Embed Size (px)
DESCRIPTION
A paper exploring the link between perfectionism and physiological stress.
Citation preview

The effects of experimentally induced stress on anxiety and physiology in high and low perfectionists

Perfectionism and the stress response
Contents
Summary 3
Introduction......................................................................................................................................4
Hypotheses 12
Method 13
Participants.............................................................................................................................13
Apparatus...............................................................................................................................14
Screening Questionnaire................................................................................................14
Frost’s Multidimensional Perfectionism Scale 15
Spielberger’s State Trait Anxiety Inventory 15
Blood pressure monitor 15
Colour-word interference task 16
Procedure 16
Results18
Participant Characteristics 18
Data Analysis 19
State Anxiety 19
Physiological changes 20
Systolic blood pressure..........................................................................................20
Diastolic blood pressure 21
Heart rate................................................................................................................22
Subjective ratings...................................................................................................................23Discussion......................................................................................................................................24
Limitations 25
Future research 27
Conclusion.............................................................................................................................28
References 30
Appendices 34
Word Count: 6,840
2

Perfectionism and the stress response
Summary
A wealth of literature exists on perfectionism and psychological outcomes, especially how
stress mediates this relationship, however there is a lack of research into how perfectionism may
influence the physiological response to stress. A sample of 43 university students was split into two
groups of high and low perfectionists, and the effects of experimentally induced stress were
observed with regards to anxiety and three physiological measures; systolic blood pressure,
diastolic blood pressure and heart rate. It was observed that neither group demonstrated an increase
in state anxiety following the stressful task, but that high perfectionists sustained a significantly
higher level of state anxiety irrespective of the introduction of stress. A significant interaction was
found between perfectionism and condition (resting, task) in relation to systolic blood pressure.
During the stressful condition diastolic blood pressure and heart rate were found to be significantly
increased relative to resting rates, regardless of group (high, low perfectionism). Few significant
differences were observed between high and low perfectionists in subjective measures, including
control, and worry. Further research in this area that has a more natural focus should be actively
encouraged, due to the potentially valuable use of any significant data in an applied healthcare
setting.
3

Perfectionism and the stress response
The effects of experimentally induced stress on anxiety and physiology in high and low perfectionists
Introduction
A large amount of research dedicated to perfectionism and negative outcomes has focused
on co-existing psychological effects; to date little attention has been paid to the potential
relationship that exists between perfectionism and physiological outcomes, specifically in relation
to stress. This research therefore has the following aims; to elaborate on the form that this
relationship could take by means of linking perfectionism to psychological and resulting
physiological outcomes; to replicate existing findings linking perfectionism and anxiety; and to
provide a further dimension to this area with the addition of physiological symptoms as an outcome
of perfectionism.
Defining Perfectionism
Perfectionism has garnered an increasing amount of attention over the last few decades,
resulting in the creation of a number of scales designed to measure this construct. It has been
defined as the self-imposed need that an individual has to be perfect in every aspect of their lives,
and this is marked by the setting of extremely high personal goals and standards that they feel they
must achieve (Flett & Hewitt, 2002). However there is still disagreement between different groups
on an ultimate definition; whilst most favour a multidimensional approach, some still argue for a
unidimensional perspective that generally involves faulty cognition (Flett & Hewitt, 2002).
Multidimensional approaches posit that perfectionism arises from a variety of factors, not
just one lone characteristic. Many dichotomous accounts of perfectionism have been established
that acknowledge how an individual can be a perfectionist in a variety of ways. For example, the
4

Perfectionism and the stress response
distinction has been made between normal and neurotic perfectionists; normal perfectionists set
themselves high goals, but these are reasonable, and achievement leads to positive affect in terms of
increased self-esteem; whereas neurotic perfectionists seek achievements higher than realistically
attainable, and thus the inevitable failure reduces positive affect (Hamachek, 1978, cited in Flett &
Hewitt, 2002). In addition, neurotic perfectionists are likely to be motivated by the fear of this
failure as opposed to potential positive rewards (Shafran, Cooper & Fairburn, 2002). A second
dichotomy is positive versus negative perfectionism, with both being motivated by the relevant
form of reinforcement. Positive perfectionists are motivated by the desirable feelings associated
with accomplishing a goal, and negative perfectionists are motivated by a need to avoid the fear of
failure (Terry-Short, Owens, Slade & Dewey, 1995), similar to neurotic perfectionism.
With regards to measuring multidimensional aspects of perfectionism there are two main
scales that are widely used in the psychological community (Frost, Marten, Lahart, Rosenblate,
1990; Hewitt & Flett, 1991), and whilst they both measure perfectionism they place emphasis on
different subsets of this construct.
Hewitt and Flett (1991) focused on three dimensions; self-oriented, other-oriented, and
socially prescribed perfectionism. Self-oriented perfectionism involves the setting of high
standards, and rigorously evaluating one’s behaviour with regards to these standards. They are
motivated by the need to fulfil these goals, but also by the fear of failure. Other-oriented
perfectionism is nearly identical to self-oriented, but in this case the high standards and evaluation
of behaviours are displaced onto others; for example, a husband demanding that his wife iron and
fold his shirts in an exacting fashion. Socially-prescribed perfectionism relates to an individual
holding the belief that others are setting extreme standards for them, judging their behaviour and
5

Perfectionism and the stress response
stressing the need to be perfect. Hewitt and Flett’s perfectionism scale has been found to have high
internal consistency and validity (1991).
Constructed around the same period Frost’s Multidimensional Perfectionism Scale (Frost,
Marten, Lahart, & Rosenblate, 1990) measures perfectionism in six different dimensions,
combining a mix of inter- and intrapersonal factors; Personal Standards; Concern Over Mistakes;
Parental Expectations; Parental Criticism; Doubting of Actions; and Organisation. Unlike Hewitt
and Flett’s (1991) this scale does not measure perfectionism that the individual displaces onto
others. Personal Standards refer to the setting of extremely high values and strictly following these
when evaluating oneself. Concern Over Mistakes is the belief that mistakes equate to failure, and
the experience of negativity felt when mistakes are made. Parental Expectations and Parental
Criticism refer to the high goals set and the highly critical nature respectively of an individual’s
parents. Doubting of Actions involves the feelings that one hasn't completed a task to a satisfactory
level. Organisation highlights the importance that an individual places on creating and keeping
order in various aspects of their lives. Frost et al. (1990) demonstrated that their scale had good
validity and that it was internally consistent to a degree; Organisation was found to correlate lower
than the other subscales so was omitted in some of their analyses.
Shafran et al. (2002) argue for a more unidimensional account by demonstrating that the
most integral aspects of perfectionism are far fewer than multidimensional scales measure. They
believe that a model of perfectionism need only focus on the domain of self-oriented perfectionism,
and that perfectionism is created by the individual as opposed to those around them. They give the
example that others may impose perfectionist standards upon us but we do not have to respond to
these, and so other-oriented perfectionism cannot reliably account for perfectionism. The
unidimensional approach however may be too simplistic in its explanation; what they are proposing
6

Perfectionism and the stress response
could be the fundamental core that predisposes an individual to become highly perfectionist, but the
multidimensional dimensions that Hewitt and Flett (1991) and Frost et al. (1990) propose that could
lead to perfectionist qualities being exhibited in an individual.
The aim of this research is to focus on multidimensional perfectionism. Unidimensional
accounts are generally widely cited in relation to psychopathological cases and so could prove to
have a limiting affect on the possible scope of any relationships investigated here. Furthermore the
existence of highly valid multidimensional perfectionism scales provides a very useful means of
measuring a variety of possible contributing factors.
Perfectionism and psychological health
An extensive search of the existing literature has revealed that the majority of research
concerned with the links between perfectionism and health specifically involves a wide variety of
negative psychological disorders.
As discussed, maladjusted perfectionism can lead to negative affect in an individual when
high standards are not achieved, and they become motivated to live their lives through a fear of
failure. It is no wonder then that some have chosen to investigate the relationship between certain
dimensions of perfectionism and depression. Hewitt and Flett (1993), using a version of their
multidimensional scale of perfectionism, demonstrated that in a group of depressed patients self-
oriented perfectionism and achievement hassles interact significantly to positively predict scores on
the Beck Depression Inventory. This indicates that, when an individual places a lot of pressure
upon themselves to be perfect, and evaluates daily events as being stressful, they risk the increased
likelihood of suffering from depression. In addition, socially-prescribed perfectionism was shown
to correlate positively with depression, something which has been successfully replicated (Martin,
7

Perfectionism and the stress response
Flett, Hewitt, Krames & Szanto, 1996). It appears that depressive symptoms are more likely in
individuals who have perfectionist standards placed upon them as opposed to generated internally.
Nonetheless those who experience self-oriented perfectionism could generally be more inclined to
appraise daily hassles as stressful because they interfere with their ability to successfully achieve
perfectionism. A recent study by O’Connor, Rasmussen & Hawton (2010) managed to replicate the
findings by Hewitt & Flett (1993), demonstrating that self-oriented perfectionism interacted
significantly with acute life stress to positively predict psychological distress. That the sample was
a group of Scottish adolescents adds to the validity of this specific relationship across the lifespan.
One reported difference was that the relationship between self-oriented perfectionism and
depression was mediated more by life stress than daily hassles, although it could be argued that
these two concepts are intrinsically linked.
In more general terms of psychological wellbeing and affect, the majority of research
points towards a significant relationship between perfectionism and negative psychological
outcomes including; worry and negative affect (Chang, 2000; Dunkley, Zuroff & Blankstein, 2003);
and stress (Chang, 2000; Chang, Watkins & Banks 2004). Furthermore socially-prescribed
perfectionism has consistently been found to have significant positive associations with general
psychological distress (O’Connor & O’Connor, 2003; Van Yperen & Hagedoorn, 2008); hostility
and anxiety (Chang & Rand, 2000); and hopelessness (O’Connor & O’Connor, 2003). Significant
negative associations have been found with autonomy, environmental mastery and purpose in life
(Chang, 2006).
Hence it would appear that stress plays a significant role in mediating the relationship
between perfectionism and other negative psychological outcomes. On a basic level it has been
suggested that those who experience perfectionist tendencies tend to appraise events as more
8

Perfectionism and the stress response
stressful and impose a greater amount of stress upon themselves by the setting of high standards.
But it has been further hypothesised that perfectionism interacts with stress in four ways to both
construct and maintain psychopathological states within the individual; stress generation, stress
anticipation, stress perpetuation, and stress enhancement (Hewitt & Flett, 2002). Each of these
approaches is fairly self explanatory; stress generation posits that perfectionists engage in an
increased number of behaviours that create stressful situations; stress anticipation refers to the
amplified preoccupation that perfectionists have with potential stressors; stress perpetuation is the
tendency of perfectionists to engage in behaviours that prolong stressful events such as rumination;
and stress enhancement explains how perfectionists are prone to maladaptive forms of cognitive
appraisals that function to magnify the amount of stress experienced (Hewitt & Flett, 2002). These
four approaches have been supported by various pieces of research that have found, amongst other
things, that perfectionists place a larger amount of pressure on themselves than non-perfectionists
(Beck, 1993), that perfectionism scales correlate significantly with levels of self-imposed pressure
(Flett, Parnes & Hewitt, 2001, cited in Hewitt & Flett, 2002), and that self-critical perfectionists are
more reactive to events that are perceived to be potentially stressful (Dunkley, Zuroff & Blankstein,
2003).
Psychological disorders and physiological stress
It is important to realise the links that could exist between the psychological outcomes of
perfectionism and subsequent physiological stress, in particular the area of cardiovascular disorders.
A meta-analysis by Chida & Hamer (2008) suggested that strong links appear to exist between
psychological states, such as anxiety and negative affect, and decreased cardiovascular reactivity
and poor recovery. Although this analysis was not directly measuring associations with
perfectionism, it could be inferred that a highly perfectionist individual experiencing subsequent
9

Perfectionism and the stress response
anxiety, and/or negative affect could therefore be predisposed to these physiological outcomes.
This assumption suggests that in a comparison of high and low perfectionists it could be expected
that those high in perfectionism would exhibit significantly reduced physiological responses relative
to low perfectionists. Conversely, a separate study by Harleston, Smith & Arey (1965) found that,
when completing a lab-based problem solving task, highly anxious participants demonstrated much
larger increases in heart rate that were far more prolonged than those observed in low anxiety
participants. The long term effects of increased strain upon the heart and cardiovascular system can
be very serious; it increases the risk of a variety of cardiovascular disorders such as hypertension,
and research suggests that sustained heart rate levels can increase the risks of myocardial infarction
(Singh, 2003). Hence any possible links between perfectionism and cardiovascular changes could
be extremely important. This is strengthened by the findings that cardiovascular disorders share a
high comorbidity with mood and anxiety disorders, that rates of hypertension have been found to be
highly prevalent in anxiety (Huang, Su, Tzeng-Ji, Chou & Bai, 2009), and that coronary heart
disease has been demonstrated to be linked to depression (Suls & Bunde, 2005).
Nevertheless, the research discussed here does not provide evidence of direct relationships
between perfectionism and physiological health, and so it is important not to over-generalise the
findings on the basis of associations between the psychological disorders here and perfectionism.
Perfectionism and physiological health
A large amount of the literature is dedicated to perfectionism and other psychological
disorders, but searches in the psychological databases of heart rate and perfectionism, and blood
pressure and perfectionism yield just 4 relevant results. Of these there is no general consensus as to
the significant relationship between perfectionism and physiological symptoms. It has been
10

Perfectionism and the stress response
suggested that no significant relationships exist between perfectionism and heart rate or diastolic
blood pressure when participants complete a potentially stressful experimental task (Besser, Flett,
Hewitt & Guez, 2008). Yet the same research did demonstrate significant interactions between
increased systolic blood pressure and high self-oriented perfectionism when coupled with poor
objective task performance, and increased systolic blood pressure and high socially-prescribed
perfectionism when coupled with negative feedback. This association, although significant, cannot
however demonstrate that perfectionism has a direct affect on the cardiovascular system. However
research concerning the specific hormones involved in the physiological stress response has
successfully demonstrated that perfectionism is positively associated with cortisol, a hormone that
acts to increase blood pressure, but that no relationship was observed between perfectionism and
norepinephrine, a hormone that actively increases heart rate (Wirtz et al., 2007). Again this
supports Besser et al (2008), in that perfectionism may exhibit links with blood pressure but not
heart rate. Wirtz, Siegrist, Rimmele and Ehlert (2008) focused on the concept of over commitment,
a behaviour linked to excessive striving, an incapacity to pull out of commitments and subsequent
exhaustion. Although not explicitly measuring perfectionism, there are obvious similarities
between the two concepts and a significant association was found between them, so this research
could be seen as relevant to this research. The findings indicated that those participants who were
grouped as being low in over commitment actually recorded lower heart rates before and after
completing a stressful public speaking task. So though this does not follow the pattern
demonstrated previously, with increases in cardiovascular pressure, they differ in that a significant
association could at least be identified with regards to heart rate. The three studies discussed here
have all been concerned with immediate effects in the cardiovascular system in response to stressful
conditions; however a piece of research conducted with a sample of Japanese women reported that
11

Perfectionism and the stress response
perfectionism was significantly associated with a decreased risk of coronary artery disease
(Yoshimasu et al., 2002). This finding further adds to the inconclusive collection of research in this
particular area, though it is important to note that being categorised as a ‘perfectionist’ in the study
was determined by only one question on a 12-item questionnaire, hence it would be irresponsible to
place too much emphasis on this outcome.
The lack of significant psychological research into the physiological effects of perfectionism
is surprising as the potential outcomes would be extremely important if they were to imply a
negative effect of perfectionism on physiological health. Although previous research in this area
has not yielded any concrete, replicated findings it would be ill-considered to dismiss possible
further avenues; especially considering that links exist between perfectionism and psychological
disorders, and psychological disorders and physiological health.
Hypotheses
On a general level it is presumed that a stressful task will increase the amount of anxiety that
an individual feels under, therefore the first hypothesis is as follows:
h1) Higher post-task anxiety will be reported relative to pre-task in both high and low perfectionists.
And at a more specific level, due to the tendency for high perfectionists to respond to stress
with a more intensely anxious state, it is further hypothesised that:
h2) High perfectionists will report higher levels of state anxiety relative to low perfectionists in both
pre- and post-task measures.
With regards to the physiological response to stress it is more difficult to confidently predict
possible relationships because of the limited and mixed previous research. However based
12

Perfectionism and the stress response
somewhat on the psychological literature it is expected that some differences will exist between
high and low perfectionists, specifically that:
h3) There will be differences in resting blood pressure and heart rates between high and low
perfectionists.
And that:
h4) There will be significant differences between high and low perfectionists in blood pressure and
heart rate during a stressful task.
It must be stressed that these last two hypotheses are not directional, rather that
perfectionism will have an effect on the physiological response to stress, and that the purpose of this
research is to investigate the specifics of this relationship.
Method
Participants
High perfectionist group. The data collected from the current study were collated with a
data set of 22 ‘high perfectionist’ participants collected by a postgraduate student the previous year,
whose experimental method this current study replicates. This group consisted of 11 female (50%)
and 11 male (50%) students from the University of Surrey. The ages of this group ranged from 19
years to 51 years (M = 26.73 years, S.D. = 7.58 years).
Low perfectionist group. Participation in the current study was advertised by means of an
initial email sent out to all undergraduate students in the Department of Psychology at the
University of Surrey. The email contained details of the study and invited those who were
13

Perfectionism and the stress response
interested to complete an initial screening questionnaire. Sixty-two responses were collected and
from this group 26 participants were selected who fulfilled the criteria of being a ‘low
perfectionist’. These 26 participants were asked to visit the Psychology department where they
would take part in the main study lasting 50 minutes, of this group 21 accepted (female n = 13
(61.9%), male n = 8 (38.1%)). All the participants were full-time undergraduate Psychology
students in either their first or second year of study, the ages of participants ranged from 18 years to
39 years (M = 20.48 years, S.D. = 4.67 years).
Apparatus
Screening Questionnaire. In order to screen participants as low perfectionists an initial
questionnaire was completed by all who had expressed an interest in participation. This
questionnaire was a reduced version of Frost’s Multidimensional Perfectionism Scale (1990) used
in the main study and contained 10 questions designed to measure general perfectionism. These
questions were answered using a 5-point likert scale ranging from 1 (strongly disagree) to 5
(strongly agree), and the 10 responses were totalled to make an overall score. As the cut-off for
high perfectionists was a score of 34 or above it was decided that those who scored a total of 30 or
below would qualify as being ‘low perfectionist’ and contacted to take part in the main study. A
copy of the screening questionnaire can be found in Appendix 1. The reliability of this scale in the
present study was found to be α = .77.
For the main study a battery of questionnaires was compiled for all participants to complete.
For the purpose of this study Frost’s Multidimensional Perfectionism Scale (FMPS), and
Spielberg’s State Trait Anxiety Inventory (STAI) were the only two of interest.
14

Perfectionism and the stress response
Frost’s Multidimensional Perfectionism Scale (FMPS). This scale contains 35 questions,
scored on a 5-point likert scale from ‘strongly disagree’ to ‘strongly agree’, it measures the extent to
which an individual could be considered a ‘perfectionist’. The highest total score is 175, and higher
scores indicate high perfectionism. The scale specifically asks questions about 6 dimensions of
perfectionism; Concern Over Mistakes (CM); Doubting of Actions (DA); Personal Standards (PS);
Parental Expectations (PE); Parental Criticism (PC); and Organisation (O). An average score of
3.06 was found to be the median score and so was used as the cut-off point, with all those who
scored lower categorised as being ‘low-perfectionists’ and all those who scored higher categorised
as ‘high-perfectionists’. A copy of this scale can be found in Appendix 2. It was found to be highly
reliable in the current study with a Cronbach’s alpha score of α = .91.
Spielberger’s State Trait Anxiety Inventory (STAI). A shortened version of this scale
was used to measure levels of state anxiety only. State anxiety is defined as the subjective tension
or fear directly caused by a stressful situation, that passes once the stressor has been removed
(Aydin, 2009). The scale contained 20 questions answered on a 4-point likert scale from ‘not at all’
to ‘very much so’ meaning that each participant could score a maximum of 156, with higher scores
indicating higher levels of state anxiety. Items 1, 2, 5, 8, 10, 11, 14, 15, 16, 19 and 20 (I feel:
“calm”; “secure”; “at ease”; “satisfied”; “comfortable”; “self-confident”; “decisive”; “relaxed”;
“content”; “steady”; and “pleasant”) were reversed scored. This scale was administered twice
throughout the experiment in order to measure state anxiety before and after the stressful task. This
scale can be found in Appendix 3. It was found to be incredibly reliable with a total Cronbach’s
alpha score of α = .94.
Blood pressure monitor. An AnD UA-767 Digital Blood Pressure Monitor was used in all
conditions to measure heart rate and systolic and diastolic blood pressure. The cuff is secured
15

Perfectionism and the stress response
around the non-dominant upper-arm and the start button pressed by the researcher which
automatically inflates the cuff. As the cuff deflates the blood pressures and heart rate are measured
and once it is fully deflated a number appears on the screen for each, this was then recorded by the
researcher. This blood pressure monitor has been found to be highly valid and is recommended for
clinical use (Rogoza, Pavlova & Sergeeva, 2000).
Colour-word interference task. A stroop task was used as a means of inducing stress in
the participant. In this computer-based task the participant is presented with a ‘test’ colour word in
the middle of the screen and four ‘answer’ colour words along the bottom of the screen. They are
required to match the physical colour of the test word with the semantic meaning of the answer
word. The difficulty of this task arises from the physical colour and semantic meaning of the test
word being different e.g. the test word ‘red’ may be printed in the colour green and so the
participant has to select the word ‘green’ from the list of answer words. In order to maintain this
difficulty the time between each word increased throughout the task. Furthermore the difficulty of
this particular task was heightened in the current study by making it double interference i.e. the
physical colour and semantic meaning of each answer words was also different.
Procedure
Participants were provided with an information sheet outlining the basic procedural structure
and what they could expect from participation. All participants were required to read this
information and a consent form which had to be signed prior to participation, copies of these can be
found in Appendix 4. All data collection took place in a lab situated in the Psychology department
at the University of Surrey. Participants began by completing the first pack of the questionnaire
booklet containing FMPS. Once this was completed blood pressure and heart rate readings were
16

Perfectionism and the stress response
taken using an electronic blood pressure monitor, after which participants were instructed to relax
for 6 minutes before a second set of readings was taken. The second pack of the questionnaire
booklet was then filled out; this section contained two 7-point likert scales on the amount of
pressure and control the participant felt they had at that moment in time, and a shortened version of
the STAI. The participant then moved on to a computer based stroop task that was designed to
induce a stressful response in the individual. Prior to the main stroop task all participants were
provided with verbal instructions on how to complete the task and a practice task which they could
repeat if necessary. The main stroop task lasted 6 minutes, and blood pressure and heart rate
readings were taken at 3 points; after 30 seconds, 150 seconds, and 240 seconds. Immediately after
completion of the stroop task the participant completed pack 3 of the questionnaire booklet, this
contained four 7-point likert scales on the extent to which the participant felt currently under
pressure, in control, how pressured they felt during the task, and the number of mistakes they felt
they had made. After this was completed participants once again rested for 6 minutes before the
last set of blood pressure and heart rate readings were taken. The final pack of the questionnaire
booklet was now completed and this contained a replication of the shortened STAI, a set of
questions asking participants to assess physiological changes within the body during the task, and
four 7-point likert scales on the extent to which participants had thought about the stroop task since
completion, how difficult and complicated they found the stroop task, and how worried they were
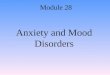
about making mistakes during the task. A timetable of the main study can be found in Diagram 1
below. Upon completion of the study all participants were provided with a debrief sheet (see
Appendix 4) that outlined the purpose of the study and provided contact details should the
participant have any questions at a later date. All participants were thanked for their time and
cooperation and reimbursed with a course credit.
17

Perfectionism and the stress response
Info and consent forms
Pack 1
BP and HR 1 Relax
BP and HR 2
Pack 2
Stroop instructions
Stroop task (29-35 mins)
Pack 3 Relax
BP and HR 6
Pack 4 Debrief
BP and HR 3
BP and HR 4
BP and HR 5
1-3 mins
3 - 10
mins
10 -12
mins
12 -18
mins
18 -20
mins
20 -25
mins25-29 mins 29.5
mins31.5 mins
33 mins
35-36
mins
36-42
mins
42-44 mins
44-48
mins
48-50 mins
Diagram 1. Timetable of the main laboratory study.
Results
This study was designed to test the effects of a stress inducing task on participants differing
in levels of perfectionism. Four hypotheses were stated; that higher levels of state anxiety would be
reported after a stressful task in both high and low perfectionists; that higher levels of state anxiety
would be observed in high perfectionists before and after a stressful task; that there will be
significant differences in baseline readings of blood pressure and heart rate between high and low
perfectionists; and that blood pressure and heart rate during the stressful task would be significantly
different between high and low perfectionists.
Participant Characteristics
The two groups did not differ significantly in gender, t (41) = 1.69, p = .09, d = .51, or BMI,
t (41) = -0.74, p = .47, d = .22. However a difference was found in terms of age, with the high
perfectionist group (M = 25.95 years, SD = 7.57 years) being significantly older than low
perfectionists (M = 21.5 years, SD = 5.56 years), t (41) = -2.20, p = .03, d = .68. See Table 1 below for
a summary of participant characteristics.
18

Perfectionism and the stress response
High Perfectionists Low Perfectionists
Mean SD Mean SD
Age (years) 25.95 7.57 21.50 5.56
BMI 22.99 4.02 22.20 3.00
Male Female Male Female
Gender 12 9 7 15
Table 1. Means, standard deviations, and frequencies of participant characteristics.
Data Analysis
State Anxiety. It was hypothesised that state anxiety would be higher post-task relative to
pre-task in both groups, but also that high perfectionists would sustain higher levels of state anxiety
relative to low perfectionists. These effects were analysed with a Group (high, low perfectionism) x
Task (pre-, post-task) ANOVA. A significant Group main effect existed, F (1,41) = 9.42, p = .004,
partial η2 = .19, but there was no significant Task main effect, F (1,41) = 1.05, p = .31, partial η2
= .02. No significant Group x Task interaction was identified, F (1,41) = 1.67, p = .20, partial η2
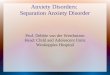
= .04. Independent-samples t-tests were conducted and it was found that high perfectionists
reported higher levels of state anxiety than low perfectionists prior to the task (M = 45.38, 35.14,
S.D. = 11.45, 7.98 respectively), t (41) = -3.42, p = .001, d = .73, and after the task (M = 45.10,
37.59, S.D. = 10.96, 9.75 respectively), t (41) = -2.38, p = .02, d = 0.07. These results indicate that
although the stroop task did not significantly alter state anxiety levels within the groups, high
perfectionists did indeed maintain significantly higher levels of state anxiety relative to low
perfectionists throughout the study. This effect is demonstrated in Figure 2 below.
19

Perfectionism and the stress response
Figure 2. State anxiety levels in high and low perfectionsists before and after the stroop task. Note
the significant between-groups effect, but the absence of any significant within-groups effects.
Physiological Changes. It was hypothesised that differences would exist in resting and task
measures of blood pressure and heart rate between high and low perfectionists. In order to obtain a
measure of resting heart rate and blood pressures an average was calculated using the pre-task and
post-task readings (readings 1, 2, and 6; see Diagram 1).
Systolic blood pressure. A Group (high, low perfectionists) x Condition (resting, task)
ANOVA was conducted, however the average measures of systolic blood pressure taken before and
during the stroop test were found to correlate significantly with BMI (r (41) = .47, p = .002, and r
(41) = .37, p = .01, respectively), therefore BMI was included as a covariate in this analysis. No
significant main effects were found for Group, F (1,40) = 0.08, p = .78, partial η2 = .01, or for
Condition F (1, 40) = 0.04, p = .84, partial η2 = .01, however a significant Group x Condition
interaction was reported, F (1,40) = 9.06, p = .01, partial η2 = .19. This interaction is demonstrated
in Figure 3 below, and indicates that high and low perfectionists differ in both the resting and task
measures. It would appear that low perfectionists recorded slightly higher resting rates (M =
20
0
10
20
30
40
50
Pre- Post-
Task
Stat
e A
nxie
ty
Low perfectionismHigh perfectionism

Perfectionism and the stress response
115.58, SD = 11.52) and that this rate was maintained regardless of the introduction of a stressful
condition (M`= 116.80, SD = 10.88), i.e. there was no significant difference between resting and
task systolic blood pressure, t (21) = -1.01, p = .32, d = .11. However high perfectionists initially
recorded lower resting levels (M = 112.74, SD = 10.69) relative to low perfectionists, but this was
not sustained and the group demonstrated a significant increase in systolic blood pressure during the
stressful task (M = 119.75, SD = 14.51), t (20) = -4.94, p = .001, d = .56.
Figure 3. Changes in systolic blood pressure in high and low perfectionists during the resting and
task periods.
Diastolic blood pressure. Diastolic blood pressure was analysed within a Group (high, low
perfectionists) x Condition (resting, task) ANOVA. There was no significant main effect of Group,
F (1,41) = 0.02, p = .89, partial η2 = .01, there was however a highly significant main effect of
Condition, F (1,41) = 27.53, p = .001, partial η2 = .40. No significant Group x Condition interaction
was found, F (1,41) = 0.33, p = .57, partial η2 = .01. The variable for resting diastolic blood
pressure was found to be non-parametric, for this reason two Wilcoxon tests were conducted. It
21
108
110
112
114
116
118
120
122
Resting Stroop
Condition
Systo
lic B
P
Low perfectionismHigh perfectionism

Perfectionism and the stress response
was demonstrated that there were significant increases in diastolic blood pressure between the
resting and task condition in low perfectionists (Mdn = 69.63, 74.83 respectively), Z = -2.74, p
= .01, and in high perfectionists (Mdn = 69.50, 76.33 respectively), Z = -3.47, p = .001. In other
words, diastolic blood pressure significantly increased in both groups in the task condition relative
to the resting condition, irrespective of perfectionism. This effect can be seen in Figure 4 below.
Figure 4. The increase in diastolic blood pressure during the task condition, irrespective of
perfectionism.
Heart rate. Heart rate was again analysed within a Group (high, low perfectionists) x
Condition (resting, task) ANOVA. There was no significant Group main effect, F (1,41) = 1.40, p
= .24, partial η2 = .03, however a significant Condition main effect did exist, F (1,41) = 33.59, p
= .001, partial η2 = .45. There was no significant Group x Condition interaction, F (1,41) = 0.64, p
= .43, partial η2 = .01. Two within-samples t-tests were conducted to determine the exact nature of
the effect of Condition. It was found that there were significant increases in heart rate during the
task condition in both low perfectionists (M = 70.36, 78.00, SD = 8.19, 8.67 respectively), t (41) = -
22
66
68
70
72
74
76
Resting Stroop
Condition
Dia
stolic
BP
Low perfectionismHigh perfectionism

Perfectionism and the stress response
5.00, p = .001, d = .91, and in high perfectionists (M = 74.37, 80.16, SD = 7.50, 12.36 respectively),
t (41) = -3.31, p = .004, d = .58. This effect can be seen in Figure 5 below.
Figure 5. The effect of the stroop task on heart rate in low and high perfectionists.
Subjective Ratings. In addition to the data on anxiety and physiological symptoms,
subjective ratings were also collected throughout the laboratory task. These measures included how
much pressure the participant felt under, how much control they felt they had, how difficult they
found the stroop task, and how much they had thought about the stroop task during the second rest
period. In addition, participants were asked to identify if they felt they had experienced any bodily
sensations during the task, for example a racing heart and a tingling in the hands or feet. Responses
to 18 subjective measures were collected for each participant, these responses were analysed using
either independent-samples t-tests or Mann-Whitney tests based on whether the data was parametric
or not. Significant differences were only found in 2 of these subjective measures. It was found that
low perfectionists rated themselves as having significantly more control before the task than high
perfectionists (M = 5.50, 4.43, SD = 0.91, 1.25 respectively), t (41) = 3.22, p = .002, d = .99, and
23
64666870727476788082
Resting Stroop
Condition
Hea
rt R
ate
(bpm
)
Low perfectionismHigh perfectionism

Perfectionism and the stress response
that high perfectionists rated themselves as significantly more worried about their stroop task
performance than low perfectionists (M = 5.57, 4.64, SD = 1.16, 1.56 respectively), t (41) = -2.22, p
= .03, d = .68.
Discussion
The aim of this research was to determine the effects of a stress inducing laboratory task and
whether these effects differed between high and low perfectionists.
It was hypothesised that state anxiety levels would be persistently elevated in high
perfectionists relative to low perfectionists, irrelevant of the stressful task, but that a stressful
situation would increase state anxiety in both groups. In addition to anxiety, physiological
responses in perfectionists were also examined; something that has been fairly neglected up until
now. It was hypothesised that differences would be found between high and low perfectionists in
resting and task readings of systolic and diastolic blood pressure, and heart rate. With regards to
these hypotheses directions were not stated due to the rather confused nature of previous findings in
this area.
High perfectionists did indeed recorded significantly increased levels of state anxiety
compared to low perfectionists, both before and after the stressful task. Although rather
unexpectedly, neither group recorded a significant increase in state anxiety levels following the
stroop task, meaning that these hypotheses were only partially supported. This raises the question
of whether the stroop task employed was able to elicit a stressful enough response in the
participants, and therefore whether it was the most appropriate measure to use, something that will
be discussed later. From this it could be concluded that perfectionism does indeed affect anxiety,
with those scoring higher in perfectionism sustaining elevated levels of anxiety irrespective of
24

Perfectionism and the stress response
whether or not they are currently in a stressful state. However it would be of interest to see whether
this difference exists in measures of self-reported trait anxiety as this may be what underlies the
sustained levels of state anxiety found here.
With regards to the physiological effects of stress no significant differences were found
between high and low perfectionists in both blood pressure measures and heart rate in the rest
condition, suggesting that perfectionism has no long-term sustained effects on these particular
physiological symptoms, and therefore resulting in this hypothesis being rejected. However it could
be argued that due to the majority of participants belonging to the younger demographic; the mean
age being 23.7 years, that if any long-term effects were to occur than they may not manifest until
later on in the lifespan. Conversely, significant within-groups differences were found between
resting and task measures of diastolic blood pressure and heart rate, with increases in both being
found irrespective of group subscription. Indicating that the stroop task may not have been as
redundant in inducing a stress response as initially concluded from the state anxiety measures. In
terms of systolic blood pressure no significant group or condition effects were found, but a
significant interaction between the variables was identified. It was reported that low perfectionists
demonstrated no real differences between the resting and task measures of systolic blood pressure,
but that high perfectionists exhibited a significant increase in systolic blood pressure during the
stroop task. It could be argued that whilst diastolic blood pressure and heart rate also significantly
increased during the stroop, because this effect was observed in both groups, systolic blood pressure
was the only physiological measure that interacted with perfectionism.
Limitations
25

Perfectionism and the stress response
As mentioned there may be some questions surrounding the suitability of the stroop task as a
measure designed to induce experimental stress. The basis of this is that no significant increases
were found between measures of before- and after-task state anxiety regardless of perfectionism
levels, something that was specifically hypothesised. One solution to this issue would be to keep
the stroop as the task of choice, but place more emphasis on performance as this is something that is
likely to affect high perfectionists specifically. A 2 x 2 design could be employed whereby groups
are split by perfectionism, as in this research, but then further divided into two, with one half
receiving negative feedback regarding performance and the other receiving positive feedback,
irrespective of actual performance. This type of feedback design was employed in the
aforementioned research by Besser, Flett, Hewitt & Guez (2008), and yielded significant
physiological changes suggesting that this would be a useful alteration to the current methodology.
Alternatively a change could be made to the task used; the use of difficult arithmetic questions may
be a good stress-inducing measure as those individuals high in perfectionism may respond
negatively to feelings of making mistakes, or not performing to a high enough standard. Of course
any change in the methodology does not overcome the issue that it is very difficult to assess
whether both high and low perfectionists are experiencing the same level of stress. In other words,
if significant changes are observed in systolic blood pressure during a stressful task in high
perfectionists, it would be difficult to identify the exact reasons why. Both high and low
perfectionists could be perceiving the same levels of stress but an aspect of high perfectionism
could exist that heightens the physiological response to this stress. Alternatively a particular
stressful task may only elicit a stressful response in high perfectionists, and so low perfectionists
don’t experience a change in blood pressure because they don’t actually feel any stress. This may
26

Perfectionism and the stress response
be a rather tenuous argument but it is one that, if supported with empirical evidence, could be of
importance in this research.
A second limitation of this research was the use of a young, student sample. It could be
argued that students are likely to experience a large amount of stress during their time at university,
and therefore did not respond positively to the stressful task in this research, however this is
something that could be overcome with the abovementioned methodological changes. Also, as
previously alluded to, a possible reason as to why differences were not found between high and low
perfectionists in resting levels of physiological measures was because the participants were sampled
from a fairly young demographic. The implication of this being that participants were too young to
exhibit many signs of sustained physiological stress; hypertension and cardiovascular diseases are
most commonly found in older adults (Marcovitch, 2006). Both of these limitations could be
overcome by using a sample with a broader age range.
Future Research
Although the current research did not produce as many significant differences between high
and low perfectionists as initially hypothesised it does not mean that this is not a highly important
area of research that should be expanded. As mentioned changes could be made with regards to the
methodology, with the most important change being the type of measure used to induce stress in the
experimental condition. In addition to this a larger and more demographically varied sample should
be employed in order to produce data that is far more generalisable, and of more use to a wider
range of groups, for example within the healthcare and therapeutic professions.
From a psychological perspective it would be of interest to investigate whether differences
exist between specific dimensions of perfectionism. The current research employed Frost’s MPS
27

Perfectionism and the stress response
(1990), and so groups could be compared on the basis of scores on each of the six dimensions could
be compared. Furthermore a large amount of the literature on perfectionism uses the MPS
developed by Hewitt and Flett (1991), which investigates perfectionism as self-oriented, other-
oriented, and socially prescribed. It may then be of even more use to repeat the current research
with this scale instead in order to produce findings that are more grounded in the current literature,
and therefore more relevant.
It is difficult to move away from a laboratory-based focus due to the need to be able to
measure the direct effects of stress on physiological symptoms. But future research could also
investigate the physiological effects of real-life stressful events on perfectionists by means of self-
reported stressful incidences and longitudinal measure of blood pressure. In this case the
physiological effects of interest would not be short-term, as in the current research, but long-term,
thus rendering them more useful in a real world context as it is undeniably the long-term effects that
have the most serious health consequences. The advantages of this more realistic approach
however would be countered by the relationships drawn between stress and physiology mediated by
perfectionism being far more speculative in nature.
Conclusion
The current research partially fulfilled what it set out to do. On one hand it was able to
replicate previous findings that perfectionism influences the relationship between stress and
anxiety, but it also failed to provide any definitive conclusions as to whether or not perfectionism
plays the same role between stress and the physiological response. Although this is disappointing it
could be suggested that research into the area of perfectionism and physiological health should not
be dismissed. This is a very important area, and one that could make significant contributions to the
28

Perfectionism and the stress response
ways in which maladaptive perfectionism is dealt with in an applied setting. It is imperative
however that if significant progress is to occur that changes are made to the methodology
employed; to date the majority of research conducted is experimental or laboratory-based, and so
may not accurately represent the processes that naturally occur on a day-to-day basis in response to
daily hassles and stressors. Nevertheless a significant interaction was found between perfectionism,
systolic blood pressure, and stress which is a promising start, and could indicate that the
physiological response to stress is influenced by perfectionism.
29

Perfectionism and the stress response
References
Ashby, J.S., & Kottman, T. (1996) Inferiority as a distinction between normal and neurotic
perfectionism. Individual Psychology, 52(3), 237-245.
Aydin, K.B. (2009). Automatic thoughts as predictors of Turkish university students’ state anxiety.
Social Behavior and Personality, 37(8), 1065-1072.
Beck, A.T. (1993). Cognitive approaches to stress. In R.L. Woolfolk & P.M. Lehrer (Eds.),
Principles and practice of stress management (pp. 333-372). New York: Guilford.
Besser, A., Flett,, G.L., Hewitt, P.L., & Guez, J. (2008). Perfectionism, and cognitions, affect, self-
esteem, and physiological reactions in a performance situation. Journal of Rational-Emotive
and Cognitive-Behavior Therapy, 26, 206-228.
Chang, E.C. (2000). Perfectionism as a predictor of positive and negative psychological outcomes:
Examining a mediation model in younger and older adults. Journal of Counseling
Psychology, 47(1), 18-26.
Chang, E.C. (2006). Perfectionism and dimensions of psychological well-being in a college student
sample: A test of a stress-mediation model. Journal of Social and Clinical Psychology,
25(9), 1001-1022.
Chang, E.C., & Rand, K.L. (2000). Perfectionism as a predictor of subsequent adjustment: Evidence
for a specific diathesis-stress mechanism among college students. Journal of Counseling
Psychology, 47(1), 129-137.
30

Perfectionism and the stress response
Chang, E.C., Watkins, A.F., & Banks, K.H. (2004). How adaptive and maladaptive perfectionism
relate to positive and negative psychological functioning: Testing a stress-mediation model
in black and white female college students. Journal of Counseling Psychology, 51(1), 93-
102.
Chida, Y., & Hamer, M. (2008). Chronic psychosocial factors and acute physiological responses to
laboratory-induced stress in healthy populations: A quantitative review of 30 years of
investigations. Psychological Bulletin, 134(6), 829-885.
Dunkley, D.M., Zuroff, D.C., & Blankstein, K.R. (2003). Self-critical perfectionism and daily
affect: Dispositional and situational influences on stress and coping. Journal of Personality
and Social Psychology, 84(1), 234-252.
Flett, G.L., & Hewitt, P.L. (2002). Perfectionism and maladjustment: An overview of theoretical,
definitional, and treatment issues. In G.L. Flett & P.L. Hewitt (Eds.), Perfectionism: Theory,
research, and treatment (pp.5-31). Washington, DC: American Psychological Association.
Frost, R.O., Marten, P., Lahart, C., & Rosenblate, R. (1990). The dimensions of perfectionism.
Cognitive Therapy and Research, 14, 449-468.
Harleston, B.W., Smith, M.G., & Arey, D. (1965). Test-anxiety level, heart rate, and anagram
solving. Journal of Personality and Social Psychology, 1(6), 551-557.
Hewitt, P.L., & Flett, G.L. (1991). Perfectionism in the self and social contexts: Conceptualization,
assessment, and association with psychopathology. Journal of Personality and Social
Psychology, 60(3), 456-470.
31

Perfectionism and the stress response
Hewitt, P.L., & Flett, G.L. (1993). Dimensions of perfectionism, daily stress, and depression: A test
of the specific vulnerability hypothesis. Journal of Abnormal Psychology, 102(1), 58-65.
Hewitt, P.L., & Flett, G.L. (2002). Perfectionism and stress processes in psychopathology. In G.L.
Flett & P.L. Hewitt (Eds.), Perfectionism: Theory, research, and treatment (pp.5-31).
Washington, DC: American Psychological Association.
Huang, K., Su, T., Tzeng-Ji, C., Chou, Y., & Bai, Y. (2009). Comorbidity of cardiovascular
diseases with mood and anxiety disorder: A population based 4-year study. Psychiatry and
Clinical Neurosciences, 63, 401-409.
Marcovitch, H. (Ed.). (2006). Black’s medical dictionary (41st Ed.). London: A & C Black.
Martin, T.R., Flett, G.L., Hewitt, P.L., Krames, L., & Szanto, G. (1996). Personality correlates of
depression and health symptoms: A test of a self-regulation model. Journal of Research in
Personality, 31, 264-277.
O’Connor, R.C., & O’Connor, D.B. (2003). Predicting hopelessness and psychological distress: The
role of perfectionism and coping. Journal of Counseling Psychology, 50(3), 362-372.
O’Connor, R.C., Rasmussen, S., & Hawton, K. (2010). Predicting depression, anxiety and self-harm
in adolescents: The role of perfectionism and acute life stress. Behaviour Research and
Therapy, 48, 52-59.
Rogoza, A.N., Pavlova, T.S., & Sergeeva, M.V. (2000). Validation of A&D UA-767 device for the
self-measurement of blood pressure. Blood Pressure Monitoring, 5(4), 227-231.
Singh, B.N. (2003). Increased heart rate as a risk factor for cardiovascular disease. European Heart
Journal Supplements, 5(G), G3-G9.
32

Perfectionism and the stress response
Shafran, R., Cooper, Z., & Fairburn, C.G. (2002). Clinical perfectionism: A cognitive-behavioural
analysis. Behavior Research and Therapy, 40, 773-791.
Suls, J., & Bunde, J. (2005). Anger, anxiety, and depression as risk factors for cardiovascular
disease: The problems and implications of overlapping affective dispositions. Psychological
Bulletin, 131(2), 260-300.
Terry-Short, L.A., Owens, R.G., Slade, P.D., & Dewey, M.E. (1995). Positive and negative
perfectionism. Personality and Individual Differences, 18(5), 663-668.
Van Yperen, N.W., & Hagedoorn, M. (2008). Living up to high standards and psychological
distress. European Journal of Personality, 22, 337-346.
Wirtz, P.H., Elsenbruch, S., Emini, L., Rüdisüli, K., Groessbauer, S., & Ehlert, U. (2007).
Perfectionism and the cortisol response to psychosocial stress in men. Psychosomatic
Medicine, 69, 249-255.
Wirtz, P.H., Siegrist, J., Rimmele, U., & Ehlert, U. (2008). Higher overcommitment to work is
associated with lower norepinephrine secretion before and after acute psychosocial stress in
men. Psychoneuroendocrinology, 33, 92-99.
Yoshimasu, K., Washio, M., Tokunaga, S., Tanaka, K., Liu, Y., Kodama, H., Arai, H., Koyanagi,
S., Hiyamuta, K., Doi, Y., Kawano, T., Nakagaki, O., Takada, K., Sasazuki, S., Nii, T.,
Shirai, K., Ideishi, M., Arakawa, K., Mohri, M., & Takeshita, A. (2002). Relations between
Type A behavior pattern and the extent of coronary atherosclerosis in Japanese women.
International Journal of Behavioral Medicine, 9(2), 77-93.
33

Perfectionism and the stress response
Appendix 1
Screening Questionnaire
Strongly Disagree Disagree
Neither Agree or Disagree
Agree Strongly Agree
1I never felt I could meet my parents’
expectations1 2 3 4 5
2I tend to get behind in my work because I repeat things over
and over
1 2 3 4 5
3 I am a neat person 1 2 3 4 5
4I never felt I could meet my parents’
standards1 2 3 4 5
5If I do not do as well
as other people it means I am not as
good as them
1 2 3 4 5
6I set higher goals
for myself than most people
1 2 3 4 5
7 I have extremely high goals 1 2 3 4 5
8If I do not do well all the time people will
not respect me1 2 3 4 5
9It takes me a long
time to do something right
1 2 3 4 5
10 I try to be a neat person 1 2 3 4 5
34

Perfectionism and the stress response
Appendix 2
Frost’s Multidimensional Perfectionism Scale (1990)
SD D N A SA
My parents set very high standards for meOrganisation is very important to meAs a child I was punished for doing things less than perfectlyIf I do not set the highest standards for myself I am likely to end up as a second rate personMy parents never tried to understand my mistakesI am a neat personIt is important to me to try to be thoroughly competent in everything I do I try to be an organised personIf I fail at work/university I am a failure as a personI should be upset if I make a mistakeMy parents wanted me to be the best at everythingI set higher goals for myself than most peopleIf someone does a task at work/university better than me I feel like I failed the whole task
SD D N A SA
If I fail partly it is as bad as being a complete failureOnly outstanding performance is good enough in my familyI am very good at focusing my efforts on achieving a goalEven when I do something very carefully I often feel that it is not being done quite rightI hate being less than the bet at thingsI have extremely high goalsMy parents have expected excellence from mePeople will probably think less of me if I make a mistakeI never felt like I could meet my parents expectationsIf I do not do as well as other people it means I am an inferior human beingOther people seem to accept lower standards for themselves than I doIf I do not do well all the time people will not respect meMy parents have always had higher expectations for my future than I haveI try to be a neat personI usually have doubts about the simple everyday things that I doNeatness is very important to me
35

Perfectionism and the stress response
SD D N A SA
I expect higher performance in my everyday tasks than most peopleI am an organised personI tend to get behind in my work because I repeat things over and overIt takes me a long time to do something ‘right’The fewer mistakes I make the more people will like meI never felt like I could meet my parents standards
36

Perfectionism and the stress response
Appendix 3
Spielberger’s State Anxiety Scale
Not at all Somewhat Moderately so Very much so
I feel calm
I feel secure
I am tense
I feel strained
I feel at ease
I feel upset
I am presently worrying about possible misfortunes
I feel satisfied
I feel frightened
I feel comfortable
I feel self-confident
I feel nervous
I feel jittery
I feel decisive
I am relaxed
I feel content
I am worried
I feel confused
I feel steady
I feel pleasant
37

Perfectionism and the stress response
Appendix 4
Information Sheet, Consent Form and Debrief Sheet
38

Perfectionism and the stress response
39

Perfectionism and the stress response
40