 1993, 2000), in contact with
the health care system (Bluebond-Langner, 1978;
Strong, 1979; Davis, 1982) and through health-promot-
ing activities in their local community (Kalnins et al.,
2002; Wallerstein, 2002; Gibbs, Mann, & Mathers,
2002).
Conclusion: the family and the child as health-promoting
actors
This paper presents a theoretical model for under-
standing the ‘health-promoting family’, which is in-
tended to encourage discussion. As a framework for

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387 385
further empirical studies the different elements in the
model and the relationships between them can be
explored, tested and modified. The health-promoting
family can ideally be seen as an ecocultural milieu that
works to promote children’s health, well-being and
development and reduces children’s risk behaviour (cf.
WHO, 2001; Weisner, 1998). I suggest the family can
also be seen as a support for the development of the
child as a health-promoting actor. Children’s
health, well-being and agency in health are treated as
the main outcomes of the model. The child as health-
promoting actor is a concept that requires further
definition and exploration including developing ways
to study and measure it. An important part of research
will involve understanding the child’s active participa-
tion in and level of information and skills in making
health choices in a life-course perspective. This process
needs to be placed within both intergenerational (for
example, parent–child relations) and intra-generational
relationships (children’s relationships with their peers).
Through this it should be possible to trace the
conditions and processes that facilitate (or hinder)
children’s health and health-promoting action in their
families.
Notes
1. This approach does not reject looking at family
structure rather it places family structure as part of
the societal context and focuses especially on the
implications of family type for the economic,
material, cultural and social resources available to a
particular family. Governmental policies about the
family, for example, can have a great influence on
how different family forms are seen and the resources
that are available to them.
2. From this point of view the approach in this paper is
sensitive to the gender division of labour highlighted
by feminist health researches. In particular they point
to an asymmetrical division of labour between men
and women in family health care and a high level of
unpaid health work carried out by women (see
Graham, 1984; Lewin and Olesen, 1985; Stacey,
1988; Charles and Kerr, 1988).
3. This approach will allow for Prout’s (1996)
suggestion in a study of family and household
health that class be treated with attention to
divisions within as well as between social class
groupings, to focus also on class trajectories
and its relationship to cultural habitus rather
than more static notions of class position
and to look at health practices in terms of different
cultural capital and their transmission between
generations.
Acknowledgements
I wish to thank Mette Madsen for her engagement,
enthusiasm and helpful comments on earlier drafts of
this paper. I am indebted to Niels Kristian Rasmussen
for his sharp insights and supportive criticism that
helped me to clarify many ideas in developing the
conceptual model. I also wish to thank Alan Prout for
continual support and contribution to refining the final
version of this paper.
References
Alanen, L. (1988). Rethinking childhood. Acta Sociologica,
31(1), 53–67.
Armstrong, D. (1983). Political anatomy of the body: Medical
knowledge in Britain in the twentieth century. Cambridge:
Cambridge University Press.
Backett, K. (1992a). Studying health in families: A qualitative
approach. In S. Cunningham-Burley, & N. McKeganey
(Eds.), Readings in medical sociology (pp. 57–85). London:
Tavistock.
Backett, K. (1992b). Talking to young children about health:
Methods and findings. Health Education Journal, 50, 34–38.
Backett-Milburn, K. (2000). Parents, children and the con-
struction of the healthy body in middle-class families. In A.
Prout (Ed.), The body, childhood and society (pp. 79–100).
London: Macmillan Press Ltd.
Barnes, H. (2001). How other countries monitor the well-being
of their children. In J. Bradshaw (Ed.), Poverty: The
outcomes for children (pp. 215–239). London: Family Policy
Studies Centre.
Barker, D. J. (1992). Fetal and infant origins of adult disease.
British Medical Journal, 301(6761), 1111.
Ben-Arieh, A., & Wintersberger, H. (1997). Monitoring and
measuring the state of children—beyond survival. Vienna:
European Centre for Social Welfare Policy and Research.
Ben-Shlomo, Y., & Kuh, D. (2002). A life course approach to
chronic disease epidemiology: Conceptual models, empirical
challenges and interdisciplinary perspectives. International
Journal of Epidemiology, 31, 285–293.
Berkman, L., & Kawachi, I. (2000). A historical framework for
social epidemiology. In L. Berkman, & I. Kawachi (Eds.),
Social Epidemiology (pp. 3–12). Oxford: Oxford University
Press.
Bluebond-Langner, M. (1978). The private worlds of dying
children. Princeton, NJ: Princeton University Press.
Brannen, J., Heptinstall, E., & Bhopal, K. (2000). Connecting
children, care and family life in later childhood. London:
RoutledgeFalmer.
Brannen, J., & Storey, P. (1996). Child health in social context.
Health Education Authority Family Health Research Re-
ports. London: Health Education Authority.
Breslow, L. (1999). From disease prevention to health promo-
tion. Journal of American Medical Association, 281(11),
1030–1033.
Carsten, J. (Ed.). (1998). Cultures of relatedness New approaches
to the study of kinship. Cambridge: Cambridge University
Press.

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387386
Charles, N., & Kerr, M. (1988). Women, food and families.
Manchester: Manchester University Press.
Cheal, D. (2002). Sociology of family life. London: Palgrave.
Christensen, P. (1993). The social construction of help among
Danish school children. Sociology of Health and Illness,
15(4), 488–502.
Christensen, P. (1998). Difference and similarity: How chil-
dren’s competence is constituted in illness and its treatment.
In I. Hutchby, & J. Moran-Ellis (Eds.), Children and social
competence: Arenas of action (pp. 187–202). London:
Falmer Press.
Christensen, P. (2000). Childhood and the cultural
constitution of vulnerable bodies. In A. Prout (Ed.), The
body, childhood and society (pp. 38–59). London:
Macmillan Press Ltd.
Christensen, P. (2002). Why more ‘quality time’ is not on the
top of children’s lists. Children and Society, 16, 1–12.
Christensen, P., Hockey, J., & James, A. (1997). You have
neither neighbours nor privacy: On the emotional well-being
of women in a farming community. Sociological Review,
45(4), 621–645.
Christensen, P., Hockey, J., & James, A. (1998). You just get on
with it: Questioning welfare dependency in a rural commu-
nity. In I. Edgar, & A. Russell (Eds.), Anthropology and
welfare (pp. 16–32). London, New York: Routledge.
Corsaro, W. A. (1997). The sociology of childhood. New York:
Sage Publications Inc.
Crawford, R. (1994). The boundaries of self and the unhealthy
other: Reflections on health, culture and AIDS. Social
Science & Medicine, 38(10), 1347–1365.
Davis, A. (1982). Children in clinics. London: Tavistock.
De Winther, M. (1997). Children as citizens: participation and
commitment. Oxford: Radcliffe Medical Press.
De Winther, M., Baerveldt, C., & Kooistra, J. (1999). Enabling
children: Participation as a new perspective on child-health
promotion. Journal of Child Care Health Development,
25(1), 15–23.
Earls, F., & Carlson, M. (2001). The social ecology of child
health and well-being. Annual Review of Public Health, 22,
143–166.
Gallimore, R., Weisner, T. S., Kaufman, S. Z., & Bernheimer,
L. P. (1989). The social construction of ecocultural niches:
Family accommodation of developmentally delayed chil-
dren. American Journal on Mental Retardation, 94(3),
216–230.
Gibbs, S., Mann, G., & Mathers, N. (2002). Child-to-child. A
practical guide: Empowering children as active citizens.
London: Child-to-Child Trust.
Graham, H. (1984). Women, health and the family. Brighton:
Wheatsheaf Books.
Green, J. (1997). Risk and the construction of social identity:
Children’s talk about accidents. Sociology of Health and
Illness, 19(4), 457–479.
Hogg, C., Barker, R., & McGuire, C. (Eds.). (1996). Health
promotion and the family: Messages from four studies.
Health Education Authority Family Health Research Re-
ports. London: Health Education Authority.
Hoghughi, M. (1998). The importance of parenting in child
health. British Medical Journal, 316, 1545.
Holland, J., Mauthner, M., & Sharpe, S. (1996). Family
matters: Communicating health messages in the family.
Health Education Authority Family Health Research Re-
ports. London: Health Education Authority.
Jackson, C., & Henriksen, L. (1997). Do as I say: Parent
smoking, antismoking socialisation, and smoking onset
among children. Journal of Addictive Behaviour, 22(1),
107–114.
Joshi, H., Cooksey, E., Wiggins, D., McCullock, A., Verro-
poulou, G., & Clarke, L. (1999,). Diverse family living
situations and child development: A multilevel analysis
comparing longitudinal evidence from Britain and the
United States. Journal of Law, Policy and the Family, 13,
292–314.
Kalnins, I., Hart, C., Ballantyne, P., Quartaro, G., Love, R.,
Sturis, G., & Pollack, P. (2002). Children’s perceptions of
strategies for resolving community health problems. Health
Promotion International, 17(3), 223–233.
Kalnins, I., McQueen, D., Backett, K., Curtice, L., & Currie, C.
(1992). Children, empowerment and health promotion:
Some new directions in research and practice. Health
Promotion International, 7(1), 53–59.
Kickbusch, I. (2002). Health literacy: A search for new
categories. Health Promotion International, 17(1), 1–2.
Kolvin, I., Muller, F. J., Scott, D., Gatzanis, S., & Fleeting, M.
(1990). Continuities of deprivation: The Newcastle 1000
family study. Avebury: Alderson.
Kuh, D., & Ben-Shlomo, Y. (1997). A life course approah to
chronic disease epidemiology: Tracing the origins of ill-health
from early to adult life. Oxford: Oxford University Press.
Lewin, E., & Olesen, V. (1985). Women, health and
healing: Towards a new perspective. London, New York:
Tavistock.
Lynch, J. W., Kaplan, G. A., & Salonen, J. T. (1997). Why do
poor people behave poorly? Variety in adult health
behaviours and psychological characteristics by stages of
the socio-economic life course. Social Science & Medicine,
44, 809–819.
Mayall, B. (1993). Keeping healthy at home and school: It’s my
body so it’s my job. Sociology of Health and Illness, 15(4),
464–487.
Mayall, B. (1996). Children, health and the social order. Milton
Keynes: Open University Press.
Mayall, B., Bendelow, G., Barker, S., Storey, P., & Veltman,
M. (1999). Children’s health in primary schools. London:
Falmer Press.
McCarthy, M. (2002). Urban development and health
inequalities. Scandinavian Journal of public Health, 30(3),
59–62.
McMunn, A. M., Nazroo, J. Y., Marmot, M. G., Boreham, R.,
& Goodman, R. (2001). Children’s emotional and beha-
vioural well-being and the family environment: Findings
from the Health Survey for England. Social Science &
Medicine, 53(4), 423–440.
Mills, C. W. (1959). The sociological imagination. Oxford:
Oxford University Press.
Morgan, D. (1996). Family connections: An introduction to
family studies. Cambridge: Polity Press.
Morgan, D. (1997). Risk and family practices: Accounting for
change and fluidity in family life. In E. Silva, & C. Smart
(Eds.), The ‘‘new’’ family?, London: Sage.
Nichter, M. (2000). Fat talk: What girls and their parents say
about dieting. Cambridge, MA: Harvard University Press.

ARTICLE IN PRESSP. Christensen / Social Science & Medicine 59 (2004) 377–387 387
Power, C., & Hertzman, C. (1997). Social and biological
pathways linking early life and adult disease. British Medical
Bulletin, 53, 210–222.
Prout, A. (1988). Off school sick: Mothers accounts of school
sickness absence. Sociological Review, 36, 4–28.
Prout, A. (1996). Families, cultural bias and health promotion.
London: Health Education Authority.
Ridge, T. (2002). Childhood poverty and social exclusion: From a
child’s perspective. Bristol: Policy Press.
Ross, C. E., & Wu, C. (1995). Education, age and the
cumulative advantage in health. Journal of Health Social
Behaviour, 37, 104–120.
Rutter, M. (1979). Protective factors in children’s responses to
stress and disadvantage. In M. W. Kent, & J. E. Rolf (Eds.),
Primary prevention and psychopatology. Vol. 3. Social
competence in children (pp. 49–74). Hanover, NH: Uni-
versity Press of New England.
Sameroff, A. J., Bartko, T., Baldwin, A., Baldwin, C., & Seifer,
R. (1998). Family and social influences on the development
of child competence. In M. Lewis, & C. Feiring (Eds.),
Families, risk and competence. Mahwah, NJ: Lawrence
Erlbaum Publishers.
Silva E., & Smart, C. (Ed.) (1997). The ‘‘new’’ family? London:
Sage Publications Ltd.
Simpson, B. (1998). Changing families. An ethnographic
approach to divorce and separation. Oxford: Berg.
Sindal, G. (1997). Health promotion and the family. Health
Promotion International, 12(3), 259–260.
Skinner, D., Burton, L., & Manlove, B. (2000). An ethno-
graphic study of parents constructions of developmental
opportunities in contexts of poverty and disability. Paper
given at ‘Discovering successful pathways in children’s
development: Mixed methods in the study of childhood and
family life’ Conference, Los Angeles, CA.
Stacey, M. (1988). The sociology of health and healing. London:
Unwin Hyman.
Strong, P. (1979). The ceremonial order of the clinic. London:
Routledge and Kegan Paul.
Wallerstein, N. (2002). Empowerment to reduce health
disparities. Scandinavian Journal of Public Health, 30(3),
72–77.
Weisner, T. S. (1996). The 5 to 7 transition as an ecocultural
project. In A.J. Sameroff, & M.H. Marshall (Eds.), The five
to seven year shift: The age of reason and responsibility.
Chicago: University of Chicago Press.
Weisner, T. S. (1998). Human development, child well-being,
and the cultural project of development. In D. Sharma, &
K.W. Fisher (Eds.), Socioemotional development across
cultures. San Francisco: Jossey-Bass.
Weisner, T. S. (2001). Children investing in their families: The
importance of child obligation in successful development. In
A.J. Fuligni (Ed.), Family obligation and assistance during
adolescene: Contextual variations and developmental implica-
tions. New Directions for Child and Adolescent Develop-
ment, Vol. 94 (pp. 77–83). New Jersey: Jossey Bass
Weisner, T. S. (2002). Ecocultural understanding of children’s
developmental pathways. Human Development, 45, 275–281.
Woodhead, M., & Faulkner, D. (2000). Subjects, objects or
participants? Dilemmas of psychological research with
children. In P. Christensen, & A. James (Eds.), Research
with children: Perspectives and practices (pp. 9–35). London:
Falmer Press.
World Health Organisation (2001). Programming for adolescent
health and development: ‘‘What should we measure and how?’’
Report of the third meeting. Washington, DC.
World Health Organisation. (1986) Ottawa Charter for health
promotion. Copenhagen: World Health Organisation, Eur-
opean Regional Office.
Zubrick, S., Silburn, S., Vimpani, G., & Williams, A. (1999).
Emergent demand for measurement indicators of social and
family functioning. Mimeo. TVW Telethon Institute for
Child Health Research, Perth.









![PROMOTING INNOVATION IN DEVELOPING COUNTRIESsiteresources.worldbank.org/KFDLP/Resources/0-3097AubertPaper[1].pdf · PROMOTING INNOVATION IN DEVELOPING COUNTRIES: A CONCEPTUAL FRAMEWORK](https://img.dokumen.tips/doc/110x75/5e4fb44eeaf20704692ca61e/promoting-innovation-in-developing-co-1pdf-promoting-innovation-in-developing.jpg)















