Embed Size (px)
Citation preview

The Endpoint from a Resistance Point of View
A Symposium to Honor the Career of William A. Craig, M.D.George Drusano, M.D.
Co-DirectorOrdway Research Institute

A Colleague Responsible for Much of What I am About to Show
Dr. Arnold Louie

A Relevant Quote
All Models Are Wrong; Some Models Are Useful
Professor G.E.P. Box, a famous and very wise biostatistician

Pharmacodynamics
• Let us look at an example of “classical antibacterial pharmacodynamics”, where a survivorship endpoint was employed

Role of PK/PD – Survivorship Endpoint
• In this P. aeruginosa rat sepsis model, where a fluoroquinolone was employed for therapy (an AUC/MIC Ratio drug), several things are evident:1. As MIC increases, survivorship decreases (same dose – isogenic mutants) 2. As Dose increases (same MIC) survivorship increases3. Equal AUC/MIC ratios produce equivalent outcomes
Drusano et al. Antimicrob Agents Chemother 1993;37:483-490

Pharmacodynamics• One also needs to think about other
desired endpoints:1. clinical outcome/survivorship2. microbiological outcome/cell kill3. suppression of resistance4. organism population eradication (TB)
• The amount of drug exposure to achieve the endpoints does differ
• Let us look at resistance suppression

Resistance Suppression and Outcome Optimization
• First, we will examine Pseudomonas aeruginosa in a hollow fiber infection model
• Then we will examine this same pathogen in a mouse thigh model of infection
• Then we will examine Staphylococcus aureus and: 1. examine the impact of therapy duration2. examine the divergent effect on sensitive and resistant subpopulations when drug is withdrawn 3. examine the impact of granulocytes

Journal of Clinical Investigation 2003;112:275-285 &Nature Reviews Microbiology 2004;2:289-300
Resistance Suppression and Outcome Optimization

Resistance Suppression and Outcome Optimization
The use of the hollow fiber model for studying antimicrobial regimens was described by Blaser and Zinner and employed extensively by Dudley
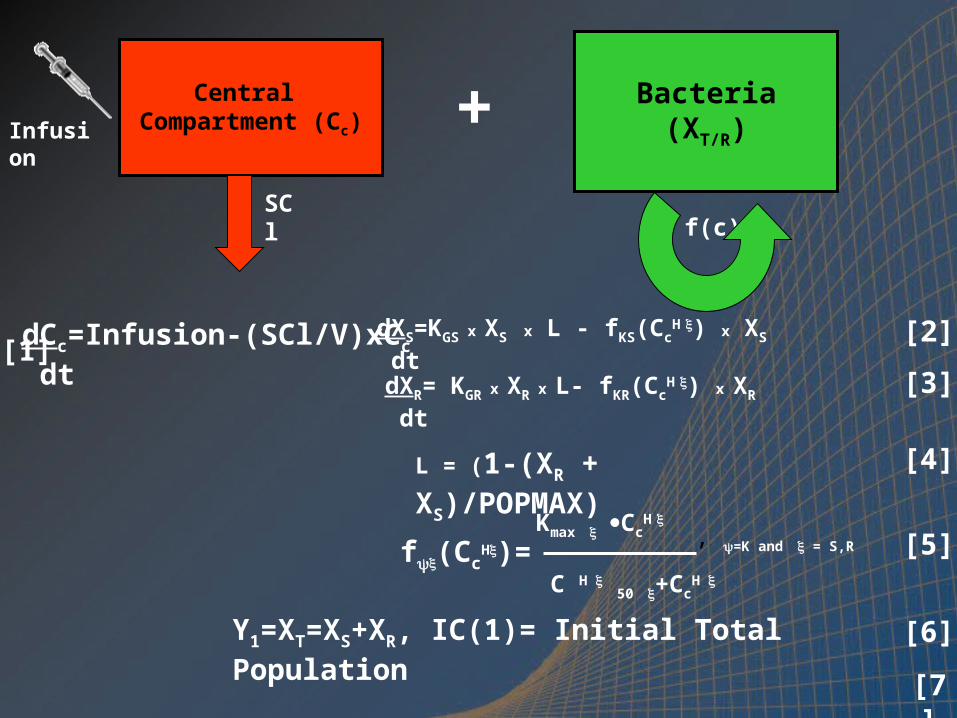
Central Compartment (Cc)Infusion + Bacteria
(XT/R)
f(c)
dCc=Infusion-(SCl/V)xCc
dt
SCl
dXS=KGS x XS x L - fKS(CcH ) x XS
dtdXR= KGR x XR x L- fKR(Cc
H ) x XR
dt
Kmax CcH
C H 50 +Cc
H
f(CcH)=
Y1=XT=XS+XR, IC(1)= Initial Total Population
Y2=XR , IC(2)= Initial Resistant Population
[2]
[3]
[4]
[5]
[6]
, =K and = S,R
[1]
L = (1-(XR + XS)/POPMAX)
[7]

Resistance Suppression and Outcome Optimization
Tam V et al. Bacterial-population responses to drug selective pressure: Examination of garenoxacin’s effect on Pseudomonas aeruginosa. J Infect Dis 2005;192:420-428
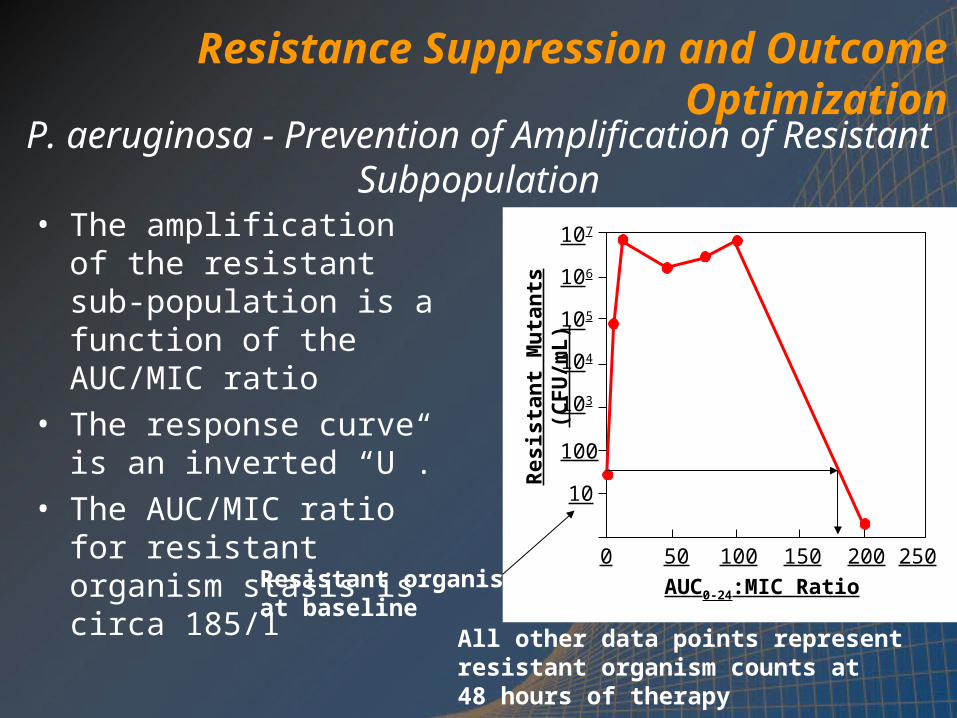
P. aeruginosa - Prevention of Amplification of Resistant Subpopulation
• The amplification of the resistant sub-population is a function of the AUC/MIC ratio
• The response curve is an inverted “U”.
• The AUC/MIC ratio for resistant organism stasis is circa 185/1
Resistant organismsat baseline
All other data points representresistant organism counts at48 hours of therapy
0 50 100 150 200 250
10
100
103
104
106
AUC0-24:MIC Ratio
Resis
tan
t M
uta
nts
(C
FU
/mL)
107
105
Resistance Suppression and Outcome Optimization

Resistance Suppression and Outcome Optimization
Propspective Validation Study
Tam V et al. Bacterial-population responses to drug selective pressure: Examination of garenoxacin’s effect on Pseudomonas aeruginosa. J Infect Dis 2005;192:420-428

Levofloxacin and Pseudomonas aeruginosa in a Mouse Thigh Infection Model
Can a drug exposure be identified that will prevent the resistant subpopulation from
taking over the total population?
In contrast to the hollow fiber system, here we have an
immune system

P. aeruginosa outcome studies
Jumbe et al J Clin Invest 2003;112:275-285

Journal of Clinical Investigation 2003;112:275-285 & Nature Reviews Microbiology 2004;2:289-300
0 mg/kg
90 mg/kg
215 mg/kg 600 mg/kg

Peripheral (thigh)Compartment (Cp)
Central Blood Compartment (Cc)IP
injection
kcp kpc
+ Bacteria(XT/R)
f(c)
dCc= kaCa+kpcCp-kcpCc-keCc
dt
ke
dXS=KGS x XS x L - fKS(CcH ) x XS
dtdXR= KGR x XR x L- fKR(Cc
H ) x XR
dt
Kmax CcH
C H
50+CcH
f(CcH)=
Y1=XT=XS+XR
Y2=XR
[4]
[5]
[6]
[7]
[8]
, =K and = S,R
[2]
L = (1- (XR + XS)/POPMAX)
[9]
dCp = kcpCc - kpc Cp
dt
[3]
dCa= -kaCa
dt[1]

Jumbe et al J Clin Invest 2003;112:275-285Drusano GL. Nat Rev Microbiol 2004;2:289-300

Resistance Suppression and Outcome Optimization
Jumbe et al J Clin Invest 2003;112:275-285Drusano GL. Nat Rev Microbiol 2004;2:289-300

Journal of Clinical Investigation 2003;112:275-285 &Nature Reviews Microbiology 2004;2:289-300

PK/PD• We studied the quinolone
garenoxacin against S. aureus
• We studied and modeled 7 regimens
• We performed a prospective validation with 4 hypotheses
• All were validated
• Resistance suppression requires more drug exposure than that for maximal rate of kill

PK/PD• We performed an experiment where 4, 5 or 6 daily
doses of drug (AUC/MIC ratio=100) were administered and the outcomes monitored out to day 13
• We fit an expanded mathematical model to all the data simultaneously
• We included a natural death rate term for sensitive and resistant populations
• This allows us to look at relative biofitness in conjunction with the growth terms for the two populations

PK/PD


PK/PD

PK/PD• So, the longer therapy continues, the more
amplification goes on of the resistant population with a suboptimal regimen
• To prevent resistance, shorter is better
• BUT, we also have to clear the infection, so therapy needs to be long enough to accomplish this end
• How much effect do we need?
• Enough to allow the immune system to do its job!

Parameter Kmax-growth POPMAX Vmax-kill * Km Units h-1 CFU/g h-1 CFU/g
Mean 0.622 0.916x1011 0.00535147660
SD 0.104 0.980x1010 0.00400203928______________________________________________________________________* Rate constant is multiplied by the granulocyte count

BRIDGING TO THE CLINIC Correlation with Pre-Clinical Models
Do These Animal and Hollow Fiber Model Findings Correlate with Suppression of
Resistance in the Clinic?

Taking the expectation demonstrates an overall target attainment of 62% and a predicted emergence of resistance rate of 38%
PK-PD TARTGET ATTAINMENT Ciprofloxacin Against P. aeruginosa
Use of Monte Carlo Simulation

• Peloquin studied 200 mg IV Q 12 h of ciprofloxacin in nosocomial pneumonia - P aeruginosa resistance rate 70% (7/10 - pneumonia only) - 77% (10/13 - all respiratory tract)
• MCS (resistance suppression target) predicts emergence of resistance in 75%
• Fink et al studied ciprofloxacin in nosocomial pneumonia (400 mg IV Q 8 h) - P aeruginosa resistance rate 33% (12/36)
• MCS at this dose and schedule predicts suppression in 62% and emergence of resistance in 38%
Peloquin et al Arch Int Med 1989;1492269-73
Fink et al AAC 1994;38:547-57
MONTE CARLO SIMUATION Is It Predictive?

WHAT ABOUT COMBINATION THERAPY FOR RESISTANCE
SUPPRESSION?
Sometimes, single agent therapy just can’t get the job done

Cefto-Levo Combo vs. P aeruginosa
• We wished to evaluate the combination of ceftobiprole plus levofloxacin
• West et al (Clin Ther 2003;25:485-506) demonstrated that levofloxacin in combination with a β-lactam suppressed Pseudomonas resistance in 17/17 instances in a HAP trial
• We employed a mouse thigh infection model to examine the cefto-levo combination for both cell kill and resistance suppression

Cefto-Levo Combo vs. P aeruginosaMethods
• The mouse thigh infection model as described by Craig was employed (inoculum 1.85 x 107 CFU)
• P aeruginosa ATCC 27853 was employed as the challenge organism (MIC 1.0 – Levo; MIC 2.0 mg/L – Cefto)
• Dose ranging studies were performed for each drug separately
• These were used to design the combination experiment using D-optimal design theory

Cefto-Levo Combo vs. P aeruginosaMethods
• Drug concentrations were measured by LC-MS/MS techniques
• Resistant organisms were determined by plating on agar infused with 2.5XMIC (Levo) or 3XMIC (Cefto)
• Combination cell kill was modeled employing the Universal Response Surface Approach of Greco et al
• The ability to suppress resistant subpopulations was evaluated by Monte Carlo Simulation (Lodise et al AAC 2007;51:2378-2387 for Ceftobiprole; Drusano et al JID 2004;189:1590-1597 for levofloxacin)

Cefto-Levo Combo vs. P aeruginosaResults
Ceftobiprole Single Drug Therapy Levofloxacin Single drug Therapy



Ceftobiprole-Levofloxacin Combination Therapy
Suppress Levofloxacin Resistance Suppress Ceftobiprole Resistance

Ceftobiprole-Levofloxacin Combination Therapy
Suppress Ceftobiprole ResistanceSuppress Levofloxacin
Resistance

Ceftobiprole-Levofloxacin Combination Therapy
• The exposures that suppress resistance in both directions are Ceftobiprole T > MIC of 40% and Levofloxacin AUC/MIC of 6.7
• Monte Carlo simulation demonstrates that doses of 750 mg daily of levofloxacin plus 500 mg of ceftobiprole as a 2 hour infusion every 8 hours achieve these targets 96.4% of the time at a minimum

Ceftobiprole-Levofloxacin Combination Therapy
• Ceftobiprole plus levofloxacin interact productively against Pseudomonas aeruginosa in the mouse thigh model
• Perhaps more importantly, resistance suppression is clearly demonstrable at modest drug exposures for both ceftobiprole and levofloxacin
• Human PK demonstrates that these resistance suppression exposures can be achieved greater that 96% of the time

Ceftobiprole-Levofloxacin Combination Therapy
• THIS MAKES NO SENSE
• For both levo and cefto, the Mex pumps cause efflux
• This means that there should be no cross protection – Right??????
• BUT pumps are Michelis-Menten processes – perhaps the combination saturates the pump
• So, this is a promising combination, at least for wild-type strain

Anti-Infective PK/PDI have been trying to interest the anti-infectivecommunity in antimicrobial pharmacodynamics for almost a quarter of a century, certainlywithout notable success.
WELL!
GeorgeGeorge

THANK YOU FOR YOUR ATTENTION





























