Embed Size (px)
Citation preview

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574i44
Accepted 1 November 2010
ABSTRACT Modern technological innovations have advanced our
understanding of the genetic basis of spondyloarthritis.
In ankylosing spondylitis (AS), where the major
histocompatibility complex (MHC) accounts for nearly
half of the predisposition, most comes from HLA-B27, for
which 65 subtypes are now recognised, although other
genes are also at work including HLA-B60 ( B*40:01 ).
Other genes have been identifi ed, including those involved
in peptide editing for loading onto class I MHC molecules
(ERAP1) and cytokine genes such as interleukin 1A (IL-
1A) and those involved in the Th17 network (IL-23R, an
association seen primarily in Caucasians) and others. In
acute anterior uveitis, these associations are also seen
as well as a region on chromosome 9p and genes whose
confi rmation is under way. Psoriasis and psoriatic arthritis
fall into this disease spectrum, with the largest region of
susceptibility coming from the MHC (most likely HLA-C,
ie, C*06:02 although additional infl uences are also being
implicated), and most of the other genetic susceptibility
coming from genes involved in cytokine production,
specifi cally genes in the Th17 pathway (IL-12B, IL-23A
and IL-23R, the latter, like in AS, not seen in Asians),
genes in the nuclear factor B pathway (TNFAIP3 and
TNIP1) and genes in the Th2 pathway (IL-4 and IL-13).
Given that more than half of patients with AS have
evidence on colonoscopy of at least occult infl ammatory
bowel disease (IBD), it is not surprising that shared
genetic infl uences are operative. In IBD, genes important
in the innate immune response (NOD2), autophagy
(ATG6L1) and regulation of the IL-23 pathway (IL-23R)
play a role in disease susceptibility.
INTRODUCTION Recent years have witnessed rapid advances in our understanding of the genetic basis of spondylo-arthritis and related diseases (ankylosing spondylitis (AS), acute anterior uveitis (AAU), psoriasis and psoriatic arthritis (PsA) and infl ammatory bowel disease (IBD)). From HLA and other candidate gene studies, genetic methodologies have progressed through family studies with microsatellite marker to more recent dense explorations of the genome through computer-based gene chip technologies. This review will explore the more recent fi ndings in spondyloarthritis and related disease susceptibility.
GENETICS OF ANKYLOSING SPONDYLITIS Studies of disease concordance in twins and fami-lies of patients with AS indicate that the suscepti-bility to the disease is largely due to genetic factors and that several loci are likely to be involved. Twin studies have shown that the MZ twin concordance rate is 63% compared with the DZ concordance rate of 12.5%. 1 Genetic variance modelling has
indicated that genetic factors contribute over 90% to overall susceptibility, with the rest due to ran-dom environmental effects. 2 The environmental trigger(s) are therefore likely to be widespread (such as gut fl ora) and do not contribute signifi cantly to the overall causation of the disease.
ROLE OF HLA-B27 For nearly 40 years it has been known HLA-B27 formed the most signifi cant association with AS, as well as with other types of spondyloarthritis (SpA), especially reactive arthritis (70% in white people), psoriatic spondylitis (60–70%), the spondylitis associated with IBD (50–60%) and AAU (50%). Other types of SpA show a much lower associa-tion (eg, peripheral PsA about 25% compared with a frequency of 6–8% in controls) or no association at all (eg, peripheral enteropathic arthritis). 3
Over 69 subtypes of HLA-B27 have now been recognised, 4 whose evolution from the parent B27 allele B*27:05 has largely followed geographi-cal grounds refl ecting human migrations ( table 1 ). The overwhelming majority of HLA-B27 alleles in Western European Caucasians comprise HLA-B*27:05 (about 90%) and HLA-B*27:02 (about 10%). In patients from Eastern Asia, HLA-B*27:04 and B*27:05 are most commonly encountered, especially in patients with AS, and in Southern Asia HLA-B*27:07 is found. Two subtypes— HLA-B*27:06 (encountered in South-east Asia) and B*27:09 (found largely in Sardinia)—appear to have lost their associ-ation with AS for reasons that are as yet still unclear. Other B27 subtypes are very rare and are mostly reported in only single individuals or families, although HLA-B*27:01 and B*27:14 have also been reported in patients with spondylitis. Molecular folding of HLA-B27 protein subtypes is determined by the global effect of polymorphic residues and shows incomplete correspondence to AS. 5
The association of HLA-B27 with AS is found in nearly all ethnic groups, although it is least strong in those of sub-Saharan African ancestry. Older studies from Africa reported AS to be rare, with a very low frequency of HLA-B27 in patients with AS. 6 7 This was attributed, as least in part, to a ‘protective’ West African B27 subtype ( B*27:03 ), 7 although subsequent studies reported an associa-tion of this subtype with AS in Africans. 8 The only previous study of HLA alleles in African Americans with AS suggested that only about 50% of patients are HLA-B27 positive; instead, HLA-B27-negative patients have been shown to be more likely to have the HLA-B7 cross-reactive group antigens ( B*7, B*40, B*42 , B*55 or B*56 ). 9 Recent studies from West Africa have implicated HLA-B*14:03 in susceptibility to AS. 10 This association has also extended to undifferentiated spondyloarthritis and
Correspondence to John D Reveille, The University of Texas–Houston Health Science Center, MSB 5.270, 6431 Fannin, Houston, TX 77030, USA; [email protected]
The genetic basis of spondyloarthritis John D Reveille
04_annrheumdis140574.indd 4404_annrheumdis140574.indd 44 1/28/2011 10:10:42 PM1/28/2011 10:10:42 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574 i45
the overall risk for SpA. The entire effect of the MHC, on the other hand, is about 50%. This suggests that other genetic infl u-ences are operative in the MHC in addition to HLA-B27.
OTHER GENES IMPLICATED IN SUSCEPTIBILITY TO AS The serological specifi city of HLA-B60 (known as HLA-B*40:01 by DNA typing) was shown to be increased in B27-positive patients with AS in fi ve independent data sets in 1989 but not increased in B27-negative patients with AS, increasing the risk for AS threefold ( table 2 ). 13 This association was subsequently confi rmed in 284 UK patients with AS, 14 as well as in HLA-B27-negative Taiwanese patients with AS 15 and in African American patients with AS (Zhang et al , unpublished data). However, it was not seen in Mexican Mestizos with SpA. 16 Other MHC alleles have also been implicated, but defi nitive associations with these have been confounded by linkage to HLA-B27.
Other than the MHC, a number of genetic infl uences have been implicated in susceptibility to AS in small cohorts that could not subsequently be replicated. The fi rst gene cluster for which independent confi rmation could be established was the inter-leukin-1 (IL-1) locus on chromosome 2q15. Initial microsatellite data implicated IL-1 receptor antagonist (IL-1RN), although this was not subsequently confi rmed. After a larger study instead suggested IL-B, a collaborative study was undertaken of nine single nucleotide polymorphisms (SNPs) in the IL-1 gene cluster, including members IL-1A, IL-1B, IL-1F10 and IL-1RN, in 2675 cases of AS and 2592 healthy controls recruited in 12 different centres in 10 countries, which confi rmed that IL-1A is associ-ated with susceptibility to AS (although association of the other IL-1 gene complex members could not be excluded in specifi c populations). 17
reactive arthritis in the setting of HIV infection where an asso-ciation is also seen with HLA-B*57:03. 10
Several theories have been put forward to explain the associa-tion of HLA-B27 and SpA. 3 The arthritogenic peptide hypoth-esis suggests that disease results from the ability of HLA-B27 to bind a unique peptide or a set of antigenic peptides. However, identifi cation of such an ‘arthritogenic peptide’ has been elusive. That said, the current genetic models favour this hypothesis.
Another theory rests on the propensity for HLA-B27 heavy chains to self-associate or form homodimers due to the pres-ence of Cys67 residue (unique to HLA-B27) in their extracellular α1 domain. HLA-B27 heavy chains would then misfold in the endoplasmic reticulum, are retained there by BiP and give rise to a proinfl ammatory unfolded protein response. Also, HLA-B27 homodimers are expressed on the cell surface and are ligands for a number of natural killer and related cell surface receptors. The fact that most HLA-B27-positive individuals do not develop SpA suggests that this theory is not adequate by itself to explain susceptibility to AS.
A third theory deals with alteration of intracellular invasion/killing of microorganisms. HLA-B27-positive individuals are more effi cient at handling certain viral infections (HIV, hepatitis C, infl uenza) and less able to combat other intracellular bacte-rial infections ( Salmonella , Shigella , Chlamydia , etc). Inability to eliminate these microorganisms contributes to susceptibility to SpA, further suggested by older data demonstrating the pres-ence of bacterial antigens or DNA in the synovium of patients with reactive arthritis. 11
Less than 5% of HLA-B27-positive people in the general population develop SpA. On the other hand, 20% of HLA-B27-positive relatives of patients with AS will develop SpA. 12 Family studies have suggested that HLA-B27 forms only about 40% of
Table 1 HLA-B27 subtype frequencies (%) in different world populations Population 27:01 27:02 27:03 27:04 27:05 27:06 27:07 27:08 27:09 27:13 27:14
Northern Europe 10 90 Denmark 10 90 Southern Europe 20 80 Spain (Galicia) 18 80 3 Northern Spain 7 91 1 1 Azores 7 86 7 Italy 30 65 2 3 Sardinia 3 77 20 Greece 34 8 50 8 Cyprus 52 32 17 Turkey 7 30 43 14 5 Lebanon 24 12 35 30 Jewish 48 3 38 13 Siberia 14 84 2North India 33 61 6 West India 34 34 18 12 2Japan 82 18 Chinese 2 66 31 2 Taiwan 0.05 0.5 87 4 7 2 0.02 Taiwan (Han) 3 94 6 Taiwan Aborigines 100 Chinese Indonesian 38 62 Native Indonesian 6 6 89 Malays 19 6 72 3 Thailand 42 5 53 Maoris 36 64 Brazil 10 6 80 3 North Africa 50 50 West Africa 32 68
Only fi rst more common B27 subtypes are shown.
04_annrheumdis140574.indd 4504_annrheumdis140574.indd 45 1/28/2011 10:10:43 PM1/28/2011 10:10:43 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574i46
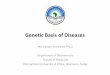
In a follow-up study of 2300 British, US and Australian cases of AS of white European descent examining 370 000 SNPs using Illumina HumHap300 microarray genotyping slides, the ERAP1 and IL-23R associations were extended and additional regions were implicated in AS susceptibility, including gene deserts at chromosome 2p15 and 21q22 and additional candidate genes IL-1 receptor 2 ( IL-1R2 ) and anthraxin receptor 2 ( ANTXR2 ) 32 ( fi gure 1 ).
The gene desert at 2p15 has not previously been associated with any other disease and there are no other genes in the immediate vicinity. The gene desert at 21q22 has previously been associated with paediatric IBD, 33 although the associa-tion in our dataset did not change with exclusion of clinical IBD cases. As with 2p15, there are no genes in the immediate vicinity.
Another gene implicated in this study was IL-1R2 , which is not associated with any other disease. It acts as a decoy recep-tor, interfering with the binding of IL-1 to IL-1R1. It may be acted upon by ERAP1 in cleavage. IL-1R2 is not differentially expressed in AS, and the association may refl ect linkage with IL-1R1 located nearby.
The fourth new gene implicated in this genome-wide associa-tion study (GWAS) was ANTXR2 . The ANTXR2 gene encodes ANTXR2 (capillary morphogenesis protein-2). The protein binds to collagen IV and laminin, suggesting that it may be involved in extracellular matrix adhesion. Mutations of this gene cause juvenile hyaline fi bromatosis and infantile systemic hyalinosis. 34 It is not known to be associated with any other disease and is not differentially expressed in AS.
More recent studies using computer-automated chip genotyp-ing have allowed denser examination of the genome. A study of British and US patients with AS (the Australo-Anglo-American Spondylitis Consortium or TASC, in collaboration with the Wellcome Trust Case Control Consortium) identifi ed an asso-ciation with a non-MHC gene encoding an endoplasmic reticu-lum aminopeptidase, ERAP1 18 (previously known as ARTS-1 ). This has been subsequently confi rmed in an independent cohort from the UK, as well as in additional patients from the USA, Canada, Portugal, Hungary and China. 19 – 23
ERAP1 has two known functions, either of which may explain its association with AS. Within the endoplasmic reticu-lum, ERAP1 is involved in trimming peptides to the optimal length for MHC class I presentation. 24 This would suggest that antigen presentation is crucial in the pathogenesis of AS. The second known function of ERAP1 is that it cleaves cell surface receptors for the proinfl ammatory cytokines IL-1 (IL-1R2), IL-6 (IL-6Rα) and TNF (TNFR1), thereby downregulating their signalling. 25
Based on the observation that the IL-23 receptor (IL-23R) locus was associated with IBD 26 and subsequently psoriasis, 27 an analy sis was performed of seven SNPs in the IL-23R gene in 532 UK and 903 North American patients with AS. The most signifi cant association was with the same SNP found in IBD, rs11209026. This SNP was associated as part of an extended hap-lotype and not independently. The association of IL-23R with AS has subsequently been confi rmed in studies from Canada, Spain, Portugal and Hungary, although it was not associated with AS in Koreans and inconsistently in two studies from China. 21 23 28 – 31
Table 2 MHC and non-MHC genes associated with ankylosing spondylitis (updated from Reveille 3 ) Genes defi nitely associated with AS Chromosome Function Comment
HLA-B27 6p21.3 Presents endogenously processed antigens to T cells Perhaps the best example of a disease association with a hereditary marker
HLA-B60 ( B*4001 ) 6p21.3 Presents endogenously processed antigens to T cells Replicated in Caucasians and non-CaucasiansERAP1 5q15 Trims intracellular peptides to the optimal length for
loading onto MHC class I moleculesReplicated in two different studies, likely a real association
IL-23R 1p31.3 Promotes the differentiation of naïve CD4 T cells into helper Th17 T cells (Th17)
Replicated in studies from Spain, the UK and Canada. Association not seen in Koreans or Chinese
Kinesin family 21B (KIF21B) 1q31 A plus end-directed kinesin motor protein used to transport essential cellular components along axonal and dendritic microtubules
Seen in recent GWAS Caucasian IBD and AS patients; additional replication pending
IL-1R2 2q11-12 Acts as a decoy receptor, interfering with the binding of IL-1 to IL-1R1
Seen and independently confi rmed in one study. Confi rmation in other cohorts pending
Anthraxin receptor 2 (ANTXR2) 4q21 Binds to collagen IV and laminin, possibly involved in extracellular matrix adhesion
Seen and independently confi rmed in one study. Confi rmation in other cohorts pending
Signal transducer and activator of transcription 3 (STAT3)
17q21 A cytoplasmic transcription factor that is activated by IL-5, IL-6, IL-11, among others
Seen in European, US and Chinese AS and IBD patients
Genes replicated but not consistently associated with AS CYP2D6 22q13.1 Involved in the metabolism of xenobiotics Limited to North European Caucasians, not seen in recent
GWASIL-1 genes (primarily IL-1A) 2q12.1 Important modulators of the Th1 response Replicated in most ethnic groups, not seen in recent
GWASANKH 5p15.2 Exports inorganic pyrophosphate from intracellular to
extracellular compartments. Regulates tissue calcifi cationSeen in a relatively small North American and marginally in a Japanese AS cohort. Not replicated in a large UK AS cohort – a disease severity gene
TLR4 9q32-33 A pattern recognition receptor in innate immunity for lipopolysaccharide
Associated in Finns and Newfoundlanders, not confi rmed in several other studies or GWASs
Killer immunoglobulin-like receptors (KIR) 19q13.4 Regulates activation of NK cells via recognition of HLA class I molecules on target cells
Seen in small cohorts of Spanish and Chinese patients, not replicated in a larger cohort of UK patients
Genes associated with AS in one study but failed replication TGFB1 19q13.1 Mediates infl ammation, fi brosis and bone remodelling Marginal association in one study, two subsequent
studies negativeCD14 5q31.1 Receptor on monocytes important in apoptosis, binds
lipopolysaccharideSeen in one small cohort of Finnish AS patients, not confi rmed elsewhere
TNAP 1p36.1 A phosphoethanolamine and pyridoxal-5′-PO4 acting-ectophosphatase. Degrades PPi
One study showing an association in Caucasians not confi rmed in Asians
AS, ankylosing spondylitis; GWAS, genome-wide association study; IBD, infl ammatory bowel disease; IL, interleukin.
04_annrheumdis140574.indd 4604_annrheumdis140574.indd 46 1/28/2011 10:10:43 PM1/28/2011 10:10:43 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574 i47
severe disease. HLA-Cw6 preferentially presented cross-reactive peptides from streptococcal M protein and the hyperprolifera-tive keratin K17 to skin homing CD8 T cells, suggesting that the evolution of guttate into chronic plaque psoriasis might refl ect a transition from a self-limited response to Streptococcus initiated in the tonsils to a sustained response to homologous peptides derived from hyperproliferative skin keratins. 39
Previous family studies using microsatellite markers impli-cated the most important region of psoriasis susceptibility mapped to a 60 kb interval telomeric to HLA-C known as PSORS1. 40 Sequencing of this region has implicated HLA-C itself. 41 Environmental factors such as trauma, stress and infec-tions such as streptococcal pharyngitis have also been impli-cated. GWASs in psoriasis have implicated a number of genes encoding cytokines and cytokine pathways in psoriasis suscep-tibility ( table 3 , fi gure 2 ). 42 43 A recent GWAS in Caucasians has identifi ed genes in the Th17 pathway including IL-12B (the p40 subunit of IL-23 and IL-12), IL-23A (the p19 subunit of IL-23) and IL-23R (encoding a subunit of the IL-23 receptor), as well as genes in the nuclear factor κB (NFκB) pathway (TNFAIP3-TNF-α induced protein 3 and TNIP1-TNFAIP3 interacting protein 1) and genes in the Th2 pathway (IL-4, IL-13). 42 A concomitant study in Chinese patients with psoriasis replicated the MHC and IL-12B associations and identifi ed a new susceptibility locus within the LCE gene cluster on 1q21, 43 which contains multiple conserved genes that encode stratum corneum proteins and are expressed relatively late during fetal assembly of the skin corni-fi ed envelope. Most recently, the Wellcome Trust Case Control Consortium 2 and the Genetic Analysis of Psoriasis Consortium have identifi ed multiple new loci in psoriasis susceptibility. Independent confi rmation will be necessary to better under-stand their role in psoriasis vulgaris and PsA susceptibility. 44
Probably due to phenotypic heterogeneity and case ascertain-ment, the genetics of PsA is not as well defi ned, although asso-ciations with HLA class I alleles (ie, HLA-B38, B39 and B27) have consistently been reported. Studies from the UK and Canada have implicated genes in the IL-1 gene complex 45 46 as well as IL-13, 47 48 and a recent GWAS has identifi ed a region at chromo-some 4q27 that has been implicated in a number of autoimmune diseases. 49
GENES AND IBD SUSCEPTIBILITY Sacroiliitis and spondylitis occur in up to 20% of patients with IBD. Moreover, studies from Europe have shown that 22–69% of patients with AS have microscopic evidence of gut infl amma-tion, although only about 7% develop Crohn’s disease. 50 51
Other SNPs that were increased in frequency but did not achieve genome-wide signifi cance in the TASC study included the gene encoding tumour necrosis factor receptor 1 ( TNFR1 ), which was seen in the discovery set but not in the confi rma-tion set, although it was also seen in a subsequent study in Han Chinese patients with AS. TNFR1 is differentially expressed in AS, and TNF overexpression signals via TNFR1 in mice led to spondyloarthritis. Other SNPs implicated included those in the TNF-associated death domain ( TRADD ) gene, which was found and confi rmed in the UK patients but not North American patients, as well as in CARD9 and STAT3 . In a subsequent study of 775 Han Chinese patients with AS and 1587 controls from Shanghai and Nanjing, the associations with ERAP1 , STAT3 , TNFR1 and the gene desert on 2p15 were further confi rmed 35 and, in another study examining genes implicated in suscep-tibility to IBD, associations with KIF21B and CDKAL1 were established. 36
GENETIC SUSCEPTIBILITY IN AAU AAU affects approximately 40% of patients with AS over time and can occur in patients with no evidence of SpA. Over 90% of patients with B27-associated AAU have SpA. Although iritis rarely precedes the clinical onset of AS, it is often the fi rst clue to the recognition that low back pain is infl ammatory. Half of patients with anterior uveitis have HLA-B27. A study of micro-satellite markers in 76 affected sibpairs with AAU found strong linkage to a region on chromosome 9p21–9p24 and, when com-pared with a companion cohort of AS families without AAU, the linkage at this region was found in association with AAU but not with AS. 37 In addition to this, a GWAS from this group has implicated ERAP1 and IL-23R as well as novel genes whose confi rmation is pending.
GENETICS OF PSORIASIS AND PSA PsA is another disease encountered in the spectrum of SpA and is associated with spondylitis. The prevalence of psoriasis is much higher among fi rst-degree relatives of probands with PsA than in the general population. Moreover, in one recent study, the recurrence risk ratio for fi rst-degree relatives (λ 1 ) for PsA was 30.4 and that for psoriasis was 7.6, suggesting a stronger heritability for PsA than psoriasis per se. 38 Early studies impli-cated HLA-B13, B37 and B57, which subsequently were found to be in linkage disequilibrium with HLA-Cw6. The HLA-Cw6 association is specifi cally seen in those with plaque and guttate (although not with palmoplantar) psoriasis and indicates higher risk for younger age at onset, familial aggregation and more
Figure 1 Innate immunity, antigen presentation and the Th17 pathway all implicated in susceptibility to ankylosing spondylitis (AS).
04_annrheumdis140574.indd 4704_annrheumdis140574.indd 47 1/28/2011 10:10:43 PM1/28/2011 10:10:43 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574i48
GWASs have also implicated genes in the Th17 pathway such as IL-23R on chromosome 1p31, a fi nding that has been reproduced extensively in replication cohorts of patients with Crohn’s disease or ulcerative colitis, 26 and others such as STAT3 . More recently, an intergenic region on chromosome 10q21.1 and a coding variant in ATG16L1 (2q37), which is expressed in intestinal epithelial cell lines, have been implicated and repli-cated in IBD susceptibility. 55 56 Functional knockdown of this gene abrogates autophagy of Salmonella typhimurium . 56 Dendritic cells (DCs) from patients with Crohn’s disease with susceptibil-ity variants in NOD2 or ATG16L1 are defi cient in autophagy induction, suggesting that NOD2 infl uences bacterial degra-dation and interacts with the MHC class II antigen presenta-tion machinery within DCs, and that ATG16L1 and NOD2 are linked within a functional pathway. 57 Also reported were strong associations with independent replication to variation in the genomic regions encoding PHOX2B, NCF4 and a predicted gene on 16q24.1 ( FAM92B ) ( fi gure 3 ). Most recently, a number
The most consistent region for IBD susceptibility on genome-wide screens has been found on chromosome 16q12 (IBD1) at NOD2/ CARD15, 52 53 whose product serves as an intracellular receptor for bacterial products in monocytes and transduces sig-nals leading to NFκB activation. Mutant alleles of NOD2 have been associated with susceptibility to Crohn’s disease in most ethnic groups; 10–30% of patients with Crohn’s disease are hetero zygotes and 3–15% are homozygotes for one of three NOD2 mutations compared with 8–15% and 0–1% of controls, respectively. NOD2 explains about 20% of the overall genetic susceptibility.
More recently, genes located in a functional haplotype in the susceptibility region IBD5 on chromosome 5, including the genes prolyl 4-hydroxylase through interferon regulatory fac-tor 1 and including the organic cation transporter ( OCTN ) gene cluster has been identifi ed and confi rmed. 54 Although the pre-cise mechanism is not known, mutations in NOD2/CARD15 or OCTNI/II may affect the host’s ability to combat bacteria that gain entry to the host through the gut.
Table 3 MHC and non-MHC genes associated with psoriasis and psoriatic arthritis (updated from Reveille 3 ) Genes defi nitely associated with psoriasis and/or psoriatic arthritis Chromosome Function Comment
HLA-C*06:02 6p21.3 Presents endogenously processed bacterial, viral, tumour or self-derived peptides to α:β T cell receptor on CB8 positive T lymphocytes
Extensively replicated, most highly seen with earlier age onset disease
HLA-B alleles 6p21.3 Presents endogenously processed bacterial, viral, tumour or self-derived peptides to α:β T cell receptor on CB8 positive T lymphocytes
Associations with HLA-B*13, B*37, B*57, B*58 with PsV likely represent linkage with HLA-C*06:02, whereas B*38, B*39 primary PsA association
IL-23 receptor 1p31 Constitutive association of IL-23R with JAK2 and ligand-dependent association with STAT3, as well as IL-23-dependent tyrosine phosphorylation of IL-23R
Not relevant in Eastern Asians
IL-12B 5q31 The IL-12 p40 subunit, or IL-12B, heterodimerises with the IL-12 p35 subunit to form IL-12 and, with the IL-23 p19 subunit, to form IL-23. In addition, IL-12 p40 exists as a monomer and as a homodimer (IL-12 p80). Important in both the Th1 and Th17 responses
Extensively replicated in Caucasian and Asian PsV patients
Genes replicated but not consistently associated with psoriasis and/or psoriatic arthritis IL-13/IL-4 5q31 Critical cytokines in the Th2 response, key in asthma
and anti-parasitic responses; also profi broticIL-13 associated with PsA in two case–control studies. Extensively described in Caucasians, not seen in one Chinese GWAS study
Late cornifi ed envelope (LCE) genes 1q21 The LCE cluster contains multiple conserved genes that encode stratum corneum proteins
A gene deletion has been described in Chinese and West European patients in both PsV and PsA, but not in Germany
Chromosome 4q27 gene cluster 4q27 This region harbours the IL-2 and IL-21 genes (both critical in the Th2 response). IL-21 has been implicated in the epidermal hyperplasia of psoriasis
Associated with four autoimmune diseases (celiac disease, type 1 diabetes, Grave’s disease and rheumatoid arthritis)
CDKAL1 6p22.3 Function unknown, highest expression in skeletal muscle and brain cells
Associated with multiple autoimmune diseases and PsV in the UK and USA, seen in case: control studies though not confi rmed in GWASs
MICA 6p21.3 Stimulates NK and T cell effector functions by engagement of NKG2D, enhances cytokine release from T effector cells
Associated with PsV in Chinese and Thai patients and MICA-A9 with PsA in Italian, Croat, Spanish, Jewish patients
IL-1 gene complex (IL-1A, IL-1B, IL-1RN) 2q12.1 Important modulators of the Th1 response Associated primarily with psoriatic arthritis in two case–control studies from the UK and Canada. Not seen on PsV GWASs
ADAM33 20p13 A member of the disintegrin and metalloproteinase domain family of proteins
Associated in UK, US, French, Chinese case: control studies but not GWASs
Genes associated with psoriasis and/or psoriatic arthritis in one study, independent replication pending TNFα-induced protein 3 (TNFAIP3) 6q23 Downregulates NFκB signalling through the
cooperative activity of its two ubiquitin-editing domains
Not seen in a GWAS of Chinese PsV patients
TNFAIP3-interacting protein 1 (TNIP1 or NAF1) 5q32 Increases cell surface expression of CD4; attenuates activated ERK2 signalling
Not seen in a GWAS of Chinese PsV patients
Novel GWAS associations pending independent replication ERAP1, IL-28RA, REL, IF1H1, TRAF31P2, NFKB1A, TYK2 Multiple genes with important impact on immunologic
functionRecently identifi ed in WTCCC2 dataset, ERAP1 interacts with HLA-C*06:02. Needs replication elsewhere
Genes associated with psoriasis and/or psoriatic arthritis in one study, not replicated Protein tyrosine phosphatase, PTPN22, MTHFR, VEGF, small proline rich (SPRR) and peptidoglycan recognition protein (PGLYRP), vascular endothelial growth factor (VEGF), SPRR and PGLYRP, IL-20RA and RB, ZNF313/RNF114, fi laggrin, serotonin receptor 2A, CTLA4, ACEI, vitamin D receptor genes, LMP and TAP, TNF, CYP2S1, retinoid X receptor, HLA-DRB1
GWAS, genome-wide association study; IL, interleukin; PsA, psoriatic arthritis; PsV, PsV, psoriasis vulgaris; TNF, tumour necrosis factor.
04_annrheumdis140574.indd 4804_annrheumdis140574.indd 48 1/28/2011 10:10:44 PM1/28/2011 10:10:44 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574 i49
However, apart from the MHC genes, the individual contribu-tions of individual non-MHC genes or SNPs is quite small, the causal variants are yet to be identifi ed, and much of the genetic variance is still unexplained. Hence, the use of genetic testing outside HLA-B27 is premature.
Funding This study was supported by grant P01-052915-01.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES 1. Brown MA, Laval SH, Brophy S, et al. Recurrence risk modelling of the genetic
susceptibility to ankylosing spondylitis. Ann Rheum Dis 2000 ; 59 : 883 – 6 .
2. Brown MA, Kennedy LG, MacGregor AJ, et al. Susceptibility to ankylosing
spondylitis in twins: the role of genes, HLA, and the environment. Arthritis Rheum
1997 ; 40 : 1823 – 8 .
3. Reveille JD. Recent studies on the genetic basis of ankylosing spondylitis.
Curr Rheumatol Rep 2009 ; 11 : 340 – 8 .
4. Reveille JD, Maganti RM. Subtypes of HLA-B27: history and implications in the
pathogenesis of ankylosing spondylitis. Adv Exp Med Biol 2009 ; 649 : 159 – 76 .
5. Galocha B, de Castro JA. Folding of HLA-B27 subtypes is determined by the global
effect of polymorphic residues and shows incomplete correspondence to ankylosing
spondylitis. Arthritis Rheum 2008 ; 58 : 401 – 12 .
6. Chalmers IM. Ankylosing spondylitis in African Blacks. Arthritis Rheum 1980 ; 23 : 1366 – 70 .
7. Hill AV, Allsopp CE, Kwiatkowski D, et al. HLA class I typing by PCR: HLA-B27 and an
African B27 subtype. Lancet 1991 ; 337 : 640 – 2 .
8. Gonzalez-Roces S, Alvarez MV, Gonzalez S, et al. HLA-B27 polymorphism and
worldwide susceptibility to ankylosing spondylitis. Tissue Antigens 1997 ; 49 : 116 – 23 .
9. Khan MA. Race-related differences in HLA association with ankylosing spon-
dylitis and Reiter’s disease in American blacks and whites. J Natl Med Assoc
1978 ; 70 : 41 – 2 .
10. Díaz-Peña R, Blanco-Gelaz MA, Njobvu P, et al. Infl uence of HLA-B*5703 and HLA-
B*1403 on susceptibility to spondyloarthropathies in the Zambian population.
J Rheumatol 2008 ; 35 : 2236 – 40 .
of new genes have been identifi ed in Crohn’s disease and UC susceptibility by GWAS and meta-analysis approaches, bringing the total of IBD susceptibility loci up to 71 58 – 60 ; their complete delineation is outside the scope of this review. However, only 25% of the genetic variance for IBD is explained by the genes ascertained thus far, suggesting a need for future studies to iden-tify rare variants and recessive traits not easily identifi able by GWAS approaches.
CONCLUSIONS AND FUTURE DIRECTIONS Signifi cant advances have been made recently in elucidating the genetic basis of SpA. In AS, along with recent studies confi rm-ing other MHC (ie, B*40:01 ) and non-MHC (IL-1A) infl uences in addition to HLA-B27, GWASs have shown an important impact of other genes such as ERAP1, IL-23R as well as other genes and genetic regions (gene deserts on chromosomes 2 and 21, IL-1R2, ANTXR2 and STAT3, TNFR1, TRADD, CARD9). In psoriasis and PsA, the MHC component has also been dissected and is likely to include at least HLA-C and possibly other MHC infl u-ences. In addition, TH17 cytokine genes in common with AS (IL-23R) and unique to Ps (IL-12, IL-23A), as well as TH2 cyto-kines (IL-4, IL-13) and NFκB pathway genes (TNFAIP3, TNIP1), have been implicated. In IBD, genes important in the innate immune response (NOD2), autophagy (ATG6L1) and regulation of the IL-23 pathway (IL-23R) play a role in disease susceptibil-ity. These data suggest that genetic markers in susceptibility to AS, psoriasis and IBD are both disease-specifi c and class-specifi c, suggesting common mechanisms of susceptibility and patho-genesis. There is also the possibility that these markers could be used along with HLA testing (particularly B27) in diagnosis.
Figure 2 Innate immunity, antigen presentation and the Th17 pathway all implicated in susceptibility to psoriasis and psoriatic arthritis.
Figure 3 Innate immunity, autophagy and the Th17 pathway all implicated in Crohn’s disease.
04_annrheumdis140574.indd 4904_annrheumdis140574.indd 49 1/28/2011 10:10:44 PM1/28/2011 10:10:44 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

Supplement
Ann Rheum Dis 2011;70(Suppl 1):i44–i50. doi:10.1136/ard.2010.140574i50
35. Davidson S, Danoy P, Thomas GP, et al. Association of STAT3 and TNFSF1A with
ankylosing spondylitis in Han Chinese. Ann Rheum Dis 2010;( In Press ).
36. Danoy P, Pryce K, Hadler J, et al. Association of variants at 1q32 and STAT3 with
ankylosing spondylitis suggests genetic overlap with Crohn’s disease. PLoS Genet
2010; 6:e1001195.
37. Martin TM, Zhang G, Luo J, et al. A locus on chromosome 9p predisposes to a
specifi c disease manifestation, acute anterior uveitis, in ankylosing spondylitis,
a genetically complex, multisystem, infl ammatory disease. Arthritis Rheum
2005 ; 52 : 269 – 74 .
38. Chandran V, Schentag CT, Brockbank JE, et al. Familial aggregation of psoriatic
arthritis. Ann Rheum Dis 2009 ; 68 : 664 – 7 .
39. Johnston A, Gudjonsson JE, Sigmundsdottir H, et al. Peripheral blood T cell
responses to keratin peptides that share sequences with streptococcal M proteins are
largely restricted to skin-homing CD8(+) T cells. Clin Exp Immunol 2004 ; 138 : 83 – 93 .
40. Nair RP, Stuart P, Henseler T, et al. Localization of psoriasis-susceptibility locus
PSORS1 to a 60-kb interval telomeric to HLA-C. Am J Hum Genet 2000 ; 66 : 1833 – 44 .
41. Elder JT. Genome-wide association scan yields new insights into the
immunopathogenesis of psoriasis. Genes Immun 2009 ; 10 : 201 – 9 .
42. Nair RP, Duffi n KC, Helms C, et al. Genome-wide scan reveals association of
psoriasis with IL-23 and NF-kappaB pathways. Nat Genet 2009 ; 41 : 199 – 204 .
43. Zhang XJ, Huang W, Yang S, et al. Psoriasis genome-wide association study
identifi es susceptibility variants within LCE gene cluster at 1q21. Nat Genet
2009 ; 41 : 205 – 10 .
44. Strange A, Capon F, Spencer CC, et al. A genome-wide association study identifi es
new psoriasis susceptibility loci and an interaction between HLA-C and ERAP1.
Nat Genet 2010 ; 42 : 985 – 90 .
45. Ravindran JS, Owen P, Lagan A, et al. Interleukin 1alpha, interleukin 1beta and
interleukin 1 receptor gene polymorphisms in psoriatic arthritis. Rheumatology
(Oxford) 2004 ; 43 : 22 – 6 .
46. Peddle L, Butt C, Snelgrove T, et al. Interleukin (IL) 1alpha, IL1beta, IL receptor
antagonist, and IL10 polymorphisms in psoriatic arthritis. Ann Rheum Dis
2005 ; 64 : 1093 – 4 .
47. Chang M, Li Y, Yan C, et al. Variants in the 5q31 cytokine gene cluster are associated
with psoriasis. Genes Immun 2008 ; 9 : 176 – 81 .
48. Duffi n KC, Freeny IC, Schrodi SJ, et al. Association between IL13 polymorphisms
and psoriatic arthritis is modifi ed by smoking. J Invest Dermatol 2009 ; 129 : 2777 – 83 .
49. Liu Y, Helms C, Liao W, et al. A genome-wide association study of psoriasis and
psoriatic arthritis identifi es new disease loci. PLoS Genet 2008 ; 4 : e1000041 .
50. Mielants H, Veys EM, Goemaere S, et al. Gut infl ammation in the
spondyloarthropathies: clinical, radiologic, biologic and genetic features in relation to
the type of histology. A prospective study. J Rheumatol 1991 ; 18 : 1542 – 51 .
51. Leirisalo-Repo M, Turunen U, Stenman S, et al. High frequency of
silent infl ammatory bowel disease in spondylarthropathy. Arthritis Rheum
1994 ; 37 : 23 – 31 .
52. Hugot JP, Chamaillard M, Zouali H, et al. Association of NOD2 leucine-rich repeat
variants with susceptibility to Crohn’s disease. Nature 2001 ; 411 : 599 – 603 .
53. Ogura Y, Bonen DK, Inohara N, et al. A frameshift mutation in NOD2 associated with
susceptibility to Crohn’s disease. Nature 2001 ; 411 : 603 – 6 .
54. Peltekova VD, Wintle RF, Rubin LA, et al. Functional variants of OCTN cation
transporter genes are associated with Crohn disease. Nat Genet 2004 ; 36 : 471 – 5 .
55. Rioux JD, Xavier RJ, Taylor KD, et al. Genome-wide association study identifi es
new susceptibility loci for Crohn disease and implicates autophagy in disease
pathogenesis. Nat Genet 2007 ; 39 : 596 – 604 .
56. Hampe J, Franke A, Rosenstiel P, et al. A genome-wide association scan of
nonsynonymous SNPs identifi es a susceptibility variant for Crohn disease in ATG16L1.
Nat Genet 2007 ; 39 : 207 – 11 .
57. Cooney R, Baker J, Brain O, et al. NOD2 stimulation induces autophagy in dendritic
cells infl uencing bacterial handling and antigen presentation. Nat Med 2010 ; 16 : 90 – 7 .
58. Imielinski M, Baldassano RN, Griffi ths A, et al. Common variants at fi ve
new loci associated with early-onset infl ammatory bowel disease. Nat Genet
2009 ; 41 : 1335 – 40 .
59. McGovern DP, Jones MR, Taylor KD, et al. Fucosyltransferase 2 (FUT2) non-secretor
status is associated with Crohn’s disease. Hum Mol Genet 2010 ; 19 : 3468 – 76 .
60. McGovern DP, Gardet A, Törkvist L, et al. Genome-wide association identifi es
multiple ulcerative colitis susceptibility loci. Nat Genet 2010 ; 42 : 332 – 7 .
11. Gérard HC, Branigan PJ, Schumacher HR, Jr, et al. Synovial Chlamydia trachomatis
in patients with reactive arthritis/Reiter’s syndrome are viable but show aberrant
gene expression. J Rheumatol 1998 ; 25 : 734 – 42 .
12. van der Linden SM, Valkenburg HA, de Jongh BM, et al. The risk of developing
ankylosing spondylitis in HLA-B27 positive individuals. A comparison of relatives of
spondylitis patients with the general population. Arthritis Rheum 1984 ; 27 : 241 – 9 .
13. Robinson WP, van der Linden SM, Khan MA, et al. HLA-Bw60 increases
susceptibility to ankylosing spondylitis in HLA-B27+ patients. Arthritis Rheum
1989 ; 32 : 1135 – 41 .
14. Brown MA, Pile KD, Kennedy LG, et al. HLA class I associations of ankylosing
spondylitis in the white population in the United Kingdom. Ann Rheum Dis
1996 ; 55 : 268 – 70 .
15. Wei JC, Tsai WC, Lin HS, et al. HLA-B60 and B61 are strongly associated with
ankylosing spondylitis in HLA-B27-negative Taiwan Chinese patients. Rheumatology
(Oxford) 2004 ; 43 : 839 – 42 .
16. Vargas-Alarcón G, Garcia A, Bahena S, et al. HLA-B alleles and complotypes
in Mexican patients with seronegative spondyloarthropathies. Ann Rheum Dis
1994 ; 53 : 755 – 8 .
17. Sims AM, Timms AE, Bruges-Armas J, et al. International Genetics of Ankylosing
Spondylitis. Prospective meta-analysis of interleukin 1 gene complex polymorphisms
confi rms associations with ankylosing spondylitis. Ann Rheum Dis 2008 ; 67 : 1305 – 9 .
18. WTCCC/TASC. Association scan of 14,500 nsSNPs in four common diseases
identifi es variants involved in autoimmunity. Nat Genet 2007; 39 :1329–37.
19. Maksymowych WP, Inman RD, Gladman DD, et al. Association of a specifi c ERAP1/
ARTS1 haplotype with disease susceptibility in ankylosing spondylitis. Arthritis Rheum
2009 ; 60 : 1317 – 23 .
20. Tsui FW, Haroon N, Reveille JD, et al. Association of an ERAP1 ERAP2 haplotype
with familial ankylosing spondylitis. Ann Rheum Dis 2010 ; 69 : 733 – 6 .
21. Pimentel-Santos FM, Ligeiro D, Matos M, et al. Association of IL23R and ERAP1
genes with ankylosing spondylitis in a Portuguese population. Clin Exp Rheumatol
2009 ; 27 : 800 – 6 .
22. Pazár B, Sáfrány E, Gergely P, et al. Association of ARTS1 gene polymorphisms with
ankylosing spondylitis in the Hungarian population: the rs27044 variant is associated
with HLA-B*2705 subtype in Hungarian patients with ankylosing spondylitis.
J Rheumatol 2010 ; 37 : 379 – 84 .
23. Davidson SI, Wu X, Liu Y, et al. Association of ERAP1, but not IL23R, with
ankylosing spondylitis in a Han Chinese population. Arthritis Rheum 2009 ; 60 : 3263 – 8 .
24. Yan J, Parekh VV, Mendez-Fernandez Y, et al. In vivo role of ER-associated peptidase
activity in tailoring peptides for presentation by MHC class Ia and class Ib molecules.
J Exp Med 2006 ; 203 : 647 – 59 .
25. Cui X, Hawari F, Alsaaty S, et al. Identifi cation of ARTS-1 as a novel TNFR1-binding
protein that promotes TNFR1 ectodomain shedding. J Clin Invest 2002 ; 110 : 515 – 26 .
26. Duerr RH, Taylor KD, Brant SR, et al. A genome-wide association study identifi es
IL23R as an infl ammatory bowel disease gene. Science 2006 ; 314 : 1461 – 3 .
27. Cargill M, Schrodi SJ, Chang M, et al. A large-scale genetic association study
confi rms IL12B and leads to the identifi cation of IL23R as psoriasis-risk genes.
Am J Hum Genet 2007 ; 80 : 273 – 90 .
28. Karaderi T, Harvey D, Farrar C, et al. Association between the interleukin 23
receptor and ankylosing spondylitis is confi rmed by a new UK case-control study and
meta-analysis of published series. Rheumatology (Oxford) 2009 ; 48 : 386 – 9 .
29. Rahman P, Inman RD, Gladman DD, et al. Association of interleukin-23 receptor
variants with ankylosing spondylitis. Arthritis Rheum 2008 ; 58 : 1020 – 5 .
30. Rueda B, Orozco G, Raya E, et al. The IL23R Arg381Gln non-synonymous
polymorphism confers susceptibility to ankylosing spondylitis. Ann Rheum Dis
2008 ; 67 : 1451 – 4 .
31. Sung IH, Kim TH, Bang SY, et al. IL-23R polymorphisms in patients with ankylosing
spondylitis in Korea. J Rheumatol 2009 ; 36 : 1003 – 5 .
32. Reveille JD, Sims AM, Danoy P, et al. Genome-wide association study of ankylosing
spondylitis identifi es non-MHC susceptibility loci. Nat Genet 2010 ; 42 : 123 – 7 .
33. Kugathasan S, Baldassano RN, Bradfi eld JP, et al. Loci on 20q13 and 21q22
are associated with pediatric-onset infl ammatory bowel disease. Nat Genet
2008 ; 40 : 1211 – 15 .
34. Hanks S, Adams S, Douglas J, et al. Mutations in the gene encoding capillary
morphogenesis protein 2 cause juvenile hyaline fi bromatosis and infantile systemic
hyalinosis. Am J Hum Genet 2003 ; 73 : 791 – 800 .
04_annrheumdis140574.indd 5004_annrheumdis140574.indd 50 1/28/2011 10:10:47 PM1/28/2011 10:10:47 PM
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from

doi: 10.1136/ard.2010.140574 2011 70: i44-i50Ann Rheum Dis
John D Reveille The genetic basis of spondyloarthritis
http://ard.bmj.com/content/70/Suppl_1/i44.full.htmlUpdated information and services can be found at:
These include:
References
http://ard.bmj.com/content/70/Suppl_1/i44.full.html#related-urlsArticle cited in:
http://ard.bmj.com/content/70/Suppl_1/i44.full.html#ref-list-1This article cites 57 articles, 17 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 1, 2014 - Published by ard.bmj.comDownloaded from