Embed Size (px)
Citation preview

The ECHELON-2 trial: Results of a randomised, double-blind,
active-controlled phase 3 study of brentuximab vedotin and CHP
vs CHOP in the frontline treatment of patients with CD30+
peripheral t-cell lymphomas
Lorenz Trümper1, Owen A. O'Connor2, Barbara Pro3, Tim M. Illidge4, Ranjana H Advani5, Nancy L. Bartlett6, Jacob Haaber Christensen7,
Franck Morschhauser8, Eva Domingo-Domenech9, Giuseppe Rossi10, Won Seog Kim11, Tatyana A. Feldman12, Anne Lennard13,
David Belada14, Árpád Illés15, Kensei Tobinai16, Kunihiro Tsukasaki17, Su-Peng Yeh18, Andrei R. Shustov19, Andreas Hüttmann20,
Kerry J Savage21, Sam Yuen22, Swaminathan Iyer23, Pier Luigi Zinzani24, Zhaowei Hua25, Veronica Bunn25, Meredith Little25,
Shangbang Rao26, Joseph Woolery26, Thomas Manley26, Steven M. Horwitz27
1Professor Lorenz Trümper, Department of Hematology and Oncology, Universitätsmedizin Göttingen, Göttingen, Germany; 2Division of Hematology/Oncology, Columbia University Medical Center, New York, NY, United States; 3Department of Medicine, Northwestern
University Feinberg School of Medicine, Chicago, IL, United States; 4Division of Cancer Sciences, Faculty of Biology, Medicine and Health, University of Manchester, NIHR Biomedical Research Centre, Manchester Academic Health Sciences Centre, Christie Hospital
NHS Foundation Trust, Manchester, United Kingdom; 5Blood and Marrow Transplant Program, Stanford Cancer Center, Palo Alto, CA, United States; 6Siteman Cancer Center, Washington University School of Medicine, Saint Louis, MO, United States; 7Department of
Hematology, Odense University Hospital, Odense, Denmark; 8Department of Hematology, CHRU de Lille, Lille, France; 9Department of Hematology, Institut Catala D'oncologia, L'Hospitalet de Llobregat, Barcelona, Spain; 10Department of Hematology, Azienda
Ospedaliera Spedali Civili di Brescia, Brescia, Italy; 11Samsung Medical Center, Seoul, Republic of South Korea; 12Hackensack University Medical Center, Hackensack, NJ, United States; 13Freeman Hospital, Newcastle upon Tyne, United Kingdom; 144th Department of
Internal Medicine - Hematology, University Hospital, Hradec Králové, Czech Republic AND Charles University, Faculty of Medicine, Prague, Czech Republic; 15Debreceni Egyetem, Debrecen, Hungary; 16Department of Hematology, National Cancer Center Hospital,
Tokyo, Japan; 17Saitama Medical University, International Medical Center, Department of Hematology, Saitama, Japan; 18China Medical University Hospital, Taichung, Taiwan; 19Division of Hematology, University of Washington Medical Center, Seattle, WA, United
States; 20Klinik für Hämatologie, Universitatsklinikum Essen, Essen, Germany; 21Department of Medical Oncology, University of British Columbia and the Department of Medical Oncology, British Columbia Cancer Agency Centre for Lymphoid Cancer, Vancouver,
Canada; 22Department of Hematology, Calvary Mater Newcastle Hospital, Waratah, Australia; 23Department of Lymphoma and Myeloma, MD Anderson Cancer Center/University of Texas, Houston, United States; 24University of Bologna, Institute of Hematology
“Seràgnoli”, Bologna, Italy; 25Takeda Pharmaceuticals International Company, Cambridge, MA, United States; 26Seattle Genetics, Inc., Bothell, WA, United States; 27Department of Medicine, Memorial Sloan Kettering Cancer Center, Basking Ridge, NJ, United States.

Disclosures
• This study was funded by Seattle Genetics, Inc. and Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited. This research was funded in part
through the National Institutes of Health/National Cancer Institute Cancer Center Support Grant P30 CA008748.
• LT, receiving grant support from Seattle Genetics and the German Ministry of Education and Research (Bundesministerium für Bildung und Forschung) and grant and non-financial support from
Genzyme; OAO, receiving support from Seattle Genetics to conduct the study; BP, receiving consultancy fees from Seattle Genetics, research funding from Seattle Genetics, honoraria fees and travel
expenses from Seattle Genetics and Takeda; TI, receiving personal fees from Takeda; RA, receiving grant support from Agensys, Celgene, Forty Seven, Infinity, Janssen, Kura Oncology, Merck,
Millennium, and Regeneron, grant support and consulting and advisory fees from Bristol Myers Squibb, Genentech/Roche, Pharmacyclics, and Seattle Genetics, consulting and advisory fees from
Astra Zeneca, Autolus, Bayer Healthcare Pharmaceuticals, Gilead, Juno, Kite, Kyowa Hakko Kirin, NanoString, Spectrum, Sutro Biopharma, and Takeda, and Data Safety Monitoring Board fees from
Cell Medica; NLB, receiving research funding from Celgene, Seattle Genetics, Genentech, Kite, Merck, Bristol-Meyers Squibb, Immune Designs, Forty Seven, Affimed, Janssen, Pharmacyclics,
Millennium, and Gilead, and advisory board fees from Acerta and Pfizer; FM, receiving honoraria from Takeda, advisory board fees from Bristol-Myers Squibb, lecture fees from Janssen, advisory
board and lecture fees from Celgene and Roche, consultant fees from Epizyme, and consultant, advisory board, and lecture fees from Gilead; EDD, receiving non-financial support from Seattle
Genetics and personal fees from Bristol-Myers Squibb, Roche, and Takeda, advisory board and consultancy fees from Takeda; GR, receiving research support from Seattle Genetics, advisory board
fees from Roche, Celgene, Janssen, Amgen, Gilead, Sanofi, Pfizer, AbbVie, Jazz Pharmaceuticals, and Teva, honoraria fees from Novartis, Bristol-Myers Squibb, Mundipharma, Daiichi, and Sandoz,
travel expenses from Alexion, Celgene, and Gilead; TF, receiving honoraria from Abbvie, Bayer, Bristol-Myers Squibb, Kite Pharma, Pharmacyclics/Janssen, Seattle Genetics and Takeda; advisory
board and consulting fees from Bayer, Bristol-Myers Squibb and Seattle Genetics; speakers’ bureau for Abbvie, Celgene, Janssen, Kite Pharma, Pharmacyclics and Seattle Genetics; Research
Funding from Amgen (Inst), Bristol-Myers Squibb (Inst), Cell Medica (Inst), Eisai (Inst), Kyowa Hakko Kirin (Inst), Kyowa Hakko Kirin (Inst), Pfizer (Inst), Portola Pharmaceuticals (Inst), Roche (Inst),
Seattle Genetics (Inst), Trillium Therapeutics (Inst) and Viracta Therapeutics (Inst); Travel, Accommodations, Expenses from Abbvie, Kite Pharma, Pharmacyclics, Seattle Genetics and Takeda; AL,
receiving honoraria and advisory board fees from Janssen and Roche, and grant support from Seattle Genetics; DB, receiving research support from Seattle Genetics and consultant and advisory
board fees from Takeda; KTo, receiving grant support from AbbVie, personal fees from Zenyaku Kogyo, HUYA Bioscience International, Yakult, Daiichi Sankyo, Bristol-Myers Squibb, Meiji Seika
Kaisha, Solasia Pharma, and Verastem, and grant support and personal fees from Takeda, Eisai, Celgene, Mundipharma, Kyowa Hakko Kirin, Chugai Pharma, and Ono Pharma; KTs, receiving grant
support from Seattle Genetics, Chugai Pharma, HUYA, and Eisai, consultancy fees from Ono Pharma, HUYA, and Daiichi-Sankyo, honoraria from Celgene, Chugai Pharma, Kyowa-hakko/ Kirin, and
Mundy Pharma; AS, receiving research funding from Seattle Genetics; AH, receiving grant support, honoraria and drug supply for study conduct from Takeda, research funding from Seattle Genetics,
and travel expenses from Celgene and Roche; KJS, receiving honoraria and advisory board fees from Seattle Genetics, and honoraria from Takeda during the conduct of the study, honoraria and
advisory board fees from Bristol-Myers Squibb, Merck, Verastem, and consulting fees from Servier; SI, receiving grant support from Seattle Genetics, Takeda, Roche, Rhizen, Spectrum, Celgene,
Gilead, Novartis, Amgen, and Trillium; PLZ, receiving advisory board fees and honoraria from Gilead, Sandoz, Johnson & Johnson, Bristol-Myers Squibb, Servier, Takeda, Celtrion, Roche, and
Celgene; ZH, employment with Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited ML, employment with Millennium Pharmaceuticals, Inc., a
wholly owned subsidiary of Takeda Pharmaceutical Company Limited, and holding shares in Takeda Pharmaceutical Company Limited; SR and JW being employed by and holding shares in Seattle
Genetics; TM, being employed by and holding shares in Seattle Genetics and has a patents 62/580,261, 62/739,631, and 62/739,635 licensed to Takeda (all ex-US, except Canada); SH, reports
receiving grant support from Spectrum, grant support and personal fees from Seattle Genetics, Inc., Takeda, Kyowa Hakka Kirin, Verastem Oncology, Aileron, ADC Therapeutics, Celgene, and Forty
Seven, and personal fees from Portola, Corvus, Miragen, and Innate. JHC, WSK, AI, SPY, and SY, have nothing to disclose.

Background
• Peripheral (mature nodal) T cell lymphoma is a rare and heterogeneous group of lymphoid malignancies
• Across all subtypes, approximately 50% of patients express to a certain degree CD301,2
– Systemic Anaplastic large cell lymphoma sALCL expresses CD30 on all lymphoma cells
– Variable CD30 expression among other T-cell lymphomas on lymphoma and bystander cells
• Frontline standard of care for PTCL is a CHOP or CHOEP regimen with curative intent, however this often
results in:3–5
– Unsatisfactory outcomes for patients with PTCL due to a high risk for early disease progression and relapse
– ALK+ sALCL is an exception, with more favourable outcomes dependent upon age and IPI
ALK, anaplastic lymphoma kinase; ALK+, ALK-postitive; CHOP, cyclophosphamide, doxorubicin, vincristine, and
prednisone; IPI, international prognostic index; PTCL, peripheral T-cell lymphoma; sALCL, systemic anaplastic large
cell lymphoma
1. Bossard C, et al. Blood 2014;124: 2983–6.
2. Sabattini E, et al. Haematologica 2013;98: e81–82.
3. Savage KJ, et al. Ann Oncol 2004;15: 1467–75.
4. Savage KJ, et al. Blood 2008;111: 5496–504.
5. Simon A, et al. Br J Haematol 2010;15: 159–66.

Background (cont’d)
• Brentuximab vedotin, an antibody-drug conjugate targeting CD30, is approved in the US,1 EU,2 and Japan3 for
relapsed/refractory sALCL
• A phase 1 study (NCT01309789) of frontline brentuximab vedotin + CHP (A+CHP) found encouraging results:4
– Manageable safety profile
– At 5 years, 50% of patients remained in remission with no subsequent anticancer therapy
– Median OS was not reached
• The relationship between tumour CD30 expression levels and response to brentuximab vedotin has not been
fully established for patients with PTCL
• The ECHELON-2 trial was designed to compare the effects of frontline A+CHP versus CHOP in patients with
CD30+ PTCL
• We present the initial results of ECHELON-2, now including response to A+CHP by CD30 expression in
patients with AITL and PTCL-NOS
CD30+, CD30-positive; A+CHP, brentuximab vedotin plus cyclophosphamide, doxorubicin, and
prednisone; EU, European union; NOS, not otherwise specified; OS, overall survival; US, United States
1. ADCETRIS® (brentuximab vedotin) US Prescribing Information, November 2018.
2. ADCETRIS® (brentuximab vedotin) Summary of Product Characteristics, March 2019.
3. ADCETRIS® (brentuximab vedotin) Japanese package insert, 2018.
4. Fanale MA, et al. Blood 2018;131: 2120–4.
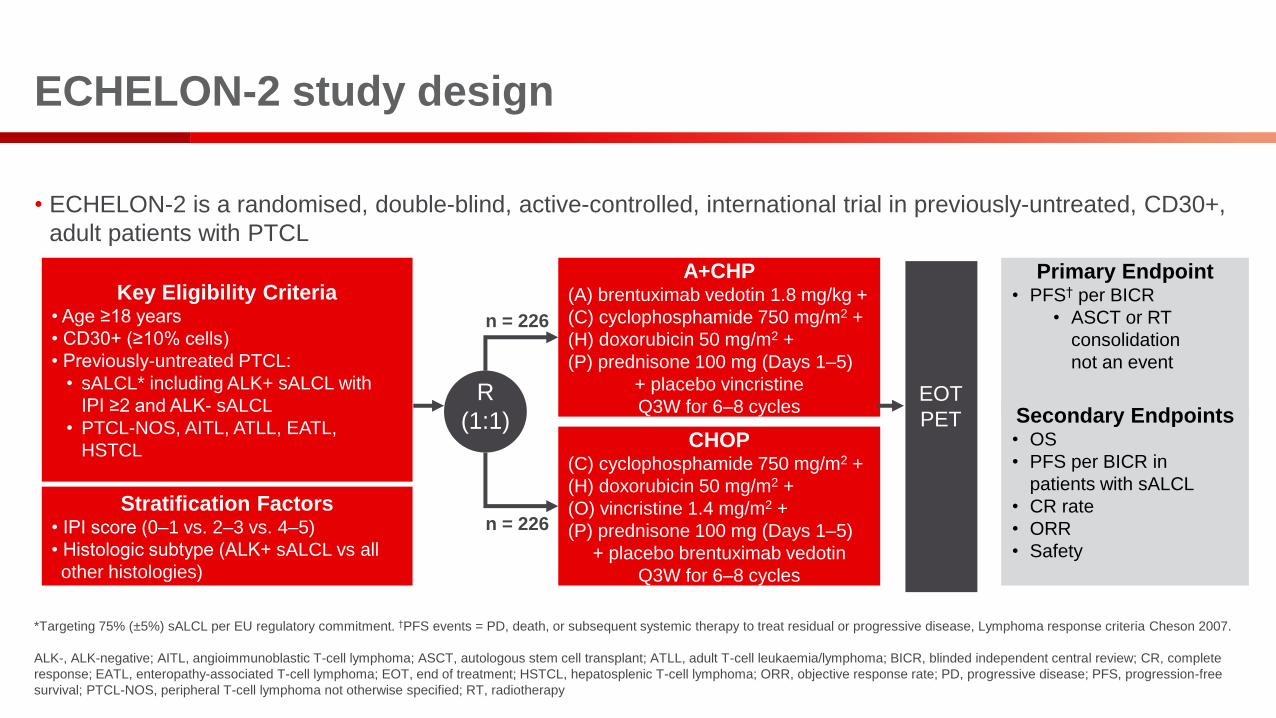
ECHELON-2 study design
• ECHELON-2 is a randomised, double-blind, active-controlled, international trial in previously-untreated, CD30+,
adult patients with PTCL
Primary Endpoint• PFS† per BICR
• ASCT or RT
consolidation
not an event
Secondary Endpoints• OS
• PFS per BICR in
patients with sALCL
• CR rate
• ORR
• Safety
CHOP(C) cyclophosphamide 750 mg/m2 +
(H) doxorubicin 50 mg/m2 +
(O) vincristine 1.4 mg/m2 +
(P) prednisone 100 mg (Days 1–5)
+ placebo brentuximab vedotin
Q3W for 6–8 cycles
A+CHP(A) brentuximab vedotin 1.8 mg/kg +
(C) cyclophosphamide 750 mg/m2 +
(H) doxorubicin 50 mg/m2 +
(P) prednisone 100 mg (Days 1–5)
+ placebo vincristine
Q3W for 6–8 cycles
Key Eligibility Criteria• Age ≥18 years
• CD30+ (≥10% cells)
• Previously-untreated PTCL:
• sALCL* including ALK+ sALCL with
IPI ≥2 and ALK- sALCL
• PTCL-NOS, AITL, ATLL, EATL,
HSTCL
Stratification Factors• IPI score (0–1 vs. 2–3 vs. 4–5)
• Histologic subtype (ALK+ sALCL vs all
other histologies)
*Targeting 75% (±5%) sALCL per EU regulatory commitment. †PFS events = PD, death, or subsequent systemic therapy to treat residual or progressive disease, Lymphoma response criteria Cheson 2007.
ALK-, ALK-negative; AITL, angioimmunoblastic T-cell lymphoma; ASCT, autologous stem cell transplant; ATLL, adult T-cell leukaemia/lymphoma; BICR, blinded independent central review; CR, complete
response; EATL, enteropathy-associated T-cell lymphoma; EOT, end of treatment; HSTCL, hepatosplenic T-cell lymphoma; ORR, objective response rate; PD, progressive disease; PFS, progression-free
survival; PTCL-NOS, peripheral T-cell lymphoma not otherwise specified; RT, radiotherapy
EOT
PET
R
(1:1)
n = 226
n = 226

Baseline characteristics and patient disposition
A+CHP
(n = 226)
CHOP
(n = 226)
Male, n (%) 133 (59) 151 (67)
Age in years, median (range) 58 (18-85) 58 (18-83)
IPI score, n (%)
0–1 53 (23) 48 (21)
2–3 140 (62) 144 (64)
4–5 33 (15) 34 (15)
Stage III/IV, n (%) 184 (81) 180 (80)
Disease diagnosis, n (%)
sALCL 162 (72) 154 (68)
ALK+ 49 (22) 49 (22)
ALK- 113 (50) 105 (46)
PTCL-NOS 29 (13) 43 (19)
AITL 30 (13) 24 (11)
ATLL 4 (2) 3 (1)
EATL 1 (0) 2 (1)
A+CHP
(n = 226)
CHOP
(n = 226)
Randomized, n (%) 226 (100) 226 (100)
Treated, n (%) 223 (99) 226 (100)
Completed treatment 192 (85) 178 (79)
Discontinued treatment
Progressive disease 7 (3) 26 (12)
AE 15 (7) 15 (7)
Other 9 (4) 7 (3)
Consolidative therapy* 61 (27) 44 (19)
Radiotherapy 14 (6) 6 (3)
Stem cell transplantation 50 (22) 39 (17)
*Patients may have received more than one type of therapy.
Enrolment: Jan 2013 – Nov 2016; Data cut-off: Aug 15, 2018AE, adverse event
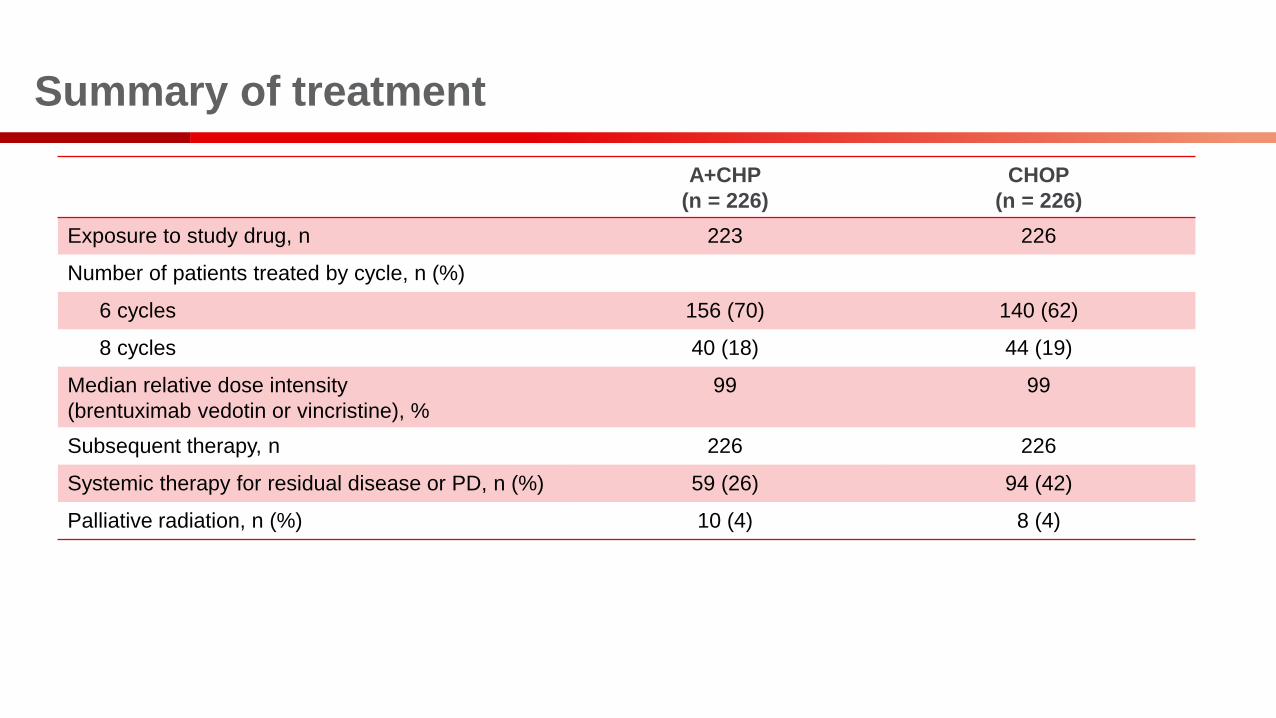
Summary of treatment
A+CHP
(n = 226)
CHOP
(n = 226)
Exposure to study drug, n 223 226
Number of patients treated by cycle, n (%)
6 cycles 156 (70) 140 (62)
8 cycles 40 (18) 44 (19)
Median relative dose intensity
(brentuximab vedotin or vincristine), %
99 99
Subsequent therapy, n 226 226
Systemic therapy for residual disease or PD, n (%) 59 (26) 94 (42)
Palliative radiation, n (%) 10 (4) 8 (4)

A+CHP significantly improved PFS in the ITT population
compared with CHOP
HR, hazard ratio; ITT, intention-to-treat; NE, not estimable

PFS for A+CHP versus CHOP across different subgroups

A+CHP significantly improved OS in the ITT population
compared with CHOP

A+CHP significantly improved all other secondary efficacy
endpoints in the ITT population compared with CHOP
A+CHP
(n = 226)
CHOP
(n = 226)
P-value
Remission rates in the ITT
population at EOT
CR rate (%) 68 56 0.0066
ORR (%) 83 72 0.0032
sALCL subset analysis 163 151
Patients with a PFS event, n (%) 56 (34) 73 (48)
Hazard ratio 0.59 (95% CI: 0.42, 0.84) 0.0031

Safety summary
0
10
20
30
40
50
A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP A+CHP CHOP
Grade <3 Grade ≥3
PSN, peripheral sensory neuropathy
Nausea PSN Neutropenia Diarrhoea Constipation Alopecia Pyrexia Vomiting Fatigue Anaemia
Adverse events, n (%) A+CHP (n = 223) CHOP (n = 226)
Any adverse events 221 (99) 221 (98)
Grade ≥3 adverse events 147 (66) 146 (65)
Serious adverse events 87 (39) 87 (38)
Deaths due to adverse events 8 (4) 16 (7)
46%
38% 38%
20%
29% 30%26%
17%
45%41%
26%
19%24%
20%
38% 38%
21%16%
26% 25%
AES in ≥20% of patients
Incid
en
ce, %

Incidence and severity of neutropenia were similar across
treatment arms
0
10
20
30
40
50
(-) (+) (-) (+) (-) (+) (-) (+)
Grade <3 Grade ≥3
*The use of G-CSF was permitted at the discretion of the treating physician based upon institutional standards. In May 2015, the Independent Data Monitoring Committee recommended that Seattle Genetics
remind investigators to administer G-CSF in accordance with American Society of Clinical Oncology or European Society of Medical Oncology guidelines.
G-CSF, granulocyte colony stimulating factor
A+CHP CHOP A+CHP CHOP
G-CSF
Neutropenia Febrile neutropenia
Incid
en
ce,
%
• Incidence of treatment-emergent
neutropenia was:
– A+CHP 38% (n=85)
– CHOP 38% (n=85)
• Incidence of treatment-emergent
febrile neutropenia was:
– A+CHP 18% (n=41)
– CHOP 15% (n=33)
• Primary prophylactic G-CSF was
permitted at the investigator’s
discretion* and reduced the incidence
and severity of grade ≥3 neutropenia
and febrile neutropenia
38% 38%
16% 16% 16%18%
15%11%

Incidence of treatment-emergent PN was similar across
treatment arms
• Treatment-emergent PN events occurred in 117 (52%) patients in A+CHP and 124 (55%) patients in CHOP
• Most PN events were grade 1 (A+CHP = 75 [64%] and CHOP = 88 [71%])
Patients, n (%) A+CHP
(n=223)
CHOP
(n=226)
Treatment-emergent PN, 117 124
Resolution* of all PN events 58 (50) 79 (64)
Ongoing PN at last follow-up 61 (52) 45 (36)
Grade 1 44 (72) 32 (71)
Grade 2 15 (25) 12 (27)
Grade 3 2 (3) 1 (2)
*Resolution was defined as resolved/recovered with or without sequelae, or return to baseline or lower severity as of the latest assessment for pre-existing events
PN, peripheral neuropathy
0
10
20
30
40
50
60
A+CHP CHOP
Grade 1 Grade 2 Grade 3 Grade 4
Patients
, %

CD30 expression by response in patients with AITL in the
A+CHP treatment arm*
• Most AITL patients (26/29, 90%) had a CD30 expression range of 10–30%
– AITL median CD30 expression = 18%
– AITL mean CD30 expression = 20%
IRF, independent review facility; PR, partial response, SD, stable disease
*This was an exploratory analysis.
40
0
20
60
All patients CR PR SD PD
Response at EOT by IRF
CD
30 (
local)
CD30 in individual patients
Mean CD30

CD30 expression by response in patients with PTCL-NOS in
the A+CHP treatment arm*
• PTCL-NOS patients had a CD30 expression range of 10–100%
– PTCL-NOS median CD30 expression = 25%
– PTCL-NOS mean CD30 expression = 41%
*This was an exploratory analysis.
40
0
20
60
All patients CR PR PD
Response at EOT by IRF
CD
30
(lo
ca
l)
80
100
CD30 in individual patients
Mean CD30

CR and PR rates across CD30 subgroups in patients with
AITL or PTCL-NOS*
• CR rates in patients with AITL (p=0.84) and PTCL-NOS (p=0.44) were independent of the level of CD30
expression (above vs below the median)
• CRs and PRs were observed across the range of CD30 expression, including CD30 = 10%
*This was an exploratory analysis.†Cochran-Mantel-Haenzel test comparing CR rates in patients with CD30 above versus below median‡Patients with CD30 = 10% were included in the category CD30 ≤ median
CD30 Patients, n CR, n (%) PR, n (%)
P-value, CR rates for
CD30 above vs
below median†
AITL
CD30 >median 14 8 (57) 1 (7)
0.84CD30 ≤median‡ 15 8 (53) 3 (20)
CD30 = 10% 8 5 (63) 0
PTCL-NOS
CD30 >median 14 8 (57) 2 (14)
0.44CD30 ≤median‡ 14 10 (71) 2 (14)
CD30 = 10% 6 4 (67) 2 (33)

Conclusions
• ECHELON-2 is the first prospective trial in PTCL to show an OS benefit of A+CHP versus CHOP
• A+CHP provided clinically meaningful improvement in PFS and OS versus CHOP including:
– 29% reduction in the risk of a progression event
• 3-year PFS: A+CHP, 57% versus CHOP, 44%
– 34% reduction in the risk of death
• A+CHP has a comparable safety profile to CHOP
• The degree of CD30 expression alone, as measured by IHC, does not predict benefit from A+CHP
• The FDA approved brentuximab vedotin in combination with CHP for adults with previously-untreated sALCL or
other CD30-expressing PTCL, including AITL and PTCL-NOS
• EMA decision is expected in early 2020
FDA, food and drug administration

Acknowledgements
• The authors would like to thank:
– The patients who participated in this study and their families
– Other investigators and staff at all ECHELON-2 clinical sites
– The members of the Independent Data Monitoring Committee and Independent Review Committee
– Bill Treppicchio for biomarker analyses and interpretation of data
• We acknowledge
– Rebecca Vickers of FireKite, an Ashfield company, part of UDG Healthcare plc, for editorial support during the
development of these slides, which was funded by Millennium Pharmaceuticals, Inc., and complied with Good
Publication Practice 3 ethical guidelines1
• This research was funded by Seattle Genetics, Inc., and Millennium Pharmaceuticals, Inc., a wholly
owned subsidiary of Takeda Pharmaceutical Company Limited
1. Battisti WP, et al. Ann Intern Med 2015;163:461–4.














![Mesa 4 [ATS] A phase I, randomised, double blind, placebo ... · [ATS] A phase I, randomised, double blind, placebo controlled, study to assess the safety, tolerability and pharmacokine8cs](https://img.dokumen.tips/doc/110x75/5d15c00d88c993a82b8b4970/mesa-4-ats-a-phase-i-randomised-double-blind-placebo-ats-a-phase.jpg)














