Embed Size (px)
Citation preview

Research ArticleThe Effects of Two Different Ankle-Foot Orthoses on Gait ofPatients with Acute Hemiparetic Cerebrovascular Accident
Noel Rao1 Jason Wening2 Daniel Hasso2 Gnanapradeep Gnanapragasam1
Priyan Perera1 Padma Srigiriraju1 and Alexander S Aruin13
1 Marianjoy Rehabilitation Hospital 26W171 Roosevelt Road Wheaton IL 60187 USA2 Scheck amp Siress 1551 Bond Street Naperville IL 60563 USA3Department of Physical Therapy (MC 898) University of Illinois at Chicago 1919 West Taylor Street Chicago IL 60612 USA
Correspondence should be addressed to Alexander S Aruin aaruinuicedu
Received 5 March 2014 Accepted 27 August 2014 Published 9 September 2014
Academic Editor Jeffrey Jutai
Copyright copy 2014 Noel Rao et alThis is an open access article distributed under the Creative CommonsAttribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Objective To compare the effects of two types of ankle-foot orthoses on gait of patients with cerebrovascular accident (CVA) andto evaluate their preference in using each AFO typeDesign Thirty individuals with acute hemiparetic CVA were tested without anAFO with an off-the-shelf carbon AFO (C-AFO) and with a custom plastic AFO (P-AFO) in random order at the time of initialorthotic fitting Gait velocity cadence stride length and step length were collected using an electronic walkway and the subjectswere surveyed about their perceptions of each device Results Subjects walked significantly faster with a higher cadence longerstride and step lengths when using either the P-AFO or the C-AFO as compared to no AFO (119875 lt 005) No significant differencewas observed between gait parameters of the two AFOs However the subjects demonstrated a statistically significant preferenceof using P-AFO in relation to their balance confidence and sense of safety during ambulation (119875 lt 005) Moreover if they hada choice 5087 plusmn 147 of the participants preferred the P-AFO and 2356 plusmn 970 preferred the C-AFO Conclusions AFO usesignificantly improved gait in patients with acute CVAThemajority of users preferred the P-AFO over the Cf-AFO especially whenasked about balance and sense of safety
1 Introduction
Cerebrovascular accident (CVA) is the leading cause ofserious long-term disability among adults Each year in theUnited States approximately 795000 people sustain a new orrecurrent CVA [1] and nearly half survive with some level ofneurological impairment and disability [2] CVA often resultsin dysfunction of one side of the body (hemiparesis) leadingto gait impairment and increased probability for falls [3 4]
Restoration of ambulation and ability to move around inthe community is considered a high priority for individualsafterCVA [5] An ankle-foot orthosis is commonly prescribedto assist a patient with hemiparetic CVA to return to ambu-lation AFOs can prevent foot drop control the ankle in thecoronal and sagittal planes during standing and walking andimprove the stability of the knee joint during ambulation [6]Several studies have concluded that plastic AFOs (P-AFOs)
have a positive influence on the walking velocity and othergait parameters of individuals with hemiparetic CVA [7ndash11]Recently carbonAFOs (C-AFOs) have been introduced to themarketplace by several manufacturers The manufacturersof the C-AFOs claim that these devices are appropriate forhemiparetic patients who meet criteria that include minimalequinus contracture of the ankle minimal coronal planedeformity of the ankle minimal fluctuating edema and noor low spasticity However the literature on the use of carbonAFOs to improve ambulation of individuals with CVA isinsufficient Moreover to the best of our knowledge noinformation exists on the patientsrsquo preference in using carbonAFOs
There is also a body of literature on the importanceof using a custom-made plastic AFO [12 13] Thus it wasreported that when a patient with posterior tibial tendondysfunction was provided with an off-the-shelf ankle-foot
Hindawi Publishing CorporationRehabilitation Research and PracticeVolume 2014 Article ID 301469 7 pageshttpdxdoiorg1011552014301469
2 Rehabilitation Research and Practice
orthosis (AFO) a custom solidAFO and a customarticulatedAFO she selected a custom articulated AFO [14] Howeverit is not known whether the patients with CVA would preferusing the prefabricated carbonAFOswhen they have a choiceto select the type of AFO Given that the cost of orthosesvaries considerably and that choosing an effective orthosisthat is affordable to the patient is largely a trial-and-errorprocess [14] it is important to obtain information on thepatientsrsquo preference when prescribing an AFO
It was reported that 353 of the study subjects whoused an AFO indicated that they walked more confidently[15] and that patients reported a 70 increase in self-confidence [13] while using an AFO These reports suggesta feeling of confidence may be more important to personswith hemiparesis than speed and distance however littleinformation exists on the subjective preference in selectingthe type of AFO by individuals with stroke
While the literature provides important information onthe beneficial effect of the AFOs there is a need for moredata describing the impact of AFOs on gait of subjects in theacute phase of rehabilitation after CVAMoreover there is notenough data on the use of the prefabricated carbon AFOs ingait of individuals with acute stroke Thus the aims of thestudy were (1) to investigate the effect of walking using theprefabricated carbon AFO in comparison with the custompolymerAFO and noAFOand (2) to obtain data on the usersrsquopreference in using either the prefabricated carbon AFO orthe custom plastic AFO
We hypothesized that individuals with acute CVA willimprove their gait while provided with an AFO and thatthe improvement will be similar whether they use the pre-fabricated carbon AFO or the custom plastic AFO We alsohypothesized that when the subjects have a choice they willprefer using the custom-made plastic AFO
2 Methods
21 Subjects Subjects in the acute phase of rehabilitation afterhemiparetic CVA were referred by a physician during theirvisit to the orthotic clinic of a free-standing rehabilitationhospital The inclusion criteria were as follows CVA lessthan 12 weeks after onset Ashworth scale score of lessthan 2 ability to walk 10m without an AFO but with anappropriate assistive device (cane or walker) a need fora custom polymer AFO for ambulation (based on evalua-tion by the clinic team) and ability to follow instructionsThe exclusion criteria were as follows histories of othersignificant neurologic or orthopedic disorders significantcoronal plane deformity or plantar flexion contracture andminimal fluctuating edema All subjects signed an informedconsent approved by the Marianjoy Rehabilitation HospitalInstitutional Review Board
Thirty individuals who satisfied inclusionexclusion cri-teria were selected to participate in the study There were15 males and 15 females with an average age of 604 plusmn 113years 16 of the subjects presented with right and 14 with lefthemiparesis The study participants received a full clinicalevaluation and assessment Based on this assessment the
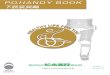
clinic team determined the type of a plastic AFO (flexiblesemirigid or rigid) that was most appropriate for eachsubject Subjects were molded for the appropriate AFO [16]and measured for an Ossur AFO dynamic carbon off-the-shelf AFO Thus based on clinical evaluation a subjectprescribed for example with a semirigid AFO was providedwith a semirigid plastic AFO or a semirigid carbon off-the-shelf AFO Individuals who required a different type ofAFO such as a metal AFO were excluded from the studyPlastic AFOs were custom modified and fabricated from31610158401015840 polypropylene and included a proximal calf strap anddistal ankle wrap around strap During the course of the studysubjects were provided with minimal information about thedesign and construction of the different AFOs Instead theAFOswere described as AFOA andAFOB for the subjects toprevent their impression of the device from being influencedby words such as ldquocustomrdquo or ldquocarbonrdquo (Figure 1) Subjectswere tested at 21 plusmn 8 days after CVA While all of the subjectswere actively receiving physical and occupational therapyas prescribed by the treating physician none of them hadexperience with anAFOprior to the day of fitting and testingSubjects received clinically appropriate AFO three subjectsreceived a flexibleAFO twenty received a semirigidAFO andseven subjects were provided with rigid AFOs
22 Experimental Setup and Procedure During the tests thesubjectswere randomly providedwith an off-the-shelf carbonAFO (C-AFO) and a custom plastic AFO (P-AFO) Testingincluded assessment of gait while walking using differentAFOs and walking with no AFO (while each subject used thesame own shoes during all the tests) and participation in asurvey about the subjectrsquos perceptions of each AFO
Temporal and spatial gait parameters were collectedusing a GAITRite electronic walkway (CIR Systems IncHavertown PA) This device has been validated to study gaitof individuals with stroke [17] The 119871-test was used to furtherassess the subjectsrsquo functional walking ability The 119871-test isa variant of the Timed Up and Go (TUG) test that usesan L shaped path instead of a straight line path [18] Twowalks were performed using the GAITRite and the 119871-test foreach condition no AFO C-AFO and P-AFO Prior to thetests the subjects were allowed for a brief adaptation withthe AFOs The order of the test conditions was randomizedacross the subjects Subjects used an appropriate assistivedevice such as a cane or walker as needed each subjectused the same assistive device during all the tests involvingambulation Subjects were allowed close supervision by aphysical therapist but no direct contact A minimum offive-minute rest between test conditions was provided tominimize the effect of fatigue
All the study participants completed the Subject Percep-tion of Functional Benefit Survey about their impression ofthe device that was just used (with assigned values of 0 beingthe most positive response and 4 the most negative) Thissurvey was conducted after the use of each AFO type Inaddition at the end of the study subjects completed theSubject AFO Preference Survey to determine if subjects hada preference for the polymer AFO carbon fiber AFO bothAFOs or neither AFO (with assigned values of 0 being
Rehabilitation Research and Practice 3
(a) (b)
Figure 1 Off-the-shelf carbon AFO (a) and custom plastic AFO (b) used in the study
the most positive response and 3 the most negative) Thesesurveys are slightly modified versions of the survey describedin the literature [18]
23 Data Processing and Analysis Walking data was pro-cessed within the GAITRite software and velocity cadenceand stride and step length were obtained as outcome mea-sures All the datawere subjected to Shapiro-Wilk test for nor-mality One-way repeated measures ANOVA was performedwith factor AFO (3 levels no AFO C-AFO and P-AFO)separately for velocity cadence and stride length Split-plotANOVA was performed with factors AFO (3 levels no AFOC-AFO and P-AFO) and side (involved and uninvolved) toanalyze the differences in step length Pairwise comparisonswere used for further analyses of significant effects Mann-Whitney test comparing survey responses for the polymerAFO and the carbonAFOwas performed to test for statisticaldifference in subject perceptions of the functional benefit ofthe two different devices For all tests statistical significancewas set at119875 lt 005 Statistical analysis was performed in SPSS17 for Windows 7 (SPSS Inc Chicago USA)
3 Results
31 Gait Velocity With no AFO the patientsrsquo gait velocitywas 3050 plusmn 1358 cmsec When they were provided with theoff-the-shelf carbon AFO (C-AFO) gait velocity increasedto 3638 plusmn 1606 cmsec When a custom plastic AFO wasused their gait velocity increased further reaching 3921 plusmn1809 cmsec The difference in gait velocity was statisticallysignificant (119865
258= 2086 119875 lt 00001) Further analysis
revealed statistically significant difference between no AFOcondition andC-AFOandP-AFO (119875 = 0001 and119875 lt 00001resp) While the subjects were able to walk faster while being
provided with P-AFO as compared to C-AFO the differencewas not statistically significant (119875 = 011) (Figure 2)
32 Cadence While walking without AFO the subjectsrsquo ca-dence was 5493 plusmn 1395 stepsmin Cadence increased whileusing the AFOs Thus it reached 6020 plusmn 1472 and 6276 plusmn1581 steps per minute when the subjects were providedwith C-AFO and P-AFO respectivelyThe difference betweenconditions was statistically significant (119865
258= 2190 119875 lt
00001) Pairwise comparison revealed that no AFO condi-tion was statistically significant compared to C-AFO and P-AFO conditions (119875 = 0001 119875 lt 00001 resp) Howeverthe difference betweenC-AFO and P-AFOwas not significant(119875 = 0099) (Figure 2)
33 Stride Length Patients walking without AFOs showedstride length of 6498 plusmn 1686 cm When they were providedwith the off-the-shelf carbon AFO (C-AFO) stride lengthincreased to 7035 plusmn 1883 cm When a custom polymer AFOwas used the stride length increased further reaching 7235plusmn2011 cm The difference in stride length was statisticallysignificant (119865
258= 1023 119875 lt 00001) Further analysis
revealed statistically significant difference between no AFOcondition and C-AFO and P-AFO (119875 = 0006 and 119875 lt 001resp) The difference in stride length between walking whilebeing provided with P-AFO and C-AFO was not statisticallysignificant (119875 = 079)
34 Step Length Step length in conditions with no AFOwas 3699 plusmn 865 cm and 2763 plusmn 1401 cm for the involvedand uninvolved lower extremities respectivelyWhen the off-the-shelf carbon AFO (C-AFO) was provided step lengthincreased to 3966 plusmn 997 cm and 3100 plusmn 1166 cm on theinvolved and uninvolved side respectively Using the customP-AFO resulted in the increase of the step length on the
4 Rehabilitation Research and Practice
No AFOCarbon AFOPolymer AFO
No AFOCarbon AFOPolymer AFO
0
25
50
75
100
Cade
nce
lowast
lowastlowast
lowast
0
20
40
60
80Ve
loci
ty (c
ms
)
Figure 2 Gait velocity and cadence measured while walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
0
30
60
90
120
0
20
40
60
80
InvolvedUninvolved
No AFO Polymer AFOCarbon AFO
Strid
e len
gth
(cm
)
Step
leng
th (c
m)
lowast
lowast
lowast
lowast
lowast
lowast
No AFOCarbon AFOPolymer AFO
Figure 3 Stride length and step length recorded during walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
involved side to 4021 plusmn 969 and on the uninvolved side to3192 plusmn 1409 The difference in step length while providedwith AFOs was statistically significant (119865
2116= 1297 119875 lt
00001) The interaction between the AFOs and the involvedor uninvolved side was however not statistically significant(1198652116
= 024 119875 = 079) Further pairwise comparison ofthe use of AFOs revealed statistically significant differencebetween no AFO condition and C-AFO and P-AFO (119875 =0001 and 119875 lt 00001 resp) The difference in step length
between walking while being provided with P-AFO and C-AFO was not statistically significant (119875 = 099) (Figure 3)
35 119871-Test While walking without AFO the time needed tocross 10m distance by the subjects was 145 plusmn 071min Thistime decreased to 125 plusmn 079min and to 133 plusmn 066minwhen the subjects were provided with C-AFO and P-AFOrespectively (119871-test data was collected for 26 subjects) Thedifference between conditions however was not statistically
Rehabilitation Research and Practice 5
Table 1 Subjects perception of Functional Benefit Survey
With the AFO I just used Response Significance(1) Lifting my toes is Much easier A little easier No different A little harder Much harder 119875 = 0053(2) Swinging my leg forward is Much easier A little easier No different A little harder Much harder P = 0023(3) Taking weight through my foot is Much easier A little easier No different A little harder Much harder 119875 = 0105(4) My walking speed Much faster A little faster Not changed A little slower Much slower 119875 = 0051(5) My balance is Much better A little better No different A little worse Much worse P = 0006(6) My confidence is Much higher A little higher Not changed A little less Much less P = 0014(7) My sense of safety is Much higher A little higher Not changed A little less Much less P = 0005(8) Walking is Much easier A little easier No different A little harder Much harder P = 0009
Table 2 Subjects perceptions regarding the AFO type119873 = 29
Plastic AFO Carbon AFO Both None(1) Lifting my toes is easier with 8 (27) 5 (17) 14 (48) 1 (3)(2) Swinging my leg forward is easier with 17 (586) 8 (27) 4 (138) 0 (0)(3) Taking weight through my foot is easier with 16 (55) 8 (27) 5 (17) 0 (0)(4) I walk faster with 18 (62) 5 (17) 6 (21) 0 (0)(5) My balance is better with 18 (62) 5 (17) 6 (21) 0 (0)(6) My sense of safety is higher with 17 (586) 2 (7) 10 (34) 0 (0)(7) I like the fit and comfort of 15 (52) 11 (38) 2 (7) 1 (3)(8) I like the appearance of 17 (586) 9 (31) 3 (10) 0 (0)(9) I would rather use to assist my walking 7 (24) 9 (31) 6 (21) 7 (24)
significant (119865252
= 635 119875 = 014) Pairwise comparisonrevealed that no AFO condition was statistically significantcompared to C-AFO (119875 = 0004) At the same time thedifference between no AFO and P-AFO and between C-AFOand P-AFO was not statistically significant (119875 = 01417119875 = 046 resp)
36 Usersrsquo Perceptions regarding the AFO Type The analysisof the outcome of the Perception of Functional BenefitSurvey about the device that was just used revealed thatin general the study participants preferred P-AFO whencompared to the C-AFO (data for 29 subjects)Thus the usersdemonstrated statistically significant preference of using P-AFO while answering question 2 (119880 = 2805 119875 = 0023)question 5 (119880 = 252 119875 = 0006) question 6 (119880 = 271 119875 =0014) question 7 (119880 = 250 119875 = 0005) and question 8(119880 = 2625 119875 = 0009) Moreover the differences betweenthe two types of AFO were just under the level of statisticalsignificance for question 1 (119880 = 301 119875 = 0053) and question4 (119880 = 3015 119875 = 0051) (Table 1)
The analysis of the outcome of the Subject AFO Prefer-ence Survey revealed that the study participants preferredthe P-AFO to the C-AFO (Table 2) This was especially truewhen they were asked about balance and sense of safetyduring ambulation On average 5087 plusmn 147 of the studyparticipants preferred P-AFO and 2356 plusmn 970 of thesubjects preferred C-AFO It is also important to mentionthat 181 plusmn 83 preferred using both types of AFOs and only
31plusmn790of the study participants preferred not using eithertype of AFO
4 Discussion
It is documented in the prior literature that individuals afterCVA walk slower than healthy individuals [19] It was alsoreported that the ability of individualswith stroke to ambulateis improved as a result of wearing an ankle-foot orthosis [20]Moreover there is a plethora of evidence on the beneficialeffect of AFOs in improving of functional mobility andquality of gait as well as decreasing the likelihood of falls inindividuals suffering from a CVA [21 22] Thus individualswith CVA provided with an AFO improved gait parameterssuch as cadence stride length and gait velocity [18 23 24]Moreover improvement in gait velocity that is believed toreflect progress in mobility is often used as a measure ofrecovery after a CVA [20 25 26] and is considered animportant goal of rehabilitation
At the same time the literature on the use of differenttypes of AFOs (especially recently introduced carbon AFOs)to improve ambulation of individuals with CVA is limited Assuch the goals of the study were to investigate the effect ofwalking using the prefabricated carbon AFO in comparisonwith the custompolymer AFO and noAFO and to investigatethe usersrsquo preference in using either the prefabricated carbonAFO or the custom plastic AFO
The results of the current study demonstrated that indi-viduals with acute CVA increased their gait velocity when
6 Rehabilitation Research and Practice
using either C-AFO or P-AFO and as a result the gapbetween ldquonormalrdquo and ldquohemipareticrdquo gait velocity decreasedThese results are in line with the literature reporting a positiveeffect of AFOs on gait velocity of individuals with hemiparesis[9 19 27] Similarly improvements in cadence were associ-ated with the use of an AFO without an AFO patients walkedwith lower cadence as compared to healthy individuals Asimilar positive effect of AFOs on cadence of individuals withhemiparesis was described in the literature [27 28] Sincecadence is the number of steps taken in a certain time theobserved increase in the velocity of gait could be due tochanges in the number of steps per minute Nevertheless theimpact of AFOs on cadence remains inconclusive as somestudies report an improvement in this variable with the AFOuse and others report no significant improvement [22] Thusthere is a need for more studies focused on the investigationof the role of different types of AFOs on gait velocity andcadence An increase in the average stride and step lengthwith either type of AFO was evident in the current study andhas been also reported in the past literature [27 28]
While in general there is a consensus in the literaturethat gait velocity is a powerful indicator of function andprognosis after CVA [26] there is an opinion that gait velocityitself may not be wholly representative of functional mobil-ity and meaningful improvement in performance [29] Toaddress this possible concern we added the 119871-test assessment(that includes rising from a chair two 90-degree turns inopposite directions a 180-degree turn and returning to aseated position) as the task that is indicative of the typesof movements that are required in household ambulationThe outcome of the 119871-test revealed that patients while usingAFOs of either type showed better performance comparedto walking with no AFO Moreover clinically the patientsshowed improvement as the time needed for the completionof the test was shorter when they were provided with eithertype of AFO
The study participants were positive about the use ofAFOs as the majority found it comfortable and felt itimproved their walking particularly the functional aspectssuch as safety and confidence This finding is in line withthe literature reporting that 96 of users felt they walkedbetter with the AFO and found it comfortable [18] Moreoverthe majority of the subjects gave a preference to the custom-made plastic AFOs the subjects perception was about 2 1 infavor of the custom-made plastic AFOThis could be becauseeach plastic AFO was specifically molded and fitted for eachsubject Nevertheless further study is needed to examine thelonger-term effects and the cost-effectiveness of prescribing acustom-made or off-the-shelf AFO for people with CVA
5 Conclusion
Both types of AFO significantly improved gait velocitycadence step length and stride length in patients with acuteCVAThe majority of users preferred the custom-made plas-tic AFO over the prefabricated carbon AFO This outcomeshould be taken into consideration while prescribing AFOsFurther study is needed to examine the longer-term effects
and the cost-effectiveness of prescribing different types ofAFO for people with CVA
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] V L Roger A S Go D M Lloyd-Jones et al ldquoHeart diseaseand stroke statisticsmdash2011 update a report from the AmericanHeart Associationrdquo Circulation vol 123 no 4 pp e18ndashe2092011
[2] M Kelly-Hayes J T Robertson J P Broderick et al ldquoTheAmerican heart association stroke outcome classificationrdquoStroke vol 29 no 6 pp 1274ndash1280 1998
[3] C Detrembleur F Dierick G Stoquart F Chantraine andT Lejeune ldquoEnergy cost mechanical work and efficiency ofhemiparetic walkingrdquo Gait amp Posture vol 18 no 2 pp 47ndash552003
[4] N Wada M Sohmiya T Shimizu K Okamoto and K Shi-rakura ldquoClinical analysis of risk factors for falls in home-livingstroke patients using functional evaluation toolsrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1601ndash1605 2007
[5] S E Lord K McPherson H K McNaughton L Rochesterand M Weatherall ldquoCommunity ambulation after stroke howimportant and obtainable is it and what measures appearpredictiverdquo Archives of Physical Medicine and Rehabilitationvol 85 no 2 pp 234ndash239 2004
[6] J F Lehmann S M Condon R Price and B J deLateurldquoGait abnormalities in hemiplegia their correction by ankle-foot orthosesrdquo Archives of Physical Medicine and Rehabilitationvol 68 no 11 pp 763ndash771 1987
[7] H Beckerman J Becher G J Lankhorst and A L M VerbeekldquoWalking ability of stroke patients efficacy of tibial nerveblocking and a polypropylene ankle-foot orthosisrdquo Archives ofPhysical Medicine and Rehabilitation vol 77 no 11 pp 1144ndash1151 1996
[8] D C M de Wit J H Buurke J M M Nijlant M J IJzermanand H J Hermens ldquoThe effect of an ankle-foot orthosison walking ability in chronic stroke patients a randomizedcontrolled trialrdquo Clinical Rehabilitation vol 18 no 5 pp 550ndash557 2004
[9] M Franceschini M Massucci L Ferrari M Agosti and CParoli ldquoEffects of an ankle-foot orthosis on spatiotemporalparameters and energy cost of hemiparetic gaitrdquo Clinical Reha-bilitation vol 17 no 4 pp 368ndash372 2003
[10] N Rao G Chaudhuri D Hasso et al ldquoGait assessment duringthe initial fitting of an ankle foot orthosis in individuals withstrokerdquo Disability and Rehabilitation Assistive Technology vol3 no 4 pp 201ndash207 2008
[11] S Roehrig andDA Yates ldquoCase report effects of a neworthosisand physical therapy on gait in a subject with longstandinghemiplegiardquo Journal of Geriatric Physical Therapy vol 31 no1 pp 38ndash46 2008
[12] H B Kitaoka X M Crevoisier K Harbst D Hansen BKotajarvi and K Kaufman ldquoThe effect of custom-made bracesfor the ankle and hindfoot on ankle and foot kinematics and
Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005

2 Rehabilitation Research and Practice
orthosis (AFO) a custom solidAFO and a customarticulatedAFO she selected a custom articulated AFO [14] Howeverit is not known whether the patients with CVA would preferusing the prefabricated carbonAFOswhen they have a choiceto select the type of AFO Given that the cost of orthosesvaries considerably and that choosing an effective orthosisthat is affordable to the patient is largely a trial-and-errorprocess [14] it is important to obtain information on thepatientsrsquo preference when prescribing an AFO
It was reported that 353 of the study subjects whoused an AFO indicated that they walked more confidently[15] and that patients reported a 70 increase in self-confidence [13] while using an AFO These reports suggesta feeling of confidence may be more important to personswith hemiparesis than speed and distance however littleinformation exists on the subjective preference in selectingthe type of AFO by individuals with stroke
While the literature provides important information onthe beneficial effect of the AFOs there is a need for moredata describing the impact of AFOs on gait of subjects in theacute phase of rehabilitation after CVAMoreover there is notenough data on the use of the prefabricated carbon AFOs ingait of individuals with acute stroke Thus the aims of thestudy were (1) to investigate the effect of walking using theprefabricated carbon AFO in comparison with the custompolymerAFO and noAFOand (2) to obtain data on the usersrsquopreference in using either the prefabricated carbon AFO orthe custom plastic AFO
We hypothesized that individuals with acute CVA willimprove their gait while provided with an AFO and thatthe improvement will be similar whether they use the pre-fabricated carbon AFO or the custom plastic AFO We alsohypothesized that when the subjects have a choice they willprefer using the custom-made plastic AFO
2 Methods
21 Subjects Subjects in the acute phase of rehabilitation afterhemiparetic CVA were referred by a physician during theirvisit to the orthotic clinic of a free-standing rehabilitationhospital The inclusion criteria were as follows CVA lessthan 12 weeks after onset Ashworth scale score of lessthan 2 ability to walk 10m without an AFO but with anappropriate assistive device (cane or walker) a need fora custom polymer AFO for ambulation (based on evalua-tion by the clinic team) and ability to follow instructionsThe exclusion criteria were as follows histories of othersignificant neurologic or orthopedic disorders significantcoronal plane deformity or plantar flexion contracture andminimal fluctuating edema All subjects signed an informedconsent approved by the Marianjoy Rehabilitation HospitalInstitutional Review Board
Thirty individuals who satisfied inclusionexclusion cri-teria were selected to participate in the study There were15 males and 15 females with an average age of 604 plusmn 113years 16 of the subjects presented with right and 14 with lefthemiparesis The study participants received a full clinicalevaluation and assessment Based on this assessment the
clinic team determined the type of a plastic AFO (flexiblesemirigid or rigid) that was most appropriate for eachsubject Subjects were molded for the appropriate AFO [16]and measured for an Ossur AFO dynamic carbon off-the-shelf AFO Thus based on clinical evaluation a subjectprescribed for example with a semirigid AFO was providedwith a semirigid plastic AFO or a semirigid carbon off-the-shelf AFO Individuals who required a different type ofAFO such as a metal AFO were excluded from the studyPlastic AFOs were custom modified and fabricated from31610158401015840 polypropylene and included a proximal calf strap anddistal ankle wrap around strap During the course of the studysubjects were provided with minimal information about thedesign and construction of the different AFOs Instead theAFOswere described as AFOA andAFOB for the subjects toprevent their impression of the device from being influencedby words such as ldquocustomrdquo or ldquocarbonrdquo (Figure 1) Subjectswere tested at 21 plusmn 8 days after CVA While all of the subjectswere actively receiving physical and occupational therapyas prescribed by the treating physician none of them hadexperience with anAFOprior to the day of fitting and testingSubjects received clinically appropriate AFO three subjectsreceived a flexibleAFO twenty received a semirigidAFO andseven subjects were provided with rigid AFOs
22 Experimental Setup and Procedure During the tests thesubjectswere randomly providedwith an off-the-shelf carbonAFO (C-AFO) and a custom plastic AFO (P-AFO) Testingincluded assessment of gait while walking using differentAFOs and walking with no AFO (while each subject used thesame own shoes during all the tests) and participation in asurvey about the subjectrsquos perceptions of each AFO
Temporal and spatial gait parameters were collectedusing a GAITRite electronic walkway (CIR Systems IncHavertown PA) This device has been validated to study gaitof individuals with stroke [17] The 119871-test was used to furtherassess the subjectsrsquo functional walking ability The 119871-test isa variant of the Timed Up and Go (TUG) test that usesan L shaped path instead of a straight line path [18] Twowalks were performed using the GAITRite and the 119871-test foreach condition no AFO C-AFO and P-AFO Prior to thetests the subjects were allowed for a brief adaptation withthe AFOs The order of the test conditions was randomizedacross the subjects Subjects used an appropriate assistivedevice such as a cane or walker as needed each subjectused the same assistive device during all the tests involvingambulation Subjects were allowed close supervision by aphysical therapist but no direct contact A minimum offive-minute rest between test conditions was provided tominimize the effect of fatigue
All the study participants completed the Subject Percep-tion of Functional Benefit Survey about their impression ofthe device that was just used (with assigned values of 0 beingthe most positive response and 4 the most negative) Thissurvey was conducted after the use of each AFO type Inaddition at the end of the study subjects completed theSubject AFO Preference Survey to determine if subjects hada preference for the polymer AFO carbon fiber AFO bothAFOs or neither AFO (with assigned values of 0 being
Rehabilitation Research and Practice 3
(a) (b)
Figure 1 Off-the-shelf carbon AFO (a) and custom plastic AFO (b) used in the study
the most positive response and 3 the most negative) Thesesurveys are slightly modified versions of the survey describedin the literature [18]
23 Data Processing and Analysis Walking data was pro-cessed within the GAITRite software and velocity cadenceand stride and step length were obtained as outcome mea-sures All the datawere subjected to Shapiro-Wilk test for nor-mality One-way repeated measures ANOVA was performedwith factor AFO (3 levels no AFO C-AFO and P-AFO)separately for velocity cadence and stride length Split-plotANOVA was performed with factors AFO (3 levels no AFOC-AFO and P-AFO) and side (involved and uninvolved) toanalyze the differences in step length Pairwise comparisonswere used for further analyses of significant effects Mann-Whitney test comparing survey responses for the polymerAFO and the carbonAFOwas performed to test for statisticaldifference in subject perceptions of the functional benefit ofthe two different devices For all tests statistical significancewas set at119875 lt 005 Statistical analysis was performed in SPSS17 for Windows 7 (SPSS Inc Chicago USA)
3 Results
31 Gait Velocity With no AFO the patientsrsquo gait velocitywas 3050 plusmn 1358 cmsec When they were provided with theoff-the-shelf carbon AFO (C-AFO) gait velocity increasedto 3638 plusmn 1606 cmsec When a custom plastic AFO wasused their gait velocity increased further reaching 3921 plusmn1809 cmsec The difference in gait velocity was statisticallysignificant (119865
258= 2086 119875 lt 00001) Further analysis
revealed statistically significant difference between no AFOcondition andC-AFOandP-AFO (119875 = 0001 and119875 lt 00001resp) While the subjects were able to walk faster while being
provided with P-AFO as compared to C-AFO the differencewas not statistically significant (119875 = 011) (Figure 2)
32 Cadence While walking without AFO the subjectsrsquo ca-dence was 5493 plusmn 1395 stepsmin Cadence increased whileusing the AFOs Thus it reached 6020 plusmn 1472 and 6276 plusmn1581 steps per minute when the subjects were providedwith C-AFO and P-AFO respectivelyThe difference betweenconditions was statistically significant (119865
258= 2190 119875 lt
00001) Pairwise comparison revealed that no AFO condi-tion was statistically significant compared to C-AFO and P-AFO conditions (119875 = 0001 119875 lt 00001 resp) Howeverthe difference betweenC-AFO and P-AFOwas not significant(119875 = 0099) (Figure 2)
33 Stride Length Patients walking without AFOs showedstride length of 6498 plusmn 1686 cm When they were providedwith the off-the-shelf carbon AFO (C-AFO) stride lengthincreased to 7035 plusmn 1883 cm When a custom polymer AFOwas used the stride length increased further reaching 7235plusmn2011 cm The difference in stride length was statisticallysignificant (119865
258= 1023 119875 lt 00001) Further analysis
revealed statistically significant difference between no AFOcondition and C-AFO and P-AFO (119875 = 0006 and 119875 lt 001resp) The difference in stride length between walking whilebeing provided with P-AFO and C-AFO was not statisticallysignificant (119875 = 079)
34 Step Length Step length in conditions with no AFOwas 3699 plusmn 865 cm and 2763 plusmn 1401 cm for the involvedand uninvolved lower extremities respectivelyWhen the off-the-shelf carbon AFO (C-AFO) was provided step lengthincreased to 3966 plusmn 997 cm and 3100 plusmn 1166 cm on theinvolved and uninvolved side respectively Using the customP-AFO resulted in the increase of the step length on the
4 Rehabilitation Research and Practice
No AFOCarbon AFOPolymer AFO
No AFOCarbon AFOPolymer AFO
0
25
50
75
100
Cade
nce
lowast
lowastlowast
lowast
0
20
40
60
80Ve
loci
ty (c
ms
)
Figure 2 Gait velocity and cadence measured while walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
0
30
60
90
120
0
20
40
60
80
InvolvedUninvolved
No AFO Polymer AFOCarbon AFO
Strid
e len
gth
(cm
)
Step
leng
th (c
m)
lowast
lowast
lowast
lowast
lowast
lowast
No AFOCarbon AFOPolymer AFO
Figure 3 Stride length and step length recorded during walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
involved side to 4021 plusmn 969 and on the uninvolved side to3192 plusmn 1409 The difference in step length while providedwith AFOs was statistically significant (119865
2116= 1297 119875 lt
00001) The interaction between the AFOs and the involvedor uninvolved side was however not statistically significant(1198652116
= 024 119875 = 079) Further pairwise comparison ofthe use of AFOs revealed statistically significant differencebetween no AFO condition and C-AFO and P-AFO (119875 =0001 and 119875 lt 00001 resp) The difference in step length
between walking while being provided with P-AFO and C-AFO was not statistically significant (119875 = 099) (Figure 3)
35 119871-Test While walking without AFO the time needed tocross 10m distance by the subjects was 145 plusmn 071min Thistime decreased to 125 plusmn 079min and to 133 plusmn 066minwhen the subjects were provided with C-AFO and P-AFOrespectively (119871-test data was collected for 26 subjects) Thedifference between conditions however was not statistically
Rehabilitation Research and Practice 5
Table 1 Subjects perception of Functional Benefit Survey
With the AFO I just used Response Significance(1) Lifting my toes is Much easier A little easier No different A little harder Much harder 119875 = 0053(2) Swinging my leg forward is Much easier A little easier No different A little harder Much harder P = 0023(3) Taking weight through my foot is Much easier A little easier No different A little harder Much harder 119875 = 0105(4) My walking speed Much faster A little faster Not changed A little slower Much slower 119875 = 0051(5) My balance is Much better A little better No different A little worse Much worse P = 0006(6) My confidence is Much higher A little higher Not changed A little less Much less P = 0014(7) My sense of safety is Much higher A little higher Not changed A little less Much less P = 0005(8) Walking is Much easier A little easier No different A little harder Much harder P = 0009
Table 2 Subjects perceptions regarding the AFO type119873 = 29
Plastic AFO Carbon AFO Both None(1) Lifting my toes is easier with 8 (27) 5 (17) 14 (48) 1 (3)(2) Swinging my leg forward is easier with 17 (586) 8 (27) 4 (138) 0 (0)(3) Taking weight through my foot is easier with 16 (55) 8 (27) 5 (17) 0 (0)(4) I walk faster with 18 (62) 5 (17) 6 (21) 0 (0)(5) My balance is better with 18 (62) 5 (17) 6 (21) 0 (0)(6) My sense of safety is higher with 17 (586) 2 (7) 10 (34) 0 (0)(7) I like the fit and comfort of 15 (52) 11 (38) 2 (7) 1 (3)(8) I like the appearance of 17 (586) 9 (31) 3 (10) 0 (0)(9) I would rather use to assist my walking 7 (24) 9 (31) 6 (21) 7 (24)
significant (119865252
= 635 119875 = 014) Pairwise comparisonrevealed that no AFO condition was statistically significantcompared to C-AFO (119875 = 0004) At the same time thedifference between no AFO and P-AFO and between C-AFOand P-AFO was not statistically significant (119875 = 01417119875 = 046 resp)
36 Usersrsquo Perceptions regarding the AFO Type The analysisof the outcome of the Perception of Functional BenefitSurvey about the device that was just used revealed thatin general the study participants preferred P-AFO whencompared to the C-AFO (data for 29 subjects)Thus the usersdemonstrated statistically significant preference of using P-AFO while answering question 2 (119880 = 2805 119875 = 0023)question 5 (119880 = 252 119875 = 0006) question 6 (119880 = 271 119875 =0014) question 7 (119880 = 250 119875 = 0005) and question 8(119880 = 2625 119875 = 0009) Moreover the differences betweenthe two types of AFO were just under the level of statisticalsignificance for question 1 (119880 = 301 119875 = 0053) and question4 (119880 = 3015 119875 = 0051) (Table 1)
The analysis of the outcome of the Subject AFO Prefer-ence Survey revealed that the study participants preferredthe P-AFO to the C-AFO (Table 2) This was especially truewhen they were asked about balance and sense of safetyduring ambulation On average 5087 plusmn 147 of the studyparticipants preferred P-AFO and 2356 plusmn 970 of thesubjects preferred C-AFO It is also important to mentionthat 181 plusmn 83 preferred using both types of AFOs and only
31plusmn790of the study participants preferred not using eithertype of AFO
4 Discussion
It is documented in the prior literature that individuals afterCVA walk slower than healthy individuals [19] It was alsoreported that the ability of individualswith stroke to ambulateis improved as a result of wearing an ankle-foot orthosis [20]Moreover there is a plethora of evidence on the beneficialeffect of AFOs in improving of functional mobility andquality of gait as well as decreasing the likelihood of falls inindividuals suffering from a CVA [21 22] Thus individualswith CVA provided with an AFO improved gait parameterssuch as cadence stride length and gait velocity [18 23 24]Moreover improvement in gait velocity that is believed toreflect progress in mobility is often used as a measure ofrecovery after a CVA [20 25 26] and is considered animportant goal of rehabilitation
At the same time the literature on the use of differenttypes of AFOs (especially recently introduced carbon AFOs)to improve ambulation of individuals with CVA is limited Assuch the goals of the study were to investigate the effect ofwalking using the prefabricated carbon AFO in comparisonwith the custompolymer AFO and noAFO and to investigatethe usersrsquo preference in using either the prefabricated carbonAFO or the custom plastic AFO
The results of the current study demonstrated that indi-viduals with acute CVA increased their gait velocity when
6 Rehabilitation Research and Practice
using either C-AFO or P-AFO and as a result the gapbetween ldquonormalrdquo and ldquohemipareticrdquo gait velocity decreasedThese results are in line with the literature reporting a positiveeffect of AFOs on gait velocity of individuals with hemiparesis[9 19 27] Similarly improvements in cadence were associ-ated with the use of an AFO without an AFO patients walkedwith lower cadence as compared to healthy individuals Asimilar positive effect of AFOs on cadence of individuals withhemiparesis was described in the literature [27 28] Sincecadence is the number of steps taken in a certain time theobserved increase in the velocity of gait could be due tochanges in the number of steps per minute Nevertheless theimpact of AFOs on cadence remains inconclusive as somestudies report an improvement in this variable with the AFOuse and others report no significant improvement [22] Thusthere is a need for more studies focused on the investigationof the role of different types of AFOs on gait velocity andcadence An increase in the average stride and step lengthwith either type of AFO was evident in the current study andhas been also reported in the past literature [27 28]
While in general there is a consensus in the literaturethat gait velocity is a powerful indicator of function andprognosis after CVA [26] there is an opinion that gait velocityitself may not be wholly representative of functional mobil-ity and meaningful improvement in performance [29] Toaddress this possible concern we added the 119871-test assessment(that includes rising from a chair two 90-degree turns inopposite directions a 180-degree turn and returning to aseated position) as the task that is indicative of the typesof movements that are required in household ambulationThe outcome of the 119871-test revealed that patients while usingAFOs of either type showed better performance comparedto walking with no AFO Moreover clinically the patientsshowed improvement as the time needed for the completionof the test was shorter when they were provided with eithertype of AFO
The study participants were positive about the use ofAFOs as the majority found it comfortable and felt itimproved their walking particularly the functional aspectssuch as safety and confidence This finding is in line withthe literature reporting that 96 of users felt they walkedbetter with the AFO and found it comfortable [18] Moreoverthe majority of the subjects gave a preference to the custom-made plastic AFOs the subjects perception was about 2 1 infavor of the custom-made plastic AFOThis could be becauseeach plastic AFO was specifically molded and fitted for eachsubject Nevertheless further study is needed to examine thelonger-term effects and the cost-effectiveness of prescribing acustom-made or off-the-shelf AFO for people with CVA
5 Conclusion
Both types of AFO significantly improved gait velocitycadence step length and stride length in patients with acuteCVAThe majority of users preferred the custom-made plas-tic AFO over the prefabricated carbon AFO This outcomeshould be taken into consideration while prescribing AFOsFurther study is needed to examine the longer-term effects
and the cost-effectiveness of prescribing different types ofAFO for people with CVA
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] V L Roger A S Go D M Lloyd-Jones et al ldquoHeart diseaseand stroke statisticsmdash2011 update a report from the AmericanHeart Associationrdquo Circulation vol 123 no 4 pp e18ndashe2092011
[2] M Kelly-Hayes J T Robertson J P Broderick et al ldquoTheAmerican heart association stroke outcome classificationrdquoStroke vol 29 no 6 pp 1274ndash1280 1998
[3] C Detrembleur F Dierick G Stoquart F Chantraine andT Lejeune ldquoEnergy cost mechanical work and efficiency ofhemiparetic walkingrdquo Gait amp Posture vol 18 no 2 pp 47ndash552003
[4] N Wada M Sohmiya T Shimizu K Okamoto and K Shi-rakura ldquoClinical analysis of risk factors for falls in home-livingstroke patients using functional evaluation toolsrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1601ndash1605 2007
[5] S E Lord K McPherson H K McNaughton L Rochesterand M Weatherall ldquoCommunity ambulation after stroke howimportant and obtainable is it and what measures appearpredictiverdquo Archives of Physical Medicine and Rehabilitationvol 85 no 2 pp 234ndash239 2004
[6] J F Lehmann S M Condon R Price and B J deLateurldquoGait abnormalities in hemiplegia their correction by ankle-foot orthosesrdquo Archives of Physical Medicine and Rehabilitationvol 68 no 11 pp 763ndash771 1987
[7] H Beckerman J Becher G J Lankhorst and A L M VerbeekldquoWalking ability of stroke patients efficacy of tibial nerveblocking and a polypropylene ankle-foot orthosisrdquo Archives ofPhysical Medicine and Rehabilitation vol 77 no 11 pp 1144ndash1151 1996
[8] D C M de Wit J H Buurke J M M Nijlant M J IJzermanand H J Hermens ldquoThe effect of an ankle-foot orthosison walking ability in chronic stroke patients a randomizedcontrolled trialrdquo Clinical Rehabilitation vol 18 no 5 pp 550ndash557 2004
[9] M Franceschini M Massucci L Ferrari M Agosti and CParoli ldquoEffects of an ankle-foot orthosis on spatiotemporalparameters and energy cost of hemiparetic gaitrdquo Clinical Reha-bilitation vol 17 no 4 pp 368ndash372 2003
[10] N Rao G Chaudhuri D Hasso et al ldquoGait assessment duringthe initial fitting of an ankle foot orthosis in individuals withstrokerdquo Disability and Rehabilitation Assistive Technology vol3 no 4 pp 201ndash207 2008
[11] S Roehrig andDA Yates ldquoCase report effects of a neworthosisand physical therapy on gait in a subject with longstandinghemiplegiardquo Journal of Geriatric Physical Therapy vol 31 no1 pp 38ndash46 2008
[12] H B Kitaoka X M Crevoisier K Harbst D Hansen BKotajarvi and K Kaufman ldquoThe effect of custom-made bracesfor the ankle and hindfoot on ankle and foot kinematics and
Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005

Rehabilitation Research and Practice 3
(a) (b)
Figure 1 Off-the-shelf carbon AFO (a) and custom plastic AFO (b) used in the study
the most positive response and 3 the most negative) Thesesurveys are slightly modified versions of the survey describedin the literature [18]
23 Data Processing and Analysis Walking data was pro-cessed within the GAITRite software and velocity cadenceand stride and step length were obtained as outcome mea-sures All the datawere subjected to Shapiro-Wilk test for nor-mality One-way repeated measures ANOVA was performedwith factor AFO (3 levels no AFO C-AFO and P-AFO)separately for velocity cadence and stride length Split-plotANOVA was performed with factors AFO (3 levels no AFOC-AFO and P-AFO) and side (involved and uninvolved) toanalyze the differences in step length Pairwise comparisonswere used for further analyses of significant effects Mann-Whitney test comparing survey responses for the polymerAFO and the carbonAFOwas performed to test for statisticaldifference in subject perceptions of the functional benefit ofthe two different devices For all tests statistical significancewas set at119875 lt 005 Statistical analysis was performed in SPSS17 for Windows 7 (SPSS Inc Chicago USA)
3 Results
31 Gait Velocity With no AFO the patientsrsquo gait velocitywas 3050 plusmn 1358 cmsec When they were provided with theoff-the-shelf carbon AFO (C-AFO) gait velocity increasedto 3638 plusmn 1606 cmsec When a custom plastic AFO wasused their gait velocity increased further reaching 3921 plusmn1809 cmsec The difference in gait velocity was statisticallysignificant (119865
258= 2086 119875 lt 00001) Further analysis
revealed statistically significant difference between no AFOcondition andC-AFOandP-AFO (119875 = 0001 and119875 lt 00001resp) While the subjects were able to walk faster while being
provided with P-AFO as compared to C-AFO the differencewas not statistically significant (119875 = 011) (Figure 2)
32 Cadence While walking without AFO the subjectsrsquo ca-dence was 5493 plusmn 1395 stepsmin Cadence increased whileusing the AFOs Thus it reached 6020 plusmn 1472 and 6276 plusmn1581 steps per minute when the subjects were providedwith C-AFO and P-AFO respectivelyThe difference betweenconditions was statistically significant (119865
258= 2190 119875 lt
00001) Pairwise comparison revealed that no AFO condi-tion was statistically significant compared to C-AFO and P-AFO conditions (119875 = 0001 119875 lt 00001 resp) Howeverthe difference betweenC-AFO and P-AFOwas not significant(119875 = 0099) (Figure 2)
33 Stride Length Patients walking without AFOs showedstride length of 6498 plusmn 1686 cm When they were providedwith the off-the-shelf carbon AFO (C-AFO) stride lengthincreased to 7035 plusmn 1883 cm When a custom polymer AFOwas used the stride length increased further reaching 7235plusmn2011 cm The difference in stride length was statisticallysignificant (119865
258= 1023 119875 lt 00001) Further analysis
revealed statistically significant difference between no AFOcondition and C-AFO and P-AFO (119875 = 0006 and 119875 lt 001resp) The difference in stride length between walking whilebeing provided with P-AFO and C-AFO was not statisticallysignificant (119875 = 079)
34 Step Length Step length in conditions with no AFOwas 3699 plusmn 865 cm and 2763 plusmn 1401 cm for the involvedand uninvolved lower extremities respectivelyWhen the off-the-shelf carbon AFO (C-AFO) was provided step lengthincreased to 3966 plusmn 997 cm and 3100 plusmn 1166 cm on theinvolved and uninvolved side respectively Using the customP-AFO resulted in the increase of the step length on the
4 Rehabilitation Research and Practice
No AFOCarbon AFOPolymer AFO
No AFOCarbon AFOPolymer AFO
0
25
50
75
100
Cade
nce
lowast
lowastlowast
lowast
0
20
40
60
80Ve
loci
ty (c
ms
)
Figure 2 Gait velocity and cadence measured while walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
0
30
60
90
120
0
20
40
60
80
InvolvedUninvolved
No AFO Polymer AFOCarbon AFO
Strid
e len
gth
(cm
)
Step
leng
th (c
m)
lowast
lowast
lowast
lowast
lowast
lowast
No AFOCarbon AFOPolymer AFO
Figure 3 Stride length and step length recorded during walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
involved side to 4021 plusmn 969 and on the uninvolved side to3192 plusmn 1409 The difference in step length while providedwith AFOs was statistically significant (119865
2116= 1297 119875 lt
00001) The interaction between the AFOs and the involvedor uninvolved side was however not statistically significant(1198652116
= 024 119875 = 079) Further pairwise comparison ofthe use of AFOs revealed statistically significant differencebetween no AFO condition and C-AFO and P-AFO (119875 =0001 and 119875 lt 00001 resp) The difference in step length
between walking while being provided with P-AFO and C-AFO was not statistically significant (119875 = 099) (Figure 3)
35 119871-Test While walking without AFO the time needed tocross 10m distance by the subjects was 145 plusmn 071min Thistime decreased to 125 plusmn 079min and to 133 plusmn 066minwhen the subjects were provided with C-AFO and P-AFOrespectively (119871-test data was collected for 26 subjects) Thedifference between conditions however was not statistically
Rehabilitation Research and Practice 5
Table 1 Subjects perception of Functional Benefit Survey
With the AFO I just used Response Significance(1) Lifting my toes is Much easier A little easier No different A little harder Much harder 119875 = 0053(2) Swinging my leg forward is Much easier A little easier No different A little harder Much harder P = 0023(3) Taking weight through my foot is Much easier A little easier No different A little harder Much harder 119875 = 0105(4) My walking speed Much faster A little faster Not changed A little slower Much slower 119875 = 0051(5) My balance is Much better A little better No different A little worse Much worse P = 0006(6) My confidence is Much higher A little higher Not changed A little less Much less P = 0014(7) My sense of safety is Much higher A little higher Not changed A little less Much less P = 0005(8) Walking is Much easier A little easier No different A little harder Much harder P = 0009
Table 2 Subjects perceptions regarding the AFO type119873 = 29
Plastic AFO Carbon AFO Both None(1) Lifting my toes is easier with 8 (27) 5 (17) 14 (48) 1 (3)(2) Swinging my leg forward is easier with 17 (586) 8 (27) 4 (138) 0 (0)(3) Taking weight through my foot is easier with 16 (55) 8 (27) 5 (17) 0 (0)(4) I walk faster with 18 (62) 5 (17) 6 (21) 0 (0)(5) My balance is better with 18 (62) 5 (17) 6 (21) 0 (0)(6) My sense of safety is higher with 17 (586) 2 (7) 10 (34) 0 (0)(7) I like the fit and comfort of 15 (52) 11 (38) 2 (7) 1 (3)(8) I like the appearance of 17 (586) 9 (31) 3 (10) 0 (0)(9) I would rather use to assist my walking 7 (24) 9 (31) 6 (21) 7 (24)
significant (119865252
= 635 119875 = 014) Pairwise comparisonrevealed that no AFO condition was statistically significantcompared to C-AFO (119875 = 0004) At the same time thedifference between no AFO and P-AFO and between C-AFOand P-AFO was not statistically significant (119875 = 01417119875 = 046 resp)
36 Usersrsquo Perceptions regarding the AFO Type The analysisof the outcome of the Perception of Functional BenefitSurvey about the device that was just used revealed thatin general the study participants preferred P-AFO whencompared to the C-AFO (data for 29 subjects)Thus the usersdemonstrated statistically significant preference of using P-AFO while answering question 2 (119880 = 2805 119875 = 0023)question 5 (119880 = 252 119875 = 0006) question 6 (119880 = 271 119875 =0014) question 7 (119880 = 250 119875 = 0005) and question 8(119880 = 2625 119875 = 0009) Moreover the differences betweenthe two types of AFO were just under the level of statisticalsignificance for question 1 (119880 = 301 119875 = 0053) and question4 (119880 = 3015 119875 = 0051) (Table 1)
The analysis of the outcome of the Subject AFO Prefer-ence Survey revealed that the study participants preferredthe P-AFO to the C-AFO (Table 2) This was especially truewhen they were asked about balance and sense of safetyduring ambulation On average 5087 plusmn 147 of the studyparticipants preferred P-AFO and 2356 plusmn 970 of thesubjects preferred C-AFO It is also important to mentionthat 181 plusmn 83 preferred using both types of AFOs and only
31plusmn790of the study participants preferred not using eithertype of AFO
4 Discussion
It is documented in the prior literature that individuals afterCVA walk slower than healthy individuals [19] It was alsoreported that the ability of individualswith stroke to ambulateis improved as a result of wearing an ankle-foot orthosis [20]Moreover there is a plethora of evidence on the beneficialeffect of AFOs in improving of functional mobility andquality of gait as well as decreasing the likelihood of falls inindividuals suffering from a CVA [21 22] Thus individualswith CVA provided with an AFO improved gait parameterssuch as cadence stride length and gait velocity [18 23 24]Moreover improvement in gait velocity that is believed toreflect progress in mobility is often used as a measure ofrecovery after a CVA [20 25 26] and is considered animportant goal of rehabilitation
At the same time the literature on the use of differenttypes of AFOs (especially recently introduced carbon AFOs)to improve ambulation of individuals with CVA is limited Assuch the goals of the study were to investigate the effect ofwalking using the prefabricated carbon AFO in comparisonwith the custompolymer AFO and noAFO and to investigatethe usersrsquo preference in using either the prefabricated carbonAFO or the custom plastic AFO
The results of the current study demonstrated that indi-viduals with acute CVA increased their gait velocity when
6 Rehabilitation Research and Practice
using either C-AFO or P-AFO and as a result the gapbetween ldquonormalrdquo and ldquohemipareticrdquo gait velocity decreasedThese results are in line with the literature reporting a positiveeffect of AFOs on gait velocity of individuals with hemiparesis[9 19 27] Similarly improvements in cadence were associ-ated with the use of an AFO without an AFO patients walkedwith lower cadence as compared to healthy individuals Asimilar positive effect of AFOs on cadence of individuals withhemiparesis was described in the literature [27 28] Sincecadence is the number of steps taken in a certain time theobserved increase in the velocity of gait could be due tochanges in the number of steps per minute Nevertheless theimpact of AFOs on cadence remains inconclusive as somestudies report an improvement in this variable with the AFOuse and others report no significant improvement [22] Thusthere is a need for more studies focused on the investigationof the role of different types of AFOs on gait velocity andcadence An increase in the average stride and step lengthwith either type of AFO was evident in the current study andhas been also reported in the past literature [27 28]
While in general there is a consensus in the literaturethat gait velocity is a powerful indicator of function andprognosis after CVA [26] there is an opinion that gait velocityitself may not be wholly representative of functional mobil-ity and meaningful improvement in performance [29] Toaddress this possible concern we added the 119871-test assessment(that includes rising from a chair two 90-degree turns inopposite directions a 180-degree turn and returning to aseated position) as the task that is indicative of the typesof movements that are required in household ambulationThe outcome of the 119871-test revealed that patients while usingAFOs of either type showed better performance comparedto walking with no AFO Moreover clinically the patientsshowed improvement as the time needed for the completionof the test was shorter when they were provided with eithertype of AFO
The study participants were positive about the use ofAFOs as the majority found it comfortable and felt itimproved their walking particularly the functional aspectssuch as safety and confidence This finding is in line withthe literature reporting that 96 of users felt they walkedbetter with the AFO and found it comfortable [18] Moreoverthe majority of the subjects gave a preference to the custom-made plastic AFOs the subjects perception was about 2 1 infavor of the custom-made plastic AFOThis could be becauseeach plastic AFO was specifically molded and fitted for eachsubject Nevertheless further study is needed to examine thelonger-term effects and the cost-effectiveness of prescribing acustom-made or off-the-shelf AFO for people with CVA
5 Conclusion
Both types of AFO significantly improved gait velocitycadence step length and stride length in patients with acuteCVAThe majority of users preferred the custom-made plas-tic AFO over the prefabricated carbon AFO This outcomeshould be taken into consideration while prescribing AFOsFurther study is needed to examine the longer-term effects
and the cost-effectiveness of prescribing different types ofAFO for people with CVA
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] V L Roger A S Go D M Lloyd-Jones et al ldquoHeart diseaseand stroke statisticsmdash2011 update a report from the AmericanHeart Associationrdquo Circulation vol 123 no 4 pp e18ndashe2092011
[2] M Kelly-Hayes J T Robertson J P Broderick et al ldquoTheAmerican heart association stroke outcome classificationrdquoStroke vol 29 no 6 pp 1274ndash1280 1998
[3] C Detrembleur F Dierick G Stoquart F Chantraine andT Lejeune ldquoEnergy cost mechanical work and efficiency ofhemiparetic walkingrdquo Gait amp Posture vol 18 no 2 pp 47ndash552003
[4] N Wada M Sohmiya T Shimizu K Okamoto and K Shi-rakura ldquoClinical analysis of risk factors for falls in home-livingstroke patients using functional evaluation toolsrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1601ndash1605 2007
[5] S E Lord K McPherson H K McNaughton L Rochesterand M Weatherall ldquoCommunity ambulation after stroke howimportant and obtainable is it and what measures appearpredictiverdquo Archives of Physical Medicine and Rehabilitationvol 85 no 2 pp 234ndash239 2004
[6] J F Lehmann S M Condon R Price and B J deLateurldquoGait abnormalities in hemiplegia their correction by ankle-foot orthosesrdquo Archives of Physical Medicine and Rehabilitationvol 68 no 11 pp 763ndash771 1987
[7] H Beckerman J Becher G J Lankhorst and A L M VerbeekldquoWalking ability of stroke patients efficacy of tibial nerveblocking and a polypropylene ankle-foot orthosisrdquo Archives ofPhysical Medicine and Rehabilitation vol 77 no 11 pp 1144ndash1151 1996
[8] D C M de Wit J H Buurke J M M Nijlant M J IJzermanand H J Hermens ldquoThe effect of an ankle-foot orthosison walking ability in chronic stroke patients a randomizedcontrolled trialrdquo Clinical Rehabilitation vol 18 no 5 pp 550ndash557 2004
[9] M Franceschini M Massucci L Ferrari M Agosti and CParoli ldquoEffects of an ankle-foot orthosis on spatiotemporalparameters and energy cost of hemiparetic gaitrdquo Clinical Reha-bilitation vol 17 no 4 pp 368ndash372 2003
[10] N Rao G Chaudhuri D Hasso et al ldquoGait assessment duringthe initial fitting of an ankle foot orthosis in individuals withstrokerdquo Disability and Rehabilitation Assistive Technology vol3 no 4 pp 201ndash207 2008
[11] S Roehrig andDA Yates ldquoCase report effects of a neworthosisand physical therapy on gait in a subject with longstandinghemiplegiardquo Journal of Geriatric Physical Therapy vol 31 no1 pp 38ndash46 2008
[12] H B Kitaoka X M Crevoisier K Harbst D Hansen BKotajarvi and K Kaufman ldquoThe effect of custom-made bracesfor the ankle and hindfoot on ankle and foot kinematics and
Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005

4 Rehabilitation Research and Practice
No AFOCarbon AFOPolymer AFO
No AFOCarbon AFOPolymer AFO
0
25
50
75
100
Cade
nce
lowast
lowastlowast
lowast
0
20
40
60
80Ve
loci
ty (c
ms
)
Figure 2 Gait velocity and cadence measured while walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
0
30
60
90
120
0
20
40
60
80
InvolvedUninvolved
No AFO Polymer AFOCarbon AFO
Strid
e len
gth
(cm
)
Step
leng
th (c
m)
lowast
lowast
lowast
lowast
lowast
lowast
No AFOCarbon AFOPolymer AFO
Figure 3 Stride length and step length recorded during walking without an AFO and with a carbon AFO or plastic AFO lowast shows statisticalsignificance (119875 lt 0001)
involved side to 4021 plusmn 969 and on the uninvolved side to3192 plusmn 1409 The difference in step length while providedwith AFOs was statistically significant (119865
2116= 1297 119875 lt
00001) The interaction between the AFOs and the involvedor uninvolved side was however not statistically significant(1198652116
= 024 119875 = 079) Further pairwise comparison ofthe use of AFOs revealed statistically significant differencebetween no AFO condition and C-AFO and P-AFO (119875 =0001 and 119875 lt 00001 resp) The difference in step length
between walking while being provided with P-AFO and C-AFO was not statistically significant (119875 = 099) (Figure 3)
35 119871-Test While walking without AFO the time needed tocross 10m distance by the subjects was 145 plusmn 071min Thistime decreased to 125 plusmn 079min and to 133 plusmn 066minwhen the subjects were provided with C-AFO and P-AFOrespectively (119871-test data was collected for 26 subjects) Thedifference between conditions however was not statistically
Rehabilitation Research and Practice 5
Table 1 Subjects perception of Functional Benefit Survey
With the AFO I just used Response Significance(1) Lifting my toes is Much easier A little easier No different A little harder Much harder 119875 = 0053(2) Swinging my leg forward is Much easier A little easier No different A little harder Much harder P = 0023(3) Taking weight through my foot is Much easier A little easier No different A little harder Much harder 119875 = 0105(4) My walking speed Much faster A little faster Not changed A little slower Much slower 119875 = 0051(5) My balance is Much better A little better No different A little worse Much worse P = 0006(6) My confidence is Much higher A little higher Not changed A little less Much less P = 0014(7) My sense of safety is Much higher A little higher Not changed A little less Much less P = 0005(8) Walking is Much easier A little easier No different A little harder Much harder P = 0009
Table 2 Subjects perceptions regarding the AFO type119873 = 29
Plastic AFO Carbon AFO Both None(1) Lifting my toes is easier with 8 (27) 5 (17) 14 (48) 1 (3)(2) Swinging my leg forward is easier with 17 (586) 8 (27) 4 (138) 0 (0)(3) Taking weight through my foot is easier with 16 (55) 8 (27) 5 (17) 0 (0)(4) I walk faster with 18 (62) 5 (17) 6 (21) 0 (0)(5) My balance is better with 18 (62) 5 (17) 6 (21) 0 (0)(6) My sense of safety is higher with 17 (586) 2 (7) 10 (34) 0 (0)(7) I like the fit and comfort of 15 (52) 11 (38) 2 (7) 1 (3)(8) I like the appearance of 17 (586) 9 (31) 3 (10) 0 (0)(9) I would rather use to assist my walking 7 (24) 9 (31) 6 (21) 7 (24)
significant (119865252
= 635 119875 = 014) Pairwise comparisonrevealed that no AFO condition was statistically significantcompared to C-AFO (119875 = 0004) At the same time thedifference between no AFO and P-AFO and between C-AFOand P-AFO was not statistically significant (119875 = 01417119875 = 046 resp)
36 Usersrsquo Perceptions regarding the AFO Type The analysisof the outcome of the Perception of Functional BenefitSurvey about the device that was just used revealed thatin general the study participants preferred P-AFO whencompared to the C-AFO (data for 29 subjects)Thus the usersdemonstrated statistically significant preference of using P-AFO while answering question 2 (119880 = 2805 119875 = 0023)question 5 (119880 = 252 119875 = 0006) question 6 (119880 = 271 119875 =0014) question 7 (119880 = 250 119875 = 0005) and question 8(119880 = 2625 119875 = 0009) Moreover the differences betweenthe two types of AFO were just under the level of statisticalsignificance for question 1 (119880 = 301 119875 = 0053) and question4 (119880 = 3015 119875 = 0051) (Table 1)
The analysis of the outcome of the Subject AFO Prefer-ence Survey revealed that the study participants preferredthe P-AFO to the C-AFO (Table 2) This was especially truewhen they were asked about balance and sense of safetyduring ambulation On average 5087 plusmn 147 of the studyparticipants preferred P-AFO and 2356 plusmn 970 of thesubjects preferred C-AFO It is also important to mentionthat 181 plusmn 83 preferred using both types of AFOs and only
31plusmn790of the study participants preferred not using eithertype of AFO
4 Discussion
It is documented in the prior literature that individuals afterCVA walk slower than healthy individuals [19] It was alsoreported that the ability of individualswith stroke to ambulateis improved as a result of wearing an ankle-foot orthosis [20]Moreover there is a plethora of evidence on the beneficialeffect of AFOs in improving of functional mobility andquality of gait as well as decreasing the likelihood of falls inindividuals suffering from a CVA [21 22] Thus individualswith CVA provided with an AFO improved gait parameterssuch as cadence stride length and gait velocity [18 23 24]Moreover improvement in gait velocity that is believed toreflect progress in mobility is often used as a measure ofrecovery after a CVA [20 25 26] and is considered animportant goal of rehabilitation
At the same time the literature on the use of differenttypes of AFOs (especially recently introduced carbon AFOs)to improve ambulation of individuals with CVA is limited Assuch the goals of the study were to investigate the effect ofwalking using the prefabricated carbon AFO in comparisonwith the custompolymer AFO and noAFO and to investigatethe usersrsquo preference in using either the prefabricated carbonAFO or the custom plastic AFO
The results of the current study demonstrated that indi-viduals with acute CVA increased their gait velocity when
6 Rehabilitation Research and Practice
using either C-AFO or P-AFO and as a result the gapbetween ldquonormalrdquo and ldquohemipareticrdquo gait velocity decreasedThese results are in line with the literature reporting a positiveeffect of AFOs on gait velocity of individuals with hemiparesis[9 19 27] Similarly improvements in cadence were associ-ated with the use of an AFO without an AFO patients walkedwith lower cadence as compared to healthy individuals Asimilar positive effect of AFOs on cadence of individuals withhemiparesis was described in the literature [27 28] Sincecadence is the number of steps taken in a certain time theobserved increase in the velocity of gait could be due tochanges in the number of steps per minute Nevertheless theimpact of AFOs on cadence remains inconclusive as somestudies report an improvement in this variable with the AFOuse and others report no significant improvement [22] Thusthere is a need for more studies focused on the investigationof the role of different types of AFOs on gait velocity andcadence An increase in the average stride and step lengthwith either type of AFO was evident in the current study andhas been also reported in the past literature [27 28]
While in general there is a consensus in the literaturethat gait velocity is a powerful indicator of function andprognosis after CVA [26] there is an opinion that gait velocityitself may not be wholly representative of functional mobil-ity and meaningful improvement in performance [29] Toaddress this possible concern we added the 119871-test assessment(that includes rising from a chair two 90-degree turns inopposite directions a 180-degree turn and returning to aseated position) as the task that is indicative of the typesof movements that are required in household ambulationThe outcome of the 119871-test revealed that patients while usingAFOs of either type showed better performance comparedto walking with no AFO Moreover clinically the patientsshowed improvement as the time needed for the completionof the test was shorter when they were provided with eithertype of AFO
The study participants were positive about the use ofAFOs as the majority found it comfortable and felt itimproved their walking particularly the functional aspectssuch as safety and confidence This finding is in line withthe literature reporting that 96 of users felt they walkedbetter with the AFO and found it comfortable [18] Moreoverthe majority of the subjects gave a preference to the custom-made plastic AFOs the subjects perception was about 2 1 infavor of the custom-made plastic AFOThis could be becauseeach plastic AFO was specifically molded and fitted for eachsubject Nevertheless further study is needed to examine thelonger-term effects and the cost-effectiveness of prescribing acustom-made or off-the-shelf AFO for people with CVA
5 Conclusion
Both types of AFO significantly improved gait velocitycadence step length and stride length in patients with acuteCVAThe majority of users preferred the custom-made plas-tic AFO over the prefabricated carbon AFO This outcomeshould be taken into consideration while prescribing AFOsFurther study is needed to examine the longer-term effects
and the cost-effectiveness of prescribing different types ofAFO for people with CVA
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] V L Roger A S Go D M Lloyd-Jones et al ldquoHeart diseaseand stroke statisticsmdash2011 update a report from the AmericanHeart Associationrdquo Circulation vol 123 no 4 pp e18ndashe2092011
[2] M Kelly-Hayes J T Robertson J P Broderick et al ldquoTheAmerican heart association stroke outcome classificationrdquoStroke vol 29 no 6 pp 1274ndash1280 1998
[3] C Detrembleur F Dierick G Stoquart F Chantraine andT Lejeune ldquoEnergy cost mechanical work and efficiency ofhemiparetic walkingrdquo Gait amp Posture vol 18 no 2 pp 47ndash552003
[4] N Wada M Sohmiya T Shimizu K Okamoto and K Shi-rakura ldquoClinical analysis of risk factors for falls in home-livingstroke patients using functional evaluation toolsrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1601ndash1605 2007
[5] S E Lord K McPherson H K McNaughton L Rochesterand M Weatherall ldquoCommunity ambulation after stroke howimportant and obtainable is it and what measures appearpredictiverdquo Archives of Physical Medicine and Rehabilitationvol 85 no 2 pp 234ndash239 2004
[6] J F Lehmann S M Condon R Price and B J deLateurldquoGait abnormalities in hemiplegia their correction by ankle-foot orthosesrdquo Archives of Physical Medicine and Rehabilitationvol 68 no 11 pp 763ndash771 1987
[7] H Beckerman J Becher G J Lankhorst and A L M VerbeekldquoWalking ability of stroke patients efficacy of tibial nerveblocking and a polypropylene ankle-foot orthosisrdquo Archives ofPhysical Medicine and Rehabilitation vol 77 no 11 pp 1144ndash1151 1996
[8] D C M de Wit J H Buurke J M M Nijlant M J IJzermanand H J Hermens ldquoThe effect of an ankle-foot orthosison walking ability in chronic stroke patients a randomizedcontrolled trialrdquo Clinical Rehabilitation vol 18 no 5 pp 550ndash557 2004
[9] M Franceschini M Massucci L Ferrari M Agosti and CParoli ldquoEffects of an ankle-foot orthosis on spatiotemporalparameters and energy cost of hemiparetic gaitrdquo Clinical Reha-bilitation vol 17 no 4 pp 368ndash372 2003
[10] N Rao G Chaudhuri D Hasso et al ldquoGait assessment duringthe initial fitting of an ankle foot orthosis in individuals withstrokerdquo Disability and Rehabilitation Assistive Technology vol3 no 4 pp 201ndash207 2008
[11] S Roehrig andDA Yates ldquoCase report effects of a neworthosisand physical therapy on gait in a subject with longstandinghemiplegiardquo Journal of Geriatric Physical Therapy vol 31 no1 pp 38ndash46 2008
[12] H B Kitaoka X M Crevoisier K Harbst D Hansen BKotajarvi and K Kaufman ldquoThe effect of custom-made bracesfor the ankle and hindfoot on ankle and foot kinematics and
Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005

Rehabilitation Research and Practice 5
Table 1 Subjects perception of Functional Benefit Survey
With the AFO I just used Response Significance(1) Lifting my toes is Much easier A little easier No different A little harder Much harder 119875 = 0053(2) Swinging my leg forward is Much easier A little easier No different A little harder Much harder P = 0023(3) Taking weight through my foot is Much easier A little easier No different A little harder Much harder 119875 = 0105(4) My walking speed Much faster A little faster Not changed A little slower Much slower 119875 = 0051(5) My balance is Much better A little better No different A little worse Much worse P = 0006(6) My confidence is Much higher A little higher Not changed A little less Much less P = 0014(7) My sense of safety is Much higher A little higher Not changed A little less Much less P = 0005(8) Walking is Much easier A little easier No different A little harder Much harder P = 0009
Table 2 Subjects perceptions regarding the AFO type119873 = 29
Plastic AFO Carbon AFO Both None(1) Lifting my toes is easier with 8 (27) 5 (17) 14 (48) 1 (3)(2) Swinging my leg forward is easier with 17 (586) 8 (27) 4 (138) 0 (0)(3) Taking weight through my foot is easier with 16 (55) 8 (27) 5 (17) 0 (0)(4) I walk faster with 18 (62) 5 (17) 6 (21) 0 (0)(5) My balance is better with 18 (62) 5 (17) 6 (21) 0 (0)(6) My sense of safety is higher with 17 (586) 2 (7) 10 (34) 0 (0)(7) I like the fit and comfort of 15 (52) 11 (38) 2 (7) 1 (3)(8) I like the appearance of 17 (586) 9 (31) 3 (10) 0 (0)(9) I would rather use to assist my walking 7 (24) 9 (31) 6 (21) 7 (24)
significant (119865252
= 635 119875 = 014) Pairwise comparisonrevealed that no AFO condition was statistically significantcompared to C-AFO (119875 = 0004) At the same time thedifference between no AFO and P-AFO and between C-AFOand P-AFO was not statistically significant (119875 = 01417119875 = 046 resp)
36 Usersrsquo Perceptions regarding the AFO Type The analysisof the outcome of the Perception of Functional BenefitSurvey about the device that was just used revealed thatin general the study participants preferred P-AFO whencompared to the C-AFO (data for 29 subjects)Thus the usersdemonstrated statistically significant preference of using P-AFO while answering question 2 (119880 = 2805 119875 = 0023)question 5 (119880 = 252 119875 = 0006) question 6 (119880 = 271 119875 =0014) question 7 (119880 = 250 119875 = 0005) and question 8(119880 = 2625 119875 = 0009) Moreover the differences betweenthe two types of AFO were just under the level of statisticalsignificance for question 1 (119880 = 301 119875 = 0053) and question4 (119880 = 3015 119875 = 0051) (Table 1)
The analysis of the outcome of the Subject AFO Prefer-ence Survey revealed that the study participants preferredthe P-AFO to the C-AFO (Table 2) This was especially truewhen they were asked about balance and sense of safetyduring ambulation On average 5087 plusmn 147 of the studyparticipants preferred P-AFO and 2356 plusmn 970 of thesubjects preferred C-AFO It is also important to mentionthat 181 plusmn 83 preferred using both types of AFOs and only
31plusmn790of the study participants preferred not using eithertype of AFO
4 Discussion
It is documented in the prior literature that individuals afterCVA walk slower than healthy individuals [19] It was alsoreported that the ability of individualswith stroke to ambulateis improved as a result of wearing an ankle-foot orthosis [20]Moreover there is a plethora of evidence on the beneficialeffect of AFOs in improving of functional mobility andquality of gait as well as decreasing the likelihood of falls inindividuals suffering from a CVA [21 22] Thus individualswith CVA provided with an AFO improved gait parameterssuch as cadence stride length and gait velocity [18 23 24]Moreover improvement in gait velocity that is believed toreflect progress in mobility is often used as a measure ofrecovery after a CVA [20 25 26] and is considered animportant goal of rehabilitation
At the same time the literature on the use of differenttypes of AFOs (especially recently introduced carbon AFOs)to improve ambulation of individuals with CVA is limited Assuch the goals of the study were to investigate the effect ofwalking using the prefabricated carbon AFO in comparisonwith the custompolymer AFO and noAFO and to investigatethe usersrsquo preference in using either the prefabricated carbonAFO or the custom plastic AFO
The results of the current study demonstrated that indi-viduals with acute CVA increased their gait velocity when
6 Rehabilitation Research and Practice
using either C-AFO or P-AFO and as a result the gapbetween ldquonormalrdquo and ldquohemipareticrdquo gait velocity decreasedThese results are in line with the literature reporting a positiveeffect of AFOs on gait velocity of individuals with hemiparesis[9 19 27] Similarly improvements in cadence were associ-ated with the use of an AFO without an AFO patients walkedwith lower cadence as compared to healthy individuals Asimilar positive effect of AFOs on cadence of individuals withhemiparesis was described in the literature [27 28] Sincecadence is the number of steps taken in a certain time theobserved increase in the velocity of gait could be due tochanges in the number of steps per minute Nevertheless theimpact of AFOs on cadence remains inconclusive as somestudies report an improvement in this variable with the AFOuse and others report no significant improvement [22] Thusthere is a need for more studies focused on the investigationof the role of different types of AFOs on gait velocity andcadence An increase in the average stride and step lengthwith either type of AFO was evident in the current study andhas been also reported in the past literature [27 28]
While in general there is a consensus in the literaturethat gait velocity is a powerful indicator of function andprognosis after CVA [26] there is an opinion that gait velocityitself may not be wholly representative of functional mobil-ity and meaningful improvement in performance [29] Toaddress this possible concern we added the 119871-test assessment(that includes rising from a chair two 90-degree turns inopposite directions a 180-degree turn and returning to aseated position) as the task that is indicative of the typesof movements that are required in household ambulationThe outcome of the 119871-test revealed that patients while usingAFOs of either type showed better performance comparedto walking with no AFO Moreover clinically the patientsshowed improvement as the time needed for the completionof the test was shorter when they were provided with eithertype of AFO
The study participants were positive about the use ofAFOs as the majority found it comfortable and felt itimproved their walking particularly the functional aspectssuch as safety and confidence This finding is in line withthe literature reporting that 96 of users felt they walkedbetter with the AFO and found it comfortable [18] Moreoverthe majority of the subjects gave a preference to the custom-made plastic AFOs the subjects perception was about 2 1 infavor of the custom-made plastic AFOThis could be becauseeach plastic AFO was specifically molded and fitted for eachsubject Nevertheless further study is needed to examine thelonger-term effects and the cost-effectiveness of prescribing acustom-made or off-the-shelf AFO for people with CVA
5 Conclusion
Both types of AFO significantly improved gait velocitycadence step length and stride length in patients with acuteCVAThe majority of users preferred the custom-made plas-tic AFO over the prefabricated carbon AFO This outcomeshould be taken into consideration while prescribing AFOsFurther study is needed to examine the longer-term effects
and the cost-effectiveness of prescribing different types ofAFO for people with CVA
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] V L Roger A S Go D M Lloyd-Jones et al ldquoHeart diseaseand stroke statisticsmdash2011 update a report from the AmericanHeart Associationrdquo Circulation vol 123 no 4 pp e18ndashe2092011
[2] M Kelly-Hayes J T Robertson J P Broderick et al ldquoTheAmerican heart association stroke outcome classificationrdquoStroke vol 29 no 6 pp 1274ndash1280 1998
[3] C Detrembleur F Dierick G Stoquart F Chantraine andT Lejeune ldquoEnergy cost mechanical work and efficiency ofhemiparetic walkingrdquo Gait amp Posture vol 18 no 2 pp 47ndash552003
[4] N Wada M Sohmiya T Shimizu K Okamoto and K Shi-rakura ldquoClinical analysis of risk factors for falls in home-livingstroke patients using functional evaluation toolsrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1601ndash1605 2007
[5] S E Lord K McPherson H K McNaughton L Rochesterand M Weatherall ldquoCommunity ambulation after stroke howimportant and obtainable is it and what measures appearpredictiverdquo Archives of Physical Medicine and Rehabilitationvol 85 no 2 pp 234ndash239 2004
[6] J F Lehmann S M Condon R Price and B J deLateurldquoGait abnormalities in hemiplegia their correction by ankle-foot orthosesrdquo Archives of Physical Medicine and Rehabilitationvol 68 no 11 pp 763ndash771 1987
[7] H Beckerman J Becher G J Lankhorst and A L M VerbeekldquoWalking ability of stroke patients efficacy of tibial nerveblocking and a polypropylene ankle-foot orthosisrdquo Archives ofPhysical Medicine and Rehabilitation vol 77 no 11 pp 1144ndash1151 1996
[8] D C M de Wit J H Buurke J M M Nijlant M J IJzermanand H J Hermens ldquoThe effect of an ankle-foot orthosison walking ability in chronic stroke patients a randomizedcontrolled trialrdquo Clinical Rehabilitation vol 18 no 5 pp 550ndash557 2004
[9] M Franceschini M Massucci L Ferrari M Agosti and CParoli ldquoEffects of an ankle-foot orthosis on spatiotemporalparameters and energy cost of hemiparetic gaitrdquo Clinical Reha-bilitation vol 17 no 4 pp 368ndash372 2003
[10] N Rao G Chaudhuri D Hasso et al ldquoGait assessment duringthe initial fitting of an ankle foot orthosis in individuals withstrokerdquo Disability and Rehabilitation Assistive Technology vol3 no 4 pp 201ndash207 2008
[11] S Roehrig andDA Yates ldquoCase report effects of a neworthosisand physical therapy on gait in a subject with longstandinghemiplegiardquo Journal of Geriatric Physical Therapy vol 31 no1 pp 38ndash46 2008
[12] H B Kitaoka X M Crevoisier K Harbst D Hansen BKotajarvi and K Kaufman ldquoThe effect of custom-made bracesfor the ankle and hindfoot on ankle and foot kinematics and
Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005

6 Rehabilitation Research and Practice
using either C-AFO or P-AFO and as a result the gapbetween ldquonormalrdquo and ldquohemipareticrdquo gait velocity decreasedThese results are in line with the literature reporting a positiveeffect of AFOs on gait velocity of individuals with hemiparesis[9 19 27] Similarly improvements in cadence were associ-ated with the use of an AFO without an AFO patients walkedwith lower cadence as compared to healthy individuals Asimilar positive effect of AFOs on cadence of individuals withhemiparesis was described in the literature [27 28] Sincecadence is the number of steps taken in a certain time theobserved increase in the velocity of gait could be due tochanges in the number of steps per minute Nevertheless theimpact of AFOs on cadence remains inconclusive as somestudies report an improvement in this variable with the AFOuse and others report no significant improvement [22] Thusthere is a need for more studies focused on the investigationof the role of different types of AFOs on gait velocity andcadence An increase in the average stride and step lengthwith either type of AFO was evident in the current study andhas been also reported in the past literature [27 28]
While in general there is a consensus in the literaturethat gait velocity is a powerful indicator of function andprognosis after CVA [26] there is an opinion that gait velocityitself may not be wholly representative of functional mobil-ity and meaningful improvement in performance [29] Toaddress this possible concern we added the 119871-test assessment(that includes rising from a chair two 90-degree turns inopposite directions a 180-degree turn and returning to aseated position) as the task that is indicative of the typesof movements that are required in household ambulationThe outcome of the 119871-test revealed that patients while usingAFOs of either type showed better performance comparedto walking with no AFO Moreover clinically the patientsshowed improvement as the time needed for the completionof the test was shorter when they were provided with eithertype of AFO
The study participants were positive about the use ofAFOs as the majority found it comfortable and felt itimproved their walking particularly the functional aspectssuch as safety and confidence This finding is in line withthe literature reporting that 96 of users felt they walkedbetter with the AFO and found it comfortable [18] Moreoverthe majority of the subjects gave a preference to the custom-made plastic AFOs the subjects perception was about 2 1 infavor of the custom-made plastic AFOThis could be becauseeach plastic AFO was specifically molded and fitted for eachsubject Nevertheless further study is needed to examine thelonger-term effects and the cost-effectiveness of prescribing acustom-made or off-the-shelf AFO for people with CVA
5 Conclusion
Both types of AFO significantly improved gait velocitycadence step length and stride length in patients with acuteCVAThe majority of users preferred the custom-made plas-tic AFO over the prefabricated carbon AFO This outcomeshould be taken into consideration while prescribing AFOsFurther study is needed to examine the longer-term effects
and the cost-effectiveness of prescribing different types ofAFO for people with CVA
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] V L Roger A S Go D M Lloyd-Jones et al ldquoHeart diseaseand stroke statisticsmdash2011 update a report from the AmericanHeart Associationrdquo Circulation vol 123 no 4 pp e18ndashe2092011
[2] M Kelly-Hayes J T Robertson J P Broderick et al ldquoTheAmerican heart association stroke outcome classificationrdquoStroke vol 29 no 6 pp 1274ndash1280 1998
[3] C Detrembleur F Dierick G Stoquart F Chantraine andT Lejeune ldquoEnergy cost mechanical work and efficiency ofhemiparetic walkingrdquo Gait amp Posture vol 18 no 2 pp 47ndash552003
[4] N Wada M Sohmiya T Shimizu K Okamoto and K Shi-rakura ldquoClinical analysis of risk factors for falls in home-livingstroke patients using functional evaluation toolsrdquo Archives ofPhysical Medicine and Rehabilitation vol 88 no 12 pp 1601ndash1605 2007
[5] S E Lord K McPherson H K McNaughton L Rochesterand M Weatherall ldquoCommunity ambulation after stroke howimportant and obtainable is it and what measures appearpredictiverdquo Archives of Physical Medicine and Rehabilitationvol 85 no 2 pp 234ndash239 2004
[6] J F Lehmann S M Condon R Price and B J deLateurldquoGait abnormalities in hemiplegia their correction by ankle-foot orthosesrdquo Archives of Physical Medicine and Rehabilitationvol 68 no 11 pp 763ndash771 1987
[7] H Beckerman J Becher G J Lankhorst and A L M VerbeekldquoWalking ability of stroke patients efficacy of tibial nerveblocking and a polypropylene ankle-foot orthosisrdquo Archives ofPhysical Medicine and Rehabilitation vol 77 no 11 pp 1144ndash1151 1996
[8] D C M de Wit J H Buurke J M M Nijlant M J IJzermanand H J Hermens ldquoThe effect of an ankle-foot orthosison walking ability in chronic stroke patients a randomizedcontrolled trialrdquo Clinical Rehabilitation vol 18 no 5 pp 550ndash557 2004
[9] M Franceschini M Massucci L Ferrari M Agosti and CParoli ldquoEffects of an ankle-foot orthosis on spatiotemporalparameters and energy cost of hemiparetic gaitrdquo Clinical Reha-bilitation vol 17 no 4 pp 368ndash372 2003
[10] N Rao G Chaudhuri D Hasso et al ldquoGait assessment duringthe initial fitting of an ankle foot orthosis in individuals withstrokerdquo Disability and Rehabilitation Assistive Technology vol3 no 4 pp 201ndash207 2008
[11] S Roehrig andDA Yates ldquoCase report effects of a neworthosisand physical therapy on gait in a subject with longstandinghemiplegiardquo Journal of Geriatric Physical Therapy vol 31 no1 pp 38ndash46 2008
[12] H B Kitaoka X M Crevoisier K Harbst D Hansen BKotajarvi and K Kaufman ldquoThe effect of custom-made bracesfor the ankle and hindfoot on ankle and foot kinematics and
Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005

Rehabilitation Research and Practice 7
ground reaction forcesrdquo Archives of Physical Medicine andRehabilitation vol 87 no 1 pp 130ndash135 2006
[13] A Slijper A Danielsson and C Willen ldquoAmbulatory functionand perception of confidence in persons with stroke with acustom-made hinged versus a standard ankle foot orthosisrdquoRehabilitation Research and Practice vol 2012 Article ID206495 6 pages 2012
[14] CNeville and JHouck ldquoChoosing among 3 ankle-foot orthosesfor a patient with stage II posterior tibial tendon dysfunctionrdquoJournal of Orthopaedic amp Sports PhysicalTherapy vol 39 no 11pp 816ndash824 2009
[15] A Dogan M Mengulluoglu and N Ozgirgin ldquoEvaluation ofthe effect of ankle-foot orthosis use on balance and mobility inhemiparetic stroke patientsrdquo Disability and Rehabilitation vol33 no 15-16 pp 1433ndash1439 2011
[16] Standards ldquoAFO ModificationFabricationStandardsrdquo 2012httpwwwaopsolutionscomformsafo modification formpdf
[17] S S Kuys S G Brauer and L Ada ldquoTest-retest reliabilityof the GAITRite system in people with stroke undergoingrehabilitationrdquo Disability and Rehabilitation vol 33 no 19-20pp 1848ndash1853 2011
[18] S F Tyson and H A Thornton ldquoThe effect of a hinged anklefoot orthosis on hemiplegic gait objective measures and usersrsquoopinionsrdquo Clinical Rehabilitation vol 15 no 1 pp 53ndash58 2001
[19] H S Jorgensen H Nakayama H O Raaschou J Vive-Larsen M Stoier and T S Olsen ldquoOutcome and time courseof recovery in stroke part II time course of recovery theCopenhagen Stroke Studyrdquo Archives of Physical Medicine andRehabilitation vol 76 no 5 pp 406ndash412 1995
[20] R-Y Wang P-Y Lin C-C Lee and Y-R Yang ldquoGait andbalance performance improvements attributable to ankle-footorthosis in subjects with hemiparesisrdquoThe American Journal ofPhysical Medicine and Rehabilitation vol 86 no 7 pp 556ndash5622007
[21] E Cakar O Durmus L Tekin U Dincer and M Z KiralpldquoThe ankle-foot orthosis improves balance and reduces fall riskof chronic spastic hemiparetic patientsrdquo European Journal ofPhysical and RehabilitationMedicine vol 46 no 3 pp 363ndash3682010
[22] L A Ferreira H P Neto L A Grecco et al ldquoEffect of ankle-foot orthosis on gait velocity and cadence of stroke patients asystematic reviewrdquo Journal of Physical Therapy Science vol 25no 11 pp 1503ndash1508 2013
[23] H Gok A Kucukdeveci H Altinkaynak G Yavuzer andS Ergin ldquoEffects of ankle-foot orthoses on hemiparetic gaitrdquoClinical Rehabilitation vol 17 no 2 pp 137ndash139 2003
[24] H Abe A Michimata K Sugawara N Sugaya and S-I IzumildquoImproving gait stability in stroke hemiplegic patients witha plastic ankle-foot orthosisrdquo Tohoku Journal of ExperimentalMedicine vol 218 no 3 pp 193ndash199 2009
[25] J Perry M Garrett J K Gronley and S J Mulroy ldquoClassifica-tion of walking handicap in the stroke populationrdquo Stroke vol26 no 6 pp 982ndash989 1995
[26] A Schmid P W Duncan S Studenski et al ldquoImprovements inspeed-based gait classifications are meaningfulrdquo Stroke vol 38no 7 pp 2096ndash2100 2007
[27] A Bartonek M Eriksson and E M Gutierrez-Farewik ldquoAnew carbon fibre spring orthosis for children with plantarflexorweaknessrdquo Gait and Posture vol 25 no 4 pp 652ndash656 2007
[28] C Bleyenheuft G Caty T Lejeune and C DetrembleurldquoAssessment of the Chignon dynamic ankle-foot orthosis usinginstrumented gait analysis in hemiparetic adultsrdquo Annales deReadaptation et de Medecine Physique vol 51 no 3 pp 154ndash160 2008
[29] S E Lord and L Rochester ldquoMeasurement of communityambulation after stroke current status and future develop-mentsrdquo Stroke vol 36 no 7 pp 1457ndash1461 2005