Embed Size (px)
Citation preview

Sm. Sci. Med. Vol. 25, No. 6, pp. 589-598, 1987 Printed in Great Britain
0277-9536/87 $3.00+0.00 Pergamon Journals Ltd
SECTION D
THE CHANGING ROLE AND LEGITIMATE
OF EPIDEMIOLOGY: COMMUNITY-BASED
PROGRAMMES
BOUNDARIES
PREVENTION
JAAKKO TUOMILEHTO’ and PEKKA PUSKA?
‘Department of Epidemiology and ‘Department of Epidemiology, National Public Health Institute, Mannerheimintie 166, 00280 Helsinki. Finland
Abstract-Epidemiology is the basic science of public health. It combines medical and social sciences, both of which are developing with new inventions. Therefore, the role of epidemiology and its boundaries are also changing over time. An important role of epidemiology is to develop and implement community- based control programmes for major diseases in the community. Such programmes are essential for large scale public health policy. It is necessary that epidemiological research can as freely as possible test new methods of disease prevention and health promotion. The first community-based control programme for cardiovascular diseases, the North Karelia Project is reviewed against this background. At present, it is still possible to define the boundaries of epidemiology geographically and culturally, but in the future, however, it will become more difficult. There is no doubt that epidemiology will remain as the basic science of public health but the scope of public health problems are growing much wider. These include the prevention of the final epidemic-the destruction of our planet by nuclear bombs. In the control of the existing epidemics and in the prevention of new ones the boundaries of epidemiology cannot stay rigid but they must be changing as new facts about the emerging public health problems are identified.
INTRODUCTION
The theory, practice and relationship of epidemiology have always been deeply influenced by social, politi- cal, economical and cultural environments and their developments. Many definitions of epidemiology have been presented during the past 50 years [l]. Epidemiology, often described as the basic science of public health, is the science on health of human populations, and thereby it can be regarded a social science. Thus, when epidemiology combines medical and social sciences, there is a natural need to discuss the boundaries between these disciplines.
Traditionally, epidemiology has been associated with disease prevention and the Oxford dictionary defines epidemiology as “that branch of medical science which treats of epidemics” [2]. The term epidemic can be replaced with the phrase “major public health problems”. Simplified illness-oriented or determinant-oriented outlooks which many epi- demiologists use in their routine work do not high- light the role of epidemiology as a force in the evaluation of human populations and their social organizations [3]. This point was well made by Frost in 1936: “Epidemiology at any given time is some- thing more than the total of its established facts. It includes their orderly arrangement into chains of inference which extend more or less beyond the bounds of direct observation” [4].
The discipline of epidemiological research has been developed as a scientific discipline to find the facts and ‘absolute proofs’. However, when large devel- opment programmes or reorganizations are imple- mented in the society, these “hard scientific facts and proofs” have had little to do with the major decisions
taken-this is true for African, American, British, Chinese, Finnish, French, Soviet and all other so- cieties. Therefore, referring to many debates in public health today one may want to raise questions, such as: “Have epidemiologists not provided enough facts on the harmful effects of certain issues like smoking?” or “Does the evidence fall short of proof to recom- mend the reduction of saturated fat intake to prevent coronary heart disease?” or “Is the research done in the way that its results are not understandable to the decision makers?” or “Has epidemiological research too often been restricted to the biological inferences disregarding social organization and administrative structure of the population studied?” or “Has the research been directed to wrong areas in an illusion that certain simple measures would solve major pub- lic health problem of multifactorial diseases?” This usually relates to the fact that more funds are allo- cated to find cure (or new drugs) than to find clues to prevention of diseases like diabetes, cancer, hyper- tension etc.
Despite these and other similar questions there is light at the end of the tunnel. Community-based programmes have effectively controlled most severe infectious diseases in the developed world, and the eradication of smallpox has taken place. Similar kinds of community based programmes have now been shown to be effective in the prevention of major modern non-communicable diseases [5-71.
The community-based strategy to prevent major public health problems such as cardiovascular dis- eases has clearly underlined the need to define the legitimate boundaries of epidemiology as a public health science and discipline [7-91. In such public health endeavours the uses of epidemiology must be
589 s s M *W-r

590 JAAKKO TUOMILEHTO and PEZKKA PUSKA
considered both from the scientific and adminis- trative point of view. Unfortunately, it is more often the lobby of scientists reluctant to agree with recom- mended changes to promote disease prevention, who argue that the evidence is less convincing than other members of society who are usually more ready for action. At this point scientific proof (or lack of it) turns into political discussion and leads to decision making. A decision not to start preventive action on a major public health problem is never value-free.
In this article we describe the role of epidemiology in community-based prevention programmes for car- diovascular diseases. This will be done by reviewing the scientific framework of such programmes and by discussing the basic strategies of the implementation of a programme in the community. Experience over I5 years of the North Karelia Project, the first community-based control programme for cardio- vascular diseases [7], has added much to under- standing the uses of epidemiology as a public health science.
USES OF EPIDEMIOLOGY IN COMMUNITY-BASED PREVENTION PROGRAMMES
It may seem unecessarily repetitious to mention that epidemiology is the backbone of such pro- grammes. In his recent excellent lecture “Epi- demiology and the art of the soluble” [IO] Marmot illustrated the views of Sir Peter Medawar who wrote [I I]; “Good scientists study the most important problems that they think they can solve. No scientist is admired for failing in the attempt to solve problems that are beyond his competence.”
Although a full concensus on causal links between health habits and disease are lacking-as it may always be-we have to act on the best currently available knowledge. This point is further reinforced by the magnitude of the problem and the realization that doing nothing is also a decision. A decision to await ‘final proof’ cannot help the great number of people in our society who suffer premature death or major disability. The first great achievements of primary prevention, the control of communicable diseases emphasized the importance of the environ- ment and were, thus, not based on ‘final proof’ of the natural course of the disease in the human body. In spite of the gaps in our knowledge, at present we understand only a few other non-communicable dis- eases as well as we understand the aetiology of coronary heart disease and stroke.
The history of public health is full of examples of successful actions that are not based on a full knowl- edge of the pathogenesis and aetiology of the disease concerned. Success has been often based on effective intervention on some parts of the causal chain that lead to severe manifestations. Carefully evaluated community programmes form an important link be- tween basic laboratory and clinical research and the large-scale application of public health programmes in society. These programmes can thus diminish our uncertainty concerning the effectiveness of such ac- tion, inform us about effective use of the existing resources (service and other community resources), and tell us about other possible consequences associ- ated with such interventions. Therefore, carrying out
a carefully evaluated community programme like the North Karelia Project [5, 71 serves not only its target area, but also as a model for testing the approach in wider applications.
The field nature of a community programme pre- vents the experimental control over many variables. The researcher is thcreforc not able to test specific epidemiological or behavioural hypotheses rigorously [7, 121. Rather, a community study tests a complex yet practical programme based on previous theory and of such a nature that it could be applied else- where, if the results demonstrate success. Thus the limited ‘internal validity’ is compensated by greater ‘external validity’ of the results, i.e. validity for use in real-life circumstances.
One of the major principles of the ‘demonstration’ or ‘pilot’ programme is that intervention is well conceived and implemented as a planned, systematic programme. The programme contents are determined by existing medical, epidemiological, behavioural, and social knowledge applied intelligently and adop- ted to the intervention community setting. Evaluation includes both continuous monitoring of progress and formative evaluation to guide the programme and comprehensive summative evaluation to assess over- all results. Several policy choices are available for the prevention and control of cardiovascular diseases [13]. These include: (1) population strategy, i.e. con- trolling the causes of high or increasing incidence; (2) high-risk strategy, i.e. screening for and treating the precursors of the disease; (3) screening for the early stages of the disease and secondary prevention of known cases with cardiovascular problems.
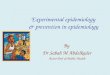
The population strategy of prevention aims to shift the distribution of risk factors towards lower levels. In the history of public health there have been many successful examples of the implementation of such mass environmental control methods, but the idea is still relatively new with regard to modern public health problems such as cardiovascular disease, can- cer and diabetes. Community strategy assumes that the magnitude and nature of the problem precludes a simple, externally initiated solution. This means to many scientists a warning sign. Even some epi- demiologists find it uneasy to accept the fact that cardiovascular diseases can be controlled and pre- vented although not all aspects of the patho- physiology of the disease are known. However, any knowledge about the natural course of the disease must be reviewed comprehensively in order to see the main issues on which the foundations of a community-based prevention programme can be laid. Figure I shows the precursors and stages of the natural course of developing cardiovascular disease [7]. The disease outcome is modified by individual host factors (genetic and others). Environmental and behavioural exposures result in undesired biological changes leading to clinical manifestations of cardio- vascular disease.
Effective community programmes for disease pre- vention imply simultaneous consideration of all or most scientific disciplines that are relevant to the natural course of the disease. With regard to cardio- vascular disease this means, first of all, the broadest possible application of epidemiology, taking into account issues related to (i) planning, (ii) evaluation
The changing role and
+---_---
-Sociology anthropology -
- Social psychology - - +
P Communication P
legitimate boundaries of epidemiology 591
Epidemiology > ------ Clinical medicine b
Environment --social -physical r-l e.g. *Media influence
*Cultural norms l Peer influence l Media influence l Social networks *Opinion leaders *Climate l Dietary customs l Food marketing l smoking policy l liealth services
- -Nutrition ,
Individual behaviours I eg -Smoking
l Diet I
l Adherence to
Biological risk factors aBlood lipids .Blood pressure .Fitness level l Body weight
Clinical disease (atherosclerosis) .Coronarv disease aStroke
Fig. 1. Precursors and sequence of factors leading to cardiovascular disease (coronary heart disease and stroke). The major disciplines needed for effective community-based research in cardiovascular disease are listed above. The traditional scope of each discipline is given in the solid portion of the line. The dotted portion of the line depicts the less common extension of the particular discipline to broader aspects of
the related components [7].
of community health education programmes, (iii) planning regulations for environmental modification, and (iv) planning and evaluation of health services for prevention and control of cardiovascular diseases. A wide variety of scientific and administrative prob- lems of such programmes are addressed by epi- demiological research. However, it is not only epi- demiological skills and methods that are needed for community-based prevention programmes but an interdisciplinary approach is required in their plan- ning, implementation and evaluation.
Clinical and epidemiological knowledge are used to identify the existing health problems and to priorize in choosing health objectives based on biological inferences in the natural history of the disease. The medical and epidemiological framework is also needed to estimate the potential of various ap- proaches in reducing disease rates in the community by modelling the different approaches. We have
RlSK factor High risk strategy Population strategy _. change:
Achieved GoaL IdeoL Achieved Goal Ideal 0
-aoJ I
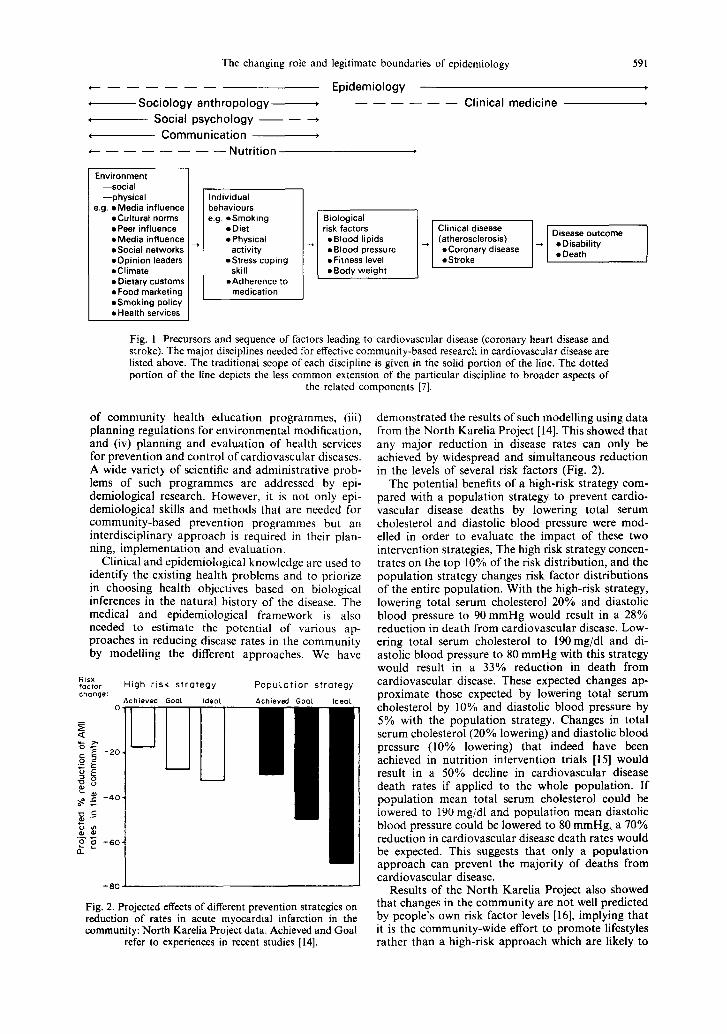
Fig. 2. Projected effects of different prevention strategies on reduction of rates in acute myocardial infarction in the community: North Karelia Project data. Achieved and Goal
refer to experiences in recent studies [14].
demonstrated the results of such modelling using data from the North Karelia Project [ 141. This showed that any major reduction in disease rates can only be achieved by widespread and simultaneous reduction in the levels of several risk factors (Fig. 2).
The potential benefits of a high-risk strategy com- pared with a population strategy to prevent cardio- vascular disease deaths by lowering total serum cholesterol and diastolic blood pressure were mod- elled in order to evaluate the impact of these two intervention strategies, The high risk strategy concen- trates on the top 10% of the risk distribution, and the population strategy changes risk factor distributions of the entire population. With the high-risk strategy, lowering total serum cholesterol 20% and diastolic blood pressure to 90mmHg would result in a 28% reduction in death from cardiovascular disease. Low- ering total serum cholesterol to 190mg/dl and di- astolic blood pressure to 80 mmHg with this strategy would result in a 33% reduction in death from cardiovascular disease. These expected changes ap- proximate those expected by lowering total serum cholesterol by 10% and diastolic blood pressure by 5% with the population strategy. Changes in total serum cholesterol (20% lowering) and diastolic blood pressure (10% lowering) that indeed have been achieved in nutrition intervention trials [I51 would result in a 50% decline in cardiovascular disease death rates if applied to the whole population. If population mean total serum cholesterol could be lowered to 190 mg/dl and population mean diastolic blood pressure could be lowered to 80 mmHg, a 70% reduction in cardiovascular disease death rates would be expected. This suggests that only a population approach can prevent the majority of deaths from cardiovascular disease.
Results of the North Karelia Project also showed that changes in the community are not well predicted by people’s own risk factor levels [16], implying that it is the community-wide effort to promote lifestyles rather than a high-risk approach which are likely to

592 JAAKKO TUOMILEHTO and PEKKA PUSKA
have impact on the population rates of cardio- basis for a model that unifies these approaches in a vascular diseases. community-based health programme [7].
The behaviour change approach SOCIAL SCIENCES IN COMMUNITY-BASED
PREVENTION PROGRAMMES FOR CARDIOVASCULAR DISEASES
Behavioural and social knowledge is needed to design the actual programme contents and activities. Also, the evaluation of health care and its adminis- tration for the programme deals with sociological inferences that are not within the scope of epi- demiology. Lilienfeld argued that only characteristic distinguishing epidemiology from medical sociology is that epidemiology is concerned with biological inference whereas sociology is not [l]. According to his definitions, community-based control pro- grammes need both of these disciplines because such programmes require both biological and social frameworks.
This socio-psychological approach deals with the determinants of an individual’s behavioural changes, and is based on Bandura’s work on the process of learning [20]. New behaviours tend to originate, at least on trial bases, from chance exposure to powerful models; external and self-enforcement and cognitive control are the consequent determinants of continued new behaviours. The planning and evaluation of such a prevention programme should include the follow- ing key steps to help individuals to modify their behaviour:
I. Improved preventive services to help people to identify risk factors and to provide appropriate atten- tion and services.
Recently, results of three major multifactorial stud- ies on primary prevention of cardiovascular diseases were published [17-191. Specific features of these studies were that only medical and epidemiological aspects were taken into account in their study design. The random allocation of subjects into the inter- vention and control groups was applied in these studies strictly in a traditional medical sense. Un- fortunately, such an approach leads to the exclusion of behavioural and social aspects which means that preventive actions are ultimately limited to a single axis only, i.e. between the agents (risk factors) and the host (people). However, many of the great achieve- ments in public health have been made possible by placing a major emphasis not on agents or host but on the environment. Against this background it is not surprising that this ‘well-controlled’ randomized trials on individuals have added only a little to our knowledge about the prevention of cardiovascular disease.
2. Information to educate people about the re- lationship between behaviours and their health.
3. Persuasion to motivate people and to promote the intentions to adopt the healthy action.
4. Training to increase the skills of self- management, environmental control, and necessary action.
5. Social support to help people to maintain the initial action.
6. Environmental change to create the oppor- tunities for healthy actions and improve un- favourable conditions.
7. Community organization to mobilize the com- munity for broad-ranged changes (through increased social support and environment modification) to support the adoption of new lifestyles.
The communication -behaviour change approach
The agents (risk factors) of cardiovascular disease are largely determined by social forces and other environment factors. Therefore, any major progress in influencing disease rates has to deal with these matters. The task of influencing people’s behaviours and lifestyles is, however, the domain of the social and behavioural sciences. More generally, it has become evident that many health goals cannot be realized through the health sector alone. Im- provements in cardiovascular health, for instance, must be perceived as a multisectoral responsibility in which several other sectors would need to collaborate with the health sector. Such intersectoral action can often best be promoted at the grassroot level, where people who are directly affected are able to mobilize the efforts of relevant sectors for the solution of health problems in question. However, at the higher level of various organizations, and especially among different scientific disciplines, it is difficult to achieve the level of intersectoral cooperation which is satis- factory. This can lead to defining the boundaries of different disciplines very strictly which then forms a major obstacle to the actions necessary in disease prevention.
The task of introducing new behaviours in the community is basically achieved by communication: mass communication and interpersonal commu- nication. A project communicates its messages through mass media to the population, in addition to its direct communication to various community lead- ers. In addition to Bandura’s social learning theory, the classical communication-persuasion model of McGuire [21], its modification by Flay et al. [22], and the belief-attitude-intention model of Ajzen and Fishbein [23] provide well-documented theoretical background for this approach.
The innovation -diffusion approach
New lifestyles are innovations that diffuse with time through the natural networks of the community to members of the given social system. This diffusion, causing social change, occurs through commu- nication over time. The innovation-diffusion theory argues that mass media are more effective in creating knowledge of innovations and are useful for ‘agenda- setting’ purposes, while interpersonal channels are more effective in actually changing attitudes and behaviours. The innovation process occurs in fOUr stages (note the similarity to the previous approach): (a) knowledge, (b) persuasion, (c) decision, and (d) confirmation.
The following four theoretical, somewhat over- lapping frameworks for behavioural change form the
Three main types of innovation decisions have been suggested: (a) optional decisions (made individ-

The changing role and legitimate boundaries of epidemiology 593
ually), (b) collective decisions (made by concensus), and (c) authority decisions (made by a superordinate power).
These central principles of innovation-diffusion theory have been developed mainly by Rogers [24]. The theory is well supplemented by the classical idea of the two-step flow of new ideas and attitudes through opinion leaders [25]. This simplified model holds that new ideas, often originating from mass media, are mediated and modified by certain opinion leaders, and most people are then influenced mainly by interpersonal contacts with these opinion leaders. Opinion leaders can be identified through their par- ticular expertise or position, or they can be informal and undistinguishable by formal criteria. Opinion leaders can either favour or resist the innovation- diffusion process.
The community organization approach
Broad-ranged changes in the community can be achieved ultimately only through existing community structures. Every community has a complex network that exercises great influence over individual behav- iour and lifestyle. The community organization ap- proach emphasizes efforts to influence individuals through changing organizations to meet the desired ends. The concept of community organization in- volves both community self-development (the com- munity initially detecting a problem, and organizing itself to cope with it) and the outside influences needed to promote the reorganization.
The community petition that initiated the North Karelia Project provided a favourable subjective cli- mate for community reorganization [26,27]. How-
ever, the Project team provided the external impetus and resources for change in the community. In doing so, the principles of persuasion and of the change agent’s role have been of central importance. The impact depends largely on the degree to which exist- ing community organizations find the proposed ac- tions fit their particular needs. It is therefore im- portant for success in community self-development that the programme offers incentives for the proposed collaboration.
The North Karelia Project team tried throughout the programme (but with greatest intensity in the beginning) to have close contact with a great many representatives of community organizations [26]. The team worked intensively with the representatives of the mass media (newspapers, radio), with people of health and other services (administrators, doctors, nurses, teachers, social workers, schools, teachers), with business leaders (dairies, sausage factories, bak- eries, groceries), with key people in voluntary or- ganizations (heart association, housewives’ organ- ization, labour organizations, sports organizations), and with local political decision makers (county and municipal leaders). The team tried to show these organizations practical, feasible ways to collaborate, while recognizing each organization’s particular needs. The aim was that such changes would ulti- mately influence behaviour in the community.
A untjied model
The approaches described above have been unified in Fig. 3 to show the behavioural/social model of community intervention found most relevant to the North Karelia Project [7]. External input from the
Communication factors Process of
behaviour change Community factors
. Channel(s) +
. Exposure +
a Importance relevance + source
l Simple concepts 4
. Match local culture
l Teaching health + behaviour skills via demonstration guided practice
0 Cues
/” l Self efficacy training
\
Attention
II
- .Audience targets (segmentation)
Motivation t) . Involvement of
u opinion leaders
Comprehension l Recruitment training
u of early adopters
Learning information
u J Attitude change (persuasion) t* . Increased relevant
u interpersonal contacts
Health skills learning u l Increased opportunity for discussion feedback
U
a Community events
Health skills performance / (target days contests locally
initiated activities etc.)
U ‘I
a Social support practical help
. Environmental factors
Maintenance of performance s
of learned health skills t* *Social support K
L l Community organization
Fig. 3. Model of the communication process in community intervention to induce behavioural change, as used in the North Karelia Project [7].

594 JAAKKO TUOMILEHTO and PEKKA PUSKA
Project affected the community both through mass media communication to the population at large (where its effect was mediated through interpersonal communication) and even more so through formal and informal opinion leaders acting as change agents to influence various aspects of community or- ganization. This two-pronged emphasis was aimed at increasing knowledge, at persuasion, at teaching practical skills, and at providing the necessary social and environmental support for the performance and maintenance of new behaviours ultimately led to a more favourable risk factor profile, reduced disease rates, and to improved health.
ILLNESS CAUSATION AND PREVENTION
Epidemiology, on the one hand, is the study of the distribution and determinants of disease frequency in human populations [28] providing us with methods of defining factors that are important in the aetiology of the disease. On the other hand the role of epi- demiology, as the basic science of preventive and community medicine, implies distinctively different approaches than in the study of causal relationships. Research into the aetiology of cardiovascular disease has for a long time demonstrated the importance of socio-economic factors in the natural course [29-331; to what extent this contribution is independent and to what extent it is due to interactions with other determinants varies between studies. The lack of commonly agreed definitions and models to charac- terize these factors-low socio-economic status, so- cial inequality, poor social support-has been the major obstacle in research of disease causation until recently. In such socio-epidemiological research the need for multidimensional analyses of phenomena of social inequality are well recognized and conceptually more advanced approaches have been developed [33,34]. This lack of multidimensional analyses is a result of the difficulties epidemiology has had to suggest appropriate biological inferences and of the limited interest of social scientists to develop concep- tually stronger approaches in this area without more specific requests from the health sector. This illus- trates the poor definitions of clear disciplinary boundaries between epidemiology and the social sci- ences. In disease causation the original requests for such interdisciplinary research issues are basically the responsibility of the health sector. It is the role of the epidemiologist to express the actual needs for more information about certain social and behavioural indicators that could be used in studying the aetiology of the disease. However, it is the task of the social scientist to develop, validate and update these indicators.
COMMUNITY INVOLVEMENT IN PREVENTION OF CARDIOVASCULAR DISEASES
During the past decade it was commonly under- stood that the prevention and control of major public health problems should be designed and carried out through existing health services, with an emphasis on primary health care development. However, it was also realized that the actual implementation of pri- mary health care is a complex issue which provides
several challenges. Efforts are being made to develop this kind of approach in order to control major public health problems. As the multifactorial origin of car- diovascular disease became obvious and major risk factors identified, and as the close link between risk factors and lifestyles and environment in the commu- nity became apparent, the next step, the involvement of an entire community in an intervention pro- gramme, was at hand [7,9, 131. The major difficulty, however, was that the medical profession has not fully understood that such programmes cannot be based on epidemiological and medical inferences only, but that it is necessary to involve the commu- nity itself in the action.
Community involvement in the development of health services includes the following:
I. Education of the community so that health problems can be identified and understood.
2. Organization of the community so that group decisions may be taken on health and the community may become self-reliant and accept responsibility for health measures.
3. Development of a mechanism that allows the community to decide on resource allocation for pri- ority problems. These priority problems may not be health problems and one has to accept the multi- sectoral nature of the process.
4. Involvement of the community in a partnership for the planning and implementation of health or health related projects.
Ideally, community involvement starts with the individual, who learns that he can exercise some control over his own health. This leads to community awareness of health and diagnosis of health or health- related problems. At this stage technical and manage- rial support can come from outside the community to develop activities that will link up with government programmes.
The community involvement is a strategy of imple- menting health care with total coverage of the popu- lation, with active participation of the community, with organizing resources of the different sectors and coordinating them, using technologies to improve and promote the health of the population in ways relevant to the problems identified. The goal is that the community itself has no longer to be taught to accept or cooperate with given health services but to mobilize community resources in terms of mo- tivation, behaviour and organizations. The North Karelia Project was the first attempt to use commu- nity involvement in the prevention of cardiovascular disease [27]. Therefore, it can be also used as an example of the role of epidemiology in the action in the community. This will be discussed below.
I. Education of the community so that the medical problem was ident$ed and understood
Ideally, community involvement in health pro- motion starts with individuals who learn that they can and should exercise some control over their health. The North Karelia Project had such an ini- tiative, based on the epidemiological inferences. The findings from mortality statistics and prospective epidemiological studies [35] provided a sufficient data base, a prerequisite for any educational action. It is

The changing role and legitimate boundaries of epidemiology 595
not methods of collecting data that is different be- tween epidemiologists and social scientists but it is the inferences, the uses of the findings where the main differences may exist. When the role of social scien- tists is to emphasize the importance of the devel- opments needed in social, educational and or- ganizational aspects of health and health care, the role of epidemiologists is to draw attention to the concept of risk and to the biological plausibility of the findings. Both are important and complementary to each other, and both of them are essential for programme development.
2. Initiative for action
The provincial governor, all North Karelian mem- bers of the national parliament, and several represen- tatives of official and voluntary organizations in the area signed in 1971 a petition for national aid to reduce the cardiovascular problem in North Karelia. The paper noted the very high cardiovascular disease frequency in the area and proposed that national authorities and organizations concerned “should ur- gently undertake efficient action to plan and imple- ment a programme which would organize and finance general health information to the public, necessary basic research, and individual health education to reduce this greatest public health problem of the province.” This petition was the necessary start of the community involvement that dictated the future ap- proach of the programme. Such initiatives have to be discussed with experts beforehand since opinions about the proposed action will vary according to discipline. For an epidemiologist with classical ana- lytical training the initiative for action could have meant a new prospective or case-control study on the causes of the disease.
3. Community preparation to become self-reliant and accept responsibility for control of cardiovascular diseases
At the planning stage of the Project, a working group reviewed the situation through contacts with national and international experts and in close coop- eration with local health services. The need for technical and managerial support from outside was found necessary in order to priority problems identified, to identify the resources and develop a further plan of action required. It was concluded that a practical, service-oriented programme serving the whole community was required rather than only to improve clinical services or to continue with obser- vational epidemiological surveys.
In the planning phase it was considered important to strengthen managerial capabilities for planning and organizing community activities; community in- volvement included the following steps:
1. Development of leadership in the community. 2. Development of a community organization able
to take decisions on health matters dealing with cardiovascular disease control in the area.
Through this planning work, both members of the community and health workers were prepared-the former became aware of the special health problem and the potential for development through commu- nity action; the latter learned about the real needs of
the community and their changing nature. Although the initial petition was seriously asking for national help to overcome the urgent cardiovascular disease problem, it was found that the province could be self-reliant, taking the major responsibility for the planned cardiovascular disease control programme.
This was the phase where the importance of epi- demiological inferences were especially valuable. The concept of risk factors, their synergistic effects on disease outcome and the understanding of ‘popu- lation attributable risk’ rely heavily on epidemiology. These facts must be explained to the community so that they understand why they need to become self-reliant and why they should accept responsibility for implementing a community-based prevention strategy. This cannot be done by a clinical cardi- ologist nor a social scientist without epidemiological reasoning about these disease phenomena in the community.
4. Community action to impIement the planned cardio - vascular diseases control activities
Community action in this sense, because of the need for lifestyle changes, needs both: (i) commu- nication with health services, and (ii) communication with other sectors of the community. Most of the preparations in North Karelia were carried out by the community itself and its health service system with the support of the organized project team.
The task of the Project was to strengthen the existing structure for health care within national guidelines to tackle the cardiovascular disease prob- lem. This was done through the preoccupation of the health workers as well as of the community devel- opers and policy makers. In order to try to measure community involvement and action in the Project, the following indicators could be used:
a. Health resource allocation for cardiovascular disease control.
b. Personal health habits of the people. c. Participation of community decision makers in
the management of cardiovascular disease related health services.
d. Communication between the community and the health workers concerning cardiovascular disease control.
e. Activities carried out by the community.
Such community action required the participation of various disciplines, but the health sector and, specifically, epidemiology was the one to take lead- ership through linking health needs in the commu- nity. However, the monitoring of the indicators of progress in community health programmes mainly concerns behavioural and social sciences rather than epidemiological inferences.
TRANSITION OF KNOWLEDGE FROM BASIC RESEARCH INTO COMMUNITY HEALTH POLICY
It is quite obvious that national policy neither exists nor develops on its own. Political decisions with regard to economy, education, employment, food policy, social policy, urban and rural planning have both direct and indirect effects on living condi- tions, and these decisions set the overall stage for the

596 JAAKKO TUOMILEHTO and F%KKA PWKA
health of communities as well as individuals. Delivery of health care plays a major role in setting the direction of disease prevention and health promotion. Health care systems consume a large portion of resources allocated for health policy and representa- tives of health care have significant power for setting plans for health policy.
Disease patterns are changing constantly. Very often the real reasons behind disease trends are poorly understood. A good example of a chronic disease which has been declining virtually throughout the whole world without any systematically planned action is stomach cancer [36]. No clear explanation is available, although many hypotheses exist. However, the decline is relatively slow and treatment of the condition is relatively expensive. Therefore, a policy to undertake no further research on aetiology of stomach cancer and to leave the patients with the disease untreated would be unacceptable. There are many similar major health problems which are slowly declining, for reasons that are unclear, and yet they still cause much burden and suffering to patients and to the community and health care systems.
For most major health problems basic research has several alternative or complementary theories. In western countries the rough estimate of the amount invested in basic research is l/400 of the amount used for health care delivery. A common problem is how to make the best use of this investment to basic research to help in planning disease prevention and health promotion. In this transition epidemiology and the related social sciences have their major roles.
Findings from basic research usually need to go through a long process before they can be effectively adopted into national health policy. At least the following phases can be identified:
1. Hypothesis development. 2. Methods development. 3. Controlled intervention trials. 4. Specific population studies. 5. Demonstration programmes.
The phases 14 are clearly based on epi- demiological reasoning and inferences, whereas in phases 45 the importance of the social sciences is gradually growing and adding significantly to the development of a national health policy. When new public health problems are involved and when large- scale community demonstration programmes are de- veloped one must often move a step further from what are regarded as the legitimate boundaries of scientific disciplines. It is true that the modern medi- cal system deals effectively with episodes of acute illness and with accidents that call for advanced hospital-based biomedical knowlege and technology. However, it is quite clear that the present system is much less effective in delivering health care needed for the prevention and treatment of the predominant chronic diseases. The complexity of the task is in- creased by the multifactorial origin of such diseases, by social factors and unhealthy lifestyles which con- tribute to their onset and by several types of struc- tural and organizational problems in dealing with chronically ill. One major obstacle is that while the technology and medical procedures available for coping with diseases that afflict our populations
today have expanded and improved, the structure of the system has tended to remain in a form determined by medical and social circumstances which were quite different from those that exist today [37]. The system is essentially passive, mainly starting to operate by the initiative of a patient or client. The result seems to be a mismatch between the technology of medicine and the system that delivers health care.
Ideally, public health activities should change with changing technology and social values but retaining the same goals to reduce the amount of disease, premature death, and disease-produced discomfort and disability in the population [38]. In this en- deavour, the legitimate boundaries of medicine are relatively narrow, whereas those for public health and for its basic science, epidemiology, are much broader; Terris has pointed out that medicine is a minor part of public health [39]. Disease prevention in medicine means essentially secondary prevention which is cer- tainly important, but it does not reduce much of the burden of major public health problems in the com- munity although it may reduce the suffering of an individual from an acute illness. The implementation of true primary prevention must be based on epi- demiologic reasoning and its target is the community. Therefore, it is necessary that epidemiological re- search can as freely as possible test new methods of disease prevention and health promotion. Without such freedom, epidemiology prevention and control of new public health problems cannot be dealt with satisfactorily.
THE IMPACT OF EPIDEMIOLOGY ON SOCIETY
By definition, epidemiology as the basic science of public health should have a major impact on health. However, it is clear that epidemiology should have an impact on society. The control of major infectious diseases, called now the ‘first epidemiological revolu- tion’ had great impact on society, not only on health. In the ‘second epidemiological revolution’ which is presently ongoing in dcvcloped countries, the rates of major non-communicable diseases and environ- mental hazards are being reduced [3]. The imple- mentation of this second epidemiologic revolution will require major changes in agriculture, industry and marketing. Potential harmful effects of various exposures in food, drinks, comforts of life are tested by epidemiological methods and the implementation of community-based programme will result in consid- erable reductions in the production of such agents. Effective prevention of environmental hazards and accidents require modifications in manufacturing processes and control of situations or tools that have been found associated with such problems.
The boundaries of epidemiology in this ‘stage of revolution’ are still possible to define geographically and culturally, although much of it is depending on large political and social structures than within one country or its region. It still has basic theory, the main concern of which is on the existing health problems, diseases. This implies active cooperation between clinical medicine and epidemiology. Such a cooperation is particularly important at early stages of programmes but it usually becomes less important later on. Clinical findings are essential in defining

The changing role and legitimate boundaries of epidemiology 591
the natural history of diseases and in assessing the severity of the health problem.
3. Terris M. The changing relationships of epidemiology and society: the Robert Cruikshank lecture. J. oubl.
4.
5.
Hlth Policj 5, 15-36, 1985.
6.
7.
It is interesting to see how the role of cardiology and cardiologists has changed during the last 20 years. In the beginning of the 1970s the cardiologist who wanted to express his/her serious interest in the field of cardiovascular disease actively participated in debates on prevention, carried out epidemiological studies (often without proper expertise) and pre- sumed that they had a leading role in the control of cardiovascular disease in the community. For epi- demiologists of a younger generation it was not easy to get the freedom that the nature and the magnitude of the problem of cardiovascular disease required. Today cardiologists are much more interested in clinical problems and technology related to the heart-for which they have been trained-than in primary prevention, which has been left to epi- demiologists. Clinical medicine has realized that their vested interests are certainly not threatened by epi- demiologists. It is clear that they recognize that effective primary prevention needs full commitment to deal with social and environmental factors and related politics; primary prevention is not a screening campaign, a leaflet to the patients or a talk given to people in the community. An important outcome from a successful community-based demonstration programme is that the boundaries between the epi- demiological and clinical disciplines related to specific health problems become settled. This has happened in Finland where a consensus report on prevention of coronary heart disease was recently produced in full agreement between several scientific disciplines.
8.
9.
10.
11.
12.
13.
14.
Frost W. H. Introduction. In Snow on Cholera (Edited by Snow J.) Hafner, New York, 1936. Maccoby N., Farquhar J. W., Wood P. D. and Alex- ander J. K. Reduction of the risk of cardiovascular disease: effects of a community-based campaign on knowledee and behavior. J. commun. Hlth 3. 10&l 14. Glasuno; I. S., Grabauskas U., Holland W. W. and Epstein F. H. An integrated programme for the pre- vention and control of noncommunicable diseases. A Kaunas report. J. chron. Dis. 36, 419426, 1983. Puska P., Nissinen A. and Tuomilehto J. The community-based strategy to prevent coronary heart disease: conclusions from the ten years of the North Karelia Project. A. Rev. pub/. Hlth 6, 147-193, 1985. Morris J. N. Loses of Epidemiology, 3rd edn. Churchill Livingston, Edinburgh, 1975. Blackburn H. Research and demonstration projects in community cardiovascular disease prevention. J. pub/. Hlth Policy 4, 398421, 1983. Marmot M. G. Epidemiology and the art of the soluble. Lancer 1, 1986. Medawar P. B. The Art of the Soluble, Vol. 7. Methuen, London, 1969. Campbell D. T. and Stanley J. C. Experimental Quasi Experimental Designs for Research. Rand McNally, Chicago, Ill., 1963. WHO Technical Report Series, No. 678, 1982 (Pre- vention of coronary heart disease: report of a WHO Expert Committee). Kottke T. E., Puska P., Salonen J. T., Tuomilehto J. and Nissinen A. Projected effects of high-risk versus population-based prevention strategies in coronary heart disease. Am. J. Epidem. 121, 697-704, 1985.
1c
In the future, epidemiology will have even greater IJ. Enholm C., Huttunen J. K., Pietinen P., Leino U.,
difficulties in defining its boundaries. There is no Mutanen M., Kostiainen E., Pikkarainen J., Dougherty
doubt that epidemiology will remain as the basic R., Iacono J. and Puska P. Effect of diet on serum
science of public health but the scope of public health lipoproteins in a population with a high risk of coronary heart disease. New Engl. J. Med. 307, 85&855, 1982.
nroblems are growing much wider. These will include 16. Salonen J. T., Heinonen 0. P., Kottke T. E. and Puska the final epidemic-rhe destruction of our planet by nuclear bombs. The actions needed are related to drastic reductions in military production and the progressive elimination of nuclear weapons. This movement to avoid the final epidemic might be called 17.
the ‘third epidemiological revolution’ which has, in fact, started already among physicians. It may not be surprising that the most active group in this move- 18. ment within the medical profession are cardio- vascular epidemiologists and cardiologists. This is an example of how successful experiences will lead to broader understanding and willingness to contribute 19, to the overall well-being of society, whatever the problem. As Terris has stated [3]: “Public health 20, workers-and epidemiologists in the first place- have a responsibility to educate both people and 21, governments of our planet on the nature and extent of the social and environmental hazards to human life and health, and on the measures required for their control. This is not an easy task, for we shall inevita- 22. bly incur the opposition of powerful vested interests.” _1
1.
2.
‘3.
REFERENCES 24.
Lilienfeld D. E. Definitions of epidemiology. Am. J. Epidem. 107, 1978. 25. The Compact Edition of the Oxford English Dictionary. Oxford University Press, Glasgow, 1971.
P. Change in health behavior in relation to estimated coronary heart disease risk during a community-based cardiovascular disease prevention programme. In;. J. Epidem. 10, 343-354, 1981. Multiple risk factor intervention trial research group. Multiple risk factor intervention trial: risk factor changes and mortality results. J. Am. med. Ass. 1465-1468, 1982. Wilhelmsen L., Berglund G., Elmfeldt D., Tibblin G., Wedel H., Pennert K., Vedin A., Wilhelmsson C. and Werkij L. The multifactor primary prevention trial in Goteborg, Sweden. Eur. Hith J. 7, 279-288, 1986. Rose G., Tunstall-Pedoe H. D. and Heller R. F. UK heart disease prevention project: incidence and mor- tality results. Lancer 1, 1062-1065, 1983. Bandura A. Social Learning Theory. Prentice-Hall, Englewood Cliffs, N.J., 19771 _ McGuire W. J. The nature of attitudes and attitude change. In Handbook of Social Psychology (Edited by Lindsay G. and Aronson E.), Vol. III. Addison-Wesley, Reading, Mass., 1969. Flay B. R., Ditecco D. and Schlegel R. P. Mass media in health promotion. Hlth Educn Q. 7, 127-143, 1980. Ajzen I. and Fishbcin M. Understanding Attitudes and Predicting Social Behavior. Prentice-Hall, Englewood Cliffs, N.J., 1980. Rogers E. Diffusion of Innovations. Free Press, New York, 1983. Katz E. and Lazarsfelf P. Personal Influence: The Part Played by People in the Flow of Mass Communications. Free Press, New York, 1955.

598 JAAKKO TUOMILEHTO and PEKKA FUSKA
26.
27.
28.
29.
30.
31.
Puska P., Tuomilehto J., Salonen J., Nissinen A., Virtamo J., Bjiirkqvist S., Koskela K., Neittaanmlki L., Takalo L., Kottke T. E.. MBki J.. Sinili P. and Var- vikko P. The North Karelia Project:‘ Evaluation of a Comprehensive Community Programme for Control of Cardiovascular Diseases in North Karelia, Finland 1972-1977. WHO/EURO, Copenhagen, 1981. Tuomilehto J., NeittaanmLki L., Salonen J. T., Puska P. and Nissinen A. Community involvement in devel- oping comprehensive cardiovascular control programs. A case study in North Karelia, Finland. Yrbk Popul. Res. Finland 21, 75-98, 1983. MacMahon B. and Pugh T. F. Epidemiology. Little, Brown, Boston Mass., 1970. Liljefors I. and Rahe R. H. An identical twin study of psychosocial factors in CHD in Sweden. Psychosom. Med. 33, 523-534, 1970. McQueen D. and Siegrist J. Social factors in the eti- ology of chronic diseasi: an overview. Sot. Sci. Med. 16, 353-367, 1982. Rose G. and Marmot M. Social class and coronary heart disease. Br. Heart J. 45, 13-19, 1981.
32. Theorell T. and Floderus-Myrhed B. “Workload” and risk of myocardial infarction-a prospective psycho- social analysis. Int. J. Epidem. 6, 17-21, 1977.
33. Siegrist J., Siegrist K. and Weber I. Sociological con- cepts in the etiology of chronic disease: the case of ischemic heart disease. Sot. Sci. Med. 22, 247-253, 1986.
34. Blau P. M. Inequality and Heterogenity. New York, 1977.
35. Keys A. Coronary heart disease in seven countries. New York. Am. Heart Ass. Monogr. No. 29, 1970.
36. Howson C. P., Hiyama T. and Wynder E. L. The decline in gastric cancer: epidemiology of an unplanned triumph. Euidem. Rev. 8. l-27, 1986.
37. Mead&s A. C. Preventive services: an educational or political issue? Hlth Policy Educn 3, 329-336, 1983.
38. Last J. A Dictionary OfEpidemiology. Oxford University Press, New York, 1983.
39. Terris M. The world need for schools of public health. Wld Hlth Forum 4, 21G-218, 1983.