Embed Size (px)
Citation preview

Journal of Infection (2002) 45: 107±132doi:10.1053/jinf.2002.1022, available online at http://www.idealibrary.com on
CASE REPORTS
The Changing Epidemiology of Infectious Mononucleosis?
M. C. Morris*1,2 and W. J. Edmunds1,3
1Immunisation Division, PHLS Communicable Disease Surveillance Centre, 61 Colindale Avenue, London NW9 5EQ,2Infectious Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, 3Department of Economics,
City University
Infectious mononucleosis is an acute and self-limitedinfection of the lymphatic system caused in over 90% ofcases by a primary infection with Epstein-Barr virus(EBV), a member of the herpes virus group [1]. Infectionduring childhood is usually subclinical, whereas infec-tion of adults results in infectious mononucleosis in 30±75% of cases and can prove severe [2,3]. EBV infection inchildhood is associated with low socioeconomic status,poor hygiene and crowding so that improved housingand decreasing family sizes may have resulted in achange in the epidemiology of EBV and therefore infec-tious mononucleosis [4,5]. To investigate this possibilitywe reviewed historical data of general practitioner (GP)consultations and hospitalisations in England and Walesover thirty years.
Data on age-specific consultation rates for infectiousmononucleosis in England and Wales were obtainedfrom the Royal College of General Practitioners (RCGP)sentinel surveillance reports [6]. The surveillance pro-gramme is based on clinical diagnoses and uses a sampleof practitioners throughout England and Wales whichcurrently covers a population of over 600,000.
Data for the calendar years 1989±1998 wereextracted from the Hospitalisation Episode Statistics(HES, Department of Health) database that records everyinpatient admission to National Health Service hospitalsin England. Cases of infectious mononucleosis wereidentified using the International Classification DiseaseCodes 075* (ICD-9 up until 1995) and B27* (ICD-10from 1996 onwards). The ICD-9 code 075* did not dis-tinguish between different viral causes of infectiousmononucleosis. For consistency, from 1996 onwards theICD-10 code B27* was used which included infectiousmononucleosis from EBV, cytomegalovirus (CMV), otherviral causes and unspecified types. However, in practice
0163±4453/02/$35.00
* Please address all correspondence to: Marianne Morris, CDSC, 61
Colindale Avenue, London NW9 5EQ, UK. Fax: 0044 208 200 7868
E-mail address: [email protected]
most cases (over 95%) were recorded as unspecifiedinfectious mononucleosis (i.e. causative agent notknown). Age and sex specific population denominatorsto calculate incidence rates from 1970±1999 wereobtained from the Office of National Statistics.
When calculating incidence rates we considered onlythe first hospital admission within a calendar year andfirst and new episodes for GP consultations.
Changes in age and sex adjusted consultation andhospitalisation rates over time were investigated usinglinear regression with a spline function to split the con-sultation data into decades (1970s, 1980s, 1990s).Regression coefficients were compared to assess howtrends had altered over time. Consultation data werelogged to reduce the effect of year-to-year variation.
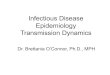
The decline in the average annual consultation ratesfor infectious mononucleosis in England and Wales isshown in Fig. 1. The gradual decline in the overallconsultation rates during the 1970s and 1980s (anaverage of 1±2% per year) accelerated in the 1990s toaround 6% per year when the decline also occurred inadults (Fig. 1). The estimated coefficient was significantlydifferent in the 1990s to those in the previous two dec-ades (F�15.86, p�0.0002 for 1990s versus 1980s;F�21.52, p<0.0001 for 1990s versus 1970s).
Although hospitalisation data were only available fora ten-year period, annual rates approximately doubledduring the 1990s (from 2.6 hospitalisations per 100,000population in 1989 to 4.8 hospitalisations per 100,000in 1998 (Fig. 1)). This increase was highly significant(average annual increase of 5% (age and sex adjusted),95% CI 3±7%) and was concentrated in the 10±24 yearolds (average annual increase for 10±14 year olds of 6%(95% CI 4±8%), 15±19 year olds 11% (95% CI 8±12%)and 20±24 year olds 6% (95% CI 4±11%)).
The data indicates a contrasting pattern of a sig-nificant decrease in GP consultation rates for infectiousmononucleosis, especially in young children, coupledwith a significant increase in the incidence of severe
# 2002 The British Infection Society

0
50
100
150
200
250
300
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
Year
0
1
2
3
4
5A
nnu
al G
P c
onsu
ltat
ion
rate
Ann
ual
hos
pit
alis
atio
n ra
te
GP consult. all ages
GP consult. 0–4yrsGP consult. 5–14yrs
GP consult. 15–44yrsHospitalisations all ages
Figure 1. Annual GP consultation and hospitalisation rates per 100,000 population for infectious mononucleosis over time.
108 Case Reports
cases requiring hospitalisation in teenagers and youngadults. However, are these conflicting patterns to bebelieved? It is possible that these trends are simply areflection of changes in diagnostic practices and consul-tation patterns, though opposing trends from two differ-ent reporting systems makes this explanation less likely.
Changes in the epidemiology of CMV and HSV-1,spread in a similar fashion to EBV, have been observedover recent decades with a fall in the incidence of child-hood infections with improvements in living conditions[7±10]. If a similar change has occurred in the epidemio-logy of EBV, the most likely explanation for the patternsobserved here would be that falling childhood infectionrates have resulted in an increase in the number of teen-agers who are susceptible to a severe primary infection.
Such an epidemiological change could have impor-tant public health implications as the increased declinein consultation rates in children during the 1990s sug-gests that the rise in hospitalisations in teenagers mayaccelerate in the near future.
Given the non-specific clinical diagnosis of infectiousmononucleosis, especially in children with mild symp-toms, and a failure in most hospitalised cases to confirmthe infectious agent; accurate and representative sero-prevalence data for the main causative agents of infec-tious mononucleosis using historical serum banks are
now needed to confirm the shift in the pattern ofinfection.
Acknowledgements
We thank Pauline Kaye for help in extracting and processing thehospital episode data, Nick Andrews for his statistical advice andDr Elizabeth Miller for comments on previous versions of the manuscript.
References
1 Evans AS. Mononucleosis, infectious. Communicable and infectiousdiseases. 433±438.
2 Niederman JA, Evans AS. Epstein-Barr virus. In: Evans AS,Kaslow RA (eds). Viral Infections of Humans: Epidemiology and Control.New York: Plenum Press, 1997: pp 253±283.
3 Auwaerter PG. Infectious Mononucleosis in Middle Age. JAMA1999; 281(5): 454±459.
4 Crowcroft NS, Vyse A, Brown DWG, Strachan DP. Epidemiology ofEpstein-Barr virus infection in pre-adolescent children: application ofa new salivary method in Edinburgh, Scotland. J EpidemiolCommunity Health 1998; 52: 101±104.
5 Office of National Statistics. Health inequalities. Drever F, WhiteheadM (eds). DS No. 15. 1997. London, Government Statistical Service.
6 Fleming DM. Weekly returns service of the Royal College of GeneralPractitioners. CDPH 1999; 2(2): 96±100.
7 Hoshiba T, Asamoto A, Yabuki Y. Decreasing seropositivity ofcytomegalovirus of pregnant women in Japan. Nippon Rinsho 1998;56(1): 193±196.
8 Lee PI, Chang MH, Lee CY, Kao CL. Changing seroepidemiologicalpatterns of cytomegalovirus infection in children in Taiwan from1984 to 1989. J Med Virol 1992; 36(2): 75±78.

d
Ha1avB
ewwms(ramrtTioiIvh
*
o
V3
�
Case Reports 109
9 Rosenthal SL, Stanberry LR, Biro FM, Slaoui M, Francotte M,Koutsoukos M et al. Seroprevalence of herpes simplex virus types 1and 2 and cytomegalovirus in adolescents. J Infect Dis 1997; 24:135±139.
oi:10.1053/jinf.2002.1028, available online at http://www.idealibrary.
Serological Evidence of HRodents in
J. Groen*1, P. Koraka1, C. N. EdwardA. D. M. E. Osterhaus
1Institute of Virology, WHO Collaborating Center for Arbov
Center Rotterdam, Rotterdam, The Netherlands and 2Univ
Research, Queen Elizabeth Hospital, and Leptosp
antavirus (HV) infections were brought into thettention of western clinicians during the Korean War in951±1953, but it was not until 1978 that Leend colleagues isolated the etiologic agent Hantaanirus (the prototype of the genus Hantavirus familyunyaviridae) [1]. The natural reservoirs of HV are sev-ral rodent species (e.g. Apodemus, Rattus, Peromyscus),hich can transmit the virus to humans and have aorldwide distribution [2]. Old World HVs may causeild febrile illness (Puumala-like viruses), or moderate to
evere hemorrhagic fever with renal syndrome (HFRS)Seoul-like or Hantaan- and Dobrava-like viruses,espectively) [3]. New World HVs including Sin Nombrend Andes viruses are responsible for Hantavirus pul-onary syndrome (HPS) [3]. In Europe and Asia HVs are
elated to the HFRS syndrome, whereas in the Americashe majority of HVs belong to the HPS related viruses [3].he clinical symptoms of leptospirosis and dengue virus
nfections are comparable with the signs and symptomsf HFRS related HVs. Recently, the presence of HV
nfections among patients suspected of dengue fever inndonesia was demonstrated [4]. In this study, we pro-ide the first serological evidence of HV infections inumans and rodents in Barbados.
Please address all correspondence to: Dr Jan Groen, Institute of Virol-
gy, WHO Collaborating Center for Arboviruses and Hemorrhagic Fever
iruses, Erasmus Medical Center Rotterdam, Dr Molewaterplein 40,015GD, Rotterdam, The Netherlands. Tel.: �31(0) 104635428; Fax:
31(0) 104363441; E-mail address: [email protected] ( J. Groen).
10 Vyse AJ, Gay NJ, Slomka KJ, Morgan-Capner P, Brown DWG. Theburden of infection with HSV-1 and HSV-2 in England and Wales:implications for the changing epidemiology of genital herpes. SexTransm Inf 2000; 76(3): 183±187.
com on
antavirus in Humans andBarbados
s2, S. L. Branch2, K. O. Douglas2,1 and P. N. Levett2
iruses and Hemorrhagic Fever Viruses, Erasmus Medical
ersity of the West Indies, School of Clinical Medicine &
ira Laboratory, Ministry of Health, Barbados
Serum samples for this study were collected from69 patients admitted to the Queen Elizabeth Hospital,Barbados with signs and symptoms suggestive ofleptospirosis or dengue fever (mean days after onset ofillness 9.9, range 2±34 days), between 1 January 2000and 31 December 2000. Of these patients, nine wereconfirmed as leptospirosis cases after investigation byculture and serology as described previously [5] andwere not tested any further. Five patients had serologicalevidence of dengue infection, using the methodsdescribed previously [6], and three were positive forhepatitis B surface antigen. From the 60 patients with-out leptospirosis, scrum samples were investigated forthe presence of HV-specific IgM and IgG antibodies witha commercially available enzyme immunoassay system(Focus Technology, Cypress, USA) [7]. Positive resultswere confirmed with commercially available immuno-fluorescence slides (PROGEN BIOTECHNIK, Heidelberg,Germany) coated with Vero cells infected with Hantaanor Puumala or Seoul viruses, as previously described [8].To investigate possible reservoir hosts of HV in Barbados,75 serum samples from different animal species, 68 fromRattus norvegicus, three from Rattus rattus and four fromHerpestes auropunctatus were tested for the presence ofHV specific antibodies with IFA using anti-rat FITCconjugate (Dako, Gulstorp, Denmark) for the rat samplesand protein-A FITC labelled conjugate (Life ScienceTechnologies, Uppsala, Sweden) for the H. auropunctatus.
In 11 out of 60 patients (18%), serological analysisindicated an acute or recent infection with HV. Seven