Embed Size (px)
Citation preview

St. Cloud State UniversitytheRepository at St. Cloud StateCulminating Projects in Communication Sciencesand Disorders
Department of Communication Sciences andDisorders
5-2016
The Effect of Baby Sign on Early LanguageDevelopment for "At-Risk" PopulationsSarah S. AndersonSt Cloud State University, [email protected]
Follow this and additional works at: https://repository.stcloudstate.edu/csd_etds
This Thesis is brought to you for free and open access by the Department of Communication Sciences and Disorders at theRepository at St. CloudState. It has been accepted for inclusion in Culminating Projects in Communication Sciences and Disorders by an authorized administrator oftheRepository at St. Cloud State. For more information, please contact [email protected].
Recommended CitationAnderson, Sarah S., "The Effect of Baby Sign on Early Language Development for "At-Risk" Populations" (2016). Culminating Projectsin Communication Sciences and Disorders. 3.https://repository.stcloudstate.edu/csd_etds/3

Running header: EFFECT OF BABY SIGN ON LANGUAGE FOR AT-RISK POPULATIONS 1
The Effect of “Baby Sign” on Early Language Development for “At-Risk” Populations
By Sarah S. Anderson
A Thesis
Submitted to the Graduate Faculty of
St. Cloud State University
in Partial Fulfillment of the Requirements
for the Degree of
Master of Science
in Communication Sciences and Disorders
May 2016
Thesis Committee:
Dr. Sarah Smits-Bandstra, Chairperson
Dr. Rebecca Crowell
Dr. Amy Knopf

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 2
Abstract
The purpose of this case study was to examine the effect of exposure to symbolic gestures or
“Baby Sign” on the development of joint attention, receptive and expressive language of children
from low socioeconomic backgrounds, including culturally/linguistically diverse children aged 9
to 20 months. Two child-parent dyads participated in the program. Both were enrolled in the
local “Head Start” (Reach-Up) program. The MacArthur Bates, Preschool Language Scales-4
(PLS-4) and video-recorded interactions with the primary caregiver were used to assess the
effectiveness of Baby Sign parent-training to facilitate early language development. Results of
the Preschool Language Scales-4 and the MacArthur Bates identified improved both receptive
and expressive language in “at risk” (low socioeconomic and culturally diverse backgrounds)
infants exposed to Baby Sign. In addition, qualitative data collected by parent interview revealed
significant barriers to service delivery for early language facilitation, particularly for
culturally/linguistically diverse children from low socioeconomic backgrounds.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 3
Acknowledgements
We would like to thank the staff at Reach-Up of St. Cloud for their collaborating during this
study, and undergraduate student, Julia McClung, for her assistance during data collection and
analysis. We would also like to thank St. Cloud State University Office of Sponsored Programs
Student Research Grant Award. Finally, we would like to thank our family and friends without
which this study could never had existed.
This study is dedicated to the child that lost his life during the process of this study.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 4
Table of Contents
Chapter I: INTRODUCTION .........................................................................................................7
Chapter II: METHOD ....................................................................................................................17
Chapter III: RESULTS ..................................................................................................................22
Chapter IV: DISCUSSION ............................................................................................................28
Chapter V: CONCLUSION ...........................................................................................................36
References ......................................................................................................................................37
Appendixes ....................................................................................................................................46
Appendix A ................................................................................................................................47
Appendix B ................................................................................................................................48
Appendix C ................................................................................................................................50
Appendix D ................................................................................................................................54

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 5
List of Tables
Table 1 ...........................................................................................................................................23
Table 2 ...........................................................................................................................................24
Table 3 ...........................................................................................................................................25
Table 4 ...........................................................................................................................................26
Table 5 ...........................................................................................................................................27
Table 6 ...........................................................................................................................................32

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 6
List of Figures
Figure 1 ..........................................................................................................................................15

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 7
Chapter I: INTRODUCTION
Recently, research has been directed to improving the quality of early childhood care to
build and develop socio-linguistic foundations and promote overall learning (Levickis,
Girolametto, & Reilly, 2014). Early intervention, particularly before age 6, has been established
in literature for communication skills, because of a “critical period” of brain development at that
time (Uylings, 2006; Werker & Hensch, 2015). The irrefutable beneficial effects of early
intervention for communication skills has been demonstrated in auditory rehabilitation
(Campbell, Macsweeney, & Woll, 2014), autism (Webb, Jones, Kelly, & Dawson, 2014),
intellectual disability (Fujinaga, Shinagawa, Watanabe, Ogihara, Sasaki, & Hori, 2005), and
children “at risk” due to low socioeconomic status (Colmar, 2014).
A rising issue for early childhood centers developed for families from low socio-
economic status (SES) backgrounds is the culturally and linguistically diverse (CLD) families
whom they serve. For example, over 17% of children enrolled in the St Cloud “Reach-Up”
program are from CLD families. Of that percentage 58% have no receptive or expressive
English and the remaining 42% have only a “moderate” proficiency in English (Storm, personal
communication). Male infants and toddlers of this population are known to be at higher risk for
developing a language delay or disorder (Campbell, Dollaghan, Rockette, Paradise, Feldman,
Shriberg, & Kurs-Lasky, 2003; Letts, Edwards, Sinka, Schaefer, & Gibbons, 2013). Several
researchers have hypothesized this discrepancy may be because females develop at a more
accelerated rate than males.
Early childhood programs attempt to meet the needs of linguistically diverse families in a
functional way to promote a strong linguistic foundation. For example, when there is a
prominent language amongst the class of preschoolers that isn’t English, Head Start employs a
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 8
staff member that is a native speaker of that language to help promote the children’s first
language (L1). There is irrefutable evidence that promoting the development of the L1 in a
language learner helps to develop their second language (L2) (David, 2005; Murphy, 2014).
These programs would also benefit from an early intervention strategy to promote a strong
communication foundation within their infants and toddlers, no matter their first language.
The purpose of this research project is to investigate whether the implementation of Baby
Sign, is an effective early language facilitation program for low SES infants and toddlers from
CLD backgrounds.
Baby Sign History
The National Institute on Deafness and Other Communication Disorders (NIDCD) (2014)
defines American Sign Language (ASL) as a “complete, complex language that employs signs
made by moving the hands combined with facial expressions and postures of the body.”
According to NIDCD, ASL is primarily used by people in North America that associate
themselves with the Deaf1 and hard-of-hearing community. Within the past decade there has
been an increase of use of a simplified version of ASL with the targeted use as a means of early
communication with infants and toddlers (Nelson, White, & Grewe, 2012). There have been
several labels to refer to this method such as; deictic gesturing, symbolic gesture, sign training,
and Baby Sign. For the purposes of this research paper we will refer to this method as Baby
Sign.
Mueller, Sepulveda, and Rodriquez (2013) defined Baby Sign as facilitating
communication of normally developing hearing infants by early exposure to sign language.
Primarily, there is a use of functional everyday signs (i.e. cookie, water, more, all-done) that are
1 When the word “deaf” is capitalized (e.g. Deaf) it is a representation of someone who is deaf and associates
themselves with Deaf culture (i.e. other Deaf individuals, uses American Sign Language as a primary mode of
communication). It is also known as being “big D deaf.”
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 9
produced by a primary caregiver during optimal exposure times (e.g. feeding time and play
time). This production is initially done with the expectation of not having the sign immediately
reproduced by the child, but introduced as a symbol for an action and/or word. Over time, and
repeated use of the symbol by the caregiver within context-rich interactions, the child can easily
employ these Baby Signs, either separate from or in conjunction with verbalizations as a means
of communication.
Minnesota Head Start Association
The Minnesota Head Start Association Inc. established in 1987. The Administration for
Children and Families is a federally operated program that was established nation-wide in 1991
to provide quality childcare for families from low SES backgrounds to support infant and toddler
development. This federally operated program was established to identify and overcome issues
impacting the development of children within low SES populations. One program they have
established is providing affordable quality childcare for people with limited financial means.
This is important due to the lack of resources available for children of low SES background and
the negative impact it can have on their development (Levine, & Zimmerman, 2010).
Reach-Up of Central Minnesota in conjunction with the Minnesota Head Start
Association (MHSA) was established in 1979. This program specifically targets at risk families
with infants and toddlers to provide and facilitate support that is fundamental to early socio-
linguistic development. According to the Glossary of Education Reform the term “at risk”
encompasses any student that is considered to have a higher probability of academic failure
(Great Schools Partnership, 2014). Children from low SES tend to have limited exposure to
language (i.e. books, magazines, verbal language input) effecting their language development
(Clearfield & Jedd, 2013).

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 10
The goal of Reach-Up is to facilitate the development in children across all areas (e.g.
motor, cognitive, language, social, behavior) to ensure a successful transition to school. Within
the infant and toddler curriculum there are opportunities for sensory experiences, literacy
exposure, cognitive decision making, fine and gross motor activities, and communicational
attempts (Minnesota Head Start Association Inc., 2014). This curriculum was specifically
designed to address the areas of common deficits found for infants and toddlers from CLD
and/or low SES families, in particular, language delays.
Implications of Low SES and CLD for Early Language Development
It has been noted that children from a low SES background are at risk for developing a
language delay (Clegg & Ginsborg, 2006). It is believed that, due to a lack of parental
education, in combination with minimal resources, children experience a language-impoverished
environment (Clegg & Ginsborg, 2006). Common resources and experiences not available to
CLD or low SES children include, but are not limited to, literacy materials such as picture books,
social interactions with other children within their peer groups, appropriate verbal parental
interactions, and motor and sensory stimuli such as age-appropriate toys.
Researchers Letts, Edwards, Sinka, Schaefer, and Gibbons (2013) described the marked
differences in language development in children from a low SES background compared to their
middle-high SES peers. They found characteristics of less developed phonological inventory and
early literacy skills (i.e. page turning, finding the title) in children from low SES background.
They reasoned that when the maternal figure’s education level is of high school equivalent or
lower, a child’s language is more likely to fall behind. They further argued that, “any negative
influence of low SES on early language development may then indirectly affect the child’s life-
long educational prospects.”
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 11
In agreement with this research, Downing and Ollila (1977) reported that children from
low SES typically have less exposure to speech, writing, and/or print until they enter school.
The authors stated that when children aren’t exposed to speech, writing, and/or print at home at a
young age they don’t develop necessary pre-literacy skills as a foundation for learning to read
and consequently fall behind.
In addition to low SES, it has been noted that children from CLD backgrounds are at risk
for language delays (Clifford, Rhodes, & Paxton, 2014). People of this population typically have
limited resources to support their dual language learning children, and it has been found that few
parents in this population are aware that programs exist to help facilitate dual language learning
(Woolfenden, 2014).
Bilingual language learning is considered a risk factor not specifically because of the
complexities of learning two spoken languages simultaneously, but the diverse conditions the
child may experience while this dual language learning is occurring (Kohnert, 2008). Researcher
Kathryn Kohnert (2008) describes potential risk factors such as: age when dual language input
first occurs (e.g. easier to acquire when exposed during infancy), the environments in which
language exposure is taking place (i.e. home, television, school), the ‘social prestige’ and
community support given for both languages (i.e. if one language is considered more useful), if
these languages share any commonalities (i.e. both are romantic languages), and the specific
purpose these languages serve (e.g. communication in public vs. home).
Typical language developmental milestones are met in multi-linguistic populations,
consistent with their monolingual peers, as long as there is a strong foundation in the L1 (Janet,
2009) and environmental support is evidenced (Bohman, Bedore, Peña, Mendez-Perez, &
Gillam, 2010). However, the problem lies when typical English Language Learners (ELL) are

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 12
not as proficient at English as their monolingual peers causing academic difficulties especially in
grades pre-k through second grade (Paradis, Emmerzael, & Duncan, 2010; Lindholm-Leary,
2014).
Typical Language Developmental Milestones
Language acquisition has a typical developmental pattern that corresponds to a child’s
age. Milestones of language acquisition can be broken down to three major areas: pre-linguistic
(birth to 18 months), emergent (18-36 months), and developing (2-5 years of age; Paul &
Norbury, 2012). For the purposes of this study, we will focus on the milestones that correspond
to the later pre-linguistic stage, and the early emergent stage.
From birth to 8 months infants evidence perlocutionary speech acts consisting of
vegetative sounds, cooing, laughing, quasi-resonant nuclei, vocal play, canonical and
reduplicated babbling (Chapman, 2000; Miller, 1981; Gordon-Brannan & Weiss, 2007). By the
time an infant reaches 11-18 months of age (locutionary speech acts) they should have the ability
to comprehend 3-50 words and should also be producing their first true words. When an
infant/toddler reaches approximately 24 months of age they are producing at least 50 words and
up to 300 words expressively (Chapman, 2000; Miller, 1981; Gordon-Brannan & Weiss, 2007).
When discussing the role gestures play in relation to language development, researchers
Goodwyn, Acredolo, and Brown (2000) discussed that “the onset of intentional communication
is signaled by a small set of gestures which essentially launch the child into purposefully
communicating with others.” Gestures used for the intentional communication, or deictic
gestures, begin to occur as a language milestone around 10 months of age (Bates, 1976; Bates,
Benigni, Bretherton, Camaioni, & Volterra, 1979; Goodwyn et al., 2000). With the onset of
‘deictic gesturing’ and the lack of fine motor control necessary for proficient verbal

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 13
communication, there are several months, in infancy, where intentional communication and
verbal ability are disjointed. With the complexities involved in spoken language development
there seems to be a supplementation of gesturing by infants/toddlers as a means to communicate
(Goodwyn et. al, 2000).
Importance of Symbolic Gesture
When a child points to an object a caregiver doesn’t disregard this action as one of little
importance. Just the opposite, the caregiver recognizes this as a communication attempt, and
goes through a trial and error series to understand what the child may be referring to. The use of
gesturing as a pre-linguistic and emergent means of communication is one that should not be
overlooked rather, substantiated as a way to promote overall communication in infants and
toddlers. Iverson and Goldin-Meadow (2005) reported
Gestures that children produce early in language development provide a way for them to
communicate information that they cannot yet express verbally, offering children a
technique for referring to objects before they have words for those objects (p. 367).
Bates, Thal, Whitesell, Fenson, and Oakes (1989) explain that by the age of 18 months
the majority of children have come to the realization of the symbolic meaning of words, that
words can be used to represent objects in the world. By promoting the use and understanding of
gestures a caregiver is facilitating information that aids in the acquisition of verbal
communication. Goodwyn et al. (2000) proposed that, just as crawling serves as a critical
stepping-stone to walking, gestures serve the same purpose for speaking.
Bates et al. (1979) viewed gestures as a variant of symbolic communication and that
when communication was attempted intentionally, utilizing ‘conventional signals,’ it is a
‘process that precedes, correlates with, and hence possibly contributes to the emergence’ of

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 14
language. Based on the evidence and research of the authors reviewed above, the main premise
of this paper is that promoting the use of symbolic gesture through utilizing Baby Sign will
facilitate a child’s intentional expressive attempt at communicating, and furthermore their spoken
vocabulary.
Constructivist Theory
It has been theorized that one way children acquire linguistic knowledge is from exposure
to environmental input (Boyd & Goldberg, 2009; MacWhinney, 2004; Piaget, 2002; Ratner,
2013). This theory has several names but is most frequently called the Constructivist approach
(a.k.a. Interactionist or Empiricist approach). According to Owens (2012) a communication base
is established first, namely nonverbal communication (e.g. gestures), then a child is able to build
upon that framework to eventually communicate verbally. This building occurs over time with
environmental exposure (i.e. caregiver input). This theory is primarily attributed to Jean Piaget
and Lev Vygotsky who theorized that more information could be obtained through child play
(Pass, 2007; see figure 1).
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 15
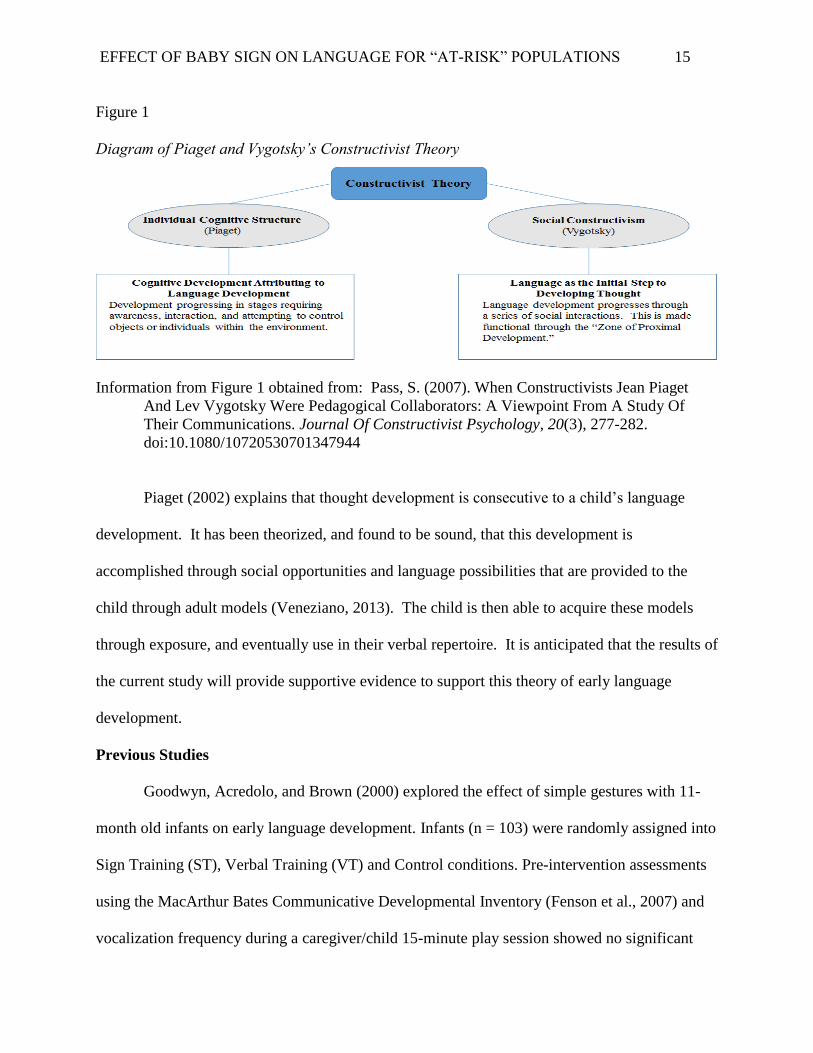
Figure 1
Diagram of Piaget and Vygotsky’s Constructivist Theory
Information from Figure 1 obtained from: Pass, S. (2007). When Constructivists Jean Piaget
And Lev Vygotsky Were Pedagogical Collaborators: A Viewpoint From A Study Of
Their Communications. Journal Of Constructivist Psychology, 20(3), 277-282.
doi:10.1080/10720530701347944
Piaget (2002) explains that thought development is consecutive to a child’s language
development. It has been theorized, and found to be sound, that this development is
accomplished through social opportunities and language possibilities that are provided to the
child through adult models (Veneziano, 2013). The child is then able to acquire these models
through exposure, and eventually use in their verbal repertoire. It is anticipated that the results of
the current study will provide supportive evidence to support this theory of early language
development.
Previous Studies
Goodwyn, Acredolo, and Brown (2000) explored the effect of simple gestures with 11-
month old infants on early language development. Infants (n = 103) were randomly assigned into
Sign Training (ST), Verbal Training (VT) and Control conditions. Pre-intervention assessments
using the MacArthur Bates Communicative Developmental Inventory (Fenson et al., 2007) and
vocalization frequency during a caregiver/child 15-minute play session showed no significant

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 16
group differences. Caregivers in the ST group implemented symbolic gestures (e.g. fish, flower)
daily while VT caregivers targeted specific words (e.g. kitty, doggy). After 25 months it was
found that the ST experimental group significantly outperformed other groups in all areas of
language. Other studies have also found similar beneficial outcomes of implementing Baby Sign
during infancy on language development (Bates’ et al., 1989; Iverson & Goldin-Meadow, 2005;
Mueller’s et al., 2014).
Objective
Mueller and Sepulveda (2014) reported that the popularity of Baby Sign is increasing
despite a lack of “empirical” research supporting its use. Although there are many claims to the
benefits of incorporating Baby Sign as an alternative mode of communication for a child, there is
still a need for more research to substantiate these claims. In particular there is a paucity of
research regarding the effectiveness of early intervention strategies for low SES or CLD
populations (Kohnert, 2008).
Therefore, the primary objective of this research paper was to investigate whether the
implementation of Baby Sign is an effective early language facilitation program for low SES
infants and toddlers from CLD backgrounds.
Research Hypothesis
Based on the Constructionist Approach theoretical framework proposed by Boyd &
Goldberg (2009) it was predicted that infants, from “at-risk” populations, exposed to Baby Sign
during a critical period of linguistic development would demonstrate an improved receptive and
expressive vocabulary relative to matched controls.
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 17
Chapter II: METHOD
Research Design
Originally, the study was devised as a mixed experimental design with both within-group
and between-group comparisons. Interpretive statistics (ANOVA comparisons) were planned to
compare the results for parent-child dyads randomly assigned to experimental (Baby Sign) vs.
control conditions (fine motor skill training). Due to unforeseen difficulties with participant
recruitment and mortality, the study became a case study (see Discussion).
Screening Criteria
Infants participating in this program were screened by the Reach-Up staff with the Ages
& Stages Questionnaires and Ages & Stages Questionnaires: Social Emotional (Squires,
Twombly, Bricker, & Potter, 2009), as well as regular hearing/vision screenings. Participants had
ongoing developmental assessment by the Teaching Strategies Gold (Heroman, Burts, Berke &
Bickart, 2010) performed by Reach-Up staff.
Participants were excluded if they did not meet the age criteria specified and/or if the
parents did not agree to sign the participation waiver. Participants were not excluded from the
study if found to have previous use of Baby Sign, more than one language spoken in the home,
multiple (3 or more) ear infections prior to the study, or any language/developmental delays.
Participants
Participants were families participating in the Reach-Up Head Start of Minnesota
program. Participants self-selected by responding to flyers distributed by the director, teachers,
or home visit staff. Written informed consent was obtained and all participants were treated
according to ethical treatment of vulnerable human participant guidelines established by St
Cloud State University (Appendix A). Three parent-child dyads passed the screening criteria and
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 18
began the study. Data from one of the parent-child dyads was excluded because the dyad
withdrew from the study before completion.
Participant 1 (P1). P1 was a multi-cultural male of African American and Caucasian
decent, and had English spoken by both parents in the home. The mother reported to have
delivered P1 at full-term with no complications during pregnancy or birth. Prior to the study P1
had met all developmental milestones, had no significant health related problems, and had no
immediate (mother/father) family history of speech/language difficulties. P1 had previous
exposure to the following Baby Signs: milk, mom, dad, and ball.
Participant 2 (P2). P2 was a multi-cultural male of Caucasian and Hispanic
(Ecuadorian) decent, and had English spoken by the mother and English/Spanish spoken by the
father in the home. The mother reported to have delivered P2 at full-term with no complications
during pregnancy or birth. Prior to the study P2 had achieved all developmental milestones, had
no significant health related problems, and had no immediate (mother/father) family history of
speech/language difficulties. P2 had no previous exposure to Baby Signs.
Tasks and Procedures
Both the initial and post-training evaluations were completed by a graduate student in a
speech-language pathology program, and supervised by a licensed speech language pathologist
certified by the American Speech Language Hearing Association. Assessments were completed
in a small quiet room with both caregiver and the child present.
Baseline Measures. To assess the comparability of both participants at the beginning of
the study, both participants were compared on several demographic variables and baseline
language and communication measures similar to the study previously done by Goodwyn,
Acredolo and Brown (2000). Demographic variables included birth order, sex, and
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 19
maternal/paternal education (4 – pt scale: 1 = high school or less; 2 = some college; 3 = college
graduate; 4 = post-graduate work). The language measures at 10 months of age included:
participant history screening form (see Appendix B), maternal report of verbal and gestural
vocabulary (MacArthur Bates Communicative Developmental Inventory or CDI; Fenson et al.,
2007), the infants’ auditory comprehension and expressive communication from a standardized
assessment (Preschool Language Scale – 4th Ed. [PLS-4]; Zimmerman, Steiner & Pond, 2002),
and a measure of vocalization, joint attention, and communication attempt frequency during a
10-minute play session.
The reliability and validity of the standardized, norm-referenced measures are well
established (Mancilla-Martinez, Pan & Vagh, 2011; Qi & Marley, 2011). Previous studies
examining early language acquisition have employed both the PLS-4 (Volden et al., 2011) and
the CDI (Mancilla-Martinez, Pan & Vagh, 2011; Reilly et al., 2009) and found significant
differences on these assessment instruments after an intervention. No significant comprehensive
differences were found between P1 and P2. At the end of the initial assessment parents of P1 and
P2 scheduled their training session2.
Baby Sign Training. Parents completed an initial 30 minute seminar and, jointly with
the Primary Investigator (PI), designed a daily practice routine for implementation of the training
at home. The seminar included a video of the PI explaining the importance of early language
development and tips for implementing the Baby Sign (e.g. get down on the child’s level, be sure
to have the child’s attention, show child an item out of child’s reach, produce the sign with its
verbal counterpart simultaneously, wait for response from infant, produce sign/word again
assisting infant in production of sign, and then give infant item being withheld). After the video
2 P2 was assessed in the Spanish versions of the MacArthur Bates and PLS-4 for any discrepancies across languages.
No discrepancies were found between English and Spanish for P2.
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 20
the PI reiterated the process, and asked the parent to explain the process to verify understanding.
Five signs, unique to each child, were selected by the parent and the PI jointly for each parent-
child dyad to practice. Signs selected were words/signs that were not previously produced by the
child, but signaled a commonly occurring message in the child’s daily routine (e.g. all-done,
more, milk). Parents were given a book of common Baby Signs, which included their five signs
as well as others (Briant, 2004). Each target Baby Sign was highlighted within the book for easy
referral. Parents were asked to demonstrate production of all of the five signs, and also
demonstrated the implementation of one sign to check for understanding of process. When
completed, the PI explained the parent log (see Appendix C) and established with parents the
optimal times of day and frequency of implementing each sign (i.e. feeding time, play time, 3-5
times daily per sign were suggested). Parents and the PI then established the most convenient
day/time to call for bi-weekly phone interviews (i.e. during infant nap time).
Qualitative and Quantitative Phone Interviews. Parents were contacted bi-weekly
during the 14-week training period to ensure they were maintaining the training protocol.
During this conversation a list of specific questions were asked (see Appendix D). The first
interview was preformed one week post-training. The interview collected information about
parent feelings and perceptions of the training program, as well as frequency and implementation
of Baby Signs.
Post-Training Evaluation. At the conclusion of the 14-week training period both
participants completed a 60-minute post-training evaluation. The post-training evaluation
included re-administration of the PLS-4, the CDI, and a 10-minute video-recorded free play
session with the caregiver.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 21
Dependent Variables. Dependent variables of performance on the task included scores
on the CDI and PLS-4 as well as the number of vocal attempts, sign attempts, joint attention, and
total communication attempts within the 10-minute play sample.
Speech samples were video and audio recorded, and all types of communication attempts
were analyzed off-line3 by the PI. The PI counted the total number of each type of attempt for
each minute of interaction. A second rater (BR), blind to the conditions of the study, also
analyzed the recordings in one-minute intervals. Percentage agreement was calculated between
the two raters for 25% of the samples to determine inter-rater reliability and to minimize
investigator bias.
3 Not in real time.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 22
Chapter III: RESULTS
A total of 3 parent-child dyad participants were recruited to participate in this study. Due
to attrition, 1 participant dyad left the study, the remaining 2 dyads continued the study in its
entirety. Both participants were initially screened at 9-months 24-days old.
Screening Results
Based upon previously discussed criteria during the screening process (see Methods), it
was deemed that both participants were appropriate subjects for this study. The following data
was collected through: parent interview, 10-minute play sample, CDI, and the PLS-4. After
initial qualitative data was collected, ongoing data was collected through bi-weekly parent phone
calls. P1 conducted re-assessments 14-weeks post-intervention using the same assessments from
the initial assessment. Due to scheduling complications, P2 was re-assessed 16-weeks post-
intervention.
Pre-Post Percentiles for CDI
Analysis was conducted using the results acquired through the use of the CDI. The CDI
assesses the child’s current abilities through the use of Early Words (e.g. Phrases Understood,
Words Understood, and Words Produced), and Actions and Gestures (e.g. Total Gestures). The
results are then represented through a percentile rank when compared to other same-aged peers.
Both participants’ results from pre-intervention and post-intervention are depicted below (see
Table 1).

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 23
Table 1
Pre-Post Intervention Results for CDI
Participant Category of Language Pre-
Intervention
Percentile
Post-Intervention
Percentile
Change
(+/-)
P1 Part I: Early
Words
Phrases
Understood
35% 55% +20%
Words
Understood
60% 65% +5%
Words
Produced
65% 80% +15%
Part II:
Actions and
Gestures
Total
Gestures
65% 85% +20%
P2 Part I: Early
Words
Phrases
Understood
50% 75% +25%
Words
Understood
65% 45% -25%
Words
Produced
55% 55% No
change
Part II:
Actions and
Gestures
Total
Gestures
40% 45% +5%
Both participants showed a percentile rank increase between 20-25% in Phrases
understood, and 5-20% in Total Gestures used when analyzed with the CDI.
Pre-Post Standardized Scores and Percentiles for PLS-4
Analysis was conducted using the results acquired through the use of the PLS-4. The
PLS-4 assesses the child’s current abilities in subtests entitled Auditory Comprehension,
Expressive Communication, and Total Language Scores. The results are then analyzed and
represented through standardized scores (SS) and percentile ranks when compared to other same-
aged peers. Both participants’ results from pre-intervention and post-intervention are depicted
below (see Table 2).

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 24
Table 2
Pre-Post Intervention Results for the PLS-4
Participant Category of
Language
Pre-
Intervention
SS
Post-
Intervention
SS
Pre-
Intervention
Percentile
Rank
Post-
Intervention
Percentile
Rank
P1 Auditory
Comprehension
93 117 32 87
Expressive
Communication
98 120 45 91
Total Language
Score
100 121 50 92
P2 Auditory
Comprehension
103 109 58 73
Expressive
Communication
97 113 42 99
Total Language
Score
100 113 50 81
Both participants showed an increase in standard score on receptive (Auditory
Comprehension) language (P1 increased 24 points and P2 increased 6 points), Expressive
Language/Communication (P1 increased 28 points and P2 increased 16 points), and Total
Language Scores (P1 increased 21 points and P2 increased 13).
Pre-Post Analysis of Video-Recorded Interaction Samples
Analysis was conducted using the number of vocal attempts, sign attempts, joint
attention, and total communication attempts within the 10-minute play video recorded samples.
A rater (BR), blind to the study, was trained in the video recording analysis (e.g. vocal attempts,
sign attempts, and joint attention). BR’s results were then compared to the PI’s analysis results.
This comparison is depicted below (see Table 3).

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 25
Table 3
Results of 10-minute Communication Sample
Video Rater
Vocal
Attempts
Rater
Consist-
ency
Sign
Attempts
# of Joint
Attention
Occur-
rences > 2
seconds
Rater
Consist-
ency
# of
conversational
turns > 2
P1V1
Julia
(Blind
Rater) 52 96.29% 0 14 85.70% 2
P1V1 Sarah 54 96.29% 0 12 85.70% 3
P1V2
Julia
(Blind
Rater) 18 94.40% 0 13 94.40% 3
P1V2 Sarah 17 94.40% 0 13 94.40% 2
P2V1 Sarah 5 N/A 0 10 N/A 0
P2V2 Sarah 15 N/A 1 (reach) 10 N/A 0
Neither of the participants showed change in joint attention, sign attempts, or number of
conversational turns greater than two. P1 showed a decrease in vocal attempts from
approximately 53 to approximately 18, whereas, P2 showed an increase of vocal attempts from 5
to 15. However, we do not consider these vocal attempts to be significant. Rather they match
appropriately to participants’ activity choice during the 10- minute segment (e.g. P1 Video 1
pulling items from a box/bin and handing them to parent, P1 Video 2 walking items from one
room to the next, P2 Video 1 book reading with parent, P2 Video 2 removing items from a
box/bin and showing them to parent).
Interview Results
Scheduled interviews were initially set up to take place bi-weekly to help reinforce the
continued use of the targeted intervention, identify barriers, and monitor progress made. It was
found during each interview that both participants reported the intervention as going “good.” It
was also found that both participants would recommend this form of intervention to other

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 26
parents. P2 reported this intervention as being “an easy way to communicate with your child
before they can talk…very cool to have that communication already.” Both participants reported
the results of the intervention being “exciting” to watch, and beneficial to their child’s ability to
receive and express communicatively. Additionally, both participants found that intervention
was most efficient during feeding time and it provided more opportunities for models of the
signs. Lastly, both participants referred to the positive benefits of explaining how their child was
communicating with others (i.e. signing to friends and family). P1 reported that her family was
“really impressed by him being able to sign.”
P1. P1 participated in 5/7 phone interview opportunities. Due to several barriers (i.e.
participant’s phone disconnected, unavailable to answer the phone, unable to return phone call)
two phone interviews did not take place. A portion of the results collected during the interviews
are reported in the table below (see Table 4).
Table 4
Results of P1 Phone Interviews
Date Avg. #of times
signs were
modeled
Ideal time to
model signs
Avg. # of signs
attempted by
child
Signs produced with or
without vocalization?
6-17 3-5x per day Feeding/play 1 Without
7-1 3-5x per day Feeding/play 3 Without
7-27 3-5x per day Feeding 4 With
8-12 2-3x per week Feeding 4 With
9-3 2-3x per week Feeding 5 With
P1 showed a notable increase in the average number of signs attempted and production of
signs with vocalization. P1 also showed a decrease in the number of models provided overtime
(3-5x per day to 2-3x per week).
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 27
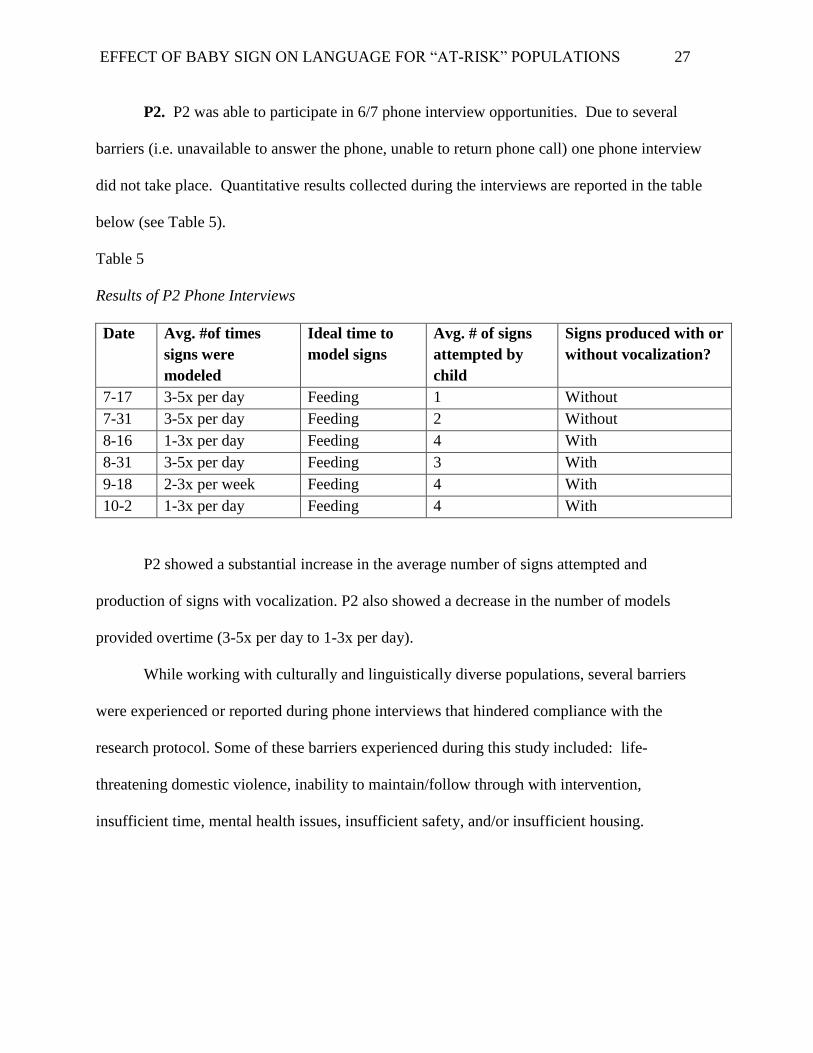
P2. P2 was able to participate in 6/7 phone interview opportunities. Due to several
barriers (i.e. unavailable to answer the phone, unable to return phone call) one phone interview
did not take place. Quantitative results collected during the interviews are reported in the table
below (see Table 5).
Table 5
Results of P2 Phone Interviews
Date Avg. #of times
signs were
modeled
Ideal time to
model signs
Avg. # of signs
attempted by
child
Signs produced with or
without vocalization?
7-17 3-5x per day Feeding 1 Without
7-31 3-5x per day Feeding 2 Without
8-16 1-3x per day Feeding 4 With
8-31 3-5x per day Feeding 3 With
9-18 2-3x per week Feeding 4 With
10-2 1-3x per day Feeding 4 With
P2 showed a substantial increase in the average number of signs attempted and
production of signs with vocalization. P2 also showed a decrease in the number of models
provided overtime (3-5x per day to 1-3x per day).
While working with culturally and linguistically diverse populations, several barriers
were experienced or reported during phone interviews that hindered compliance with the
research protocol. Some of these barriers experienced during this study included: life-
threatening domestic violence, inability to maintain/follow through with intervention,
insufficient time, mental health issues, insufficient safety, and/or insufficient housing.
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 28
Chapter IV: DISCUSSION
The results of the present study support the research hypothesis that infants, from “at-
risk” populations, exposed to Baby Sign during a critical period of linguistic development would
demonstrate an improved receptive and expressive vocabulary relative to matched controls. In
addition, these results also support the constructivist theory suggesting that one way children
acquire linguistic knowledge is from exposure to environmental input (Boyd & Goldberg, 2009;
MacWhinney, 2004; Piaget, 2002; Ratner, 2013).
Research Design
Due to unforeseen difficulties with participant recruitment and mortality the study
became a case study. Some of the strengths of conducting a case study include: getting a more
thorough understanding of the participant’s emotional and environmental needs instead of just
the notation of exhibited behaviors, as well as the allowance for creativity and innovative therapy
approaches. In addition, case studies can be used as a basis for theory in clinical application, and
they allow for direction in further research (Portney & Watkins, 2009).
However, as with any study design, case studies have several drawbacks as well. Some
drawbacks of utilizing a case study include difficulty justifying that the outcomes of the study
were solely produced from the experimental variable, and not from an outside variable. For
example, a case study design does not allow control for improvement due to maturation.
However, utilization of the norm-referenced PLS-4 assessment test allowed comparison of
participants with same-age peers to, at least partially address this confound. With larger studies
it is easier to determine the effectiveness of treatment based on the magnitude of participant
outcomes. When the participant size is smaller there is more to be justified when providing

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 29
supportive evidence for the experimental variable outcome (i.e. listing all possible variables and
how they impact the study results; Portney & Watkins, 2009).
Initially, we had anticipated having a larger subject size (6-12 subjects), but had
challenges recruiting participants within our criteria and experienced attrition. Had we known
prior to our study the participant size would result in two parent-dyads we would have
implemented a single-subject experimental research design with multiple baselines across
subjects because of the strengths of this design. Within a multiple baseline design, by providing
and removing treatment for a length of time, researchers have an opportunity to observe the
effects that therapy provides. In addition, this type of research design provides the ability to rule
out any other subsequent, non-therapy behaviors that may be affecting the outcome (Morgan &
Morgan, 2009).
CDI
Support for the research hypothesis was evidenced by the notable increase in receptive
and expressive language outcomes captured by the CDI. Results of the CDI Early Words showed
an increase of percentile rank for both participants (P1, 20%; P2, 25%) in Phrases Understood,
and an increase of percentile rank for Total Gestures when compared to same-aged peers (P1,
20%; P2, 5%). These results mirror those found in previous research (Goodwyn, Acredolo, &
Brown, 2000; Suanda & Namy, 2013).
However, it should be noted that there was a decrease in the Words Understood
percentile rank for P2 (25%) on the CDI, which was not consistent with the results of previous
research (Suanda & Namy, 2013).
This difference could be accounted for in several ways. For example, this effect may be
due to the parents’ habitual use of phrases with the determiner/pronoun “that” with their child

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 30
versus specific words (i.e. “bring me that” vs. “bring me the ball”). Parent 2 reported in
interviews that she was, at times, unsure if her child knew the specific words, but she was
confident in knowing that her child understood phrases clearly at the post-intervention
assessment. The results for single words understood may not be representative to P2’s skill level
at the time. A clinician-administered vocabulary test/screening may have been useful as a
supplement to parent reported treatment outcome measures and may have captured different
results for this area of development.
PLS-4
Results of the PLS-4 expressive and receptive language showed a substantial increase in
standard scores by both participants on Auditory Comprehension (P1 increased 24 points and P2
increased 6 points), Expressive Communication (P1 increased 28 points and P2 increased 16
points), and Total Language Scores (P1 increased 21 points and P2 increased 13). Language
improvements found on standardized tests were also found by the information collected during
continued bi-weekly phone interviews. Results from these two data sources support the research
hypothesis and constructivist theory. These results are similar to those found by researchers
Goodwyn, Acredolo, and Brown (2000). For example, these researchers also found that there
was a significant increase in receptive and expressive language when compared to both of their
control groups (verbal training and non-intervention).
Video-Recorded Interactions
Results of the 10-minute video showed that both participants had no change in joint
attention, sign attempts, or number of conversational turns greater than two. P1 showed a
decrease in vocal attempts from approximately 53 to approximately 18, whereas, P2 showed an
increase of vocal attempts from 5 to 15. Vocal attempts captured in one 10-minute video pre and

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 31
post-treatment did not appear to reliably reflect participants learning or the experimental effect.
Rather, communication attempt frequency tended to correspond to participants’ activity choice
during the 10- minute segment (e.g. P1V1 pulling items from a box/bin and handing them to
parent, P1V2 walking items from one room to the next, P2V1 book reading with parent, P2V2
removing items from a box/bin and showing them to parent).
The finding that short videos were not optimal measures for detecting experimental
effects is not unexpected. Researchers Goodwyn, Acredolo, and Brown (2000) also indicated
that the information collected during their video play segments was insightful, but did not
indicate any significant change for participants in the earliest age group. They concluded,
however, that more reliable data and significant changes in communication behavior during
infant video-recorded play was for subjects 24-months of age or older. This finding suggests that
parent interview and report may serve as more valid and reliable measures of communication
change of over time for children younger than two. This finding also suggests that a range of
different measures, including clinician-administered standardized tests, parent report, and video
are necessary to get a true picture of child communication changes.
Interview Results
The research hypothesis was also supported by the information collected during bi-
weekly phone interviews. These results were similar to those found by researchers Goodwyn et
al., 2000). Goodwyn et al. (2000) reported that subjects in their “sign training” group out
preformed their same aged subjects in their control group in receptive, expressive, and non-
verbal communication (p. 94-96).
Results of the bi-weekly phone interview showed a noteworthy increase in the average
number of signs attempted and production of signs with vocalization with both P1 and P2. Both

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 32
participants also showed a decrease in the number of models provided over time. This indicated
that the number of models needed for the participants to successfully engrain the newly acquired
signs decreased as the signs became more habitual and generalized. Results indicated that the
ideal modeling time for both participants over time was during feeding. This could be due to the
direct one-on-one attention received by the participants, and their parents’ ability to hold the
participants’ attention for a length of time. This finding indicated that future interventions
planned for children of this age in the home may consider implementing/training strategies
around regular home routines such as feeding.
Implications for Future Studies
Data acquired through phone interviews, and entering the home, also suggested several
barriers to the study when working with at-risk populations (e.g. phone being disconnected, not
always modeling signs daily, life threatening domestic violence, insufficient time). These results
had important implications for future studies to consider when working with these populations
(see Table 6)
Table 6
Implications for Future Studies
Concerns While Entering
the Home
Loss and Mandated Reporting Barriers
Primary Investigator safety Child safety Domestic violence
Disarray and disorder in the home
(e.g. food remnants and clothing on
the floor)
Mandated Reporting of abuse and
neglect
Housing relocation
Aggressive behavior from family
members
Loss of life Phone disconnection

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 33
Disconnected Phone. In one instance, the PI attempted to call P1 several times over a 2-
week period where the P1’s phone services were disconnected. This instance affected the ability
to collect data effectively (both qualitative and quantitative). In addition, this experience
appeared to initially cause some embarrassment for P1’s mother the next time the PI was able to
make contact. The PI expressed to her that “these things happen,” which reassured the mother,
but it could be something that could negatively impact future studies (i.e. attrition).
Concerns While Entering the Home. In another instance, the PI and an assistant went
to a participant’s home. This home was overwhelmingly in disarray. It was difficult for the PI
the assistant to find a place to sit due to the abundance of toys, clothing, food remnants, and
garbage that littered the floor. This did not seem to upset the children and/or parents, but it did
make it difficult for the PI and the assistant to assess, train, and collect data affectively. It was
difficult to ensure standardized/regulated assessment conditions. The participant would play
with toy items that were not brought by the PI/assistant, and the participant would put food items
into their mouth that had been sitting on the floor for an undetermined amount of time. The
PI/assistant would assist the parent often by removing the food items, and asking if they could
move some toys/clothes to an area out-of-reach. However, future researchers should be aware of
these potentials issues, and devise a plan in case they run into similar issues.
There were moments of concern for the investigators when the PI and assistant entered a
participant’s home. The PI followed the protocol of calling someone, to let them know where
they were going, how long they would be gone, and that they would call when the PI was out of
the home. This was done for the safety of the PI and assistant. The participants lived in areas
that were known to have frequent crime, and safety was important to consider. Additionally,
several participants’ mothers had significant others with a history of aggressive behavior. Future
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 34
studies should consider a similar protocol for investigators’ safety, and have a system in place for
immediate assistance if in danger (i.e. texting an outside source to call the police).
There were moments of concern for the participants when the PI entered the home. One
of these concerns was due to the older siblings being physically aggressive towards the
participants (i.e. pushing, pulling, hitting, throwing toys). There were several instances where
the parent needed to interfere on the participant’s behalf. These situations were potentially fatal,
and were not always swiftly remedied by the observing parent. Lastly, one participant’s parent
(not involved in the study) had a known history of aggression and drug use. Even though this
parent was not a part of the household at the time, it is important to consider in case that parent
should return. It should be recommended that researchers be prepared for situations in which
mandated reporting are necessary.
Loss and Mandated Reporting. Researchers should also be prepared for the loss of a
participant. Due to the risk of domestic abuse and heightened stress in these populations it is
important for researchers to know that there is a chance were their participant could be
physically harmed and/or die. During the course of this study one potential participant lost their
life due to domestic abuse. This event happened 3 days prior to the PI going into the infant’s
home. Throughout the study the PI had grown to know the participant and their family well.
The news of the death was devastating.
It is important for future researchers to consider the possibility of domestic abuse, infant
neglect, and harm done to the investigators. The safety of the research team and participants
should not be taken lightly, and the investigators should know where to go if they should need to
seek other professional help (i.e. police, counselor, social work professionals).

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 35
Barriers. Additional qualitative results found during the phone interview, and
throughout the study, indicated several barriers while working culturally and linguistically
diverse populations. These barriers made it difficult and/or impossible for participants to access
early intervention services during this study. While some experienced a majority of the barriers
listed, all experienced at least three: life threatening domestic violence, participant resident
relocation, financial difficulty, child care, transportation, inability to maintain/follow through
with intervention, insufficient time, mental health issues, insufficient safety, and/or insufficient
housing. These barriers were significant findings to consider for any further research conducted
with similar populations.
Continued Research. The results found by this study have multiple implications, and
provide numerous areas of continued research. It is recommended that more research be
conducted in this area with more participants, longer duration, and additional measures.
Additional research may include a team approach including other professions such as social
work, physical and occupational therapy, and/or applied behavior analysts. In addition, with
longer duration, it is recommended that literacy should be another targeted area to be included in
a longitudinal study.
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 36
Chapter V: CONCLUSION
In summary, the results of this study support the research hypothesis that implementation
of Baby Sign as a form of early language development intervention for “at-risk” populations can
be beneficial to the infants/toddlers. More and more, early childhood center programs are
developed for families from low SES and CLD populations. Within these populations early
intervention is crucial for optimal language development. Results of this study further
substantiate the advantages found in the implementation of Baby Sign as a form of early
intervention for receptive and expressive language in infants of “at-risk” populations. However,
it is recommended that further, and more extensive, research be conducted to study the long-term
benefits of such an intervention within this population.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 37
References
Acredolo, L. P., & Goodwyn, S. W. (1985). Symbolic gesturing in language development: A
case study. Human Development, 28, 40±49.
Acredolo, L. P., & Goodwyn, S. W. (1988). Symbolic gesturing in normal infants. Child
Development, 59, 450±466.
Bates, E. (1976). Language and context: The acquisition of pragmatics. New York, NY:
Academic Press.
Bates, E., Benigni, L., Bretherton, I., Camaioni, L., & Volterra, V. (1979). The emergence of
symbols: Cognition and communication in infancy. New York: Academic Press.
Bates, E., Bretherton, I., Shore, C., & McNew, S. (1983). Names, gestures, and objects:
Symbolization in infancy and aphasia. In K. Nelson (Ed), Children’s language: Volume
IV (pp. 59-124). Hillsdale, NJ: Erlbaum.
Bates, E., Thal, D., Whitesell, K., Fenson, L., & Oakes, L. (1989). Integrating Language and
Gesture in Infancy. Developmental Psychology, 25(6), 1004-1019.
Briant, Monta Z. (2004). Baby Sign Language Basics: Early Communication for Hearing Babies
and Toddlers. Carlsbad, CA: Hay House Inc.
Bohman, T. M., Bedore, L. M., Peña, E. D., Mendez-Perez, A., & Gillam, R. B. (2010). What
you hear and what you say: language performance in Spanish-English
bilinguals. International Journal Of Bilingual Education & Bilingualism,13 (3), 325-344.
doi:10.1080/13670050903342019
Boyd, J. K., & Goldberg, A. E. (2009). Input Effects Within a Constructionist
Framework. Modern Language Journal, 93(3), 418-429. doi:10.1111/j.1540-
4781.2009.00899.x

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 38
Campbell, R., Macsweeney, M., & Woll, B. (2014). Cochlear implantation (CI) for prelingual
deafness: The relevance of studies of brain organization and the role of first language
acquisition in considering outcome success. Frontiers in Human Neuroscience, 8(OCT).
doi:10.3389/fnhum.2014.00834
Carpenter, M. & Liebal, K. Joint attention, communication, and knowing together in infancy. In
A. Seeman (ed). Joint attention: New Developments (in press).
Clearfield, M. W., & Jedd, K. E. (2013). The Effects of Socio-Economic Status on Infant
Attention. Infant & Child Development, 22(1), 53-67. doi:10.1002/icd.1770
Clegg, J., & Ginsborg, J. (2006). Language and social disadvantage: Theory into practice.
Hoboken, NJ, US: John Wiley & Sons Inc.
Clifford, V., Rhodes, A., & Paxton, G. (2014). Learning difficulties or learning English
difficulties? Additional language acquisition: An update for paediatricians. Journal of
Peadiatrics & Child Health, 50(3), 175-181. doi:10.1111/jpc.12396
Colmar, S. H. (2014). A Parent-Based Book-Reading Intervention for Disadvantaged Children
with Language Difficulties. Child Language Teaching and Therapy, 30(1), 79-90.
David, J. (2005). Head Start Embraces Language Diversity. Young Children, 60(6), 40-43.
Doherty-Sneddon, G. (2008). The great Baby Signing debate. The Psychologist, 21(4), 300-303.
Dowshen, S. A., Izenberg, N., & Bass, E. R. (2002). The Kidshealth Guide for Parents:
Pregnancy to Age 5. Chicago: Contemporary Books.
Edwards, C., & Willis, L. (2000). Integrating Visual and Verbal Literacies in the Early
Childhood Classroom. Early Childhood Education Journal, 27(4), 259.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 39
Fenson, L., Marchman, V. A., Thal, D. J., Dale, P. S., Reznick, J. S., & Bates, E. (2007).
MacArthur-Bates Communicative Development Inventories (2nd ed.). Baltimore:
Brookes.
Fujinaga, T., Shinagawa, R., Watanabe, C., Ogihara, M., Sasaki, T., & Hori, A. (2005). Early
Therapeutic Intervention for Down Syndrome Children, and Mothers' Attitudes toward
Childrearing. Japanese Journal of Developmental Psychology, 16(1), 81-91.
Goodwyn, S. W., & Acredolo, L. P. (1993). Symbolic gesture versus word: Is there a modality
advantage for onset of symbol use?. Child Development, 64(3), 688-701.
doi:10.1111/1467-8624.ep9308115009
Goodwyn, S. W., Acredolo, L. P., & Brown, C. A. (2000). Impact of Symbolic Gesturing on
Early Language Development. Journal of Nonverbal Behavior, 24(2), 81-103.
Gordon-Brannan, M. E., & Weiss, C. E. (2007). Clinical management of articulatory and
phonologic disorders. Philadelphia: Lippincott Williams & Wilkins, c2007.
Great Schools Partnership. (2014). The Glossary of Education Reform: For Journalists, Parents,
and Community Members. Retrieved from: http://edglossary.org/at-risk/.
Gunnar, M. R., & Donahue, M. (1980). Sex Differences in Social Responsiveness between Six
Months and Twelve Months. Child Development, 51(1), 262-265. doi:10.1111/1467-
8624.ep12325484
Heroman, D.C., Burts, K., Berke, T.S., Bickart. (2010) Teaching Strategies for Early Childhood.
GOLD. Baltimore: Paul H. Brookes Publishing.
Holmes, K.M., & Holmes, D. W. (1980). Signed and spoken language development in a hearing
child of hearing parents. Sign Language Studies, 28, 239-254.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 40
Iverson, J. M., & Goldin-Meadow, S. (2005). Gesture Paves the Way for Language
Development. Psychological Science (Wiley-Blackwell), 16(5), 367-371.
doi:10.1111/j.0956-7976.2005.01542.x
Janet F., W. (2009). Bilingual beginnings to learning words. Philosophical Transactions of the
Royal Society B: Biological Sciences, 364(1536), 3649-3663.
Kohnert, K. (2008). Language disorders in bilingual children and adults. San Diego, CA: Plural
Pub., c2008.
Levickis, P., Girolametto, L., & Reilly, S. (2014). Maternal behaviors promoting language
acquisition in slow-to-talk toddlers: prospective community-based study. Journal of
Developmental & Behavioral Pediatrics, (4). 274.
Levine, Phillip B. & Zimmerman, David J. (2010). Targeting Investments in Children: Fighting
Poverty When Resources Are Limited. University of Chicago Press.
doi:10.7208/chicago/9780226475837.001.0001
Letts, C., Edwards, S., Sinka, I., Schaefer, B., & Gibbons, W. (2013). Socio‐economic status and
language acquisition: Children's performance on the new Reynell Developmental
Language Scales. International Journal of Language & Communication Disorders, 48(2),
131-143.
Lindholm-Leary, K. (2014). Bilingual and Biliteracy Skills in Young Spanish-Speaking Low-
SES Children: Impact of Instructional Language and Primary Language
Proficiency. International Journal of Bilingual Education and Bilingualism, 17(2), 144-
159.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 41
Mancilla-Martinez, J., Pan, B. A., & Vagh, S. B. (2011). Assessing the Productive Vocabulary of
Spanish-English Bilingual Toddlers from Low-Income Families. Applied
Psycholinguistics, 32(2), 333-357.
MacWhinney, B. (2004). Emergent Language. In K. p. Trott, S. p. Dobbinson, P. p. Griffiths
(Eds.), The Child Language Reader (pp. 259-276). London, England: Routledge.
Morales, M., Mundy, P., Crowson, M. M., Neal, A., & Delgado, C. F. (2005). Individual
differences in infant attention skills, joint attention, and emotion regulation behaviour.
International Journal of Behavioral Development, 29(3), 259-263.
doi:10.1080/01650250444000432
Morgan, David L., & Morgan, Robin K. (2009). Single-Case Research Methods: for the
Behavioral and Health Sciences (pp. 127-134). Thousand Oakes, California: SAGE
Publications Inc.
Mueller, V., & Sepulveda, A. (2014). Parental perception of a Baby Sign workshop on stress and
parent–child interaction. Early Child Development & Care, 184(3), 450-468.
doi:10.1080/03004430.2013.797899
Mueller, V., Sepulveda, A., & Rodriguez, S. (2014). The effects of Baby Sign training on child
development. Early Child Development & Care, 184(8), 1178-1191.
doi:10.1080/03004430.2013.854780
Murphy, A. F. (2014). The Effect of Dual-Language and Transitional-Bilingual Education
Instructional Models on Spanish Proficiency for English Language Learners. Bilingual
Research Journal, 37(2), 182-194. doi:10.1080/15235882.2014.934971

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 42
Nelson, L. H., White, K. R., & Grewe, J. (2012). Evidence for Website Claims about the
Benefits of Teaching Sign Language to Infants and Toddlers with Normal Hearing. Infant
& Child Development, 21(5), 474-502. doi:10.1002/icd.1748
Normand, M. P., Machado, M. A., Hustyi, K. M., & Morley, A. J. (2011). Infant Sign Training
and Functional Analysis. Journal of Applied Behavior Analysis, 44(2), 305-314.
Owens, R. J. (2012). Language development: an introduction. Boston: Pearson, c2012.
Paradis, J., Emmerzael, K., & Duncan, T. S. (2010). Assessment of English language learners:
Using parent report on first language development. Journal of Communication
Disorders, 43(Clinics in Communication Disorders: Assessment and intervention of
bilingual children with SLI), 474-497. doi:10.1016/j.jcomdis.2010.01.002
Pass, S. (2007). When Constructivists Jean Piaget And Lev Vygotsky Were Pedagogical
Collaborators: A Viewpoint From A Study Of Their Communications. Journal of
Constructivist Psychology, 20(3), 277-282. doi:10.1080/10720530701347944
Piaget, J. (2002). The language and thought of the child. London; New York: Routledge, 2002,
c1959.
Leslie Portney, D. F., & Mary Watkins, D. M. (2009). Foundations Of Clinical Research.
Pearson Health Science.
Qi, C. H., & Marley, S. C. (2011). Validity Study of the Preschool Language Scale-4 With
English-Speaking Hispanic and European American Children in Head Start Programs.
Topics in Early Childhood Special Education, 31(2), 89-98. doi:
10.1177/0271121410391108

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 43
Ratner, N. (2013). Why talk with children matters: Clinical implications of infant- and child-
directed speech research. Seminars in Speech and Language, 34(4), 203-214.
doi:10.1055/s-0033-1353449
Reilly, S., Bavin, E., Bretherton, L., Conway, L., Eadie, P., Cini, E., & ... Wake, M. (2009). The
Early Language in Victoria Study (ELVS): a prospective, longitudinal study of
communication skills and expressive vocabulary development at 8, 12 and 24 months.
International Journal of Speech-Language Pathology, 11(5), 344-357.
Paul, R. & Norbury, C. (2012). LANGUAGE DISORDERS FROM INFANCY THROUGH
ADOLESCENCE. Elsevier Health Sciences.
Ruff, Holly A.; & Rothbart, Mary K. (1996). Attention in Early development: Themes and
variations. New York: Oxford University Press.
Suanda, S. H., & Namy, L. L. (2013). The Organization of Words and Symbolic Gestures in 18-
Month-Olds' Lexicons: Evidence from a Disambiguation Task. Infancy, 18(2), 276-288.
Tayloe Jr., D. T. (2009). What you need to know about your baby's development
milestones. Baby Talk, 74(3), 54. (MOTOR TASKS REF)
Tomasello, M., Carpenter, M., & Liszkowski, U. (2007). A new look at infant pointing. Child
Development, 78, 705-722.
Tomasello, M., & Farrar, J. (1986). Joint attention and early language. Child Development, 57,
1454-1463.
Uylings, H. M. (2006). Development of the Human Cortex and the Concept of "Critical" or
"Sensitive" Periods.Language Learning, 56(1), 59-90.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 44
Vallotton, C. D. (2012). Infant signs as intervention? Promoting symbolic gestures for preverbal
children in low-income families supports responsive parent–child relationships. Early
Childhood Research Quarterly, 27(3), 401-415. doi:10.1016/j.ecresq.2012.01.003
Veneziano, E. (2013). A cognitive-pragmatic model for the change from single-word to
multiword speech: A constructivist approach. Journal of Pragmatics, 56133-150.
doi:10.1016/j.pragma.2013.03.013
Volden, J., Smith, I. M., Szatmari, P., Bryson, S., Fombonne, E., Mirenda, P., & ... Thompson,
A. (2011). Using the Preschool Language Scale, Fourth Edition to Characterize Language
in Preschoolers With Autism Spectrum Disorders. American Journal of Speech-Language
Pathology, 20(3), 200-208. doi:10.1044/1058-0360(2011/10-0035)
Wagner, S. M., Nusbaum, H., & Goldin-Meadow, S. (2004). Probing the Mental Representation
of Gesture: Is Handwaving Spatial?. Journal of Memory and Language, 50(4), 395-407.
doi:10.1016/j.jml.2004.01.002
Webb, S. J., Jones, E. H., Kelly, J., & Dawson, G. (2014). The motivation for very early
intervention for infants at high risk for autism spectrum disorders. International Journal
of Speech-Language Pathology, 16(1), 36-42. doi:10.3109/17549507.2013.861018
Werker, J. F., & Hensch, T. K. (2015). Critical Periods in Speech Perception: New
Directions. Annual Review of Psychology, 66(6), 173-196. doi:10.1146/annurev-psych-
010814-015104
Woolfenden, S., Posada, N., Krchnakova, R., Crawford, J., Gilbert, J., Jursik, B., & ... Kemp, L.
(2014). Equitable access to developmental surveillance and early intervention -
understanding the barriers for children from culturally and linguistically diverse (CALD)

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 45
backgrounds. Health Expectations: An International Journal of Public Participation in
Health Care And Health Policy, doi:10.1111/hex.12318
Zimmerman, I.L., Steiner, V.G., & Pond, R.E. (2002). Preschool Language Scale (4th-edition).
US: Pearson Corp Inc.

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 46
Appendixes

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 47
Appendix A

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 48
Appendix B
Early Development Research Screening Form
Investigators: Sarah Anderson, M.S. Candidate, St Cloud State University
Julia McClung, B.S. Candidate, St Cloud State University
Sarah Smits-Bandstra, Assistant Professor, St Cloud State
University
Participant Screening Form to be filled out with Primary Caregiver
Date: __________________ Name of Child: _________________ Child’s Date of Birth: ____________ Name of Caregiver: __________________________ Gender: Male Female Email: _______________________
(optional) Telephone: Home: ______________ Address: ______________________________________________________ Current Profession: _____________ Highest Education Level:_________
Medical/Developmental History
1. Did your child have difficulty learning to hold their head up, sit up, make sounds,
reach and grab, crawl, or eat? Yes No If yes, please describe________________________________________
2. Do you have any concerns about your child’s hearing or vision?
If yes, please describe________________________________________
3. Is your child seeing a doctor regularly or taking any medication(s) for a disease or
disorder? Yes No If yes, please list them________________________________________

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 49
4. Has your child ever had seizures, epilepsy or fits? Yes No
5. Has your child even been in the hospital for a serious injury or illness (car accident,
head injury, meningitis, high fever)? Yes No If yes, please describe __________________________________________
6. To the best of your knowledge, did you or the child’s father ever have difficulty
learning to speak or learn in school as a child? Yes No If yes, please describe__________________________________________
7. . Is English your native language? Yes No
If not, what is/are your native language/s ___________________________
8. What languages are spoken to the child? 9. What language do you plan to use for the training?
10. Do you know any type of sign language? Yes No If yes, please describe__________________________________________
11. Do you use sign language with your child? Yes ٱ No ٱ
If yes, please describe__________________________________________
12. Do you or another person work with the child to improve their hand strength and
skill? Yes No If yes, please describe__________________________________________

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 50
Appendix C
Baby Sign Log
Days
Models
While
Eating/Feedi
ng
Response From
Child
Models
During Play
Response
From Child
WE
EK
1
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
2
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
3
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
4
Monday
Tuesday
Wednesda
y
Thursday
Friday

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 51
Saturday
Sunday

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 52
Days
Models
While
Eating/Feedi
ng
Response From
Child
Models
During Play
Response
From Child W
EE
K 5
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
6
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
7
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
8
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 53

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 54
Days
Models
While
Eating/Feedi
ng
Response From
Child
Models
During Play
Response
From Child W
EE
K 9
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
10
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
11
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
12
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 55

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 56
Days
Models
While
Eating/Feedi
ng
Response From
Child
Models
During Play
Response
From Child W
EE
K 1
3
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
14
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
15
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday
WE
EK
16
Monday
Tuesday
Wednesda
y
Thursday
Friday
Saturday
Sunday

EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 57
EFFECT OF BABY SIGN ON LANGUAGE FOR “AT-RISK” POPULATIONS 58
Appendix D
Phone Interview Template for Baby Sign Group
1. How have things been going (open-ended)?
2. How many times per day would you say you model each sign?
a. < 3 times per day (how often per week)
b. 3 – 5 times per day
c. 6 – 9 times per day
d. 10 times or more per day
3. When do you model each sign?
a. During feeding
b. During play
c. During both feeding and play
d. Other (explain)
4. Has your child made any attempts to communicate with Baby Sign?
a. If yes, continue with questions
b. If no, skip to question 11
5. Which sign/s has your child used?
6. Did they use the sign after it was modeled or spontaneously?
7. Were they using the sign appropriately to the context (i.e. the sign MORE when
asking for more of something)?
8. Was/were the sign/s used with vocalization or without vocalization?
9. Where were you when your child used the sign/s (i.e. at home)?
10. How did you respond to their use of Baby Sign?
11. How have you been feeling about the Baby Sign program?
12. How do you feel about the number of signs you are training with?
a. Too many (explain)
b. Too few (explain)
c. Just right
13. How do you feel about the functionality of the signs (i.e. do they fit with the needs
of your child)?
14. How do you feel about using Baby Sign with your baby?
15. Would you recommend using Baby Sign to other parents (explain)?





























