Embed Size (px)
Citation preview

640
THE CLASSIFICATION AND PROGNOSIS OFNEPHRITIS AND ALLIED RENAL DISEASES
By M. D. MILNE, M.D., Ch.B., M.R.C.P.Physician and Lecturer, Postgraduate Medical School, London
A satisfactory classification of nephritis whichwill correlate with pathological findings and willpermit an accurate prognosis, has proved a matterof great difficulty. It is a constant source of worryto the postgraduate student who fears that theparticular classification and nomenclature he haslearned and adopted may be anathema to examinersfor higher degrees and diplomas who may happento belong to a rival school of thought. The maindifficulty is that the clinician observes manifesta-tions of abnormal renal function, whilst the morbidanatomist is concerned with structural abnormal-ities which are frequently the terminal results oflongstanding renal disease.
Different diseases may produce an almostidentical clinical and functional abnormality andthe same pathological process may vary widely inits effects on renal function and in the rapidity ofits progression or resolution. Correlation ofclinical and pathological data will probably befacilitated in the future by greater use of renalbiopsy techniques (Kark and Muehrake, 1954;Iversen and Brun, 195I), but it is doubtful whetherthis method will ever prove as popular and usefulas aspiration biopsy of the liver in the assessment ofhepatic disease. Diagnosis and classification ofnephritis must, in the main, be dependent on anaccurate clinical history to give an indication ofpast events and on tests of renal function to definethe existing state. Modem clearance methods havepreviously been regarded as research procedures,but are now becoming used as routine methods inthe difficult case. Their significance and averagenormal values are given in Table i. In most cases,however, more simple tests suffice, including theurea clearance which is roughly proportional to,but always lower than, the clearance of inulin, andthe determination of maximal concentrating powerto give an indication of distal tubular function. Inaddition, it is essential to examine the spun de-posit for red cells, leucocytes and casts, and todetermine the degree of proteinuria expressed asthe amount in grams lost each day.
All authorities now agree that primarynephritis can be divided into the two maincategories of glomerulo-nephritis and pyelo-nephritis. Glomerulo-nephritis, as its name sug-gests, primarily affects the glomeruli, and at itsonset is diffuse and uniform throughout bothkidneys. At some stage of the disease proteinuriais usually of severe degree, casts are plentiful andthere is in most cases an oedematous stage. Pyelo-nephritis primarily affects the pelvris, collectingand distal tubules, although it may involve theglomeruli later. It is patchy in distribution andmay be unilateral. Proteinuria is never of severedegree, almost always amounting to less than 2 g.each day and completely absent in some cases(Raaschou, 1945). Casts are scanty and oedemanever occurs unless it is secondary to hypertensivecardiac failure. Pyuria and bacteriuria are presentin the acute stage and during acute exacerbations,but may be completely absent for long periodsduring the chronic stage.Acute Glomerulo-NephritisThe course and prognosis of this disease have
been well described by Rudebeck (1946) and byEllis (I942), who terms it 'Type i nephritis.' Itcommonly commences from one to three weeksafter a streptococcal infection, usually acute ton-sillitis. It is considered to be due to an abnormalimmune response, since the anti-streptolysin titreis usually found to be high (Lyttle et al., I938) andserum complement to be low (Lange et al., I95 ;Kellett, I952). A similar condition may be pro-duced in animals by injection of anti-serum pre-pared from homologous kidney (Masugi, I934).Rammelkamp et al. (1952) have emphasized thedifferences in the response from that seen in acuterheumatism which may similarly follow strepto-coccal infections. Glomerulo-nephritis eitheroccurs sporadically or in large (Brown, I9I6) orsmall (Kempe et al., I95 ) epidemic waves follow-ing infection with streptococci showing' nephrito-genic' tendencies, most commonly a Type I2
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from

December I954 MILNE: The Classification and Prognosis of Nephritis and Allied Renal Diseases 641
TABLE IClearance Methods of Assessment of Renal Function
Average Value Effect of Nephritis on clearanceClearance corrected to Function Measured
surface area Glomerulo- Pyelo-of 1.73 sq.m. nephritis nephritis
Inulin clearance I23 ml./min. Glomerular filtration rate - (early) - (late)
Para-aminohippurate (PAH) 634 ml./min. Renal plasma flow - or Nclearance
Inulin clearance: PAH clearance. 19.4 per cent. Fraction of plasma filtered N or +(Filtration fraction) through glomeruli
Extraction ratio PAH (EPAH) 92 per cent. Fraction ofplasma perfus-ing functional renal tissue
Tubular maximal resorptive 78.9 mg./min. Proximal tubular function N (early)capacity (TmPAH) - (late)
Inulin clearance: TmPAH 1.55 ml./mg. Ratio of glomerular to - +tubular function
Figures quoted are mean values taken from Smith, H. W. (1951), ' The Kidney: Structure and Function in Healthand Disease.' New York.
organism (Rammelkamp and Weaver, I953).Rheumatic fever occurs sporadically after in-fections with any group A streptococcus and tendsto relapse with later infections. A second attackof acute glomerulo-nephritis is very rare provideda full recovery from the first attack takes place.The classical symptoms and signs are haema-
turia, oedema of slight or moderate degree,oliguria and hypertension. There is considerableproteinuria and the urine is usually of high specificgravity and contains very little sodium chloride.Hospital physicians, other than physicians in feverhospitals, do not see sub-clinical cases, but there isno doubt that these occur. If cases of scarlet feverare followed after apparent recovery a proportionwill show sub-clinical nephritis recognizable onlyby careful examination of the urine (McCrae,I913; Weinstein et al., I950). Similarly, duringepidemics of acute nephritis (Kempe et al., I95I)sub-clinical cases are to be found by urinaryexamination of cases of tonsillitis who never showovert clinical nephritis. Long-term follow-updata on such sub-clinical cases is insufficient forus to be certain whether the proportion going onto chronic nephritis is similar to that followingovert acute nephritis, but there is indirect evidencethat it may be. Rudebeck (x946) has shown that,apart from death in the acute stage of the disease,the prognosis as to complete recovery dependsonly on the age of the patient. Over 90o per cent.of cases under 3o, but less than 50 per cent. over50o, recover completely. The prognosis does notappear to be influenced by the severity of thealbuminuria, haematuria or oedema. Severe
hypertension is an adverse feature, but the highestblood pressures are seen in the more elderly cases.Acute nephritis results in an acute increment ofblood pressure above the basal level which isknown to rise with increasing age (Hamilton et al.,I954). It seems likely, therefore, that the prog-nosis in sub-clinical cases of acute nephritis will beuninfluenced by the mildness of the disease, andthat a proportion will not resolve completely andaccount for some examples of chronic glomerulo-nephritis without a previous history of acute attack.
Ellis (i942) showed that in overt cases therewere four possible alternatives with regard to theoutcome of the disease.
(a) The great majority (82 per cent. of Ellis'scases) recovered completely, as shown by dis-appearance of hypertension, haematuria, oedemaand, finally, albuminuria.
(b) A small proportion ( 4 per cent.) died in theacute stage. Possible causes of death are un-controlled streptococcal infection, cardiac failurewhich is commoner in the elderly patient, repeatedconvulsions and anuria or severe oliguria. Thelast possibility is an especially serious complicationsince the prognosis is more grave than in oliguriaor anuria due to acute tubular necrosis. Theanuria occurring as a complication of acuteglomerulo-nephritis is more often absolute andtends to be more prolonged (Swann and Merrill,I953), the anuric or oliguric phase sometimeslasting longer than four weeks before diuresiseventually supervenes.
(c) Some cases (4 per cent.) never lost theoedema or haematuria. Proteinuria increased
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from

642 POSTGRADUATE MEDICAL JOURNAL December 1954
steadily in amount and the patients passed into anephrotic stage before dying of uraemia within ayear of the onset of the illness.
(d) The remainder (IO per cent.) gradually losttheir oedema and haematuria and often the hyper-tension, but retained their proteinuria. Theybecame symptomatically recovered, often formany years. Throughout this period, however,there was an insidious and progressive failure ofrenal function until hypertension recurred and thepatients died of uraemia many years after the acuteattack.
The Nephrotic SyndromeThere is still considerable controversy with re-
gard to the terminology and'classification of casesof the nephrotic syndrome. It is a conditioncharacterized by massive oedema'often associatedwith serous effusions, severe albuminuria, hypo-albuminaemia and hypercholesterolaemia. Someauthorities exclude cases complicated by haema-turia, hypertension and retention of non-proteinnitrogen. This seems to be an artificial distinctionsince cases which originally do not show any ofthese features may develop them as the conditionprogresses. In addition, it is very difficult todraw an exact dividing line between the normaland abnormal in any bf these three complications.In particular, definition of a normal blood pressurecan only be based on statistical data (Hamilton etal., i954) and the level of blood urea is dependenton the amount of protein ingested as well as onrenal function. Most cases show some degree ofmicroscopic haematuria from the onset (Galan,1949). It is considered preferable therefore torefer to such cases as examples of the nephroticsyndrome complicated by hypertension, haema-turia or uraemia according to the abnormalitiesfound.The basic functional disorder is an increased
permeability of the glomeruli to the plasma pro-teins (Chinard et al., I954), particularly to the lowmolecular weight fractions, e.g. albumin and ,o-globulin (Squire, I953). There is no evidence thatplasma proteins in the nephrotic syndrome arequalitatively abnormal. Both plasma and urinaryalbumin have been shown to be of normal com-position by immunological methods (Gitlin andJaneway, I952). Although the correlation is farfrom absolute, there is in general a parallel be-tween the amount of urinary protein loss, thelowering of plasma albumin and the magnitude ofthe oedema (Squire, I953). Oedema is liable todevelop in the adult patient at levels of urinaryprotein loss of between 5 and io g. each day andis usually present if the loss is higher than this.Any, codldition which can so alter glomerular
filnction thatithere is prolonged excessive urinary
protein loss can therefore cause the nephroticsyndrome. Less severe manifestations of the samedisorder may result in smaller urinary protein lossand oedema will then not occur. Theoreticallythere is no fundamental difference between thesetwo typ'es of renal abnormality, but to the patientand the clinician the practical difference of thepresence or absence of oedema is all important andmay determine whether the renal disorder isalmost symptomless or completely incapacitating.Protein deficiency and oedema secondary tourinary loss of abnormal proteins should not beclassed as examples of the syndrome. For example,a patient was recently seen with gross anasarca andwith a constant proteinuria of 15 g. each day.There was severe hypoalbuminaemia, plasmaalbumin being 2.0 g./Ioo ml. More careful urinetesting showed that most of the urinary proteinwas Bence-Jones protein and this was confirmedby electrophoresis, almost all the protein being aY-globulin with only a small quantity of albumin.Although the low plasma albumin was almostcertainly secondary to the severe urinary proteinloss this case did not show the fundamentalabnormality of the nephrotic syndrome, i.e. in-creased glomerular permeability to albumin.Bence-Jones protein is of small molecular weightand is filtered through normal glomeruli.The causes of the nephrotic syndrome can be
classified as follows:(a) Cases resulting from renal complications of
various systemic diseases, particularly diabetesmellitus, amyloidosis, disseminated lupus ery-thematosus and syphilis. In this country diabeticglomerulo-sclerosis or the Kimmelstiel-Wilsonsyndrome (1936) is the commonest cause of thenephrotic syndrome in adults. It has becomemore common in recent years due to the fact thatdiabetics are kept alive for many years by insulinand to the increased incidence of diabetes in obeseelderly subjects in an ageing population. Theprognosis is poor, there being a steady progressionto terminal uraemia. Renal amyloidosis is usuallyof the secondary variety but occasionally primaryamyloidosis may involve the kidney to a significantextent (Thingstad, I95I; Reimann et al., I954).
Amyloidosis secondary to chronic sepsis and un-controlled tuberculosis is now becoming lesscommon and the chief cause of this condition inmany hospital series is rheumatoid arthritis. Itshould be suspected in any case of rheumatoidarthritis showing albuminuria. In many cases theproteinuria is slight and the case then shows a slowprogression to renal failure rather than thenephrotic syndrome. The prognosis is poor unlessthe primary disease can -be radically cured.Similarly, although renal involvement in cases ofdisseminated lupus erythematosus is not un-
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from

December 1954 MILNE: The Classification and Prognosis of Nephritis and Allied Renal Diseases 643
- An.-
la
|- | -
;1 l· * - |
E = ! w>= , A. ... An..... -# A.:·tB5~rrp Adi i;PB"Ecrlem
fi,inti~;·-;.--5"--·- ASP...................-. ( ar
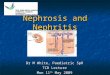
FIG. I.-Section through main tributary of renal vein in a case of the nephrotic syndrome. There is organizingthrombus becoming recanalized. This thrombus involved all the smaller tributaries of the renal veins but didnot extend into the main renal vein trunks. x 17.
common, the nephrotic syndrome occurs in only aproportion (Stickney and Keith, I940; Daughertyand Baggenstoss, I950). The prognosis is muchmore grave if there is evidence of renal involve-ment. Whilst most of the manifestations of thisdisease respond favourably to ACTH or cortisone,the renal complications are much more re-sistant to treatment. Syphilis is now rarelycomplicated by the nephrotic syndrome, pre-sumably because of efficient means of therapy.The condition used to be seen in the secondarystage and usually responded well to anti-syphilitictherapy (Munk, I9I3).
(b) As a result of drug toxicity. The nephroticsyndrome has been described after trimethadioneused in the treatment of petit mal (Barnett et al.,1948; White, I949), gold salts (Vallery-Radot etal., 1942), inorganic mercury (Wilson et al., I952)and after poison oak dermatitis (Rytand, 1948).Although there is little doubt from the clinicaldescriptions of the cases that all these agents cancause the syndrome, the case due to trimethadionedescribed by Barnett et al. (I948) is most con-clusive since the condition cleared when the drugwas stopped, only to recur when it was taken again.The prognosis of this type of nephrotic syndromeis good if the aetiology is recognized early in thecourse of the disease and administration of thenoxious agent is stopped. Clinicians should care-fully question all patients with a nephrotic syn-
drome of unknown cause with regard to ingestionof drugs, since it is highly probable that many othermedicaments may cause this condition.
(c) Following renal vein thrombosis and othercauses of increased pressure in the renal veins.Thrombosis of the inferior vena cava involving therenal veins may lead to the nephrotic syndrome(Derow et al., 1939). This is relatively easy todiagnose if signs of inferior vena caval obstructionare present. In doubtful cases this may be con-firmed by venography. In some cases, however,both renal veins may be thrombosed without in-volvement of the main caval trunk. In a recentcase treated at Hammersmith Hospital, a boy, aged7, appeared to be a typical case of the nephroticsyndrome of unknown cause. He died of pneumo-coccal peritonitis, and at necropsy it was found thatall the main tributaries of the renal veins were filledwith organizing thrombus (Fig. I), the main renalvein trunks and the inferior vena cava not beinginvolved. The thrombus clearly antedated theperitonitis and could well have dated from theonset of the disease. Such a case would be com-pletely missed at necropsy if the renal veins andtheir tributaries within the kidney substance werenot carefully examined.
Cardiac failure may very occasionally lead toproteinuria of sufficient degree to cause depressionof plasma albumin and a nephrotic syndrome.Squire (1953) records a case of constrictive peri-
C1
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL December I954
carditis with many features typical of the nephroticsyndrome. The massive proteinuria and othernephrotic features cleared after pericardectomy.
(d) Cases secondary to acute glomerulo-nephritis. This is the rapidly progressive courseof Ellis (I942). Such cases are easy to recognizeif they follow an overt attack of acute nephritis,but difficult if secondary to a sub-clinical attack.They are likely to show haematuria and hyper-tension from the onset and death from uraemiaoccurs less than one year from the start of theillness. This rapidly progressive course seems tobe not uncommon following acute nephritisassociated with Henoch-Schonlein purpura (Har-rison et al., 1954).
(e) Cases of unknown cause (Type 2 nephritis ofEllis, I942; 'pure lipoid nephrosis' of Volhardand Fahr, 1914). It may well be that this classdoes not form a uniform entity and as more causesof the nephrotic syndrome are discovered it willbecome a still smaller group. There is little doubtthat this is a disease different from acute glomerulo-nephritis (Type I, Ellis). The course may beprolonged over many years unless death fromintercurrent infection occurs. Many cases recovercompletely with disappearance of the oedema andalbuminuria-I 5 per cent. of Ellis's series, 26 percent. of the series of Barnett et al. (I952). Thisdisease, like acute glomerulo-nephritis, is com-monest in childhood but the exact age distributionis different. Type 2 nephritis occurs most fre-quently in the age group two to four years; Type Inephritis in the age group five to nine years(Barnett et al., 1952). It is clear from this agedistribution that Type 2 nephritis cannot followType I; no one has ever suggested that thereverse occurs. In addition, the two conditionshave a different pathological picture. Type Inephritis shows acute glomerular inflammation inthe acute stage followed by organization andfibrosis in the cases which become chronic. Type 2nephritis shows a degenerative pathological picturewith thickening of the basement membrane andhyalinization of the glomeruli. The combinedclinical and pathological investigation of Davsonand Platt (I949) gives further evidence that theconditions are distinct.
In doubtful cases special laboratory investiga-tions may assist in the diagnosis. The inulinclearance has many advantages over the ureaclearance in the assessment of glomerular functionin the nephrotic syndrome (Bruck et al., I954).The urea clearance is especially liable to error inthe presence of oliguria. The level of blood ureatends to be variable in the nephrotic syndromesince a high protein diet is usually prescribeddespite the notoriously capricious appetite of thesepatients. Reduction in the inulin clearance early
in the course of the disease suggests that thediagnosis is not Type -2 nephritis. In Type Inephritis the ratio of inulin to PAH clearance(filtration fraction) is depressed and this tends topersist if the condition passes into the nephroticstage. This ratio is usually normal in Type 2nephritis. Paper electrophoresis of plasma pro-teins may also be of value (Lagrue et al., 1954).In Type 2 nephritis the concentration of r-globulin tends to be below normal. In Type Inephritis it is normal or high and is always in-creased in amyloidosis or lupus erythematosus.
Pyelo-NephritisThere is comparatively little controversy with
regard to the classification and definition ofpyelo-nephritis, but we are still completely unableto explain the diverse clinical features of thisdisease. Acute pyelo-nephritis provides no diag-nostic problem, being associated with a typicalclinical picture of loin pain, frequency of mic-turition and dysuria and always showing evidenceof urinary infection and pyuria. Chronic pyelo-nephritis usually follows an incompletely treatedacute attack and runs a prolonged course associatedwith exacerbations and remissions. Bacteriuriaand pyuria are present in the exacerbations, butthe urine may be almost normal during the re-missions of the disease. Some cases give nohistory of an acute attack and present with evidenceof progressive renal failure. Tests of renal func-tion can assist in the diagnosis of such cases sincethere is always evidence of greater loss of tubularthan of glomerular function. In particular, loss ofconcentrating power usually precedes urea re-tention (Raaschou, I943) and the ratio of inulinclearance to tubular maximal reabsorptive capacityfor PAH (Cn/TmPAH) is increased (Raas-chou, 1948). The reverse applies in glomerulo-nephritis. There is also clear pathologicalevidence (Staemmler and Dopheide, 1930) that inchronic pyelo-nephritis, tubular damage precedesinvolvement of the glomeruli.
Pyelo-nephritis may or may not lead to secondaryhypertension and this may develop at a time whenrenal function is perfectly normal. This isespecially well seen in cases of severe hypertensiondue to unilateral pyelo-nephritis in whom excisionof the affected kidney may lead to restoration of anormal blood pressure (Pickering and Heptinstall,I953). In other cases electrolyte abnormalitiesmay dominate the clinical picture. Cases of so-called 'salt-losing nephritis' presenting with aclinical picture similar to Addison's disease arealmost always examples of chronic pyelo-nephritis(Enticknap, 1952). Inability to acidify the urineleads to cases of renal tubular acidosis usuallyassociated with hypercalcuria causing rickets and
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from

December 1954 MILNE: The Classification and Prognosis of Nephritis and Allied Renal Diseases 645
osteomalacia (Albright et al., 1946). Cases show-ing a disproportionate loss of potassium maypresent with attacks of hypokalaemic paralysissimilar to those seen in familial periodic paralysis(Evans and Milne, 1954). Any combination ofthese several defects of electrolyte reabsorptionmay be seen in a single case and no convincingexplanation has been offered to account for thisdifferential effect of pyelo-nephritis on renaltubular function. Other cases of chronic pyelo-nephritis may present with insidious renal failurewith or without hypertension. The reason whyincrease of blood pressure occurs in some cases ofthe disease and not in others is likewise a completemystery.The prognosis in pyelo-nephritis is dependent
on whether the infection can be controlled, onthe degree of renal impairment as measured byinulin or urea clearance and on the level of theblood pressure. In all varieties of nephritis, casesassociated with severe hypertension show a morerapidly progressive course to terminal renalfailure. Some cases of chronic pyelo-nephritis inwhom the infection is well controlled and with anormal blood pressure may survive for many yearseven although there is moderately severe uraemiathroughout.Chronic Nephritis
All of the various types of renal disease dis-cussed above may terminate in a stage of chronicnephritis with uraemia. Cases differ especiallywith regard to associated oedema or hypertension.Some cases of the nephrotic syndrome die ofuraemia without losing their oedema, whilst othersdevelop polyuria and a salt-losing rather than asalt-retaining state, with complete loss of oedema,before death from uraemia finally occurs. Uraemiawithout hypertension is an insidious and slowlyprogressive condition, the main evidence of thedisease being normochromic anaemia and polyuria.When there is associated hypertension the clinicalpicture is much more acute and is dominated bysymptoms and signs due to the hypertension alone,e.g. severe headaches, papilloedema and retinitisleading to loss of visual acuity and left ventricularfailure. Other causes of renal failure have to beconsidered in the differential diagnosis, e.g.malignant essential hypertension, multiple myelo-matosis and any condition causing chronic hyper-calcuria. If the case is seen for the first time atthis stage, diagnosis is usually dependent on aclear and accurate history. The single mostimportant feature in assessment of the prognosis isthe level of the diastolic blood pressure.Conclusion
Classification of nephritis has now reached a
reasonably rational state, but nomenclature isstill not satisfactory. The division of primaryglomerulo-nephritis into two separate types isclearly necessary, but indefinite retention of theterms 'Type i ' and 'Type 2' is probably un-desirable. These terms were chosen by Ellis(I942) as being non-committal with regard toaetiology. They have never been widely adoptedby American and Continental clinicians whousually require an explanation before understand-ing them. In addition, these names are not inaccordance with the general nomenclature ofdisease. Generally acceptable alternative namesare required, however, before they can be dis-carded since they have the great advantage ofcovering the whole of the disease process frominception to resolution or death. Whilst thegreat majority of cases of primary glomerulo-nephritis can be placed accurately into one or theother group, there is the occasional case which isdifficult to classify and which shows features ofboth. The irreverent have been tempted to termthese cases ' Type one point five.'
AcknowledgmentsThanks are expressed to Professor J. McMichael
and Dr. C. V. Harrison for advice, to Dr. C. E.Newman and Dr. C. L. Cope for permission tomention cases under their medical care and to Dr.C. V. Harrison for permission to reproduce themicro-photograph.
REFERENCES'ALBRIGHT, F., BURNETT, C. H., PARSON, W., REIFEN-
STEIN, E. C. and ROOS, A. (1946), Medicine, 25, 399.'BARNETT, H. L., FORMAN, C. W. and LAUSON, H. D.
(1952), Adv. Paediat., 5, 53.3BARNETT, H L., SIMONS, D. J. and WELLS, R. E. (1948),
Amer. .. Med., 4, 760.'BROWN, L. (1916), Brit. med. .7., 2, 723.5BRUCK, E., RAPOPORT, M. and RUBIN, M. I. (I954), 7.
clin. Invest., 33, 699.:CHINARD, F. P., LAUSON, H. D., EDER, H. A., GREIF,
R. L. and HILLER, A. (1954), J. clin. Invest., 33, 621.'DAUGHERTY, G. W. and BAGGENSTOSS, A. H. (I950)
Arch. int. Med., 85, 9oo.ODAVSON, J. and PLATT, R. (I949), Quart. J. Med., (n.s.), I8,
I49.'DEROW, H. A., SCHLESINGER, M. J. and SAVITZ, H. A.
(I939), Arch. int. Med., 63, 626."0ELLIS, A. (1942), Lancet, i, i."ENTICKNAP, J. B. (1952), Lancet, ii, 458."2EVANS, B. M., and MILNE, M. D. (I954), Brit. med. .., in press."3GALAN, E. (I949), Amer. Y. Dis. Child., 77, 328."GITLIN, D. and JANEWAY, C. A. (I952),.7. clin. Invest., 3I, 223."HAMILTON, M., PICKERING, G. W., FRASER ROBERTS,
J. A. and SOWRY, G. S. C. (I954), Clin. Sci., 13, I."HARRISON, C. V., MILNE, M. D., SEAL, R. M. E. and
VENNING, G. R., to be published."IVERSEN, P. and BRUN, C. (I95I), Amer. .7. Med., II, 324."8KARK, R. M. and MUEHRAKE, R. C. (I954), Lancet, i, 1047"9KELLETT, C. E. (1952), Lancet, ii, 9I I."°KEMPE, C. H., OLMSTED, R. W. and CURNEN, E. C. (ig95),
Pediatrics, 8, 393.2"KIMMELSTIEL, P. and WILSON, C. (I936), Amer. J. Path.,
12, 83.22LAGRUE, G., MOZZICONACCI, P. and VIALATTE J. (I954),
Ann. de Med., 55, I96.References continued on page 654
C2
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from

654 POSTGRADUATE MEDICAL JOURNAL December 1954
mucus secretion. I wonder whether this changecannot rather be related to the malnutrition fromwhich he suffered. May not this be a hypo-proteinaemic fatty change with fibrosis ? I thinkthat the degree of bile duct proliferation is notexcessive for that. The presence of mucousglands in the small bile ducts in the liver is notusually accepted, though of course the largerducts secrete mucus. If there was a mucusblockage of larger ducts then I would expect moreevidence of bile retention. There is a recentpaper (Webster and Williams, I953) describingfive children dying with fibrocystic disease, andhaving cirrhosis of the liver; they all showed muchthe same picture as this patient but there was noevidence of abnormal mucus retention. Andfinally I would just like to ask if Dr. Bodian couldgive us any idea whether he thinks this is anabnormal mucus which is secreted, or whetherthere is an abnormality in the enzyme whichdestroys mucus ? I think we discussed this withDr. Elmes last time we conferenced a case ofmucosis.
Professor Dible: Could I ask Dr. Bodian onequestion-can he relate the lack of sexualdevelopment to this condition ?
Dr. Lennox: I guess that if Dr. Russell Fraserwere here, he would say that it was simply theresult of prolonged malnutrition-that you wouldget it in any long-standing chronic illness.
Dr. Cope: He had steatorrhoea surely.Dr. Bodian: May I answer Professor Dible's
question first ? We have certainly *seen thisinhibition of sexual development in other condi-tions of chronic malnutrition, such as for instanceHirschsprung's disease, when the patient livedlong enough. I don't think it is specific for thisparticular condition.With regard to what Dr. Sherlock said, I am
rather reluctant to take issue with such an eminentexpert on liver pathology. I would have expectedthat if this condition was related to chronic fattychange, it would be diffuse. Yet here it isdemonstrably focal even in this old-standing case.It is a very focal condition and I think you canfind considerable areas of liver not showing thechange at all. Moreover, as I said initally, wehave seen a similar change (though to a lesserdegree with regard to fibrosis) in new-borninfants, and I think that in itself would make anutritional factor unlikely. I am prepared Ithink now to diagnose mucosis on the basis of aliver section alone.
Dr. Scadding: Before we go I must say a wordabout the lung changes. Relatively little has beensaid about them though they were the cause of thispatient's first coming to this hospital and theimmediate cause of his death. However, thediscussion which we have had makes it abundantlyclear that these changes are indeed a manifestationof a much wider-spread underlying disorder.Granted the hypothesis that there is this abnormalmucus secretion which is unduly tenacious,tending to block up ducts and to block bronchiand difficult to expectorate, the whole patho-genesis of the lung changes becomes clear. ButI would like to close with the reflection that thisrelatively rare disease may perhaps emphasize forus the extreme importance of the physico-chemicalqualities of respiratory mucus (and that probablyapplies to the mucus of the alimentary system also)in the causation of a number of much morecommon diseases; and in connection with therespiratory system I am thinking particularly of avery common and disabling condition in thiscountry, chronic bronchitis.(The discussion in this case was considerably
curtailed by shortage of time.)
References continued from page 645--M. D. Milne, M.D., Ch.B., IM.R.C.P.'3LANGE, K., GRAIG, F., OBERMAN, J., SLOBODY, L.,
OGUR, G. and LOCASTO, F. (I95I), Arch. int. Med., 88,433-
'4LYTTLE, J. D., SEEGAL, D., LOEB, E. N. and JOST, E. L.(1938), J. clin. Invest., 17, 631.
"'McCRAE, J. (1913), Tr. A. Amer. Physicians, 28, I94.'"MASUGI, M. (I934), Beitr. path. Anat., 92, 429.'7MUNK, F. (I9I3), Ztschr. f.klin. Med., 78, I.'8PICKERING, G. W. and HEPTINSTALL, R. H. (I953), Quart.
J. Med., (n.s.), 22, I.1'RAASCHOU, F. (I943), Acta Med. Scandinav., II4, 4I4.'°RAASCHOU, F. (1945), Nord. Med., 25, 457.31RAASCHOU, F. (1948), 'Studies of Chronic Pyelonephritis.'
Copenhagen."SRAMMELKAMP, C. H. and WEAVER, R. S. (I953), 7. clin.
Invest., 32, 345-"SRAMMELKAMP, C. H., WEAVER, R. S. and DINGLE, J. H
(1952), Tr. A. Amer. Physicians, 65, I68.3'REIMANN, H. A., SAHYOUN, P. F. and CHAGLASSIAN,
H. T. (I954), Arch. int. Med., 93, 673.
35RUDEBECK, J. (x946), Acta Med. Scandinav., Supp. I73.36RYTAND, D. A. (1948), Amer. J. Med., 5, 548.8?SQUIRE, J. R. (I953), Brit. med. J., ii, 1389.38STAEMMLER, M. and DOPHEIDE, W. (1930), Virchow's Arch.
f. path. Anat., 277, 7I3.V3STICKNEY, J. M. and KEITH, N. M. (1940), Arch. int. Med.,
66, 643.40SWANN, R. C. and MERRILL, J. P. (I953), Medicine, 32, 2I5."THINGSTAD, R. (i95i), Acta Med. Scandinav., x40, I.42VALLERY-RADOT, P., MAURIC, G., WOLFROMM, R. and
GUIOT, G. (I942), Bull. et Mem. Soc. Med. hop. Paris., 58,96.
'3VOLHARD, F. and FAHR, T. (1914), Die Brightsche Nieren-krankenheit. Berlin.
"4WEINSTEIN, L., BACHRACH, L. and BOYER, N. H. (1950),New Engl. J. Med., 242, I 002.
45WHITE, J. C. (I949), J. Amer. med. Ass., 139, 376.46WILSON, V. K., THOMSON, M. L. and HOLZEL, A. (1952),
Brit. med. J., i, 358.
by copyright. on M
ay 10, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.350.640 on 1 D
ecember 1954. D
ownloaded from