Embed Size (px)
Citation preview

World Medical & Health Policy www.psocommons.org/wmhp
Vol. 2: Iss. 1, Article 19 (2010)
The Ecology of Health Policymaking and Reform in the United States of
America Sunday E. Ubokudom, PhD, The University of Toledo
Jagdish Khubchandani, MBBS, MPH, The University of Toledo
Abstract
This article demonstrates how constitutional, political, legal, economic, technological, social and cultural, physical, demographic, and global factors affect health policymaking in the United States of America. The ecological factors that influence health policy in the United States are uniquely different from those of other countries. Therefore, even though a number of problems may be common to health systems worldwide, these problems may require different solutions in different countries, or in different sections of the same country. The article concludes that the above ecological factors, individually or collectively, cause U.S. health policies to be inconsistent. For example, policies were adopted in the past to promote the concentrated interests of health providers. Recently, the rise of opposing concentrated interests, a lingering economic recession, a weakened resistance to change, and policy learning from the practices of other industrialized countries and from scholarly publications give us hope that reform, although still difficult to achieve, may finally be in sight.
Keywords: health reform, health policymaking, ecological factors, United States of America
Author Notes: This paper grew out of a speech the lead author was invited to give at a meeting of the Toledo Surgical Society on November 13, 2008. I am thankful to the members of this group, especially Dr. Munier Nazzal, for their invitation. Sincere thanks also go to my wife, Mfon Ubokudom, a nursing provider, for her many useful suggestions. We also thank the journal editors and two anonymous reviewers whose suggestions significantly improved the manuscript. Finally, Linda
- 331 -
© 2010 Policy Studies Organization

Neuhausel deserves commendation for her excellent secretarial support. We are not advocating for the journal, our employer, or for any of the two major political parties in the United States. Rather, our opinions are based on our professional convictions of what we believe are in the best interest of U.S. healthcare consumers. Any errors in the manuscript are solely our own.
Recommended Citation: Ubokudom, Sunday E. and Khubchandani, Jagdish (2010) "The Ecology of Health Policymaking and Reform in the United States of America," World Medical & Health Policy: Vol. 2: Iss. 1, Article 19. DOI: 10.2202/1948-4682.1010 http://www.psocommons.org/wmhp/vol2/iss1/art19
- 332 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

Introduction
Healthcare is a major issue facing policymakers in the United States. Increases in expenditures and in the population of the uninsured and underinsured, declines in employer-sponsored insurance (ESI), avoidable illness and premature deaths, and health disparities based on race, ethnicity, and income have placed healthcare reform on the public and governmental agendas (AMA 2008).
Efforts to enact major reforms of the healthcare system failed numerous times from 1920 to 1994 when President Clinton’s reform plan was defeated. Each time the reform was attempted, the reformers ran into a well-organized opposition that expended immense resources to impede change (Hacker 2009, 4).
Public opinion was very supportive of President Clinton’s September 1993 reform proposal. But after powerful groups began to attack the proposal, public interest and support waned (Weissert and Weissert 2002, 75; Patel and Rushefsky 2006, 392). Consequently, the Congress did not vote on the Clinton plan or on any of the competing proposals that were introduced.
Health reform was one of the major issues of the 2008 presidential election campaign. Senators Barack Obama and John McCain offered different reform proposals. About two months after President Obama took office, a healthcare reform summit was held in the White House. Another debate has begun about the merits of the healthcare system and the need for change (Pauly 2008, 482; Hacker 2009, 4).
The above discussion raises the following questions: Why is the U.S. healthcare system so resistant to change? Given the system’s resiliency and resistance to change, will the Obama initiative succeed or fail like its predecessors? What factors are likely to enhance or impede this new initiative?
Some of the above questions are not new to the public, politicians, and health policy experts. Book chapters and journal articles have been devoted to analyzing the reasons for the failure of the 1993 Clinton plan. In sometimes biased, scattered, and incoherent ways, scholars have discussed a variety of environmental factors that affect U.S. healthcare policymaking and reforms. Consequently, not only are these discussions incomprehensive, but the ideology and political inclinations of the analysts influence the issues they emphasize. As Anderson (2006, 45) observes, political scientists continue to spend most of their time studying the policy effects of political variables, with which they are most comfortable.
- 333 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

On the one hand, conservative thinkers illuminate government or political interference, a defective tort system, and the excesses of the welfare state as the major factors impeding efficient healthcare delivery and reform. Liberal thinkers, by contrast, blame the existing constitutional arrangements, the medical–industrial complex, economic interest groups, the marketing techniques used by private health insurers, and the lack of progressive financing of health benefits as significantly contributing to the problems of the healthcare system (Cutler 2004, 76). These contrasting causal explanations help explain why Morone (2008, 49) writes that health science constantly wrestles with self-interested politics, resulting in robust findings that are only as good as the policy coalition that assembles around them.
Because of the shortcomings of previous research identified above, our paper takes a more balanced approach by analyzing all the ecological factors, market based or politics oriented, that, in our opinion, influence healthcare policymaking in the U.S. The paper is built on the premise that the U.S. health policy environment is uniquely different from those of other industrialized countries. Consequently, even though a number of problems may be common to health systems worldwide, these problems may require different solutions in different countries, or even in different sections of the same country, because of dissimilar social, cultural, and political systems, stages of development, and geography (Payer 1996, 23; Kettl and Fesler 2005, 21; Ubokudom 2008a, 2). Therefore, the key to understanding the problems of the U.S. health system is to study the ecology of the healthcare system. Another unique strength of this investigation is that in addition to social, economic, and political factors, we place equal emphasis on global factors and on the likely beneficiaries of a reformed healthcare system. First, with regard to global influences, previous researchers included discussions of other nations when foreign and defense policies were discussed (Anderson 2006, 39). However, recent events have made globalization an important part of the discussion of American health policy. Second, with regard to those who are likely to benefit from healthcare reform, again, Morone’s (2008, 53) admonition that “the politics of social policy always turns on the mental images we create of the beneficiaries” is very instructive in this respect. Public support for the present reform effort will depend, in part, on how those who are expected to benefit from the reform are perceived. Still on the merits of this study, it is equally important to note that even well-designed programs cannot be left unattended. Rather, they must be adapted to changing environmental conditions. Therefore, whether the current reform effort in the U.S. succeeds or fails, this analysis is expected to
- 334 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

serve as one of the starting points for determining what went right, what went wrong, and what must be avoided or embraced in the future. Further, the study is expected to serve as a guide for researchers doing ecological analysis elsewhere in the world.
Theoretical Framework
Before proceeding, it is necessary to clarify our usage of the word “ecology.” Depending on the context, the words “ecology,” “surroundings,” and “environment” may be used interchangeably. But they are not used interchangeably in this paper. The concepts “environment” and “surroundings” are too inclusive to be of any significant help in this study. Therefore, the paper focuses on a narrower concept, the ecology or that portion of the general environment of the U.S. with which the health system is closely intertwined (Dubnick and Romzek 1991, 93).
Writing in the 1940s, American scholar John Gaus introduced the concept of ecology into the public policy and administration vocabulary (Gaus 1947). According to Gaus,
An ecological approach to public administration builds, then, quite literally from the ground up, from the elements of a place—soils, climate, location, for example—to the people who live there—their numbers and ages and knowledge, and the ways of physical and social technology by which from the place and in relationships with one another, they get their living. It is within this setting that their instruments and practices of public housekeeping should be studied so that they may better understand what they are doing, and appraise reasonably how they are doing it. (p. 1)
Gaus proposed a list of factors that he found useful in explaining “the ebb and flow of the functions of government in the United States.” These included people, place, physical technology, social technology, wishes and ideas, catastrophe, and personality. This theory is relevant for our study of the U.S. health system. In any country, certain external factors determine the characteristics of the health system (Shi and Singh 2008, 9). The ecological factors that we believe influence the health system in the U.S., which are by no means exhaustive, involve constitutional, political, legal,
- 335 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

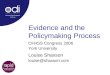
economic, technological, social and cultural, physical, demographic, and global dimensions. Even though we emphasize that the characteristics of the U.S. health system are shaped by the ecological factors identified, the healthcare system also shapes the ecological factors. For example, the $2.24 trillion spent for healthcare in 2007 accounted for 16.2% of the nation’s gross domestic product (GDP) (CMS 2009a), implying that healthcare is one of the important drivers of the American economy. The impacts of the healthcare system on the ecological factors qualify as another subject area for research and analysis. Relationship between Ecological Factors and the U.S. Healthcare System Having identified the nine ecological dimensions of the U.S. healthcare system, next we analyze how these factors help answer the questions we posed in the introductory section of the paper—how do they cause the healthcare system to be resistant to change and how are they likely to enhance or impede reform? We now turn to this task, beginning with the constitutional ecology of the health system. Constitutional Ecology Health policymaking and reform are heavily constrained by the nation’s constitutional ecology, a system of government comprised of three coequal branches sharing power, and by federalism or the division of governmental authority between the national and state governments (Anderson 2006, 35). At the national level, power for making policies is divided between the executive, legislature, and judiciary. But since the judiciary is passive, depending on citizens to bring cases before it, much of the formal policy-making process involves the executive and the legislature. In addition, as shown in Figure 1, both houses of the legislature must agree on a bill before it can be presented to the president for his signature or veto. This Bicameralism checks on the emergence of radical policies, so to speak.
- 336 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

FIGURE 1
Constitutional Ecology of the U.S.
Executive
1 3 4
Judiciary Legislative
House
5
6
Senate
1. Nomination of judges 2. Judicial Review 3. Vetoing Legislation 4. Budget control, veto override, oversight functions, impeachment power,
confirmation of appointments. 5. Impeachment of judges, confirmation of judicial appointments 6. Judicial review
Federalism and Intergovernmental RelationsFederal government ↔ State government ↔ Local government
2
- 337 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

The conflict described above becomes more pronounced when different political parties control the White House and Congress. A president facing at least one house controlled by the opposition party has to use a different strategy from one whose party controls both chambers. A president who faces a Congress led by the opposition party must rely on the veto power and public support. This is because members of the opposition, conscious of the next election, will try to frustrate the president (Weissert and Weissert 2002, 96).
The above discussion does not imply that a president who faces a unified Congress will always be successful in enacting his proposals. The failure of the Clinton healthcare reform proposal in 1994 is very instructive in this regard. At the time, President Clinton faced a unified Congress, but this partisan majority did not guarantee him a policy majority. Therefore, the unified Congress that President Obama now enjoys does not guarantee passage of his health reform proposal. As the rest of the article shows, there are other ecological factors at work. Added to the conflict caused by power sharing between the three branches of government and by divided government is the principle of federalism. Although the national government has elaborate powers, state governments are important policymakers in many areas, including health. Consequently, the national government shares many responsibilities with state governments. For example, the national and state governments cooperate to pay for medical services for poor Americans under the Medicaid program. Whereas, the intent of the framers of the Constitution was to use the principles of the separation of powers to prevent abuse of power, these principles have had other positive and negative consequences. These include decentralization of power; inefficiency in the operation of government; the need for cooperation, deference, bargaining, and compromise among policymakers; turf battles; gridlock; inability to formulate consistent and comprehensive sets of policies; duplications of efforts; blaming others for problems; and the dodging of responsibilities by different levels of government (Anderson 2006, 140; Weissert and Weissert 2002, 86). These conflicts generated by the constitutional ecology are dealt with in the political and legal arenas. Political Ecology The political ecology consists of various stakeholders with different perspectives and interests. It includes, but is not limited to, interest groups,
- 338 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

the electoral cycle or how near to an election a healthcare reform proposal is proposed, political parties, and the governmental-politics model of decision making (Allison 1971, 144). We will briefly examine each of the elements of the political ecology, beginning with interest groups.
Interest Groups
Interest groups are organizations of people with similar policy goals entering the political process to try to achieve those goals. They seek to persuade elected officials that their policy preferences serve the public interest and should be enacted into law. But groups may not always act in the public interest. In several instances, they attempt to veto policy changes, innovations, and reforms (Weissert and Weissert 2002, 119).
The numbers and types of groups involved in healthcare politics are very large (Feldstein 1991, 209). Some of them include the Health Insurance Association of America (HIAA), American Medical Association (AMA), American Healthcare Association (AHCA), American Nurses Association (ANA), American Association of Health Plans (AAHP), and the American Association of Retired Persons (AARP). These groups may lobby members of Congress and the executive branch, or they may engage in grassroots lobbying.
Interest groups also influence policymaking by using their political action committees (PACs) to contribute money to candidates for elections. For example, the Center for Responsive Politics reported in 2009 that during the 2008 election cycle, about 127 health PACs contributed a total of about $49.3 million to federal candidates.
Electoral Cycle
Patronage appointees in government agencies, including those responsible for managing the vast outlays for health services, may be changed after elections, at the discretion of a new administration (Hall 1987, 221; Ubokudom 2008a, 7). In the health arena, these changes may result in the replacement of pro-reform political appointees with those who are anti-reform or indifferent. An example of this occurred in the environmental arena in the early 1980s, when President Reagan selected Anne M. Gorsuch to head the Environmental Protection Agency and James G. Watt as Secretary of Interior. Both appointees were attorneys who had spent years litigating against environmental regulation (Vig 2000, 98).
Apart from the president appointing pro- or anti-reformers, legislative policymaking is also influenced by the quest for reelection.
- 339 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

Therefore, legislative voting behavior takes into account the possible political costs or benefits of such decisions (Arnold 1990). A good example in the health arena that illustrates how the electoral cycle influences legislative decisions is the public’s quest for a patients’ bill of rights in the late 1990s. The public’s discontent with managed care practices during the period led to efforts to enact a patients’ bill of rights to check these questionable practices (Mechanic and Schlesinger 1996, 1693). About one thousand bills were introduced in state legislatures in 1996 to regulate managed care practices (Bodenheimer 1996, 1601). Also, between 1999 and 2000, the House of Representatives and the Senate passed different versions of a patients’ bill of rights and set up a conference committee to reconcile the bills (Ubokudom 2003, 68). A compromise was not reached by the conference committee because legislators were more concerned about exploiting the issue for political advantage in the 2000 election than they were on a compromise (Families USA 2001). Political Parties Political parties are defined as groups of people who seek political power so that their policy preferences may become public policy. Some of their most important functions involve organizing the competition in an election, unifying the electorate, helping to organize the government, translating preferences into policy, and closely monitoring the actions of the party in power (Magleby, O’Brien, Light, Burns, Peltason and Cronin 2006, 162). The two major American political parties differ on the role of government in virtually all policy arenas, including healthcare. Similarly, Americans’ views about the role of government in healthcare are heavily influenced by their ideological orientations and party identification. Republicans are much more likely to share conservative views, to advocate for a limited government, and to oppose more government intervention in healthcare. Democrats, on the other hand, are more likely to share liberal views, to advocate for an activist government, and to support more government intervention in healthcare. Furthermore, Republicans are more likely to hold individuals accountable for their health, while Democrats are more likely to argue for a collective responsibility for health (Brodie and Blendon 2008, 259). The differences in the health policy positions of the Democratic and Republican platforms for the 2008 presidential election were along the lines described above. Briefly, the Democrats advocated a collective responsibility for health between employers, workers, insurers, providers, and government. Republicans, on the other hand, proposed to give control of
- 340 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

the health system to patients and health providers, instead of bureaucrats in government or business, and to generate more market competition (Woolley and Peters 2008). These party platforms identify the two parties’ beliefs about healthcare policy. They are said to be excellent predictors of a party’s actual performance in office (Pomper 1980, 161).
The Government-Politics Model of Decision Making
The government-politics model of decision making views decisions as the product of bargaining among many influential decision makers. The problems of the health system fit this model. Whether it is cost control or universal coverage, the participants include the federal and state governments, employers, insurance companies, managed care plans, and various healthcare providers. The success of any policy proposal is influenced by the actions of the participants, who differ in their ability to shape the outcome (Allison 1971, 6), and by the political feasibility of the solution proposed to solve the problem (Huitt 1970, 400). Incrementalism and consensus building are uniquely suited to this pluralistic environment of the government-politics model of decision making. According to Johnson (1996, 299), the “buck” may not stop anywhere in this model but may keep revolving around the circle of the participants.
Another important dimension of the government-politics model of decision making is the degree of difficulty of the decisions to be reached. The problems afflicting the healthcare system are divergent—problems that have many potential definitions and solutions, most of which are not compatible with one another (Johnson 1996, 296). For example, rising costs in the U.S. may be blamed on consumers, providers, equipment manufacturers, government regulations, malpractice lawsuits, insurers, etc. Just as the problem may be defined in different ways, different solutions may also be proffered to solve it. The proposed solutions, as well as the problem definition itself, do not meet with everyone’s approval. Therefore, there is need for consensus building, compromises, consideration of citizens’ opinions, and considerations of the costs of implementing the solutions agreed upon. This scenario complicates policymaking and may even result in inaction.
Legal Ecology
Statutory laws, legislative and administrative rules and regulations relating to healthcare, are intended to subordinate the healthcare system to the rule of
- 341 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

law. Even though the legislative and executive branches of government have primary responsibility for making policy, the judiciary also plays an important role for several reasons. First, the legislative and executive branches delegate to the courts the power to determine health providers’ liability for medical negligence (Rosenblatt 2008, 128). In particular, courts determine the substantive and procedural rules to be followed in the course of deciding individual cases of fraud, negligence, and malpractice. Second, because legislative and administrative rules and regulations are often unclear or ambiguous, courts must determine the constitutionality and meaning of the regulations. In other words, courts and the relevant administrative agencies implement health laws and regulations. Third, although the U.S. Constitution makes no specific mention of healthcare, the provisions protecting citizens from malicious, arbitrary, or capricious deprivation of life, liberty, or property, and guarantees of equal protection of the laws, have been used by courts to rule on issues such as access to contraceptives, abortion rights, and the right to die (Rosenblatt 2008, 128). Another area of healthcare that is affected by public laws is health insurance. Insurance is regulated by the states. In some cases, state laws may impose premium taxes on insurance plans and health providers in order to generate money to reimburse providers for uncompensated care (disproportionate share payments); state insurance laws may also impose certain mandatory benefits and other consumer protection requirements. Whereas the primary purpose of the federal Employee Retirement Income Security Act (ERISA) of 1974 was to guarantee the security of workers’ retirement pension benefits, it also exempts self-insured employers from paying premium taxes, and to avoid other types of state insurance regulations, such as financial reserves and consumer protection requirements. This federal law essentially undercuts states’ authority for health insurance regulation (Shi and Singh 2008, 203). Economic Ecology The economic ecology deals with concerns about the types of health services to produce, where they should be produced, production costs, and who should benefit from the produced services. In the health policy arena, current and anticipated economic conditions influence the financing for services. Financing, in turn, influences the demand for services. Increased demand
- 342 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

results in greater utilization of services, given adequate supply (Shi and Singh 2008, 199).
As was discussed earlier, healthcare financing influences production levels. Innovations and new services proliferate when there is adequate reimbursement for them. Therefore, financing gives rise to new technologies and services. These services are likely to be used extensively when there is reimbursement for them.
Financing for health services also influences both the supply and the distribution of health professionals. Greater reimbursement for specialty care has been implicated for the increase in specialists and the decrease in the numbers of generalists. Explicit government policies designed to influence physician supply and distribution, such as the resource-based relative value scales (RBRVS) used by Medicare to pay physicians, are designed to cut payments for specialty care and to attract younger physicians into general practice.
In addition to current and anticipated economic conditions, the level of economic development influences government expenditures. The level of economic development affects both the capacity of a society to support the public sector and the level of demand for services. Higher levels of economic development increase government’s ability to generate needed revenues, provided that taxpayers are willing to shoulder the burden.
When taxpayers are reluctant to pay additional levies, government may be forced to cut programs. Concerns about rising expenditures led to efforts to contract the healthcare system beginning around 1970 and continuing till today. Some of the efforts to cut costs, which have been widely documented, include President Nixon’s 1971 Economic Stabilization Program (ESP); the establishment of Professional Standards Review Organizations (PSROs); the Health Maintenance Organization (HMO) Act of 1973; the Health Planning and Resources Development Act of 1974, which required certificates-of-need (CON) for health facilities wanting to expand; the institution of a prospective payment system for Medicare based on diagnosis-related groups (DRGs) in 1984; and the utilization of novice delivery and reimbursement regimes, such as contracts, managed care, and capitation (Davis et al. 1989; Ubokudom 2003, 64).
Technological Ecology
We define medical technology broadly to include drugs, devices, sophisticated machines and ultramodern facilities, computer-supported information systems, and medical and surgical procedures used in medical
- 343 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

care, as well as organizational and supportive systems within which such care is provided (Riley and Brehm 1989, 21). This technology involves the standardized physical and social means used to treat patients. Physical technologies include those standardized inanimate tools that are relied upon to provide medical care. Some examples include magnetic resonance imaging facilities and devices, computer axial tomography scanners, computerized electro-cardiograph machines, renal dialysis machines, etc. These technologies tend to change rapidly and to create high expectations from both consumers and providers. Social technologies are those standardized social means and methods used to solve certain problems (Dubnick and Romzek 1991, 127). Compared to physical technologies, social technologies are not inanimate objects, but standardized human behavior patterns. They are less standardized than physical technologies. Social technologies can be classified into two types: traditional and designed. Some examples of traditional social technologies include families, schools, and churches. These institutions provide social support, informal care, companionship, and economic security. An example in the health arena is the fact that most long-term care services in the U.S. are provided by family members of elderly or disabled persons (Wiener et al. 1994, 5). Nurses also provide primary care services in schools. Industrialization and other changes in society have made people less reliant on traditional social technologies to carry out basic economic, political, and social functions. To make up for the loss, designed social technologies have been invented to accomplish these tasks. Some examples of health-related designed social technologies include managed care corporations, health interest groups, nursing homes, hospitals, counseling centers, etc. These designed social technologies are important and unavoidable parts of the health system. Physical and social technologies have had profound effects on both the health of the people and the healthcare system. For example, whereas advances in chemistry have allowed us to grow and store more food through the use of fertilizers, pesticides, and additives, some of these devices can have adverse effects on people’s health. Similarly, whereas advances in telecommunications, electrical and mechanical engineering, and physics have led to the development of telemedicine, radiology, cardiology, and magnetic resonance imaging, some of the undesirable side effects of these devices include increased costs, depersonalization of care, ethical dilemmas, such as unnecessarily prolonging or shortening life, and the generation of radioactive byproducts that are difficult to dispose of.
- 344 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

Physical and social technologies have also had significant effects on the healthcare system itself. Specifically, the technologies have driven the scope and content of medical training and the practice of medicine, governed the organization and financing of medical services, influenced the status accorded to different medical workers, and raised consumer expectations about the types of treatment and outcomes that are possible (Shi and Singh 2008, 177; Patel and Rushefsky 2006, 318). When these expectations are not met, frustration sets in and lawsuits are filed.
Social and Cultural Ecology
Virtually all health policy matters are influenced by the nation’s culture and numerous subcultures. Culture refers to the shared views that people have formed about how their world works and about the methods for problem solving that will be effective in that world (Schein 1985, 5). Added to this world view are the people’s values, which reflect what they think are the appropriate and desirable roles for government to perform. These values can be divided into social and political dimensions.
Social values determine whether Americans prefer immediate or deferred gratification of individual needs or desires; whether there should be favoritism in the application of rules; whether the society has an individual or a collective interest orientation; and whether people are evaluated based on their personal achievements or on other factors over which they have little or no control, such as wealth, family ties, race, or gender (Dubnick and Romzek 1991, 141).
The American political culture rests on democratic values. These include liberty, equality of opportunity, individualism, democracy, justice, the rule of law, patriotism, optimism, and idealism. These widely shared democratic values overlap and sometimes conflict (Magleby et al. 2006, 82).
The above political values, or at least some of them, make up what is called the American dream—the notion that the U.S. is a land of opportunity and that individual initiative and hard work can lead to economic success. These values account for why the people value capitalism, market justice, economic incentives, and a limited government role in the economy (Magleby et al. 2006, 87).
The U.S. healthcare system is deeply rooted in the beliefs and values held by the people (Payer 1996, 16). Some aspects of the health system that are the result of the nation’s value system include more private influence and less government funding and involvement in the system; the lack of a central agency to administer the numerous health insurance programs in the country;
- 345 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

the diffusion of responsibility among numerous levels of government; the lack of comprehensive and universal coverage for all citizens; minimal cross-subsidization of the uninsured or underinsured; the denunciation of national health insurance as a form of socialism; and the belief that healthcare is a private good, as opposed to a public good. Furthermore, Americans’ beliefs and values influence the training and general orientation of health providers, the organization of medical practice, the association of high technology with high-quality care, and the recognition of physicians as private entrepreneurs who should practice medicine as they were trained. These values also influence the way Americans conduct themselves within the political system, the standards they use to evaluate government activities, and how they feel about government and politics. Perhaps, this explains why the people are generally agreeable that the health system should be reformed, but are less supportive of government-led reform efforts. Physical Ecology Some of the factors we count as being part of the physical ecology of health policymaking include air pollution, food and water contaminants, radioactive substances, illicit drugs, disease vectors, safety hazards, habitat alterations and outbreaks of communicable diseases (Shi and Singh 2008, 51). The relationship between physical ecology and health is well documented. Medical care or those practices that are used for the care and rehabilitation of the sick (hospitals, nursing homes, prescription drugs, etc.) make only modest contributions to the health status of the population. On the contrary, the health status of the population is largely determined by a different set of factors that involve important physical and economic dimensions. These factors are preventive medicine, environmental control, behavior modification, and the totality of environmental, social, and cultural interactions experienced by a population (Winkelstein 1993, 2504; Wilkinson 1997, 1504). As was noted previously, of the $2.24 trillion spent for healthcare in 2007, only $64.1 billion, or about 2.9% of the total expenditures was accounted for by those factors identified above as having the most effect on population health (CMS 2009a, b). This finding is confirmation of the continued dominance of the medical model that has governed the healthcare system since its inception. Health policymaking and resource allocation continue to focus on clinical diagnosis and interventions to treat disease or symptoms of disease, to the neglect of physical ecological factors.
- 346 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

In addition to the effects of physical factors on population health, spatial factors or the locations of health facilities and personnel are important considerations. For example, physicians themselves decide where they will practice, without necessarily considering the needs of the population (Long 1994, 31). Similarly, hospitals’ locations and operations are influenced by financial considerations, without regard to duplications or shortages of services and technology (Shi and Singh 2008, 61). These conditions result in the maldistribution of healthcare providers and facilities. Physicians in the U.S. are more likely to locate in metropolitan and suburban areas than in rural and inner city areas. Also, publicly run health institutions are generally located in large inner cities and certain rural areas. These conditions create vast amounts of provider shortage localities. The publicly operated facilities that are located in inner city and rural areas tend to treat a disproportionate population of the uninsured, thereby causing them serious financial hardships (Ubokudom 1998, 68).
The environment or physical ecology is also known to significantly influence developmental health. Research by Wynder and Orlandi (1984) and by Shellenbarger (1997, B1) shows that children who are isolated and do not associate much with their peers tend to be overrepresented among delinquents and adults with mental health issues.
Demographic Ecology
Demographic ecology refers to population characteristics; the age distribution of the people; literacy rates; health needs; social morbidity, such as acquired immune deficiency syndrome (AIDS), drugs, homicides, and injuries; and the perceptions, attitudes, and values the people bring to the healthcare system as consumers.
The population of the United States was about 302 million in 2007. Per capita expenditure for the year was $7,421, an increase of 5.1% from 2006. The number of people covered by private health insurance (202 million) in 2007 was not statistically different from 2006, while the number of people covered by government health insurance increased slightly from 80.3 million in 2006 to 83 million in 2007 (CMS 2009a, U.S. Census Bureau 2007b).
In 2007, 37.3 million people were in poverty, up from 36.5 million in 2006. The poverty rates in 2007 were statistically unchanged from 2006 for non-Hispanic whites (8.2%), blacks (24.5%), and Asians (10.2%); it increased slightly (about 1%) for Hispanics between 2006 and 2007.
- 347 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

The poverty rate and the number in poverty increased for children less than 18 years of age in 2007. In both 2006 and 2007, the poverty rate for children was higher than the rates for people 18–64 years old and those 65 years and older. In 2007 alone, children under 18 years old represented 35.7% of the people in poverty and 24.8% of the total U.S. population. Even though the poverty rate and the number in poverty increased for children in 2007, the percentage and number of children under 18 years old without health insurance were lower that year than in 2006 (U.S. Census Bureau 2007b), most likely due to efforts by Medicaid and the State Children’s Health Insurance Program (SCHIP) to expand coverage for poor children. Even then, children in poverty were more likely to be uninsured than all children. As has been the case since 2000, most Americans were covered by employer-sponsored insurance (ESI) plans in 2007. At its peak in 2000, ESI covered about 67% of the non-elderly population (Blumenthal 2006, 83). By 2004, only about 61% of the non-elderly Americans under 65 years old were covered by ESI (Clemans-Cope and Garrett 2006, 6). Continuing the downward trend, only about 59.3% of the non-elderly Americans were covered by ESI for some or all of 2007 (U.S. Census Bureau 2007b), a decline of about 7.7% since 2000. This is a strong indication of the weakening of the long-standing association between work and health insurance (Ubokudom 2008b, 19; Blumenthal 2006, 84). The current economic recession is expected to lead to more steep declines in ESI for the foreseeable future. In 2004, the year that complete information is available, life expectancy at birth in the United States was 77.8 years (75.2 years for males and 80.4 years for females) (Arias 2007, 4). The white–black difference in life expectancy narrowed from 14.6 years in 1900 to 5.7 years in 1982, but increased to 7.0 years in 1994. The increase in the gap from 1983 to 1993 was said to be due to increases in mortality among the black male population resulting from HIV infection and homicide (Anderson 1999; Kochanek et al. 1994). However, homicides and HIV disease dropped from among the top five causes of death among the black population during the 1990s to sixth and ninth, respectively, in 2004. Unfortunately, as deaths due to HIV disease decline among blacks, diabetes has become one of the top five causes of death for them. In 2004, differences in the 10 leading causes of death in the United States were evident by age, gender, race, and Hispanic origin. Health disparities based on race, ethnicity, income, and gender continue to converge in some instances, and to fluctuate in other instances. For example, whereas the proportions of deaths due to cancer and kidney disease were identical for
- 348 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

both men and women in 2004, the relative burden of mortality from unintentional injuries was higher for men than women. Similarly, the burden of mortality from diabetes, relative to other causes, has typically been higher for women than men (Heron 2007, 8).
The last demographic factor that we want to examine is the age distribution of the population. This is important because we expect healthcare needs to differ based on people’s ages. In 2007, about 172 million people were between 0 and 41 years of age, 85 million were between 42 and 62 years old, and about 45 million were more than 62 years old (Schill 2008). Federal health officials report that persons reaching age 65 have an average life expectancy of an additional 19.0 years (DHHS 2008). Consequently, the 85 years of age and above population is projected to increase from 4.2 million in 2000 to 5.7 million in 2010, and then to 6.6 million in 2020. The percentage of the elderly living in nursing homes or institutional settings increases dramatically with age, ranging from about 1.3% for persons 65–74 years to 4.1% for persons 75–84 years and 15.1% for persons 85 years of age and older. These data are indicative of a pressing need for long-term care services for the elderly in the near future.
Global Influences
The global ecology includes the effects of migration and population mobility, trade and travel, terrorism, and the emerging and reemerging infectious disease paradigms. These factors present new challenges for healthcare delivery and policymaking throughout the world.
Globalization refers to various forms of cross-country economic activities. The process is driven by the current global exchange of culture and information, the growth of migration and population mobility, international trade, outsourcing of the manufacturing business from the developed countries to the developing countries where labor costs are lower, and the increased interdependence of the world’s economic systems These changes now shape global health, and raise an awareness that changes in the ecology of human living, in relation to both the natural and social environments, account for much of the ebb and flow of diseases over time (McMichael and Beaglehole 2000, 495).
The principal agents of a globalized market-based economic system are international agencies such as the World Bank, the International Monetary Fund (IMF), and the World Trade Organization (WTO). The policies they promote have resulted in reduced expenditures for social programs, especially in developing economies. These policies have impaired
- 349 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

population health, and slowed the advances in literacy for women, fertility reduction, and improved reproductive health in the developing countries (Kinnon 1998, 397; Gray 1998; Watts 1997). Globalization is also blamed for increased smoking and tobacco-attributable mortality in the developing countries (Murray and Lopez 1997, 1498). Also noteworthy is the escalation in the sale of weapons, much of it facilitated by western governments. The wars that have raged on and off in sub-Saharan Africa, Latin America, and Asia are tragic examples of the ill effects of aggressive weapon sales to these places (McMichael and Beaglehole 2000, 497). Although the adverse consequences of globalization tend to affect developing countries more than the U.S., there are significant adverse consequences of globalization for the United States as well. Some of these include the perpetuation and exacerbation of the gap between the rich and the poor, job insecurity and reduced wages, the collapse of large manufacturing businesses, increased availability and demand for illicit drugs, and the emergence of new infectious diseases that spread more easily because of increased migration and population mobility.
The sudden appearance of the previously unknown acquired immune deficiency syndrome (AIDS) in the U.S. in the early 1980s challenged the widely held belief that infectious diseases were under control. Since then, new diseases and ailments have surfaced, such as the hantavirus, believed to have originated in Korea; encephalitis cases in New York and California in 2002; the spread of Severe Acute Respiratory Syndrome (SARS) from China in 2003; the polio virus that originated in India in 2005; and the 2009 outbreak of the deadly H1N1—swine flu—influenza believed to have originated in Mexico (CDC 2009; Shi and Singh 2008, 578). The terrorist attacks in the United States on September 11, 2001, elevated public health to an important national instrument for anticipating and dealing with terrorism. The 2001 experience has led to the development of large-scale plans to deal with the threat of bioterrorism. Consequently, expenditures for government public health activities, while still low relative to expenditures for medical care, rose from $47 billion in 2001 to $64.1 billion in 2007, an increase of 36.4% from 2001 (CMS 2009a). The global influences on health are introducing health issues into the U.S. foreign policy discussions (MacPherson et al. 2007, 200). Other aspects of the U.S. health system that are affected by the global ecology are medical technology and healthcare professionals and consumers. Because the United States is widely believed to be the world leader in the development and utilization of high-technology procedures, foreign dignitaries come here for specialty care. Also, nurses and foreign
- 350 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

medical graduates (FMGs) move to the United States to acquire licenses to practice in the country. This so-called brain drain leads to shortages of medical practitioners in the developing countries, and alleviates some of the shortages in the understaffed areas of the U.S.
Telemedicine allows physicians in the U.S. to transmit radiological images to other countries where they are interpreted at lower costs. On the other hand, U.S. consulting pathologists and radiologists are able to provide their services to other parts of the world. Furthermore, medical equipment and supplies that are discarded here a few years after deployment are shipped to the developing and less technology-intensive developed countries at low costs. The high costs paid by U.S. consumers are used to subsidize the low costs paid by the developing countries.
We have just finished a detailed excursion into the ecology of health policymaking in the U.S. This exercise was intended to allow us identify some of the constraints and opportunities for health reform presented by the ecological factors. Therefore, this final section of the paper will discuss the opportunities and constraints, and the policy implications or types of reform proposals that are likely to be embraced in this environment. First, we identify the constraints posed by the ecological factors.
Constraints Posed by the Ecological Factors
The constitutional and political ecological factors discussed earlier cause healthcare policymaking to be in a constant state of fluidity, resulting in inconsistencies and conflicting programs and values. As was stated earlier, power is decentralized among the different branches of government and among individual policymakers. A person who is not very familiar with the U.S. system of government may conclude that there are 536 policy-making agendas competing with each other (one agenda for each of the 435 members of the House of Representatives, 100 Senators, and the president). This assertion is wrong when one considers the various interest groups and other influences on the healthcare system. The challenge is how to aggregate all these different, and sometimes conflicting, values. The failures of previous reform efforts point to the fact that value aggregation is no easy task.
The extensive reliance on ESI is another constraint on health policymaking and reform. At the outset, the nation delegated the provision of health insurance for its citizens to private companies. Therefore, between 1940 and 1950, the number of people with private health insurance increased from 20.6 million to 142.3 million (Thomasson 2002, 233). By 2004, the
- 351 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

number of non-elderly Americans with ESI was more than 159 million (Blumenthal 2006, 82). Even though ESI has been on the decline, the continued reliance and investments in ESI seriously limit consideration of alternative financing mechanisms, a phenomenon economists call “sunk costs” (Anderson 2006, 124). This is probably why the reform proposal currently under consideration “builds on the current system in which employers, government, and individuals share responsibility for health insurance” (Alonso-Zaldivar and Werner 2009). For the most part, healthcare reform involves concentrating the costs of the reforms on a few groups, while spreading the benefits in minute quantities to the general population. Under this scenario, those who are expected to bear the costs of the reforms have more incentive to organize to oppose the reform than the masses that would reap the benefits (Weissert and Weissert 2002, 252; Ubokudom 2003, 70). This explains why insurers, hospitals, and employers oppose a provision of the new proposal, which calls for a government-sponsored insurance plan to compete with private companies (Alonso-Zaldivar and Werner 2009). Meanwhile, the masses do not seem to be paying attention to the debate. Another important constraint that cannot be ignored at this time of high unemployment and budget deficits is cost inflation. The Kaiser Family Foundation’s annual survey of employer benefit plans for 2008 shows that healthcare spending continues to rise at a rate that affects business operations and family expenses. In 2008, the average annual combined employer and employee premiums for ESI were $4,704 for single coverage and $12,680 for family coverage, up about 5% from 2007. In addition to premium contributions, most covered workers face a general annual deductible, physician office visit copayments, and a portion of the cost of prescription drugs. Among employers that offer health insurance benefits, large numbers anticipate future increases in worker premium contributions and co-payments (Claxton et al. 2008). It follows, then, that healthcare cost increases are continuing at a time of declining employment. Declining employment and loss of ESI increase citizens’ demands for government assistance. Similarly, the more the number of unemployed citizens, the less revenues available for government to deal with the increased demand for public assistance. This limits government’s ability to provide health insurance for both the chronically and recently uninsured. Paradoxically, declines in employment and insurance can provide government with the cover necessary to advocate universal coverage. For a long time, the popular belief had been that the aging of the American population would drive up both the demand and spending for
- 352 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

healthcare. This line of thinking ignored the supply side of the healthcare equation. Research shows consistently that when supply-side variables are controlled for, the aging of the population, by itself, tends to be only a minor determinant of the annual growth in aggregate healthcare use and spending. This is so because the rise in the age 65 and older population group is gradual (Reinhardt 2003, 27).
Even though recent studies have debunked the myth that the aging of the population is a major driver of the annual growth in the demand and spending for healthcare, the aging of the population still constrains health policymaking and reform. This is so because the current fertility rate is significantly below the “replacement rate” needed to maintain the present or desired age-dependency ratio (Graig 1999, 180; Reinhardt 2003, 27). For example, in their 2009 report, the Trustees of the Hospital Insurance and Supplementary Medical Insurance Trust Funds predicted that in the future, Medicare trust fund income is expected to increase less rapidly than expenditures. This is because with past declines in birth rates, continuing improvements in life expectancy, and prevailing rates of disability incidence, the number of workers is expected to grow more slowly while the number of beneficiaries is expected to increase much more rapidly (CMS 2009b).
The last constraint to policymaking and reform is the existing, although narrowing, health disparities based on race, ethnicity, and income. Although the race-based gap in health status is narrowing, millions of Americans, many of them racial and ethnic minorities, lack access to healthcare. Since other factors, in addition to healthcare, affect the health status of the population, any effort to reduce health disparities must be comprehensive to be effective. Policies must address the disproportionately low level of access to healthcare for minorities, the relatively low levels of healthcare quality for minority groups, and the adverse social and economic conditions faced by minorities in their communities (Lavizzo-Mourey et al. 2005, 313). This will be no easy task, especially since minorities usually have the least amount of resources, political and economic.
The discussion of the constraints facing the health system does not imply that all hope for reform is gone. On the contrary, the ecology also presents some real opportunities that, although fewer than the constraints, can be harnessed to achieve desired reforms. These opportunities are examined below.
- 353 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

Opportunities Presented by the Ecological Factors From the beginning of the U.S. healthcare system till about 1980, health policy costs or the economic interests of consumers were diffused, whereas the economic interests of health providers were concentrated. Consequently, there was a strong incentive for providers to organize and lobby for beneficial legislation because the payoffs they expected to receive were large and attractive (Feldstein 1991, 209). The fee-for-service reimbursement method, states’ restrictions on prepaid group practice, appropriations for health professional educational institutions, etc., were enacted based on the economic interests of providers, who had a concentrated interest in their outcomes. Since the 1980s, much of the diminished political power and economic benefits enjoyed by the medical profession are the result of the rise of opposing concentrated interests—costs for payers have increased to the point where they become concentrated (Feldstein 1997, 220). These cost increases, continuing during a deep economic recession, have made healthcare one of the leading issues among the public. At the moment, public support for reform appears to be high. However, there are significant differences about the specific forms of reform the public will support. Increased public and labor support for reform, a less vigorous business and provider resistance to reform, policy learning from the practices of other industrialized countries, and policy learning from the publications of health policy scholars in the U.S. and around the world give us hope that the coalition needed to push for universal coverage and cost containment can be built in the Congress and among the general population this time around. With regard to how the United States can learn from other industrialized countries, Theodore R. Marmor and Morris Barer (1997, 315) write that the rest of the developed world figured out some time ago that providing universal coverage did not have to mean uncontrolled costs and that controlling costs did not have to mean foregoing universal coverage. Some of the countries that have learned this lesson include England, Australia, Germany, The Netherlands, Canada, and Japan. Although the systems in these countries are not devoid of quality or cost problems, they have been able to provide at least basic coverage to all their citizens at a fraction of the costs incurred by the United States. Moreover, some of their health statistics are comparable to, or in some instances better than, those of the United States (Graig 1999, 176). From within the U.S., the Institute of Medicine (IOM) reported in 2002 that about 18,314 Americans die annually due to uninsurance. That
- 354 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

death toll is expected to increase as the uninsurance rate increases during these hard economic times. These alarming statistics, if well communicated to the population, may be the impetus for public support of heath care reform.
But, let there be no mistake. Success in building the coalition needed to push for universal coverage and cost containment also depends on the ability of the president to use his popularity and speaking ability to convince Americans that the majority of them—the middle class, men and women, the young and the elderly, small and large businesses, the insured and uninsured or underinsured, conservatives and liberals alike—would benefit from a reformed healthcare system.
Poor health does not discriminate along party lines, gender, age, social status, race, etc. Health is not a negotiable commodity—one either has or does not have it. All Americans, regardless of political beliefs, would like to be healthy, not unhealthy. The existing system is not conducive to prevention and better longevity despite high expenditures. Some of the ways to remedy the current situation are to get rid of all the financial and legal intermediaries that stand between patients and their healthcare providers, strengthen the fiduciary responsibilities of healthcare providers, including the curtailment of defensive medicine, control costs, and pay better attention to educating the public about making healthy choices. The Administration must not only educate the public on the above issues, it must also quickly and vigorously dispel any misinformation or half-truths by those who are willing to go to any length to preserve the status quo.
The above point reminds us of a debate Professor Morone (2008, 49) tells us he had in 1994 with a politician who opposed the Clinton reform plan. Briefly, the politician’s claim that the proposed reform plan required “deserving” citizens “to go into the same health alliances as the crackheads in the city of Chicago” effectively ended the positive reception the professor had received to that point. The rumors spread in the summer of 2009 that the Obama Administration planned to insure illegal immigrants and to set up “death panels” to kill seniors as a way of cutting costs are indications that antireformers will go to any length to block change. The Administration must anticipate these rumors and misinformation and must not allow antireformers to put it on the defensive. The plan that is presented to the American people must be simple enough for the average citizen to understand, and must follow the neoconservative approach (Battistella and Ostrick 1997, 75). It must seek balance and moderation between equity and efficiency, and must be able to adapt to changing local and global circumstances.
- 355 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

Conclusion
The purpose of this paper was to examine the ecological factors that make the U.S. health system resistant to change, and to explore the prospects of passage of the reform agenda pursued by the Obama Administration. We identified and analyzed nine ecological factors that influence health policymaking in the U.S. These ecological factors, individually and collectively, cause the U.S. healthcare policymaking to be inconsistent. In the past, health policies and programs were enacted to support the concentrated interests of providers. Recently, however, the rise of opposing concentrated interests on the demand side of the healthcare equation, an economic recession that is described as the worst since the Great Depression, a weakened business and provider resistance to reform, and policy learning from the practices of other industrialized countries and from the publications of health policy scholars in the U.S. and around the world give us hope that health reform may soon become a reality. However, given previous experience, the constraints that reformers face are still very serious. A neoconservative reform proposal that builds on existing structures stands a better chance of being adopted than a proposal that involves sweeping changes to the existing system.
References
Allison, G.T. 1971. Essence of Decision: Explaining the Cuban Missile Crisis. Boston, MA: Little, Brown and Company.
Alonso-Zaldivar, R., E. Werner. 2009. “Proposal Would Require All to Have Health Coverage.” http://news.yahoo.com/s/ap/20090514/ap_on_go_co/us_health_overhaul/(May 14, 2009)
American Medical Association [AMA]. 2008. “Overview of the AMA Reform Proposal.” Retrieved April 4, 2009 from http://www.voiceforthefuture.org/amaproposal.html.
Anderson, J.E. 2006. Public Policymaking, 6th ed. Boston, MA: Houghton Mifflin.
Anderson, R.N. 1999. “Some Trends and Comparisons of United States Life Table Data: 1900–1991.” U.S. Decennial Life Tables for 1989-91, 1(3): Hyattsville, MD: National Center for Health Statistics.
Arias, E. 2007. “United States Life Tables, 2004.” National Vital Statistics Reports, 56(9): Hyattsville, MD: National Center for Health Statistics.
- 356 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

Arnold, R.D. 1990. The Logic of Congressional Action. New Haven, CT: Yale University Press.
Battistella, R.M., J. B. Ostrick. 1997. “The Political Economy of Health Services: A Review and Assessment of Major Ideological Influences and the Impact of New Economic Realities.” In Health Politics and Policy, 3rd ed., eds. T.J. Litman and L.S. Robins. Albany, NY: Delmar, 75-108.
Blumenthal, D. 2006. “Employer-Sponsored Health Insurance in the United States – Origins and Implications.” The New England Journal of Medicine 355(1): 82-88.
Bodenheimer, T.S. 1996. “The HMO Backlash – Righteous or Reactionary?” The New England Journal of Medicine 335 (21): 1601-1604.
Brodie, M., R. J. Blendon. 2008. “Public Opinion and Health Policy.” In Health Politics and Policy, 4th ed., eds. J.A. Morone, T.J. Litman and L.S. Robins. Clifton Park, NY: Delmar, 249-270.
Center for Responsive Politics. 2009. “Health PACS Contribution to Federal Candidates, 2008 Election Cycle.” Retrieved June 9, 2009 from http://www.opensecrets.org/pacs/sector.php?cycle=2008&txt=HO1.
Claxton, G., B. DiJulio, B. Finder, M. Jarlenski. 2008. “Employer Health Benefits: 2008 Annual Survey.” Menlo Park, CA, and Chicago, IL: The Kaiser Family Foundation and Health Research & Educational Trust.
Clemans-Cope, L., B. Garrett. 2006. “Changes in Employee-Sponsored Health Insurance Sponsorship, Eligibility and Participation: 2001 to 2005.” Washington, DC: The Kaiser Commission on Medicaid and the Uninsured.
Cutler, D.M. 2004. Your Money or Your Life: Strong Medicine for America’s Healthcare System. NY: Oxford University Press.
Davis, K., G. F. Anderson, D. Rowland, E. Steinberg. 1989. Health Care Cost Containment. Baltimore, MD: Johns Hopkins.
Dubnick, M.J., and B.S. Romzek. 1991. American Public Administration: Politics and the Management of Expectations. NY: Macmillan.
Families USA. 2001. “Whither the Patient’s Bill of Rights?” Retrieved March 15, 2001 from http://www.familiesusa.org/asap/up720pbr.htr.
Feldstein, P.J. 1991. “Health Associations and the Legislative Process.” In Health Politics and Policy, 2nd ed., eds. T.J. Litman and L. S. Robins. Albany, NY: Delmar, 209-225.
Feldstein, P.J. 1997. “The Demand for Legislation and National Health Care Reform.” In Health Politics and Policy, 3rd ed., eds. T.J. Litman and L.S. Robins. Albany, NY: Delmar, 220-230.
Gaus, J. 1947. Reflections on Public Administration. University, AL: University of Alabama Press.
- 357 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

Graig, L.A. 1999. Health of Nations: An International Perspective on U.S. Health Care Reform, 3rd ed. Washington, DC: CQ Press.
Gray, J. 1998. False Dawn: The Delusions of Global Capitalism. London: Granta.
Hacker, J.S. 2009. “Yes We Can? The New Push for American Health Security.” Politics and Society 37 (1): 3-32.
Hall, R.H. 1987. Organizations: Structures, Processes & Outcomes. Englewood Cliffs, NJ: Prentice Hall.
Heron, M.P. 2007. “Deaths: Leading Causes for 2004.” National Vital Statistics Reports, 56(5). Hyattsville, MD: National Center for Health Statistics.
Huitt, R. 1970. “Political Feasibility.” in Policy Analysis in Political Science, ed. I. Sharkansky. Chicago, IL: Markham, 399-412.
Institute of Medicine. 2002. “Care Without Coverage: Too Little, Too Late.” Washington, DC: National Academy Press.
Johnson, W.C. 1996. Public Administration: Policy, Politics, and Practice, 2nd ed. Boston, MA: McGraw Hill.
Kettl, D.F. and J.W. Fesler. 2005. The Politics of the Administrative Process, 3rd ed. Washington, DC: CQ Press.
Kinnon, C.M. 1998. “World Trade: Bringing Health into the Picture.” World Health Forum 19: 397-406.
Kochanek, K.D., J.D. Maurer, and H.M. Rosenberg. 1994. “Causes of Death Contributing to Changes in Life Expectancy: United States, 1984-89.” Vital Health Statistics 20(23): 1-35.
Lavizzo-Mourey, R., W.C. Richardson, R.K. Ross, and J.W. Rowe. 2005. “Foreword: A Tale of Two Cities.” Health Affairs 24(2): 313-315.
Long, M.J. 1994. The Medical Care System: A Conceptual Model. Ann Arbor, MI: Health Administration Press.
MacPherson, D.W., B.D. Gushulak, and L. Macdonald. 2007. “Health and Foreign Policy: Influences of Migration and Population Mobility.” Bulletin of the World Health Organization 85(3): 200-206.
Magleby, D.B., D.M. O’Brien, P.C. Light, J.M. Burns, J.W. Peltason, and T.E. Cronin. 2006. Government By The People: National Version, 21st ed. Upper Saddle River, NJ: Pearson/Prentice Hall.
McMichael, A.J., and R. Beaglehole. 2000. “The Changing Global Context of Public Health.” The Lancet 356: 495-499.
Marmor, T.R., and M.L. Barer. 1997. “The Politics of Universal Health Insurance: Lessons For and From the 1990s.” In Health Politics and Policy, 3rd ed., eds. T.J. Litman and L.S. Robins. Albany, NY: Delmar, 306-322.
- 358 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

Mechanic, D., and M. Schlesinger. 1996. “The Impact of Managed Care on Patient’s Trust in Medical Care and Their Physicians.” JAMA 275 (21): 1693-1697.
Morone, J.A. 2008. “Morals and Health Policy.” In Health Politics and Policy, 4th ed., eds. J.A. Morone, T.J. Litman and L.S. Robins. Clifton Park, NY: Delmar, 49-60.
Murray, C.J.L., and A.D. Lopez. 1997. “Alternative Projections of Mortality and Disability by Cause 1990-2020: Global Burden of Disease Study.” The Lancet 349: 1498-1504.
Patel, K., and M. Rushefsky. 2006. Health Care Politics and Policy in America, 3rd ed. Armonk, NY: Sharpe.
Pauly, M.V. September 16, 2008. “Blending Better Ingredients for Health Reform.” Health Affairs – Web Exclusive: do1:10.1377/hlthaff.27.6.w482
Payer, L. 1996. Medicine & Culture. NY: Henry Holt and Co. Pomper, G.M. 1980. Elections in America. NY: Longman Reinhardt, U.E. 2003. “Does the Aging of the Population Really Drive the
Demand for Health Care?” Health Affairs 22(6): 27-39. Riley, J.G., and H.P. Brehm. 1989. “Technological Innovations and Their
Impact on Care Delivery.” In Health Care, Technology, and the Competitive Environment, eds. H.P. Brehm and R.M. Mullner. NY: Praeger, 21-39.
Rosenblatt, R.E. 2008. “The Courts.” In Health Politics and Policy, 4th ed., eds. J.A. Morone, T.J. Litman and L.S. Robins. Clifton Park, NY: Delmar, 127-152.
Schein, E.H. 1985. Organizational Culture and Leadership: A DynamicView. San Francisco, CA: Jossey-Bass.
Shellenbarger, S. April 9, 1997. “Good, Early Care Has a Huge Impact on Kids, Studies Say.” The Wall Street Journal, B1.
Shi, L., and D.A. Singh. 2008. Delivering Health Care in America: A Systems Approach, 4th ed. Sudbury, MA: Jones and Bartlett.
Schill, M. 2008. “U.S. Population Distribution by Age, 2007, Baby Boom Generation.” Retrieved May 9, 2009 from http://www.newgeography.com/content/00193-us-population-distribution-age-2007-baby-b.
Thomasson, M. 2002. “From Sickness to Health: The Twentieth Century Development of U.S. Health Insurance.” Exploratory Economic History32: 233-253.
Ubokudom, S.E. 1998. “The Association Between the Organization of Medical Practice and Primary Care Physician Attitudes and Practice Orientations.” Socia Science and Medicine 46(1): 59-71.
- 359 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization

Ubokudom, S.E. 2003. “Managed Care and the Agitation for a Patient’s Bill of Rights: A Historical and Theory-Based Analysis.” Journal of Public Affairs & Issues 7(1), 57-76.
Ubokudom, S.E. 2008a. “The Ecology of Public Policy and Administration in Nigeria.” Public Policy Journal (APPA-Nigeria) 2(1), 1-19.
Ubokudom, S.E. 2008b. “Employer-Sponsored Insurance (ESI), Medicare and Medicaid Policy Changes, and the Future.” Pulse (Ohio Chapter, American College of Surgeons, Membership Edition, 2008 Desktop Reference Guide): 19-25.
U.S. Census Bureau. 2007a. “2007 Population Estimates.” Retrieved April 12, 2009 from http://factfinder.census.gov/servlet/DTTable?_bm=y&-geo_id=01000US&-ds_name=PEP.
U.S. Census Bureau. 2007b. “Income, Poverty, and Health Insurance Coverage in the United States: 2007.” (U.S. Department of Commerce Publication No. P60-235), Washington, DC: U.S. Government Printing Office.
U.S. Centers for Disease Control and Prevention. 2009. “Key Facts About Swine Influenza.” Retrieved May 20, 2009 from http://www.cdc.gov/h1n1flu/key_facts.htm
United States Centers for Medicare & Medicaid Services (CMS) 2009a. “National Health Expenditure Web Tables.” Retrieved April 6, 2009 from http://www.cms.hhs.gov/NationalHealthExpendData/downloads/tables.pdf.
United States Centers for Medicare & Medicaid Services (CMS) 2009b. “2009 Annual Report of the Board of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds.” Retrieved April 6, 2009 from http://www.cms.hhs.gov/ReportsTrustFunds/download/tr2009.pdf.
U.S. Department of Health & Human Services. 2008. “A Profile of Older Americans, 2008.” Retrieved April 8, 2009 from http://www.aoa.gov/AOARoot/Aging_Statistics/Profile/2008/2.aspx
Vig, N.J. 2000. “Presidential Leadership and the Environment: From Reagan to Clinton,” in Environmental Policy, 4th ed., eds. N.J. Vig and M.E. Kraft. Washington, DC: CQ Press, 98-120.
Watts, S. 1997. Epidemics in History: Disease, Power and Imperialism. New Haven, CT: Yale.
Weissert, C., and W. Weissert. 2002. Governing Health: The Politics of Health Policy, 2nd ed. Baltimore, MD: Johns Hopkins.
Wiener, J.M., L.H. Illston, and R.J. Hanley. 1994. Sharing the Burden: Strategies for Public and Private Long-Term Care Insurance. Washington, DC: Brookings.
- 360 -
World Medical & Health Policy, Vol. 2 [2010], Iss. 1, Art. 19
http://www.psocommons.org/wmhp/vol2/iss1/art19DOI: 10.2202/1948-4682.1010

Wilkinson, R.G. 1997. “Comment: Income Inequality, and Social Cohesion.” American Journal of Public Health 87: 1504-1506.
Winkelstein, Jr. W. 1993. “Letter: Medical Care is Not Health Care.” JAMA 269(19): 2504.
Woolley, J.T. and G. Peters. 2008. “The American Presidency Project: Democratic and Republican Party Platforms.” Retrieved March 26, 2009 from http://www.presidency.ucsb.edu/ws/print.php?pid=78283&78545
Wynder, E.L. and M.A. Orlandi. 1984. The American Health Foundation Guide to Lifespan Health. A Family Program for Physical and Emotional Well-Being. NY: Dodd, Mead & Company.
- 361 -
Ubokudom and Khubchandani: Ecological Factors and U.S. Health Policy
© 2010 Policy Studies Organization