Embed Size (px)
Citation preview

EVIDENCE-BASED CHILD HEALTH: A COCHRANE REVIEW JOURNALEvid.-Based Child Health 5: 3–10 (2010)Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ebch.482
The Cochrane Neonatal Review Group: who we areand what we have doneRoger F. Soll*Department of Pediatrics, University of Vermont, Burlington, VT, USA
Evidence-based medicine (EBM) is the integrationof clinical expertise, patient values and the bestavailable evidence into the decision making processfor patient care (1). The practice of EBM requiresthe synthesis of up-to-date, valid evidence concerningthe efficacy and safety of treatments and timelydissemination of that evidence to practitioners (2,3).In the field of Neonatal-Perinatal Medicine, this isa daunting task. A quick ‘search’ of Medline usingPubMed (using the key word ‘newborn’ and limitingthe search to ‘randomized controlled trials’ and ‘allinfant’) produces over 7000 citations of randomized,controlled trials that have been published in thefield of neonatology. Over 600 have been publishedin the previous two years. Practicing pediatriciansand neonatologists, policy makers and families ofpatients cannot readily keep up with this large bodyof evidence. Resources that allow all these involvedparties to quickly access high order evidence to answerpressing clinical questions are essential in order tocreate evidence-based practices and guidelines.
The Cochrane Neonatal Review Group (CNRG) isone of over 50 collaborative review groups registeredin the Cochrane Collaboration. The specific goal ofthe Cochrane Neonatal Review Group is to prepare anddisseminate evidence-based, regularly updated system-atic reviews on the effects of therapies in Neonatal-Perinatal Medicine (4). The CNRG includes an edi-torial group based in the United States and Canada,regional coordinating editors in the United Kingdomand Australia, and over 70 review authors world-wide. The CNRG receives funding from the AmericanNational Institute of Child Health and Human Devel-opment. These funds support the infrastructure of theNeonatal Review Group and allow for the preparationand updating of systematic overviews of randomizedtrials in the field of Neonatal-Perinatal Medicine.
Reviews produced by Cochrane Review Groupshave a precise ‘systematic’ methodology that distin-guishes these reviews from non-systematic reviews.This ‘systematic’ review methodology is designed toproduce unbiased and precise estimates for the effectsof treatment on outcomes of clinical importance along
*Correspondence to: Roger F. Soll, Division of Neonatal-PerinatalMedicine, University of Vermont, Fletcher Allen Health Care, Smith552A, 111 Colchester Avenue, Burlington Vermont 05401, USA.E-mail: [email protected]
with some measures of confidence about the precisionof the estimate.
A systematic review begins with an explicit searchstrategy that allows for identification of all the highorder evidence from randomized controlled trials ofthe intervention of interest. Systematic reviews pro-duced by the CNRG may use statistical methods toaggregate and summarize the results of individualstudies (meta-analyses) in order to increase the powerto detect treatment effects and to provide more pre-cise estimates of the size of treatment effects thanare provided in the individual trials (5,6). In addi-tion, meta-analysis creates a structure in which to viewthe current status of trials information. This methodol-ogy is clearly different from traditional non-systematicreviews. In non-systematic reviews, the methodologyof the review process is not made explicit and theopinion of the review author may be mixed with rec-ommendations more firmly grounded in the availableevidence. This may lead to bias and the propagation oftreatment practices that, while popular and supportedby expert opinion, have little basis in science.
Reviews produced by the CNRG are publishedin the Cochrane Database of Systematic Reviews,which is contained in the Cochrane Library. Neonatalreviews can also be accessed on a web site, maintainedby the National Institute of Child Health and HumanDevelopment (www.nichd.nih.gov/cochraneneonatal).The CNRG has published 258 completed reviews and77 protocols of reviews in progress. Currently, thereare 575 authors or co-authors of reviews, protocolsor assigned titles from over 37 countries around theworld.
How Have Reviews from the CochraneNeonatal Review Group ImprovedNeonatal Care?
Two recent publications have reviewed the accom-plishments of the CNRG and the Cochrane Collab-oration in reference to neonatal care (7,8). Theseaccomplishments are illustrated in a variety of clinicalsituations. The paradigm for a Cochrane review hav-ing a significant impact on practice comes not fromthe CNRG, but from its ‘sister’ group, the CochranePregnancy and Childbirth Group, and its review of‘Antenatal corticosteroids for accelerating fetal lung
Copyright 2010 John Wiley & Sons, Ltd.

4 R. F. Soll
Typical Relative Risk (95% CI)
OUTCOME (N STUDIES)
TypicalRelative Risk
( 95% CI ) 0.5 1.0 2.0 4.00.2Decreased IncreasedRisk
0.5 1.0 2.0 4.00.2
CORTICOSTEROIDS PRIOR TO PRETERM BIRTH
RDS (14) 0.64 (0.56, 0.72)
OVERVIEW OF 18 RANDOMIZED CONTROLLED TRIALS
IVH (4) 0.57 (0.41, 0.78)
NEC (4) 0.60 (0.33, 1.09)
BPD (3) 1.38 (0.90, 2.11)
NEONATAL DEATH (13) 0.63 (0.51, 0.77)
Crowley 1992
Figure 1. Corticosteroids prior to preterm birth
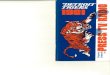
maturation for women at risk of preterm birth’ (9,10).In lamb studies of parturition, Liggins and colleaguesnoted that the offspring of ewes treated antenatallywith steroids had increased survival. This observationwas followed shortly by a randomized controlled trialthat demonstrated that fewer neonates whose moth-ers received antennal corticosteroids had RDS or died(11). Multiple randomized controlled trials of ante-natal corticosteroids followed in the 1970s and 1980sand provided consistent evidence of benefit for preterminfants. Despite the availability of this evidence, mostwomen with impending preterm delivery during thatera did not receive antenatal steroids and further con-trolled trials continued to be approved, funded andundertaken. A systematic review published by Crow-ley and coworkers in the 1990s included a total of18 randomized, controlled trials, enrolling over 3700infants. This review confirmed that antenatal steroidssubstantially reduced the risk of respiratory distresssyndrome, neonatal mortality and morbidity with-out increasing the risk of adverse maternal outcomes(9) (Fig. 1). This review has since been updated byRoberts and colleagues in 2006 and now includes 21studies (10).
In a cumulative meta-analysis, Jack Sinclair, theoriginal Coordinating Editor of the Cochrane NeonatalReview Group, asked the question, ‘At what point inthe history of trials of antenatal corticosteroids for fetallung maturation was the aggregated evidence sufficientto show that this treatment reduces the incidence ofRDS and neonatal death?’ (12). In Sinclair’s analysis,trials were ordered by their data publication and meta-analyses were performed sequentially. As previouslynoted, the initial trial of Liggins and coworkersdemonstrated a significant reduction in the risk ofRDS and the risk of neonatal death (11). As each newtrial was added to the cumulative meta-analysis, thereduction in the risk of death remained statisticallysignificant. The point estimate of the risk reductionchanged little with the addition of each new trial;
however, the 95% Confidence Interval (CI) narrowed,giving increased precision to the estimate of effect.
When presented in this fashion, one is hard pressedto justify the need for so many clinical trials. Despiteoverwhelming evidence from randomized controlledtrials, the utilization of antenatal steroids in verylow birth weight infants remained low throughout the1980s. The reasons that this evidence was not incor-porated into clinical practice are unclear. In part, thelack of acceptance of this data was attributable toinappropriate subgroup analyses. Clinicians were con-cerned that antenatal corticosteroids were ineffectivein twin gestation, male infants, prolonged rupture ofmembranes, and a variety of other clinical situations.The meta-analysis conducted by Crowley evaluates theeffect of antenatal steroids in several of these sub-groups and establishes that antenatal steroids wereeffective in a broad range of clinical situations andnot affected by issues such as multiple gestation orgender (9).
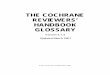
The evidence from this systematic review providedthe cornerstone of the National Institute of Health’sconsensus statement regarding the use of antenatalcorticosteroids (13). The consensus statement recom-mended the use of antenatal corticosteroids for womenat risk of preterm delivery in a broad range of gesta-tional ages with few exceptions. This strong evidence-based recommendation had a major impact on clinicalpractice. Attitudes and understanding of the benefits ofantenatal corticosteroids improved (14). This changein attitude was reflected by increased utilization ofsteroids (Fig. 2). In 1999, more than 79% of at riskinfants were treated with either a partial or full courseof antenatal corticosteroids compared with 16% in1987 (15,16). Increased use of antenatal steroids inthe early 1990s in conjunction with increased utiliza-tion of postnatal surfactant therapy led to improvementin survival of very low birth weight infants (17).
Reviews conducted by the CNRG have had a similarimpact on clinical practice and outcome. The use of
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482

The Cochrane Neonatal Review Group 5
0%
10%
20%
30%
40%
50%
60%
70%
80%
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
VERMONT OXFORD NETWORK ANNUAL REPORTS 1991-2008
USE OF ANTENATAL CORTICOSTEROIDS
NIHConference
CochraneReview
Figure 2. Increased utilization of corticosteroids after Cochrane review and NIH Statement
Typical Relative Risk and 95% CI
OUTCOME (N STUDIES)
TypicalRisk Difference
( 95% CI ) 0.5 1.0 2.0 4.00.2Decreased IncreasedRisk
0.5 1.0 2.0 4.00.2
EARLY (≤ 7 DAYS) POSTNATAL STEROID THERAPY
CLD @ 28 DAYS (17) -0.07 (-0.10,-0.03)
META-ANALYSIS OF 27 RANDOMIZED CONTROLLED TRAILS
CLD @ 36 WEEKS (21) -0.07 (-0.10, -0.04)
DEATH/CLD @ 36 WKS (22) -0.06 (-0.09, -0.02)
MORTALITY (27) 0.00 (-0.03, 0.03)
Halliday 2009
Figure 3. Postnatal corticosteroids for the prevention of chronic lung disease and death
antenatal corticosteroids was proven to be extremelybeneficial, but the use of postnatal corticosteroid ther-apy given directly to critically ill preterm neonates inhigher doses in order to ameliorate lung injury andbronchopulmonary dysplasia (BPD) was quite anotherstory. There is a strong theoretical basis for the useof postnatal corticosteroids in these infants. Postna-tal corticosteroid therapy may decrease lung injurythrough a variety of mechanisms, including stabi-lization of cell membranes, decreasing inflammatoryresponse and decreasing pulmonary edema (18). Mul-tiple trials have been conducted to assess the use ofpostnatal corticosteroids for the prevention of chroniclung disease. Halliday and colleagues have publishedand updated several reviews in the Cochrane Libraryaddressing the use of postnatal corticosteroids in pre-venting and treating BPD (19). In these reviews, itis clear that postnatal corticosteroids given within thefirst week of life to infants at risk of developing BPDor after the first week in life to infants with evolvingBPD ameliorates the underlying lung injury. Infantswho receive early postnatal corticosteroids require lessoxygen at 28 days [17 studies: typical Relative Risk
(RR) 0.87, 95% CI 0.81, 0.93]) and less oxygen at36 weeks postmenstrual age (21 studies: typical RR0.79, 95% CI 0.71, 0.88) (Fig. 3).
These trials of postnatal corticosteroids represent aheterogeneous group of studies, differing in time oftreatment onset, steroid preparation, steroid dose andlength of treatment. However, the meta-analysis is use-ful in providing an understanding of the risks andbenefits of the therapy. Despite the benefits regard-ing decreased BPD, many serious side effects havebeen reported. Clinicians were quickly aware of themany short-term side effects of postnatal corticos-teroid therapy like hypertension, hyperglycemia, gas-trointestinal bleeding, gastrointestinal perforation anddecreased somatic growth; however, there was littleawareness of the long-term problems regarding growthand neurodevelopment. Although fewer studies con-tributed to the meta-analysis, it is clear that there is anincreased risk of cerebral palsy associated with post-natal corticosteroid treatment (12 studies: typical RR1.45, 95% CI 1.06, 1.98) (Fig. 4). The concern overthese findings regarding the risks of cerebral palsy
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482

6 R. F. Soll
Typical Relative Risk and 95% CI
OUTCOME (N Studies)
TypicalRisk Difference
( 95% CI ) 0.5 1.0 2.0 4.00.2Decreased IncreasedRisk
0.5 1.0 2.0 4.00.2
EARLY (≤ 7 DAYS) POSTNATAL STEROID THERAPY
NEURODEVELOPMENTAL OUTCOME IN SURVIVORS
BAYLEY MDI < 2SD (3) -0.01 (-0.09, 0.09)
BAYLEY PDI < 2SD (3) 0.04 (-0.04, 0.11)
DEVELOPMENTAL DELAY (1)
CEREBRAL PALSY (12) 0.07 (0.02, 0.11)
MOD/SEVERE IMPAIRMENT (7) 0.03 (-0.03, 0.10)
PVL (12)
ABNORMAL NEURO EXAM (5)
0.01 (-0.01, 0.03)
0.18 (0.10, 0.26)
0.27 (0.12, 0.42)
Halliday 2009
Figure 4. Neurodevelopmental outcome in surviving infants given postnatal corticosteroid therapy to prevent chronic lung disease
0%
10%
20%
30%
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
VERMONT OXFORD NETWORK ANNUAL REPORTS 1991-2008
POSTNATAL CORTICOSTEROID USE IN VLBW INFANTS
AAPStatement
CochraneReview
Figure 5. Decreased utilization of postnatal corticosteroids after publication of Cochrane review and statement from theAmerican Academy of Pediatrics
and poor developmental outcome led to a strong state-ment from the American Academy of Pediatrics andthe Canadian Pediatric Society (20). The statementrecommended severe restriction in the use of postna-tal corticosteroids in the prevention and treatment ofchronic lung disease, noting that ‘outside the contextof a randomized, controlled trial, the use of corticos-teroids should be limited to the exceptional clinical cir-cumstances’. These evidence-based recommendationshave led to significant changes in clinical practice, notyet to a new trial. The exposure of at risk babies hasdecreased dramatically. In the Vermont Oxford Net-work, up to 28% of very low birth weight infants wereexposed to postnatal corticosteroid therapy prior to theAcademy statement (1997) and only 8% were exposedafter (although there is great variation in practice, withthe interquartile difference ranging from 2–11%) (21)(Fig. 5).
Decisions regarding an intervention are not alwaysmade easier despite an abundance of evidence. Theuse of prophylactic indomethacin in the preventionof intraventricular hemorrhage has been extensively
studied in randomized controlled trials. Intraventric-ular hemorrhage (IVH) remains a major problem ofthe very low birth weight infant, with 26% havingsome degree of bruising or bleeding and 9% havingthe more severe grades of hemorrhage. Prophylacticindomethacin has been evaluated, both in the pre-vention of patent ductus arteriosus (PDA) and in theprevention of IVH. Indomethacin, a cyclooxygenaseinhibitor of prostaglandin synthesis, has been demon-strated to modulate cerebral blood flow, decreaseserum prostaglandin levels and promote germinalmatrix maturation. A meta-analysis of multiple clini-cal trials suggests that indomethacin lowers the risk ofpatent ductus arteriosus (14 studies: typical RR 0.44,95% CI 0.38, 0.50) and severe intraventricular hem-orrhage (14 studies: typical RR 0.66, 95% CI 0.53,0.82) (22). These short-term clinical effects seem tobe of real benefit. However, there is concern that cere-bral ischemia and necrotizing enterocolitis may be sideeffects of indomethacin treatment, although neitherof these complications was demonstrated in previous
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482

The Cochrane Neonatal Review Group 7
Relative Risk and 95% CI
OUTCOME (N STUDIES)Risk Difference
( 95% CI) 0.5 1.0 2.0 4.00.2Decreased IncreasedRisk
0.5 1.0 2.0 4.00.2
ELECTIVE HIGH FREQUENCY OSCILLATORY VENTILATION
IVH (11) 0.02 (-0.01, 0.05)
META-ANALYSIS OF 17 RANDOMIZED CONTROLLED TRIALS
SEVERE IVH (16) 0.02 (-0.01, 0.04)
PVL (15) 0.01 (-0.01, 0.02)
SEVERE RETINOPATHY (10) -0.04 (-0.07, -0.01)
CHRONIC LUNG DISEASE (15) -0.04 (-0.08, 0.00)
DEATH (15) 0.00 (-0.03, 0.02)
CLD/DEATH @ 36 WKS PMA (15) -0.05 (-0.11, 0.01)
PULMONARY AIRLEAK (12) 0.05 (0.01, 0.08)
Cools 2009
Figure 6. Elective high frequency ventilation in preterm infants
trials (23). Given this uncertainty, Schmidt and col-leagues conducted a large pragmatic trial to evaluatethe effects of prophylactic indomethacin on neurode-velopmental outcome (24). This study demonstratedsimilar effects on short-term outcomes (PDA closure,IVH) as were reported in the meta-analysis of previoussmaller trials. However, the trial of Schmidt and col-leagues clearly demonstrated that there was no differ-ence in developmental outcome. This further evidencehas actually made the decision making more complex.Although the short-term benefits are proven, the lackof long-term benefits means that any potential sideeffect may lead many clinicians to choose not to treat.However, this cannot be considered a problem basedon a deficiency in the evidence. These trials includedin the meta-analysis, and Schmidt’s trial in particular,gives us precise estimates of the risks and benefits ofprophylactic indomethacin treatment. Clinicians andfamilies must weigh these risks and benefits to decideif the short-term benefits are worth any (unproven) riskgiven the similar long-term outcomes.
In other situations, there may be abundant evidencethat an intervention has little clinical impact, but thereis little evidence that the neonatal community has beeninfluenced by this evidence. This appears to be thecase with the use of elective high frequency ventilation(HFV). High frequency ventilation uses a uniqueapproach to ventilation. HFV delivers continuousdistending pressure and small tidal volumes (lessthan the anatomic dead space) superimposed on anextremely rapid rate. Experimental work in animalmodels suggests that ventilation strategies using HFV(either as high frequency oscillatory ventilation or highfrequency jet ventilation) hold great promise in theprevention of lung injury in preterm infants. However,clinical trials of either modality demonstrate littleclinical benefit and raise the possibility of adverseeffects, including increased risk of intraventricularhemorrhage and poor neurological development.
Henderson-Smart and colleagues reviewed the ran-domized controlled trials comparing elective use ofHFOV to conventional ventilation (CV) in preterminfants who are mechanically ventilated for pulmonarydysfunction. This review was recently updated byCools and colleagues (25) (Fig. 6). The systematicreview of elective HFOV includes studies that enrolledpreterm or low birth weight infants with pulmonarydysfunction mainly due to respiratory distress syn-drome (RDS) who required mechanical ventilation.Studies were included if randomization to either elec-tive HFOV or to CV occurred early in the course ofRDS, soon after mechanical ventilation was begun.In their search of the literature, the authors found 17randomized controlled trials (enrolling 3652 infants)that met the criteria. There was a fair amount of clini-cal heterogeneity between the studies. The size of thestudies varied considerably, ranging from 43 to 273infants. Although all studies included preterm infants,the upper limit for birth weight and gestational agediffered between the studies. The age and random-ization varied from less than 1 h to 9 h of age. Inaddition, a heterogeneous group of ventilators wereused to deliver HFOV.
In an overall analysis, few changes in clinicaloutcome were noted. Surprisingly, the meta-analysissuggests a slight increase in the risk of pulmonaryair leak associated with the use of elective HFOV(12 studies: typical RR 1.19, 95% CI 1.05, 1.34).No difference in the risk of death at approximatelyterm equivalent age is noted (15 studies: typical RR0.98 95% CI 0.83, 1.14). The effect on the combinedoutcome death or CLD at 36–37 weeks postmenstrualage or discharge was marginally affected by electiveHFOV (9 studies: typical RR 0.92, 95% CI 0.85, 1.00).No differences in mortality were noted in a variety ofsubgroup analyses, including evaluation of ventilationstrategy (high lung volume strategy).
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482

8 R. F. Soll
0%
10%
20%
30%
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
% V
LB
W I
NF
AN
TS
VERMONT OXFORD NETWORK ANNUAL REPORTS 1991-2008
HIGH FREQUENCY VENTILATION
Figure 7. Increased utilization of high frequency ventilation
0%
10%
20%
30%
40%
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
% V
LB
W I
NF
AN
TS
VERMONT OXFORD NETWORK ANNUAL REPORTS 1994-2008
CHRONIC LUNG DISEASE IN VLBW INFANTS
Figure 8. Incidence of chronic lung disease in the Vermont Oxford Network 1994–2008
Fortunately, the concern regarding increased riskof any of severe IVH is not supported by the meta-analysis [any IVH (11 trials), typical RR 1.05, 95%CI 0.96, 1.15; severe IVH (16 trials), typical RR1.11, 95% CI 0.95, 1.30]. No significant increasein the risk of white matter damage is demonstratedin the meta-analysis (15 studies: typical RR 1.10,95% CI 0.85, 1.43). Few trials have discussed long-term neurodevelopmental status. Although only twotrials reported on neurodevelopmental outcome at1–3 years, an increased risk of neurodevelopmentalproblems was reported (typical RR 1.26, 95% CI 1.01,1.58).
Based on the results of the updated systematicoverview, Cools and colleagues concluded that therewas no clear evidence that elective HFOV, as com-pared with CV, offered important advantages whenused as an initial ventilation strategy to preterm babieswith acute pulmonary dysfunction. In particular, theynoted that there was no evidence of a reduction in thedeath rate, although there may be a small reduction inthe rate of CLD. This evidence that CLD was reducedis marginally significant and is weakened by the incon-sistency of this effect across trials. Adverse effectson short-term neurological outcome were observed in
some studies, but these effects were not significantoverall. Information about the effects of long-term out-come was inadequate. Despite the evidence for a lackof meaningful effect of this new technology, HFV hascome into widespread use. Ever increasing numbers ofvery low birth weight infants are placed on HFV; oneout of every five VLBW infants in the Vermont OxfordNetwork is supported with HFV at some point in theirhospital stay (interquartile range 9.1% to 28.3%) (21)(Fig. 7); however, little change can be documented inthe incidence of chronic lung disease, the target out-come of HFV (Fig. 8).
Cochrane reviews have demonstrated that recenttherapies, in particular, cooling for infants with mod-erate to severe hypoxic ischemic encephalopathy, havebeen demonstrated to be of great benefit. In a meta-analysis of these trials, Jacobs and colleagues demon-strated a strong effect on mortality and severe devel-opmental problems (26). Eight randomized controlledtrials are included in this review, comprising 638 terminfants with moderate to severe encephalopathy. Ther-apeutic hypothermia results in a statistically signifi-cant and clinically important reduction in mortalityand neurodevelopmental disability (4 studies: typi-cal RR 0.76, 95% CI 0.65, 0.89) (Fig. 9). The point
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482

The Cochrane Neonatal Review Group 9
TYPICAL ESTIMATE -0.14 (-0.21, -0.08)
Subtotal -0.16 (-0.23, -0.09)
TOBY 2008 -0.07 (-0.18, 0.04)
EUROPEAN 2008 -0.32 (-0.48, -0.15)
SHANKARAN 2005 -0.18 (-0.31,-0.05)
EICHER 2005 -0.32 (-0.56,-0.08)
WHOLE BODY COOLING
Subtotal -0.09 (-0.21, 0.03)
GLUCKMAN 2005 -0.12 (-0.25, 0.01)
GUNN 1998 0.08 (-0.26, 0.42)
Relative Risk and 95% CI
STUDY Risk Difference(95% CI) 0.5 1.0 2.0 4.00.2
Decreased IncreasedRisk
0.5 1.0 2.0 4.00.2
HYPOTHERMIA FOR HYPOXIC ISCHEMIC ENCEPHALOPATHY
DEATH OR MAJOR DISABILITY
SELECTIVE HEAD COOLING
Modified from Jacobs 2007
Figure 9. The effect of hypothermia on death or major disability in infants with moderate to severe hypoxic ischemicencephalopathy
estimate for these important clinical outcomes suggeststhat for every seven infants with moderate to severehypoxic, ischemic encephalopathy treated with cool-ing therapy, one additional infant will survive withoutdevelopmental problems. This analysis has contributedto the creation of guidelines (ILCOR) suggesting thatit is time to introduce this therapy into routine practice(27).
Conclusion
Cochrane reviews, including many from the CNRG,have had an important role in creating more preciseestimates of the effects of interventions that have beenincorporated into guidelines and policies and have con-tributed in measurable ways to the improvement ofoutcome in neonates. Still, there are many circum-stances where people ignore the results of randomizedtrials or are unaware of what the evidence shows.To date, fewer than one-third of all the randomized,controlled trials that have been published in the fieldof neonatology have been incorporated in systematicreviews. Much remains to be done in order to create abetter evidence-based framework on which to practiceNeonatal-Perinatal Medicine.
References
1. Sackett DL, Rosenberg WM, Gray JA, et al. Evidence-basedmedicine what it is and what it isn’t. Br Med J. 1996; 312: 71–72(editorial).
2. Akobeng AK. Principles of evidence based medicine. Arch DisChild. 2005; 90: 837–840.
3. Sackett DL, Richardson WS, Rosenberg W, et al. Evidence-BasedMedicine. How to Practice and Teach EBM, 2nd edn. London:Churchill Livingston; 2000.
4. Sinclair JC, Bracken MB, Horbar JD, et al. Introduction toneonatal systematic reviews. Pediatrics. 1997; 100: 892–895.
5. Cunningham AS. Meta-analysis and methodology review: what’sin a name? J Pediatr. 1988; 113: 328–329.
6. Cook DJ, Mulrow CD, Haynes RB. Systematic reviews: synthesisof best evidence for clinical decisions. Ann Intern Med. 1997;126(5): 376–380.
7. McGuire W, Fowlie PW, Soll RF. What has the Cochranecollaboration ever done for newborn infants? Arch Dis Child FetalNeonatal Ed. 2010; 95(1): F2–6. (Epub 2009 May 3).
8. Soll RF. Evaluating the medical evidence for quality improvement.Clinics in Perinatology, in press.
9. Crowley P, Chalmers I, Keirse MJ. The effects of corticosteroidadministration before preterm delivery: an overview of theevidence from controlled trials. Br J Obstet Gynaecol. 1990; 97(1):11–25.
10. Roberts D, Dalziel SR. Antenatal corticosteroids for acceleratingfetal lung maturation for women at risk of preterm birth. CochraneDatabase System Rev 2006; Issue 3. Art. No.: CD004454.
11. Liggins GC, Howie RN. A controlled trial of antepartumglucocorticoid treatment for prevention of the respiratory distresssyndrome in premature infants. Pediatrics. 1972; 50(4): 515–525.
12. Sinclair JC. Meta-analysis of randomized controlled trials ofantenatal corticosteroids for the prevention of respiratory distresssyndrome: discussion. Am J Obstet Gynecol. 1995; 173: 335–344.
13. NIH Consensus Development Panel on the Effect of Corticos-teroids for Fetal Maturation on Perinatal Outcomes. JAMA. 1995;273: 413–418.
14. Wright LL, Merenstein GB, Goldenberg RL, et al. Impact of theNIH Consensus Development Conference on Corticosteroids forFetal Maturation: change in obstetric attitudes. Pediatr Res. 1996;39: 254 (abstract).
15. Fanaroff AA, Hack M, Walsh MC. The NICHD neonatal researchnetwork: changes in practice and outcomes during the first15 years. Sem Perinatol 2003; 27: 281–287.
16. Walsh MC, Yao Q, Horbar JD, et al. Changes in the Use ofPostnatal Steroids for Bronchopulmonary Dysplasia in 3 LargeNeonatal Networks. Pediatrics. 2006; 118: e1328–e1335.
17. Schwartz RM, Luby AM, Scanlon JW, Kellogg RJ. Effect ofsurfactant on morbidity, mortality, and resource use in newborninfants weighing 500 to 1500 g. N Engl J Med. 1994; 330(21):1476–1480.
18. Bancalari E. Corticosteroids and neonatal chronic lung disease.Eur J Pediatr. 1998; 157: [Suppl 1]: S31–S37.
19. Halliday HL, Ehrenkranz RA, Doyle LW. Early (<8 days)postnatal corticosteroids for preventing chronic lung disease inpreterm infants. Cochrane Database System Rev 2009; Issue 1.Art. No.: CD001146.
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482

10 R. F. Soll
20. Committee on Fetus and Newborn. Postnatal corticosteroids totreat or prevent chronic lung disease in preterm infants. Pediatrics.2002; 109(2): 330–338.
21. The Vermont Oxford Network Database 2008; http://www.vtoxford.org/ (accessed March 15, 2010).
22. Fowlie PW, Davis PG. Prophylactic intravenous indomethacin forpreventing mortality and morbidity in preterm infants. CochraneDatabase System Rev, 2002; Issue 3. Art. No.: CD000174.
23. Schmidt B, Davis P, Moddemann D, et al. Long-term effects ofindomethacin prophylaxis in extremely-low-birth-weight infants.N Engl J Med. 2001; 344(26): 1966–1972.
24. Cools F, Henderson-Smart DJ, Offringa M, et al. Elective highfrequency oscillatory ventilation versus conventional ventilation
for acute pulmonary dysfunction in preterm infants. CochraneDatabase System Rev, 2009; Issue 3. Art. No.: CD000104.
25. Jacobs SE, Hunt R, Tarnow-Mordi WO, et al. Cooling fornewborns with hypoxic ischaemic encephalopathy. CochraneDatabase System Rev, 2007; Issue 4. Art. No.: CD003311.
26. Hoehn T, Hansmann G, Buhrer C, Simbruner G, Gunn AJ,Yager J, Levene M, Hamrick SE, Shankaran S, Thoresen M.Therapeutic hypothermia in neonates. Review of currentclinical data, ILCOR recommendations and suggestions forimplementation in neonatal intensive care units. Resuscitation.2008; 78(1): 7–12.
Copyright 2010 John Wiley & Sons, Ltd. Evid.-Based Child Health 5: 3–10 (2010)DOI: 10.1002/ebch.482