Embed Size (px)
Citation preview
The Glaucoma Guidelines of the SwedishOphthalmological Society
Published in Acta Ophthalmologica with permission of the Swedish Ophthalmological Society
ª Swedish Ophthalmological Society
Authors
Anders Heijl, Professor and Senior Consultant, Department of Ophthalmology, Skane University Hospital Malmo,Chair of the Expert Panel on Open-Angle Glaucoma of the Swedish Council on Health Technology Assessment(SBU), and Chair of the Swedish Glaucoma Society.
Albert Alm, Professor Emeritus, Department of Ophthalmology, Academic Hospital, Uppsala, member of the SBUExpert Panel on Open-Angle Glaucoma, and member of the Board of the Swedish Glaucoma Society.
Boel Bengtsson, Associate Professor, Clinical Sciences Malmo, Department of Ophthalmology, Lund University,member of the SBU Expert Panel on Open-Angle Glaucoma, and member of the Board of the Swedish GlaucomaSociety.
Anders Bergstrom, Senior Consultant, Department of Ophthalmology, Skane University Hospital Malmo-Lund, andmember of the Board of the Swedish Glaucoma Society.
Berit Calissendorff, Associate Professor, member of the SBU Expert Panel on Open-Angle Glaucoma, and formerSenior Consultant and Director of St. Erik Eye Hospital, Stockholm.
Bertil Lindblom, Professor and Senior Consultant, Sahlgrenska Academy, University of Gothenburg, and formerChair of the Swedish Glaucoma Society.
Christina Linden, Associate Professor and Senior Consultant, Department of Clinical Sciences, Ophthalmology,Umea University, member of the SBU Expert Panel on Open-Angle Glaucoma, and Secretary of the SwedishGlaucoma Society.
Acta Ophthalmologica 2012

Preface
In 1995, the Swedish Glaucoma Society proposed Guidelines for the Management of Open-Angle Glaucoma and OcularHypertension, which were subsequently accepted and recommended by the Swedish Ophthalmological Society. In 1997, theSwedish National Board of Health and Welfare published a state-of-the-art report entitled Open-Angle Glaucoma.
Requests to update these documents were long expressed, and it seemed rather reasonable that that should be performedconsidering the important advances that have been made in the field of glaucoma over the past decade, for example, inlarge randomized studies of this disease. Nonetheless, it was necessary to put such improvement on hold pending the out-come of several years’ work on an extensive systematic evaluation of treatment and diagnostics of glaucoma. The resultsof that assessment were published by SBU in October 2008 in the report Diagnostics, follow-up, and treatment in open-angle glaucoma: a systematic review of the literature.
After the SBU report appeared, it was logical that the next step would be to develop new guidelines. Work on that taskwas commissioned by the Swedish Ophthalmological Society and was performed by the members of the SBU Expert Panel(Albert Alm, Boel Bengtsson, Berit Calissendorff, Christina Linden and myself) and two experts from the Board of theSwedish Glaucoma Society (Anders Bergstrom and Bertil Lindblom). On assignment from the Swedish OphthalmologicalSociety, the guidelines that were created were reviewed by Bjorn Fristrom and Enping Chen and subsequently revised.
It is the ambition of the Swedish Ophthalmological Society that these new guidelines be put to widespread use in glau-coma care in Sweden.
The authors also hope that these Guidelines will be of interest to an international readership, when they have now beentranslated into English for publication in Acta Ophthalmologica.
Anders Heijlon behalf of the Expert Panel
30 December 2011
Conflicts of InterestAnders Heijl is a paid consultant to Carl Zeiss Meditec, Allergan and Alcon. Boel Bengtsson is a paid consultant to CarlZeiss Meditec. Anders Bergstrom briefly served as a paid consultant to Alcon. Christina Linden is a member of the Aller-gan Nordic Advisory Board. Bertil Lindblom, Berit Calissendorff and Albert Alm have no potential conflicts to declare.
Acta Ophthalmologica 2012
List of Contents
1 DEFINITION OF GLAUCOMA, VISUAL DISABILITY,AND QUALITY OF LIFE
6
Definition of glaucoma 6
Risk of visual disability and blindness 6
Quality of life 6
Assessment of QoL 6
QoL in glaucoma patients 7
2 EPIDEMIOLOGY AND RISK FACTORS 7Epidemiology 7Risk factors for open-angle glaucoma and
glaucoma progression
8
Risk factors—individuals 8
Age 8Ethnicity ⁄Race 8Heredity 8
Risk factors—eyes 8
Increased IOP 8Fluctuations in IOP 8Perfusion pressure 8–9Exfoliation syndrome 9Myopia 9Central corneal thickness (CCT) 9Signs of glaucoma 9
Risk factors—general diseases 9
Blood pressure 9Cardiovascular disease 9Diabetes mellitus 9Migraine and Raynaud’s syndrome 9Sleep apnoea 9–10
Medications 10
Lifestyle factors 10
3 CLINICAL FINDINGS AND DIAGNOSTICS 10The optic disc and retinal nerve fiber layer 10
The optic disc 10
The retinal nerve fiber layer 11
Examination techniques 11
Ophthalmoscopy 11Direct ophthalmoscopy 11
Indirect ophthalmoscopy 11
Biomicroscopy 11
Optic disc photography 11Analogue (film) photography 11
Digital photography 11
Methods for analyzing the optic disc andnerve fiber layer
11
Scanning laser tomography 11
GDx VCC and GDx ECC 11–12
Optical coherence tomography (OCT) 12
Perimetry 12
Examination techniques 12
Screening and threshold programs 13Interpretation of visual field test results: diagnosis 14
Follow-up: Interpretation of visual field tests and progression 14–15
Event analysis 15Trend analysis 15
High-pass resolution (ring) perimetry 17
IOP and tonometry 17
Normal IOP 17
Variation in IOP 17
Factors that influence IOP 17–18
Methods 18
The Goldmann applanation tonometer 18Perkins tonometer 19‘‘Air-puff’’ or non-contact tonometry (NCT) 19Ocular response analyzer (ORA) 19Tonopen� 19Dynamic contour tonometry (DCT) ⁄Pascal� 19
Rebound tonometry ⁄ Icare� 19Corneal thickness and pachymetry 19
Methods 19
Ultrasound pachymetry 19Orbscan�—slit-scan pachymetry 20
Future aspects 20
Gonioscopy 20
Methods 20
Static gonioscopy 20Dynamic gonioscopy 20Assessment of anterior chamber depth by vanHerick’s method 20
4 PRINCIPLES FOR MANAGEMENT OF GLAUCOMA 21Making a diagnosis 21
Optic nerve damage with a normal visual field 21
Visual field damage with a normal optic nerve 21–22
Instrumental examination of optic disc topography
and thickness of the retinal nerve fiber layer
22
Radiological investigations 22
General treatment principles 22
Goal of treatment 22
Treatment methods and effects 22–23
Risk analysis and target IOP 23
Rate of progression 23
Individualized glaucoma management 24
Overall assessment 24
5 TREATMENT METHODS 25Pharmacological treatment of glaucoma 25
Beta-receptor-blocking drugs 25
Prostaglandin analogues 25
Sympathomimetics 25–26
Parasympathomimetics 26
Carbonic anhydrase inhibitors 26–27
Combination preparations 27
Use in children and during pregnancy and lactation 27
Treatment stages and strategies 27
Switch or add 27
Combination treatments 27–28
Medical treatments other than pressure reduction 28
When are eye drops insufficient? 28
Laser treatment 28
LTP ⁄ALT 28
SLT 28–29
Primary laser treatment 29
Diode laser cyclophotocoagulation 29
Surgery 29
Surgical methods 29
Trabeculectomy 29–30NPT techniques (deep sclerectomy, viscocanalostomy) 30Shunts 30Cyclodestructive procedures 30
Cyclocryotherapy 30Diode laser cyclophotocoagulation 30
Intraoperative antimetabolites 30Radiation 30
Postoperative management 30–31
Massage 31Suture removal 31
Parameters for laser suture lysis 31Releasable and adjustable sutures 31Needling 31YAG laser goniopuncture 31Postoperative 5-FU 31
6 MANAGEMENT OF SUSPECTED GLAUCOMA ANDOCULAR HYPERTENSION
31
Ocular hypertension 31–32
Suspicious optic discs 32
Acta Ophthalmologica 2012
4

Optic disc haemorrhage 32
Exfoliation syndrome 32
Glaucoma and positive family history 32
7 POPULATION SCREENING AND CASE FINDING 32–33
REFERENCES 33–38
Acta Ophthalmologica 2012
5

1 Definition of Glaucoma,Visual Disability, andQuality of Life
Definition of glaucoma
Glaucoma is defined as a progressive dis-ease that causes characteristic degenera-tive changes in the optic disc, the retinalnerve fibre layer and the visual field.Increased intraocular pressure (IOP) wasinitially considered to be a prerequisitefor a diagnosis of open-angle glaucoma,whereas such a rise in pressure is nolonger included in the definition of thisdisease. Patients with normal IOP werepreviously classified as having low-ten-sion glaucoma. However, today a diag-nosis of primary open-angle glaucoma isgiven to patients who have elevated IOPas well as those who have normal pres-sure, and the disease in the latter groupis preferably called normal-tension ratherthan low-tension glaucoma. In primaryopen-angle glaucoma, the anterior cham-ber angle is open and there are no identi-fiable causes of the disease.
Exfoliation glaucoma is regarded asa secondary form of glaucoma in mostparts of the world, although notalways in the Nordic countries. Exfoli-ation glaucoma is a synonym for theterms pseudoexfoliation glaucoma andcapsular glaucoma, which were usedmore often in the past.
Risk of visual disability and
blindness
In the Western world, open-angle glau-coma is the second most commoncause of blindness after macular degen-eration (Resnikoff et al. 2004). About3–5% of patients with glaucoma areblind (Quigley & Broman 2006), butglaucoma is a progressive disease andthus that proportion increases withadvancing age. Consequently, a largernumber of people with glaucoma goblind during their lifetimes, with figuresin the range 6–15% at the last exami-nation before death (Hattenhauer et al.1998; Forsman et al. 2007). It is morecommon to be blind in one eye only.
Intraocular pressure is no longer includedin the definition of glaucomaA large minority of all glaucoma patientsbecome blind in both eyes during theirlifetimes, and blindness in one eye is com-mon
The main risk factor for blindnessis having extensive visual impairmentat diagnosis (Chen 2004), althoughyounger age at diagnosis obviouslyincreases the risk as well. The aver-age age at diagnosis is approximately70 years, and hence a 60-year oldwho is diagnosed with manifest glau-coma must be regarded as a rela-tively young patient (Rudnicka et al.2006).
The proportion of blind individualsvaries with the definition of blindness.The WHO definition (sidebar) is usedin Sweden. The United States hasintroduced disability benefits for glau-coma patients with severe visualimpairment defined as a mean devia-tion (MD) value worse than )22 dBon Humphrey threshold perimetry inthe best eye (section 2.03 at http://ssa.gov/disability/professionals/bluebook/2.00-SpecialSensesandSpeech-Adult.htm)
The WHO defines blindness as visual acu-ity < 3 ⁄ 60 or a remaining visual fieldwith a diameter < 10�
Quality of life
Research and interest in quality of life(QoL) have increased steadily in recentyears. The influence of QoL is highlyimportant from the perspective of thepatient. Information about QoL helpsto create a more balanced picture ofthe consequences of the disease thanwould be possible if only functionalimpairments caused by the disease wereto be included in the description.
There is no scientific basis for overallassessment of quality of life
Assessment of quality of lifeThe concept of QoL is multidimen-sional and complex in that it includesphysical and psychological functions,and also mental and general health, aswell as social and economic aspects.The way a patient experiences QoLdepends on the person’s state of mindand possible presence of comorbidi-ties. In addition, many survey instru-ments are designed to address an issuemore from the perspective of theresearcher (i.e. considering theexpected outcome of the disease) thanfrom the standpoint of the individualpatient.
Awareness of the significance of thesurvey tools has led to developmentand validation of an increasing num-ber of instruments over the last dec-ade. Depending on the topic ofinterest, various validated instrumentsare available:
(1) General ⁄Global instruments mea-sure general dimensions of QoLand are used to compare differ-ent groups of disorders.
(2) Vision-specific instruments assessvisual function in relation to QoL.
(3) Utility estimates patients’ ownevaluations of their state ofhealth.
Some general or global QoL instru-ments have been validated for compar-ing groups or for conductingintraindividual assessment over time.The SF-36 Health Survey questionnaireis used most widely and has been trans-lated into several different languages.EuroQoL (EQ-5D), which is based onBritish material, is frequently used inEurope, and it is also the instrumentemployed most often in both clinicaland population studies in Sweden. Inas-much as the type of disease per se affectsQoL, in recent years specific strategieshave been developed for investigatingvarious disorders. An example of this isthe Visual Activities Questionnaire(VAQ), which has been modified toassess certain eye diseases. The vision-related instrument VFQ-25 has alsobeen translated into Swedish and vali-dated. A review article published by Se-vern et al. (2008) illustrates thedifficulties associated with designinginstruments that can adequately evalu-ate QoL in patients with glaucoma.
To achieve a better basis for alloca-tion of resources, an instrument thatassesses patient ‘benefit’ (utility) hasalso been developed to allow patients’own experiences of their diseases to becorrelated with cost efficiency. Thistool measures how a patient evaluatesa given state of health on a scale rang-ing from perfect health (score 1) todeath (score 0).
Quality of life is so complex andmultidimensional in nature that thereare no instruments for comprehensiveassessment of this concept. Further-more, validity problems and the lackof a ‘gold standard’ make it difficultto interpret and compare findings.Indeed, even internationally approvedand validated questionnaires can
Acta Ophthalmologica 2012
6

provide disparate results when analy-sing the same patient material.
Quality of life in patients withglaucomaMost studies of QoL in glaucoma haveconcerned visual function and haveshown that marked loss of vision leadsto lower QoL (Gutierrez et al. 1997;Sherwood et al. 1998; Janz et al. 2001;Hyman et al. 2005; Varma et al. 2006).However, there is no consensus regard-ing what degree and type of impair-ments reduce QoL. Many eye-specificassessment instruments focus on visualacuity, and few concern any particularvisual field defects, which makes it dif-ficult to compare results. Conclusionsare also contradictory with respect towhether QoL is affected by the treat-ment provided or by economic factors.On the other hand, there is agreementthat being informed of the diagnosishas a negative impact on the patient.Nonetheless, the initial anxietydecreases over time, as shown in somelongitudinal studies (Janz et al. 2007).
Receiving a diagnosis of glaucoma has atemporary negative impact on quality oflife
Strongly impaired vision reduces qualityof life
Two large treatment studies calledthe Early Manifest Glaucoma Trial(EMGT; Hyman et al. 2005) and theCollaborative Initial Glaucoma Treat-ment Study (CIGTS; Janz et al. 2001)have compared the effects of differenttherapeutic strategies on QoL duringlong-term follow-up. After 5 years inthe CIGTS, local eye problems werefound to be somewhat more commonin the surgically treated patients thanin those given only medications,although the two patient groups wereessentially comparable in other aspectsand showed relatively good QoL. Inthe EMGT, no difference in QoL wasobserved between treated anduntreated patients at 6-year follow-up.
One of the difficulties in assessingQoL in patients with glaucoma, com-pared to individuals who do not havethis disease, is the above-mentionedchoice of survey instrument. Otherproblems are related to finding age-matched controls. Control patients areoften younger. Also, some investigatorshave found no definite difference in
QoL between patients with glaucomaand controls (Gutierrez et al. 1997;Parrish et al. 1997; Wandell et al.1997), whereas others have noted lowerQoL in patients with glaucoma (Sher-wood et al. 1998; Wilson et al. 1998).In Sweden, Wandell et al. (1997) com-pared patients with glaucoma with anage-matched group of nonglaucoma-tous subjects by using the Swedish ver-sion of the general Health-RelatedQuality of Life (HRQoL) question-naire. These authors found no differ-ence in QoL between the two groups,nor did it appear that QoL was affectedby treatment with beta-blockers.
Quality of life is not necessarily lower inpatients with glaucoma as a group thanin corresponding age-matched controlsubjects
2 Epidemiology and RiskFactors
Epidemiology
Glaucoma is the most widespreadage-related eye disease after cataract(Ryskulova et al. 2008), and it is thesecond most common cause of blind-ness in the world (Resnikoff et al.2004; Quigley & Broman 2006). It hasbeen estimated that about 60 millionpeople over the age of 40 would beaffected in 2010, and that one-fourthof those would have angle-closureglaucoma and the rest open-angleglaucoma. Calculations have indicatedthat the prevalence of open-angleglaucoma (i.e. the proportion of thepopulation suffering from the disease)is approximately 2% in populatitonsover the age of 40 (Quigley & Broman2006), although the rate variesdepending on the age group and thepopulation under consideration.
In the European population, theprevalence of glaucoma has been foundto be 2% in people over the age of 40(Quigley & Broman 2006) or 6% inpeople over the age of 70 (Rudnickaet al. 2006). Similar results wereobtained in the large Swedish screeningstudy entitled the Malmo Eye Survey,which showed a prevalence of morethan 5% in 75-year-olds (SBU, 2008)and more than 2% in the age group57–79 years. Other investigations inSweden have indicated both lower
(Bengtsson 1981) and higher (Ekstrom1996; Astrom et al. 2007) prevalences.Some of these discrepancies might beexplained by the occurrence of exfolia-tion syndrome.
Exfoliation syndrome is common inSweden, predominantly in women (Ek-strom 1996; Astrom & Linden 2007),and prevalence increases substantiallywith greater age (Astrom et al. 2007).In the north of Sweden, Astrom andcolleagues (2007) detected exfoliationsin 23% of all 66-year-olds, and, after21 years of follow-up (subjects aged87), 61% of the cohort had developedexfoliations in one or both eyes.
Ocular hypertension (elevated IOPwithout signs of glaucoma damage) isanother risk factor that increases withage. A number of studies have foundprevalence of 5–9% for this condition,which is several times higher than thelevel noted for open-angle glaucoma.In the Malmo Eye Survey, ocularhypertension was found to be twice ascommon as glaucoma (SBU, 2008).
Glaucoma is the second most commonage-related eye disease
In Sweden, ocular hypertension is twiceas common as glaucoma
Since there is no difference in lifeexpectancy between people with andwithout glaucoma (Grødum et al.2004), age-specific prevalence data canbe used to estimate the incidence of thisdisease (i.e. the proportion whorecently developed glaucoma; Podgoret al. 1983). Since the prevalenceincreases exponentially with advancingage, most markedly in the white popu-lation, it can be concluded that the inci-dence also rises with age (Rudnickaet al. 2006). Accordingly, older age isassociated with a greater risk of devel-oping glaucoma. Only a few studies inthe literature have addressed the inci-dence of glaucoma, and several of themwere conducted in Sweden. The inci-dence found in those investigationsvaries from 0.24% among 65- to 80-year-olds in Dalby (Bengtsson 1989) to0.64% in the corresponding age groupin Tierp (Ekstrom 2008) and 0.9% in66- to 87-year-olds in Skelleftea(Astrom et al. 2007). Such high inci-dence numbers have otherwise onlybeen reported in a black population(Leske et al. 2007b).
It has been shown that half (Ek-strom 1996; Quigley 1996) or more
Acta Ophthalmologica 2012
7
than half (Quigley & Broman 2006) ofall cases of glaucoma revealed by pop-ulation surveys are undiagnosed. It isnot known exactly how many peoplein Sweden have been identified as hav-ing glaucoma. Nonetheless, the num-ber has been estimated to beapproximately 100 000, although thatvalue is highly uncertain. Consideringthat 4.6 million people in Sweden areover the age of 40 (SCB. StatistiskaCentralbyran 2008), 100 000 knowncases of glaucoma would imply thefollowing:
(1) most of the people with glau-coma in this country are identi-fied, which is contradicted byprevalence studies performedthus far;
(2) or glaucoma prevalence is higherthan 2%, an assumption forwhich there is some support;
(3) or the estimate is incorrect andalso includes, for example,patients with ocular hypertension.
In a fairly recent meta-analysis thatcomprised 25 studies including morethan 60 000 subjects, 1355 of themwith glaucoma, Rudnicka et al. (2006)noted that glaucoma prevalence wasmore than about 1.4 times greater inmen than in women. However, otheranalyses have provided conflictingresults.
At least half of all glaucomas are undiag-nosed
In Sweden, the number of people with aglaucoma diagnosis is uncertain but hasbeen estimated to be 100 000
Patients with glaucoma identified in clini-cal practice differ from those detected byscreening
The prevalence of open-angle glaucoma inthe adult population is approximately 2%in Europe and the rest of the world, andat least 2% in Sweden
It is not clear whether there are gender-related differences
Patients with glaucoma detected bypopulation screening differ in manyways from patients who are diagnosedat an eye department. Individuals inthe latter group are much more likelyto exhibit higher IOP, more extensivevisual field damage and bilateral dis-ease (Grødum et al. 2002a), as well asexfoliation syndrome. In Malmo andTierp, exfoliation glaucoma consti-tuted 44% and 60% of clinically diag-
nosed patients with glaucoma,respectively, but only 16% of thecases detected at screening, in bothcities. On the other hand, normal-ten-sion glaucoma was detected moreoften by screening. In Malmo, half ofthe cases identified by screening hadlow-tension glaucoma, one-third inTierp. Clinically diagnosed patientswere considerably fewer, 14% and 0%in Malmo and Tierp, respectively (Ek-strom 1996; Grødum et al. 2002a).These observations suggest that nor-mal-tension glaucoma is frequentlyoverlooked in clinical examinations.
Exfoliation syndrome is common inSweden and occurrence increases with age
Risk factors for open-angle
glaucoma and glaucoma
progression
A risk factor is an event, a condition,a behaviour or some other aspect thatcan have an impact on developmentof a disease. There is both a causaland a statistical relationship betweena risk factor and the illness in ques-tion. A simple statistical relationshipbetween the risk and the disease cansuffice as a marker or an indicator ofrisk. In many cases, we do not distin-guish between these two concepts andinstead, somewhat imprecisely, referto them as risk factors, which alsoapplies in these guidelines. Many riskfactors are confirmed in cross-sec-tional epidemiological studies, andhence it is important to have a uni-form definition of the disease whenstudying risk factors. Vision 2020 is aglobal initiative that was establishedjointly by the WHO and other organi-zations with the intention of eliminat-ing all avoidable blindness. Vision2020 defines glaucoma as both struc-tural and functional damages.
In some cases, for instance, opticdisc changes or abnormal values in avisual field index are interpreted asrisk factors for glaucoma. These aresigns of disease and thus cannot actu-ally be regarded as risk factors fordeveloping glaucoma. A number ofother factors have been reported toincrease the risk of both occurrenceand progression of glaucoma. How-ever, although these factors are oftenthe same, it seems that they may differ
regarding their impact on develop-ment and progression of the disease.
Risk factors—individualsAgeOlder age is strongly related to glau-coma. Both incidence and prevalenceincrease with age (Gordon et al. 2002;de Voogd et al. 2005; Miglior et al.2007b; Leske et al. 2008), and olderage is also a risk factor for glaucomaprogression (Lichter et al. 2001; Theadvanced glaucoma intervention study(AGIS) 2002; Leske et al. 2007a,b;Chauhan et al. 2008b).
Ethnicity ⁄ racePrevalence of glaucoma is higher inpeople of African descent than in thoseof European ancestry (Leske et al.1994). In one study (Tielsch et al.1991), prevalence in the comparativelyyoung age range of 51–60 years wasfound to be four times higher in blackAmericans than in white Americans.
HeredityGlaucoma in first- or second-degreefamily members is a risk factor, regard-less of IOP (Hulsman et al. 2002; Leskeet al. 2008). The risk may be greater ifa sibling has glaucoma than if a parenthas the disease (Wolfs et al. 1998). Rec-ommendations concerning medicalcheckups are given in the sectionheaded Glaucoma and positive familyhistory (p. 32).
Risk factors – eyesIncreased intraocular pressureElevated IOP is the most importantrisk factor for both development(Kass et al. 2002) and progression(Heijl et al. 2002) of glaucoma. Inaddition, raised eye pressure is theonly treatable risk factor.
Fluctuations in intraocularpressureThere is no evidence that fluctuationin IOP is an independent risk factorfor development or progression ofglaucoma. Several studies have pro-vided contradictory results (Singh &Shrivastava 2009).
Perfusion pressureSeveral investigations have demon-strated a relationship between low ocu-lar perfusion pressure and bothdevelopment and progression of glau-coma (Leske 2009). The clinical signifi-cance of these observations is not clear.
Acta Ophthalmologica 2012
8

Elevated IOP is the most important andthe only treatable risk factor for bothdevelopment and progression of glaucoma
Perfusion pressure is related to howblood pressure can affect circulationin the eye, but this concept is muchtoo imprecise to be used in the man-agement of individual patients. In‘Terminology and Guidelines forGlaucoma’ published by the EuropeanGlaucoma Society (2008, p. 89), ocu-lar perfusion pressure is defined as thedifference between arterial blood pres-sure and IOP. However, perfusionpressure is a concept based on generalphysiological principles, and it doesnot take into account the decrease inpressure between the eye and theheart, which is also determined by theposition of the body or by the drop inpressure in the small vessels leading tothe eye. Measuring blood pressureand IOP in a single patient cannotgive a definite picture of the perfusionpressure in the eye that is examined inthat particular person.
Exfoliation syndromeThe risk of glaucoma is markedlyincreased in the presence of exfoliationsyndrome accompanied by elevatedIOP, although it seems that exfoliationsyndrome alone does not raise the riskof glaucoma (Grødum et al. 2005; Ek-strom & Alm 2008). Exfoliation syn-drome is also a strong risk factor forglaucoma progression, and there is evi-dence that this is independent of IOP(Leske et al. 2003). Exfoliation syn-drome is common in the Nordiccountries. For more information, seethe section of this chapter entitledEpidemiology (p. 7). For recommen-dations regarding management ofpatients with exfoliation syndrome, seepage 32 in the chapter entitled ‘Man-agement of suspected glaucoma andocular hypertension’.
MyopiaMyopia is a risk factor for glaucoma inpeople with normal IOP (Grødumet al. 2001; Oku et al. 2009). It is moredifficult to detect glaucoma damage ineyes with small optic discs (Heijl &Molder 1993). Accordingly, larger discsin myopic eyes might explain the asso-ciation between myopia and glaucoma,although the results of studies of opticdisc size and refraction are contradic-tory (Miglior et al. 1994; Varma et al.
1994). Myopia is probably not a riskfactor for progression (Leske et al.2007a,b).
Increased IOP in connection with exfolia-tion is a very strong risk factor for devel-oping glaucoma
Exfoliation syndrome is a strong andlikely independent risk factor for glau-coma progression
Central corneal thicknessThe Goldmann applanation tonome-ter gives erroneously low measure-ments in eyes with a thin cornea andinaccurately high values in those witha thick cornea. Therefore, a thin cor-nea is a risk factor for developingglaucoma (Kass et al. 2002) but repre-sents a nonimportant risk for progres-sion (Leske et al. 2007a,b).
Signs of glaucomaStructural and functional changesincluded in the definition of glaucomacannot be regarded as risk factors fordeveloping this disease. Consequently,the impact or the size of such changescan only be evaluated in relation toprogression of glaucoma. The diseaseprogresses at a faster rate in eyes thathave more visual field loss than inthose with less loss (Leske et al.2007a,b). Optic disc haemorrhagesincrease the risk of progression (Sieg-ner & Netland 1996; Leske et al.2007a,b; Bengtsson et al 2009a).
Risk factors – general diseasesBlood pressureThere is a positive correlation betweenblood pressure and IOP, whereas noassociation exists between blood pres-sure and development or progressionof glaucoma (Tielsch et al. 1995b). Anexplanation for this might be that highblood pressure improves ocular perfu-sion pressure and thereby reduces therisk caused by elevated IOP.
Cardiovascular diseaseReports in the literature on this sub-ject are not unequivocal. Somerecently published epidemiologicalstudies found an association betweencardiovascular disease and glaucoma(Lee et al. 2006; Wu et al. 2008),which other earlier investigations hadnot been able to demonstrate (Kleinet al. 1995; Borger et al. 2003). In theEarly Manifest Glaucoma Trial con-ducted in Sweden, cardiovascular dis-
ease was not a significant risk factorfor progression of glaucoma after6 years of follow-up, whereas it wassuch a factor after 8 years (Leskeet al. 2007a,b). In a longitudinal studyperformed in Canada (Chauhan et al.2008b), an association was observedafter 5 years of follow-up.
Diabetes mellitusDiabetes has long been considered arisk factor for glaucoma, which maybe explained by bias: patients withdiabetes undergo regular eye examina-tions, which other groups do not, andhence there is a greater probability ofdetecting glaucoma in diabetics. Not-withstanding, the Blue Mountains EyeStudy did find a relationship betweendiabetes and glaucoma (Mitchell et al.1997), whereas several other contem-porary studies obtained no indicationthat diabetes was a risk factor forglaucoma in the subjects that wereexamined, even though IOP washigher in those with diabetes (Tielschet al. 1995a; de Voogd 2006). Also, inthe Ocular Hypertension TreatmentStudy (Gordon et al. 2002), diabeteswas observed to protect against glau-coma. Thus, it seems that there is noevidence that diabetes is a risk factorfor glaucoma.
Migraine and Raynaud’s syndromeIt has been suggested that vasospasm,which occurs in both migraine andRaynaud’s syndrome, entails a riskfor normal-tension glaucoma (Gasseret al. 1990). However, it is not clearwhether these two conditions arerelated to existence or progression ofglaucoma. Both the Blue MountainsEye Study (Wang et al. 1997) and theBeaver Dam Eye Study (Klein et al.1993) found migraine to be a risk fac-tor for glaucoma, but the definition ofmigraine differed in those two investi-gations and has been disputed. TheSwedish Early Manifest GlaucomaTrial found neither migraine nor Ray-naud’s syndrome to be risk factors forprogression of glaucoma (Leske et al.2003).
Sleep apnoeaIt is uncertain whether sleep apnoea isassociated with glaucoma. Two clini-cal studies (Mojon et al. 2000; Girkinet al. 2006) have suggested that such arelationship does exist, whereas otherinvestigations (Geyer et al. 2003;
Acta Ophthalmologica 2012
9

Bendel et al. 2008; Roberts TV et al.2009b) have not found any connec-tion.
MedicationsIt has long been known that use ofeye drops containing cortisoneincreases IOP. Moreover, oral cortico-steroid therapy has been shown toraise the risk of ocular hypertensionand glaucoma (Garbe et al. 1997).The results of a subsequent study(Mitchell et al. 1999) suggest thatnasal sprays and inhalants containingcorticosteroids increase the risk ofocular hypertension and glaucoma,particularly in people with a familyhistory of glaucoma. The patients inthe cited investigations had both ocu-lar hypertension and glaucoma, andapparently no studies have focusedsolely on patients with glaucoma.Therefore, it seems reasonable toassume that the risk of glaucomaposed by corticosteroids is mediatedindirectly through ocular hyperten-sion.
Lifestyle factorsNo associations have been foundbetween glaucoma and physical activ-ity (Passo et al. 1991), smoking, bodymass index (BMI), alcohol or coffeeconsumption, or diet.
There is no association between lifestylefactors and glaucoma
3 Clinical Findings andDiagnostics
The optic disc and retinal nerve
fibre layer
The optic discThe basis for the glaucoma diagnosisis optic nerve damage. Such damage isalmost always associated with visualfield loss. However, damage to theoptic disc can occur either with orwithout accompanying visual fielddamage (the latter is called preperi-metric glaucoma). Also, visual fielddefects without any identifiable opticdisc damage are seen in rare casesinvolving an unusually small disc. Itcan be difficult to detect the glauco-matous damage in such a disc, partic-ularly if the disease is bilateral and
thus there is no healthy disc for com-parison.
Therefore, it is of fundamentalimportance to assess the size of theoptic disc during an examination.Exact measurement is difficult toachieve and is seldom of clinical inter-est. To estimate disc size, the heightof the split beam can be adjusted tocoincide with the vertical (or horizon-tal) disc diameter, and the readingsare converted according to the auxil-iary lens that is used (Lim et al. 1996).Another simple method is to compareoptic disc diameter (DD) with disc-to-fovea distance (DM) measured fromthe centre of the disc to the fovea.The mean of the ratio of DM to DDis 2.5 (Mok & Lee 2002). Withincreasing experience, it is often possi-ble to estimate the size of the opticdisc without relying on measured val-ues. In this context, it can suffice toroughly divide discs into these fiveclasses: very large, large, mediumsized, small and very small. A largeoptic disc will usually have a largephysiologic cup (excavation) that caneasily be mistaken for glaucomatousdamage (Heijl & Molder 1993). Thecup in a small optic disc will normallybe very small or lacking, and thus itwill be difficult to detect early glauco-matous changes. Therefore, whenanalysing the appearance of the opticdisc, it is important not to concentrateon the size of the cup, but instead tofocus on assessing the appearance ofthe neuroretinal rim and, if possible,also the thickness of the retinal nervefibre layer (Fig. 1).
Assessment of optic disc size is essentialin diagnosis of glaucoma
In glaucoma, a definite sign of opticdisc damage is a focal thinning of theneuroretinal rim, which is called anotch (Fig. 2). Such a disc change isassociated with localized thinning ofthe retinal nerve fibre layer in thesame area.
Another less reliable sign of opticdisc damage in glaucoma is a generalthinning of the neuroretinal rim (anenlarged cup). The size of the opticdisc is of vital importance in this con-text. A measurement such as the cup-to-disc (C ⁄D) ratio is of very littlevalue, unless it is considered in rela-tion to disc size. Moreover, this ratiooffers low sensitivity as a measure inlongitudinal follow-up, and thus it canbe questioned whether C ⁄D should beused at all.
Nonetheless, the thickness of theneuroretinal rim can facilitate theanalysis. According to the ISNT rule,in a normal rim the inferior (I) area isthickest, followed by the superior (S),nasal (N) and temporal (T) areas(Jonas et al. 1988a). Deviation fromthis rule should raise suspicion ofglaucomatous damage, although it isneither a sensitive nor a specific signof glaucoma (Sihota et al. 2008).
It is important to notice any differ-ence in size between the cups in the twoeyes, but it is first necessary to verifythat there is no corresponding sizedivergence between the optic discs.
A common finding in glaucoma is asmall haemorrhage on either the edgeor the surface of the optic disc(Drance 1989). Such haemorrhagesare more common in normal-tensionglaucoma than in high-pressure glau-
Fig. 1. A large normal optic disc with a large
physiologic cup (excavation). The neuroreti-
nal rim is intact and even in width.
Fig. 2. Glaucomatous optic disc showing
notching of the neuroretinal rim (arrow).
Acta Ophthalmologica 2012
10

coma (Kitazawa et al. 1986), and theyare often of short duration. The cause ofthese haemorrhages is unclear, althoughit is known that they occur more fre-quently in persons who have diabetes orusemedications containing salicylic acid(Grødum et al. 2002b; Soares et al.2004). Even though disc haemorrhagesare seen in individuals who do not haveglaucoma (Healey et al. 1998), theyshould arouse suspicion of this disease,especially if other risk factors are alsopresent (Diehl et al. 1990).
Optic disc haemorrhage is a commonfinding in open-angle glaucoma
When assessing optic discs, a poten-tial source of error is that it can bedifficult to delineate the margin ofdiscs exhibiting peripapillary atrophy.If the atrophy is mistakenly includedin the disc area, the degree of cuppingwill be underestimated (Fig. 3). Peri-papillary atrophy is common in glau-coma, but this finding is not specificand often occurs in older people whodo not have glaucoma (Curcio et al.2000) and in individuals with eye con-ditions other than glaucoma, such assevere myopia (Jonas et al. 1988b)
The retinal nerve fibre layerThinning of the retinal nerve fibre layeris often seen at an early stage of glau-coma. Among the factors that can facil-itate evaluation are clear media, densepigmentation and young age of the sub-ject. It is usually difficult to assess a gen-eral decrease in the thickness of thenerve fibre layer. Localized defects areeasier to detect, either by direct ophthal-moscopy (red-free light facilitatesexamination) or by fundus photogra-phy (Airaksinen &Nieminen 1985).
Examination techniquesOphthalmoscopySeveral new techniques have beendeveloped for analysis of the opticdisc and retinal nerve fibre layertopography, but ophthalmoscopy anddisc photography still representimportant examinations for diagnosisof glaucoma. The methods used toevaluate the fundus differ.
Direct ophthalmoscopyAdvantages. Provides an image withhigh magnification.
By far the best method for inspect-ing the retinal nerve fibre layer, partic-ularly when using red-free light.Disadvantages. Monocular viewing.
Indirect ophthalmoscopyAdvantages. Easier viewing through asmall pupil.Disadvantages. Low magnification.Monocular viewing.
BiomicroscopyAdvantages. High magnification, par-ticularly with the 60D lens.Binocular viewing (may require pupildilation).Disadvantages. Requires a slit-lampmicroscope.
Optic disc photographyPhotography of the optic disc is themost important method of permanentdocumentation. Modern techniques fortopographical analysis of the optic discor the retinal nerve fibre layer are underrapid development, but there is no guar-antee that the equipment used in thefuture will be compatible with theinstruments that are available today.Therefore, regardless of the equipmentused, it is essential to obtain photo-graphic records of the appearance ofthe optic disc, at least during diagnosis.An exception to this might be casesinvolving very advanced disc damage; itcan be impossible to detect disease pro-gression in a totally cupped optic disc.
Analogue (film) photographyAdvantages. Excellent image quality.Disadvantages. Time-consuming.Difficult to assess the results.
If possible, the optic disc should be pho-tographed at the time glaucoma or ocularhypertension is diagnosed
Digital photographyAdvantages. Fast.Results can be assessed immediately.Easy to process images.Disadvantages. Image quality can besuboptimal, particularly with olderequipment.
Opinions differ regarding theimportance of stereoscopic imaging.Obviously, use of three-dimensionalimaging can facilitate evaluation ofoptic disc cupping. On the other hand,stereophotography is seldom donewith a fixed stereo base, which may
represent a source of error in theassessment.
Methods for analysing the opticdisc and nerve fibre layer
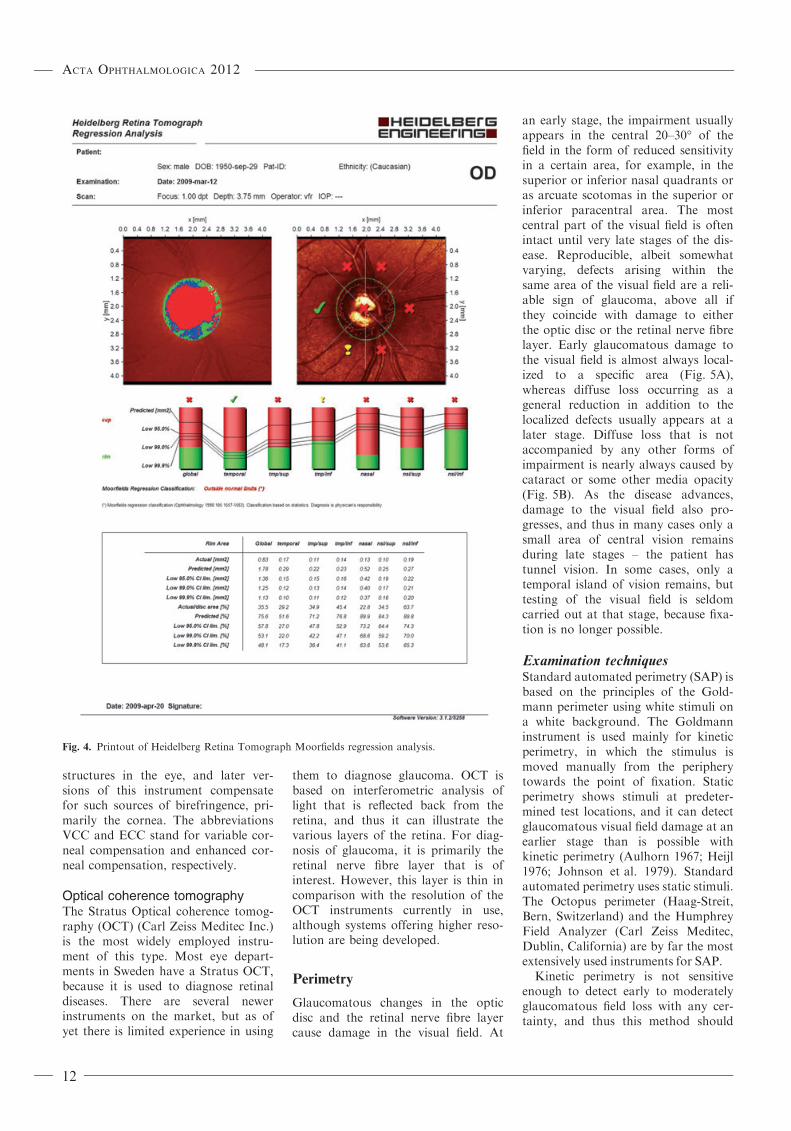
Scanning laser tomographyThis is a confocal technique that useslaser light to acquire multiple imagesat different levels in the fundus. Theimages are subsequently integrated toform a three-dimensional picture. Theinstrument in most widespread use isthe Heidelberg Retina Tomograph(HRT; Heidelberg Engineering, Hei-delberg, Germany). A third version ofthis instrument (HRT III) is nowavailable, which is compatible withthe earlier versions. In the HRT IIIsystem, the optic disc is classified byboth Moorfields regression analysisand the Glaucoma Probability Score(Fig. 4). Because an HRT instrumentanalyses the appearance of the opticdisc cup, it includes a source of errorthat is the same as that associatedwith ophthalmoscopic disc analysis:there is a risk of over-diagnosis ofglaucoma damage in large optic discs,whereas the opposite is true for smal-ler discs.
GDx VCC and GDx ECCThe GDxVCC (Carl Zeiss MeditecInc, Dublin, CA, USA) uses laserlight to analyse the retinal nerve fibrelayer (RNFL). The light is polarizedas it passes through the RNFL, andmeasurements of the changes in thepolarization state (birefringence) areused to calculate the RNFL thickness.Polarization can also occur in other
Fig. 3. Glaucomatous optic disc with peri-
papillary atrophy. The arrow indicates the
neuroretinal rim.
Acta Ophthalmologica 2012
11
structures in the eye, and later ver-sions of this instrument compensatefor such sources of birefringence, pri-marily the cornea. The abbreviationsVCC and ECC stand for variable cor-neal compensation and enhanced cor-neal compensation, respectively.
Optical coherence tomographyThe Stratus Optical coherence tomog-raphy (OCT) (Carl Zeiss Meditec Inc.)is the most widely employed instru-ment of this type. Most eye depart-ments in Sweden have a Stratus OCT,because it is used to diagnose retinaldiseases. There are several newerinstruments on the market, but as ofyet there is limited experience in using
them to diagnose glaucoma. OCT isbased on interferometric analysis oflight that is reflected back from theretina, and thus it can illustrate thevarious layers of the retina. For diag-nosis of glaucoma, it is primarily theretinal nerve fibre layer that is ofinterest. However, this layer is thin incomparison with the resolution of theOCT instruments currently in use,although systems offering higher reso-lution are being developed.
Perimetry
Glaucomatous changes in the opticdisc and the retinal nerve fibre layercause damage in the visual field. At
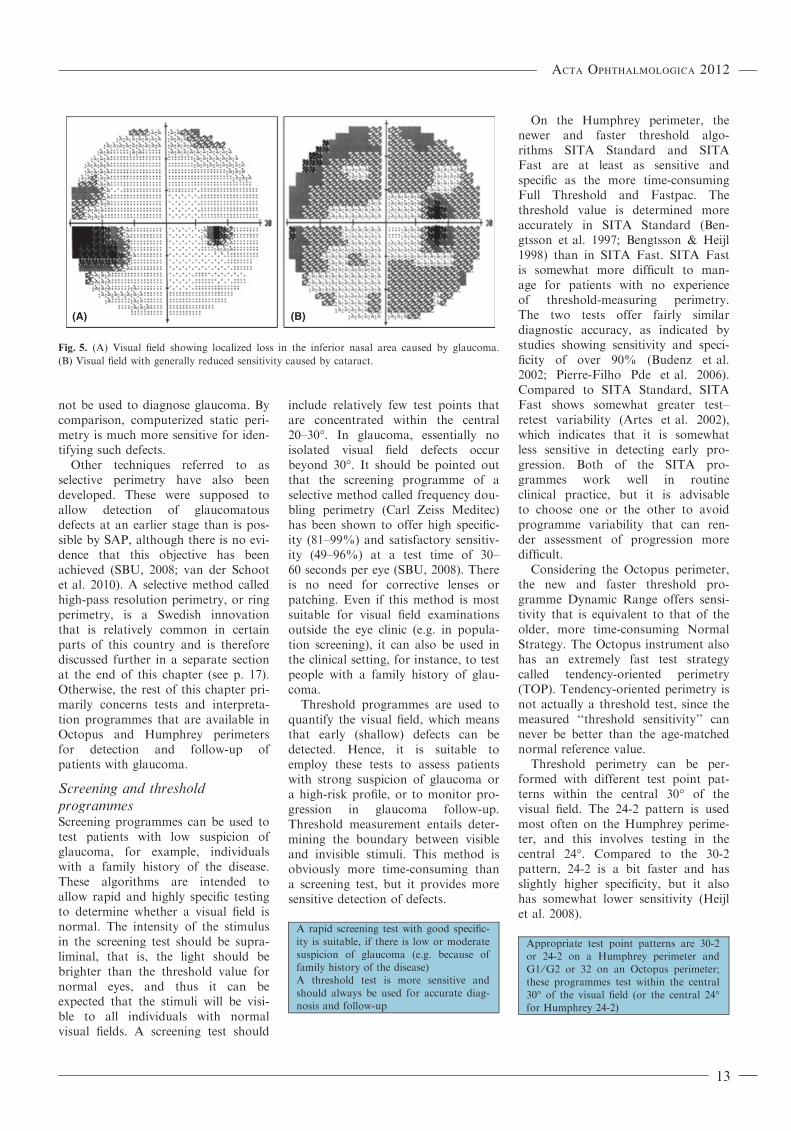
an early stage, the impairment usuallyappears in the central 20–30� of thefield in the form of reduced sensitivityin a certain area, for example, in thesuperior or inferior nasal quadrants oras arcuate scotomas in the superior orinferior paracentral area. The mostcentral part of the visual field is oftenintact until very late stages of the dis-ease. Reproducible, albeit somewhatvarying, defects arising within thesame area of the visual field are a reli-able sign of glaucoma, above all ifthey coincide with damage to eitherthe optic disc or the retinal nerve fibrelayer. Early glaucomatous damage tothe visual field is almost always local-ized to a specific area (Fig. 5A),whereas diffuse loss occurring as ageneral reduction in addition to thelocalized defects usually appears at alater stage. Diffuse loss that is notaccompanied by any other forms ofimpairment is nearly always caused bycataract or some other media opacity(Fig. 5B). As the disease advances,damage to the visual field also pro-gresses, and thus in many cases only asmall area of central vision remainsduring late stages – the patient hastunnel vision. In some cases, only atemporal island of vision remains, buttesting of the visual field is seldomcarried out at that stage, because fixa-tion is no longer possible.
Examination techniquesStandard automated perimetry (SAP) isbased on the principles of the Gold-mann perimeter using white stimuli ona white background. The Goldmanninstrument is used mainly for kineticperimetry, in which the stimulus ismoved manually from the peripherytowards the point of fixation. Staticperimetry shows stimuli at predeter-mined test locations, and it can detectglaucomatous visual field damage at anearlier stage than is possible withkinetic perimetry (Aulhorn 1967; Heijl1976; Johnson et al. 1979). Standardautomated perimetry uses static stimuli.The Octopus perimeter (Haag-Streit,Bern, Switzerland) and the HumphreyField Analyzer (Carl Zeiss Meditec,Dublin, California) are by far the mostextensively used instruments for SAP.
Kinetic perimetry is not sensitiveenough to detect early to moderatelyglaucomatous field loss with any cer-tainty, and thus this method should
Fig. 4. Printout of Heidelberg Retina Tomograph Moorfields regression analysis.
Acta Ophthalmologica 2012
12
not be used to diagnose glaucoma. Bycomparison, computerized static peri-metry is much more sensitive for iden-tifying such defects.
Other techniques referred to asselective perimetry have also beendeveloped. These were supposed toallow detection of glaucomatousdefects at an earlier stage than is pos-sible by SAP, although there is no evi-dence that this objective has beenachieved (SBU, 2008; van der Schootet al. 2010). A selective method calledhigh-pass resolution perimetry, or ringperimetry, is a Swedish innovationthat is relatively common in certainparts of this country and is thereforediscussed further in a separate sectionat the end of this chapter (see p. 17).Otherwise, the rest of this chapter pri-marily concerns tests and interpreta-tion programmes that are available inOctopus and Humphrey perimetersfor detection and follow-up ofpatients with glaucoma.
Screening and thresholdprogrammesScreening programmes can be used totest patients with low suspicion ofglaucoma, for example, individualswith a family history of the disease.These algorithms are intended toallow rapid and highly specific testingto determine whether a visual field isnormal. The intensity of the stimulusin the screening test should be supra-liminal, that is, the light should bebrighter than the threshold value fornormal eyes, and thus it can beexpected that the stimuli will be visi-ble to all individuals with normalvisual fields. A screening test should
include relatively few test points thatare concentrated within the central20–30�. In glaucoma, essentially noisolated visual field defects occurbeyond 30�. It should be pointed outthat the screening programme of aselective method called frequency dou-bling perimetry (Carl Zeiss Meditec)has been shown to offer high specific-ity (81–99%) and satisfactory sensitiv-ity (49–96%) at a test time of 30–60 seconds per eye (SBU, 2008). Thereis no need for corrective lenses orpatching. Even if this method is mostsuitable for visual field examinationsoutside the eye clinic (e.g. in popula-tion screening), it can also be used inthe clinical setting, for instance, to testpeople with a family history of glau-coma.
Threshold programmes are used toquantify the visual field, which meansthat early (shallow) defects can bedetected. Hence, it is suitable toemploy these tests to assess patientswith strong suspicion of glaucoma ora high-risk profile, or to monitor pro-gression in glaucoma follow-up.Threshold measurement entails deter-mining the boundary between visibleand invisible stimuli. This method isobviously more time-consuming thana screening test, but it provides moresensitive detection of defects.
A rapid screening test with good specific-ity is suitable, if there is low or moderatesuspicion of glaucoma (e.g. because offamily history of the disease)A threshold test is more sensitive andshould always be used for accurate diag-nosis and follow-up
On the Humphrey perimeter, thenewer and faster threshold algo-rithms SITA Standard and SITAFast are at least as sensitive andspecific as the more time-consumingFull Threshold and Fastpac. Thethreshold value is determined moreaccurately in SITA Standard (Ben-gtsson et al. 1997; Bengtsson & Heijl1998) than in SITA Fast. SITA Fastis somewhat more difficult to man-age for patients with no experienceof threshold-measuring perimetry.The two tests offer fairly similardiagnostic accuracy, as indicated bystudies showing sensitivity and speci-ficity of over 90% (Budenz et al.2002; Pierre-Filho Pde et al. 2006).Compared to SITA Standard, SITAFast shows somewhat greater test–retest variability (Artes et al. 2002),which indicates that it is somewhatless sensitive in detecting early pro-gression. Both of the SITA pro-grammes work well in routineclinical practice, but it is advisableto choose one or the other to avoidprogramme variability that can ren-der assessment of progression moredifficult.
Considering the Octopus perimeter,the new and faster threshold pro-gramme Dynamic Range offers sensi-tivity that is equivalent to that of theolder, more time-consuming NormalStrategy. The Octopus instrument alsohas an extremely fast test strategycalled tendency-oriented perimetry(TOP). Tendency-oriented perimetry isnot actually a threshold test, since themeasured ‘‘threshold sensitivity’’ cannever be better than the age-matchednormal reference value.
Threshold perimetry can be per-formed with different test point pat-terns within the central 30� of thevisual field. The 24-2 pattern is usedmost often on the Humphrey perime-ter, and this involves testing in thecentral 24�. Compared to the 30-2pattern, 24-2 is a bit faster and hasslightly higher specificity, but it alsohas somewhat lower sensitivity (Heijlet al. 2008).
Appropriate test point patterns are 30-2or 24-2 on a Humphrey perimeter andG1 ⁄G2 or 32 on an Octopus perimeter;these programmes test within the central30� of the visual field (or the central 24�for Humphrey 24-2)
(A) (B)
Fig. 5. (A) Visual field showing localized loss in the inferior nasal area caused by glaucoma.
(B) Visual field with generally reduced sensitivity caused by cataract.
Acta Ophthalmologica 2012
13

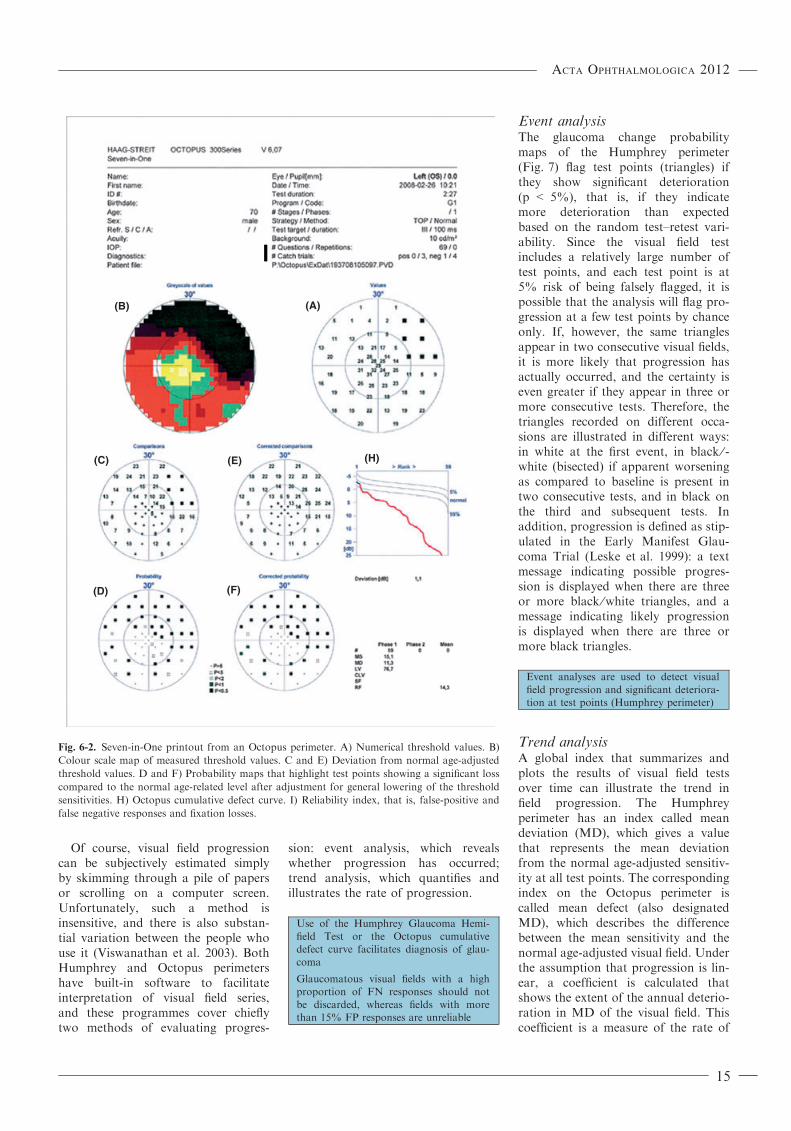
Interpretation of visual field testresults: diagnosisA printout of a visual field testcontains several maps and indices(Fig 6-1 and 6-2).
As a rule, glaucomatous visualdefects can be seen in probabilitymaps (Fig. 6D,F) before they can beclearly discerned in numerical maps(Fig. 6C,E) or the grey or colour scaleof the measured threshold values(Fig. 6B). The best aid in interpretingresults is provided by a probabilitymap that has been adjusted for bothage-related and general loss (Fig. 6F);
such a map can reveal the locationand extent of glaucomatous defectswithout being disturbed by mediaopacities such as cataract. The Hum-phrey Glaucoma Hemifield Test(Fig. 6G) and the Octopus cumulativedefect curve (Fig. 6H) are two otherindices that can facilitate detection ofearly glaucomatous visual field dam-age. Global visual field indices likemean deviation (MD), pattern stan-dard deviation (PSD) and the visualfield index (VFI) on the Humphreyperimeter, mean defect (MD) and lossvariance (LV) on the Octopus perime-
ter are not suitable for making a diag-nosis.
The reliability parameters false-posi-tive (FP) responses, false-negative(FN) responses and fixation losses(FL) (Fig. 6I) are meant to show howreliably a patient performs during atest. FP responses indicate that the per-son being tested pressed the button toooften, that is, that he or she respondedeven if no stimulus was shown. Today,the upper limit of reliability is set at15%, and that level is based on datarepresenting a large normal population(n � 330) (Bengtsson & Heijl 2000a).Visual fields with more than 15% FPresponses cannot be evaluated, and apatient with such results should begiven new and probably differentinstructions on how to perform thetest. A test with a large proportion ofFN responses suggests that the patientdid not react to visible stimuli. How-ever, the method used to measure FNresponses cannot be applied to individ-uals who have visual field defects (Katz& Sommer 1988; Bengtsson & Heijl2000b), and thus a high rate of suchresponses by patients with glaucomashould be disregarded. On the otherhand, the rate of FN responses shouldbe low for people who have healthyeyes with a normal visual field.
Probability maps, particularly thosethat are adjusted for both age andgeneral loss (often caused by cata-ract), provide valuable informationabout the extent and location ofvisual field defects, and these arecalled either pattern deviation proba-bility maps (Humphrey) or correctedprobability maps (Octopus).
Follow-up: interpretation of visualfield tests and progressionIn most cases, several visual field testsare needed to correctly estimate therate of visual field progression or toascertain whether progression hasoccurred. Test–retest variability isgreater in a glaucomatous visual fieldthan in a healthy one (i.e. reproduc-ibility is poorer in glaucoma), whichexplains why a number of examina-tions must be performed to achievesatisfactory precision regarding pro-gression. Sudden large changes arerare in glaucoma, but it can appearthat such events have occurred ifvisual field testing is not performedoften enough.
(A)
(C) (E)
(G)
(F)(D)
(B)
Fig. 6-1. Single Field Analysis of a visual field test on a Humphrey Perimeter. A) Numerical
threshold values. B) Grey scale map of measured threshold valued. C and E) Deviation from
normal age-adjusted threshold values. D and F) Probability maps that highlight test points
showing a significant loss compared to the normal age-related level after adjustment for general
lowering of the threshold sensitivities. G) Glaucoma Hemifield Test. I) Reliability index, that is,
false-positive and false-negative responses and fixation losses.
Acta Ophthalmologica 2012
14
Of course, visual field progressioncan be subjectively estimated simplyby skimming through a pile of papersor scrolling on a computer screen.Unfortunately, such a method isinsensitive, and there is also substan-tial variation between the people whouse it (Viswanathan et al. 2003). BothHumphrey and Octopus perimetershave built-in software to facilitateinterpretation of visual field series,and these programmes cover chieflytwo methods of evaluating progres-
sion: event analysis, which revealswhether progression has occurred;trend analysis, which quantifies andillustrates the rate of progression.
Use of the Humphrey Glaucoma Hemi-field Test or the Octopus cumulativedefect curve facilitates diagnosis of glau-coma
Glaucomatous visual fields with a highproportion of FN responses should notbe discarded, whereas fields with morethan 15% FP responses are unreliable
Event analysisThe glaucoma change probabilitymaps of the Humphrey perimeter(Fig. 7) flag test points (triangles) ifthey show significant deterioration(p < 5%), that is, if they indicatemore deterioration than expectedbased on the random test–retest vari-ability. Since the visual field testincludes a relatively large number oftest points, and each test point is at5% risk of being falsely flagged, it ispossible that the analysis will flag pro-gression at a few test points by chanceonly. If, however, the same trianglesappear in two consecutive visual fields,it is more likely that progression hasactually occurred, and the certainty iseven greater if they appear in three ormore consecutive tests. Therefore, thetriangles recorded on different occa-sions are illustrated in different ways:in white at the first event, in black ⁄ -white (bisected) if apparent worseningas compared to baseline is present intwo consecutive tests, and in black onthe third and subsequent tests. Inaddition, progression is defined as stip-ulated in the Early Manifest Glau-coma Trial (Leske et al. 1999): a textmessage indicating possible progres-sion is displayed when there are threeor more black ⁄white triangles, and amessage indicating likely progressionis displayed when there are three ormore black triangles.
Event analyses are used to detect visualfield progression and significant deteriora-tion at test points (Humphrey perimeter)
Trend analysisA global index that summarizes andplots the results of visual field testsover time can illustrate the trend infield progression. The Humphreyperimeter has an index called meandeviation (MD), which gives a valuethat represents the mean deviationfrom the normal age-adjusted sensitiv-ity at all test points. The correspondingindex on the Octopus perimeter iscalled mean defect (also designatedMD), which describes the differencebetween the mean sensitivity and thenormal age-adjusted visual field. Underthe assumption that progression is lin-ear, a coefficient is calculated thatshows the extent of the annual deterio-ration in MD of the visual field. Thiscoefficient is a measure of the rate of
(A)(B)
(C)
(D) (F)
(E) (H)
Fig. 6-2. Seven-in-One printout from an Octopus perimeter. A) Numerical threshold values. B)
Colour scale map of measured threshold values. C and E) Deviation from normal age-adjusted
threshold values. D and F) Probability maps that highlight test points showing a significant loss
compared to the normal age-related level after adjustment for general lowering of the threshold
sensitivities. H) Octopus cumulative defect curve. I) Reliability index, that is, false-positive and
false negative responses and fixation losses.
Acta Ophthalmologica 2012
15
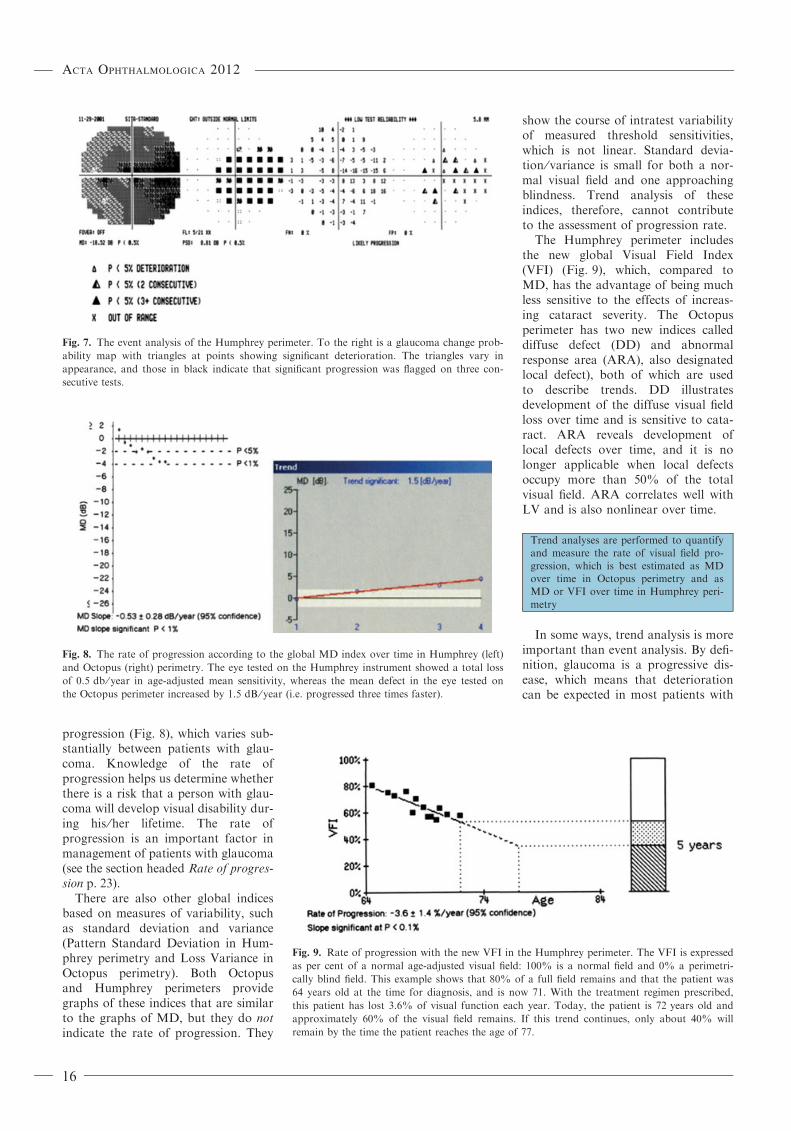
progression (Fig. 8), which varies sub-stantially between patients with glau-coma. Knowledge of the rate ofprogression helps us determine whetherthere is a risk that a person with glau-coma will develop visual disability dur-ing his ⁄her lifetime. The rate ofprogression is an important factor inmanagement of patients with glaucoma(see the section headed Rate of progres-sion p. 23).
There are also other global indicesbased on measures of variability, suchas standard deviation and variance(Pattern Standard Deviation in Hum-phrey perimetry and Loss Variance inOctopus perimetry). Both Octopusand Humphrey perimeters providegraphs of these indices that are similarto the graphs of MD, but they do notindicate the rate of progression. They
show the course of intratest variabilityof measured threshold sensitivities,which is not linear. Standard devia-tion ⁄ variance is small for both a nor-mal visual field and one approachingblindness. Trend analysis of theseindices, therefore, cannot contributeto the assessment of progression rate.
The Humphrey perimeter includesthe new global Visual Field Index(VFI) (Fig. 9), which, compared toMD, has the advantage of being muchless sensitive to the effects of increas-ing cataract severity. The Octopusperimeter has two new indices calleddiffuse defect (DD) and abnormalresponse area (ARA), also designatedlocal defect), both of which are usedto describe trends. DD illustratesdevelopment of the diffuse visual fieldloss over time and is sensitive to cata-ract. ARA reveals development oflocal defects over time, and it is nolonger applicable when local defectsoccupy more than 50% of the totalvisual field. ARA correlates well withLV and is also nonlinear over time.
Trend analyses are performed to quantifyand measure the rate of visual field pro-gression, which is best estimated as MDover time in Octopus perimetry and asMD or VFI over time in Humphrey peri-metry
In some ways, trend analysis is moreimportant than event analysis. By defi-nition, glaucoma is a progressive dis-ease, which means that deteriorationcan be expected in most patients with
Fig. 7. The event analysis of the Humphrey perimeter. To the right is a glaucoma change prob-
ability map with triangles at points showing significant deterioration. The triangles vary in
appearance, and those in black indicate that significant progression was flagged on three con-
secutive tests.
Fig. 8. The rate of progression according to the global MD index over time in Humphrey (left)
and Octopus (right) perimetry. The eye tested on the Humphrey instrument showed a total loss
of 0.5 db ⁄ year in age-adjusted mean sensitivity, whereas the mean defect in the eye tested on
the Octopus perimeter increased by 1.5 dB ⁄ year (i.e. progressed three times faster).
Fig. 9. Rate of progression with the new VFI in the Humphrey perimeter. The VFI is expressed
as per cent of a normal age-adjusted visual field: 100% is a normal field and 0% a perimetri-
cally blind field. This example shows that 80% of a full field remains and that the patient was
64 years old at the time for diagnosis, and is now 71. With the treatment regimen prescribed,
this patient has lost 3.6% of visual function each year. Today, the patient is 72 years old and
approximately 60% of the visual field remains. If this trend continues, only about 40% will
remain by the time the patient reaches the age of 77.
Acta Ophthalmologica 2012
16

glaucoma, if they are followed for asufficiently long period and are testedusing methods that allow reasonablysensitive measurement of progression.Trend analysis can identify patientswho exhibit rapid progression andrequire special attention and intensifiedtreatment. It can also reveal patientswho can be examined less frequently,because their disease is advancingslowly and it appears that the efficacyof the treatment they are receiving issatisfactory. Nevertheless, compared totrend analysis, event analysis candetect progression earlier, and thus it isvaluable in management of newly diag-nosed patients with glaucoma. Severeand acute changes are very rare inglaucoma and usually depend on someother factor, such as stroke or retinalvessel occlusion. Obviously, both eventand trend analysis are affected by suchvisual field damage and cannot distin-guish it from glaucoma. Accordingly,in cases involving substantial acutechanges, the examiner should suspectsome other disease and, depending onthe patient’s condition, create a newvisual field baseline to allow continuedmonitoring of glaucoma progression.Event and trend analysis complementeach other: both use the same visualfield tests, and both analyses areavailable in the perimeters.
High-pass resolution (ring)perimetryHigh-pass resolution perimetry (HRP)was introduced in 1987 (Frisen 1987)as a test method that would be bettercorrelated with the density of retinalganglion cells compared to conven-tional perimetry. This test also hadthe benefit of being fast and patientfriendly, although the time advantagecompared to traditional perimetry waslater reduced by the development ofSAP.
The method is called high-pass reso-lution or ring perimetry, because ituses low-contrast, high-spatial-fre-quency-filtered, ring-shaped test tar-gets. The targets vary in size duringthe examination. The results are pre-sented in a straightforward manner:the smaller the rings, the better thevisual function. In a normal visualfield, the rings are small in the centraltest locations and are successively lar-ger towards the periphery. Deviationfrom the expected progression is con-
sidered abnormal. Testing is facilitatedby various indices in the same way asin SAP. High-pass resolution perime-try global deviation is a measure ofthe total age-related deviation, whichcorresponds to the Humphrey MD.In the same way, local deviationcorresponds to Humphrey PSD andOctopus LV. High-pass resolutionperimetry has no equivalent to theHumphrey Glaucoma Hemifield Test.However, an older version of ringperimetry includes an instrumentalassessment to determine whether avisual field is normal, whereas such atool is not included in the Windows-based HRP. Longitudinal follow-upcan be achieved as in SAP by printinga series of visual fields and obtaininga plot of the global deviation againsttime. Notwithstanding, the ring perim-eter lacks the newer, more detailedmethods for evaluating glaucoma pro-gression, which are available primarilyin the Humphrey perimeter.
A number of studies have indi-cated that HRP is comparable toSAP with regard to the capacity todetect early glaucomatous damageand progression of glaucoma (Marti-nez et al. 1995; Chauhan et al. 1999;Sample et al. 2006). No larger inves-tigations have been performed onthis topic.
Intraocular pressure and tonometry
It is now accepted that IOP affects thedevelopment (Kass et al. 2002) and theprogression (Collaborative Normal-Tension Glaucoma Study Group,1998a,b; Heijl et al. 2002) of glaucoma:the higher the pressure, the greater therisk of both occurrence and progres-sion of the disease. All available treat-ments are intended to lower IOP, andtherefore measurement of IOP isalways included in the diagnostic andfollow-up examinations of patientswith suspected or confirmed glaucoma.
Normal intraocular pressureFrom a functional perspective, all lev-els of IOP that are not deleterious forthe eye are ‘normal’. However, thelevel that is harmful varies betweenindividuals, and thus it is often impos-sible to unambiguously determinewhether IOP can be considered nor-mal after only a few measurementoccasions. The clinically less relevantcut-off value of 21 mmHg emanated
from numerous population studies inwhich the mean pressure was found tobe approximately 16 mmHg in adults,with a standard deviation of2.5 mmHg (Schiose 1990). However,among people over the age of 40, IOPis not normally distributed, but thereis a skewness towards higher values.Since glaucoma can develop at allIOP levels, measurement of IOP alonecannot suffice in glaucoma screening,although more attention should begiven to patients with high pressure.
Intraocular pressure is lower in chil-dren than in adults. The pressure is6–8 mmHg at birth and increases byapproximately 1 mmHg every otheryear until the age of about 12 years(European Glaucoma Society 2008, p.61). In healthy individuals, the IOP isfairly stable or rises somewhat withincreasing age (Gabelt & Kaufman2005), perhaps a millimetre each dec-ade after the age of 40 (Martin 1992).
Variation in intraocular pressureMeasurement of IOP provides a snap-shot of the level at the time of exami-nation, but the pressure actuallyvaries with time. Diurnal fluctuationsare proportional to the level of IOP(Bengtsson & Heijl 2005b). In moststudies, such fluctuations are in therange £ 6 mm in normal individuals(Shield 2005), whereas the average dis-tribution is broader in patients withelevated IOP. Knowledge of variationin IOP levels is of uncertain value.
To gain an understanding of theuntreated IOP, repeated measurementscan be performed before initiatingtherapy. This is usually possible inpatients with chronic open-angle glau-coma, because the course of the dis-ease is slow in most cases. Owing tothe diurnal variation in pressure, itcan be beneficial to make several mea-surements at different time-points. Itis recommended that the time atwhich each measurement is performedbe recorded, in particular to enablecomparison of the results with thoseobtained in subsequent examinations.
Factors that influence intraocularpressureMany different factors affect IOP.
(1) External pressure on the eye: forexample, caused by eyelid posi-tion, squinting, or vigorous cry-ing in babies.
Acta Ophthalmologica 2012
17
(2) Episcleral venous pressure: canbe raised by actions such as theValsalva manoeuvre or wearingof a tight collar or necktie, whichincreases IOP.
(3) Eye or head position: IOP isoften slightly elevated during up-gaze or downgaze, and it ishigher when leaning backwardsthan when sitting (Anderson &Grant 1973; Jain & Marmion1976; Krieglstein et al. 1976),and even higher when doing aheadstand (Weinreb et al. 1984).
(4) Repeated IOP measurements:will lower IOP if performed overa short period of time.
(5) Certain drugs: IOP is raised byLSD but lowered by alcohol andcannabinoids.
(6) The cardiac cycle: causeschanges known as ocular pulseamplitude (OPA); these are usu-ally in the range 1–2 mmHg,although there can be larger dif-ferences between diastole andsystole.
(7) General anaesthesia: in children,it is common to use fluorinatedhydrocarbons such as sevofluraneand halothane (inhalation anaes-thetics), which lower IOP, or ke-tamine (e.g. intramuscularadministration), which increasesIOP. After procedures in whichintravitreal gases, for example,SF6 or perfluorocarbon, areused, nitrous oxide should not beadministered because it can dif-fuse into closed spaces, expandand interact with the intravitrealgas to markedly increase IOP(Yang et al. 2002; Astrom et al.2003).
MethodsMeasurement of IOP (tonometry) forclinical purposes is always taken fromoutside the eye, and thus the resultsobtained represent an estimation ofthe actual pressure inside the eye.Four fundamentally different mea-surement methods are in use today.Traditionally, we differ between inden-tation tonometry and applanationtonometry, which deform the corneathrough controlled force achieved byeither indentation (depression) orapplanation (flattening), respectively.Many tonometers combine both theseprinciples. Moreover, in recent years,
other techniques have been introducedthat are based on two additional con-cepts called contour-matching andrebound tonometry. An overview ofthe methods used to measure IOP waspublished in the journal Survey ofOphthalmology in 2008 (Kniestedtet al. 2008).
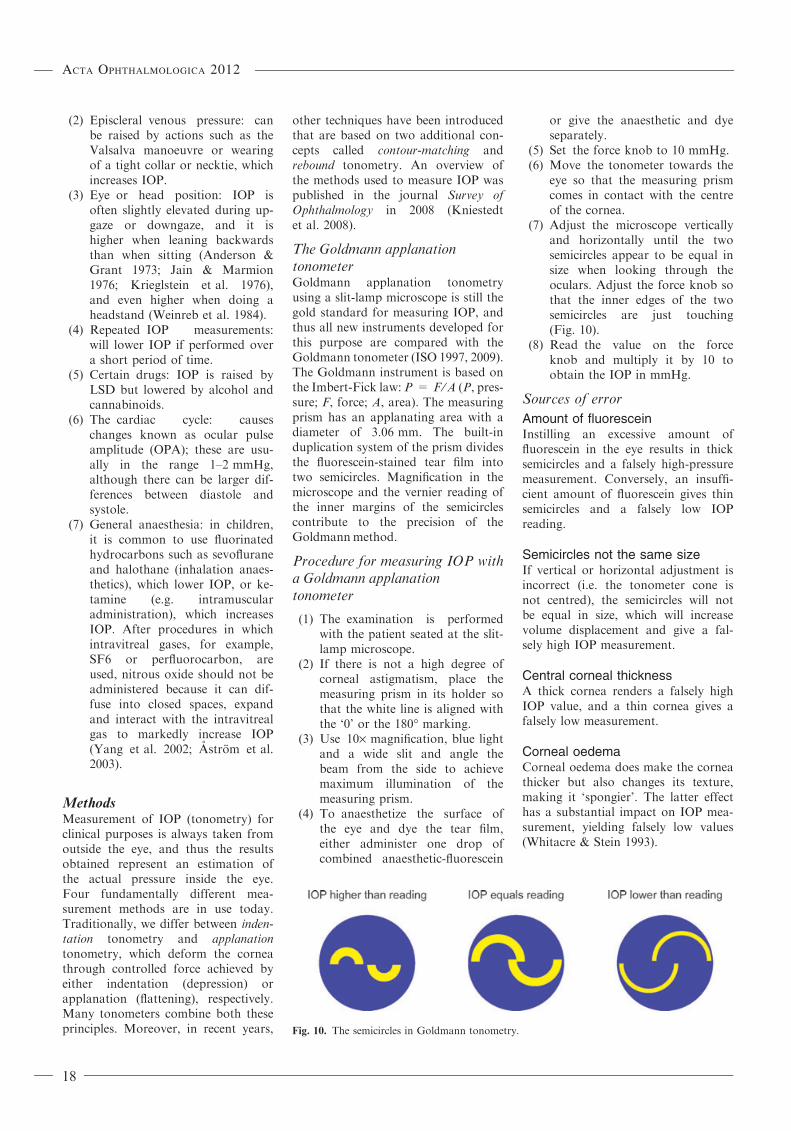
The Goldmann applanationtonometerGoldmann applanation tonometryusing a slit-lamp microscope is still thegold standard for measuring IOP, andthus all new instruments developed forthis purpose are compared with theGoldmann tonometer (ISO 1997, 2009).The Goldmann instrument is based onthe Imbert-Fick law: P = F ⁄A (P, pres-sure; F, force; A, area). The measuringprism has an applanating area with adiameter of 3.06 mm. The built-induplication system of the prism dividesthe fluorescein-stained tear film intotwo semicircles. Magnification in themicroscope and the vernier reading ofthe inner margins of the semicirclescontribute to the precision of theGoldmannmethod.
Procedure for measuring IOP witha Goldmann applanationtonometer
(1) The examination is performedwith the patient seated at the slit-lamp microscope.
(2) If there is not a high degree ofcorneal astigmatism, place themeasuring prism in its holder sothat the white line is aligned withthe ‘0’ or the 180� marking.
(3) Use 10· magnification, blue lightand a wide slit and angle thebeam from the side to achievemaximum illumination of themeasuring prism.
(4) To anaesthetize the surface ofthe eye and dye the tear film,either administer one drop ofcombined anaesthetic-fluorescein
or give the anaesthetic and dyeseparately.
(5) Set the force knob to 10 mmHg.(6) Move the tonometer towards the
eye so that the measuring prismcomes in contact with the centreof the cornea.
(7) Adjust the microscope verticallyand horizontally until the twosemicircles appear to be equal insize when looking through theoculars. Adjust the force knob sothat the inner edges of the twosemicircles are just touching(Fig. 10).
(8) Read the value on the forceknob and multiply it by 10 toobtain the IOP in mmHg.
Sources of error
Amount of fluoresceinInstilling an excessive amount offluorescein in the eye results in thicksemicircles and a falsely high-pressuremeasurement. Conversely, an insuffi-cient amount of fluorescein gives thinsemicircles and a falsely low IOPreading.
Semicircles not the same sizeIf vertical or horizontal adjustment isincorrect (i.e. the tonometer cone isnot centred), the semicircles will notbe equal in size, which will increasevolume displacement and give a fal-sely high IOP measurement.
Central corneal thicknessA thick cornea renders a falsely highIOP value, and a thin cornea gives afalsely low measurement.
Corneal oedemaCorneal oedema does make the corneathicker but also changes its texture,making it ‘spongier’. The latter effecthas a substantial impact on IOP mea-surement, yielding falsely low values(Whitacre & Stein 1993).
Fig. 10. The semicircles in Goldmann tonometry.
Acta Ophthalmologica 2012
18

Corneal curvatureIncreased refractive power leads tofalsely high IOP measurements andreduced refractive power results in fal-sely low values. A rule of thumb isthat a shift in refractive power of3 dioptres leads to a change in IOP ofapproximately 1 mmHg.
AstigmatismIf there is pronounced corneal astig-matism (>3D), it is recommendedthat the measuring prism be rotatedso that the negative cylinder axis isaligned with the red marking on theholder (i.e. 43�). A simpler approachis to take two pressure readings, onehorizontal and one vertical, and thencalculate the mean value.
Refractive surgeryMethods involving modification of thecornea to correct myopia (e.g. PRK,LASIK and LASEK) lead to underes-timation of IOP (Rosa et al. 1998;Johannesson et al. 2012).
ReproducibilityMeasurement results for an individualeye vary between repeated examina-tions. If the same examiner measurestwice on a particular eye, the resultswill differ by 2 mmHg or more in 8%of the cases. The corresponding pro-portion will be 40% if two differentexaminers conduct the measurements(Thorburn 1978).
Perkins� tonometerThe Perkins tonometer is a hand-held,portable version of the Goldmanninstrument that can be used with thepatient in a sitting or supine position.
‘Air-puff’ or noncontact tonometryThis method uses an air jet ofincreasing intensity to flatten thecornea. It is performed withoutanaesthesia. The measurements are ofsuch short duration that the ocularpulse exerts a significant effect. Oneof the drawbacks of noncontact to-nometry (NCT) is that the results aremore variable.
Ocular response analyser�
The Ocular response analyzer (ORA)is a further development of air-pufftonometry. It also measures cornealhysteresis, which in this contextdescribes the viscoelastic properties ofthe cornea.
Tonopen�
The Tonopen is a hand-held portabledevice. It is brought in contact withthe cornea, which is simultaneouslyapplanated by the central plunger.The force required to keep the plungerat the same level as the foot plate isrelated to the IOP. Each measurementrequires several applanations, andtopical anaesthesia is necessary.
Dynamic contour tonometry ⁄Pascal�
The Dynamic contour tonometry(DCT) instrument has a design similarto that of the Goldmann tonometerand is mounted on a biomicroscope.It has been claimed that this methodis less influenced by corneal proper-ties. The tonometer cone matches thecontour of the cornea, and the centralpiezoresistive pressure sensor, measur-ing the IOP, is thereby less influencedby extraneous forces. Even though itis the diastolic IOP that is measured,there is a tendency for assessments togive higher values than those obtainedby Goldmann tonometry. Further-more, differences are greater at lowerpressures (Schneider & Grehn 2006;Johannesson et al. 2008). Pressure isrecorded continuously, and hence it ispossible to monitor OPA. Some exam-iners find this technique more difficultto use compared with other methodsof measuring IOP (Chihara 2008;Johannesson et al. 2008).
Rebound tonometry ⁄ Icare�
Icare is a hand-held portable tonome-ter that measures IOP by rapidly pro-pelling a very thin metal probe out ofa magnetic field and bouncing it onthe cornea. The change in the speed ofthe probe as it bounces back is relatedto the IOP. On average, this methodgives higher IOP values compared toGoldmann tonometry (ElMallah &Asrani 2008; Johannesson et al. 2008).It can be performed without anaesthe-sia, and that feature, together with therelative simplicity of the technique,has made rebound tonometry a popu-lar choice in paediatric care.
Corneal thickness and pachymetry
Corneal thickness is known to affectthe results of IOP measurement (Gold-mann 1959; Doughty & Zaman 2000).A thin cornea gives a falsely low valueand is also considered to increase the
risk of developing glaucoma (Gordonet al. 2002). A meta-analysis hasshown that a deviation of 10% fromthe mean corneal thickness of 544 lm(measured by ultrasound pachymetry)represents a pressure difference of3.4 mmHg in healthy individuals(Doughty & Zaman 2000). Accordingto another model called the Dresdnercorrection table (Kohlhaas et al.2006), which is based on 125 cannulat-ed eyes, the applanation IOP valuethat is obtained should be adjusted byapproximately 1 mmHg for every25 lm of deviation from 550 lm.However, the results of different stud-ies vary substantially, and hence con-siderable caution should be observedwhen using any of the numerous for-mulas that exist for adjusting IOP inrelation to corneal thickness.
There are many methods for mea-suring corneal thickness, althoughultrasound pachymetry is the mostwidely applied technique when thereis suspicion of glaucoma. It is alsopossible to employ new instrumentssuch as Orbscan� or a Scheimpflugcamera, which not only measure cor-neal thickness, but also reveal theappearance of the cornea by use oftopographic and tomographic imag-ing. However, the results of differentmeasurement methods are not com-pletely comparable.
Goldmann applanation tonometry is stillthe gold standard for measuring intraocu-lar pressureAvoid frequent switching between meth-odsMeasurement of corneal thickness is asimple procedure that can be performedwith high precision
The cornea is thinnest at its centreand thicker in the periphery. If nototherwise stated, information givenusually concerns central corneal thick-ness (CCT). It has been found thatcorneal thickness is fairly stablethroughout life in white adults(Doughty & Zaman 2000). Thus, itseems that a single measurementshould suffice when considering glau-coma, as long as there is no reason tosuspect corneal oedema.
Methods
Ultrasound pachymetryMany different instruments are avail-able to conduct ultrasound pachyme-
Acta Ophthalmologica 2012
19
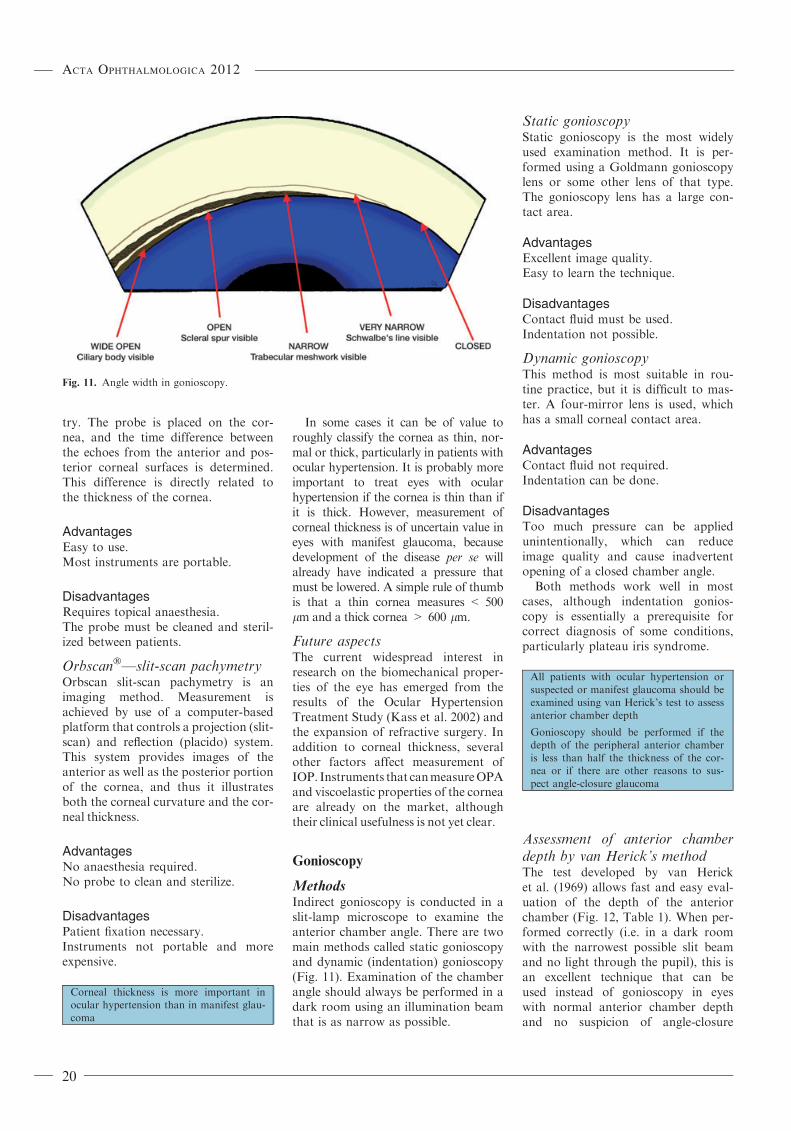
try. The probe is placed on the cor-nea, and the time difference betweenthe echoes from the anterior and pos-terior corneal surfaces is determined.This difference is directly related tothe thickness of the cornea.
AdvantagesEasy to use.Most instruments are portable.
DisadvantagesRequires topical anaesthesia.The probe must be cleaned and steril-ized between patients.
Orbscan�—slit-scan pachymetryOrbscan slit-scan pachymetry is animaging method. Measurement isachieved by use of a computer-basedplatform that controls a projection (slit-scan) and reflection (placido) system.This system provides images of theanterior as well as the posterior portionof the cornea, and thus it illustratesboth the corneal curvature and the cor-neal thickness.
AdvantagesNo anaesthesia required.No probe to clean and sterilize.
DisadvantagesPatient fixation necessary.Instruments not portable and moreexpensive.
Corneal thickness is more important inocular hypertension than in manifest glau-coma
In some cases it can be of value toroughly classify the cornea as thin, nor-mal or thick, particularly in patients withocular hypertension. It is probably moreimportant to treat eyes with ocularhypertension if the cornea is thin than ifit is thick. However, measurement ofcorneal thickness is of uncertain value ineyes with manifest glaucoma, becausedevelopment of the disease per se willalready have indicated a pressure thatmust be lowered. A simple rule of thumbis that a thin cornea measures < 500lm and a thick cornea > 600 lm.
Future aspectsThe current widespread interest inresearch on the biomechanical proper-ties of the eye has emerged from theresults of the Ocular HypertensionTreatment Study (Kass et al. 2002) andthe expansion of refractive surgery. Inaddition to corneal thickness, severalother factors affect measurement ofIOP. Instruments that canmeasureOPAand viscoelastic properties of the corneaare already on the market, althoughtheir clinical usefulness is not yet clear.
Gonioscopy
MethodsIndirect gonioscopy is conducted in aslit-lamp microscope to examine theanterior chamber angle. There are twomain methods called static gonioscopyand dynamic (indentation) gonioscopy(Fig. 11). Examination of the chamberangle should always be performed in adark room using an illumination beamthat is as narrow as possible.
Static gonioscopyStatic gonioscopy is the most widelyused examination method. It is per-formed using a Goldmann gonioscopylens or some other lens of that type.The gonioscopy lens has a large con-tact area.
AdvantagesExcellent image quality.Easy to learn the technique.
DisadvantagesContact fluid must be used.Indentation not possible.
Dynamic gonioscopyThis method is most suitable in rou-tine practice, but it is difficult to mas-ter. A four-mirror lens is used, whichhas a small corneal contact area.
AdvantagesContact fluid not required.Indentation can be done.
DisadvantagesToo much pressure can be appliedunintentionally, which can reduceimage quality and cause inadvertentopening of a closed chamber angle.
Both methods work well in mostcases, although indentation gonios-copy is essentially a prerequisite forcorrect diagnosis of some conditions,particularly plateau iris syndrome.
All patients with ocular hypertension orsuspected or manifest glaucoma should beexamined using van Herick’s test to assessanterior chamber depth
Gonioscopy should be performed if thedepth of the peripheral anterior chamberis less than half the thickness of the cor-nea or if there are other reasons to sus-pect angle-closure glaucoma
Assessment of anterior chamberdepth by van Herick’s methodThe test developed by van Hericket al. (1969) allows fast and easy eval-uation of the depth of the anteriorchamber (Fig. 12, Table 1). When per-formed correctly (i.e. in a dark roomwith the narrowest possible slit beamand no light through the pupil), this isan excellent technique that can beused instead of gonioscopy in eyeswith normal anterior chamber depthand no suspicion of angle-closure
Fig. 11. Angle width in gonioscopy.
Acta Ophthalmologica 2012
20

glaucoma (e.g. no pressure peaks orpain). Gonioscopy is recommended ifthe peripheral chamber depth is lessthan half the thickness of the cornea.If the depth is less than one-fourth ofthe corneal thickness, gonioscopymust be done on at least one occasionduring the course of the investigation.
The website http://www.gonioscopy.org provides all pertinent informationabout gonioscopy and is highly rec-ommended.
4 Principles forManagement of Glaucoma
Making a diagnosis
In many cases, confirming a diagnosisof glaucoma is a straightforward pro-cess based on typical changes in boththe optic disc and the visual field. How-ever, it can be difficult or nearly impos-sible to reach a diagnosis in some
patients, and factors that can hamperthis work include the following:
(1) Abnormal appearance of theoptic disc (often very small orvery large)
(2) Optic disc anomalies (e.g. hypo-plasia, myopia or optic disc dru-sen)
(3) Media opacities(4) Visual field measurement impos-
sible (in children, people withdementia or the very elderly)
(5) Previous eye diseases (e.g. retinalvessel occlusions)
Notwithstanding, a diagnosis is usu-ally confirmed by observation of com-bined damage to the optic nerve andvisual field, in many cases supportedby elevated IOP. To achieve a definitediagnosis, it can be stipulated that thedamage must be progressive. How-ever, this principle cannot be appliedin clinical practice, because it wouldtake too long to confirm progression.
Optic nerve damage with anormal visual fieldIf it is found that the optic disc showsglaucomatous damage despite normalresults of a visual field examination,the following should be considered:
(1) Is the optic disc (and its cup)unusually large? Such discs repre-sent a common explanation for
over-diagnosis of glaucoma (Heijl& Molder 1993). Are there con-vincing localized optic disc find-ings, such as notching or rimloss?
(2) Is the visual field examinationreliable? (This issue is discussedin Chapter 3.) A large proportionof false-positive (FP) responsesgive unreliable visual field results,although a high rate of false-neg-ative (FN) responses does notindicate an unreliable visual fieldin glaucomatous eyes.
Glaucoma can be present even if theresults of visual field testing are nor-mal. Confirmation of such ‘preperimet-ric’ glaucoma can be difficult and isbased entirely on evaluation of theappearance of the optic disc and ⁄or theretinal nerve fibre layer. Obviously,IOP plays an important role in thiscontext: elevated pressure increases thelikelihood of glaucoma.
In general, a large optic disc willhave a large physiologic cup, and asmall optic disc will have a smallphysiologic cup. Therefore, assessmentof disc size is fundamental in glau-coma diagnostics.
If there is doubt regarding the pres-ence of glaucoma, it is acceptable towait and follow development in mostpatients, possibly with the exception ofyoung people or those who have mark-edly elevated IOP. Indeed, if the IOP isnormal or only slightly increased, thereis good reason to defer treatment.
In almost all cases, a diagnosis of glau-coma is based on both optic disc andvisual field damage
Visual field damage with a normaloptic nerveWhen evaluating the results of avisual field test, it is important to bearin mind that appearance of the visualfield is never completely pathogno-monic of glaucoma. Arcuate nasaldefects that respect the nasal horizon-tal meridian are nearly always causedby glaucoma, especially if they arefound in both the superior and theinferior half of the field. Nonetheless,even such visual fields cannot withabsolute certainty be correlated withglaucoma disease.
If the visual field exhibits changesthat concur with glaucoma-induced
Fig. 12. Assessment of the peripheral anterior chamber depth using van Herick’s test. In this
case, the peripheral chamber depth is greater than half the thickness of the cornea.
Table 1. Estimation of the depth of the ante-
rior chamber according to van Herick.
Peripheral anterior chamber
depth compared with
corneal thickness
Degree
(Shaffer)
‡1 ⁄ 2 4
1 ⁄ 4–1 ⁄ 2 3
1 ⁄ 4 2
<1 ⁄ 4 1
0 0
Acta Ophthalmologica 2012
21

damage but the optic nerve appearsnormal, the following should be takeninto consideration:
(1) Is the optic disc unusually small?If so, is the cup disproportionatelylarge in relation to the diameter ofthe optic disc? A small disc gener-ally has a small physiologic cup orno cup at all, and even a smallcup can be associated with glauco-matous damage.
(2) Are there signs of optic disc dru-sen or other disc anomalies?
(3) Are there signs of present orpast retinal disease?
(4) Is the eye severely myopic?White atrophic retinal areas insuch eyes correspond with defi-nite visual field defects.
(5) Is it possible to assess the retinalnerve fibre layer? Under favour-able conditions, damage to thenerve fibre layer can be detectedeven if the optic disc appearsnormal.
(6) Was the patient co-operativeduring visual field testing? (Seeabove and Chapter 3.)
(7) Was the examination performedusing very inaccurate correction(e.g. +3 instead of )3)? Such anerror will result in a generaldecrease in sensitivity.
(8) Are there pronounced changes inthe ocular media (e.g. cataract)?Cataract does not give rise tolocal visual field defects (Hayashiet al. 2001) but does cause a gen-eral reduction in sensitivity.
(9) A relative afferent pupil defectdemonstrated by a swinging flash-light test indicates neuronalinjury. If there is asymmetric opticnerve damage, there is often a rel-ative afferent pupil defect in thedamaged or most damaged eye.Inasmuch as glaucoma is seldomstrictly symmetrical, this alsoapplies to bilateral disease (Kala-boukhova et al. 2007).
Instrumental examination of opticdisc topography and thickness ofthe retinal nerve fibre layerAs mentioned in the previous chapter(see p. 11), investigation of structuralchanges in the appearance of the opticdisc or the retinal nerve fibre layer is ofconsiderable value in diagnosis and ⁄ormonitoring of glaucoma. However,
computer-based examination of thedisc and the nerve fibre layer (e.g. usingHRT, GDx, or OCT) offers only mod-erate diagnostic accuracy (SBU, 2008),which is nonetheless comparable tothat achieved by glaucoma experts.Reliable long-term follow-up data arelacking with regard to the capacity ofavailable instruments to detect progres-sion of glaucoma.
Radiological investigationsToday, a large number of CT andMRI examinations are performed onpatients with suspected glaucoma,particularly if they have normal IOP.Those investigations nearly alwaysprove to be unnecessary, and theyare also experienced as unpleasant bythe patients and entail considerablecost to the health care system. Onthe other hand, it is not unusual thatconditions involving compression ofthe optic nerve or chiasm are errone-ously diagnosed as glaucoma, whichin some cases results in visual impair-ment that might have been preventedby correct diagnosis and treatment.Presence of optic disc changes thatare typical of glaucoma should be aprerequisite for confirming a diagno-sis of normal-tension glaucoma (seep. 10). Ordinarily, in the presence ofsuch optic disc changes, a radio-graphic investigation is not indicated(Greenfield 1999); normal-tensionglaucoma is not a diagnosis of exclu-sion. Visual field defects in theabsence of such optic nerve damageshould lead to further investigation,which can, among other things,include radiographic examination. Asalready mentioned, in cases involvingsuspected optic nerve damage, it isimportant to determine whether a rel-ative afferent pupil defect is present.If there is uncertainty regardingoccurrence of glaucomatous opticnerve damage, before decidingwhether a radiological examination isnecessary, it is advisable to performoptic disc photography, preferablyincluding the opinions of one ormore additional examiners.
A diagnosis of low or normal-tensionglaucoma is not a diagnosis of exclusion,that is, it can be made without moreextensive investigation in patients withvisual field defects and a glaucomatousoptic disc
General treatment principles
Goal of treatmentThe goal of glaucoma treatment is topreserve the patient’s visual functionand quality of life (QoL), not to main-tain IOP below a certain level. Studiesof QoL in glaucoma have often shownthat definite, measurable effects onQoL are relatively small and do notoccur until there are already extensivevisual field defects in the best eye(Wandell et al. 1997; Hyman et al.2005). However, other investigators(Varma et al. 2006) have suggestedthat even minor field defects havesome impact on QoL, and increasedrisk of slip-and-fall and traffic acci-dents has been observed in peoplewith minor to moderate loss of visualfunction (McGwin et al. 2005; Cole-man et al. 2007; Freeman et al. 2007;Haymes et al. 2007, 2008). Also, theright to drive a motor vehicle can beaffected by even relatively minorvisual field damage, if both eyes showfield defects.
If the aim of treatment is to main-tain QoL, it is obvious that effortsshould be made to ensure thatpatients do not lose 50% or more ofthe field of vision in the best eye dur-ing their lifetime. It is likely that thisgoal is not sufficiently stringentbecause of the above-mentioned fac-tors. Moreover, the instruments formeasuring QoL that are availabletoday may be far too insensitive.
Treatment methods and effectsIt is now well established that lower-ing IOP reduces the risk of visual fieldloss and decreases the rate of diseaseprogression (Collaborative Normal-Tension Glaucoma Study Group,1998b; Heijl et al. 2002). No sucheffects have been found for other ther-apeutic approaches, such as neuropro-tection or the use of saline ornifedipine to raise blood pressure inpatients with low-tension glaucoma.
Lowering IOP is effective in treatingglaucoma, both in patients whoseuntreated pressure is higher than thestatistically normal range and in casesof normal-tension glaucoma (Collabo-rative Normal-Tension GlaucomaStudy Group, 1998b; Heijl et al.2002). Reducing IOP also lessens therisk of developing glaucoma inpatients with ocular hypertension(Kass et al. 2002).
Acta Ophthalmologica 2012
22

The effect of reducing IOP isgreater than previously assumed. Inthe Early Manifest Glaucoma Trial(Leske et al. 2003), it was found thatevery 1-mmHg decrease in pressurelowered the risk of progression by 10–14%. Other studies have obtainedsimilar reduction in risk per mmHg ofpressure reduction (Chauhan et al.2008b) and also in ocular hyperten-sion (Gordon et al. 2002; Miglioret al. 2007a,b). Obviously, this doesnot imply that it is always best to tryto lower IOP as much as possible.However, studies in the literaturesuggest that if the IOP reductionachieved is not adequate (e.g. becauseprogression is too rapid at that IOPlevel), even reducing the pressurea few mmHg extra may be clearlybeneficial.
The goal of treatment in glaucoma is topreserve the patient’s visual function andquality of life
Reduction of intraocular pressure, evenbelow statistically normal levels, canretard progression of glaucoma
It seems that every 1-mmHg decrease inpressure can have an impact
Risk analysis and targetintraocular pressureThe risk of blindness, disability, orreduced QoL is greatest in patientswho already have extensive visual fielddamage in both eyes at the time ofdiagnosis. Conversely, the risk is lowin older patients who have limited orunilateral visual impairment. Clearly,age plays an important role, and thusyounger patients with visual fielddefects should always be regarded asbeing at risk of serious visual impair-ment during their lifetime. The rate ofprogression in the individual patientwill not be measurable until severalyears have passed, but can then beused to calculate the risk of futurevisual incapacity.
Increased intraocular pressure isanother important factor. Patientswith higher IOP are at increased riskof progression compared to patientswith lower IOP. It is also known thatthe natural history of progression ofopen-angle glaucoma is much morefavourable in normal-tension glau-coma then for primary open-angleglaucoma with elevated IOP (Heijlet al., 2009). Additional independent
risk factors include exfoliation syn-drome and optic disc haemorrhages(cf. pp. 21, 27, and 86).
The target pressure depends on allof the mentioned factors. Concur-rently, a proportional decrease inIOP from the untreated level isalmost invariably part of the defini-tion of target pressure, often incombination with a numerically des-ignated highest acceptable IOP. Thismeans that it should be possible toaccept somewhat higher tension inpatients who have a higher IOP atthe time of a glaucoma diagnosis,and, conversely, that lower targetIOP levels should be required inthose who have had lower pressuresduring development of the disease.
Thus, all of the following factorspoint towards a lower target IOP(and the opposite conditions suggesta somewhat higher target pressure):
(1) Younger age(2) Larger visual field defects(3) Lower untreated IOP(4) Exfoliation syndrome(5) Optic disc haemorrhages.
It is not possible to stipulate a numer-ical limit that can apply to all patientswith glaucoma. It was long assumedthat ‘normalization’ of IOP (to<21 mmHg) was equivalent to goodpressure control. However, even ifthere is now scientific evidence that amore ambitious approach should beused, it is probably best not to decideon any specific numerical recommen-dation that is intended to apply in allcases.
When diagnosing glaucoma, severaluntreated IOP measurements shouldbe made to better assess the effective-ness of the implemented therapy.
It is important to understand thatthe target pressure is dynamic. The var-ious formulae that are used to definetarget IOP, which often take theuntreated pressure into account, are ofgreatest interest when the patient hasjust received a diagnosis of glaucoma.After the patient has been under obser-vation for a few years, and the rate ofprogression can be estimated, it ismuch easier to determine whether thetarget pressure that was originally spec-ified can be regarded as correct. Inshort, the amount of visual field dam-age, the progression rate and the lifeexpectancy should be taken into con-sideration to help establish whether the
reduction in IOP has been sufficient orif a new target pressure must be stipu-lated at a level lower than the IOP mea-surements recorded during thetreatment period.
At diagnosis, lower target pressure is indi-cated by the following factors: youngerage, larger visual field defects, loweruntreated pressure, exfoliation and opticdisc haemorrhages
Rate of progressionGlaucoma is a progressive disease,and most patients show progressioneven if they receive treatment and IOPremains within the statistically normalrange. It is no longer particularly real-istic to assume that all deteriorationcan be prevented. However, it is alsoknown that the rate of progressionvaries markedly among patients, evenin those with the same IOP level, ageand other risk factors. A sizeableminority of treated patients with glau-coma exhibit rapid disease progres-sion, despite treatment and moderateIOP levels. Important goals of modernglaucoma care should be to identifythese patients in time to allow intensi-fication of treatment and also to esti-mate the rate of progression in allpatients. The European GlaucomaSociety (2008, p. 87) supports therecommendation of performing threevisual field tests annually during thefirst two years after diagnosis (Chau-han et al. 2008a), although measure-ments made every six months over thefirst three years can also provide agood estimation of the progressionrate.
The rate of progression varies substan-tially between patients
Frequent visual field testing duringthe first few years after diagnosis (e.g.six fields during the first two to threeyears) can help identify harmful progres-sion before damage has become tooextensive
Considering that the goal of glau-coma treatment is related to visualfunction, the rate of progression ofvisual impairment is of primary inter-est. Loss of vision is measured byrepeated visual field examinations,and thus it should be possible to esti-mate the progression rate after a fewyears of follow-up.
Acta Ophthalmologica 2012
23

Visual function affects QoL, andthus it seems logical to initially followthe patient by visual field testing.Documentation of the optic disc andretinal nerve fibre layer do not pro-vide the same possibility of assessingvisual disability, which is why thesemethods are usually not an alternativeto visual field measurements. The pri-mary reason for electing to documentthe optic disc and ⁄or retinal nervefibre layer is that such an approachcan provide an early warning of anychanges that occur during the courseof the disease. There is less need for aseries of examinations if optic discphotography is performed than ifvisual fields are used.
Once it is determined that apatient’s disease is progressing at adangerously rapid rate, and measureshave been taken to lower IOP more tohalt further deterioration, it is veryimportant, if possible, to re-examinethe patient at relatively short intervals(visual field testing two or three timesa year). That is the only way to ascer-tain whether the rate of progressionhas been reduced, or if the target pres-sure should be even lower. However,if the pressure is already at a levelthat is considered to be so low that itprobably cannot be reduced any fur-ther, it is obviously of little value tomonitor glaucoma damage by per-forming visual field tests or measuringthe optic disc or retinal nerve fibrelayer.
After a few years of follow-up, the rate ofprogression should be available based onrepeated visual field tests
Individualized glaucoma manage-
ment
Management of patients with glau-coma should always be individualized,and this applies to the choice of exam-ination techniques, as well as the fol-low-up interval and the treatmentprescribed. The objective is to preventvisual disability and an accompanyingdecrease in QoL, and hence the riskof visual impairment should be theprimary factor guiding the selection oftreatment and the frequency of moni-toring.
Groups of patients that are at onlylimited risk of serious disease can be
identified immediately, and theseinclude patients with unilateral diseaseor very old persons who have onlysmall visual field defects despite thepresence of bilateral disease. Individu-als with ocular hypertension, at leastif they are 70 years of age or older,constitute another group with onlyvery little risk of reduced QoL. At theother end of the spectrum are patientsat substantial risk of visual impair-ment, and these include individualsdiagnosed with significant bilateralvisual field defects or younger peoplewith field defects. A 60-year-oldpatient with bilateral field defectsmust be regarded as being at high riskof visual disability during his ⁄her life-time, even if the defects are initiallyrelatively small.
If measurement of the rate of diseaseprogression is reasonably accurate, it ispossible to extrapolate visual fielddevelopment for the number of yearsthe patient is expected to live. Ofcourse this estimation will be uncer-tain, although a linear extrapolationcan be regarded as the best predictionof the subsequent course of the diseaseif treatment remains unchanged(Bengtsson et al. 2009a). If suchextrapolation indicates that the patientis at risk of losing at least half of thevisual field in both eyes during his ⁄herlifetime, it can be concluded that thereis a very high risk of reduced QoLand ⁄or visual disability. It is essentialthat the fairly large number of patientswho fit this description be identifiedsufficiently early, and that treatmentand follow-up be performed at shorterintervals in these cases.
Glaucoma management should be indi-vidualized so that patients at higher riskof serious impairment will be treated andmonitored more extensively than those atlower risk
On the other hand, it is often war-ranted to lengthen the follow-up inter-val in patients who have been underprolonged observation and have ameasured rate of progression that ispresumed to entail a low risk of visualdisability, even in a lifelong perspec-tive. According to this line of think-ing, it is quickly apparent that longerfollow-up intervals (e.g. every otheryear) can be used in elderly patientswith ocular hypertension.
Overall assessment
In management of patients with glau-coma, it is essential to perform anoverall assessment of the developmentof the disease at intervals of a fewyears. This should include judgingwhether the rate of progression cancause concern about QoL (see the sec-tion above headed Rate of progression).If the progression rate is high andclearly suggests future visual disability,the IOP levels that were recorded dur-ing the follow-up period should be con-sidered, a substantially lower targetpressure should be chosen. Attemptsshould then be made to reach the des-ignated level, even if that can requireexpanding treatment in a way thatmight be problematic for the patient,for example, by necessitating usage ofseveral bottles with eye drops or expo-sure to the risks of surgery. If the rateof progression is possibly unsafe, treat-ment should be intensified, as long assuch an approach does not involve anyobvious disadvantages.
If the data are still inadequate toallow assessment of the rate of pro-gression, but the IOP seems unneces-sarily high and the patient is onmonotherapy, it can be necessary toincrease treatment. This strategy canalso be contemplated in a patient whois stable or shows only very slow pro-gression, if the IOP starts to increasecompared to earlier levels at whichdevelopment of the disease wasregarded as tolerable. Conversely, inan elderly patient who has been underobservation for a long period of timeand exhibits little damage or progres-sion, treatment can be reduced, if thepatient finds it difficult to managetaking eye drops or to tolerate harm-less and minor side-effects of the glau-coma treatment.
Such overall assessments can bemuch faster and easier, if they are per-formed by ophthalmologists or oph-thalmic nurses with extensiveexperience in this context. Also, it willdefinitely be beneficial if as manypatients with glaucoma as possiblecan be treated by professionals whohave special expertise and interest inglaucoma care. This is at least asimportant as the aspect of continuity,which is another important factoraffecting the quality of care.
Acta Ophthalmologica 2012
24

Overall assessment of the patient isimportant
Physicians as well as ophthalmic nursesplay an important role in glaucoma careSpecial interest and continuity of care arepositive factors
5 Treatment Methods
Pharmacological treatment of
glaucoma
The main objective of pharmacologi-cal treatment of glaucoma is to lowerIOP. That goal is achieved either byreducing the production of aqueoushumour or by increasing the outflowthrough the trabecular meshwork orthe uveoscleral pathway.
When selecting a therapeutic regi-men, several other factors besides apressure-reducing effect must be takeninto consideration, including possibleadverse effects, cost, QoL and thelikelihood of good compliance. Inmany cases, a preservative can causelocal reactions, and, if that occurs, itis preferable to prescribe unit-dosevials without preservatives. It has alsobeen assumed that a simpler dosageschedule, including fewer drop bottlesand instillations, can improve compli-ance, although the literature offerslittle support for that assumption(Gray et al. 2009).
Only approximately 20% of thecontent of an eye drop is absorbed bythe eye (Mishima 1981; Korte et al.2002). The amount that is absorbedby the nasopharyngeal mucosa has noeffect on the eye but can give rise togeneral side-effects. Using a siliconeplug to occlude the lacrimal ductreduces the overall uptake (Salminen1990) and markedly increases absorp-tion in the eye (Linden & Alm 1990).However, there is no evidence that theamount of drug that is actuallyabsorbed by the eye can be signifi-cantly increased by either closing theeye or applying pressure on the lacri-mal duct for one minute after admin-istering a drop of medication (Linden& Alm 1990).
The pharmaceutical preparationsthat were available in Sweden inautumn 2010 are described below (seealso Table 2). The values given repre-sent the maximum pressure-reducingeffect (the peak level) given as a percent of the untreated IOP and the
lowest pressure-reducing effect (thetrough level) measured soon beforetime for the next dose. These valueswere obtained from van der Valket al. (2005) in a meta-analysis of 27randomized studies of patients treatedfor at least 1 month with the drugs inquestion. For more detailed informa-tion about the individual medicationsinvestigated, see the Swedish Pharma-copeia (FASS). The classes of drugsthat are of interest here are discussedin the following sections.
Beta-receptor-blocking drugsThe ciliary body epithelium containsadrenergic beta receptors, chieflybeta-2 receptors, and stimulationincreases the production of aqueoushumour. Timolol is a nonselectivebeta adrenergic receptor blocker thatcan lower the production of aqueoushumour by 30–40% during daytime(Brubaker 1991). The relatively selec-tive beta-1 receptor antagonist be-taxolol presumably exerts its effect byblocking beta-2 receptors, but it isnot as efficacious as timolol (Gaulet al. 1989), which is also reflected byits effect on IOP. At night, the activ-ity of the adrenergic beta receptors isso low that a blocking agent has nosubstantial impact on the basal rateof aqueous humour production dur-ing that time (Topper & Brubaker1985; Brubaker 1991).
For timolol and betaxolol, the rec-ommended dose is once a day fordepot formulations and once or twicea day for solutions. Timolol at a con-centration of 0.008% (0.08 mg ⁄ml)has a measurable effect on IOP(Mottow-Lippa et al. 1990), and theeffect of a daily dose on IOP is thesame regardless of whether given inthe morning or at night (Letchingeret al. 1993). This suggests that instilla-tion of the lower dose once daily cansuffice for most eyes.
The systemic effect of topical beta-blockers is not negligible (Korte et al.2002), and timolol is contraindicatedin patients with asthma, serious lungdisease, uncompensated cardiac insuf-ficiencies, or grade II or III AV block.Betaxolol has the same cardiac con-traindications, and a certain degree ofcaution should be observed in patientswith asthma, even if the risk of clini-cally significant blockade of beta-2receptors in the lungs is small.
Prostaglandin analoguesCompared to the parent compoundprostaglandin F2 alpha (PGF2alpha),the analogues latanoprost, travo-prost, bimatoprost and tafloprost aremore selective for FP receptors (Stj-ernschantz 2001) and consequentlyhave less effect on blood vessels andcause less irritation (Stjernschantzet al. 2000). Prostaglandins lowerIOP by increasing the uveoscleraloutflow (Stjernschantz 2001). This isbrought about through a reductionin the collagen content of the ciliarymuscle, which in turn affects hydrau-lic resistance in the uveoscleral out-flow pathway (Sagara et al. 1999).This action is long-lasting, and thedrug should be given only oncedaily; in fact, more frequent adminis-tration reduces the effect (Alm et al.1995).
Prostaglandins are not believed tocause systemic side-effects. Theadverse reaction that has receivedmost attention is a colour change ofthe iris, which occurs in about one-third of eyes treated with latanoprost(Alm et al. 2004) but is considered tobe solely of cosmetic concern (Albertet al. 2008). The change in colour isattributed to an effect on melanin pro-duction, which can also lead to darkerand longer eyelashes and ⁄or increasedpigmentation of the skin of the eye-lids. In contrast to the altered colourof the iris, the effects on the eyelidsare reversible and disappear within afew months after withdrawal of thedrug. Conjunctival hyperaemia is seenin connection with all prostaglandinanalogues. Caution should also beobserved in eyes at increased risk ofintraocular inflammation, includingcystoid macular oedema.
SympathomimeticsThe adrenergic alpha-2 agonists apra-clonidine and brimonidine activate areceptor in the ciliary body epithe-lium, which reduces the production ofaqueous humour. Apraclonidineshould only be used temporarily toprevent a rise in IOP in patients whohave undergone argon laser trabecularsurgery or are scheduled for filteringsurgery. Brimonidine is a much moreselective adrenergic alpha-2 receptoragonist (Burke & Schwartz 1996), andit is also rather fat soluble and canpass through the blood–brain barrier.
Acta Ophthalmologica 2012
25
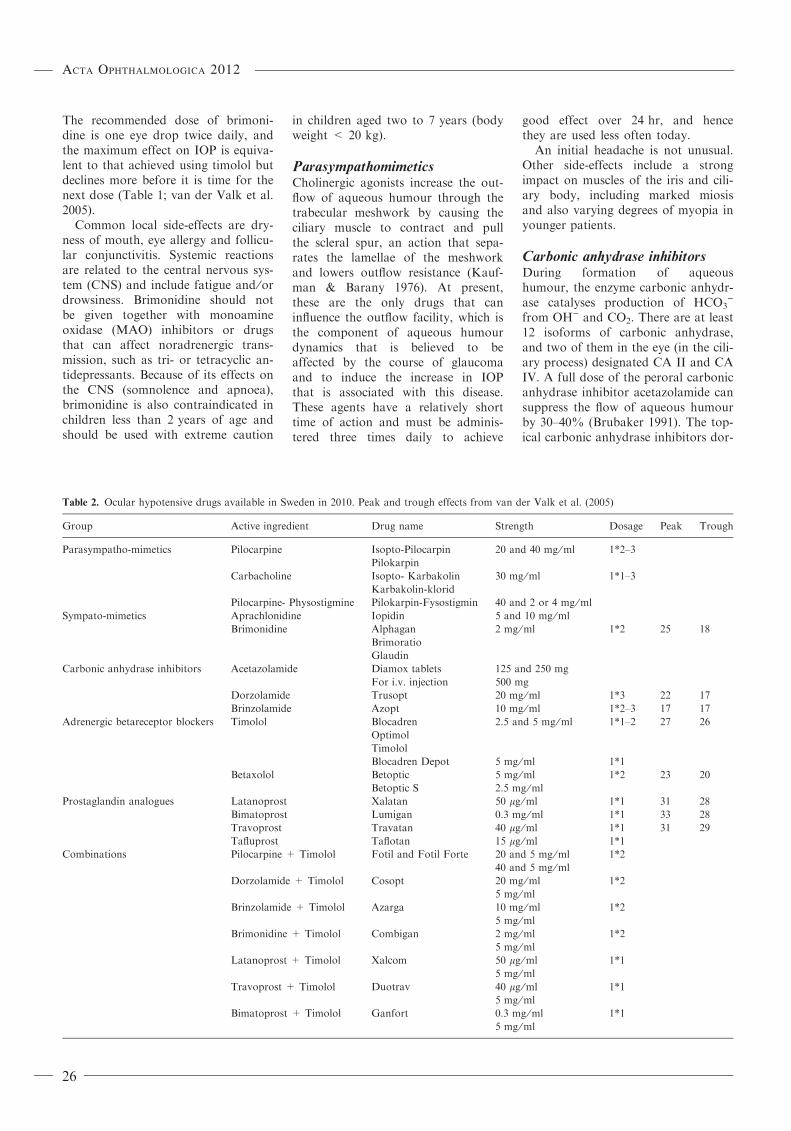
The recommended dose of brimoni-dine is one eye drop twice daily, andthe maximum effect on IOP is equiva-lent to that achieved using timolol butdeclines more before it is time for thenext dose (Table 1; van der Valk et al.2005).
Common local side-effects are dry-ness of mouth, eye allergy and follicu-lar conjunctivitis. Systemic reactionsare related to the central nervous sys-tem (CNS) and include fatigue and ⁄ordrowsiness. Brimonidine should notbe given together with monoamineoxidase (MAO) inhibitors or drugsthat can affect noradrenergic trans-mission, such as tri- or tetracyclic an-tidepressants. Because of its effects onthe CNS (somnolence and apnoea),brimonidine is also contraindicated inchildren less than 2 years of age andshould be used with extreme caution
in children aged two to 7 years (bodyweight < 20 kg).
ParasympathomimeticsCholinergic agonists increase the out-flow of aqueous humour through thetrabecular meshwork by causing theciliary muscle to contract and pullthe scleral spur, an action that sepa-rates the lamellae of the meshworkand lowers outflow resistance (Kauf-man & Barany 1976). At present,these are the only drugs that caninfluence the outflow facility, which isthe component of aqueous humourdynamics that is believed to beaffected by the course of glaucomaand to induce the increase in IOPthat is associated with this disease.These agents have a relatively shorttime of action and must be adminis-tered three times daily to achieve
good effect over 24 hr, and hencethey are used less often today.
An initial headache is not unusual.Other side-effects include a strongimpact on muscles of the iris and cili-ary body, including marked miosisand also varying degrees of myopia inyounger patients.
Carbonic anhydrase inhibitorsDuring formation of aqueoushumour, the enzyme carbonic anhydr-ase catalyses production of HCO3
)
from OH) and CO2. There are at least12 isoforms of carbonic anhydrase,and two of them in the eye (in the cili-ary process) designated CA II and CAIV. A full dose of the peroral carbonicanhydrase inhibitor acetazolamide cansuppress the flow of aqueous humourby 30–40% (Brubaker 1991). The top-ical carbonic anhydrase inhibitors dor-
Table 2. Ocular hypotensive drugs available in Sweden in 2010. Peak and trough effects from van der Valk et al. (2005)
Group Active ingredient Drug name Strength Dosage Peak Trough
Parasympatho-mimetics Pilocarpine Isopto-Pilocarpin
Pilokarpin
20 and 40 mg ⁄ml 1*2–3
Carbacholine Isopto- Karbakolin
Karbakolin-klorid
30 mg ⁄ml 1*1–3
Pilocarpine- Physostigmine Pilokarpin-Fysostigmin 40 and 2 or 4 mg ⁄ml
Sympato-mimetics Aprachlonidine Iopidin 5 and 10 mg ⁄ml
Brimonidine Alphagan
Brimoratio
Glaudin
2 mg ⁄ml 1*2 25 18
Carbonic anhydrase inhibitors Acetazolamide Diamox tablets
For i.v. injection
125 and 250 mg
500 mg
Dorzolamide Trusopt 20 mg ⁄ml 1*3 22 17
Brinzolamide Azopt 10 mg ⁄ml 1*2–3 17 17
Adrenergic betareceptor blockers Timolol Blocadren
Optimol
Timolol
2.5 and 5 mg ⁄ml 1*1–2 27 26
Blocadren Depot 5 mg ⁄ml 1*1
Betaxolol Betoptic
Betoptic S
5 mg ⁄ml
2.5 mg ⁄ml
1*2 23 20
Prostaglandin analogues Latanoprost Xalatan 50 lg ⁄ml 1*1 31 28
Bimatoprost Lumigan 0.3 mg ⁄ml 1*1 33 28
Travoprost Travatan 40 lg ⁄ml 1*1 31 29
Tafluprost Taflotan 15 lg ⁄ml 1*1
Combinations Pilocarpine + Timolol Fotil and Fotil Forte 20 and 5 mg ⁄ml
40 and 5 mg ⁄ml
1*2
Dorzolamide + Timolol Cosopt 20 mg ⁄ml
5 mg ⁄ml
1*2
Brinzolamide + Timolol Azarga 10 mg ⁄ml
5 mg ⁄ml
1*2
Brimonidine + Timolol Combigan 2 mg ⁄ml
5 mg ⁄ml
1*2
Latanoprost + Timolol Xalcom 50 lg ⁄ml
5 mg ⁄ml
1*1
Travoprost + Timolol Duotrav 40 lg ⁄ml
5 mg ⁄ml
1*1
Bimatoprost + Timolol Ganfort 0.3 mg ⁄ml
5 mg ⁄ml
1*1
Acta Ophthalmologica 2012
26

zolamide and brinzolamide are not asefficacious as acetozolamide (Mauset al., 1997), possibly by not com-pletely blocking both CA II and themembrane-bound CA IV (Larsson &Alm 1998).
Acetazolamide is given in the formof tablets at a dose of 0.5–1 g ⁄day.For dorzolamide and brinzolamide,the recommended dose is one droptwo to three times a day; the lowerdosage is sufficient if used in combina-tion with timolol, because timololreduces the flow of aqueous humourand thereby decreases the rate atwhich other drugs are removed fromthe eye.
Since carbonic anhydrase is presentin most tissues of the body, and aceta-zolamide is known to effectively inhibitmost isoforms of this enzyme, peroraltreatment with this drug causes dis-tressing adverse effects such as fatigue,paraesthesia, loss of appetite, nauseaand other gastrointestinal disturbances.Carbonic anhydrase inhibitors alsoincrease the risk of kidney stones,because they decrease urinary excretionof citrate, which in turn leads to higherrisk of calcium deposits in the urinarytract. These drugs are chemically simi-lar to sulphonamides and can result inagranulocytosis, thrombocytopeniaand aplastic anaemia. Furthermore,many patients discontinue treatment(Lichter et al. 1978), and therefore per-oral therapy is rarely prescribed today.
Dorzolamide and brinzolamide aregiven as eye drops, and, as expected,they are associated with a much lowerrisk of systemic side events. Patientswith serious kidney or liver damageshould not be treated with thesedrugs. Common adverse effectsinclude headache, a bitter taste in themouth and local irritation includingallergic reactions.
Combination preparationsAll combination eye drops include thebeta-blocker timolol together withsome other drug. Contraindicationsand adverse effects depend on thecomponents in the formulation.
Use in children and during preg-nancy and lactationWhen IOP-lowering treatment isdeemed necessary in a child or a preg-nant or nursing woman, there is littledata available on which to base a reli-
able assessment of the risks of foetaldamage or negative effects on thechild.
In most cases, treatment with eyedrops is considered to be associatedwith a low risk of foetal injury, par-ticularly with the drugs pilocarpineand timolol, which have long been inuse. Use of timolol eye drops duringpregnancy does not affect birthweight (Ho et al. 2009), and there isno evidence that the concentration oftimolol present in breast milkinvolves any risk for a healthy infant(Madadi et al. 2008). Accordingly, itis reasonable to regard timolol as thedrug of choice in pregnant womenwho have elevated IOP and are con-sidered to need pressure-loweringtherapy where laser treatment is notan option.
Topical beta-blockers at low con-centrations, topical carbonic anhydr-ase inhibitors and latanoprost are welltolerated by young children (Ott et al.2005; Coppens et al. 2009). Beta-blockers should obviously not be usedif there are contraindications to thesedrugs. Miotics are of little interestbecause of the effect they have on thelens. Also, adrenergic alpha-2 agonistsshould not be given to children aged2 years or younger, and they shouldbe used with caution in children whoare 2–7 years old or weigh less than20 kg because of possible adverseeffects on the CNS (Al-Shahwan et al.2005).
Treatment stages and strategiesInitially, only one drug is used. TheIOP-lowering effects and side-effectprofiles of the various medicationssuggest that timolol or a prostaglan-din analogue should be the first choicefor treatment, if there are no contrain-dications. The maximum pressure-reducing effect is usually reachedwithin one to two hours with most ofthe available drugs, except the prosta-glandin analogues, which show peakeffect after 6–8 hr (Alm & Villumsen1991). The effect of beta-blockers andprostaglandin analogues can persistfor several weeks after discontinuation(Schlecht & Brubaker 1988; Lindenet al. 1997).
Beta-blockers or prostaglandin analoguesare first choice alternatives if there are nocontraindications
Switch or addIf monotherapy does not achieve thetarget IOP, it is necessary to altertreatment either by testing a differentdrug or by adding another pressure-reducing agent. If monotherapy wasrecently initiated and has had goodeffect on IOP but has not succeededin reaching the target pressure, it isreasonable to add another drug.Alternatively, if the effect of the origi-nal therapy has been limited, the firststep should be to test some otherdrug. In both those cases, laser treat-ment can also be a suitable option. Insome patients, the IOP can rise afterprolonged successful treatment with aparticular drug, and it can be impossi-ble to ascertain whether this change isattributable to diminishing effect ofthe agent used or to increased resis-tance in the aqueous outflow pathway.Under such circumstances, it can beappropriate to add some other medi-cation, and later to try to withdrawthe drug that is currently in use, or toimmediately switch to another drug.
Combination treatmentsIn many cases, more than one drug isneeded to achieve a designated targetIOP, and various combinations ofproducts have been shown to providethe desired pressure reduction. Not-withstanding, the use of prostaglandinanalogues combined with cholinergicagonists such as pilocarpine has beenquestioned because contraction of theciliary body might prevent a prosta-glandin analogue from reaching itstarget – the ciliary muscle. However,the intense contraction of the ciliarymuscle is of short duration, and thepressure-lowering effect has beenfound to be additive (Fristrom& Nilsson 1993; Linden & Alm1997).
When combining two drugs tolower IOP, it is often recommendedthat agents with different modes ofaction be used, for example, one thataffects outflow and another that influ-ences production of aqueous humour.As of yet, no studies have been con-ducted to determine differencesbetween various drug combinationswith regard to their impact on pro-gression rate.
Prescriptions should as a rule notinclude more than two bottles of IOP-lowering eye drops for simultaneous
Acta Ophthalmologica 2012
27
use, because that can be difficult forpatients to manage and can lead tononcompliance. However, many com-bination drops containing two differ-ent active ingredients in the samebottle are currently available, and thesecan make it fairly easy for patients tohandle three active medications at thesame time. It can be assumed that add-ing a fourth agent will not provide anyappreciable enhancement of the pres-sure-reducing effect.
A dosage schedule should be simple tofacilitate compliance
For eye drops, more than two applica-tions a day and use of more than twobottles on each dosing occasion should beavoided if possible
Medical treatments other than
pressure reduction
In glaucoma treatment, considerablediscussion has focused on possiblepositive effects of two types of drugsthat do not influence IOP, namely,agents that increase blood flow andthose that have a potentially neuro-protective effect (i.e. prevent cell deathin nervous tissue). However, thus far,no studies have convincingly demon-strated that a drug that does notreduce IOP can have any impact onthe course of disease. Moreover, thereare no conclusive data showing thatthe glaucoma drugs that are presentlyin use have any effect on blood flowin the optic nerve or the retina (Costaet al. 2003).
The NMDA glutamate receptoragonist memantine is the only neuro-protective agent that has been testedin a randomized, blinded study onpatients with glaucoma. It is a regis-tered product (Ebixa�) for treatmentof mild Alzheimer’s disease. However,research has not shown any effect ofmemantine on the progression of glau-coma (Osborne 2009).
There is no evidence that treatment otherthan intraocular pressure–lowering canaffect the course of glaucoma
When are eye drops insufficient?
In patients whose disease progressesat a rate that can result in visual
impairment despite maximum treat-ment, or in those who have difficultyfollowing prescribed therapy, surgeryor laser treatment should be consid-ered if not already implemented.These alternatives should also beconsidered if eye drops cannotachieve sufficient pressure reductionwithout causing considerable side-effects.
In the short term, it is obvious thattreatment of glaucoma cannot beguided solely by visual field progres-sion, which is why the concept of tar-get IOP is used (see Risk analysis andtarget IOP in Chapter 4). Isolatedpressure measurements that are abovethe target level do not necessarily callfor adjustment of the therapeutic regi-men. However, if high pressures arerecorded on several occasions eventhough the patient is receiving what isjudged to be maximum treatment,there is reason to suspect inadequateefficacy or poor compliance. In thatsituation, laser treatment or surgeryshould be considered.
Laser treatment
LTP ⁄ALTHere, the terms argon laser trabecu-loplasty (ALT) and laser trabeculo-plasty (LTP) are used synonymously(Wise & Witter 1979).
Good knowledge of the anatomy ofthe anterior chamber angle is impor-tant in laser treatment (see the sectionheaded Gonioscopy on pages 20–21).When LTP was introduced, treatmentwas carried out on 360� of the ante-rior chamber angle. However, aneffect can be achieved by treating only180�, and thus it is suitable to startwith half the angle and wait with theother half (Fig. 13). The laser beam isapplied to the pigmented (anterior)portion of the trabecular meshwork.The power setting should cause onlylimited formation of gas bubbles andno visible whitening; if the mentionedeffects are more pronounced, thepower level is probably too high,which will increase the risk of periph-eral anterior synechiae (Rolim de Mo-ura et al. 2007). The parameters andtime-point of the treatment should benoted in the patient’s records to aidany subsequent supplementary treat-ment.
LTP parametersSpot size: 50 lmDuration: 0.1 secondsPower setting: varies depending on theequipment used, usually 400–1000 mW50 nonoverlapping laser pulses appliedover 180�
Laser trabeculoplasty can give rise towhat is usually only minor irritation ofthe iris, which can be handled by short-term treatment with a topical steroid ifnecessary. At least initially, the IOP-reducing therapy that the patient isalready receiving can remainunchanged, because it often takes froma few weeks up to a month or more forthe effect of LTP to become apparent.It is generally recommended that LTPshould not be repeated at the samelocation, because it is assumed thatsuch an approach can lead to moreextensive inflammation and a greaterrisk of increased IOP. As of yet, thereare no conclusive research results tosupport that suggestion.
Randomized controlled studies haveshown that LTP has a better IOP-reducing effect than can be achieved bythe older classes of eye drops. How-ever, investigations are needed to com-pare LTP with newer drugs such asprostaglandin analogues, brimonidineand topical carbonic anhydrase inhibi-tors (Rolim de Moura et al. 2007).
SLTSelective laser trabeculoplasty (SLT) isa newer type of LTP (Realini 2008)that requires the use of a Q-switched,frequency-doubled YAG laser. Onehundred laser spots are applied over360� of the trabecular meshwork,although, as in LTP, it is possible tobegin by treating only a smaller por-tion of the circumference (Chen et al.2004).
SLT parametersSpot size: 400 lmPulse duration: 3 nsPower setting: start at 0.8 mJ and thenadjust to the highest level at which no gasbubbles are formed
Selective laser trabeculoplasty hasproven to have an IOP-lowering effectequivalent to that of LTP (Damjiet al. 2006; Realini 2008) and eventhat of latanoprost (Nagar et al.2005). Selective laser trabeculoplasty
Acta Ophthalmologica 2012
28

delivers less energy to the trabecularmeshwork, and the theoretical advan-tage of this method is that it allowsrepeated treatment of the same area inthe meshwork. However, no con-trolled studies have yet been per-formed that can confirm thatassumption, even though SLT hasbeen available for many years.
Primary laser treatmentPrimary LTP has long been discussed(The glaucoma laser trial (GLT) 1990;Bergea et al. 1994), and it is definitelyan alternative, particularly if there isreason to avoid eye drops, such as inelderly patients who have difficultiesapplying that type of medication.
Diode laser cyclophotocoagulationTrans-scleral treatment of the ciliarybody using diode laser cyclophotoco-agulation is an alternative for treatingpatients with advanced glaucoma(Bloom et al. 1997; Walland 1998;Fankhauser et al. 2004). This methodis based on the same principle as cy-clocryotherapy (see p. 30), and it isused mainly on blind eyes andrequires adequate anaesthesia (e.g. ret-robulbar block or subtenonal anaes-thesia).
Parameters for cyclophotocoagulationperformed using an 810-nm IRIS diodelaser, blind eye
Duration: 2000 ms
Power setting: 1500–2000 mW
Approximately 20 pulses applied over360�; the G probe is placed on the borderof the limbus and is moved half the widthof the probe between each pulse
If a decision is made to use thismethod to treat an eye that still hasvision, greater caution should beobserved because of the risk of phthi-sis. Inflammation is one of the com-
mon complications of this laserapproach, which is why topical ste-roids should be used after the treat-ment. Less common complicationsinclude hypotonia and phthisis, andthere have also been reports of scleralperforation (Amariotakis et al. 2007),staphyloma (Prata et al. 2008), supra-choroidal haemorrhage (Tay et al.2006) and sympathetic ophthalmia(Roberts et al. 2009a).
Depending on local practice, manyinstitutions now use this method as analternative to shunts (Yildirim et al.2009). The advantage of a diode laseris that it entails a smaller and fasterintervention. The drawbacks are thatit is difficult to regulate, and severaltreatments are often required, whichcan lengthen the time needed for theseries of treatments.
Surgery
The main indication for filtering sur-gery is progression of glaucoma inwhich medical or laser treatment can-not provide adequate reduction inIOP. Accordingly, this procedure isnot the first choice for treatment ofglaucoma, primarily because of thelow, but real, risks of serious andvision-threatening complications thatare associated with surgery. On theother hand, it is clear that surgery ismore effective than both drug andlaser therapy in reducing IOP (Migdalet al. 1994; Lichter et al. 2001). Simi-lar to laser treatment, filtering surgerydoes not require patient compliance.The impact of compliance on drugtreatment of glaucoma is often a topicof discussion, although conclusivedata are lacking with regard to theeffect of poor compliance. Missing afew doses is probably of little conse-quence, because most of the drugsthat are used today have a residual
effect that is still apparent long afteradministration of the latest dose.
The risks associated with surgeryoften constitute the reason for post-poning a surgical procedure, which isregarded as a last resort. Two studies(Migdal et al. 1994; Lichter et al.2001) have compared filtering surgeryand drug therapy with respect to post-operative risks and effects on thecourse of disease. In both those inves-tigations, it was clearly demonstratedthat filtering surgery provided betterIOP reduction, and that the risksassociated with surgery were at anacceptable level. Nonetheless, overallassessment of the results of thosestudies has not yet been able to showthat filtering surgery is more beneficialthan treatment with medicines. TheAdvanced Glaucoma InterventionStudy (The advanced glaucoma inter-vention study (AGIS) 2000) conducteda post hoc analysis and found thatvisual fields were stable over a pro-longed period in most eyes that hadpersistently low IOP levels after sur-gery (i.e. pressure < 18 mmHg at allfollow-up visits). Also, the EMGTand other prospective studies (Heijlet al. 2002; Chauhan et al. 2008a,b)have shown that the risk of glaucoma-tous progression in treated eyesdecreases with each 1-mmHg reduc-tion in IOP. Together, these observa-tions indicate that it should presentlybe assumed that filtering surgeryoffers benefits that clearly justify therisks. This procedure should be con-sidered at an early stage in casesinvolving either initially very high IOPor progression occurring early in thecourse of the disease.
Surgical methodsRandomized controlled studies ofglaucoma surgery are often lacking,and thus the scientific knowledge basein this area is inadequate.
TrabeculectomyTrabeculectomy is the gold standardin glaucoma surgery (Sugar 1961;Cairns 1968; Linner 1970). Theunderlying principle is to construct anew pathway for aqueous humouroutflow. In short, an opening is cre-ated in the trabecular meshwork orperipheral cornea under a scleral flap,and the fluid is drained through theopening and then flows to the sub-
Fig. 13. Placement of the laser beam in argon laser trabeculoplasty.
Acta Ophthalmologica 2012
29
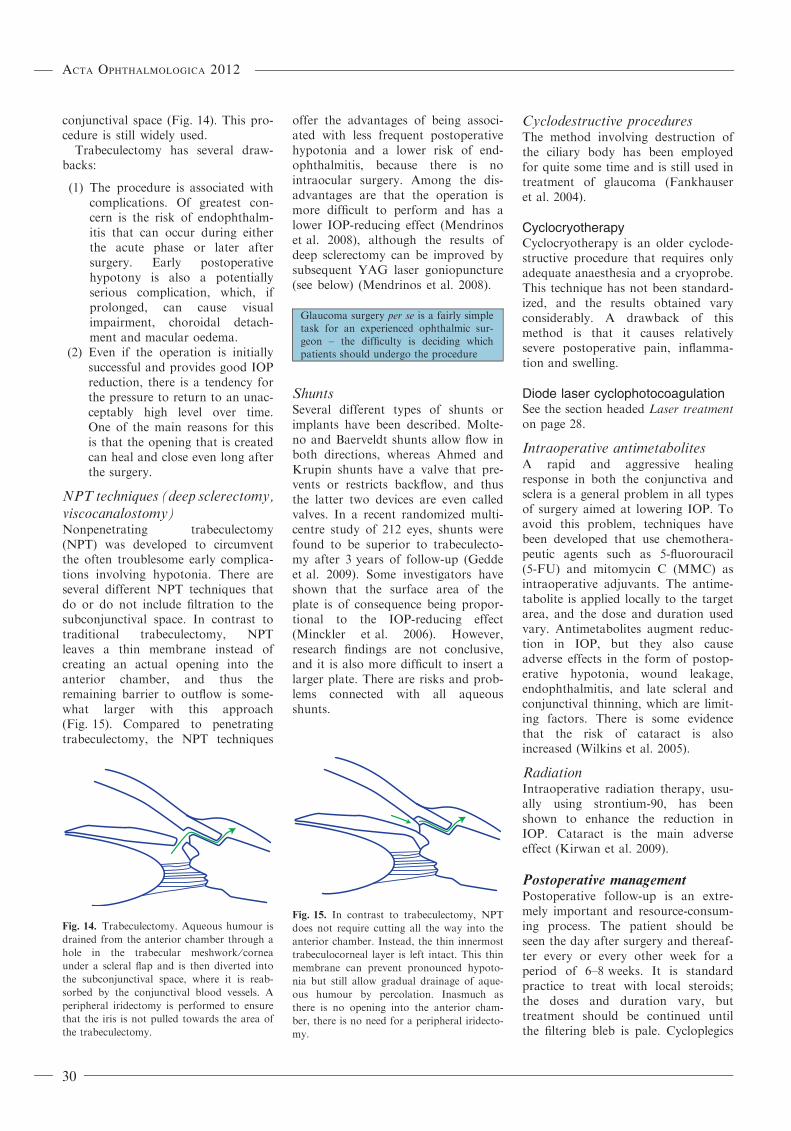
conjunctival space (Fig. 14). This pro-cedure is still widely used.
Trabeculectomy has several draw-backs:
(1) The procedure is associated withcomplications. Of greatest con-cern is the risk of endophthalm-itis that can occur during eitherthe acute phase or later aftersurgery. Early postoperativehypotony is also a potentiallyserious complication, which, ifprolonged, can cause visualimpairment, choroidal detach-ment and macular oedema.
(2) Even if the operation is initiallysuccessful and provides good IOPreduction, there is a tendency forthe pressure to return to an unac-ceptably high level over time.One of the main reasons for thisis that the opening that is createdcan heal and close even long afterthe surgery.
NPT techniques (deep sclerectomy,viscocanalostomy)Nonpenetrating trabeculectomy(NPT) was developed to circumventthe often troublesome early complica-tions involving hypotonia. There areseveral different NPT techniques thatdo or do not include filtration to thesubconjunctival space. In contrast totraditional trabeculectomy, NPTleaves a thin membrane instead ofcreating an actual opening into theanterior chamber, and thus theremaining barrier to outflow is some-what larger with this approach(Fig. 15). Compared to penetratingtrabeculectomy, the NPT techniques
offer the advantages of being associ-ated with less frequent postoperativehypotonia and a lower risk of end-ophthalmitis, because there is nointraocular surgery. Among the dis-advantages are that the operation ismore difficult to perform and has alower IOP-reducing effect (Mendrinoset al. 2008), although the results ofdeep sclerectomy can be improved bysubsequent YAG laser goniopuncture(see below) (Mendrinos et al. 2008).
Glaucoma surgery per se is a fairly simpletask for an experienced ophthalmic sur-geon – the difficulty is deciding whichpatients should undergo the procedure
ShuntsSeveral different types of shunts orimplants have been described. Molte-no and Baerveldt shunts allow flow inboth directions, whereas Ahmed andKrupin shunts have a valve that pre-vents or restricts backflow, and thusthe latter two devices are even calledvalves. In a recent randomized multi-centre study of 212 eyes, shunts werefound to be superior to trabeculecto-my after 3 years of follow-up (Geddeet al. 2009). Some investigators haveshown that the surface area of theplate is of consequence being propor-tional to the IOP-reducing effect(Minckler et al. 2006). However,research findings are not conclusive,and it is also more difficult to insert alarger plate. There are risks and prob-lems connected with all aqueousshunts.
Cyclodestructive proceduresThe method involving destruction ofthe ciliary body has been employedfor quite some time and is still used intreatment of glaucoma (Fankhauseret al. 2004).
CyclocryotherapyCyclocryotherapy is an older cyclode-structive procedure that requires onlyadequate anaesthesia and a cryoprobe.This technique has not been standard-ized, and the results obtained varyconsiderably. A drawback of thismethod is that it causes relativelysevere postoperative pain, inflamma-tion and swelling.
Diode laser cyclophotocoagulationSee the section headed Laser treatmenton page 28.
Intraoperative antimetabolitesA rapid and aggressive healingresponse in both the conjunctiva andsclera is a general problem in all typesof surgery aimed at lowering IOP. Toavoid this problem, techniques havebeen developed that use chemothera-peutic agents such as 5-fluorouracil(5-FU) and mitomycin C (MMC) asintraoperative adjuvants. The antime-tabolite is applied locally to the targetarea, and the dose and duration usedvary. Antimetabolites augment reduc-tion in IOP, but they also causeadverse effects in the form of postop-erative hypotonia, wound leakage,endophthalmitis, and late scleral andconjunctival thinning, which are limit-ing factors. There is some evidencethat the risk of cataract is alsoincreased (Wilkins et al. 2005).
RadiationIntraoperative radiation therapy, usu-ally using strontium-90, has beenshown to enhance the reduction inIOP. Cataract is the main adverseeffect (Kirwan et al. 2009).
Postoperative managementPostoperative follow-up is an extre-mely important and resource-consum-ing process. The patient should beseen the day after surgery and thereaf-ter every or every other week for aperiod of 6–8 weeks. It is standardpractice to treat with local steroids;the doses and duration vary, buttreatment should be continued untilthe filtering bleb is pale. Cycloplegics
Fig. 15. In contrast to trabeculectomy, NPT
does not require cutting all the way into the
anterior chamber. Instead, the thin innermost
trabeculocorneal layer is left intact. This thin
membrane can prevent pronounced hypoto-
nia but still allow gradual drainage of aque-
ous humour by percolation. Inasmuch as
there is no opening into the anterior cham-
ber, there is no need for a peripheral iridecto-
my.
Fig. 14. Trabeculectomy. Aqueous humour is
drained from the anterior chamber through a
hole in the trabecular meshwork ⁄ corneaunder a scleral flap and is then diverted into
the subconjunctival space, where it is reab-
sorbed by the conjunctival blood vessels. A
peripheral iridectomy is performed to ensure
that the iris is not pulled towards the area of
the trabeculectomy.
Acta Ophthalmologica 2012
30

and topical NSAIDs are also pre-scribed in some cases. If there is a ten-dency towards aggressive healing withan accompanying rise in IOP, the fol-lowing measures can be considered:massage, suture removal, needling, go-niopuncture and 5-FU injections. Useof any of those methods will requiremore frequent follow-up.
MassageEarly occlusion of the surgically cre-ated drainage opening can occurbecause of formation of a clot or afibrous plug, and can be removed bymassaging the eye with the patientseated at a slit lamp. The eyelid iskept closed, and a clean finger or acotton-tipped applicator is used tomassage the globe on and around thescleral flap. Alternatively, a sterileglass rod can be applied directly onthe globe.
Suture removalThe commonly used scleral sutures(e.g. 10-0 nylon) are dark in colourand thus can easily be removed usinga laser, if the surgical area is not hid-den by blood or an oedematous con-junctiva. A burning laser (e.g. anargon laser) is used to melt andthereby cut sutures. The procedurecan be facilitated using a tool such asthe tip of a glass rod or a speciallydesigned Hoskins lens to push sur-rounding tissue out of the way.
Parameters for laser suture lysis.
Spot size: 50–100 lm
Duration: 0.1–0.2 seconds
Power: moderate (200–400 mW)
Releasable and adjustable suturesIf releasable or adjustable sutures areused during surgery, it will later beeasy to remove or adjust them by useof a forceps and a slit lamp. A largenumber of different suture knots havebeen described (de Barros et al. 2008).
NeedlingTo open up an encapsulated filteringbleb, the patient should be seated ata slit lamp (or lying on an operatingtable) and given topical anaesthesia(drops). A very fine hypodermic nee-dle is inserted in the conjunctiva toreach the filtering bleb, where it isused to puncture or cut open either
the conjunctiva or the sclera (underthe scleral flap). This is performedto improve drainage from the trabe-culectomy or other routes. The alter-native method of using IOP-reducingeye drops to treat eyes with anencapsulated bleb can provideequally satisfactory results. Notably,according to the Cochrane Collabo-ration, only one randomized studyhas been performed in this area thusfar (Feyi-Waboso & Ejere 2004), andit actually showed that a better out-come was achieved with eye dropsthan by needling.
YAG laser goniopunctureYAG laser goniopuncture can only beperformed after NPT, because NPTleaves a thin membrane consisting ofthe innermost trabeculocorneal layer.With the aid of the gonioscopy lens,the laser is used to create a hole in themembrane and thereby improve filtra-tion. In some cases, the effect that isachieved can continue long (up toyears) after surgery. It is often neces-sary to use a surprisingly high energylevel with this technique.
Postoperative 5-FUThe methods described above can becombined with repeated postoperativeinjections of 5-FU, which are givenunder the conjunctiva after anaes-thetic eye drops, with the patientseated at a slit lamp. Corneal erosionsare the most common adverse effect,and thus it is necessary to examine forsuch erosions before each injection. Iferosions do occur, the injections mustbe discontinued. A study has shownthat 5-FU can improve IOP reduction,if it is administered as five 5-mg injec-tions, but not if it is given at a lowerdosage or in fewer injections (Worm-ald et al. 2001).
Postoperative follow-up is particularlyimportant and requires relatively extensiveresources, because both glaucoma surgeryand the postoperative course vary mark-edly, thus necessitating more frequentmonitoring and readiness to implementpostoperative measures
Unfortunately, few randomized controlledstudies have been performed, and thusmuch still depends on the experience androutine of the surgeon
The Moorfields Safe Surgery System web-site is very helpful: http://www.ucl.ac.uk/ioo/research/khawlibrary.htm
6 Management ofSuspected Glaucoma andOcular Hypertension
Many patients with suspected glau-coma are monitored at eye care cen-tres. Ocular hypertension is the mostcommon cause, but suspect glaucomacan occur also without an elevatedIOP. Such cases of suspect glaucomausually involves eyes with large physi-ologic cups, suspected notching ordefects in the retinal nerve fibre layer.As a rule, patients who fit thisdescription should not be treatedunless, of course, they have manifestglaucoma with visual field loss.
Ocular hypertension
Ocular hypertension is defined as ele-vated IOP (>21 mmHg) that is notaccompanied by damage to the visualfield, the optic disc or the retinalnerve fibre layer. Ocular hypertensionis more common than manifest glau-coma, and the risk of developing glau-coma is five times greater in patientswith ocular hypertension than in thosewith normal IOP (Ekstrom 1993). TheOcular Hypertension Treatment Study(OHTS) included eyes with IOP levelsof 24–32 mmHg, and damage wasfound in 9.5% of the untreated eyesafter a mean follow-up time of6 years, although more than half ofthose eyes still had normal visualfields (Kass et al. 2002). The risk ofglaucoma is greater at higher IOPand ⁄or if the central corneal thicknessis low (Gordon et al. 2002).
Patients whose IOP levels frequentlyexceed 25 mmHg should be offeredannual or biennial follow-up as longas the elevated pressure persists.Treatment should be considered if theIOP is above 28–30 mmHg or exfolia-tion is present (see below). Age shouldalso be taken into consideration: thereis more reason to treat youngerpatients. Follow-up examinationsshould be done at intervals of one totwo years and should aim to identifypossible glaucomatous damage byincluding repeated visual field testingor imaging of the optic disc.
Eyes with IOP levels above35 mmHg have not been included inthe studies mentioned above. Sucheyes require more frequent monitor-ing (initially every three months) or
Acta Ophthalmologica 2012
31

treatment. Patients who have bothocular hypertension and exfoliationsyndrome represent a special riskgroup. Compared to eyes that haveneither exfoliation syndrome nor ocu-lar hypertension, eyes that have onlyexfoliation syndrome are at 5–10times greater risk of developing glau-coma, and those with both ocularhypertension and exfoliation are at50 times greater risk of glaucoma(Ekstrom 1993) and in many casesalso show glaucomatous damageafter 10 years (Grødum et al. 2005).Exfoliation syndrome with normalIOP occurs in a very large propor-tion of the elderly population(Astrom et al., 2007), and thus it isnot realistic to offer this group regu-lar eye examinations.
Suspicious optic discs
The size of the optic disc should bedetermined if an eye is found to havea large physiologic cup, because mea-surements of these two structures arestrongly correlated in normal eyes(Bengtsson 1976). Normal optic discsthat are large are often mistakenlyclassified as glaucomatous (Heijl &Molder 1993), and hence the term pre-perimetric glaucoma should be usedwith particular caution if the IOP isnormal. In many people, asymmetriccups are the result of different sizedoptic discs (Bengtsson 1980). Accord-ingly, if glaucoma is suspected on thebasis of cup asymmetry, the patient’soptic disc sizes should be measured. Ifdisc diameters differ between eyes, itis highly likely that the person doesnot have glaucoma.
Optic disc haemorrhage
Optic disc haemorrhages are probablymore significant than a slightly ele-vated IOP as a risk factor for glauco-matous damage. Eyes with suchhaemorrhages but no visual fielddefects should be examined at inter-vals of several years.
Exfoliation syndrome
In Sweden, exfoliation syndrome iscommon in older people and is highlyprevalent among the elderly (Astrom& Linden 2007). Therefore, a patientwith exfoliation but normal IOP does
not need to undergo regular examina-tions, whereas the situation is com-pletely different if the IOP is elevated(Grødum et al. 2005), as discussedabove.
Glaucoma and positive family
history
Knowledge concerning inheritance ofglaucoma is increasing rapidly, but asof yet that information is of littlevalue in routine clinical practice.Many patients with glaucoma areelderly and do not know or cannotremember whether any of their rela-tives had the disease. Furthermore,glaucoma is still frequently confusedwith cataract. Indeed, there is seldomconvincing data to support the advicegiven and examinations performed.For clinical use, it can be appropriateto limit the definition of a family his-tory of glaucoma to having at leastone first-degree relative (parent, sib-ling or child) who has (or has had)some form of the disease as an adult.If resources are available, people whoare over 50 years of age and have afamily history of glaucoma should beoffered an ophthalmic investigation.Increased intraocular pressure mea-surement alone is not sufficient; it isalso necessary to conduct one ormore tests that can detect glaucoma-tous damage, such as visual fieldanalysis or evaluation of the opticdisc and retinal nerve fibre layer. Ifthe results of all tests are normal, theperson in question can be offered fur-ther examination every 5 years.Examinations should be done moreoften in families that have severalmembers with glaucoma, especially ifthe disease appeared at a youngerage. When examining people whohave a history of glaucoma (most ofwhom are healthy), it is important toperform tests that provide high speci-ficity and instead accept lower sensi-tivity. A visual field screeningtechnique is suitable for this purpose(see p. 13).
If patients with a family history ofglaucoma are to be referred to anoptometrist or optician for examina-tions, this professional should be ablenot only to measure IOP, but also toperform visual field testing and ⁄oroptic disc photography. Developmentof such co-operation agreements must
be guided by local availability ofresources and circumstances.
The examination protocol should beplanned locally with regard to contentand the person or persons in charge,and also with the understanding thatit must be designed to identify glauco-matous damage and thus cannotinclude only tonometry.
Encourage patients with glaucoma tourge their siblings and children to haveregular examinations for glaucoma afterthe age of 50.
Recommend that an examination be doneevery 5 years.
7 Population Screeningand Case Finding
Many patients with glaucoma alreadyhave serious visual impairment at thetime they are diagnosed with the dis-ease, which is a major problem, par-ticularly because the risk ofpermanent visual disability is greatestwhen diagnosis is made at a late stage(Chen 2004). In a study conducted inMalmo (Grødum et al. 2004), it wasfound that patients with glaucomatousdamage in both eyes at the time ofclinical diagnosis had, on average, lostmore than half of the visual field inthe worst eye. By comparison, visualimpairment was much less extensive inpatients identified by screening.Indeed, a fairly significant number ofpatients with normal-tension glau-coma revealed by screening had beenmissed in previous clinical examina-tions performed because of a positivefamily history of glaucoma. It is wellknown that at least 50% of peoplewith glaucoma remain undiagnosed indeveloped countries.
It is essential that glaucoma is diag-nosed at earlier stages than today, andthere is certainly more to gain here,than by trying to achieve earlier diag-nosis in patients who are already underobservation because of suspected glau-coma (e.g. because they have ocularhypertension). Today, suspicion of thisdisease is usually based on tonometryresults (Quigley & Jampel 2003), butthis is not sufficient.
Tonometry performed by anoptometrist or optician can identifysome patients, but that is not a com-plete solution to the problem, becausethe majority of people with undetected
Acta Ophthalmologica 2012
32

glaucoma have normal or only slightlyelevated IOP values. To be able toidentify the unidentified cases, we can-not recommend that a low limit forIOP be used as a prerequisite forreferral to an ophthalmologist. Suchan approach would result in a largenumber of ‘false alarms’, which inturn would reduce the amount ofresources available for patients whoactually have glaucoma.
The following can be recommendedto enable earlier diagnosis of glau-coma:
(1) Consistently encourage patientswith glaucoma to urge their chil-dren and siblings to have regularexaminations for glaucoma afterthey reach the age of 50.
(2) Examine the optic disc consider-ing the possibility of glaucoma inall who are over the age of 60,who are undergoing an ophthal-mic examination.
(3) Population screening should beinvestigated but cannot be rec-ommended at present (Wilsonet al. 2006).
Ad (1) This examination should notconsist solely of tonometry.
Ad (2) For example, all cataractpatients.
Ad (3) It is important that all popu-lation screening for glaucomabe limited to certain riskgroups. For example, theprevalence of undetected glau-coma at younger ages is solow that screening peopleunder the age of 60 years canhardly be justified. The inci-dence of glaucoma is also low,and thus frequent screeningexaminations are unnecessary(Stoutenbeek et al. 2008). Fur-thermore, it is essential to usehighly specific methods tostrongly limit the number offalse-positive cases. Since veryhigh specificity cannot becombined with high sensitiv-ity, it must be accepted thatscreening will not detect allcases of very early or earlyglaucoma. On the other hand,it is hardly acceptable to usescreening methods that canfail to detect more advancedglaucomatous damage. Beforepopulation screening can berecommended, it must be eval-
uated in large-scale studiesconducted in the same settingas where it will be undertakenin the future, such as atoptometry services.
References
Airaksinen PJ & Nieminen H (1985): Retinal
nerve fiber layer photography in glaucoma.
Ophthalmology 92: 877–879.
Albert DM, Gangnon RE, Grossniklaus HE,
Green WR, Darjatmoko S & Kulkarni AD
(2008): A study of histopathological fea-
tures of latanoprost-treated irides with or
without darkening compared with non-la-
tanoprost-treated irides. Arch Ophthalmol
126: 626–631.
Alm A & Villumsen J (1991): PhXA34, a new
potent ocular hypotensive drug. A study
on dose-response relationship and on aque-
ous humor dynamics in healthy volunteers.
Arch Ophthalmol 109: 1564–1568.
Alm A, Widengard I, Kjellgren D, Soder-
strom M, Fristrom B, Heijl A & Stjers-
chantz J (1995): Latanoprost administered
once daily caused a maintained reduction
of intraocular pressure in glaucoma
patients treated concomitantly with timo-
lol. Br J Ophthalmol 79: 12–16.
Alm A, Schoenfelder J & McDermott J
(2004): A 5-year, multicenter, open-label,
safety study of adjunctive latanoprost ther-
apy for glaucoma. Arch Ophthalmol 122:
957–965.
Al-Shahwan SM, Al-Torbak AA, Turkmani
SM, Al-Omran MM, Al-Jadaan IM &
Edward DP (2005): Side-effect profile of
brimonidine tartrate in children. Ophthal-
mology 112: 2143–2148.
Amariotakis G, Ressiniotis T, Voros GM &
Birch M (2007): Scleral perforation after
trans-scleral cyclodiode laser for intraocu-
lar pressure reduction. Clin Experiment
Ophthalmol 35: 290–291.
Anderson DR & Grant WM (1973): The
influence of position on intraocular pres-
sure. Invest Ophthalmol 12: 204–212.
Artes PH, Iwase A, Ohno Y, Kitazawa Y &
Chauhan BC (2002): Properties of perimet-
ric threshold estimates from full threshold,
SITA standard, and SITA fast strategies.
Invest Ophthalmol Vis Sci 43: 2654–2659.
Astrom S & Linden C (2007): Incidence and
prevalence of pseudoexfoliation and open-
angle glaucoma in northern Sweden: I.
Baseline report. Acta Ophthalmol Scand
85: 828–831.
Astrom S, Kjellgren D, Monestam E &
Backlund U (2003): Nitrous oxide anesthe-
sia and intravitreal gastamponade. Acta
Anaesthesiol Scand 47: 361–362.
Astrom S, Stenlund H & Linden C (2007):
Incidence and prevalence of pseudoexfolia-
tions and open-angle glaucoma in northern
Sweden: II. Results after 21 years of fol-
low-up. Acta Ophthalmol Scand 85: 832–
837.
Aulhorn E (1967): Early visual field defects in
glaucoma: I Leydhecker W (redaktor) glau-
coma, Tutzing symposium, sid. 151–86.
Karger Basel.
de Barros DS, Gheith ME, Siam GA & Katz
LJ (2008): Releasable suture technique. J
Glaucoma 17: 414–421.
Bendel RE, Kaplan J, Heckman M, Fredrick-
son PA & Lin SC (2008): Prevalence of
glaucoma in patients with obstructive sleep
apnoea – a cross-sectional case-series. Eye
22: 1105–1109.
Bengtsson B (1976): The variation and
covariation of cup and disc diameters. Acta
Ophthalmol (Copenh) 54: 804–818.
Bengtsson B (1980): The alteration and asym-
metry of cup and disc diameters. Acta
Ophthalmol (Copenh) 58: 726–732.
Bengtsson B (1981): The prevalence of glau-
coma. Br J Ophthalmol 65: 46–49.
Bengtsson B (1989): Incidence of manifest
glaucoma. Br J Ophthalmol 73: 483–487.
Bengtsson B & Heijl A (1998): SITA fast, a
new rapid perimetric threshold test.
Description of methods and evaluation in
patients with manifest and suspect glau-
coma. Acta Ophthalmol Scand 76: 431–
437.
Bengtsson B & Heijl A (2000a): Acceptable
frequencies of false answers in computer-
ized perimetry. Abstract ARVO. Invest
Ophthalmol Vis Sci 41: 478.
Bengtsson B & Heijl A (2000b): False-nega-
tive responses in glaucoma perimetry: indi-
cators of patient performance or test
reliability. Invest Ophthalmol Vis Sci 41:
2201–2204.
Bengtsson B & Heijl A (2005b): Diurnal IOP
fluctuation: not an independent risk factor
for glaucomatous visual field loss in high-
risk ocular hypertension. Graefes Arch Clin
Exp Ophthalmol 243: 513–518.
Bengtsson B, Olsson J, Heijl A & Rootzen H
(1997): A new generation of algorithms for
computerized threshold perimetry, SITA.
Acta Ophthalmol Scand 75: 368–375.
Bengtsson B, Patella VM & Heijl A (2009a):
Prediction of glaucomatous field loss by
extrapolation of linear trends. Arch Oph-
thalmol 127: 1610–1615.
Bengtsson B, Leske MC, Yang Z & Heijl A
(2009b): Disc hemorrhages and treatment
in the early manifest glaucoma trial. Oph-
thalmology 115: 2044–2048.
Bergea B, Bodin L & Svedbergh B (1994):
Primary argon laser trabeculoplasty vs
pilocarpine. II: long-term effects on intra-
ocular pressure and facility of outflow.
Study design and additional therapy. Acta
Ophthalmol (Copenh) 72: 145–154.
Bloom PA, Tsai JC, Sharma K, Miller MH,
Rice NS, Hitchings RA & Khaw PT
(1997): ’’Cyclodiode’’ trans-scleral diode
laser cyclophotocoagulation in the treat-
ment of advanced refractory glaucoma.
Ophthalmology 104: 1508–1519. discussion
1519–20.
Borger PH, van Leeuwen R, Hulsman CA,
Wolfs RC, van der Kuip DA, Hofman A
& de Jong PT (2003): Is there a direct asso-
Acta Ophthalmologica 2012
33

ciation between age-related eye diseases
and mortality? The Rotterdam study Oph-
thalmology 110: 1292–1296.
Brubaker RF (1991): Flow of aqueous humor
in humans [the Friedenwald lecture]. Invest
Ophthalmol Vis Sci 32: 3145–3166.
Budenz DL, Rhee P, Feuer WJ, McSoley J,
Johnson CA & Anderson DR (2002): Sen-
sitivity and specificity of the Swedish inter-
active threshold algorithm for
glaucomatous visual field defects. Ophthal-
mology 109: 1052–1058.
Burke J & Schwartz M (1996): Preclinical
evaluation of brimonidine. Surv Ophthal-
mol 41(Suppl 1): S9–S18.
Cairns JE (1968): Trabeculectomy. Prelimin-
ary report of a new method. Am J Oph-
thalmol 66: 673–679.
Chauhan BC, House PH, McCormick TA &
LeBlanc RP (1999): Comparison of con-
ventional and high-pass resolution perime-
try in a prospective study of patients with
glaucoma and healthy controls. Arch Oph-
thalmol 117: 24–33.
Chauhan BC, Garway-Heath DF, Goni FJ,
Rossetti L, Bengtsson B, Viswanathan AC
& Heijl A (2008a): Practical recommenda-
tions for measuring rates of visual field
change in glaucoma. Br J Ophthalmol 92:
569–573.
Chauhan BC, Mikelberg FS, Balaszi AG, Le-
Blanc RP, Lesk MR & Trope GE (2008b):
Canadian glaucoma study: 2. risk factors
for the progression of open-angle glau-
coma. Arch Ophthalmol 126: 1030–1036.
Chen PP (2004): Risk and risk factors for
blindness from glaucoma. Curr Opin Oph-
thalmol 15: 107–111.
Chen E, Golchin S & Blomdahl S (2004): A
comparison between 90 degrees and 180
degrees selective laser trabeculoplasty. J
Glaucoma 13: 62–65.
Chihara E (2008): Assessment of true intraoc-
ular pressure: the gap between theory and
practical data. Surv Ophthalmol 53: 203–
218.
Coleman AL, Cummings SR, Yu F et al.
(2007): Binocular visual-field loss increases
the risk of future falls in older white
women. J Am Geriatr Soc 55: 357–364.
Collaborative Normal-Tension Glaucoma
Study Group (1998a): Comparison of glau-
comatous progression between untreated
patients with normal-tension glaucoma and
patients with therapeutically reduced intra-
ocular pressures. Am J Ophthalmol 126:
487–497.
Collaborative Normal-Tension Glaucoma
Study Group (1998b): The effectiveness of
intraocular pressure reduction in the treat-
ment of normal-tension glaucoma. Am J
Ophthalmol 126: 498–505.
Coppens G, Stalmans I, Zeyen T & Casteels
I (2009): The safety and efficacy of glau-
coma medication in the pediatric popula-
tion. J Pediatr Ophthalmol Strabismus 46:
12–18.
Costa VP, Harris A, Stefansson E et al.
(2003): The effects of antiglaucoma and
systemic medications on ocular blood flow.
Prog Retin Eye Res 22: 769–805.
Curcio CA, Sauncers PL, Younger PW &
Malek G (2000): Peripapillary chorioretinal
atrophy. Bruch¢s membrane changes and
photoreceptor loss. Ophthalmology 107:
334–343.
Damji KF, Bovell AM, Hodge WG, Rock
W, Shah K, Buhrmann R & Pan YI
(2006): Selective laser trabeculoplasty ver-
sus argon laser trabeculoplasty: results
from a 1-year randomised clinical trial. Br
J Ophthalmol 90: 1490–1494.
Diehl DL, Quigley HA, Miller NR, Sommer
A & Burney EN (1990): Prevalence and
significance of optic disc hemorrhage in a
longitudinal study of glaucoma. Arch Oph-
thalmol 108: 545–550.
Doughty MJ & Zaman ML (2000): Human
corneal thickness and its impact on intraoc-
ular pressure measures: a review and meta-
analysis approach. Surv Ophthalmol 44:
367–408.
Drance SM (1989): Disc hemorrhages in the
glaucomas. Surv Ophthalmol 33: 331–337.
Ekstrom C (1993): Elevated intraocular pres-
sure and pseudoexfoliation of the lens cap-
sule as risk factor for chronic open-angle
glaucoma. A population-based five-year
follow-up study. Acta Ophthalmol
(Copenh) 71: 189–195.
Ekstrom C (1996): Prevalence of open-angle
glaucoma in central Sweden. The Tierp
glaucoma survey. Acta Ophthalmol Scand
74: 107–112.
Ekstrom C (2008): Incidence of open-angle
glaucoma in central Sweden. Acta Ophthal-
mol 86: 747–754.
Ekstrom C & Alm A (2008): Pseudoexfolia-
tion as a risk factor for prevalent open-
angle glaucoma. Acta Ophthalmol 86: 741–
746.
ElMallah MK & Asrani SG (2008): New
ways to measure intraocular pressure. Curr
Opin Ophthalmol 19: 122–126.
European Glaucoma Society (2008): Termi-
nology and guidelines for glaucoma.
Savona. Editrice Dogam S.r.l.
Fankhauser F, Kwasniewska S & Van der
Zypen E (2004): Cyclodestructive proce-
dures. I. Clinical and morphological
aspects: a review. Ophthalmologica 218:
77–95.
Feyi-Waboso A & Ejere HO (2004): Needling
for encapsulated trabeculectomy filtering
blebs. Cochrane Database Syst Rev
2004;(2):CD003658. Review.
Forsman E, Kivela T & Vesti E (2007): Life-
time visual disability in open-angle glau-
coma and ocular hypertension. J Glaucoma
16: 313–319.
Freeman EE, Munoz B, Rubin G & West SK
(2007): Visual field loss increases the risk
of falls in older adults: the Salisbury eye
evaluation. Invest Ophthalmol Vis Sci 48:
4445–4450.
Frisen L (1987): A computer-graphics visual
field screener using high-pass spatial fre-
quency resolution targets and multiple
feedback devices. Doc Ophthalmol Proc
Ser 49: 441–446.
Fristrom B & Nilsson SE (1993): Interaction
of PhXA41, a new prostaglandin analogue,
with pilocarpine. A study on patients with
elevated intraocular pressure. Arch Oph-
thalmol 111: 662–665.
Gabelt BT & Kaufman PL (2005): Changes
in aqueous humor dynamics with age and
glaucoma. Prog Retin Eye Res 24: 612–
637.
Garbe E, LeLorier J, Boivin JF & Suissa S
(1997): Risk of ocular hypertension or
open-angle glaucoma in elderly patients on
oral glucocorticoids. Lancet 350: 979–982.
Gasser P, Flammer J, Guthauser U & Mahler
F (1990): Do vasospasms provoke ocular
diseases? Angiology 41: 213–220.
Gaul GR, Will NJ & Brubaker RF (1989):
Comparison of a noncardioselective beta-
adrenoceptor blocker and a cardioselective
blocker in reducing aqueous flow in
humans. Arch Ophthalmol 107: 1308–1311.
Gedde SJ, Schiffman JC, Feuer WJ, Herndon
LW, Brandt JD & Budenz DL (2009):
Three-year follow-up of the tube versus
trabeculectomy study. Am J Ophthalmol
148: 670–684.
Geyer O, Cohen N, Segev E, Rath EZ, Mela-
mud L, Peled R & Lavie P (2003): The
prevalence of glaucoma in patients with
sleep apnea syndrome: same as in the gen-
eral population. Am J Ophthalmol 136:
1093–1096.
Girkin CA, McGwin G Jr, McNeal SF &
Owsley C (2006): Is there an association
between pre-existing sleep apnoea and the
development of glaucoma? Br J Ophthal-
mol 90: 679–681.
Goldmann H (1959): Some basic problems of
simple glaucoma. Am J Ophthalmol
48(Part 2): 213–220.
Gordon MO, Beiser JA, Brandt JD et al.
(2002): The ocular hypertension treatment
study: baseline factors that predict the
onset of primary openangle glaucoma.
Arch Ophthalmol 120: 714–720. discussion
829–30.
Gray TA, Orton LC, Henson D, Harper R &
Waterman H (2009): Interventions for
improving adherence to ocular hypotensive
therapy. Cochrane Database Syst Rev
15(2): CD006132. Review.
Greenfield DS (1999): Glaucomatous versus
nonglaucomatous optic disc cupping: clini-
cal differentiation. Semin Ophthalmol 14:
95–108.
Grødum K, Heijl A & Bengtsson B (2001):
Refractive error and glaucoma. Acta Oph-
thalmol Scand 79: 560–566.
Grødum K, Heijl A & Bengtsson B (2002a):
A comparison of glaucoma patients identi-
fied through mass screening and in routine
clinical practice. Acta Ophthalmol Scand
80: 627–631.
Grødum K, Heijl A & Bengtsson B
(2002b): Optic disk hemorrhages and gen-
eralized vascular disease. J Glaucoma 11:
226–230.
Acta Ophthalmologica 2012
34

Grødum K, Heijl A & Bengtsson B (2004):
Glaucoma and mortality. Graefes Arch
Clin Exp Ophthalmol 242: 397–401.
Grødum K, Heijl A & Bengtsson B (2005):
Risk of glaucoma in ocular hypertension
with and without pseudoexfoliation. Oph-
thalmology 112: 386–390.
Gutierrez P, Wilson MR, Johnson C et al.
(1997): Influence of glaucomatous visual
field loss on health-related quality of life.
Arch Ophthalmol 115: 777–784.
Hattenhauer MG, Johnson DH, Ing HH,
Herman DC, Hodge DO, Yawn BP, But-
terfield LC & Gray DT (1998): The proba-
bility of blindness from open-angle
glaucoma. Ophthalmology 105: 2099–2104.
Hayashi K, Hayashi H, Nakao F & Hayashi
F (2001): Influence of cataract surgery on
automated perimetry in patients with glau-
coma. Am J Ophthalmol 132: 41–46.
Haymes SA, Leblanc RP, Nicolela MT, Chi-
asson LA & Chauhan BC (2007): Risk of
falls and motor vehicle collisions in glau-
coma. Invest Ophthalmol Vis Sci 48: 1149–
1155.
Haymes SA, LeBlanc RP, Nicolela MT, Chi-
asson LA & Chauhan BC (2008): Glau-
coma and on-road driving performance.
Invest Ophthalmol Vis Sci 49: 3035–3041.
Healey PR, Mitchell P, Smith W & Wang JJ
(1998): Optic disc hemorrhages in a popu-
lation with and without signs of glaucoma.
Ophthalmology 105: 216–223.
Heijl A (1976): Automatic perimetry in glau-
coma visual field screening. A clinical
study. Albrecht Von Graefes Arch Klin
Exp Ophthalmol 200: 21–37.
Heijl A & Molder H (1993): Optic disc diam-
eter influences the ability to detect glauco-
matous disc damage. Acta Ophthalmol
(Copenh) 71: 122–129.
Heijl A, Leske MC, Bengtsson B, Hyman L
& Hussein M (2002): Reduction of intraoc-
ular pressure and glaucoma progression:
results from the early manifest glaucoma
trial. Arch Ophthalmol 120: 1268–1279.
Heijl A, Bengtsson B, Chauhan BC, Lieber-
man MF, Cunliffe I, Hyman LK & Leske
MC (2008): A comparison of visual field
progression criteria of 3 major glaucoma
trials in early manifest glaucoma trial
patients. Ophthalmology 115: 1557–1565.
Heijl A, Bengtsson B, Hyman L & Leske
MC; Early Manifest Glaucoma Trial
Group (2009): Natural history of open-
angle glaucoma. Ophthalmology 116:
2044–2048.
van Herick W, Shaffer RN & Schwartz A
(1969): Estimation of width of angle of
anterior chamber. Incidence and signifi-
cance of the narrow angle. Am J Ophthal-
mol 68: 626–629.
Ho J-D, Hu C-C & Lin H-C (2009): Anti-
glaucoma medications during pregnancy
and the risk of low birth weight: a popula-
tion-based study. Br J Ophthalmol 93:
1283–1286.
Hulsman CA, Houwing-Duistermaat JJ, Van
Duijn CM, Wolfs R, Borger PH, Hofman
A & De Jong PT (2002): Family score as
an indicator of genetic risk of primary
open-angle glaucoma. Arch Ophthalmol
120: 1726–1731.
Hyman LG, Komaroff E, Heijl A, Bengtsson
B & Leske MC (2005): Treatment and
vision-related quality of life in the early
manifest glaucoma trial. Ophthalmology
112: 1505–1513.
ISO (1997): Ophthalmic instruments – Funda-
mental requirements and test methods.
Swedish Standards Institution. Book 15004.
29 May 1998. http://www.iso.org.
ISO (2009): Ophthalmic instruments – Ton-
ometers. International standard. Book 8612.
1 October 2009. http://www.iso.org.
Jain MR & Marmion VJ (1976): Rapid pneu-
matic and Mackey-Marg applanation to-
nometry to evaluate the postural effect on
intraocular pressure. Br J Ophthalmol 68:
7–93.
Janz NK, Wren PA, Lichter PR, Musch DC,
Gillespie BW, Guire KE & Mills RP
(2001): The collaborative initial glaucoma
treatment study: interim quality of life find-
ings after initial medical or surgical treat-
ment of glaucoma. Ophthalmology 108:
1954–1965.
Janz NK, Wren PA, Guire KE, Musch DC,
Gillespie BW & Lichter PR (2007): Fear of
blindness in the collaborative initial glau-
coma treatment study: patterns and corre-
lates over time. Ophthalmology 114: 2213–
2220.
Johannesson G, Hallberg P, Eklund A &
Linden C (2008): Pascal, ICare and Gold-
mann applanation tonometry – a compara-
tive study. Acta Ophthalmol 86: 614–621.
Johannesson G, Hallberg P, Koskela T, Ekl-
und A & Linden C (2012): Change in intra-
ocular pressure measurement after myopic
LASEK – a study evaluating Goldmann,
Pascal and Applanation Resonance Tonom-
etry. J Glaucoma 21: 255–259.
Johnson CA, Keltner JL & Balestrery FG
(1979): Suprathreshold static perimetry in
glaucoma and other optic nerve disease.
Ophthalmology 86: 1278–1286.
Jonas JB, Gusek GC & Naumann GOH
(1988a): Optic disc, cup and neuroretinal
rim size, configuration and correlations in
normal eyes. Invest Ophthalmol Vis Sci 29:
1151–1158.
Jonas JB, Gusek GC & Naumann GOH
(1988b): Optic disk morphometry in high
myopia. Graefes Arch Clin Exp Ophthal-
mol 226: 587–590.
Kalaboukhova L, Fridhammar V & Lindb-
lom B (2007): Relative afferent pupillary
defect in glaucoma: a pupillometric study.
Acta Ophthalmol Scand 85: 519–525.
Kass MA, Heuer DK, Higginbotham EJ
et al. (2002): The ocular hypertension treat-
ment study: a randomized trial determines
that topical ocular hypotensive medication
delays or prevents the onset of primary
open-angle glaucoma. Arch Ophthalmol
120: 701–713. discussion 829–30.
Katz J & Sommer A (1988): Reliability
indexes of automated perimetric tests. Arch
Ophthalmol 106: 1252–1254.
Kaufman PL & Barany EH (1976): Loss of
acute pilocarpine effect on outflow facility
following surgical disinsertion and retrodis-
placement of the ciliary muscle from the
scleral spur in the cynomolgus monkey.
Invest Ophthalmol 15: 793–807.
Kirwan JF, Rennie C & Evans JR (2009):
Beta radiation for glaucoma surgery. Coch-
rane Database Syst Rev 15(2): CD003433.
Review.
Kitazawa Y, Shirato S & Yamamoto T
(1986): Optic disc hemorrhage in low-ten-
sion glaucoma. Ophthalmology 93: 853–
857.
Klein BE, Klein R, Meuer SM & Goetz LA
(1993): Migraine headache and its associa-
tion with open-angle glaucoma: the Beaver
Dam eye study. Invest Ophthalmol Vis Sci
34: 3024–3027.
Klein R, Klein BE & Moss SE (1995): Age-
related eye disease and survival. The Bea-
ver Dam eye study. Arch Ophthalmol 113:
333–339.
Kniestedt C, Punjabi O, Lin S & Stamper RL
(2008): Tonometry through the ages. Surv
Ophthalmol 53: 568–591.
Kohlhaas M, Boehm AG, Spoerl E, Pursten
A, Grein HJ & Pillunat LE (2006): Effect
of central corneal thickness, corneal curva-
ture, and axial length on applanation to-
nometry. Arch Ophthalmol 124: 471–476.
Korte JM, Kaila T & Saari KM (2002): Sys-
temic bioavailability and cardiopulmonary
effects of 0.5% timolol eyedrops. Graefes
Arch Clin Exp Ophthalmol 240: 430–435.
Krieglstein GK, Brethfeld V & von Collani E
(1976): Comparative intraocular pressure
measurements with position independent
hand-applanatation tonometers. Albrecht
Von Graefes Arch Klin Exp Ophthalmol
199: 101–113.
Larsson LI & Alm A (1998): Aqueous humor
flow in human eyes treated with dorzola-
mide and different doses of acetazolamide.
Arch Ophthalmol 116: 19–24.
Lee AJ, Wang JJ, Kifley A & Mitchell P
(2006): Open-angle glaucoma and cardio-
vascular mortality: the blue mountains eye
study. Ophthalmology 113: 1069–1076.
Leske MC (2009): Ocular perfusion pressure
and glaucoma: clinical trial and epidemio-
logic findings. Curr Opin Ophthalmol 20:
73–78.
Leske MC, Connell AM, Schachat AP & Hy-
man L (1994): The Barbados eye study.
Prevalence of open angle glaucoma. Arch
Ophthalmol 112: 821–829.
Leske MC, Heijl A, Hyman L & Bengtsson B
(1999): Early manifest glaucoma trial:
design and baseline data. Ophthalmology
106: 2144–2153.
Leske MC, Heijl A, Hussein M, Bengtsson B,
Hyman L & Komaroff E (2003): Factors
for glaucoma progression and the effect of
treatment: the early manifest glaucoma
trial. Arch Ophthalmol 121: 48–56.
Leske MC, Heijl A, Hyman L, Bengtsson B,
Dong L & Yang Z (2007a): Predictors of
long-term progression in the early manifest
Acta Ophthalmologica 2012
35

glaucoma trial. Ophthalmology 114: 1965–
1972.
Leske MC, Wu SY, Honkanen R, Nemesure
B, Schachat A, Hyman L & Hennis A
(2007b): Nine-year incidence of openangle
glaucoma in the Barbados eye studies.
Ophthalmology 114: 1058–1064.
Leske MC, Wu SY, Hennis A, Honkanen R
& Nemesure B (2008): Risk factors for inci-
dent open-angle glaucoma: the Barbados
eye studies. Ophthalmology 115: 85–93.
Letchinger SL, Frohlichstein D, Glieser DK,
Higginbotham EJ, Wilensky JT, Viana MA
& Zeimer R (1993): Can the concentration
of timolol or the frequency of its adminis-
tration be reduced? Ophthalmology 100:
1259–1262.
Lichter PR, Newman LP, Wheeler NC & Be-
all OV (1978): Patient tolerance to carbonic
anhydrase inhibitors. Am J Ophthalmol 85:
495–502.
Lichter PR, Musch DC, Gillespie BW, Guire
KE, Janz NK, Wren PA & Mills RP
(2001): Interim clinical outcomes in the col-
laborative initial glaucoma treatment study
comparing initial treatment randomized to
medications or surgery. Ophthalmology
108: 1943–1953.
Lim CS, O’Brien C & Bolton NM (1996): A
simple clinical method to measure the optic
disc size in glaucoma. J Glaucoma 5: 241–
245.
Linden C & Alm A (1990): The effect of
reduced tear drainage on corneal and aque-
ous concentrations of topically applied
fluorescein. Acta Ophthalmol (Copenh) 68:
633–638.
Linden C & Alm A (1997): Latanoprost and
physostigmine have mostly additive ocular
hypotensive effects in human eyes. Arch
Ophthalmol 115: 857–861.
Linden C, Nuija E & Alm A (1997): Effects
on IOP restoration and blood-aqueous bar-
rier after long-term treatment with latano-
prost in open angle glaucoma and ocular
hypertension. Br J Ophthalmol 81: 370–
372.
Linner E (1970): Microsurgical trabeculecto-
my ‘ab externo’ in glaucoma. Trans Oph-
thalmol Soc U K 89: 475–479.
Madadi P, Koren G, Freeman DJ, Oertel R,
Campbell RJ & Trope GE (2008): Timolol
concentrations in breast milk of a woman
treated for glaucoma: calculation of neona-
tal exposure. J Glaucoma 17: 329–331.
Martin XD (1992): Normal intraocular
pressure in man. Ophthalmologica 205: 57–
63.
Martinez GA, Sample PA & Weinreb RN
(1995): Comparison of high-pass resolution
perimetry and standard automated perime-
try in glaucoma. Am J Ophthalmol 119:
195–201.
Maus TL, Larsson LI, McLaren JW & Bru-
bakr RF (1997): Comparison of dorzola-
mide and acetazolamide as suppressors of
aqueous flow in humans. Arch Ophthalmol
115: 45–9.
McGwin G Jr, Xie A, Mays A, Joiner W,
DeCarlo DK, Hall TA & Owsley C (2005):
Visual field defects and the risk of motor
vehicle collisions among patients with glau-
coma. Invest Ophthalmol Vis Sci 46: 4437–
4441.
Mendrinos E, Mermoud A & Shaarawy T
(2008): Nonpenetrating glaucoma surgery.
Surv Ophthalmol 53: 592–630.
Migdal C, Gregory W & Hitchings R (1994):
Long-term functional outcome after early
surgery compared with laser and medicine
in open-angle glaucoma. Ophthalmology
101: 1651–1656. discussion 1657.
Miglior S, Brigatti L, Velati P, Balestreri C,
Rossetti L, Bujtar E & Orzalesi N (1994):
Relationship between morphometric optic
disc parameters, sex and axial length. Curr
Eye Res 13: 119–124.
Miglior S, Pfeiffer N, Torri V, Zeyen T,
Cunha-Vaz J & Adamsons I (2007a): Pre-
dictive factors for open-angle glaucoma
among patients with ocular hypertension in
the European glaucoma prevention study.
Ophthalmology 114: 3–9.
Miglior S, Torri V, Zeyen T, Pfeiffer N, Vaz
JC & Adamsons I (2007b): Intercurrent
factors associated with the development of
open-angle glaucoma in the European glau-
coma prevention study. Am J Ophthalmol
144: 266–275.
Minckler DS, Vedula SS, Li TJ, Mathew
MC, Ayyala RS & Francis BA (2006):
Aqueous shunts for glaucoma. Cochrane
Database Syst Rev 19(2): CD004918.
Review.
Mishima S (1981): Clinical pharmacokinetics
of the eye. Proctor lecture. Invest Ophthal-
mol Vis Sci 21: 504–541.
Mitchell P, Smith W, Chey T & Healey PR
(1997): Open-angle glaucoma and diabetes:
the blue mountains eye study, Australia.
Ophthalmology 104: 712–718.
Mitchell P, Cumming RG & Mackey DA
(1999): Inhaled corticosteroids, family his-
tory, and risk of glaucoma. Ophthalmology
106: 2301–2306.
Mojon DS, Hess CW, Goldblum D, Bohnke
M, Korner F & Mathis J (2000): Primary
open-angle glaucoma is associated with
sleep apnea syndrome. Ophthalmologica
214: 115–118.
Mok KH & Lee VW (2002): Disc-to-macula
distance to disc-diameter ratio for optic
disc size estimation. J Glaucoma 11: 392–
395.
Mottow-Lippa LS, Lippa EA, Naidoff MA,
Clementi R, Bjornsson T & Jones K
(1990): 008% timolol ophthalmic solution.
A minimal-effect dose in a normal volun-
teer model. Arch Ophthalmol 108: 61–64.
Nagar M, Ogunyomade A, O’Brart DPS, Ho-
wes F & Marshall J (2005): A randomised,
prospective study comparing selective laser
trabeculoplasty with latanoprost for the
control of intraocular pressure in ocular
hypertension and open angle glaucoma. Br
J Ophthalmol 89: 1413–1417.
Oku Y, Oku H, Park M, Hayashi K, Takah-
ashi H, Shouji T & Chihara E (2009): Long
axial length as risk factor for normal ten-
sion glaucoma. Graefes Arch Clin Exp
Ophthalmol 247: 781–787.
Osborne NN (2009): Recent clinical findings
with memantine should not mean that the
idea of neuroprotection in glaucoma is
abandoned. Acta Ophthalmol 87: 450–454.
Ott EZ, Mills MD, Arango S, Getson AJ,
Assaid CA & Adamsons IA (2005): A ran-
domized trial assessing dorzolamide in
patients with glaucoma who are younger
than 6 years. Arch Ophthalmol 123: 1177–
1186.
Parrish RK 2nd, Gedde SJ, Scott IU, Feuer
WJ, Schiffman JC, Mangione CM & Mon-
tenegro-Piniella A (1997): Visual function
and quality of life among patients with
glaucoma. Arch Ophthalmol 115: 1447–
1455.
Passo MS, Goldberg L, Elliot DL & Van
Buskirk EM (1991): Exercise training
reduces intraocular pressure among sub-
jects suspected of having glaucoma. Arch
Ophthalmol 109: 1096–1098.
Pierre-Filho Pde T, Schimiti RB, de Vascon-
cellos JP & Costa VP (2006): Sensitivity
and specificity of frequency-doubling tech-
nology, tendency-oriented perimetry, SITA
Standard and SITA Fast perimetry in peri-
metrically inexperienced individuals. Acta
Ophthalmol Scand 84: 345–350.
Podgor MJ, Leske MC & Ederer F (1983):
Incidence estimates for lens changes, macu-
lar changes, open-angle glaucoma and dia-
betic retinopathy. Am J Epidemiol 118:
206–212.
Prata TS, Lima VC, Pinto LM, Costa EF &
Melo LA Jr (2008): Diode laser transscleral
cyclophotocoagulation-induced staphyloma
following trabeculectomy with mitomycin
C. Ophthalmic Surg Lasers Imaging 39:
343–345.
Quigley HA (1996): Number of people with
glaucoma worldwide. Br J Ophthalmol 80:
389–393.
Quigley HA & Broman AT (2006): The num-
ber of people with glaucoma worldwide in
2010 and 2020. Br J Ophthalmol 90: 262–
267.
Quigley HA & Jampel HD (2003): How are
glaucoma patients identified? J Glaucoma
12: 451–455.
Realini T (2008): Selective laser trabeculopl-
asty: a review. J Glaucoma 17: 497–502.
Resnikoff S, Pascolini D, Etya’ale D, Kocur
I, Pararajasegaram R, Pokharel GP &
Mariotti SP (2004): Global data on visual
impairment in the year 2002. Bull World
Health Organ 82: 844–851.
Roberts MA, Rajkumar V, Morgan G &
Laws D (2009a): Sympathetic ophthalmia
secondary to cyclodiode laser in a 10-year-
old boy. J AAPOS 13: 299–300.
Roberts TV, Hodge C, Graham SL, Burlut-
sky G & Mitchell P (2009b): Prevalence of
nocturnal oxygen desaturation and self-
reported sleep-disordered breathing in glau-
coma. J Glaucoma 18: 114–118.
Rolim de Moura C, Paranhos JRA & Worm-
ald R (2007): Laser trabeculoplasty for
Acta Ophthalmologica 2012
36

open angle glaucoma. Cochrane Database
Syst Rev 17(4): CD003919. Review.
Rosa N, Cennamo G, Breve MA & La Rana
A (1998): Goldmann applanation tonome-
try after myopic photorefractive keratecto-
my. Acta Ophthalmol Scand 76: 550–554.
Rudnicka AR, Mt-Isa S, Owen CG, Cook
DG & Ashby D (2006): Variations in pri-
mary open-angle glaucoma prevalence by
age, gender, and race: a Bayesian meta-
analysis. Invest Ophthalmol Vis Sci 47:
4254–4261.
Ryskulova A, Turczyn K, Makuc DM, Cotch
MF, Klein RJ & Janiszewski R (2008):
Self-reported age-related eye diseases and
visual impairment in the United States:
results of the 2002 national health inter-
view survey. Am J Public Health 98: 454–
461.
Sagara T, Gaton DD, Lindsey JD, Gabelt
BT, Kaufman PL & Weinreb RN (1999):
Topical prostaglandin F2alpha treatment
reduces collagen types I, III, and IV in the
monkey uveoscleral outflow pathway. Arch
Ophthalmol 117: 794–801.
Salminen L (1990): Review: systemic absorp-
tion of topically applied ocular drugs in
humans. J Ocul Pharmacol 6: 243–249.
Sample PA, Medeiros FA & Racette L
(2006): Identifying vision loss with visual-
function-specific perimetry in the diagnostic
innovations in glaucoma study. Invest
Ophthalmol Vis Sci 47: 3381–3389.
SBU (2008): Diagnostik, Uppfoljning Och
Behandling av Oppenvinkelglaukom (gron
starr). En Systematisk Litteraturoversikt.
Stockholm: Statens beredning for medic-
insk utvardering (SBU).
SCB. Statistiska Centralbyran (2008): Sveri-
ges officiella statistik. Sveriges befolkning
efter kon och alder.
Schiose Y (1990): Intraocular pressure: new
perspectives. Surv Ophthalmol 34: 413–435.
Schlecht LP & Brubaker RF (1988): The
effects of withdrawal of timolol in chroni-
cally treated glaucoma patients. Ophthal-
mology 95: 1212–1216.
Schneider E & Grehn F (2006): Intraocular
pressure measurement-comparison of
dynamic contour tonometry and Gold-
mann applanation tonometry. J Glaucoma
15: 2–6.
van der Schoot J, Reus JN, Colen TP &
Lemij HG (2010): The ability of short-
wavelength automated perimetry to predict
conversion to glaucoma. Ophthalmology
117: 30–34.
Severn P, Fraser S, Finch T & May C (2008):
Which quality of life score is best for glau-
coma patients and why? BMC Ophthalmol
8: 2.
Sherwood MB, Garcia-Siekavizza A, Meltzer
MI, Hebert A, Burns AF & McGorray S
(1998): Glaucoma’s impact on quality of
life and its relation to clinical indicators. A
pilot study. Ophthalmology 105: 561–566.
Shields B (2005): Shields’ Textbook of Glau-
coma, 5th edn. Philadelphia: Lippincott,
Williams and Wilkins: s 38 sektion 1.
Siegner SW & Netland PA (1996): Optic disc
hemorrhages and progression of glaucoma.
Ophthalmology 103: 1014–1024.
Sihota R, Srinivasan G, Dada T, Gupta V,
Ghate D & Sharma A (2008): Is the ISNT
rule violated in early primary open-angle
glaucoma – a scanning laser tomography
study. Eye 22: 819–824.
Singh K & Shrivastava A (2009): Intraocular
pressure fluctuations: how much do they
matter? Curr Opin Ophthalmol 20: 84–87.
Soares AS, Artes PH, Andreou P, Leblanc
RP, Chauhan BC & Nicolela MT (2004):
Factors associated with optic disc hemor-
rhages in glaucoma. Ophthalmology 111:
1653–1657.
Stjernschantz JW (2001): From PGF(2alpha)-
isopropyl ester to latanoprost: a review of
the development of xalatan: the Proctor
lecture. Invest Ophthalmol Vis Sci 42:
1134–1145.
Stjernschantz J, Selen G, Astin M & Resul B
(2000): Microvascular effects of selective
prostaglandin analogues in the eye with
special reference to latanoprost and glau-
coma treatment. Prog Retin Eye Res 19:
459–496.
Stoutenbeek R, de Voogd S, Wolfs RC, Hof-
man A, de Jong PT & Jansonius NM
(2008): The additional yield of a periodic
screening programme for open-angle glau-
coma: a population-based comparison of
incident glaucoma cases detected in regular
ophthalmic care with cases detected during
screening. Br J Ophthalmol 92: 1222–1226.
Sugar HS (1961): Experimental trabeculecto-
my in glaucoma. Am J Ophthalmol 51:
623–627.
Tay E, Aung T & Murdoch I (2006): Supra-
choroidal haemorrhage: a rare complica-
tion of cyclodiode laser therapy. Eye 20:
625–627.
The advanced glaucoma intervention study
(AGIS) (2000): The advanced glaucoma
intervention study (AGIS): 7. The relation-
ship between control of intraocular pres-
sure and visual field deterioration. The
AGIS investigators. Am J Ophthalmol 130:
429–440.
The advanced glaucoma intervention study
(AGIS) (2002): The advanced glaucoma
intervention study (AGIS): 12. Baseline
risk factors for sustained loss of visual field
and visual acuity in patients with advanced
glaucoma. Am J Ophthalmol 134: 499–512.
The glaucoma laser trial (GLT) (1990): The
glaucoma laser trial (GLT): 2. Results of
argon laser trabeculoplasty versus topical
medicines. The glaucoma laser trial
research group. Ophthalmology 97: 1403–
1413.
Thorburn W (1978): The accuracy of clinical
applanation tonometry. Acta Ophthalmol
(Copenh) 56: 1–5.
Tielsch JM, Sommer A, Katz J, Royall RM,
Quigley HA & Javitt J (1991): Racial varia-
tions in the prevalence of primary openan-
gle glaucoma. The Baltimore eye survey.
JAMA 266: 369–374.
Tielsch JM, Katz J, Quigley HA, Javitt JC &
Sommer A (1995a): Diabetes, intraocular
pressure, and primary open-angle glaucoma
in the Baltimore eye survey. Ophthalmol-
ogy 102: 48–53.
Tielsch JM, Katz J, Sommer A, Quigley HA
& Javitt JC (1995b): Hypertension, perfu-
sion pressure, and primary open-angle
glaucoma. A population-based assessment.
Arch Ophthalmol 113: 216–221.
Topper JE & Brubaker RF (1985): Effects of
timolol, epinephrine, and acetazolamide on
aqueous flow during sleep. Invest Ophthal-
mol Vis Sci 26: 1315–1319.
van der Valk R, Webers CA, Schouten JS,
Zeegers MP, Hendrikse F & Prins MH
(2005): Intraocular pressure-lowering
effects of all commonly used glaucoma
drugs: a meta-analysis of randomized clini-
cal trials. Ophthalmology 112: 1177–1185.
Varma R, Tielsch JM, Quigley HA, Hilton
SC, Katz J, Spaeth GL & Sommer A
(1994): Race-, age-, gender-, and refractive
error-related differences in the normal optic
disc. Arch Ophthalmol 112: 1068–1076.
Varma R, Wu J, Chong K, Azen SP & Hays
RD (2006): Impact of severity and bilater-
ality of visual impairment on health-related
quality of life. Ophthalmology 113: 1846–
1853.
Viswanathan AC, Crabb DP, McNaught AI,
Westcott MC, Kamal D, Garway-Heath
DF, Fitzke FW & Hitchings RA (2003):
Interobserver agreement on visual field
progression in glaucoma: a comparison of
methods. Br J Ophthalmol 87: 726–730.
de Voogd S (2006): Is diabetes mellitus a risk
factor for open angle glaucoma? The Rot-
terdam study Ophthalmology 113: 1827–
1831.
de Voogd S, Ikram MK, Wolfs RC, Janso-
nius NM, Hofman A & de Jong PT (2005):
Incidence of open-angle glaucoma in a gen-
eral elderly population: the Rotterdam
study. Ophthalmology 112: 1487–1493.
Walland MJ (1998): Diode laser cyclophoto-
coagulation: dosestandardized therapy in
end-stage glaucoma. Aust N Z J Ophthal-
mol 26: 135–139.
Wandell PE, Lundstrom M, Brorsson B &
Aberg H (1997): Quality of life among
patients with glaucoma in Sweden. Acta
Ophthalmol Scand 75: 584–588.
Wang JJ, Mitchell P & Smith W (1997): Is
there an association between migraine
headache and open-angle glaucoma? Find-
ings from the blue mountains eye study
Ophthalmology 104: 1714–1719.
Weinreb RN, Cook J & Friberg TR (1984):
Effect of inverted body position on intraoc-
ular pressure. Am J Ophthalmol 98: 784–
787.
Whitacre MM & Stein R (1993): Sources of
error with use of Goldmann-type tonome-
ters. Surv Ophthalmol 38: 1–30.
Wilkins M, Indar A & Wormald R (2005):
Intra-operative mitomycin C for glaucoma
surgery. Cochrane Database Syst Rev
19(4): CD002897. Review.
Acta Ophthalmologica 2012
37

Wilson MR, Coleman AL, Yu F, Bing EG,
Sasaki IF, Berlin K, Winters J & Lai A
(1998): Functional status and well-being in
patients with glaucoma as measured by the
medical outcomes study short form-36
questionnaire. Ophthalmology 105: 2112–
2116.
Wilson RLC, Lee P, Yamamoto T, Grigera
D, Healey P, Zangwill L & Heijl A (2006):
Screening for open-angle glaucoma: where
are we now and where to from here?
Report from the global AIGS committee
on screening for open angle glaucoma Int
Glaucoma Rev 7: 350–354.
Wise JB & Witter SL (1979): Argon laser
therapy for open-angle glaucoma. A pilot
study. Arch Ophthalmol 97: 319–322.
Wolfs RC, Klaver CC, Ramrattan RS, van
Duijn CM, Hofman A & de Jong PT
(1998): Genetic risk of primary open-angle
glaucoma. Population-based familial aggre-
gation study. Arch Ophthalmol 116: 1640–
1645.
Wormald R, Wilkins MR & Bunce C (2001):
Post-operative 5-Fluorouracil for glaucoma
surgery. Cochrane Database Syst Rev (3):
CD001132. Review.
Wu SY, Nemesure B, Hennis A, Schachat
AP, Hyman L & Leske MC (2008): Open-
angle glaucoma and mortality: the Barba-
dos eye studies. Arch Ophthalmol 126:
365–370.
Yang YF, Herbert L, Ruschen H & Cooling
RJ (2002): Nitrous oxide anaesthesia in the
presence of intraocular gas can cause irre-
versible blindness. BMJ 325: 532–533.
Yildirim N, Yalvac IS, Sahin A, Ozer A &
Bozca T (2009): A comparative study
between diode laser cyclophotocoagulation
and the Ahmed glaucoma valve implant in
neovascular glaucoma: a long-term follow-
up. J Glaucoma 18: 192–196.
Correspondence:
Anders Heijl
Department of Ophthalmology
Skane University Hospital Malmo
SE20502 Malmo
Sweden
Tel: +46 60 332741
Fax: +46 40 336212
Email: [email protected]
Acta Ophthalmologica 2012
38
Keyword index
acetazolamide, 27adjustable sutures, 31age, 8, 23, 31air-puff or noncontact tonometry, 19alcohol, 10, 18antimetabolites, 30applanation tonometry, 18apraclonidine, 25ALT, 28ARA, 16argon laser trabeculoplasty, 28
benefit, 6beta-receptor-blocking drugs, 25betaxolol, 25bimatoprost, 25biomicroscopy, 11blindness, 6blood flow, 28blood pressure, 9BMI, 10body mass index, 10brimonidine, 26brinzolamide, 26
cannabinoids, 18carbachol, 25carbonic anhydrase inhibitors, 26, 27cardiovascular disease, 9case finding, 32cataract, 12, 22CCT, 9, 18C/D ratio, 10central corneal thickness, 9, 18chamber depth, 21children, 26coffee consumption, 10combination preparations, 27combination treatments, 27compliance, 29continuity, 24corneal thickness, 19corticosteroids, 10cortisone, 10CT examination, 22cumulative defect curve, 14cup, 10cyclodestructive procedures, 30cyclocryotherapy, 30
DCT, 19deep sclerectomy, 30definition of glaucoma, 6
diabetes, 9diagnosis, 21diffuse defect (DD), 16diode laser cyclophotocoagulation, 29disc diameter, 10disc haemorrhages, 11diet, 10documentation of the optic disc, 24dorzolamide, 27dynamic contour tonometry, 19dynamic gonioscopy, 21dynamic range, 13
effect of reducing IOP, 23endophthalmitis, 30epidemiology, 7ethnicity/race, 8event analysis, 15excavation, 10exfoliations, 7, 32exfoliation syndrome, 8, 32extrapolation, 24EuroQoL, 6
factors that influence intraocularpressure, 17
false-negative responses (FN), 14false-positive responses (FP), 14family history, 8, 13, 32Fastpac, 13fetal damage, 27fetal injury, 27filtering surgery, 29fluctuations in IOP, 85-fluorouracil, 30FN responses, 14follow-up, 24FP responses, 14frequency doubling perimetry, 135-FU, 31Full Threshold, 13
GDx, 11, 22GDx ECC, 11GDx VCC, 11general anaesthesia, 18glaucoma, 6glaucoma and positive family history,8, 13, 32glaucoma change probability maps, 15Glaucoma Hemifield Test, 14Glaucoma Probability Score, 11global deviation, 17
goal of treatment, 22Goldmann applanation tonometer, 18gonioscopy, 20gray scale, 14
Heidelberg Retina Tomograph(HRT), 11
heredity, 8, 13, 32high blood pressure, 9high-pass resolution perimetry, 13, 17HRQoL, 7HRT, 22Humphrey Field Analyzer, 12hypotonia, 30
i-care tonometer, 19incidence, 7individualized glaucoma management,24interpretation of visual field tests, 15intervals, 24intraocular pressure, 8, 17IOP, 8, 17ISNT rule, 10
kinetic perimetry, 12
laser trabeculoplasty, 28laser treatment, 28latanoprost, 25life expectancy, 7lifestyle factors, 10likely progression, 15loss variance (LV), 14lowering IOP, 22low-tension glaucoma, 6LSD, 18LTP, 28
management of glaucoma, 21management of ocular hypertension,31management of suspected glaucoma,31massage, 31measurement of IOP, 17mean defect (MD), 14mean deviation (MD), 14media opacity, 12memantine, 28migraine, 9mitomycin C, 30MMC, 30
Acta Ophthalmologica 2012
39
Moorfields regression analysis, 11MRI examination, 22myopia, 9
natural history, 23needling, 31neuroprotection, 22neuroprotective, 28neuroretinal rim, 10nifedipine, 22non-penetrating trabeculectomy, 30normal intraocular pressure, 6normal-tension, 6NPT, 30NPT techniques, 30numerical maps, 14, 15numerical threshold values, 14nursing, 27
occlude the lacrimal duct, 25OCT, 22Octopus perimeter, 12ocular hypertension, 7ocular response analyser (ORA), 19open-angle glaucoma, 6ophthalmoscopy, 11optic disc, 10optic disc haemorrhage, 32optic disc photography, 11optical coherence tomography, 12ORA, 19orbscan, 20overall assessment, 24
pachymetry, 20parameters for cyclophotocoagulation,29parameters for laser suture lysis, 31parasympathomimetics, 26Pascal, 19pattern deviation probability maps, 15pattern standard deviation, 14peak level, 25perfusion pressure, 8perimetric glaucoma, 10perimetry, 12peripapillary atrophy, 11
Perkins tonometer, 19pharmacological treatment, 25physical activity, 10pilocarpine, 26population screening, 32possible progression, 15postoperative 5-FU, 31postoperative management, 30pregnancy, 27pregnant woman, 27preperimetric glaucoma, 21preservative, 25prevalence, 7primary laser treatment, 29probability maps, 14, 15progression, 27prostaglandin analogues, 25PSD, 14
QoL, 6, 22quality of life, 6, 22
radiation, 30radiological investigations, 22rate of progression, 14, 16, 23rate of visual field progression, 14, 16,23Raynaud’s syndrome, 9rebound tonometry, 19reliability parameters, 14retinal nerve fibre layer, 10ring perimetry, 13risk analysis, 23risc factors, 8
salicylic acid, 11SAP, 12scanning laser tomography, 11screening and threshold programmes,13selective laser tabeculoplasty, 28selective perimetry, 13seven-in-one, 14severely myopic, 22SF-36, 6shunts, 30single-field analysis, 14
SITA Fast, 13SITA Standard, 13size of the optic disc, 10, 32sleep apnea, 9slit-scan pachymetry, 20SLT, 28SLT parameters, 28smoking, 10standard automated perimetry (SAP),12static gonioscopy, 20static perimetry, 13supraliminal, 13surgery, 28, 29suspicious optic discs, 32suture removal, 31switch, 27sympathomimetics, 25
tafloprost, 25target intraocular pressure, 23, 28tendency-oriented perimetry, 13timolol, 25tonometry, 17tonopen, 19TOP, 13trabeculectomy, 29traffic accidents, 22travoprost, 25treatment methods, 25treatment methods and effect, 22treatment stages, 27trough level, 25
ultrasound pachymetry, 20utility, 6
van Herick’s method, 20VFI, 16VFQ-25, 6viscocanalostomy, 30visual disability, 6, 24visual field index (VFI), 14
YAG laser goniopuncture, 31
Acta Ophthalmologica 2012
40