Embed Size (px)
Citation preview

Thorax (1962), 17, 310.
THE EFFECT OF SYMPATHECTOMY, VAGOTOMY, ANDOESOPHAGEAL INTERRUPTION ON THE CANINE
GASTRO-OESOPHAGEAL SPHINCTERBY
RICHARD K. GREENWOOD,* JERRY F. SCHLEGEL, CHARLES F. CODE,AND F. HENRY ELLIS, Jr.
From the Mayo Clinic and Mayo Foundation, Rochester, Minnesota, U.S.A.
The nature of the control of the gastro-oesophageal sphincter is obscure. It has beenthought to be under the regulation of theautonomic nervous system so that through theinfluences of the vagus and sympathetic nervesthe resting tone is maintained and relaxation andcontraction are initiated. Beyond this broadgeneralization, however, there is considerabledivergence of opinion as to the precise functionof the various nervous elements and their inter-relationships.The purpose of this investigation was to deter-
mine the effect of certain nerve and oesophagealinterruption procedures on the resting tone of thesphincter and its relaxation and contraction duringswallowing.
REVIEW OF THE LITERATUREA comprehensive review of the work of previous
investigators in this field is given by Ingelfinger(1958) in his treatise on oesophageal motility.Most studies have involved stimulation or destruc-tion of the vagus and sympathetic nerves. Theusual methods of observation have been mano-metric estimations and radiological examination.
All workers agree that the vagus has someinfluence in the lower end of the oesophagus.Many believe that the vagus exerts both inhibitoryand motor actions on the sphincter, and it hasbeen suggested that these impulses travel bydifferent routes. Openchowski (1889) postulatedthe existence of a distinct ' dilator cardiac ' nervein man. This has not been re-identified, butZeller and Burget (1937) suggested that in the doginhibitory impulses left the cervical vagus andtravelled down the wall of the oesophagus, eitherby way of vagal fibres or by propagation in theintramural plexus. Support for this concept wasprovided by Grondahl and Haney (1940) and by
'Recipient of a travelling fellowship from the Wellcome Trust.Present address: St. Thomas' Hospital, London.
Lehmann (1945), who interrupted these impulsesin dogs by oesophageal section.
Although unilateral and supradiaphragmaticbilateral vagotomy are without effect on thedog's inferior gastro-oesophageal sphincter, highbilateral section has been shown to cause anarrowing of the lower part of the oesophagus(Zeller and Burget, 1937; Hwang, Essex, andMann, 1947). Cannon (1907) showed that inthe cat the lower part of the oesophagus wasstill capable of peristalsis even after bilateralvagotomy.The role of the sympathetic system is disputed.
Knight (1934) concluded that sympathetic andvagal nerves were antagonistic in their action onthe cat's gastro-oesophageal sphincter and thatthe resting tone of the latter was maintained bythe sympathetics. Carlson, Boyd, and Pearcy(1922), working on a variety of animals, suggestedthat it was the state of muscular tone at the timeof stimulation which determined the response tosympathetic and vagal stimulation. Alnor andOhnesorge (1958) showed that sympatheticstimulation in the cat and rabbit caused anincrease in sphincteric tone, but that the cardiawas nevertheless capable of normal function aftersympathectomy. Zeller and Burget (1937) agreedthat sympathectomy was without effect on thesphincter.The possibility that the sphincter might be
partly autonomous has been considered by severalauthors. Kronecker and Meltzer (1883) statedthat in man the lower parc of the oesophagusexhibits spontaneous acti'vity. Cannon (1907)thought that the lower part of the oesophagus,being smooth muscle, was capable of peristalsiswithout an extrinsic innervation. Burget andZeller (1936) showed that sphincteric relaxationin the dog was independent of local extrinsicnervous supply, whereas Alnor and Ohnesorge(1958) thought that the lower portion of the
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

SYMPATHECTOMY, VAGOTOMY, AND OESOPHAGEAL INTERRUPTION
oesophagus possessed intrinsic tone which wasinhibited by the vagus.
Interpretation of these findings is difficult. AsIngelfinger (1958) pointed out, devices which havebeen used for the study of sphincteric motilitymay themselves distort the normal pattern bytheir very presence. However, the work reportedin the literature suggests that the lower portionof the oesophagus is under vagal control, inhibi-tion being mediated by impulses transmittedintramurally.More recently, Carveth, Schlegel, Code, and
Ellis (1962) studied dogs and employed mano-metric methods. They found that bilateral sub-hilar vagotomy reduced both the resting tone ofthe sphincter and the incidence of relaxation inresponse to deglutition.The present investigation was undertaken to
test the action of the gastro-oesophageal sphincterafter sympathetic denervation, after sympatheticdenervation combined with vagotomy, or aftervarious oesophageal interruption procedures.
METHODSHealthy adult mongrel dogs weighing 10 to 15 kg.
were used. The dogs were trained to lie quietly duringradiological and manometric studies so that no anaes-thesia was necessary.
Fluoroscopic and cineradiographic studies of theoesophagus and gastro-oesophageal sphincteric regionwere carried out on intact dogs and on all those whohad undergone some form of oesophageal interruption.The study was made after the instillation of 30 ml.of contrast medium (Micropaque) into the oesophagusthrough a catheter.The methods used for the manometric studies were
similar to those previously described by Schlegel andCode (1958). Intraluminal pressures were detected bythree or four small-calibre water-filled polyethylenetubes connected proximally to strain gauges (Statham,Model P-23De) and recorded photokymographically.The open tip of the distal tube was covered with asmall latex balloon 5 mm. in diameter, as describedby Code and Schlegel (1958), and lateral orifices werecut in each of the other tubes at intervals of 5 cm.(Fig. 1). During tests the balloon and all the tubes werefilled with water and connected to externally placedpressure transducers. To achieve some degree ofrigidity, a fine wire within an extra tube was incor-porated into the unit. Pressures were recorded underresting conditions at intervals of 0.5 cm. as the tubeswere withdrawn from the stomach through the gastro-oesophageal sphincter region and into the oesophagus.Responses to deglutition initiated by the injection of asmall quantity of water into the pharynx were alsorecorded at similar intervals through the sphincter.Respiratory movements were recorded by a beltpneumograph fastened around the thorax of eachanimal and connected to another strain gauge.
1cm.
FIG. 1. Pressure-detecting probes employed in mano-metric studies. The arrows indicate the lateral orificesof the tubes referred to as open-tip tubes.
ANALYSIS OF RECORDS.-Analysis of the manometricrecords was basically the same as that described byFyke, Code, and Schlegel (1956). The restingpressures were measured at end-expiratory and end-inspiratory phases of respiration and referred to meangastric fundic pressures, which were arbitrarily desig-nated as zero. The point on inspiration where thepressure deflection changed from positive to negativewas noted and referred to as the "respiratoryreversal" point. When more than one test was carriedout on any dog the mean values were calculated. In agroup of dogs which had undergone the same pro-cedure, the mean, standard deviation, and standarderror of the mean were calculated. Differencesbetween pre-operative and post-operative values werecompared statistically using Student's t test for thesignificance of the differences (Fisher, 1930).
Duration, maximal amplitude, and time from theinstant of swallowing to the onset and the peak ofdeglutitive responses were measured. In addition, theincidence of sphincteric relaxation and contraction inresponse to swallowing was determined in the pre-operative and post-operative studies.OPERATIVE PROCEDURES.-A11 operative procedures
were carried out with the animal under etheranaesthesia.
Radical Sympathectomy.-In seven dogs an exten-sive sympathetic denervation of the cardiac end of thestomach, including the gastro-oesophageal sphinctericzone, was effected. Through a left thoraco-abdominalapproach the left thoracic sympathetic chain andganglia were removed from the level of the eighthrib to the diaphragm. The solitary splanchnic nervearising from the chain at the level of the thirteenthrib also was removed. The right sympathetic chainwas exposed by mobilizing the aorta; it was dividedand a strip 2 cm. wide was excised from its lowerthoracic part. The right and left coeliac ganglia,which were enmeshed in a plexus of sympatheticnervous tissue around the coeliac artery, were removedand the adventitia was stripped from the vessel andfrom the proximal few centimetres of its three
311
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

RICHARD K. GREENWOOD AND OTHERS
branches. The left gastric artery was divided nearits origin to interrupt any nerve fibres which hadescaped the above ablations (Fig. 2 A, A', B, C).Other Sympathetic Denervations.-In one dog,
division of the left gastric artery was combined withgastric transection 2 cm. below the gastro-oesophagealsphincter (Fig. 2 C, D). Gastric transection wasperformed to cut any sympathetic fibres within thestomach wall. It was also carried out as a secondarymanoeuvre in one of the dogs on which sympathec-tomy had been performed previously (Fig. 2 D).Sympathectomy and Vagotomy.-At a second stage,
in four of the sympathectomized dogs a bilateralsubhilar thoracic vagotomy was done through a rightthoracotomy approach (Fig. 2 E, E). At this secondoperation it was confirmed that the right sympatheticchain had been interrupted. The remainder of thechain and splanchnic nerve were removed down tothe diaphragm (Fig. 2 A').
Oesophageal Interruption.-Three varieties of oeso-phageal interruption were used. A low oesophagealtransection 0.5 cm. above the sphincter was performedin one dog (Fig. 3 A). In another animal a 21 to 3 cm.segment of jejunum on its vascular pedicle was raisedinto the thorax and inserted antiperistaltically intothe lower part of the oesophagus by two end-to-endanastomoses after excision of an appropriate segmentof oesophagus (Fig. 3 B). In both of these animalsa vagal oesophageal branch was resected to permit ofadequate mobilization of the oesophagus.
In the remaining six dogs of this series, an artificialprosthesis was inserted into the lower part of theoesophagus (Fig. 3 C). Two types of prosthesis wereused: one was made of an outer layer of knitted,crimped Teflon and an inner layer of Silastic; theother was made of two layers of crimped Teflon.The prostheses were of varying lengths (1 to 5 cm.)
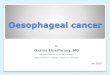
FIG. 2. Diagram of denervation procedures: A and A',removal of thoracic sympathetic chain and gangliawithin area indicated by bracket; B, splanchnicec-tomy and coeliac gang.ionectomy; C, division of leftgastric artery; D, gastric transection; E and E',subhilar bilateral vagotomy.
SITE OFTRANSECTION
A BFIG. 3. Diagram of oesophageal interruption procedures: A, oesophageal transection; B, jejunal
prosthesis; and C, artificial prosthesis.
312
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

SYMPA THECTOMY, VAGOTO VM Y, AND OESOPHAGEA L INTERRUPTION 313
and were inserted at different levels in the lower partof the oesophagus, appropriate segments of the latterbeing removed to accommodate them. The prostheseswere inserted with two end-to-end anastomoses andwith varying degrees of vagal resection from minimaloesophageal branch division to total bilateral subhilarvagotomy.
RESULTSCONTROL OBSERVATIONS. - During the pre-
operative period the dogs were healthy, had nodysphagia, and did not lose weight.
O TIETP _ /W\iA
*OPEN-TIP~~~~~~~t I. , |{ sJ 'A,
BALLOON + i
Stomach
No dilatation of the oesophagus was seen inthe cineradiograph of any of the intact dogs, andin each the radio-opaque material reached thelower end of the oesophagus rapidly and passedthrough the sphincter without delay (Fig. 4).
Resting manometric studies were performed on31 intact dogs, each having one or more tests.As the units were withdrawn from the stomach tothe oesophagus, the gastro-oesophageal sphincterwas always identified as a zone of raised pressure(Figs. 4 and 5).
TING
K++ , t
I
11
I=50 cm.H20 Press,re
Sphinc ter21 seconds Esophagus
DEGLUTI TION
PO'SION OF UNITS:
OPEN -IP
OPEN - TIP-
BALLOONSPHINCTERE
OPEN- TIP
p
--'F.I~~~.
)PEN-TIP
BALLOONzPHINCTER 'V0
Swaliow
xneumogroph
FIG. 4. Resting and deglutition pressures at the gastro-oesophageal sphincter ofan intact dog. Upperpanel: Resting pressure detected by an open-tip and balloon-tip tube: (+) increase ofpressurewith inspiration; (-) decrease ofpressure with inspiration; each upright arrow signifies a 0.5 cm.
oral withdrawal ofthe detecting units as they were withdrawn from the stomach into the oesophagus.Note the sharp change in the direction of the pressure swingsfrom (+) to (-) with inspiration andthe distinct rise ofpressure as the units passed through the sphincter. Lower right panel: Pressurechanges after deglutition. Note the peristaltic sequence in the oesophagus and that the pressurein the sphincter declines and remains lowered until the wave ofdeglutition reaches it; the sphincterthen closes with a prolonged contraction. Lower left panel: No evidence ofdelay in the passageof the contrast medium through the oesophagus or sphincter was noted.
z
S~
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

RICHARD K. GREENWOOD AND OTHERS
Deglutition studies were made on 12 dogs.Each swallow was followed by a sphinctericresponse of relaxation followed by a phase ofcontraction (Fig. 4). Relaxation commenced 2.6sec. after deglutition, lasted 7.8 sec., and wasfollowed by a phase of contraction lasting 6.9 sec.(mean values).
POST-OPERATIVE OBSERVATIONS.-Studies weremade as early as 24 hours and as late as sixmonths after operation; the majority, however,were carried out during the first three post-operative weeks.RADICAL SYMPATHECTOMY.-Seven dogs were
studied after radical sympathectomy. Theirclinical post-operative course was withoutincident; they remained well for a significantperiod and eventually were studied after furtherinterruption procedures.The resting pressure profile of the gastro-oeso-
phageal sphincter and its responses to swallowing
LuJ
Uf)(I)
LuJ
C)jev
20
0
-20
60
LaiU:
cLU=
2:
40
20
0
-20
Open - Tip (3/ Dogs)
4 3 2 1 2 3 4 5cm. below cm. above
Res pirotoryReversol
FIG. 5. Mean resting pressure profile of the gastro-oesophageal junction of 31 intact dogs. o- j=mean and S.E. of mean.
were not affected significantly by sympathectomy(Fig. 6, left).OTHER SYMPATHECTOMY PROCEDURES. -The
clinical course and results of the manometric testsin the two dogs that had an upper gastric tran-section were essentially the same as those in thelarger sympathectomy series. Neither the restingprofile nor the responses of the sphincter todeglutition were altered by the operation.SYMPATHECTOMY AND VAGOTOMY. -Bilateral
subhilar vagotomy was performed in four of thesympathectomized dogs. After vagotomy all ofthe animals regurgitated food and lost weight.Manometric studies revealed a definite band of
raised pressure persisting between the stomachand the oesophagus in each of the four dogs (Fig.6, right). The amplitude of the resting pressurein the sphincter, however, was less than before thevagotomy. In contrast, the resting pressures inthe lower part of the oesophagus were increasedafter vagotomy.
Deglutition studies after vagotomy showed thatthe sphincter still relaxed and contracted (Fig. 6,right), but the incidence of these responses,particularly relaxation, was reduced. The rangeof the pressure changes during those responseswhich did occur was normal. The onset ofcontraction in the sphincter above the level ofthe hiatus was premature, and the duration andamplitude were reduced, the alteration as detectedby open tip being highly significant (P>0.01).While the animals were still healthy, each was
given an overdose of anaesthetic and necropsywas performed. The oesophagus of each animalwas found to be dilated, and this dilatation prob-ably accounted for the increased resting pressurein the lower part of the oesophagus.OESOPHAGEAL INTERRUPTION PROCEDURES.
Clinically, all dogs that had undergone some formof oesophageal interruption exhibited markeddysphagia with regurgitation of food. At necropsyorganic stricture was not found at the site ofoperation in the dogs that had undergone tran-section or in those with jejunal transplant. Oneof the dogs with an artificial prosthesis survivedfor several months. At necropsy no sign of theprosthesis could be found. A stricture 1 cm. indiameter had developed at the site of its insertion.
In the cineradiographic studies, the animal thathad undergone low transection showed retentionof contrast medium in the lower part of theoesophagus without dilatation (Fig. 7). Thesphincter did relax from time to time, allowingpassage of material into the stomach. In theanimal with a jejunal transplant, obstruction
314
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

SYMPATHECTOMY, VAGOTOMY, AND OESOPHAGEAL INTERRUPTION
SwollowPneumograph
FIG. 6. Resting and deglutition pressures at the gastro-oesophageal sphincter after sympathectomyand sympathectomy plus bilateral subhilar vagotomy. Left panels: Sympathectomy alone waswithout effct upon the resting pressure and deglutition response of the sphincter. Right panels:After the addition of vagotomy the resting pressure at the sphincter was lowered and that in theoesophagus raised. With deglutition oesophageal complexes were simultaneous. Note, however,that the sphincter relaxed. The pattern is similar to that after vagotomy alone.
developed at the site of the transplant and alsoat the site of the gastro-oesophageal sphincter.The oesophagus proximal to each was dilated.Continuous tonic activity in the jejunum andconsiderable delay in the lower part of theoesophagus were noted before the sphincterrelaxed to allow emptying (Fig. 8). In each dogwith an artificial prosthesis, no delay in thepassage of contrast medium was seen at the levelof the prosthesis but considerable delay occurredin the lower part of the oesophagus where thedegree of dilatation was variable (Fig. 9). Thesphincter in these dogs also relaxed from time totime to allow oesophageal emptying.
Manometric findings were the same in this seriesof dogs as in the animals that had undergone
vagotomy. The resting pressure of the gastro-oesophageal sphincter was reduced and that inthe oesophagus just proximal to the sphincterwas increased (Figs. 7, 8, and 9). Sphinctericresponses to deglutition also were reduced,particularly relaxation. The responses which didoccur were qualitatively normal with the exceptionof suprahiatal contraction, which was diminished.
DISCUSSIONAlthough the sympathetic innervation of the
canine gastro-oesophageal sphincter is not welldefined, it is said to arise from below thediaphragm, originating in the coeliac ganglionand being distributed via the coeliac plexus alongthe trunk and terminal branches of the left gastric
315
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

RICHARD K. GREENWOOD AND OTHERS
? ES TING
Lj/'~~~~~~~~~~~~~~~~~,^^ChA
;;)<-^ Jh
R e S 7
1'
DEGLUL FT/ON
III
OPEK5 - v/
'Is
(iREDv
BA, O);j
FIG. 7. Pressures at the gastro-oesophageal junction after transection and resuture of the lower partofthe oesophagus. Upper right panel: Resting pressure profile contains a zone ofraisedpressurenormal in amplitude andcontour. Lower rightpanel: With deglutition aperistaltic wave traversedtheoesophagus and nonnal relaxation occurred within the sphincteric region. Lower leftpanel: A radio-graph revealed evidence ofdelay in thepassage of the radio-opaque material through the oesophagus.
artery (Knight, 1934; Alnor and Ohnesorge, 1958;McCrea, 1926; and Mizers, 1955). Coeliacganglionectomy combined with left gastric divisionshould interrupt these fibres; however, in thisstudy a more radical procedure was performed toensure the severance of all sympathetic fibres to thesphincteric zone. In addition to coeliac ganglion-ectomy, interruption and removal of both lowerthoracic sympathetic chains and splanchnic nerveswere performed. To divide any possible fibreswithin the stomach wall which might have escapedthe other ablations, the upper part of the stomachwas transected at a later stage in one dog, and
this latter procedure was combined with leftgastric division in another animal. These sympa-thetic denervations did not affect the function ofthe canine gastro-oesophageal sphincter, and theconclusion is justified that this sphincter operatesindependently of the sympathetic nervous system.The effect of vagotomy at different levels on
the gastro-oesophageal sphincter has recently beenstudied by Carveth and associates (1962) by meansof a similar manometric technique. They showedthat whereas bilateral subhilar vagotomy loweredthe resting sphincteric pressure barrier between thestomach and the oesophagus and altered its
316
.-
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

SYMPATHECTOMY, VAGOTOMY, AND OESOPHAGEAL INTERRUPTION
RESTING
= 50 cm.H20 Pressure
+
BALLOON 30 seconds+A
' ~~SphincferPneumogra h jun=it-
SWAgnol I 4I M-__
DEGLUrI TION
OPEN-TIP
OPEN -
J 1~~TI
IBALLOON 1A
SPHINCTER Vv
Swllow 5 seconds
Pneumograph
FIG. 8. Intraluminal pressures after interposing a segment of jejunum into the distal oesophagus.Upper panel: Resting pressures. Note the raised pressure at the sphincter and the rhythmicalcontractions occurring in the jejunum at a rate of 14 to 15 waves/min. Lower right panel: Withdeglutition the pressures in the oesophagus andjejunum increased simultaneously while the pressureof the sphincter declined. Lower mid panel: Contrast radiography revealed a dilated oesophagusabove and below thejejunal segment with considerable retention ofMicropaque. Note the narrowedsegment ofjejunum.
responses to deglutition, cervical vagotomy com-pletely abolished the zone of raised pressure andeliminated all response to deglutition. An explana-tion for these findings could be that fibres in thecervical vagi leave these nerves above the hilumof the lung and travel to the gastro-oesophagealsphincter by a different route, possibly via thesympathetic system.
In the present study, bilateral subhilar vago-tomy was combined with radical sympathectomy.In theory this procedure should eliminate allextrinsic autonomic nervous supply to the gastro-oesophageal sphincter and should reveal whetherthe action of the vagus is in any way dependent onthe integrity of the sympathetic system. Bilateral
subhilar vagotomy in animals that had alreadyundergone sympathectomy produced resultssimilar to or identical with those previouslyreported for bilateral subhilar vagotomy alone.The dogs suffered from dysphagia and regurgita-tion. Manometrically, the resting sphinctericpressure was reduced but not eliminated. Theincidence of sphincteric responses to deglutitionwas reduced, but those that occurred were normalexcept for diminished contraction above thehiatus. Thus sphincteric function was notabolished by the combination of sympathectomywith subhilar vagotomy. This result forces theconclusion that other nerve fibres must reach thesphincteric area by routes not affected by these
IM- 0--- 1---- mommimm
317
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

RICHARD K. GREENWOOD AND OTHERS
RES TING
PEGL; T.' Otv
I)PENV-T!
OPEN. F
PHALNCuvrvISPHIA/NC
'4
FIG. 9. A segment of oesophagus is replaced by an artificial prosthesis. Upper panel: Restingpressure profile contains a zone of raised pressure which is within normal limits. Lower rightpanel: With deglutition, aperistaltic contractionprogressed through the oesophagus and thesphincterrelaxed and contracted normally. Lower mid panel: Some retention of contrast medium andslight dilatation of the oesophagus are evident radiographically. The prosthesis is clearly defined.
ablative procedures or else the gastro-oesophagealsphincter enjoys a considerable degree ofautonomy.A possible additional route of access of extrinsic
nerve fibres to the sphincter is down and in thewall of the oesophagus, either as actual nervesor as propagated impulses within the intramuralplexuses. Such a route has been proposed byZeller and Burget (1937). Oesophageal transectionwould be an effective method of interrupting suchnerve fibres or impulses. This has been performedalone or in combination with vagotomy withdivergent results. Grondahl and Haney (1940)and Carveth and associates (1962) found musclegirding or transection alone to be without effect.Lehmann (1945) noted that it abolished sphinctericrelaxation. When thoracic vagotomy was added
to the procedure, Grondahl and Haney (1940)found that sphincteric relaxation was prevented,but Carveth and associates (1962) noted thatrelaxation persisted. In the present study, oeso-phageal transection was performed as low aspossible in order to achieve maximal isolation ofthe sphincter and to remove any immediatelyproximal oesophageal segment in which a peristalticwave might be initiated. The regurgitation,delay in the radiograph, and manometric findingswhich this dog showed were undoubtedly attribut-able to the interruption of the vagal branch whichaccompanied the transection. The sphincter itselfbehaved nearly normally.
In view of the possibility that a peristaltic impulsemight " jump" across a short area at the site of asimple transection, or that the severed nerve and
318
!A ., 1, p, , t j. ., p
I '. 4 AV,
-) ." q _r
'r zi i .-. n
A"
..
:..!..4%
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from

SYMPATHECTOMY, VAGOTOMY, AND OESOPHAGEAL INTERRUPTION
muscle fibres might quickly reunite, it was decidedto excise a segment of oesophagus and interposea prosthesis in order to interrupt oesophagealcontinuity more effectively. A living autograft,a segment of jejunum, was chosen initially. It wasinserted retrogradely so that the jejunum would beworking in the opposite direction to oesophagealperistalsis. The clinical course, cineradiographicstudies, and necropsy findings showed that thisoccurred, there being a functional obstruction atthe level of the prosthesis for which no organiccause could be found. Apart from the obstructionso induced, the findings in this animal were similarto those found in the low transection, a band ofraised pressure capable of relaxation still persistingin the sphincteric region.As a final stage in this series of experiments a
foreign rigid prosthesis was interposed in theoesophagus to effect the interruption, thuseliminating any remote possibility of "reverseperistalsis " that might have been established in theliving autograft. Differing degrees of coincidentvagotomy also were affected; in some cases onlyminimal division of oesophageal branch resectionwas performed, in others total bilateral subhilarvagotomy was carried out. Therefore, the effectof these vagal interruptions was added to thepresence of the prosthesis. The findings in thesedogs were the same as in those with vagal inter-ruption alone, namely, oesophageal delay, reducedresting sphincteric pressure, and a sphincter thatrelaxed and contracted with relatively normalcharacter but reduced incidence.From the observations made on these animals,
the concept that complete control of the gastro-oesophageal sphincter is mediated by nerve fibresor impulses coursing for some distance down thewall of the oesophagus is no longer tenable. Theseresults combined with those of the denervationstudies suggest that the gastro-oesophagealsphincter can function in the absence of extrinsicnerve supply. The data indicate that while thereis no doubt that the vagus nerve exerts someinfluence over the canine gastro-oesophagealsphincter, the sphincter nevertheless enjoys adegree of autonomy that is independent of anylocal extrinsic nerve supply. Such a hypothesisis not new (Kronecker and Meltzer, 1883;Cannon, 1907; Burget and Zeller, 1936; andAlnor and Ohnesorge, 1958); our data simplystrengthen its likely truth. Why and how thedenervated sphincter maintains an inherent restingtone is obscure, but it is possible that the occur-rence of relaxation, when a bolus presents fromabove, may be mediated by the local autonomic
nerve plexuses within the structure of the sphinc-teric region itself, perhaps stimulated by thedistending force of the bolus (Creamer andSchlegel, 1957). Alternatively, the action may bea property of the sphincteric musculature.
SUMMARYThe effect of certain nerve and oesophageal
interruption procedures on the function of thecanine gastro-oesophageal sphincter has beenstudied clinically, radiographically, and, moreparticularly, by manometric determination ofoesophageal and sphincteric motility, both in theresting phase and on deglutition.
Radical sympathetic extirpation was withouteffect.
Radical sympathetic extirpation combined withbilateral subhilar vagotomy has an effect similarto that of subhilar vagotomy alone, that is,diminution of resting sphincteric tone with reducedincidence of sphincteric response to deglutition,particularly relaxation.
Various oesophageal interruptions and inter-positions have a relatively minor effect on thesphincter, the changes depending entirely on thedegree of concomitant vagotomy carried out.A band of raised pressure capable of relaxation
and contraction persisted in the sphincteric areaafter all of these procedures. The conclusion hasbeen drawn that the canine gastro-oesophagealsphincter can relax and contract in co-ordinationwith swallowing independently of local extrinsicnerves and that it thus enjoys a considerabledegree of autonomy.
This investigation was supported in part by researchgrants A-2015 and A-5457 from the National Institutesof Health, U.S. Public Health Service.
REFERENCESAlnor, P .C., and Ohnesorge, F. K. (1958). Z. ges. exp. Med., 129, 51 1.Burget,G. E., and Zeller, W. E. (1936). Proc. Soc. exp. Biol. (N.Y.),
34,433.Cannon, w. B. (1907). Amer. J. Physiol., 19,436.Carlson, A. J., Boyd, T. E., and Pearcy, J. F. (1922). Amer. J.
Physiol., 61, 14.Carveth. S. W., Schlegel, J. F., Code, C. F., and Ellis, F. H., Jr.
(1962). Su.g. Gynec. Obstet., 114, 31.Code, C. F., and Schlegel, J. F. (1958). Proc. Mayo Clin., 33.406.Creamer. B., and Schlegel, J. (1957). J. appl. Phvsiol., 10. 498.Fisher, R. A. (1930). Statistiral Methods for Research Workers, 3rd
ed. Oliver and Boyd, Edinburgh.Fyke, F. E., Jr., Code, C. F., and Schlegel, J. F. (1956). G'zstro-
enterologia, Basel, 86, 135.Grondahl, J. W.. and Haney, H. F. (1940). Proc. Soc. exp. Biol.
(N.Y.), 44, 126.Hwang, Kao, Essex, H. E., and Mann, F. C. (1947). Amer. J.
Physiol., 149, 429.Ingelfinger, F. J. (1958). Physiol. Rev., 38, 533.Knight. G. C. (1934). B-it. J. Surg., 22. 155.Kronecker, H.. and Meltzer, S. J. (1883). Arch. Anat. Physiol.,
Suppl.-Bd. (Physiol. Abt.), p. 328.Lehmann, G. (1945). Amer. J. Physiol., 143, 163.McCrea, E. D'Arcy (1926). Brit. J. Surg.. 13, 621.Mizers, N. J. (1955). Amer. J. Anat., 96, 285.Openchowski, T. von (1889). Arch. Anat. Physiol. (Physiol. Abt.),
p. 549.Schlegel, J. F., and Code, C. F. (1958). Amer. J. Physiol., 193, 9.Zeller, W., and Burget, G.E. (1937). Amer. J. dig. Dis., 4, 113.
319
copyright. on O
ctober 4, 2021 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.17.4.310 on 1 Decem
ber 1962. Dow
nloaded from













![Peripheral Sympathectomy for Raynaud's Phenomenon: A ... · sympathectomy [1–3,6,7]. Conventional cervical sym-pathectomy has been used, but the results are disap-pointing. It has](https://img.dokumen.tips/doc/110x75/602abfd7d9da841d876f1382/peripheral-sympathectomy-for-raynauds-phenomenon-a-sympathectomy-1a367.jpg)