The Deadly Hoover: A curiouser and curiouser case of
28
Providence St. Joseph Health Providence St. Joseph Health Providence St. Joseph Health Digital Commons Providence St. Joseph Health Digital Commons Providence Portland Medical Center Internal Medicine 2021 Providence Portland Medical Center Internal Medicine 5-2021 The Deadly Hoover: A curiouser and curiouser case of The Deadly Hoover: A curiouser and curiouser case of disappearing platelets disappearing platelets Rachael Starcher Follow this and additional works at: https://digitalcommons.psjhealth.org/oaa_ppmc_21 Part of the Internal Medicine Commons
The Deadly Hoover: A curiouser and curiouser case of
The Deadly HooverA c urious e r and c urious e r c a s e of d is appea ring pla te le ts
Rac hae l W. Sta rc he r, MD MA
Presenter
Presentation Notes
Hello, as mentioned, I’m Rachael Starcher and I’m here to tell you about [Next] The Deadly Hoover: a curioser and curioser case of disappearing platelets. So [Next] hold onto your hats and join me down the rabbit hole of this case…
Case Presentation
History of Present Illness• 42 yo Male• Symptoms x4 days PTA:
• SOB with produc tive c ough• Mouth pa in• Epis taxis
Medical & Social History• Tobac c o us e (10 pac k- yea rs )• Methamphe tamine (inha la tiona l)• Works on an apple orc ha rd• Expos ed to c hic kens & dog• Sprays pes tic ides• Denies woodworking, me ta l
working• Lives in rura l, north- c entra l
Oregon with no trave l
Presenter
Presentation Notes
I saw a 42 yo male with 4 days of shortness of breath accompanied by a productive cough, mouth pain, and nose bleeding. His medical history was significant for tobacco and inhalational meth use. He worked on an apple orchard with exposures to chickens, dogs, and pesticides, but denied woodworking, metalworking, and travel.
Case Presentation
Physical Exam• HEENT: poor dentition,
g ingiva l b leeding, dried blood nea r mouth and nos e
• Lungs : c rac kle s in the bas es b ila te ra lly
• Lymph: pa lpable , non-tende r, mobile axilla ry and inguina l nodes b ila te ra lly
Presenter
Presentation Notes
On exam, he had evidence of prior bleeding in his mouth and nose, bilateral lung crackles and non-tender axillary and inguinal lymphadenopathy. These photos show the skin of his feet– his hands appeared similar.
Presenter
Presentation Notes
Imaging demonstrated bilateral ground glass opacities and lymphadenopathy with no PE.
Case Presentation
Initial Vitals & Labs36.8º C, 104/ 64, HR 97, RR 16, 86% on RA - > 93% on 3L NC
MCV: 93.6
Eos inophils : 3.9 [ 0.0 – 0.5 109/ L] Proc a lc itonin: 0.76
11.9
2
32.8
14.8*
*
*
* 1.28(Bas e line 0.9)
22*
AST 132
152
400
ALT
Alk Phos
Presenter
Presentation Notes
On admission, he was tachycardic and hypoxic. [Next] He had a mild anemia, leukocytosis from eosinophilia, mild renal insufficiency, acute hepatitis, and [Next] MARKED thrombocytopenia with only 2,000 platelets.
Summary
Problem list• Thromboc ytopenia (s eve re )
• Spontaneous epis taxis
• Hypoxic re s pira tory fa ilure (mild)• Pneumonitis • Bila te ra l ground gla s s opac itie s
• Eos inophilia (modera te )
• Normoc ytic anemia (mild)• Hepa titis (mild)• AKI (mild)• Exfolia tive de rma titis (mild)• Tac hyc a rdia (mild)• Lymphadenopa thy
• Axilla ry• Inguina l
Presenter
Presentation Notes
In summary, this is a 42 yo male with tobacco, meth use, and multiple environmental exposures who presented with dyspnea and epistaxis, found to have severe thrombocytopenia and multiorgan dysfunction. Here I found myself at a crossroads, wrestling with whether there are multiple things going on OR if there is one unifying diagnosis?
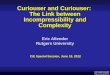
“Would you te ll me , p leas e , whic h way I ought to go from he re?”
“Tha t depends a good dea l on where you want to ge t to ,” s a id the Ca t.
-Alice and the Cheshire CatAlice’s Adventures in Wonderland (Lewis Carroll)
Presenter
Presentation Notes
I found inspiration in this exchange between Alice and the Cheshire Cat where Alice asks, “‘Would you tell me, please, which way I ought to go from here?’”… ‘That depends a good deal on where you want to get to,’ said the Cat.” Because his thrombocytopenia was inarguably the most critical life-threatening issue, I directed my focus on those missing platelets…
Thrombocytopenia
Decreased Production• Bone marrow
• Failure• Suppre s s ion• Infiltra tion
• Myelodys pla s tic s yndrome• B12 and fo la te de fic ienc y
Increased Consumption• DIC/ Seps is• Drug reac tion• HIT• Allo immune des truc tion (pos t-
trans fus ion or pos t- trans planta tion)
• Autoimmune d is eas e• Primary ITP• Mec hanic a l des truc tion• TTP/ HUS
Sequestration• Infec tions :
• Vira l• Ric ke tts ia l• Paras itic
• Splenomega ly• PE• Pulmonary HTN
Multifactorial
Presenter
Presentation Notes
Based upon history and work up to this point, we eliminated quite a few etiologies on the front end [1next]. Through additional work up, splenic sequestration [2next], DIC, [3next], and infection [4next] were quickly ruled out. We were then left with primary hematologic versus immune-mediated processes.
• Periphe ra l s mea r• Flow c ytome try• Myeloid and MDS gene pane l• Malignant eos inophilia FISH
pane l
Hematologic Work-Up
Next steps
Presenter
Presentation Notes
We first checked a peripheral smear which showed eosinophilia but no evidence of blasts, dysplasia, or schistocytes. His [1Next] flow cytometry, myeloid panel, and eosinophilic FISH analysis were all normal. [2Next] So, what now?... On down the rabbit hole we go… https://www.researchgate.net/figure/The-peripheral-blood-smear-showed-eosinophilic-leukocytosis-microcytic-hypochromic_fig1_49840804
Thrombocytopenia
Decreased Production• Bone marrow
• Failure• Suppre s s ion• Infiltra tion
• Myelodys pla s tic s yndrome• B12 and fo la te de fic ienc y
Increased Consumption• DIC/ Seps is• Drug reac tion• HIT• Allo immune des truc tion (pos t-
trans fus ion or pos t- trans planta tion)
• Autoimmune d is eas e• Primary ITP• Mec hanic a l des truc tion• TTP/ HUS
Sequestration• Infec tions :
• Vira l• Ric ke tts ia l• Paras itic
• Splenomega ly• PE• Pulmonary HTN
Multifactorial
Presenter
Presentation Notes
With hematologic causes ruled out, we were left with immune-mediated processes… Without meeting specific diagnostic criteria, autoimmune diseases were deemed unlikely [1next], leaving us with primary (idiopathic) thrombocytopenia, or ITP – a diagnosis of exclusion. But we couldn’t help wonder… were we right? Sarcoid = upper lung predominance SLE = no significant renal findings, bland UA, atypical skin findings Antiphospholipid syndrome = no thrombosis
Primary (Idiopathic) ITP
Epidemiology• Bimoda l d is tribution (0- 14 and >60 years )
• More c ommon in fema les
0
1
2
3
4
5
6
0- 14 15- 39 40- 59 >60Inci
denc
e (p
er 1
00,0
00 p
er y
ear)
Age
Inc idenc e of Primary ITP by Age and Gende r
Female Male
Clinical manifestations• Pla te le ts wors en with trans fus ion• Is ola ted thromboc ytopenia• Pa tients a s ymptomatic• Improves with s te roids , IVIG
Diffe rs from s ec onda ry ITP c aus ed by:Malignanc y, autoimmune dis eas e s ,
drugs / toxins
Presenter
Presentation Notes
ITP is autoimmune-mediated platelet destruction with no secondary cause. [1next] It has a bimodal age distribution and female predominance. [2next] Classically, platelets worsen after transfusion, no other CBC abnormalities coexist, patients are asymptomatic, and platelets improve with steroids and IVIG. Our patient, [3next] fell into the LEAST likely demographic with only SOME clinical signs -- this hat just didn’t seem to fit.
“I c an’t go bac k to ye s te rday, bec aus e I was a d iffe rent pe rs on then.”
-AliceAlice’s Adventures in Wonderland (Lewis Carroll)
Presenter
Presentation Notes
With the case evolving before our eyes, we were reminded of Alice’s realization quoted here: “I can’t go back to yesterday, because I was a different person then.”… As her adventure inevitably changed her, our patient’s admission transformed him as well.
Complications Arise
Hospital Day 4• Intrapa renc hymal, s uba rac hnoid ,
and intraventric ula r hemorrhage• 1.1 c m midline s hift
• Pla te le ts <4 (109/ L)• Rec e ived 8 units pre - and
intraope ra tive ly
Presenter
Presentation Notes
On his 4th hospital day, he developed an acute hemorrhagic stroke with aphasia.
Platelet Trend
200
10050
0
Hospital Day
Pla
tele
ts (1
09 /L)
NORMAL
• 1.5% of pa tients with <10k pla te le ts
• Urgenc y of trans fus ion and trea tment
NORMAL
Severe spontaneous hemorrhage
Presenter
Presentation Notes
Complications like this occur about 1.5% of the time platelets are less than 10, explaining the urgency for appropriate treatment. Our patient’s early undetectable platelets [1next] initially responded to standard ITP therapy, but drifted back down prompting a [2next] dose of ROE-mip-low-stem (a colony stimulating factor) that only helped for a week. His refractory thrombocytopenia seemed atypical, but we weren’t sure what else to do…
Breakthrough!
“You s hould c hec k for merc ury
pois oning…”
Presenter
Presentation Notes
That was when we had a curious breakthrough! [1next] Family called saying we “should check for mercury poisoning.” They then hung up and could no longer be reached.
“Why, s ome times I've be lieved a s many as s ix impos s ible things be fore breakfas t.”-AliceAlice’s Adventures in Wonderland, Lewis Carroll
Presenter
Presentation Notes
Mercury poisoning seemed like an entirely IMpossible explanation for the missing platelets, but as Alice points out: “Why, sometimes I’ve believed as many as six IMpossible things before breakfast.” … We didn’t have 6 impossibilities to believe, just one! But it felt as if this phone call RAISED more questions than it seemed to answer. We decided to follow this white rabbit with the clues we could gather.
Mercury Poisoning – The History
Minamata(s ta rring and produc ed by
Johnny Depp) –doc udrama to
be re leas ed
Firs t des c rip tion of inha la tiona l
merc ury pois oning
Merc ury touted a s c ure for
feve rs
Minamata Bay, Japan: merc ury in s ea food
identified a s c aus e of mas s dea th and
d is ability
Minamata Convention - 128 c ountrie s
p ledge to reduc e merc ury pollution by
banning c e rta in produc ts by 2020
Presenter
Presentation Notes
First, we went to the history books, assuming that mercury poisoning is a disease of the past. [next] We found that it used to have clinical utility before discovering [next] that felt hat makers inhaling mercury developed what is dubbed “mad hatter’s disease.” While Disney [next] animated the Mad Hatter, Minamata Bay, Japan learned that mercury-rich seafood could be fatal. More recently, [next] Johnny Depp turned the Mad Hatter introspectively while world leaders at the Minamata Convention focused outwardly on curbing mercury pollution. [next] Finally, Johnny Depp returns us to Minamata for a docudrama on the famous bay-- which you’ll hopefully be able to catch in theaters nationwide next year! But with all this attention on mercury for 2 centuries, what’s the state of mercury toxicity today?
Mercury Poisoning
Background• Mos t toxic non- radioac tive me ta l in
the world• Found in the environment• Main s ourc e s of expos ure :
• Eating c ontamina te d s e a food• Outgas s ing of de nta l ama lgam• Oc c upa tiona l
• Artis ana l gold mining• Manufac turing
• 3 forms :• Meta llic / e lementa l• Inorganic• Organic (does not re s pond to c he la tion)
Na tura l (e .g . volcanic ,
geothermal)
Pollutant (e .g. fos s il
fue l extrac tion,
a rtis ana l gold
Remobiliza tion (e .g. wildfires ,
b iomass burning)
Environmenta l Sources
Presenter
Presentation Notes
Mercury is the most toxic non-radioactive metal in the world. It [1next] occurs naturally with the most common sources shown on this pie chart. With regards to human exposures, [2next] most are from seafood, dental amalgams, and occupational exposures. [3next] Mercury has 3 different forms—all of which are toxic. Organic mercury from seafood is unique in that it cannot be chelated. With that in mind, we wondered how mercury poisoning could explain our patient’s presentation?
Mercury Poisoning
Routes of Exposure• Inges tion
• Inte s tina l ne c ros is• He morrhagic gas troe nte ritis• ATN or ne phrotic s yndrome• Ere this m – “mad ha tte r d is e as e”
• Trans de rmal• Hype rs e ns itivity re ac tions
• Erythema• Exfolia tive de rma titis
• Inha la tiona l• Rapid uptake , ac ute s ymptoms• Mos t dange rous e xpos ure route• Ac ute pne umonitis• Ere this m – “mad ha tte r d is e as e”
Hg
shyness,memory loss,
insomnia, excitability, mood changes,
delirium
Presenter
Presentation Notes
The 3 possible exposure routes differ clinically. [1next] Ingestion is the most common, but its predominant GI symptoms were not seen in our patient. [2next] Transdermal exposure provokes localized dermatitis. [3next] With nearly 100% of INHALED mercury rapidly absorbed, this dangerous route causes acute pneumonitis, systemic symptoms, and EAR-a-thism, or mad hatter’s disease, [4next] a neuropsychiatric syndrome of behavioral changes seen here. So, armed with the assumption that our patient had transdermal and inhalational exposure, we were nearing the end of our adventure only to have our original question unanswered – where did the platelets go?? Could mercury be our culprit?
Where did the platelets go?
Thrombocytopenia & Mercury• Hematologic abnorma litie s
pre s ent in 24% of c a s e of merc ury pois oning
• Thromboc ytopenia is a ra re manife s ta tion of merc ury pois oning
• Reported in only 0.23% of c as e s• Has a ve ry high morta lity ra te
Died from hemorrhage
76%
Survived24%
Thrombocytopenia Outcomes
Presenter
Presentation Notes
24% of patients with mercury exposure have hematologic abnormalities. Only A QUARTER OF A PERCENT have thrombocytopenia, but, when present, have the worst outcomes due to hemorrhage. I couldn’t help but wonder why this rare but dangerous abnormality develops. Cases: Bonhomme (1996) Alexander (1971) McNeil (1984) Hryhorczuk (2006) Zelman (1991) Fuortes (1995) Sexton (1978) Florentine (1991) Crysochoou (2003) Schwartz (1992) Solis (2000) Yildirim (2012)
Where did the platelets go?
Toxin-Induced ITP• Many drugs have been implic a ted• Studie s c ompare e ffec ts of me rc ury
to the rapeutic gold• Both a lte r s urfac e g lyc oprote ins on
p la te le ts• Pres ented as antigens in Clas s II HLA
immune re s pons e• Leads to anti- p la te le t immunoglobulin
produc tion & pla te le t de s truc tion
• Merc ury- induc ed ITP re s ponds to c he la tion
• Gold leads to c hronic ITP
Abc iximabAc ec lofenacAc e taminophenAlemtuzumabAmiodaroneAztreonamBeta - lac tam antib io tic sBis oprolo lCarbamazepineDaptomyc inDexame thas oneEptifiba tideEthambutolEthos uximideExena tideFe lbamateFuros emideGoldHalope ridolIbuprofenIVIGIrinotec anLeuc ovorinLe fofloxac in
Pla te le t
Presenter
Presentation Notes
Mercury-induced thrombocytopenia is similar to toxin-induced ITP. [1next] Many medications have been implicated. Mercury-- like the more widely studied gold-- alters [2next] platelet surface glycoproteins. The altered protein [3next] is then presented as an antigen through Class II HLA immune mechanisms. Through T-helper cells and [4next] anti-platelet immunoglobulin production, platelets are targeted for immune attacks. [5next] Unlike gold, mercury induced ITP resolves with chelation.
Rodent Autoimmunity
Rodent models• Mic e exhibit autoimmune type
s yndrome when expos ed to merc ury
• Inc ludes dos e - dependent IgM, IgG, and IgE produc tion
• Induc es ec topic lymphoid tis s ue• Frequently us ed a s an anima l
mode l for autoimmune dis eas e
• Relie s on c e rta in gene tic s us c eptib ility
Mous e lung with lymphoid tis sue a fte r mercury exposure
Normal mous e lung
Presenter
Presentation Notes
Mice exposed to mercury can develop an autoimmune type syndrome. You can see here a normal mouse lung on top compared to a mouse lung on the bottom exposed to mercury vapor. The dark purple lymphoid tissue produces immunoglobulins directly in the lung. These mice also exhibit immune complex deposition in the kidneys and positive ANAs [1next] which is why mercury is frequently used as a mouse model for lupus. However, only certain mouse strains are susceptible to this reaction. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5831116/
Suspected genetic susceptibility
Gene tic s us c eptib ility
Autoimmune reac tion IgE Eosinophilia
Lymphadenopathy
Thrombocytopenia
Presenter
Presentation Notes
For my patient, I supposed that: if mercury is culprit, [1next] then he was likely genetically susceptible to produce an [2next] autoimmune-type reaction, which led to [3next] increased lymphoid tissue causing lymphadenopathy, [4next] increased immunoglobulins leading to eosinophilia, [5next] and direct platelet toxicity through antigen presentation. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5831116/
Mercury poisoning…?
Do we chelate?• Aphas ia (from s troke ) prevented
pa tient his tory• Family and friends not
re s ponding to c ontac t• Sus pec ted inha la tiona l and
de rma l expos ure• Elementa l me rc ury mos t like ly• Res ponds to c he la tion
Normal 10 Normal 5
Pa tient > 160
Pa tient > 80
0
20
40
60
80
100
120
140
160
Serum Mercury Urinary Mercury
Mer
cury
Con
cent
ratio
n (u
g/L)
Pa tient Se rum & Urinary Mercury Leve ls Compared to Normal Ranges
Presenter
Presentation Notes
With a better understanding of mercury poisoning, we found our patient’s [1next] mercury levels to be off the charts! Even though he couldn’t speak and family was unreachable, we had sufficient evidence to presume [2next] he had inhalational and dermal exposure, which-- unlike ingested mercury-- SHOULD respond to chelation.
Case Conclusion
Effects of chelation• 30 days of c he la tion the rapy
• Menta l s ta tus improved• Pla te le ts normalized
• No evidenc e of c hronic ITP
The rest of the story…• Illega lly purifying mined gold with
merc ury• Spilled merc ury and tried to
c lean it up • Cove ring his hands d irec tly
• Vac uumed the s pill from the c a rpe t
• 12 c as e reports• Inha la tiona l pois oning
Presenter
Presentation Notes
So, what happened? [1next] He completed chelation and showed both mental status improvement (which apparently was not all attributable to his stroke!) and normalized platelets... [2next] We DID eventually find out the story… He had been illegally purifying gold with mercury when it spilled, exposing his skin directly. [3next] He vacuumed it, vaporizing mercury through agitation – something described in a dozen case reports as one of the most dangerous routes of exposure. So, as we start wrapping up, I’m sure you’re wondering how this will ever relate to your clinical practice...
Mercury rising
Impact of Climate Change• Environmenta l merc ury
trip led ove r la s t 150 yea rs• Warmer wa te r tempera ture s
inc reas e merc ury c onc entra tions in edible fis h
• Fores t fire s re lea s e merc ury previous ly s a fe ly s tored in p lant life
• Oregon 2020 fire s re le as ed 8x normal yea rly pollution
• Es tima te 28% inc reas e in wildfire emis s ions by 2050
Presenter
Presentation Notes
The answer is “climate change.” Over the past 150 years, environmental Hg has tripled due to pollution. [1next] With warmer water temperatures, fish more readily absorb mercury. [2next] Additionally, forest fires are the second largest source of mercury pollution in the U.S. due to the release of mercury safely harbored in plants. [3next] It’s estimated that Oregon’s 2020 fires released more than 8 times typical annual mercury pollution. [4next] With current trajectories, experts estimate a 28% increase in wildfire-associated mercury emissions over the next 30 years. Environmental chemists worry that this could be the next Minamata, right here in the Pacific Northwest.
Take Home Points
• Merc ury pois oning is ra re .• Mos t people think of “mad ha tte r’s d is eas e”
• Toxin- as s oc ia ted ITP is exc eedingly ra re (0.23% inc idenc e ) but highly fa ta l.
• Res ponds to ITP the rapy and merc ury c he la tion• Does not le ad to c hronic ITP
• Des pite improvements in c ontrolling merc ury re lea s e , it is on the ris e .• Driven in pa rt by c lima te c hange
• Emphas izes importanc e of deve loping pa tient trus t for hobby his tory• Sec re t and illega l hobbie s c ould be the key when c linic a l p ic ture does n’t s eem to fit
Extens ive lis t of re fe renc es ava ilable upon reques t
Presenter
Presentation Notes
So, to conclude, mercury poisoning is rare and the neuropsychiatric “mad hatter’s disease” is the most common manifestation. [1next] The highly fatal mercury-associated ITP is exceedingly rare, but fortunately, responds to chelation. [2next] Despite efforts to decrease mercury’s harmful effects, climate change is raising the mercury levels in our fish and environment. [3next] Finally, when the clinical picture just doesn’t seem to fit, don’t discount the importance of patient trust in revealing secret hobbies which could include possible exposures, because, who knows? What seems impossible today could be just one of six impossible things before breakfast tomorrow. At this time, I am happy to take any questions you might have.