Embed Size (px)
Citation preview

MA
STER
THESIS

The effects on knee abduction angular
velocity after a 6-weeks training period with
the new training device ProPrioPlate- a
pilot study
Johan Herö
2014-04-07
Master Thesis 30 credits in Sports and Exercise Science – Human Performance
Halmstad University
School of Business and Engineering
Supervisors: Ann Bremander, Sofia Brorsson
Examiner: Charlotte Olsson

Abstract
Background: ACL injuries is common and can result in long term disability or even have a
career ending outcome for the athlete. Women are more exposed to ACL injuries than men
are and several factors increase the risk of ACL injuries for women where one is the knee
angle velocity. It seems that prevention programs involving plyometric- and strength training
has been most effective on altering these risk factors for knee injuries. But many programs
involve several exercises which makes it very time consuming. Since the gluteus muscles is
our main hip abductor and hip stabilizer it is of great importance for controlling the knee. The
ProPrioPlate (PPP) is a device that has been validated and shown to activate the gluteus
medius 40% more in a squat compared to a regular bodyweight squat.
Purpose: To investigate if a 6 week long training period, 3 sessions/ week, 5minutes/session
with the PPP could decrease the mean abduction angular velocity (°/sec) of the knee joint in a
Drop jump (DJ) in women with poor knee stability
Method: An experimental study design was used. Twelve female athletes with poor knee
stability and signs of knee valgus in a drop jump conducted a 6 weeks training program to
investigate any changes in abduction angular velocity in a DJ. 3D motion analyzes were
performed before and after the training period. Wilcoxon signed ranked test was used to
investigate if there were any changes in results between the different test occasions.
Results: Median abduction angular velocity of the test performed before the intervention was -
34. 34 (min -70. 65 max -11. 53) deg/sec and after the intervention median -34. 22 deg/sec
(min -51. 97 max -3. 28). The P value was 0.24 which indicate that there were no statistical
significant differences between the three testing occasions. Compliance to the intervention
was low, 15%.
Conclusion: A 6 weeks training period with the PPP did not decrease the abduction angular
velocity. Due to low compliance rate amongst of subjects no conclusion regarding the effect
of the device can be made.
Abstrakt:
Bakgrund: Svenska ligament registret rapporterar ungefär 5000 främre korsbandsskador
(ACL) årligen i Sverige. ACL skador kan resultera i långvarig frånvaro från sporten eller till
och med att idrottaren inte längre kan fortsätta sin karriär. Kvinnor är mer utsatta för ACL
skador än män och det är flera faktorer som ökar risken för ACL skador hos kvinnor.
Forskningen pekar mot att träningsprogram som syftar till att minska risken för knäskador
innefattar styrketräning och plyometrisk träning. Många träningsprogram för att minska risken
för knäskador innefattar många övningar vilket gör det tidskrävande. ProPrioPlate (PPP) är ett
träningsredskap som är validerat och har visats aktivera gluteus medius 40% mer i en knäböj
på PPP jämfört med vanliga knäböj.
Syftet med denna studie var att undersöka knätabduktionshastighet i ett dropp vertikalhopp
innan och efter ett 6 veckors träningsprogram med PPP för kvinnor med bristande
knästabilitet.
Metod: En exprementell studiedesign har använts. Tjugo frivilliga kvinnliga idrottar med
bristande knästabilitet och teckan på valgus vid dropjump genomförde ett 6 veckors
träningsprogram för att undersöka om knäabduktionshastighet i ett dropp vertikalhopp
förändrades efter träningsperioden. 3D analyser på testpersonerna genomfördes innan och
efter träningsperioden. Wilcoxons signed ranked test användes för att undersöka skillnader
mellan de olika test tillfällena.
Resultat: Medianen av abduktionshastigheten före interventionen var -47,88 grader/sek (min -
74,76 max -30.16), -34.34 (min -70.65 max -11.53) och efter interventionen -34.22 (min -
51.97 max -3.28) grader/sek. P värdet var 0.24 vilket indikerar att det inte fanns någon
signifikant skillnad mellan före- och eftertesterna. Följsamheten till träningen hos deltagarna
var låg (15%).
Slutsats: En 6 veckors träningsperiod med PPP minskade inte abduktionshastigheten i ett DJ.
Låg åtföljnad av våra testpersoner till träningsperioden innebar att inga slutsatser gällande
PPP kan utgöras.

Table of content.
1. Background 1
1.1. Purpose 4
2. Method 4
2.1. Subjects 4
2.2. Study design 5
2.3. Kinematics 3D motion analyze of drop jump (DJ) 5
2.4. Training device 6
2.5. Control- & Training period 7
2.6. Ethical and social considerations 7
2.7. Statistical analyses 7
3. Results 8
4. Discussion 10

1. Background
In Sweden the incidence of anterior crucial ligament (ACL) injuries is approximately 5000
per year. Sports like soccer, handball, basketball and alpine skiing has a very high incidence
of ACL injuries in Sweden. ACL injuries can result in long term disability or even have a
career ending outcome for the athlete (Roos, Ornell et al. 1995; Lohmander, Englund et al.
2007). These athletes also have a high risk of developing osteoarthritis 10-15 years after their
injury (Roos, Ornell et al. 1995; von Porat, Roos et al. 2004). The injury appears in turning,
landing with fully extended knees and/or sudden deceleration actions (Moeller and Lamb
1997). Shimokochi and Shultz (2008) found in their literature study that non-contact ACL
injuries are caused by a high quadriceps force combined with frontal plane and/or transverse
plane knee loadings with insufficient hamstring co-contraction, especially when the knee is at
near full extension or in hyperextension. Women are more exposed to ACL injuries than men
and has a 3-5 higher risk to obtain an ACL injury (Frobell, Lohmander et al. 2007). There are
several factors that increase the risk of ACL injuries for women - anatomical biomechanics,
hormonal, neuromuscular function, proprioception and muscle weakness in the stabilizing
muscles for the knee joint during sports- and daily activities (Huston and Wojtys 1996; Lewis
2000). Women’s biomechanical anatomy differs from males which make women more
susceptible to ACL injuries and it is thus more important for them to train properly to avoid
injuries.
Subtalar pronation is associated with ACL injuries (Loudon, Jenkins et al. 1996) and can
increase the valgus angle of the knee joint by increasing the internal rotation of the tibia
(Ford, Myer et al. 2005). Mclean, Lipfert et al. (2004) showed in his study that women
pronated more in a side-cutting movement compared to men, and had significant more knee
valgus. Knee valgus angle and knee abduction movement has shown to be a significant
predictor for ACL injuries (Hewett, Myer et al. 2005). Knee valgus is an unwanted position
both for performance (Schoenfeld 2010) and the risk of injury (Quatman and Hewett 2009).
Knee valgus is a combination of rotation from the three lower extremities joints, hip
adduction and internal rotation, knee abduction which is external rotation of the tibia, and
subtalar eversion also known as foot pronation (Hewett, Myer et al. 2006). Lateral movement
of the trunk has also been associated with knee valgus motion. When the weight of the body
1

shifts over one leg the knee abduction load will increase over that leg and the hip adductor
needs to counteract that force to maintain an upright stance (Hewett, Torg et al. 2009).
The neuromuscular control in men and women seems to differ in several areas. Women
involved in jumping and pivoting sports showed a significant less voluntary isometric knee
stiffness against a rotational force compared with sport-matched men and women involved in
non-pivoting sports (Wojtys, Huston et al. 2003). According to Rozzi, Lephart et al. (1999)
female soccer and basketball players had a significant higher knee laxity and deficiency in
their ability to detect passive knee motion (extension). In another study made by Ahmad,
Clark et al. (2006) they measured knee laxity, quadriceps to hamstring strength ratio in
immature boys and girls, and mature boys and girls. They found that mature boys had
significant less knee laxity compared to the other groups and they found that the mature girls
group had significantly higher quadriceps to hamstring strength ratio compared with the other
groups.
Simultaneous hamstring and quadriceps contraction stabilizes the knee in the sagittal plane
against anterior translation but also in the frontal plane against knee abduction and valgus
(Besier, Lloyd et al. 2003). However, if the hamstring is weak or under-recruited, quadriceps
activation may be reduced in a co-contraction that supposed to protect the knee joint (Hewett,
Myer et al. 2005). Studies have also shown that women have a different contraction pattern in
the way they contract their hamstrings and quadriceps compared to men. For example, Myer,
Ford et al. (2005) measured and compared lateral and medial quadriceps activation in 20
active students. They found that women had a significant decreased lateral to medial
quadriceps activation compared to the male students. In another study (Rozzi, Lephart et al.
1999) where they measured hamstring activation during a landing task, they found that
women had a significant higher lateral to medial activation ratio compared to men.
The gluteus maximus and gluteus medius musculature act synergistically to stabilize the hip
and has an important role of controlling our knees and pelvis in daily activities and during
sport tasks (Gottschalk, Kourosh et al. 1989; Krause, Jacobs et al. 2009). Gluteus medius is
the main hip abductor, whereas the gluteus maximus primary function is hip extension and its
secondary function is hip external rotation (Mendiguchia, Ford et al. 2011). Jacobs and
Mattacola (2005) showed a significant relationship between eccentric hip abductor (gluteus
medius & gluteus maximus) strength and knee valgus in a single leg forward hop test in
females. Studies have shown that women use a different landing strategy when performing
2

jumping and landing tasks, landing in a more erect position and absorbing more energy to the
knee- and ankle joint (Decker, Torry et al. 2003). Zazulak, Ponce et al. (2005) showed that
women has a lower activation of gluteus maximus and a higher activation of rectus femoris
during drop landings compared to men. Women also tend to have less hip- and knee flexion in
landings which again, contributes to a stiffer and more abrupt landing (Lephart, Ferris et al.
2002; Decker, Torry et al. 2003). Valgus motion is well documented but few studies have
investigated the abduction angular velocity.
The faster the joint reaches the end position the less time the muscles has to absorb the impact
force during a landing (Lephart, Ferris et al. 2002). The joint velocity has been measured in
the frontal plane by Joseph, Rahl et al. (2011) during a drop jump landing. They measured and
compared timing of maximum hip adduction, knee valgus, ankle eversion in relation to
maximal knee flexion between highly competitive men and women. Women reached their
peak hip adduction, valgus and ankle eversion significantly faster than male athletes. They
also measured the abduction angular velocity of the valgus motion and showed that women
had almost twice as fast valgus abduction angular velocity (57.71deg/s) compared to men
(32.17deg/s) (Joseph, Rahl et al. 2011).
Intervention studies that have shown improvements in decreasing risk factor parameters and
increasing strength have mostly performed plyometric training and strength training. In a
study made by Nagano, Ida et al. (2011) eight female basketball athletes performed a jump-
balance training program for 5 weeks. The training sessions included different variations of
unilateral- and bilateral jumps and had a duration of twenty minutes and were performed three
times a week. They found a significant improvement in knee flexion and hamstrings
activation in a single leg landing task (Nagano, Ida et al. 2011). In another study that resulted
in significant improvements in strength and knee kinematics made by Lim, Lee et al. (2009)
they also had a duration of twenty minutes were the performed stretching, strength exercises
and plyometric exercises (Lim, Lee et al. 2009). However, studies that have shown
improvements in kinematics use programs consisting of several exercises, making them time
consuming. A training program that is time effective and injury preventing is important not
only for professional teams but also for amateur teams that have less sessions per week.
Therefore it is important to investigate the effectiveness in more specific exercises focusing in
hip abduction.
3

In our earlier study we validated a new training device called ProPrioPlate (PPP). PPP was
made to strengthening the stabilizing muscles that protects the knee joint in a more sport
specific movement than most exercises today. For example, many exercises that are
performed to strengthen the gluteus medius are performed with a fixed hip with movement
occurring in the hips. From a functional perspective the gluteus medius is divided into three
parts (Gottschalk, Kourosh et al. 1989). At 0 degrees of hip flexion the anterior part of the
gluteus medius accounts as the primary hip abductor and stabilizer. As the hip flexes the
intermediate part becomes the primary hip abductor and stabilizer. If there is no movement in
the hips during training of the gluteus, the muscle will not be trained properly.
The PPP is activating the knee stabilizers (all parts of gluteus, hamstrings- and quadriceps
muscles) during the whole range of motion in a squat. It also activates the gluteus medius
muscles 40 % more during squats compared with regular bodyweight squats (Andersson,
Herö et al. 2012)
The purpose of this study was to investigate if a 6 week long training period, 3 sessions/ week
5 minutes/session with the PPP could decrease the abduction angular velocity (°/sec) of the
knee joint in a drop jump (DJ) in women with poor knee stability
2. Methods
2.1. Subjects
One female soccer team and one female floor ball team were invited to participate in the
study, a total of 45 subjects. Exclusion criteria included any history of knee injury. Inclusion
criteria included poor knee stability in the DJ during the visual screening test.
A first visual screening test at the club was performed to identify subjects with poor knee
stability. We made a visual screening during a DJ of the 45 female athletes that volunteered to
participate. Subjects were told to just take a step out from a bench (height 31 cm), land with
both feet shoulder width at the same time and then jump as high as possible. The DJ has
demonstrated high within-session reliability with intraclass correlation coefficients of greater
than 0.93 (Ford, Myer et al. 2003). Poor knee stability was determined by the two test leaders
during the first visual screening, if both the test leaders considered poor knee stability in the
DJ the subject were asked to participate in the study. 20 of the 45 tested subjects were
thereafter included in the study (figure 3). The mean and standard deviation (SD) of the 20
4
athletes that were included in the intervention study were for age 19 (5) years, height 167 (4)
cm, and weight 63 (6) kg.
2.2. Study design
We used an experimental study design with no control group. Our subjects were tested with
3D motions analysis before and after the intervention period which lasted for 6 weeks.
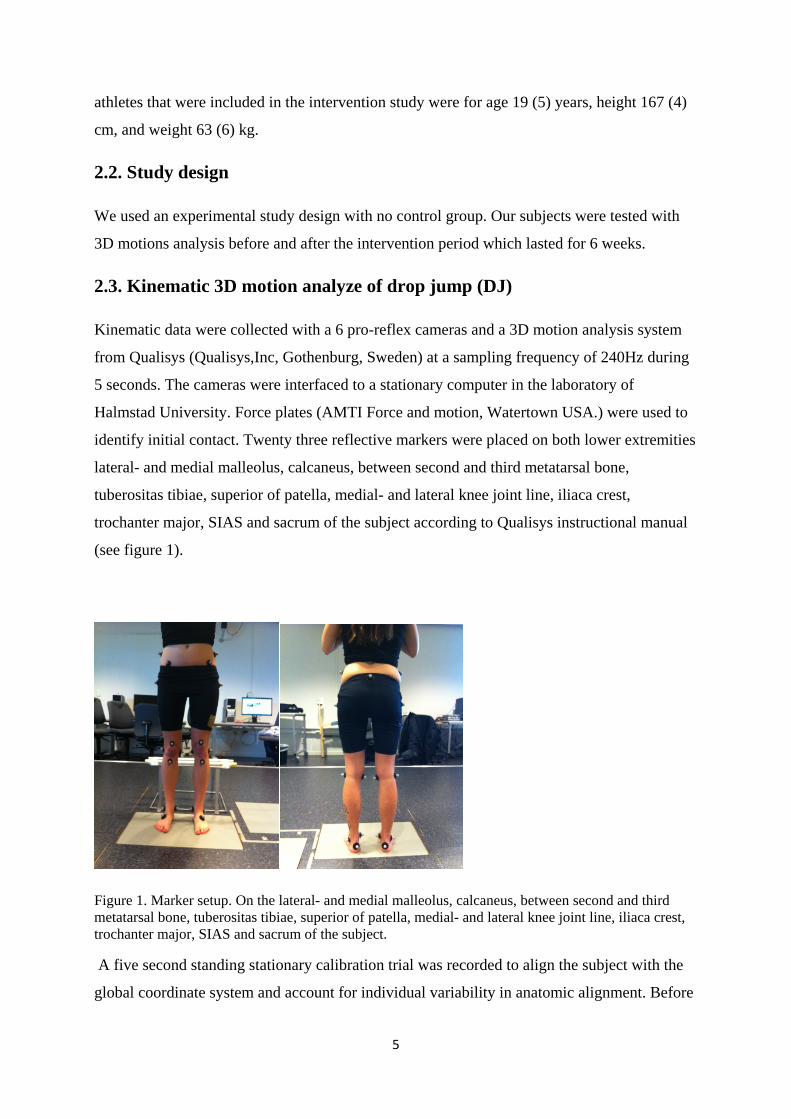
2.3. Kinematic 3D motion analyze of drop jump (DJ)
Kinematic data were collected with a 6 pro-reflex cameras and a 3D motion analysis system
from Qualisys (Qualisys,Inc, Gothenburg, Sweden) at a sampling frequency of 240Hz during
5 seconds. The cameras were interfaced to a stationary computer in the laboratory of
Halmstad University. Force plates (AMTI Force and motion, Watertown USA.) were used to
identify initial contact. Twenty three reflective markers were placed on both lower extremities
lateral- and medial malleolus, calcaneus, between second and third metatarsal bone,
tuberositas tibiae, superior of patella, medial- and lateral knee joint line, iliaca crest,
trochanter major, SIAS and sacrum of the subject according to Qualisys instructional manual
(see figure 1).
Figure 1. Marker setup. On the lateral- and medial malleolus, calcaneus, between second and third metatarsal bone, tuberositas tibiae, superior of patella, medial- and lateral knee joint line, iliaca crest, trochanter major, SIAS and sacrum of the subject.
A five second standing stationary calibration trial was recorded to align the subject with the
global coordinate system and account for individual variability in anatomic alignment. Before
5

the measurements the subjects got familiarized with the DJ by performing the task until they
felt comfortable with it. Subject was told to have a shoulder width stance, take a step out, land
with both feet at the same time and perform a jump as high as possible with both feet on the
force plate and with their arms above the markers on the iliaca crest. This testing procedure
has been used by other authors (Joseph, Tiberio et al. 2008; Joseph, Rahl et al. 2011) and the
reliability for kinematic data has been shown to be excellent (Chappell and Limpisvasti 2008).
Thereafter 5 successful trials of DJ from a height of 31 cm were recorded. Qualisys Track
manager and Visual 3d (Qualisys AB, Gothenburg) was used to analyze the motion data. In
trials that resulted in multiple trajectories for the same markers, the trajectories were joined
together and gap-filled, for gaps not exceeding 30 frames which is the standard option for
Qualisys track manager. The motion files that were captured during the tests were exported to
3.d files and then a pipeline were created to compute joint velocity and knee abduction angle.
The abduction angular velocity of the right knee joint from initial contact to peak abduction
was obtained. If the data from the right leg was disturbed the left leg was used. The mean
abduction angular velocity (°/sec) in each of the three first correct trials was obtained and the
mean value of these three trials was then calculated and used in the statistical analysis.
2.4. Training device
ProPrioPlate (PPP) is the name of the new device that has been used in this study. PPP consist
of 2 plates that are centered over each other. The top plate rotates internally over the bottom
plate when the athlete abducts the hip (figure 2 a-c), if the athlete performs the exercise
correct the gluteus muscles should be contracted during the whole squat. For further details
about the device see our earlier validation study (Andersson, Herö et al. 2012).
Figure 2. (a) Side view of PPP, Ø 0.32 m, height 0.07 m. (b) Starting position before exercise begins. (c) By pushing feet apart the top plate will rotate internally and the subject can start her squat.

2.5. Intervention period
During the training period of 6 weeks the subjects trained on the PPP in accordance to the
regular team session supervised by team coaches. The subjects were instructed to place both
feet on each device, pushing the feet apart and perform a squat while trying to keep their
weight on the heels. Training volume per session was designed to be 4 sets with 15
repetitions, 3 times a week. To induce muscle stiffness which leads to a higher muscle spindle
stretch sensitivity and proprioceptive feedback we used high repetitions with low rest between
sets (Swanik, Lephart et al. 1997). During the first session we instructed the athletes and
insured that every athlete performed the exercise correctly. Subjects were required to
participate in at least 80% of the training sessions. Two of the subjects did their training at
home because they were not able to participate in the group training sessions during that
period of time. A training diary was given to each team were the subjects could mark every
training session they finished.
2.6. Ethical and Social considerations
Written informed consent was collected from every subject or guardian if the athletes were
under 18. Participation was voluntary, anonymous and the subjects could leave the study at
any time. The exercises performed on PPP have a potential to improve knee stability and
decrease the number of injuries which may have a substantial impact on both the individual
health and on lowering the cost to society.
2.7. Statistical analyses
A value of < 0.05 in the Shapiro-Wilks test indicated that the test data were not normally
distributed why non parametric analysis has been performed. Descriptive data included
median and min-max values. The Wilcoxon signed ranks test was used to investigate if there
were any changes in results after the intervention. Significant level was set P <0.05. IBM
SPSS Statistics 19 was used to perform the statistical analyzes.
7
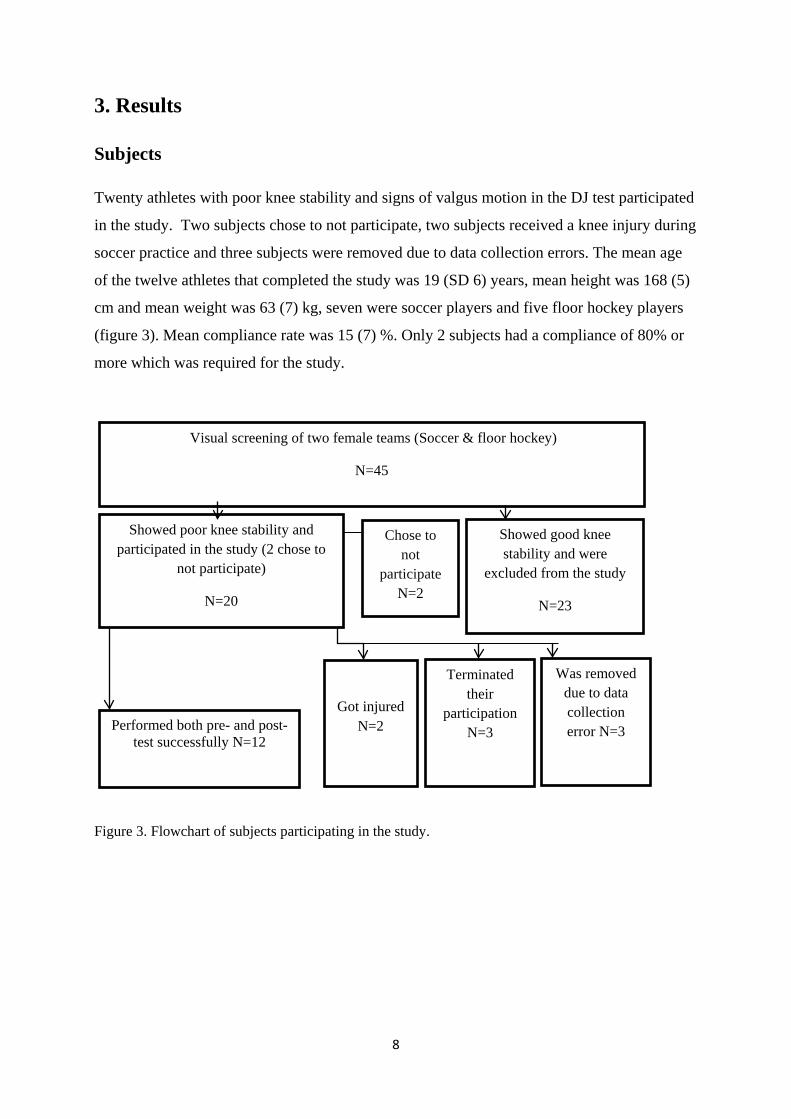
3. Results
Subjects
Twenty athletes with poor knee stability and signs of valgus motion in the DJ test participated
in the study. Two subjects chose to not participate, two subjects received a knee injury during
soccer practice and three subjects were removed due to data collection errors. The mean age
of the twelve athletes that completed the study was 19 (SD 6) years, mean height was 168 (5)
cm and mean weight was 63 (7) kg, seven were soccer players and five floor hockey players
(figure 3). Mean compliance rate was 15 (7) %. Only 2 subjects had a compliance of 80% or
more which was required for the study.
Figure 3. Flowchart of subjects participating in the study.
Visual screening of two female teams (Soccer & floor hockey)
N=45
Showed poor knee stability and participated in the study (2 chose to
not participate)
N=20
Performed both pre- and post-test successfully N=12
Showed good knee stability and were
excluded from the study
N=23
Got injured N=2
Terminated their
participation N=3
Was removed due to data collection error N=3
Chose to not
participate N=2
8

Abduction Angular velocity of the knee joint
Because the data was not normally distributed the Wilcoxon signed-ranked test was used to investigate if there were any differences in abduction angular velocity of the knee joint before and after the intervention. The median value of the pre-test was -34.34 (min: -70.65; max: -11.53) °/sec and the post-test was -34.22 (min: -51.97; max: -3.28) °/sec. The P value of the Wilcoxon signed rank test was 0.24 which indicate that there were no statistical significant differences between the two test occasions (Table 1).
Table 1. Median values (abduction is negative) of knee abduction angular velocity (°/sec) before and after the exercise intervention for both the total group and individually.
A lower knee abduction angular velocity (°/sec) indicates a better control of the knee during the eccentric phase of the landing. In this study 7 subjects exhibited a decreased knee abduction angular velocity after the exercise intervention, while 5 subjects exhibited an increase in abduction angular velocity, please see table 1 and figure 4.
°/sec, before intervention
°/sec, after intervention
P-value
All (N=12) median (min ;
max)
-34.34 (-70.65 ; -11.53)
-34.22 (-51.97 ; -3.28)
0.24
Individual data
Subject 1 -24.47 -42.71
Subject 2 -34.21 -51.97
Subject 3 -70.65 -33.78
Subject 4 -11.53 -16.15
Subject 5 -29.35 -29.05
Subject 6 -34.47 -47.26
Subject 7 -52.76 -43.15
Subject 8 -21.80 -3.28
Subject 9 -52.64 -34.67
Subject 10 -33.69 -37.08
Subject 11 -53.09 -29.93
Subject 12 -39.98 -16.35
9
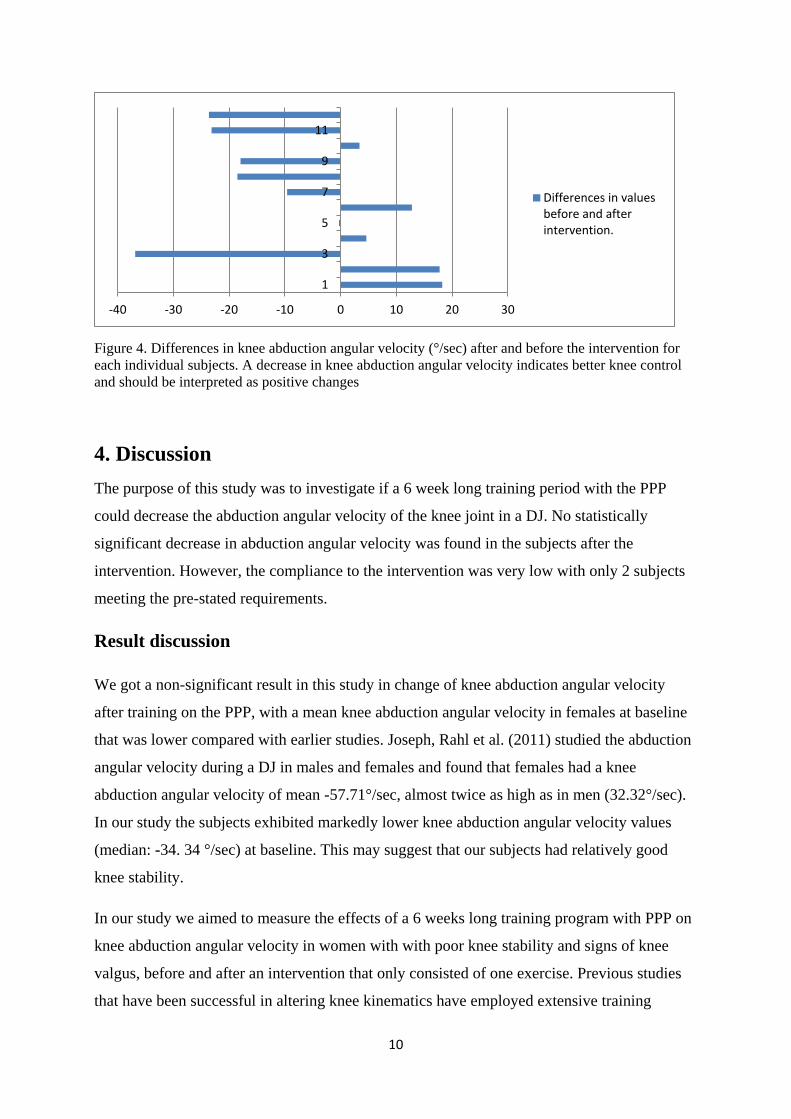
Figure 4. Differences in knee abduction angular velocity (°/sec) after and before the intervention for each individual subjects. A decrease in knee abduction angular velocity indicates better knee control and should be interpreted as positive changes
4. Discussion The purpose of this study was to investigate if a 6 week long training period with the PPP
could decrease the abduction angular velocity of the knee joint in a DJ. No statistically
significant decrease in abduction angular velocity was found in the subjects after the
intervention. However, the compliance to the intervention was very low with only 2 subjects
meeting the pre-stated requirements.
Result discussion
We got a non-significant result in this study in change of knee abduction angular velocity
after training on the PPP, with a mean knee abduction angular velocity in females at baseline
that was lower compared with earlier studies. Joseph, Rahl et al. (2011) studied the abduction
angular velocity during a DJ in males and females and found that females had a knee
abduction angular velocity of mean -57.71°/sec, almost twice as high as in men (32.32°/sec).
In our study the subjects exhibited markedly lower knee abduction angular velocity values
(median: -34. 34 °/sec) at baseline. This may suggest that our subjects had relatively good
knee stability.
In our study we aimed to measure the effects of a 6 weeks long training program with PPP on
knee abduction angular velocity in women with with poor knee stability and signs of knee
valgus, before and after an intervention that only consisted of one exercise. Previous studies
that have been successful in altering knee kinematics have employed extensive training
-40 -30 -20 -10 0 10 20 30
1
3
5
7
9
11
Differences in valuesbefore and afterintervention.
10

programs. Chappell and Limpisvasti (2008) used a program with several exercises focusing
on strength, stability, plyometric training and successfully altered knee kinematics in young
women. In contrast, Herman, Weinhold et al. (2008) did not have any success either in
improving hip and knee kinetics and kinematics during a stop-jump task with a 9 week band
resistance training program. This points to the complexity of the knee stability problem and
suggests that many factors are involved. It is therefore possible we would not have seen an
effect from our program even if our subjects had complied with the intervention.
Studies measuring knee abduction angular velocity is lacking but it is of great importance and
can add to the knowledge of knee stability. Lephart, Ferris et al. (2002) compared abduction
angular displacement and time to abduction angular displacement in hip flexion, hip
abduction, hip rotation, knee flexion, lower leg rotation between males and females during a
one legged landing and in a forward hop. He found that the females had significant less time
to maximum abduction angular displacement in lower leg internal rotation and knee flexion.
Lower leg rotation is a component of the valgus movement and the faster time to maximum
abduction angular displacement the lesser time the muscles has to absorb the force (Lephart,
Ferris et al. 2002). These results indicate that abduction angular displacement in relation to
velocity and abduction angular velocity are important variables when investigating knee
injuries or knee instability and that our chosen assessments were relevant. More research in
this area may be an important component to further evaluate severe and common knee
injuries, especially amongst women.
Method discussion
Two subjects in the present study got knee injuries two weeks into the intervention and were
excluded from the study which might indicate that the visual screening test was successful in
allocating the subjects with affected knee stability. The injuries did not occur during training
with PPP. It is possible that these two subjects could have gained the most benefit from the
intervention program which could have had an effect on the results. Myer, Ford et al. (2007)
performed a neuromuscular training program on a group classified as “high-risk” and a group
classified as “low-risk”. They found that the high-risk group decreased their knee abduction
moment while the low-risk group showed no significant improvements. In the discussion they
mentioned that an even higher intensity and volume was probably needed to see changes in
the “low risk” group. Similarly, the subjects with poor knee stability included in our study
could be considered falling into the “low-risk” group, and it is very likely that our volume and
11
intensity were too low to alter the abduction angular velocity of our subjects since so few of
the actually fulfilled their training regimen properly (only 2 out of 12 subjects). Future studies
should take this into consideration when selecting subjects and programming training.
There were some methodological errors that very likely could have an effect on these results.
Only two of our subjects did train sufficiently (80% of all sessions). These two subjects had
one pair of PPP at home and did the training there because they were not able to participate in
the regular team sessions and because of that no one was able to supervise their training. The
other subjects that were supposed to perform the exercise on the PPP at the team sessions had
a very low compliance of the exercise on the device for various reasons. One of the teams
finished their competition season during the training period and their team sessions went
down to 1 practice/ week.
Sluijs, Kok et al. (1993) investigated factors for compliance rate in physical therapy. They
found that three main factors related to noncompliance. Barriers that patients perceived, lack
of positive feedback from and the perceived helplessness. Unfortunately these factors were
not measured during our study but could have had an impact on the compliance rates. No staff
related to the study was present during trainings to supervise or give positive feedback to the
subjects.
New studies should focus on implementing training with the device in a more controlled
environment and including a control group. In addition, future studies should look at muscle
activation and cocontraction when comparing different exercises with PPP. Perhaps training
with the device should be incorporated in a more extensive training program and then
compared with a group that did the same training program except exercises on the device.
12

Conclusion
The current study investigated if a 6 week training program with the PPP would decrease the
abduction angular knee velocity during a DJ. No statistical significant changes were seen after
a 6 week intervention. But because of low compliance rates amongst our subjects no
conclusion regarding the effects of the device can be made. However, many lessons have been
learned regarding the study implementation which can come to use in future studies on the
device.
13

References
Ahmad, C. S., A. M. Clark, et al. (2006). "Effect of Gender and Maturity on Quadriceps-to-Hamstring Strength Ratio and Anterior Cruciate Ligament Laxity." The American Journal of Sports Medicine 34(3): 370-374.
Andersson, N., J. Herö, et al. (2012). "Increasing activation of the gluteus medius using a new training device." Journal of sport and health research 4(3): 311-320.
Besier, T., D. Lloyd, et al. (2003). "Muscle activation strategies at the knee during running and cutting maneuvers." Medicine & Science in Sports & Exercise 35(1): 119-127.
Chappell, J. D., D. C. Herman, et al. (2005). "Effect of Fatigue on Knee Kinetics and Kinematics in Stop-Jump Tasks." The American Journal of Sports Medicine 33(7): 1022-1029.
Chappell, J. D. and O. Limpisvasti (2008). "Effect of a Neuromuscular Training Program on the Kinetics and Kinematics of Jumping Tasks." The American Journal of Sports Medicine 36(6): 1081-1086.
Decker, M. J., M. R. Torry, et al. (2003). "Gender differences in lower extremity kinematics, kinetics and energy absorption during landing." Clinical Biomechanics 18(7): 662-669.
Ford, K. R., G. D. Myer, et al. (2003). Reliability of dynamic knee motion in female athletes. American society of biomechanics annual meeting. 34.
Ford, K. R., G. D. Myer, et al. (2005). "Gender Differences in the Kinematics of Unanticipated Cutting in Young Athletes." Medicine & Science in Sports & Exercise 37(1): 124-129.
Frobell, R. B., L. S. Lohmander, et al. (2007). "Acute rotational trauma to the knee: poor agreement between clinical assessment and magnetic resonance imaging findings." Scandinavian Journal of Medicine & Science in Sports 17(2): 109-114.
Gottschalk, F., S. Kourosh, et al. (1989). "The functional anatomy of tensor fasciae latae and gluteus medius and minimus." Journal of anatomy 166: 179-189.
Herman, C. D., S. P. Weinhold, et al. (2008). "The Effects of Strength Training on the Lower Extremity Biomechanics of Female Recreational Athletes During a Stop-Jump Task." American journal of sports medicine 36: 733-740.
Hewett, T. E., G. D. Myer, et al. (2006). "Anterior Cruciate Ligament Injuries in Female Athletes." The American Journal of Sports Medicine 34(2): 299-311.
Hewett, T. E., G. D. Myer, et al. (2005). "Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes." The American Journal of Sports Medicine 33(4): 492-501.
Hewett, T. E., J. S. Torg, et al. (2009). "Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism." British Journal of Sports Medicine 43(6): 417-422.
Huston, L. J. and E. M. Wojtys (1996). "Neuromuscular Performance Characteristics in Elite Female Athletes." The American Journal of Sports Medicine 24(4): 427-436.
Jacobs, C. and C. Mattacola (2005). "sex differences in exxentric hip-abductors strength and kne-joint kinematics when landing from a jump." journal of sport rehabil. 14: 346-355.
Joseph, M., D. Tiberio, et al. (2008). "Knee Valgus During Drop Jumps in National Collegiate Athletic Association Division I Female Athletes." The American Journal of Sports Medicine 36(2): 285-289.
Joseph, M. F., M. Rahl, et al. (2011). "Timing of Lower Extremity Frontal Plane Motion Differs Between Female and Male Athletes During a Landing Task." The American Journal of Sports Medicine 39(7): 1517-1521.
Krause, D. A., R. S. Jacobs, et al. (2009). "Electromyographic Analysis of the Glutues Medius in Five Weight Bearing Exercises." Journal of Strength & Conditioning Research 23: 2689-2694.
Lephart, S. M., C. M. Ferris, et al. (2002). "Gender Differences in Strength and Lower Extremity Kinematics During Landing." Clinical Orthopaedics and Related Research 401.

Lewis, T. (2000). "Anterior Cruciate Ligament Injury in Female Athletes: Why are women so vulnerable?: Literature review." Physiotherapy 86(9): 464-472.
Lim, B.-O., Y. S. Lee, et al. (2009). "Effects of Sports Injury Prevention Training on the Biomechanical Risk Factors of Anterior Cruciate Ligament Injury in High School Female Basketball Players." The American Journal of Sports Medicine 37(9): 1728-1734.
Lohmander, L. S., P. M. Englund, et al. (2007). "The Long-term Consequence of Anterior Cruciate Ligament and Meniscus Injuries." The American Journal of Sports Medicine 35(10): 1756-1769.
Loudon, J. K., W. Jenkins, et al. (1996). "The relationship between static posture and ACL injury in female athletes." The Journal of orthopaedic and sports physical therapy 24(2): 91-97.
Mclean, S. G., S. W. Lipfert, et al. (2004). "Effect of Gender and Defensive Opponent on the Biomechanics of Sidestep Cutting." Medicine & Science in Sports & Exercise 36(6): 1008-1016.
Mendiguchia, J., K. R. Ford, et al. (2011). "Sex Differences in Proximal Control of the Knee Joint." Sports Medicine 41(7): 541-557.
Moeller, J. and M. Lamb (1997). "Anterior cruciate ligament injuries in female athletes: Why are woman more susceptible?" Physican and sportsmedicine 25: 31-51.
Myer, G., K. Ford, et al. (2007). "Differential neuromuscular training effects onACL injury risk factors in"high-risk" versus "low-risk" athletes." BMC Musculoskeletal Disorders 8(1): 39.
Myer, G. D., K. R. Ford, et al. (2005). "The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position." Journal of Electromyography and Kinesiology 15(2): 181-189.
Nagano, Y., H. Ida, et al. (2011). "Effects of jump and balance training on knee kinematics and electromyography of female basketball athletes during a single limb drop landing: pre-post intervention study." Sports medicine, arthroscopy, rehabilitation, therapy & technology 3(14): 1-8.
Quatman, C. E. and T. E. Hewett (2009). "The anterior cruciate ligament injury controversy: is “valgus collapse” a sex-specific mechanism?" British Journal of Sports Medicine 43(5): 328-335.
Roos, H., M. Ornell, et al. (1995). "Soccer after anterior cruciate ligament injury— an incompatible combination? A national survey of incidence and risk factors and a 7-year follow-up of 310 players." Acta Orthopaedica 66(2): 107-112.
Rozzi, S. L., S. M. Lephart, et al. (1999). "Knee Joint Laxity and Neuromuscular Characteristics of Male and Female Soccer and Basketball Players." The American Journal of Sports Medicine 27(3): 312-319.
Schoenfeld, B. J. (2010). "Squatting Kinematics and Kinetics and Their Application to Exercise Performance." The Journal of Strength & Conditioning Research 24(12): 3497-3506.
Shimokochi, Y. and S. J. Shultz (2008). "Mechanisms of Noncontact Anterior Cruciate Ligament Injury." Journal of Athletic Training 43(4): 396-408.
Sluijs, E. M., G. J. Kok, et al. (1993). "Correlates of Exercise Compliance in Physical Therapy." Physical Therapy 73(11): 771-782.
Swanik, B. C., S. M. Lephart, et al. (1997). "Reestablishing proprioception and neuromuscular control in the ACL-injured athlete." Journal of Sport Rehabilitation 6: 182-206.
Wojtys, E. M., L. J. Huston, et al. (2003). "Gender differences in muscular protection of the knee in torsion in sized-matched athletes." Journal of Bone & Joint Surgery, American Volume 85(5): 782.
von Porat, A., E. M. Roos, et al. (2004). "High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: a study of radiographic and patient relevant outcomes." Annals of the Rheumatic Diseases 63(3): 269-273.
Zazulak, B. T., P. L. Ponce, et al. (2005). "Gender comparison of hip muscle activity during single-leg landing." The Journal of orthopaedic and sports physical therapy 35(5): 292-299.

HALMSTAD UNIVERSITY • PO Box 823 • SE-301 18 Halmstad, Sweden • www.hh.se