Embed Size (px)
Citation preview

Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746
Contents lists available at ScienceDirect
Best Practice & Research ClinicalObstetrics and Gynaecology
journal homepage: www.elsevier .com/locate /bpobgyn
4
The E-learning revolution in obstetrics and gynaecology
Oliver Jones, MA, ODE, BSc (Hons), Education Projects Manager a,*,Helen Saunders, MSci, E-learning Publication Manager a, Gary Mires, MD,FRCOG, FHEA, Director of E-learning, Professor of Obstetrics andUndergraduate Teaching Dean a,b
aRoyal College of Obstetricians and Gynaecologists, London, UKbNinewells Hospital and Medical School, Dundee, Scotland, UK
Keywords:e-learningdistance learningonline learningeportfolioStratOG.net
* Corresponding author.E-mail address: [email protected] (O. Jones).
1521-6934/$ – see front matter � 2010 Elsevier Ltdoi:10.1016/j.bpobgyn.2010.04.009
The explosion of information technology has created new oppor-tunities and tools to assist the trainee in the process of learning.This chapter describes how the Royal College of Obstetricians andGynaecologists (RCOG) is embracing the opportunities provided bythis technology to create interactive and engaging learning pro-grammes designed to support trainees in achieving the knowl-edge, skills and attitudes required to practise. It considers how theRCOG has developed a number of online initiatives to supporttraining, the drivers for doing so and presents some ideas forfuture developments.
� 2010 Elsevier Ltd. All rights reserved.
Background
The Internet boom continues and accessing information and communicating online has becomea significant part of all clinicians’ working and personal lives. In the last decade the advent of infor-mation technology has influenced how trainees think about learning in terms of the way they want tolearn, the way they realise they can learn and the sophistication of learning technology whichpotentially allows them to enjoy a high quality, stimulating experience.14
The RCOG has established that learners who are becoming accustomed to e-learning have fargreater expectations for interaction with a learning resource than a traditional learner and indeed,digital natives’ attention spans work very differently. Traditional learning resources such as books andjournals have always been broken down into chapters, and text, images and figures have been used forlearners to visualise and digest concepts more easily. However, e-learning has taken learners’
d. All rights reserved.

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746732
expectations to another level and a certain amount of entertainment is expected through realisticvideo, animation and audio used in an e-learning format.
Learners require approaches to teaching and learning that suit their individual learning styles andthat are:
� Accessible� Intuitive� Memorable� Enjoyable� Affordable
E-learning has the potential to meet all of these criteria. It is appropriate that an organisation suchas the RCOG, in striving to meet all learners’ needs, should consider how it can best use all the toolsavailable to enhance the learning experience for all learners, which includes those in training andcontinuing professional development (CPD) programmes. It is vital, however, to remember that thetechnology is a means to an end and not an end in its own right, and that educational content remainskey with technology simply being a means to facilitate its delivery.
Time for education and training
The European TimeWorking Regulation (EWTR) was introduced in 2009 1b following the EuropeanWorking Time Directive 1a and in association with Modernising Medical Careers (MMC).9 The intro-duction of the EWTR andMMC has reduced the amount of time individual trainees now spend at work,including study time. The combined effect of this means that trainees now have to achieve clinicalcompetencies, develop skills and confidence and continually develop knowledge to achieve therequirements of the Specialty Training and Education Programme in Obstetrics and Gynaecology ina much shorter time period than before. This means that teaching and learning opportunities must bemaximised within the available workplace time. In addition, UK study budgets and the professionalleave allowance for trainees to travel to national meetings, for example, those organised by the RCOG,have been reduced. Trainees are therefore now seeking alternative approaches to support theirlearning both to maximise workplace learning and to facilitate self-directed learning at other times.
E-learning has the potential to deliver such opportunities. It is convenient, it provides access toeducational materials at any time, it allows progress at the individual learner’s own pace, it accom-modates many learning styles and can enhance the learning process with the use of multimedia andinteraction. Online learners also have more time to reflect on their learning and have more flexibility tojoin ‘chat rooms’ or threaded discussions compared with learners in a classroom-based course.
Trainees quite rightly demand teaching resources of high quality. Feedback from trainees inobstetrics and gynaecology suggests that local courses vary in terms of quality and frequency. Theproduction of high quality teaching resources is time-consuming and represents an unrealisticexpectation for the majority of practising consultants. To address these issues the RCOG has invested indistance learning programmes and subject-specific resources for trainees. The RCOG believes that byimplementing pre-constructed learning modules to support clinical practice, it will not only provideaccessible resources for trainees, but also enable supervisors to use these resources to deliver highquality training locally and to provide consistency in content across the different training regions.
The RCOG has therefore embraced e-learning and the next section discusses the evolution inapproach adopted by the RCOG over the past decade.
The evolution of e-learning at the RCOG
Over the last decade distance learning opportunities provided by the RCOG have evolved andcontinue to do so. The first distance learning product to support trainees produced by the RCOG wasStratOG (2000). Initially paper-based supported by a static website and now an interactive onlineeducational package (StratOG.net), StratOG is a Structured Training Resource to Assist Trainees in

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 733
Obstetrics and Gynaecology. In its original format the website held a library of archived journal articles,answers to assessments, a chat room and message board. To standardise the educational experience,provide familiarity and provide a common structure, tutorials all had the same format (Table 1).
At the same time, the RCOG also worked with a partner to develop a case-based learning CDresource called DIALOG (Distance Interactive Learning in Obstetrics and Gynaecology) producedprincipally for CPD purposes. The format is described in Table 2.
Influences on the evolution of RCOG e-learning resources
Feedback
Feedback from trainees on the first edition of StratOG indicated that they found the resource usefulin preparing for the MRCOG examination, they considered the level of content appropriate, they valuedthe electronic support resources and would recommend it to other trainees. However, it was clear thatthere were deficiencies in the topics covered and the structure did not have a clear relationship to thenew curriculum format. Also, the split paper-based/online elements were not user friendly and hadlimited interactivity. It was very text heavy and the self-assessments were limited.
The curriculum launched in 2007
By 2007, a new RCOG specialty training curriculum had been developed to produce safe, competentclinicians who would meet the requirements detailed in The Future Role of the Consultant 10 and GoodMedical Practice.5 Its defined objectives related to:
� Knowledge� Clinical competencies� Professional skills and attitudes
Table 1StratOG learning design
StratOG tutorial content Description and purpose
Aims and objectives Clearly defined aims and objectives which relatedto the RCOG curriculum modules
Preliminary reading Background reading for the learner to read beforecommencing the tutorial. The preliminary readingwas designed to provide preparatory material toenhance understanding of the tutorial. The textswere available online
Pre-test A set of true or false questions to assess the learner’scurrent knowledge of the tutorial subject
Educational text Learning text to support learningImages, graphs, figures Visual presentations to further explain text and
enhance understandingDetailed references to guidelines
and relevant recommended readingsFurther texts for learners to access throughout the tutorial.Texts available online
True or false, multiple choice questionsand short essay questions
Questions to test learner understanding and progress towardsachieving the objectives of the tutorial at relevant parts. Answerswould be available online but with no control as to when thelearner accessed the answers
Case studies Case-based learning for learners to understand the subject incontext and apply the knowledge gained from the educational text
Peer-based exercises Allied to the case studies, these exercises structured a discussionbetween the learner and their colleagues in real time or using thechat forum or discussion board
Post-test Repetition of the pre-test for the learner to re-assess the knowledgegained and confirm achievement of the objectives

Table 2DIALOG learning design
DIALOG content Description and purpose
Aims and objectives Clearly defined aims and objectivesBackground Based around clinical scenariosManagement Question-based management options (RCOG guidelines referenced)Justifications Justifications for the management options. Enables the learner to be
assessed on their decision making abilitiesImages, graphs, figures Colour images, video and audio clips to enhance understandingTrue or false, multiple
choice questionsVarious question formats to test learner understanding andachievement of tutorial objectives
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746734
The curriculum is modular and for each module the above criteria were clearly defined.12 Thisprovided a potential structure around which to design the next version of StratOG to deliver appro-priate elements of the curriculum.
Advances in technology, meeting individuals’ learning style requirements and consideration of optimisinglearning designs
Learning technology (LT) and internet connectivity in the workplace and at home had developedmaking it possible to improve elements identified as weaknesses in the feedback from the first editionof StratOG. In recognising the importance of not overwhelming trainees with “the razzmatazz of thelatest technology” 13 the RCOG was cautious about re-developing StratOG with too many multimediacomponents, but it also realised that improvements to certain functions would improve the learnerexperience.
In surveys carried out in 2006, trainees stated that they increasingly used the internet for bothworkand personal purposes. They could see how the internet could provide them with an opportunity togain knowledge in ‘bite-sized’ portions when studying alongside commitments in the workplace andclinical practice. This would allow them to see theories in practice with access to e-learning (text, videoor animation) close by. With these e-learning approaches, concepts can be more easily demonstratedthan in textbooks and journals. If an individual can visualise a concept by seeing a graphic or animationthen understanding and learning is potentially easier and the retention of information is potentiallygreater. The use of visual aids in learning has been demonstrated to be the most effective means ofachieving effective learning, regardless of age and experience, in secondary and also postgraduateeducation or beyond postgraduate education.8
For the purposes of implementing e-learning and distance learning inmedicine, there is a particularneed for programmes to promote critical thinking and, rather than constantly teach, to facilitate self-directed deeper learning, irrespective of different learning styles. Each learner has a different approachand response to learning and the RCOG’s learning design takes learning styles into consideration byincluding core knowledge, case-based discussions for the application of knowledge, self-assessments,and reflective learning exercises to review, reflect and conclude concepts from newly acquiredknowledge. Honey & Mumford 6 defined groups of learners as:
� Activists (Do)� Reflectors (Review)� Theorists (Conclude)� Pragmatists (Plan)
There are several requirements underpinning the obstetrics and gynaecology curriculum, whichessentially requires trainees to ‘do, review, conclude and plan’. The curriculum is diverse and sometrainees will manage the theoretical components more than the practical elements; however, duringa training programme, they must meet the required standards in all areas. It is essential to have theknowledge and experience to make decisions; it is essential to have the practical skills and also to havethe correct professional attitude and self-awareness. It is evident that e-learning and assessmentcannot directly develop or assess all these skills, but the RCOG sees e-learning as more than a tool to

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 735
deliver knowledge. The RCOG has intentionally developed e-learning to support key areas of thecurriculum so that learners regularly access learning content for the duration of a programme; not justto develop knowledge in a defined period leading up to an examination. Videos and case-basedlearning sessions, such as those in DIALOG, would ideally be accessed regularly to allow learners tocontinually evaluate their own practice and to keep up to date with developments to guidelines. Thereis a clear link between the curriculum and training support options.
Online training resources can assist with the development of practical skills, with online demon-strations of practices assisting trainees by preparing them for their first experience in clinical training:the early stages of a learning process defined as ‘knows’ and ‘knows how’ in Miller’s triangle (Fig. 1).
� Knows� Knows how� Shows how (competent)� Does (consistently performs competently)
Another useful classification of learning styles considered and used by the RCOG when designinge-learning is Fleming’s ‘VARK’,4 which emerged from neuro-linguistic programming models whichexplain that learning styles differ by a learner’s preferred modality of sensory intake:
� Visual (V) (Graphics, animations, charts)� Aural/auditory (A) (Audio clips, e-lectures)� Read/write (R) (Reading and reflective writing)� Kinesthetic (K) (Video clips, simulation, case studies)
E-learning can provide a ‘tactile’ learning environment when designed and built using differentmedia objects and tools as it is multi-faceted and has an ability to provide excellent provision for themajority of learning styles within any single e-learning session.
Current RCOG approaches to e-learning and future plans
STRATOG.NET
In 2005, based on the above drivers and considerations, the RCOG embarked upon a project toenhance the first edition of StratOG and to produce a fully online e-learning programme to support thenew curriculum: StratOG.net. The RCOG is an international organisation and by publishing completelyonline, the College could better serve its Fellows, Members and trainees due to the increased acces-sibility of e-products. A fully online programme would also be easier to keep up to date, and thetutorials could be quickly updated to reflect changes to the curriculum and new developments andguidelines.
Fig. 1. Miller’s triangle.
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746736
Successful components of the learning design of StratOG and DIALOG were to remain but, withmore sophisticated learning technology features and functionality, the overall educational experiencewas to be improved.
The team required to develop 12modules of StratOG.net included a team of Fellows andMembers ofthe RCOG. An Editor-in-Chief, 12 module leaders and over 100 authors have been engaged in theauthorship process and the continued success of StratOG.net is dependent on authors remainingdedicated to updating content based on changes to guidelines, changes to the curriculum and thefeedback received by the StratOG.net Editorial Board by users and expert reviewers. Two internaleditors with biomedical qualifications, instructional design expertise and experience of the e-learningpublication process are dedicated to ensure the standard of StratOG.net is maintained in the long termand that, as technology and learning media evolves, StratOG.net e-learning content remains suitablymodern.
StratOG.net aims
The principal function of StratOG.net is to facilitate trainees’ learning in preparation for theMembership of the Royal College MRCOG Part 2 examination and the content is set at this level. It can,however, be used by trainees in other countries and other professions as a learning resource and alsofor CPD purposes.
StratOG.net is amodular, self-directed e-learning resource. It consists of 12modules (Table 3), whichmirror in terms of content the 19 RCOG curriculum modules. Each StratOG.net module includes a vari-able number of e-tutorials written to address the knowledge and, where possible, skills and attitudinalelements of the curriculum. Table 4 gives examples of the e-tutorial content for three of the StratOG.netmodules. The e-tutorials were written by Fellows and Members of the RCOG and peer-reviewed.
E-tutorial design
As for the first edition of StratOG, all StratOG.net tutorials have a common format (Fig. 2), whichincludes:
� A brief introduction to the subject� A set of learning objectives� The author (e-tutor) profile� Hyperlinks to preliminary reading� Introductory assessments to assess existing knowledge� The main learning section, including:
B Main textB Hyperlinks to references, guidelines and external websitesB Key points and regular summaries (relating to the aims and objectives)
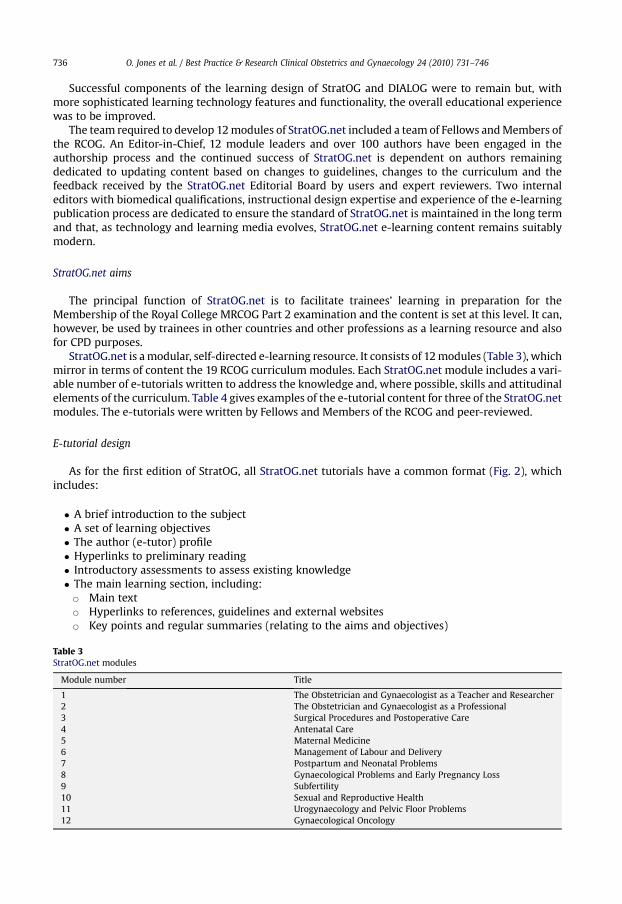
Table 3StratOG.net modules
Module number Title
1 The Obstetrician and Gynaecologist as a Teacher and Researcher2 The Obstetrician and Gynaecologist as a Professional3 Surgical Procedures and Postoperative Care4 Antenatal Care5 Maternal Medicine6 Management of Labour and Delivery7 Postpartum and Neonatal Problems8 Gynaecological Problems and Early Pregnancy Loss9 Subfertility10 Sexual and Reproductive Health11 Urogynaecology and Pelvic Floor Problems12 Gynaecological Oncology

Table 4List of e-tutorials in three example StratOG.net modules.
StratOG.net module E-tutorials in module
The Obstetrician and Gynaecologistas a Professional
AppraisalClinical governanceEthical and legal issuesMentoringReflective practice
Antenatal Care Principles of antenatal careFetal growth restrictionPre-eclampsiaGenetic disordersAlloimmune disorders of pregnancyDomestic abuse and drug and alcohol misuseMultiple pregnancyAntepartum haemorrhageAnomaly scanning in early pregnancy andcongenital malformationsAnomaly scanning in the second trimester
Urogynaecology and Pelvic Floor Problems Assessment of lower urinary tract functionUrinary tract infectionUrinary incontinenceUrogenital prolapse
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 737
B Images, figures, animations, graphs, scans, video and audio assets (Fig. 3)B A variety of assessments including true or false questions, multiple-choice questions (MCQs)
and extended matching questions (EMQs)� Discussion forums for learners to communicate and discuss specific topics� Case-based scenarios towards the end of the tutorials for trainees to apply their knowledge to real
situations.
The programme consists of approximately 100 tutorials that supplement trainees’ clinical training.Trainees can pick and choose some or all of the tutorials in any order depending on the way in whichtheir training placements are arranged. No tutorials are compulsory, in the same way that it is notcompulsory to read journals, or read specific textbooks published by the RCOG. However, the popu-larity of StratOG.net and the increasing number of UK deaneries purchasing StratOG.net for all theirtrainees suggests that StratOG.net is becoming an integral part of many trainees’ education.
StratOG.net is a self-directed learning programme and so self-assessments are for trainees’ own use.However, trainees have case-based discussion workplace-based assessments to assess knowledge, andtherefore StratOG.net tutorials provide a useful resource for learners to access and to assist withprogressing personal development plans set in the clinic with their supervisors following practicalexperiences.
Balanced learning, assessment and interaction
Tutorials include self-assessments, interactive, engaging exercises and stimulating animations,videos and audio clips. The balance of teaching and assessment has been very carefully consideredbecause it is recognised that interactivity alone is not sufficient for a valuable learning experience, andlearner engagement is necessary. Although an activist learning approach is required to maintainengagement, over-activity can lead to an overwhelming experience and a period of time for moreintense concentration and reflection is crucial in single learning session. Case-based learning is chal-lenging for authors to produce for an e-learning environment. However, the inclusion of such case-based material allows the application of knowledge gained by trainees as they work through thetutorial to clinical practice. Case-based exercises can also provide a useful assessment tool.
The RCOG editorial teams were keen to implement a small number of interactive tools in a cleverway rather than overwhelming learners with so many tools and functions that they lose the ability toconcentrate on any one learning object and become more interested in the technology. Moreover, too

Fig. 2. Introduction to e-tutorial with learning objectives and the tutorial structure.
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746738
many advanced e-tools increase the possibility of technical problems, which will distract and frustratethe learner and can completely ruin the learning experience.
How do we believe StratOG.net enhances learning?StratOG.net was designed to conform to educational theory. Ellington et al 3 described four domains
that were important in enhancing the learning experience:
� Wanting� Doing� Digesting� Feedback.

Fig. 3. Clearly annotated and simplified figures.
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 739
The first domaindwanting to learndis central to learning; if the learner has no motivation tolearn then limited learning will take place. A motivator for learning may be the need to pass anexamination or to meet CPD or recertification requirements. Learning is generally more effectivewhen it is active and engages the learner, and when the learner is given time to reflect on newconcepts. Opportunities for learners to apply knowledge gaineddfor example, to solve case studiesthat simulate real-life situationsdwill also enhance learning. Feedback is essential to the learner aspositive feedback and evidence of progress will encourage further learning. Negative feedbackdforexample, an explanation of why a learner’s answer to an assessment was incorrectdcan alsomotivate the learner to improve their performance.

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746740
StratOG.net has been designed to contribute to all of these domains with a view to providinga learning resource that meets the needs of trainees and improves their learning experience. Table 5indicates how we are trying to achieve this.
Feedback on StratOG.net
In 2009 a user survey indicated that 80% (n¼ 100) of respondents considered that StratOG.net hadhelped them in their clinical training, and 87% (n¼ 110) said it helped them in their learning. Positivecomments from users regarding StratOG.net included:
Table 5Domain
Doma
Want
Doing
Diges
Feedb
“A very quick source of obstetrical knowledge loaded with new articles and research work”“StratOG is a world class learning tool which genuinely puts the RCOG at the forefront ofe-training. It is faultless (except possibly the name, but at least it’s memorable!)”
The aspects of the site that were rated the highest (‘good’ or excellent’) by respondents were thelevel of content (83%, n¼ 100), presentation (80%, n¼ 97) and currentness of content (79%, n¼ 92)(Fig. 4).
Users were also asked what they would like to see a lot more of, some more of, the same and less:
� Users would like to see a lot more short essay questions (52%, n¼ 61)� Users would like to see some more explanatory diagrams (42%, n¼ 48), images (38%, n¼ 43) andcase studies (36%, n¼ 43)
� Users would like to see the same number of references (52%, n¼ 59) and text (34%, n¼ 40)
s of learning. Taken from Saunders et al 2010.15
in Why domain is significant Aspects of StratOG.net that contribute to the learning domain
ing Key domain; if learners do not want tolearn then limited learning will take place
� Programme was developed to assist preparationfor the MRCOG examination
� ‘Mirrors’ the RCOG curriculumPeople learn best when doing things, i.e.active rather than passive learning
� Animations simplify complex principles� Videos and scans enable visualisation of proceduresand anomalies to enhance understanding
� Hyperlinks to guidelines and reading materials toprovide background and additional informationabout the subject area
� Interactive reflective activities and opportunitiesto engage with other trainees to seek clarificationand discuss issues
� Assessment opportunities throughout tutorial toevaluate progress with understanding and meeting theobjectives of the tutorial
� Problem solving/case-based activities to applylearned knowledge to clinical situations
ting Learners need time to digest new ideas andto see how new learning fits inwith existing knowledge
� Facility to attach reflective notes and revisit thinkingaround topics and issues
� Facility, through discussion forum, to engage withother trainees and discuss issues
� Ability to complete e-tutorials at own paceand revisit material
ack Positive feedback encourages further learning.Guidance on how to improve performanceis crucial to learning
� Ability to monitor progress in completing tutorialsthrough the e-learning history
� Interactive assessment opportunities with instantfeedback and explanations of why answers arecorrect/incorrect
� Facility to save assessment scores and monitorimprovement and progress towards achievingthe tutorial outcomes
� Progress reports can be included in learner’sportfolio as evidence for annual review meetings

Fig. 4. Results from the StratOG.net user survey.
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 741
Following on from the survey, the StratOG.net Editorial Board and authors are undertakinga review all of the tutorials with the specific aim of adding new assessments and multimediaelements. The survey also illustrates the challenges facing the e-learning provider: the need to keepthe material up to date, to add sophisticated assessments (which are difficult for authors to write),and to add advanced multimedia (which can be very expensive). It is important to consider the cost ofthe e-learning product to the user, and the RCOG struggles to balance the cost of developing andmaintaining StratOG.net with the desire to keep the cost to the user as low as possible.
E-lectures
Some face-to-face courses are mandatory during training to allow opportunities for question andanswer sessions. However, with increasing time restrictions and limited study budgets, many manda-tory courses of several days’ duration will necessarily become shorter. Accordingly, using e-lecturesmeans that trainees can cover the basics of the course before attending and can then engage in themoreinteractive elements of courseswhen they physically attend. Following the course, further exercises andself-assessments can be made available online. This is deemed to be a more efficient and educationallysuperior approach to delivering education and e-lectures are the next step forward for the College.
In order to provide a blend of media to the learner and to maximise the engagement of the learner,the RCOG is also capturing e-lectures at the request of many learners, particularly internationally. Thiscaptures Fleming’s ‘VARK’ learning styles (see above) and the fact that many learners respond posi-tively to aural and auditory learning objects. Feedback suggests that the value of these lectures online isthat they can be accessed at convenient times and can be revisited. From a practical and logisticalperspective, international clinicians appreciate having access to these lectures without the need to visitthe RCOG to hear them. Additionally, many real-time face-to-face lectures are components ofa conference; engagement is minimal and learners become overwhelmedwith information that is verydifficult to absorb. Therefore, these lectures are ideally suited to be re-packaged in an online formatthat clinicians can access in their own time and can reflect on at leisure.
In 2010, a new series of e-lectures on the subject of abortion care has been introduced by the RCOG.These were introduced to deal with a sensitive area of clinical practice. Some trainees may havea conscientious objection to performing these procedures, or work with colleagues who have such anobjection. Despite having a conscientious objection, traineesmust still have knowledge about the subject

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746742
area in order to effectively referwomen to the service that they need, and the CD-based e-lecture series isa comprehensive, engaging and discreet resource for trainees and professionals of all levels to access.
The RCOG recognises that using audio learning content does not comply completely with the UKDisability Discrimination Act 16 and so all audio learning objects are transcribed to ensure full acces-sibility for learners with hearing problems.
Learning and assessment of cardiotocograph interpretation
Current literature and training resources allow trainees to visualise abnormal and pathologicalcardiotocograph (CTG) traces but there is no book or e-learning program available that can promptquestions at appropriate trigger points in a case-based learning session featuring a CTG trace. Severale-learning programmes have been developed, but the programmes have included separate learningand assessment domains. Books and journals present traces but lack the interactivity to test decisionmaking skills and so the RCOG is currently working with a UK NHS and Department of Healthcollaboration, e-Learning for Healthcare (eLfH), to develop a comprehensive resource which will teachand assess learners about CTG interpretation and monitoring. Structured multiple-choice assessmentswill indicate whether learners are correct, incorrect or not entirely correct, and detailed automaticfeedback provided is predicted to improve and enhance knowledge. The challenging nature of ques-tions in the interpretation of CTGs and appropriate management will provide the learners withvaluable and sustained knowledge that does not exist in current resources.
The e-learning resource will educate users using assessment-driven, case-based learning. An inter-active learning session will test knowledge of CTG interpretation and clinical management, and willindicate outcomes. To successfully complete assessments, learners will need to provide the optimalanswers that would rationalise best management. It is proven that e-learning can teach and assess ina way that creates true to life cases and situations 7 and state of the art simulated trace presentation onscreenwill appear in away that the real traces do on CTGmachines. To succeed andminimisemistakes,learners need time to evaluate, interpret and reflect in education of this analytical nature. Based oninterpretations and actions, positive and negative outcomes will result so that learners can see theresults of their actions. Where incorrect interpretations and management plans are used, the learnerwouldbe informedof the real-life impact,which could indicate the life threateningdamage toababyandthe litigation consequences for the doctor.
The RCOG currently has a short e-learning tutorial in StratOG.net that introduces fetal monitoring.However, in accepting that repetition drives deeper learning, the RCOGand eLfHwill initially launch 100online case scenarios. Trainees, and indeed fully-qualified professionals (midwives and consultants),will be able to periodically assess themselves and to apply their knowledge in the same way that theywould in real-life situations. The RCOG intends to add 100 cases every five years in order to mirror thefive-year CPD and recertification cycle, thereby requiring obstetricians to follow this mandatory pro-gramme throughout their career. Evidence of achievement can be used for recertification of specialistsby the RCOG and then revalidation by the GMC.
A clinician’s assessment history would be recorded within the system and assessment summariescould be generated so that supervisors and assessors could monitor a clinician’s progress andachievement in a structured way.
E-learning to support practical skills courses
The reduced working hours for training as a result of the EWTR and MMC changes previously dis-cussed reduce the opportunities available to a trainee to gain competence and confidence in practicalprocedures in obstetrics and gynaecology under supervision.With this reduced exposure, trainees find itdifficult to grasp the finer techniques and to gain the expertise that is required for them to be confident inperforming practical procedures. In addition, it is recognised that in obstetrics, trainees spend three tofour times more time carrying out a procedure for the first few times, which impacts on patient care.17
Educational resources including small lectures and demonstration videos that the RCOG plans tomake available and deliver online will provide opportunities for trainees to gain initial understanding

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 743
of the procedures. This early experience can be further enhanced by practice on mannequins whilstreferring to videos and animations under supervision. Ideally, learners should acquire competencies ina simulated situation (see chapters 5 and 6), having accessed e-learning to gain familiarity and visualiseprocedures, before embarking on performing procedures on patients.
Obstetric drills simulate an emergency situation where all members involved should communicateandwork as a team; eachmember has a crucial role to provide a different skill. Knowledge of teamworkand dynamics, which are essential to properly manage these problematic situations, can be taught byvideo demonstration. The teamworkdynamics can be difficult to explain in the actual clinical setting, sodetailed analysis of videowithin an e-learning session can be very useful for a trainee to ensure that theycan act in the most efficient manner when in a real-life situation. While not replacing the need for livedrills, this approach could again act as an introductory element to training.
DIALOG successfully used a case-based approach to teaching and learning. Using this approach andgiving learners more time to evaluate, interpret and reflect on cases and clinical actions with anopportunity to see the consequences based on interpretations and actions in a simulated onlineenvironment would be expected to have positive benefits in terms of future clinical practice. Thisapproach would also be potentially valuable for rarer clinical conditions to which trainees may havedifficulty in gaining exposure in real-life.
Proposed formats for the development of this work include:
� Video of real-life situations� Video of simulated situations� Animations/enhanced graphics� Assessment tools (technical competency, management, communication)� E-learning to prepare trainees before practical skills courses or real clinics� Examples of good practice, satisfactory practice and unsatisfactory practice� Examples of misdiagnosis� ‘Layered’ approach to learning using simulated scenarios on video
B Basics (technical skills)B Add communication and multidisciplinary functions.
This blend of media and approaches would be expected to improve trainee competence and thenconfidence.
In linewith an emerging simulation strategy for the RCOG, simulation should be accessed regularly inorder to develop and refine skills, and regular access to e-learning will fit into this package. The doctor ormidwife will be able to view the e-learning sessions at their convenience and will be able to learn byvisualisation before they start to practise onmannequins and thenperformprocedures under supervisionon patients. Teaching materials will be standardised and will be delivered across geographical regions.
Supporting trainers
The availability of learning content can be maximised by re-packaging the content in order toprovide teaching resources for trainers. An RCOG project in 2010 is to re-purpose key content fromStratOG.net so that trainers who have a responsibility for training trainees in regional training days canhave access to standardised resources for these sessions and will not have to produce their ownresources. The aspiration is that pre-prepared teaching content will enable supervisors to deliversuperior training and to offer more personalised educational sessions as their resources have alreadybeen developed and are available online at any point where a trainee needs support.
Connecting trainees
Forums and constructivist learning
A chat room and discussion board existed in the first edition of StratOG and aimed to encouragelearners to communicate bothpractical issues and todiscuss subjectswithin the programme.Discussion

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746744
forums exist in e-learning to facilitate constructivist learning and to allow trainees to build theirknowledge together.
“learners actively construct their own knowledge and meaning from their experiences”..2
It was hoped that this would be of use and value for trainees to apply knowledge to rarer cases butexperience showed that the forums were not used because they were very general. The RCOG neededdiscussion forums to function to enable discussions to evolve without the need for a supervisor.Consequently, many discussion forums were introduced to StratOG.net and a statement, discussion topicor article to critique were added to each forum. It was thought that supervisor contributions would beuseful, but not essential, and that peer interaction would facilitate learning via personal experience.
A reviewof discussion forums in 2009 showed that discussion forums are not themost popular featureof StratOG.net and it was concluded that ever-changing, discussion forums with hot topics and currentissues, available for a defined period of timemight bemore popular amongst trainees. In order to engagewith trainees, discussion forumswould needmonitoring byand input from senior trainees or consultants.
ePortfolios
Since Modernising Medical Careers (MMC),9 a UK NHS and Department of Health initiative, medicaltrainees have become far more connected with colleagues, both locally and nationally. Technology hasplayed a major part in this connection and trainees are now able to share knowledge and tocommunicate remotely far more than before.
Trainees often comment on the ‘Big Brother’ style that medical training could becomewith regard totechnology being used to monitor training and document submission to ePortfolios. At the same time,however, trainees comment on how supervision and effective feedback can be difficult to arrange.Consequently, trainees are increasingly using the peer-to-peer communication tools available throughtheir ePortofolios since feedback can still be effective if given a short time after the event usinge-communications. The aim is to avoid the loneliness associated with training for trainees in smallunits, where e-mentoring can be achieved by becoming a part of an online network of trainees.
Quote: “If I log on to a social networking website, I get messages telling me what people havebeen doing and what events are running that I could be interested in. .I work in a small unitwith very senior trainees but communicate online with more junior colleagues who I learn a lotfrom . it’s really useful as I feel I miss out on a lot and don’t know whether my difficulties areexperienced by others until we chat online.”. a third year obstetrics and gynaecology trainee.11
The RCOG now provides all new trainees with an ePortfolio which enables more practical, portablerecording of clinical skill development. The electronic format also improves the process for quicklylocating and accessing information within the curriculum or logbooks. In addition, the ePortfolioprovides opportunities for trainees to reflect on their learning experiences and identify future learningneeds by hyperlinking workplace-based assessments, reflective writing entries, logs of clinical expe-riences and StratOG.net learning history records. Trainees can consider personal development plan-ning to be a chore but regular access to an ePortfolio, even more so with mobile technology, canfacilitate the easy organisation that postgraduate trainees require.
Evaluation of e-learning and the future
All publications at the RCOG have an editorial board of clinicians and editors overseeing theauthoring and editorial work. The editorial role for online content requires regular updates andlearners continually suggest improvements relating to the interactivity and use of multimedia.
In face-to-face education, a lecturer can sense boredom or confusion from body language or fromimmediate feedback, but in e-learning this is not possible. From a quality assurance point of view,e-learning instructional designers and editors are eager to receive feedback regularly to find out howthe content is perceived, whether the design is successfully delivering a quality educational experienceand whether the e-learning experience is enjoyable.

O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746 745
How to evaluate each component?
The features that are evaluated are:
� The programme structure� The content� The design
The course structure and content of e-learning will normally match the obstetrics and gynaecologycurriculum and when the curriculum or guidelines change, the content is amended to reflect this sothat as new standards, practices or techniques are introduced, the e-learning content is updated toreflect this. The content needs to be evaluated by the trainees and supervisors who give their opinionsof whether it correctly matches the curriculum and guidelines and covers the correct level of detail,and whether the design of the learning experience is stimulating, motivating and engaging.
The real incentive to continue to develop e-learning is that is allows trainees to manage their ownlearning and to take control of learning content in a way that suits them. The learner sets the pace andchooses the most appropriate media and customises their own personal learning objectives. The futureof specialty training and education leans towards workplace-based assessment and the drive is toensure that the curriculum is supported with a blend of resources which include carefully designedpackages of e-learning, face-to-face learning sessions, conventional book and journal-based resourcesand workplace-based assessment.
The key to trainees’ success in the days of the EWTR are to ensure bite-sized knowledge developmentopportunities are available and that repeated, regular practical skills sessions are also available. However,the way in which an institution evolves and develops its education is a high-risk process if it is to meetthe requirements of its learners. To replace books with e-books, traditional face-to-face study sessionswith videoconferences, practical demonstrations and conferences with video and animation andconversationwith discussion forums is neither desirable nor feasible. An over-reliance upon e-learning ispossible and many Fellows, Members and trainees can be severely disadvantaged if technical abilityprevents them from being able to access learning content. Similarly, the RCOG has a very internationalaudience and although e-learning solutions are developed to not require powerful internet connections,a complete lack of internet access is obviously problematic. To this end, the RCOG will not ever move alleducational support to the online environment, not just because of practical reasons, but to appreciatethe value of other learning resources and the preferences that our learners have.
The RCOG’s goal is to use technology to complement and integrate with other approaches toteaching and learning to maximise the advantages of all approaches and to provide an appropriatepackage of learning opportunities. In a modern day health service with many challenges, the RCOGwillbe rising to the challenges to ensure that its e-learning experiences are innovative, stimulating andenjoyable and that they successfully produce the skilled practitioners that the profession requires.
Practice points
� An e-learning experience will be most successful if it is easily accessible, intuitive, memo-rable, enjoyable, affordable
� A standardised learning design with clear learning objectives and ‘bite-sized’ learningsessions will be effective for learners.
� Based on VARK’s model, learning can be visual (V) (graphics, animations, charts), aural/auditory (A), read/write (R) (reading and reflective writing), kinesthetic (K), (video clips,simulation, case studies)
� A robust quality assurance structure must be in place to ensure that editorial, production andtechnical standards are adhered to so that the overall e-learning session is of a high standardand continually reviewed and updated.

Research agenda
� The effect of e-learning on examination performance� The effect of animation and video-based e-learning on trainees’ ability to master practicalskills
� The effect of case-based learning and video-based e-learning on trainees’ ability to managescenarios and master the communication and leadership skills required of a modern-daypractitioner.
O. Jones et al. / Best Practice & Research Clinical Obstetrics and Gynaecology 24 (2010) 731–746746
References
1. a Department of Health. European working time directive. London: Department of Health, 2004;b Department of Health. European working time regulation. London: Department of Health, 2009.
2. Doolittle PE & CampWG. Constructivism: the career and technical education perspective. Journal of Vocational and TechnicalEducation 1999; 16(1) [Online version].
3. Ellington H, Percival F & Race P (eds.). Handbook of educational technology. 3rd ed. London: Kogan Page, 1993.4. Fleming. Teaching and learning styles: VARK strategies. New Zealand: Fleming, 1987.5. GMC. Good medical practice. UK: General Medical Council, 2004.6. Honey P & Mumford A. ‘The manual of learning styles’, available direct from Dr Peter Honey, 10 Linden Avenue, Maidenhead,
Berks. Quoted by: Rowntree D (2005) ‘block 1 overview essay’ Knowing our learners in ODL’, implementing open and distancelearning. Milton Keynes: The Open University, 1986. p.15.
7. Kolodner J. Case-based learning: machine learning 1993; vol. 10. Netherlands: Kluwer Academic Publichers, 1993. pp .195–199.
8. Lockwood F (ed.). Materials production in open and distance learning. London: Paul Chapman, 1994. pp. 35–46.9. Modernising medical careers. UK National Health Service, 2007.
10. RCOG. The future role of the consultant. London: RCOG, 2005.11. RCOG ePortfolio User Group. 2008.12. RCOG. Basic specialty training working party report. London: RCOG, 2005.13. Rowntree D. Preparing materials for open, distance and flexible learning. London: Kogan Page, 2007. p.35.14. Ruiz JG, Mintzer MJ & Leipzig RM. The impact of e-learning in medical education. Academic Medicine March 2006; 81(Issue
3): 207–212. IT in Medical Education.15. Saunders H, Hundal K, Mires G. StratOG.net: the RCOG’s online learning resource to support curriculum delivery and
postgraduate training. The Obstetrician & Gynaecologist; 2010;12 (in press).16. UK Disability Discrimination Act. 1995.17. Williams JC. A data based method for assessing and reducing human error to improve operational performance. Proceedings
of IEEE Fourth Conference on Human Factors in Power Plants; 5-9 June: Monterey, CA. 1988 pp. 436–450.