Embed Size (px)
Citation preview

The genetic sonogram: its use in the detection of chromosomalabnormalities in fetuses of women of advanced maternal age
Greggory R. DeVore*
Al®gen-The Genetics Institute and The Fetal Diagnostic Center of Pasadena, Pasadena, CA, USA
Real-time and color Doppler ultrasound were used to examine 103 second trimester fetuses with abnormalchromosomes (trisomies 13, 18, 21 and sex aneuploidy =86; other =17) and 2000 controls from women ofadvanced maternal age who electively underwent genetic amniocentesis. Ten ultrasound markers wereanalyzed and likelihood ratios were computed for each abnormal ultrasound ®nding and for a normalultrasound study if none of the ten markers were present. Abnormal ultrasound markers were present in81% of fetuses with abnormal karyotypes. The false-positive rate was 13%. The likelihood ratios and the 5%and 95% con®dence limits for each of the ultrasound markers were as follows: choroid plexus cyst(s) 1.5(0.7±3.6); central nervous system abnormalities 16.2 (4.4±60.3); abnormal nuchal skin fold 20.9 (8.4±52.1);ventricular septal defect 8.3 (4.7±14.9); out¯ow tract defects of the heart 3.6 (0.9±14.6); right-to-left chamberdisproportion of the heart 36.9 (14.4±94.5); pericardial effusion 7.2 (3.2±16.1); tricupsid regurgitation 4.7(2.1±10.7); hyperechoic bowel 3.7 (1.8±7.7); and pyelectasis 2.7 (1.0±7.7). All ultrasound markers wereindependent of each other. The likelihood ratio following a normal ultrasound study was 0.20. Isolatedultrasound markers were present in 20.4% (n=21) of fetuses. When all markers were compared to non-cardiovascular markers, the detection rate for fetuses with a chromosomal abnormality decreased from 81%to 52% ( p<0.01). Given the above data, the posterior risk following an ultrasound examination using theultrasound markers evaluated in this study can be used to compute the risk for an abnormal karyotypes inwomen of advanced maternal age. Copyright # 2001 John Wiley & Sons, Ltd.
KEY WORDS: genetic ultrasound; congenital heart defects; trisomy 21; amniocentesis
INTRODUCTION
For the patient 35 years of age and older who choosesnot to undergo invasive diagnostic testing for chro-mosomal abnormalities, the most widely availableoption is maternal serum screening. The use of serumscreening in this group of high-risk patients was ®rstreported in 1994 from two prospective populationstudies in which the combined detection rate for allchromosomal abnormalities was 67% and for trisomy21 it was 87% (Haddow et al., 1994; Rose et al., 1994).In 1994 and 1996 the American College of Obstetri-cians and Gynecologists (ACOG) did not endorsereplacing universal genetic amniocentesis with mater-nal serum screening for women 35 years of age andolder because of (1) the varied detection rates fortrisomy 21 in women of different maternal ages, (2) thelow sensitivity for the detection of chromosomaldefects other than trisomy 21, and (3) the increasingfalse-positive rates associated with advancing maternalage (ACOG, 1994, 1996). The ACOG suggested,however, that triple marker screening could be offeredto women who did not accept the risk of pregnancyloss associated with amniocentesis if they wereinformed of the above three limitations (ACOG,1996). Although the ACOG discouraged triplemarker screening for women of advanced maternalage, during 1998 45.1% of 74 151 women 35 years ofage and older in the state of California elected triple
marker screening compared to 43.7% (32 370) whochose genetic amniocentesis (personal communicationfrom the Genetic Disease Branch of the State ofCalifornia). These data would suggest that utilizationof triple marker screening by women 35 years of ageand older is a clinical option.
During 1995 four groups of investigators reportedresults from studies in which diagnostic ultrasoundwas used to adjust the risk for chromosomal abnorm-alities in high-risk patients (DeVore and Al®, 1995;Nadel et al., 1995; Nyberg et al., 1995; Vintzileos andEgan, 1995). From this work the concept of `geneticultrasound' evolved. Although genetic ultrasound is analternative screening test for women 35 years of ageand older who decline amniocentesis, it has focusedprimarily on the detection of trisomy 21 (DeVore andAl®, 1995; Nadel et al., 1995; Nyberg et al., 1995;Vintzileos and Egan, 1995; Bahado-Singh et al., 1998;Deren et al., 1998; Bahado-Singh et al., 1999). Thosecritical of maternal serum screening as an option togenetic amniocentesis may also be critical of geneticultrasound because of the lack of data available as toits performance relating to the detection of allchromosomal abnormalities in women 35 years ofage and older.
The purpose of the present study was to evaluateultrasound markers that would identify fetuses withabnormal chromosomes in women 35 years of age andolder and provide data that would allow the clinicianto compute the patient's individual risk for chromo-somal abnormalities following a normal or abnormalsecond-trimester ultrasound examination.
*Correspondence to: G. R. DeVore, Suite 206, 301 South Fair Oaks,Pasadena, CA 91105, USA. E-mail: [email protected]
PRENATAL DIAGNOSIS
Prenat Diagn 2001; 21: 40±45.
Copyright # 2001 John Wiley & Sons, Ltd.
METHODS
The institutional review board of Al®gen-The GeneticsInstitute, Pasadena, CA, approved the study. Between1990 and 1999 all fetuses with abnormal karyotypesand 2000 controls were identi®ed from a database thatcontained women electing to undergo genetic amnio-centesis as the result of advanced maternal age. Nofetuses were included in the study if an abnormalkaryotype or abnormal fetal anatomy had beenidenti®ed prior to the referral.
Each patient was allocated 15 min for ultrasoundevaluation and amniocentesis, both of which wereperformed by a single examiner. An Acuson 128(Acuson, Mountain View, CA, USA) with a 5 and/or7 MHz curvilinear transducer was used for real-timeand color Doppler ultrasound examination of thefetus. Biometric measurements of the head, abdomen,and femur were obtained. This was followed by ananatomical survey of the head, chest, abdomen, pelvis,and limbs. Examination of the heart with colorDoppler was used to identify whether the ventricles
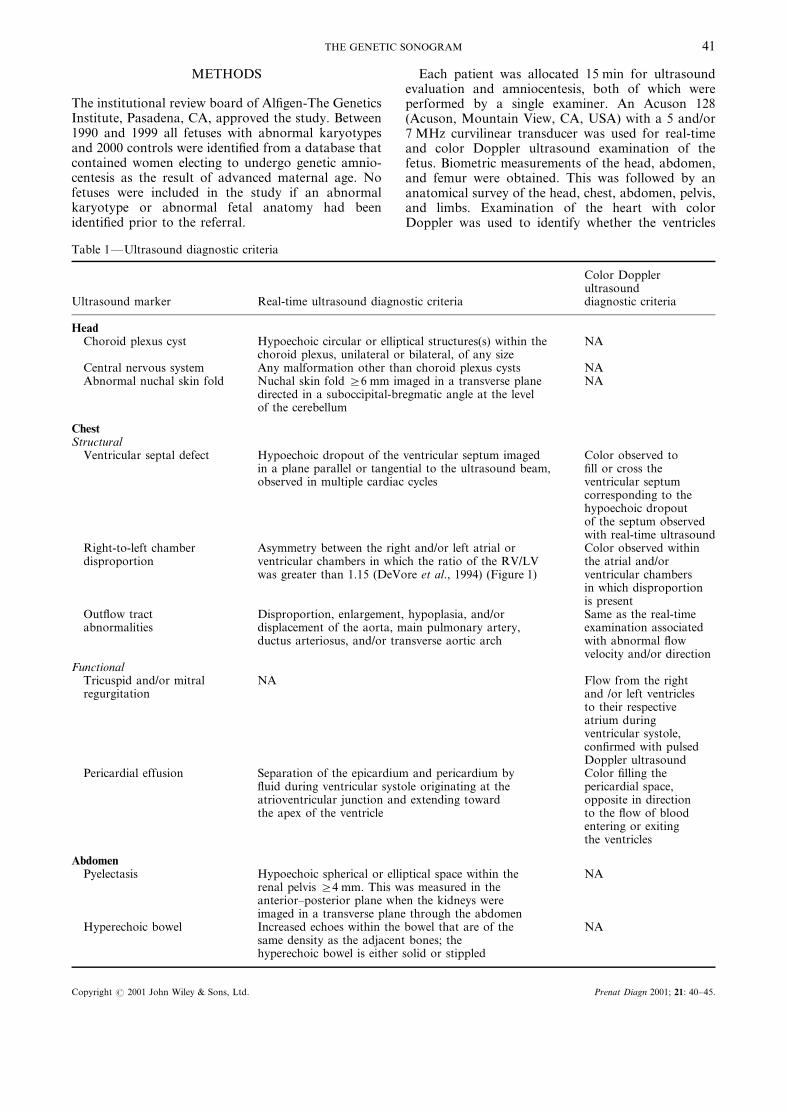
Table 1ÐUltrasound diagnostic criteria
Ultrasound marker Real-time ultrasound diagnostic criteria
Color Dopplerultrasounddiagnostic criteria
HeadChoroid plexus cyst Hypoechoic circular or elliptical structures(s) within the
choroid plexus, unilateral or bilateral, of any sizeNA
Central nervous system Any malformation other than choroid plexus cysts NAAbnormal nuchal skin fold Nuchal skin fold i6 mm imaged in a transverse plane
directed in a suboccipital-bregmatic angle at the levelof the cerebellum
NA
ChestStructural
Ventricular septal defect Hypoechoic dropout of the ventricular septum imagedin a plane parallel or tangential to the ultrasound beam,observed in multiple cardiac cycles
Color observed to®ll or cross theventricular septumcorresponding to thehypoechoic dropoutof the septum observedwith real-time ultrasound
Right-to-left chamberdisproportion
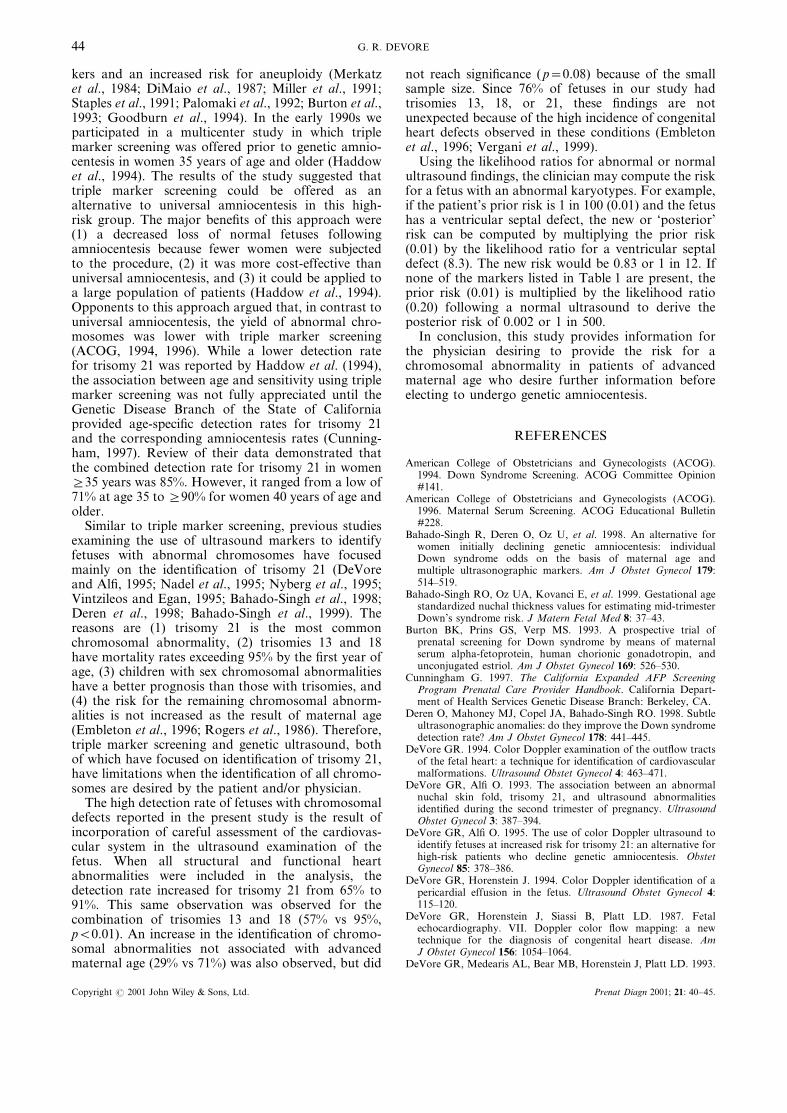
Asymmetry between the right and/or left atrial orventricular chambers in which the ratio of the RV/LVwas greater than 1.15 (DeVore et al., 1994) (Figure 1)
Color observed withinthe atrial and/orventricular chambersin which disproportionis present
Out¯ow tractabnormalities
Disproportion, enlargement, hypoplasia, and/ordisplacement of the aorta, main pulmonary artery,ductus arteriosus, and/or transverse aortic arch
Same as the real-timeexamination associatedwith abnormal ¯owvelocity and/or direction
FunctionalTricuspid and/or mitralregurgitation
NA Flow from the rightand /or left ventriclesto their respectiveatrium duringventricular systole,con®rmed with pulsedDoppler ultrasound
Pericardial effusion Separation of the epicardium and pericardium by¯uid during ventricular systole originating at theatrioventricular junction and extending towardthe apex of the ventricle
Color ®lling thepericardial space,opposite in directionto the ¯ow of bloodentering or exitingthe ventricles
AbdomenPyelectasis Hypoechoic spherical or elliptical space within the
renal pelvis i4 mm. This was measured in theanterior±posterior plane when the kidneys wereimaged in a transverse plane through the abdomen
NA
Hyperechoic bowel Increased echoes within the bowel that are of thesame density as the adjacent bones; thehyperechoic bowel is either solid or stippled
NA
THE GENETIC SONOGRAM 41
Copyright # 2001 John Wiley & Sons, Ltd. Prenat Diagn 2001; 21: 40±45.

and atria ®lled equally with color, abnormal ¯uid waspresent within the pericardial space, tricuspid and/ormitral regurgitation were present, color within theventricular chambers was separated by the interven-tricular and interatrial septa, and ¯ow was unidirec-tional as it exited the aortic and pulmonary out¯owtracts (DeVore et al., 1987; DeVore and Al® 1993;DeVore, 1994; DeVore and Horenstein, 1994). Table 1lists the criteria for identi®cation of the ultrasoundmarkers used in this study.
All karyotypes were analyzed by a single referencelaboratory (Al®gen-The Genetics Institute, Pasadena,CA). Normal variants, common inversions, balancedtranslocations, and pseudomosaicisms were classi®edas normal for this study.
The methods used for termination of pregnancyvaried for those who elected this option, mainlybecause of the choices offered by healthcare providersand patient preference. Autopsy material was notconsistently available for correlation with ultrasound®ndings. Therefore, classi®cation of abnormal anat-omy was based upon ®ndings identi®ed during theultrasound study immediately preceding amniocentesis(Table 1).
The gestational age and presence or absence ofabnormal anatomy as de®ned in Table 1 were tabu-lated for statistical analysis using a computer-basedprogram (NCSS 2000, Kaysville, UT, USA and SPSS,Chicago, IL, USA). If a fetus had more than oneabnormal ultrasound ®nding, each abnormality waslisted separately. The control group consisted of 2000fetuses from women of advanced maternal age thatunderwent ultrasound evaluation followed by amnio-centesis in which the karyotype was normal. Todetermine if the ultrasound markers were independentfrom each other, backward logistic regression was
performed on individual as well as combinations ofmarkers listed in Table 1. The likelihood ratio wascomputed for each ultrasound marker by deriving thevalue from the log e of the corresponding coef®cientfollowing logistic regression. The likelihood ratio fora normal ultrasound study (absence of all ultra-sound markers) was computed by the equation [(1xsensitivity)/speci®city] (Ingel®nger et al., 1983).
RESULTS
From 1990 to 1999 105 fetuses with abnormalchromosomes were identi®ed following genetic amnio-centesis. The mean gestational age at the time of theultrasound examination was 17 weeks and 4 days (t1week 4 days) with a range from 14±23 weeks. Twofetuses were excluded from analysis because ofinadequate ultrasound imaging secondary to maternalobesity (DeVore et al., 1993). Table 2 classi®es the 103fetuses with abnormal karyotypes and the numberwith abnormal ultrasound ®ndings. Eighty-one per-cent of fetuses with abnormal chromosomes hadultrasound ®ndings listed in Table 1, with a false-positive rate of 13%. Four fetuses (one trisomy 13, onedeletion, and two 45X) had abnormal ultrasound®ndings not listed in Table 1.
Cardiac markers were present in 68% (n=70) offetuses, of which 81.4% (57/70) were structural. Sixpercent (n=6) of fetuses had an endocardial cushiondefect. Because this malformation was not present inthe control population, it was classi®ed with ventri-cular septal defects. Out¯ow tract abnormalitiesconsisted of a hypoplastic aorta with a dilated mainpulmonary artery (n=3), pulmonary atresia (n=1),and tetralogy of Fallot (n=3). Mixtures of cardiovas-cular and non-cardiovascular markers were present in44% (n=45). Abnormalities only involving the cardi-ovascular system were present in 24% (n=25).Abnormal markers involving only non-cardiovascularsystems were present in 17% (n=17). Isolated ultra-sound markers were identi®ed in 20.38% (n=21) offetuses as follows: ventricular septal defects (n=5),right-to-left disproportion of the heart chambers(n=7), pericardial effusion (n=2), tricuspid regurgita-tion (n=2), abnormal nuchal skin fold (n=2), choroidplexus cysts (n=1), hyperechoic bowel (n=2), pyelec-tasis (n=2). Two markers were present in 30.10%(n=32), three in 20.39% (n=21), four in 6.79% (n=7),and ®ve or more in 1.94% (n=2).
Table 3 lists the sensitivity, false-positive rate, andlikelihood ratio for the individual ultrasound markerslisted in Table 1. Cardiovascular markers had thehighest sensitivities, followed by an abnormal nuchalskin fold and hyperechoic bowel. The false-positiverates for individual markers were less than 6%(Table 3). All ultrasound markers, except for mitralregurgitation, were signi®cantly (p<0.05) more pre-valent in fetuses with chromosomal abnormalities thanin controls.
When the interaction of all ultrasound markers inTable 1 were evaluated using backward logistic regres-
Table 2ÐUltrasound ®ndings in fetuses with abnormalkaryotypes
Karyotype Fetuses (n)
Percentageof fetuseswith anabnormalultrasoundexamination (n)
Associated with advanced maternal ageTrisomy 13 6 83% (5)Trisomy 18 15 93% (14)Trisomy 21 57 91% (52)XXX 5 40% (2)XXY 2 50% (1)XXXY 1 100% (1)Subtotal 86 87% (75)
Not associated with advanced maternal age45X 4 50% (2)Unbalanced translocation 3 0% (0)Mosaicism 6 67% (4)Deletions 2 0% (0)69,xxx 2 100% (2)Subtotal 17 47% (8)
Total 103 81% (83)
G. R. DEVORE42
Copyright # 2001 John Wiley & Sons, Ltd. Prenat Diagn 2001; 21: 40±45.

sion, all ultrasound markers were independent fromeach other. The likelihood ratio following a normalstudy is 0.20.
When all markers (cardiovascular plus non-cardiovascular) are compared to only non-cardiovascular markers, the detection rate for fetuseswith a chromosomal abnormality decreases from 81%to 52% (p<0.01). This is also observed (87% to 57%;p<0.01) in fetuses with chromosomal defects that areassociated only with advancing maternal age (triso-mies 13, 18, 21; and sex aneuploidy).
DISCUSSION
Prior to 1984 genetic amniocentesis was only offeredto women 35 years of age and older and/or to patientsin whom a fetal malformation was diagnosed prena-tally (Tabor et al., 1988). Following the recognition ofthe association between a low maternal serum alpha-fetoprotein and trisomies 18 and 21 by Merkatz et al.(1984), screening for Down syndrome was offered tolow-risk patients after numerous investigators con-®rmed the association between maternal serum mar-
Table 3ÐUltrasound markers identi®ed in second trimester fetuses with chromosomal abnormalities
Ultrasound marker
All chromosomalabnormalities(n=103)
Controls(n=2000)
Sensitivity(%)
False-positive ratefor individualultrasound markers(%)
Likelihood ratio(5% and 95%con®dence limits)
HeadChoroid plexus cysts 9 56 8.7 2.8 1.5 (0.7±3.6)*Central nervous system 10 7 9.7 0.4 16.2 (4.4±60.3)Nuchal skin fold 19 15 18.5 0.8 20.9 (8.4±52.1)
CardiovascularStructural
Ventricular septal defect 40 107 38.8 5.4 8.3 (4.7±14.9)Right/left disproportion 21 13 20.4 0.7 36.9 (14.4±94.5)Out¯ow tracts 7 6 6.8 0.3 3.6 (0.9±14.6)*
FunctionalPericardial effusion 16 48 15.5 2.4 7.2 (3.2±16.1)Tricuspid regurgitation 23 34 22.3 1.7 4.7 (2.1±10.7)Mitral regurgitation 0 3 0 0.2 ±
AbdomenHyperechoic bowel 19 70 18.5 3.5 3.7 (1.8±7.7)Pyelectasis 7 33 6.8 ± 2.7 (1.0±7.7)*
*p>0.05 for the likelihood ratio.
Figure 1ÐNormal four-chamber view and two cases of atrial and ventricular disproportion at 18 and 27 weeks' gestation. The lower panelcontains the real-time images and the upper panel the real-time images in which the chambers of the heart are outlined. RA, Right atrium;LA, left atrium; RV, right ventricle; LV, left ventricle
THE GENETIC SONOGRAM 43
Copyright # 2001 John Wiley & Sons, Ltd. Prenat Diagn 2001; 21: 40±45.
kers and an increased risk for aneuploidy (Merkatzet al., 1984; DiMaio et al., 1987; Miller et al., 1991;Staples et al., 1991; Palomaki et al., 1992; Burton et al.,1993; Goodburn et al., 1994). In the early 1990s weparticipated in a multicenter study in which triplemarker screening was offered prior to genetic amnio-centesis in women 35 years of age and older (Haddowet al., 1994). The results of the study suggested thattriple marker screening could be offered as analternative to universal amniocentesis in this high-risk group. The major bene®ts of this approach were(1) a decreased loss of normal fetuses followingamniocentesis because fewer women were subjectedto the procedure, (2) it was more cost-effective thanuniversal amniocentesis, and (3) it could be applied toa large population of patients (Haddow et al., 1994).Opponents to this approach argued that, in contrast touniversal amniocentesis, the yield of abnormal chro-mosomes was lower with triple marker screening(ACOG, 1994, 1996). While a lower detection ratefor trisomy 21 was reported by Haddow et al. (1994),the association between age and sensitivity using triplemarker screening was not fully appreciated until theGenetic Disease Branch of the State of Californiaprovided age-speci®c detection rates for trisomy 21and the corresponding amniocentesis rates (Cunning-ham, 1997). Review of their data demonstrated thatthe combined detection rate for trisomy 21 in womeni35 years was 85%. However, it ranged from a low of71% at age 35 to i90% for women 40 years of age andolder.
Similar to triple marker screening, previous studiesexamining the use of ultrasound markers to identifyfetuses with abnormal chromosomes have focusedmainly on the identi®cation of trisomy 21 (DeVoreand Al®, 1995; Nadel et al., 1995; Nyberg et al., 1995;Vintzileos and Egan, 1995; Bahado-Singh et al., 1998;Deren et al., 1998; Bahado-Singh et al., 1999). Thereasons are (1) trisomy 21 is the most commonchromosomal abnormality, (2) trisomies 13 and 18have mortality rates exceeding 95% by the ®rst year ofage, (3) children with sex chromosomal abnormalitieshave a better prognosis than those with trisomies, and(4) the risk for the remaining chromosomal abnorm-alities is not increased as the result of maternal age(Embleton et al., 1996; Rogers et al., 1986). Therefore,triple marker screening and genetic ultrasound, bothof which have focused on identi®cation of trisomy 21,have limitations when the identi®cation of all chromo-somes are desired by the patient and/or physician.
The high detection rate of fetuses with chromosomaldefects reported in the present study is the result ofincorporation of careful assessment of the cardiovas-cular system in the ultrasound examination of thefetus. When all structural and functional heartabnormalities were included in the analysis, thedetection rate increased for trisomy 21 from 65% to91%. This same observation was observed for thecombination of trisomies 13 and 18 (57% vs 95%,p<0.01). An increase in the identi®cation of chromo-somal abnormalities not associated with advancedmaternal age (29% vs 71%) was also observed, but did
not reach signi®cance ( p=0.08) because of the smallsample size. Since 76% of fetuses in our study hadtrisomies 13, 18, or 21, these ®ndings are notunexpected because of the high incidence of congenitalheart defects observed in these conditions (Embletonet al., 1996; Vergani et al., 1999).
Using the likelihood ratios for abnormal or normalultrasound ®ndings, the clinician may compute the riskfor a fetus with an abnormal karyotypes. For example,if the patient's prior risk is 1 in 100 (0.01) and the fetushas a ventricular septal defect, the new or `posterior'risk can be computed by multiplying the prior risk(0.01) by the likelihood ratio for a ventricular septaldefect (8.3). The new risk would be 0.83 or 1 in 12. Ifnone of the markers listed in Table 1 are present, theprior risk (0.01) is multiplied by the likelihood ratio(0.20) following a normal ultrasound to derive theposterior risk of 0.002 or 1 in 500.
In conclusion, this study provides information forthe physician desiring to provide the risk for achromosomal abnormality in patients of advancedmaternal age who desire further information beforeelecting to undergo genetic amniocentesis.
REFERENCES
American College of Obstetricians and Gynecologists (ACOG).1994. Down Syndrome Screening. ACOG Committee Opinion#141.
American College of Obstetricians and Gynecologists (ACOG).1996. Maternal Serum Screening. ACOG Educational Bulletin#228.
Bahado-Singh R, Deren O, Oz U, et al. 1998. An alternative forwomen initially declining genetic amniocentesis: individualDown syndrome odds on the basis of maternal age andmultiple ultrasonographic markers. Am J Obstet Gynecol 179:514±519.
Bahado-Singh RO, Oz UA, Kovanci E, et al. 1999. Gestational agestandardized nuchal thickness values for estimating mid-trimesterDown's syndrome risk. J Matern Fetal Med 8: 37±43.
Burton BK, Prins GS, Verp MS. 1993. A prospective trial ofprenatal screening for Down syndrome by means of maternalserum alpha-fetoprotein, human chorionic gonadotropin, andunconjugated estriol. Am J Obstet Gynecol 169: 526±530.
Cunningham G. 1997. The California Expanded AFP ScreeningProgram Prenatal Care Provider Handbook. California Depart-ment of Health Services Genetic Disease Branch: Berkeley, CA.
Deren O, Mahoney MJ, Copel JA, Bahado-Singh RO. 1998. Subtleultrasonographic anomalies: do they improve the Down syndromedetection rate? Am J Obstet Gynecol 178: 441±445.
DeVore GR. 1994. Color Doppler examination of the out¯ow tractsof the fetal heart: a technique for identi®cation of cardiovascularmalformations. Ultrasound Obstet Gynecol 4: 463±471.
DeVore GR, Al® O. 1993. The association between an abnormalnuchal skin fold, trisomy 21, and ultrasound abnormalitiesidenti®ed during the second trimester of pregnancy. UltrasoundObstet Gynecol 3: 387±394.
DeVore GR, Al® O. 1995. The use of color Doppler ultrasound toidentify fetuses at increased risk for trisomy 21: an alternative forhigh-risk patients who decline genetic amniocentesis. ObstetGynecol 85: 378±386.
DeVore GR, Horenstein J. 1994. Color Doppler identi®cation of apericardial effusion in the fetus. Ultrasound Obstet Gynecol 4:115±120.
DeVore GR, Horenstein J, Siassi B, Platt LD. 1987. Fetalechocardiography. VII. Doppler color ¯ow mapping: a newtechnique for the diagnosis of congenital heart disease. AmJ Obstet Gynecol 156: 1054±1064.
DeVore GR, Medearis AL, Bear MB, Horenstein J, Platt LD. 1993.
G. R. DEVORE44
Copyright # 2001 John Wiley & Sons, Ltd. Prenat Diagn 2001; 21: 40±45.

Fetal echocardiography: factors that in¯uence imaging of the fetalheart during the second trimester of pregnancy. J Ultrasound Med12: 659±663.
DeVore GR, Siassi B, Platt LD, 1994. Fetal echocardiography IV:M-mode assessment of ventricular size and contractility duringthe second and third trimesters of pregnancy in the normal fetus.Am J Obstet Gynecol 150: 981±988.
DiMaio MS, Baumgarten A, Greenstein RM, Saal HM, MahoneyMJ. 1987. Screening for fetal Down's syndrome in pregnancy bymeasuring maternal serum alpha-fetoprotein levels. N Engl J Med317: 342±346.
Embleton ND, Wyllie JP, Wright MJ, Burn J, Hunter S. 1996.Natural history of trisomy 18. Arch Dis Child Fetal Neonatal Ed75: 38±41.
Goodburn SF, Yates JR, Raggatt PR, et al. 1994. Second-trimestermaternal serum screening using alpha-fetoprotein, human chor-ionic gonadotrophin, and unconjugated oestriol: experience of aregional programme. Prenat Diagn 14: 391±402.
Haddow JE, Palomaki GE, Knight GJ, Cunningham GC, Lustig LS,Boyd PA. 1994. Reducing the need for amniocentesis in women 35years of age or older with serum markers for screening. N EnglJ Med 330: 1114±1118.
Ingel®nger JA, Mosteller F, Thibodeau LA, Ware JH. 1983.Biostatistics in Clinical Medicine. Macmillan: New York, NY;29±30.
Merkatz IR, Nitowsky HM, Macri JN, Johnson WE. 1984. Anassociation between low maternal serum alpha-fetoprotein andfetal chromosomal abnormalities. Am J Obstet Gynecol 148:886±894.
Miller CH, O'Brien TJ, Chatelain S, Butler BB, Quirk JG. 1991.Alteration in age-speci®c risks for chromosomal trisomy bymaternal serum alpha-fetoprotein and human chorionic gonado-tropin screening. Prenat Diagn 11: 153±158.
Nadel AS, Bromley B, Frigoletto Jr FD, Benacerraf BR. 1995. Canthe presumed risk of autosomal trisomy be decreased in fetuses ofolder women following a normal sonogram? J Ultrasound Med 14:297±302.
Nyberg DA, Luthy DA, Cheng EY, Sheley RC, Resta RG, WilliamsMA. 1995. Role of prenatal ultrasonography in women withpositive screen for Down syndrome on the basis of maternalserum markers. Am J Obstet Gynecol 173: 1030±1035.
Palomaki GE, Knight GJ, Haddow JE, Canick JA, Saller Jr DN,Panizza DS. 1992. Prospective intervention trial of a screeningprotocol to identify fetal trisomy 18 using maternal serum alpha-fetoprotein, unconjugated oestriol, and human chorionic gonado-tropin. Prenat Diagn 12: 925±930.
Rose NC, Palomaki GE, Haddow JE, Goodman DB, Mennuti MT.1994. Maternal serum alpha-fetoprotein screening for chromoso-mal abnormalities: a prospective study in women aged 35 andolder. Am J Obstet Gynecol 170: 1073±1078.
Rogers DB, Shapiro LJ. 1986. X-Linked diseases and disorders ofthe sex chromosomes. In Genetic Disorders and the Fetus,Milunsky A (ed.). Plenum Press: New York, NY; 331.
Staples AJ, Robertson EF, Ranieri E, Ryall RG, Haan EA. 1991. Amaternal serum screen for trisomy 18: an extension of maternalserum screening for Down syndrome. Am J Hum Genet 49:1025±1033.
Tabor A, Philip J, Madsen M, Bang J, Obel EB, Norgaard-PedersenB. 1986. Randomised controlled trial of genetic amniocentesis in4606 low-risk women. Lancet 8493: 1287±1293.
Vergani P, Locatelli A, Piccoli MG, et al. 1999. Best second trimestersonographic markers for the detection of trisomy 21. J UltrasoundMed 18: 469±473.
Vintzileos AM, Egan JF. 1995. Adjusting the risk for trisomy 21 onthe basis of second-trimester ultrasonography. Am J ObstetGynecol 172: 837±844.
THE GENETIC SONOGRAM 45
Copyright # 2001 John Wiley & Sons, Ltd. Prenat Diagn 2001; 21: 40±45.